
Abstract
Background
Despite the prevalence and challenge of Alzheimer's disease and related dementias, glimmers of hope arise during lucid moments. Caregivers, often burdened, play a crucial role. The study explored emotional responses to witnessed episodes of unexpected lucidity in deeply forgetful people, aiming to highlight the significance and varying reactions, especially among caregivers of this population.
Objective
The aim of this study was to elucidate how moments of unexpected lucidity are experienced by those who witness them, and to examine whether caregivers and non-caregivers, as well as different types of caregivers may have different emotional reactions to the episodes.
Methods
A probability-based sample representative of the United States adult population aged 40 and older with internet access was employed. 5944 respondents completed screening questions regarding whether they knew an individual with dementia and had witnessed unexpected lucidity. Close to 2000 individuals answered questions regarding their emotional reactions to witnessing unexpected lucidity, which we aimed to examine in more detail.
Results
Both caregivers and non-caregivers showed a tendency towards positive emotions in response to lucid episodes, yet negative emotions were also mentioned. We observed group differences (caregivers versus non-caregivers, different caregiver types) in the emotional responses for some of the examined emotions.
Conclusions
Caregivers can find inspiration in these fleeting moments. The research aims to guide caregivers and enhance the understanding of the enduring self-identity of deeply forgetful people, promoting compassionate care and recognizing the significance of our shared humanity.
Keywords
Introduction
As reported in the Aging, Demographics and Memory Study funded by the NIH, approximately 14% of Americans 71 years of age and older experience some form of Alzheimer's disease and related dementias (ADRD), with Alzheimer's disease comprising an estimated 70% of those cases. 1 As the deeply forgetful among us age and become less cognitively and physically adept, the negative consequences of these disease states are absorbed by caregivers. Caregiving is often thankless and sometimes characterized as burdensome. Conversely, the joys of caregiving for those with progressive and terminal neurodegenerative disease is underemphasized in the scientific literature and popular media. Without seeking to obviate the real struggles of those caring for the deeply forgetful, we seek to report their full panoply of emotional experiences when accompanying the deeply forgetful through the disease process, peppered with intermittent recall.
Specifically, throughout the illness experience of ADRD, such individuals can and do surprisingly come back into themselves as often manifested in some forms of verbal or non-verbal lucidity. These inexplicable moments of lucidity can be stimulated by deeply meaningful music, simply singing to a loved one who has become very deeply forgetful, reading a familiar poem, or connecting them with a familiar object from the past. But these moments can also be entirely spontaneous and unstimulated. These breakthrough moments of relative mental clarity in loved ones with otherwise moderate to severe dementia have been validated by caregiver reports. In this study we examine their reactions to such surprising episodes with the aim of illuminating this common experience and spotlighting the various emotions it may or may not invoke in caregivers. We are especially interested in the emotional responses of self-described primary caregivers, but we also have interest in the responses of secondary caregivers, as well as professional caregivers, and those who report having served in multiple caregiver roles.
This research about lucidity in ADRD comes amid a burgeoning milieu of studies and theoretical articles, primarily in the last five years. 2 Earlier case reports and research throughout the twentieth century tended to focus on the properly perimortem phenomenon of terminal lucidity, whereas that is now often understood to be part of the broader neurological phenomenon of paradoxical or unexpected lucidity in the context of neurodegenerative disorders. 3 Although debated, paradoxical lucidity marks the “unexpected, spontaneous, meaningful, and relevant communication or connectedness in a patient who is assumed to have permanently lost the capacity for coherent verbal or behavioral interaction due to a progressive and pathophysiologic dementing process,” as delineated by the National Institute on Aging Workshop on Lucidity in Dementia. 4 Previous research consists of case reports and small sample surveys. 5 Much of the remaining literature published on the topic focuses on methodological validity and mechanistic speculation, with glimmering hopes for an as-yet evanescent cure. 6 Finally, a more recent national prevalence study found that upwards of 44% of ADRD patients have experienced unexpected lucidity “according to observations of witnesses” (Levin J et al., unpublished manuscript).
The caregivers of “deeply forgetful people” are the fulcrum of this research, for they hold the narrative locus and key insight from these episodes as witnesses.7,8 While prior research has examined caregiver experiences in lucid episodes based on case reports and interviews, 9 there is a need to explore on a larger scale the emotions and meaning attached to the events. Our national Gallup survey focuses on the caregiver emotional responses to these episodes while precluding the selection bias that characterizes many historical case reports and summaries. We hypothesize that caregivers may find renewed meaning and inspiration when they witness these instances of lucidity, although we expect that there will be some cases in which caregivers find these episodes disturbing, sad, or productive of anxiety. While some may find renewed meaning in providing care knowing that “grandma's still there,” rather than finding the person's former self seemingly “gone,” we cannot assume that this will always be the case. 10 It is also expected that the more proximal the caregiver is to the deeply forgetful patient, the more positive their emotional response to the episode of lucidity may be. For this reason, primary caregivers were expected to have a higher proportion of positive emotions than secondary or other caregivers.
Methods
This is a survey study which is a component of a larger study about dementia (memory loss, usually among older people), how it is perceived by people, caregivers in particular, and its effects on attitudes in society, families, and individuals. The Center for Medical Humanities, Compassionate Care & Bioethics of the Renaissance School of Medicine at Stony Brook University collaborated with the Gallup Organization to develop a draft questionnaire, which served as the starting point for survey development and idea generation. This collaboration included the Institute for Studies of Religion at Baylor University as well, with the three institutions working together to create a comprehensive questionnaire aligned with their research objectives.
Survey design
The questionnaire that was developed, the Unexpected Lucidity Survey, is comprised of seven sections with a total of 55 survey items using various question formats (e.g., Likert-scale, Yes/No response, and open-ended). This research utilized data collected regarding caregiver demographic information, caregiver relationship status with the care recipient, and questions related to their unexpected lucidity experiences. Specific measures and survey questions used in this study are listed as key independent and dependent measures.
Sampling procedure
All respondents were selected from the Gallup Panel. The Gallup Panel is a probability-based panel of U.S. adults recruited using address-based sampling methods (ABS) and random digit-dial (RDD) phone interviews that cover landline and cell phones. Recruitment efforts typically oversample households predicted to have demographics needed to replace groups that tend to attrite from the panel at higher rates, including individuals with lower education levels, who are younger, and who are Black or Hispanic.
Approximately 90,000 panel members can be reached for web, mail, or telephone surveys. Another 20,000 panel members do not have email access but have provided a mailing address and can be reached for mail or telephone surveys. Members who have consented to receive text messages can also receive survey invitations or related communications via text message. Gallup maintains a database of demographic attributes on all panel members, which can be used for efficient and cost-effective sampling of low-incidence populations that would otherwise be difficult to reach. This study included members who can be reached to complete an online survey.
Sample design
The sample design for the Stony Brook Unexpected Lucidity Survey was developed to ensure a representative probability-based sample at the national level. The target population for this survey included adults ages 40 + . The Gallup Panel was used as the sampling frame.
A simple stratified sample design was employed. The Gallup panel was stratified into eighteen strata using the following stratification variables: (i) Age-group (40–64 and 65 plus), (ii) Education (High School, Some College, College Grad), and (iii) Race/Ethnicity (Hispanic, Non-Hispanic Black, and Other). Crossing the two categories of age-group, three categories of Education and three categories of Race/Ethnicity variables, a total of eighteen strata were formed.
Following a simple stratified design, samples were drawn independently and randomly from each of the eighteen strata. The sample allocation across strata was not proportional to stratum size. To ensure an adequate number of completed surveys for the Hispanic and African American groups, those groups were oversampled by allocating a higher proportion of sample sizes to the corresponding strata. Remaining strata were sampled in line with their census percentages to ensure representativeness within strata. A sampling weight was provided by Gallup to minimize the risk of bias and to project the sample data to known characteristics of the target population (adults aged 40+) which was based on the Census’ Current Population Survey's December 2022 release. Per Gallup documentation, “Population targets for people who have experienced unexpected lucidity are not available. Therefore, the full sample, including people who had experienced unexpected lucidity had not had this experience were included in the weights.” Extreme weights were trimmed by Gallup. We provide weighted estimates in the main text of this manuscript and unweighted estimates in the Supplemental Material.
Key independent measures
Respondents were asked, “Have you ever been a caregiver for a friend, family member, or any individual with dementia?” and were prompted to select all that applied from the following list of options: 1) “Yes, I have been the primary caregiver for an individual with dementia,” 2) “Yes, I have cared for an individual with dementia, but I don’t care for them every day,” 3) “Yes, I have been a professional caregiver for an individual with dementia,” and 4) “No, I have not been a caregiver to someone with dementia.” The last option was exclusive. For this study, another separate category was created to include individuals who selected multiple roles.
Dependent measures
Respondents were queried, “When you witnessed an episode of unexpected lucidity, did the experience make you feel: …” with a list of sixteen options following (see Table 2 under the “Feelings” column). Respondents were prompted to select all categories that applied. Response options included: hopeful, resilient, stressed, grateful, frustrated, loving, angry, supportive, overwhelmed, discouraged, energized, spiritual, fearful, mindful, connected to [person of interest], or other (with a text box option to specify).
Data analysis
Descriptive statistics for our sample and relevant sub-samples where distributions across a variety of sociodemographic measures along with the relationship with the person who exhibited the lucid episode were calculated. Percentage distributions of evoked feelings across several samples were computed. Furthermore, two additive scales were constructed to assess the overall emotional tone, where positive emotions and negative emotions were combined respectively. The positive emotions scale included responses of hopeful, resilient, grateful, loving, supporting, energized, spiritual, mindful, and connected. The responses to the “other” category of the list of emotions was coded qualitatively. Responses were either added to the existing categories if they were very similar to the already provided options or coded into separate categories.
Difference tests were conducted to assess whether evoked feelings differed between caregivers and non-caregivers, as well as between any of the caregiver sub-groups. Upon first glance, Stata does not allow sampling weights for their standard Chi-square, t-test, and ANOVA procedures. As such, the authors employed alternative strategies to gain weighted p-values for the difference tests shown in this manuscript. Using the svy command, used for complex sampling designs, and specifying the sampling weight (pweight in Stata) provided by Gallup, weighted Chi-square tests provided a design-based F test statistic and p-value, which were used to infer statistical significance here. For weighted t-tests, we used the lincom command to compare weighted means (we want to note that a regression-based approach yielding an F statistic would have led to the same conclusions). The F statistic reported for our positive and negative emotions scale comparisons by caregiver type stems from an OLS regression approach, using factor variable coding for the independent variable. Different software packages may employ slightly different weighting techniques and specifications. Unweighted tests are shown in the Supplemental Material and largely yielded similar results, with a few exceptions. Notably, the comparison of caregiver types and the emotion of “frustrated” indicated smaller p-values when using weighted data, and only when using weighted data did we find a statistically significant difference when examining feeling “energized.”
Supplementary analyses in addition to these difference tests were also conducted, which provide a bit more detailed information. Both unadjusted logistic and ordinary least squares (OLS) regressions were performed. Results are mentioned in the text below and results tables are shown in the Supplemental Material. In interpreting the results, we also want to urge the reader to not only consider statistical significance based on p-values, but also actual percentage and mean differences in terms of their potential clinical impacts. Furthermore, caution should be used in interpreting some of our findings for the professional caregivers and those holding multiple roles due to their relatively low sample size.
For the open-ended responses asking respondents to share their personal experiences, insights, or reflections on unexpected lucidity, the authors reviewed the responses to generate an initial coding list and categories of themes. After an initial coding list of themes was developed, the authors then independently reviewed and coded each response for all applicable themes, and the number of themes per response was determined. Discrepant coding was resolved by discussion among the study investigators.
This study was approved by the Institutional Review Board of Stony Brook University (IRB#: 2023-00040).
Results
On behalf of Stony Brook University and Baylor University, the Gallup Organization conducted research with 5944 people aged 40 and over, including 2573 individuals who have observed unexpected lucidity in a friend or family member with ADRD as indicated by their selection regarding two of three screener questions. These screening questions included: “Have you ever known someone with dementia? This could be a friend, family member, or another individual” and – after providing a definition of unexpected lucidity – “Have you ever witnessed an unexpected return of mental clarity in a family member, friend, or any individual with dementia?” Respondents were able to indicate whether they knew someone with dementia and whether they had witnessed unexpected lucidity, as well as their relationship to this person (family member, friend, another individual). For individuals who selected that they did not know anyone with dementia and that they had not witnessed unexpected lucidity, the survey was terminated. A third screening question asked respondents if they had heard about the phrase “unexpected lucidity” prior, but this question was not actually used to determine who would screen into the full survey. This survey flow is illustrated in Figure 1. The survey also gathered information about whether the respondent held a caregiver role, and if so what type. In total, the survey contains 886 cases who identified themselves as caregivers, who also constitute a key sub-sample for this study. Results from this research aim to be representative of U.S. adults over the age of 40 who have access to the internet.
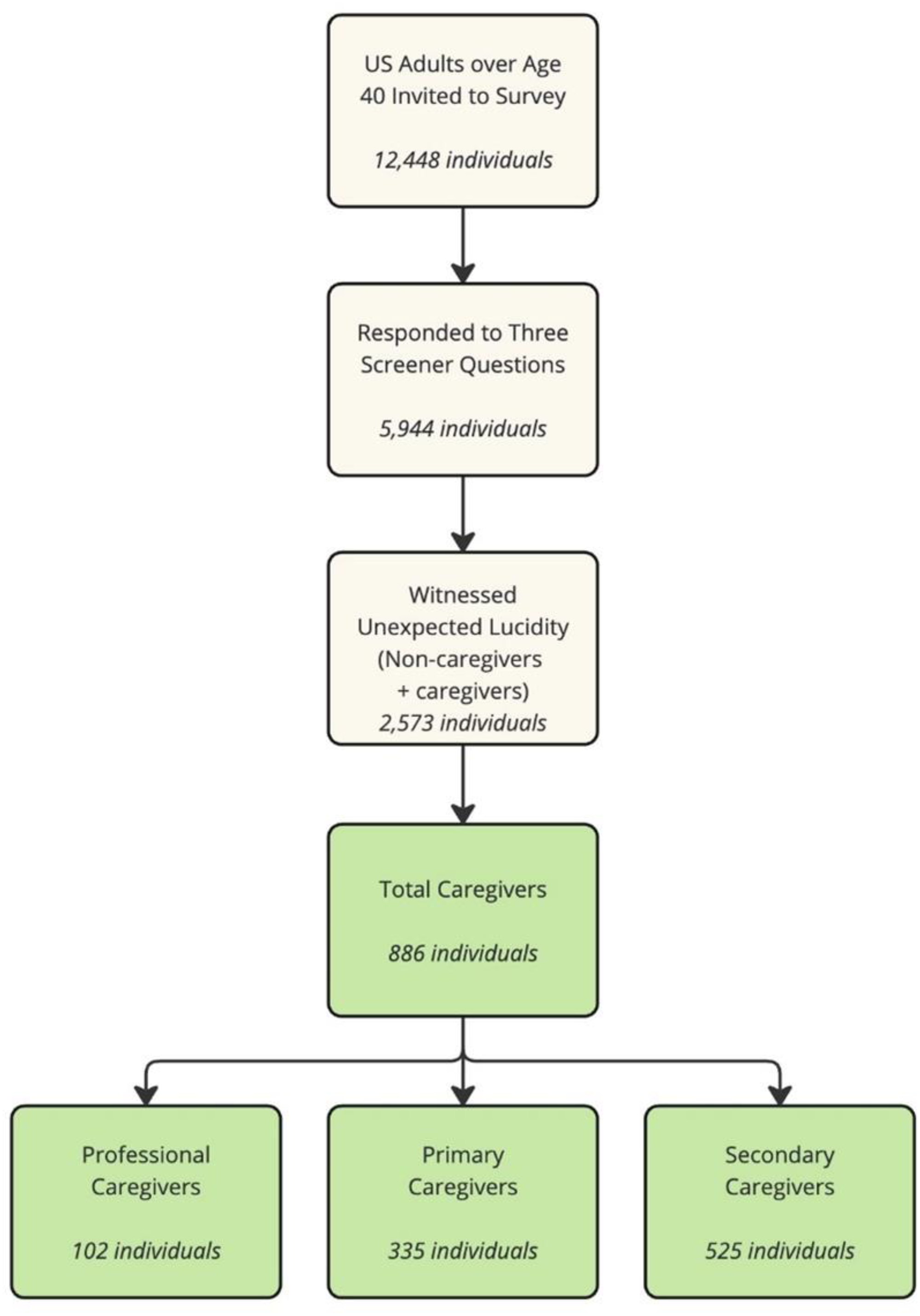
Survey progression pathway for the 2023 unexpected lucidity national survey.
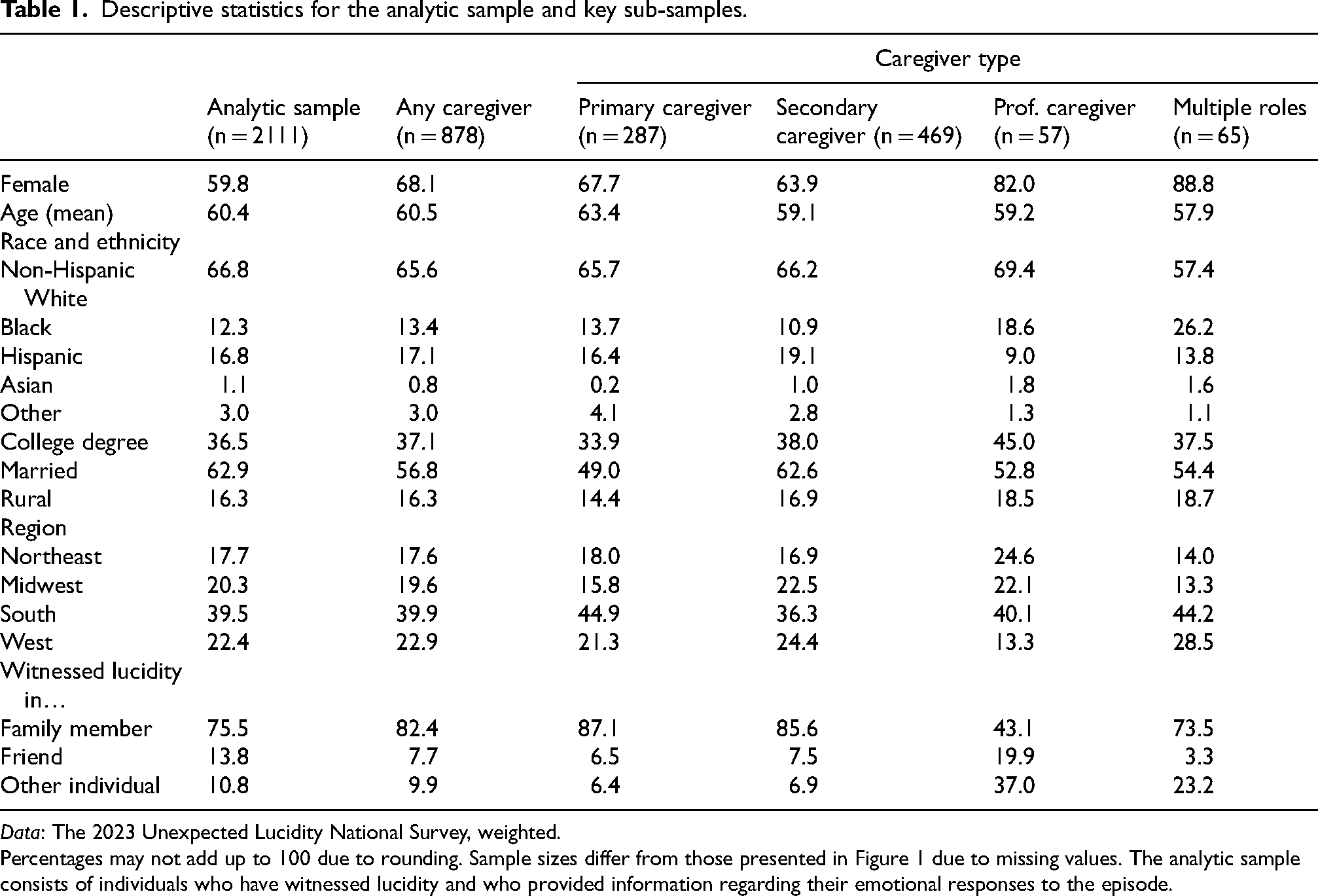
Descriptive statistics for the analytic sample and key sub-samples.
Data: The 2023 Unexpected Lucidity National Survey, weighted.
Percentages may not add up to 100 due to rounding. Sample sizes differ from those presented in Figure 1 due to missing values. The analytic sample consists of individuals who have witnessed lucidity and who provided information regarding their emotional responses to the episode.
During data cleaning, four cases were removed from the original sample since they did not meet the specifications of having personal experiences with unexpected lucidity. Of the respondents who claimed to have witnessed unexplained lucidity in another individual, 2111 answered the question of interest regarding their emotional response to the episode, constituting the analytic sample of this study, with only slightly reduced sample sizes for difference tests once those missing on the caregiver measure were excluded.
Caregiver and witness demographics
Descriptive statistics in Table 1 show that a majority of our analytic sample is female, the proportion of which increases for caregivers. The average age of respondents was close to 60 years old, with only slight deviations across caregiver categories. A majority of respondents identified themselves as non-Hispanic white (about 67%), with professional caregivers showing a higher percentage (70%) and those in multiple roles showing a lower percentage (about 57%). A significant proportion of respondents held at least a four-year college degree (36.5%), and a majority of overall respondents were married. A small share of respondents resided in rural areas of the United States (16.3%) and all four major regions of the US were represented, with the largest share of respondents stemming from the South (39.5%). Most made reference to a family member as the person who exhibited unexplained lucidity, with the exception of professional caregivers who showed a more mixed distribution.
Emotional responses in witnesses of unexpected lucidity
Figure 2 illustrates graphically the overall distribution of emotions for the whole sample (all witnesses of unexpected lucidity) sorted from most frequently selected to least frequently selected (see also Table 2, first column for unsorted distributions). The average number of emotions selected from the total 16 choices was 3.8 (median = 4, sd = 2.2, prior to qualitative coding). We observed a general pattern of positive emotions being more frequently selected compared to negative emotions, with the most commonly chosen expressions being grateful (58.7%), connected (53.4%), and supporting (47.4%). Large shares of respondents also opted for the descriptors of loving (46.1%) and hopeful (42.5%). However, a significant minority reported feeling stressed (14.1%) or overwhelmed (13%), and only 6.9% reported that the episode made them feel more resilient. Feeling discouraged or angry were the categories chosen the least. Among the qualitatively coded responses, expressions of sadness (2.2%) and joy (1%) were the most common.
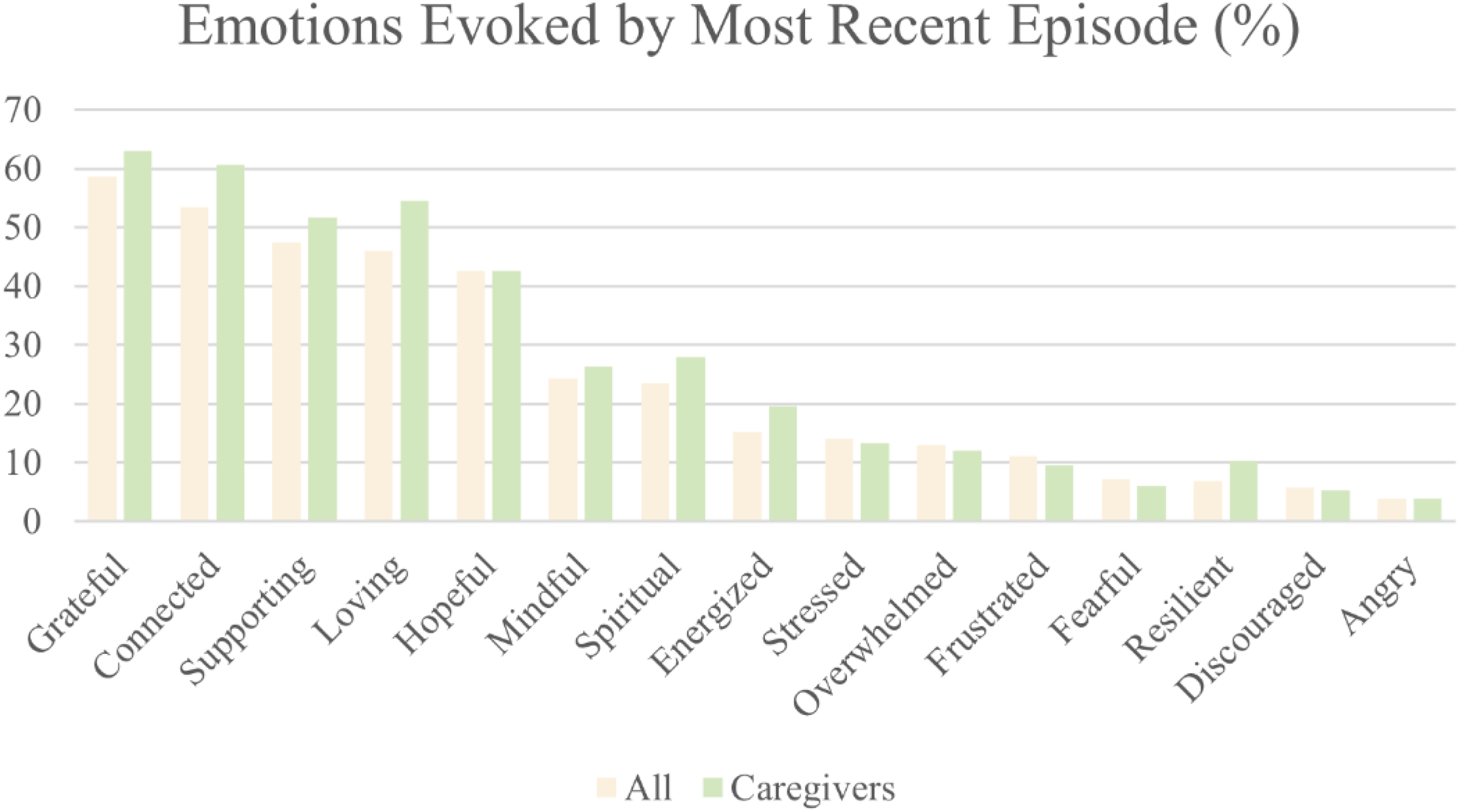
Emotions evoked by lucid episode in caregivers and U.S. general population.
Emotion distribution and differences between caregivers and non-caregivers.
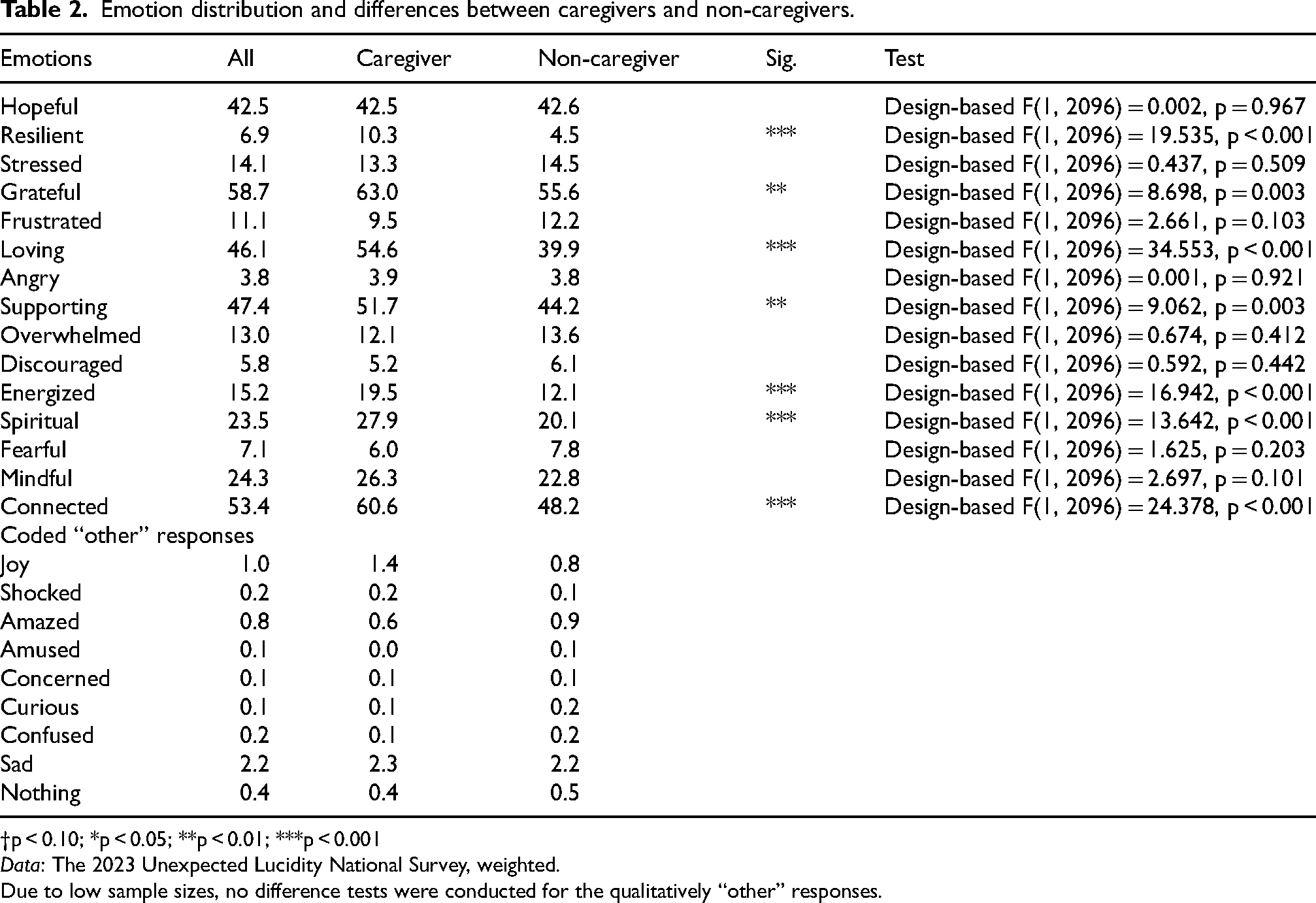
†p < 0.10; *p < 0.05; **p < 0.01; ***p < 0.001
Data: The 2023 Unexpected Lucidity National Survey, weighted.
Due to low sample sizes, no difference tests were conducted for the qualitatively “other” responses.
Emotional differences between caregivers and non-caregivers
Difference tests contrasting those holding any caregiver role with those who did not identify as caregivers (see Table 2) indicated statistically significant differences for feeling resilient (p < 0.001), grateful (p = 0.003), loving (p < 0.001), supporting (p = 0.003), energized (p < 0.001), spiritual (p < 0.001), and connected (p < 0.001). For several categories, the differences were not statistically significant or negligible. For instance, both caregivers and non-caregivers showed high rates of reporting feeling hopeful when recounting their emotional reaction to witnessing paradoxical lucidity (42.5% of caregivers compared to 42.6% of non-caregivers). The results were mirrored in supplementary analyses using logistic regression analyses, where odds ratios are shown for an alternative interpretation method for interested readers (see Supplemental Table 1). Remarkably, although not a particularly commonly chosen emotion overall, caregivers showed much greater odds of selecting “resilient” compared to non-caregivers.
Emotional differences between caregiver types
When considering differences between caregiver types (primary [n = 287], secondary [n = 469], or professional caregivers [n = 57], as well as those who selected multiple roles [n = 65]), we found statistically significant group differences for some emotions yet not for others. Comparing different types of caregivers in their emotional responses (see Table 3) indicated that statistically significant differences exist in responses of feeling “hopeful,” “frustrated,” “loving,” “supporting,” “energized,” and “mindful,” with marginally statistically significant differences for feeling “overwhelmed,” “discouraged,” and “connected,” although the finding for “discouraged” should probably be disregarded due to incredibly low sample sizes for some groups (see also supplementary analyses in Supplemental Table 2). Primary caregivers showed the highest percentage in terms of indicating feeling hopeful due to the episode (50.2%), followed by those holding multiple roles (42.1%), professional caregivers (39.4%), and secondary caregivers (38.2%). Notable differences are also evident for feeling frustrated, with primary caregivers showing the largest percentage (15.5%), while professional caregivers chose this category much less often (1.9%). Throughout all caregiver categories, significant portions of respondents selected feeling loving, with primary caregivers and multiple role holders showing both around 65%. Even the presumably less engaged secondary and professional caregivers still showed high rates of recounting this emotional response (47.2% for secondary caregivers, close to half of professional caregivers). Similarly, for feelings of “supporting” those having held multiple caregiving roles and primary caregivers showed slightly higher percentages compared to other caregiver categories.
Emotion distribution and differences across caregiver categories.
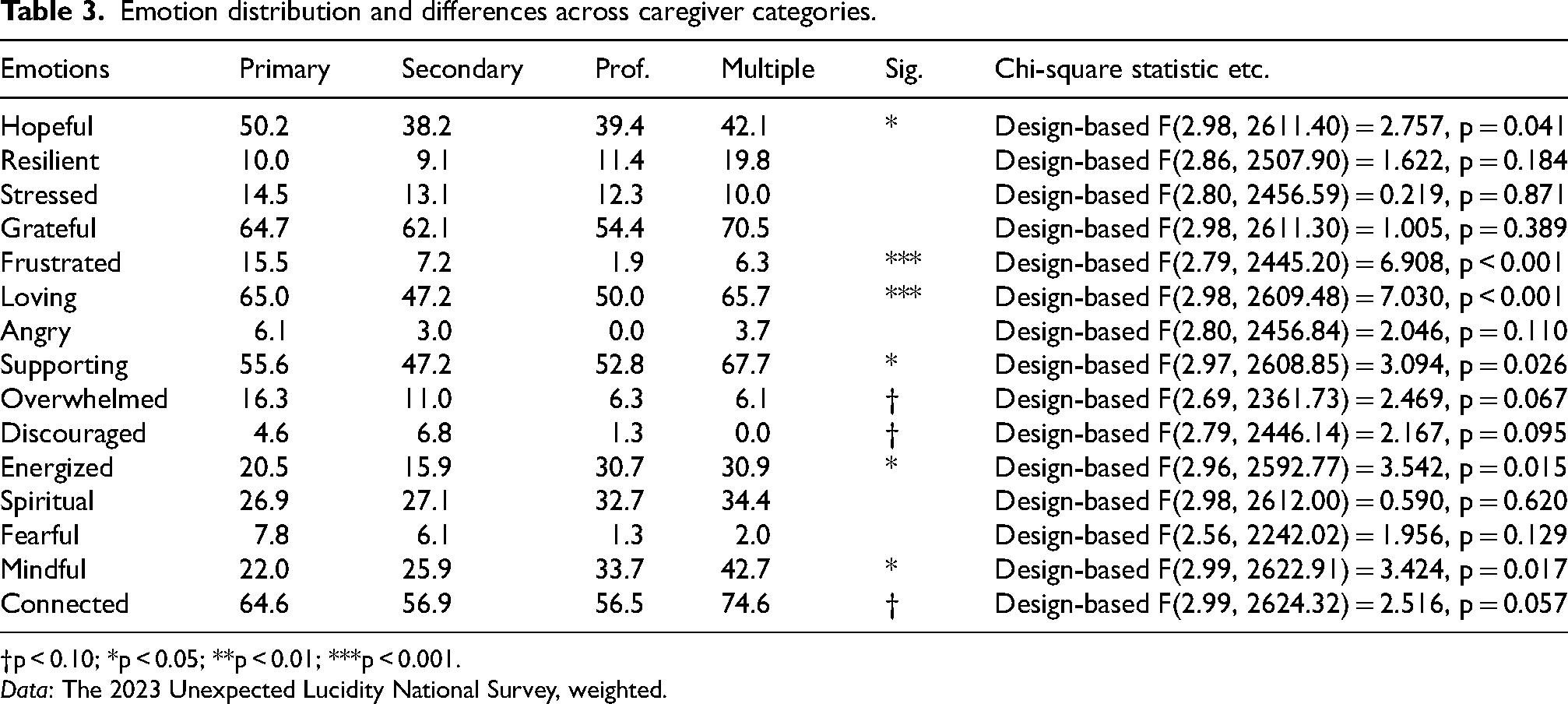
†p < 0.10; *p < 0.05; **p < 0.01; ***p < 0.001.
Data: The 2023 Unexpected Lucidity National Survey, weighted.
Yet, for feeling energized, both professional caregivers and those having held multiple caregiving roles reported feeling this emotion more often than primary or secondary caregivers. When it comes to feeling mindful, those holding multiple roles reported this feeling most frequently (42.7%), followed by professional caregivers (33.7%), secondary caregivers (25.9%), and primary caregivers (22%). This measure appears to indicate that primary caregivers are not always the most emotionally affected; other caregiver types appeared to feel mindful more often. Supplementary analyses were conducted, which were more closely targeted towards the expectation that primary caregivers would be more emotionally affected compared to other types of caregivers. Logistic regression analyses compared the odds of selecting a certain emotion for different caregivers, using primary caregivers as the reference category. Results indicated that secondary caregivers showed significantly lower odds of feeling hopeful during the witnessing of unexpected lucidity compared to primary caregivers. Additionally, both secondary and professional caregivers showed notably lower odds of selecting “frustrated” to describe their emotional impact. Secondary caregivers also appeared less affected when examining the responses of “loving” and “supporting.” Interestingly, those indicating having held multiple roles showed lower odds of feeling overwhelmed, but greater odds of feeling mindful compared to primary caregivers.
Positive, negative, and ambivalent emotions
Treating emotional responses as scales of positive or negative emotions showed that, on average, respondents selected about three positive emotions from the provided list or qualitatively coded other responses (see Table 4). Selecting a negative emotion was much rarer (mean < 1). However, about 24% of respondents selected at least one positive and one negative emotion, indicating that a significant proportion of observers may feel ambivalent emotions about witnessing an episode of unexplained lucidity. A two-sample t-test compared the mean number of positive emotions for caregivers and non-caregivers. We found a statistically significant difference in positive emotions between caregivers (mean = 3.6, sd = 2.2) and non-caregivers (mean = 2.9, sd = 1.9; t (2096) = −6.3, p < 0.001). A similar comparison for negative emotions did not yield statistically significant results at the p < 0.05 level. Testing for differences in the number of positive emotions reported for the different caregiver groups indicated that there was a statistically significant difference (F(3, 874) = 5.75, p < 0.001). The percentages for these groups showed slightly higher means for primary caregivers and for those holding multiple roles than for secondary and professional caregivers. Supplementary analyses based on OLS regression results (see Supplemental Table 3) indicated that, on average, secondary caregivers were expected to select about 0.5 fewer positive emotions compared to primary caregivers (p = 0.004), while having held multiple roles, in contrast to only being a primary caregiver, showed a marginally statistically significant positive association with reporting positive emotions, where we would expect these individuals to report on average about 0.69 more positive emotions compared to primary caregivers. Moreover, we observed differences when examining negative emotions across caregiver groups (p < 0.001). Based on regression analyses, professional caregivers are expected to, on average, select 0.42 fewer negative emotions compared to primary caregivers (p = 0.001), and those holding multiple roles are expected to select 0.37 fewer negative emotions in contrast to primary caregivers (p = 0.003). The regression analyses also indicate, however, that in terms of effect sizes, caregiver type may have quite modest explanatory power regarding the number of positive or negative emotions selected (see standardized coefficients and R-squared values).
Positive, negative, and ambivalent emotions across caregiver categories.
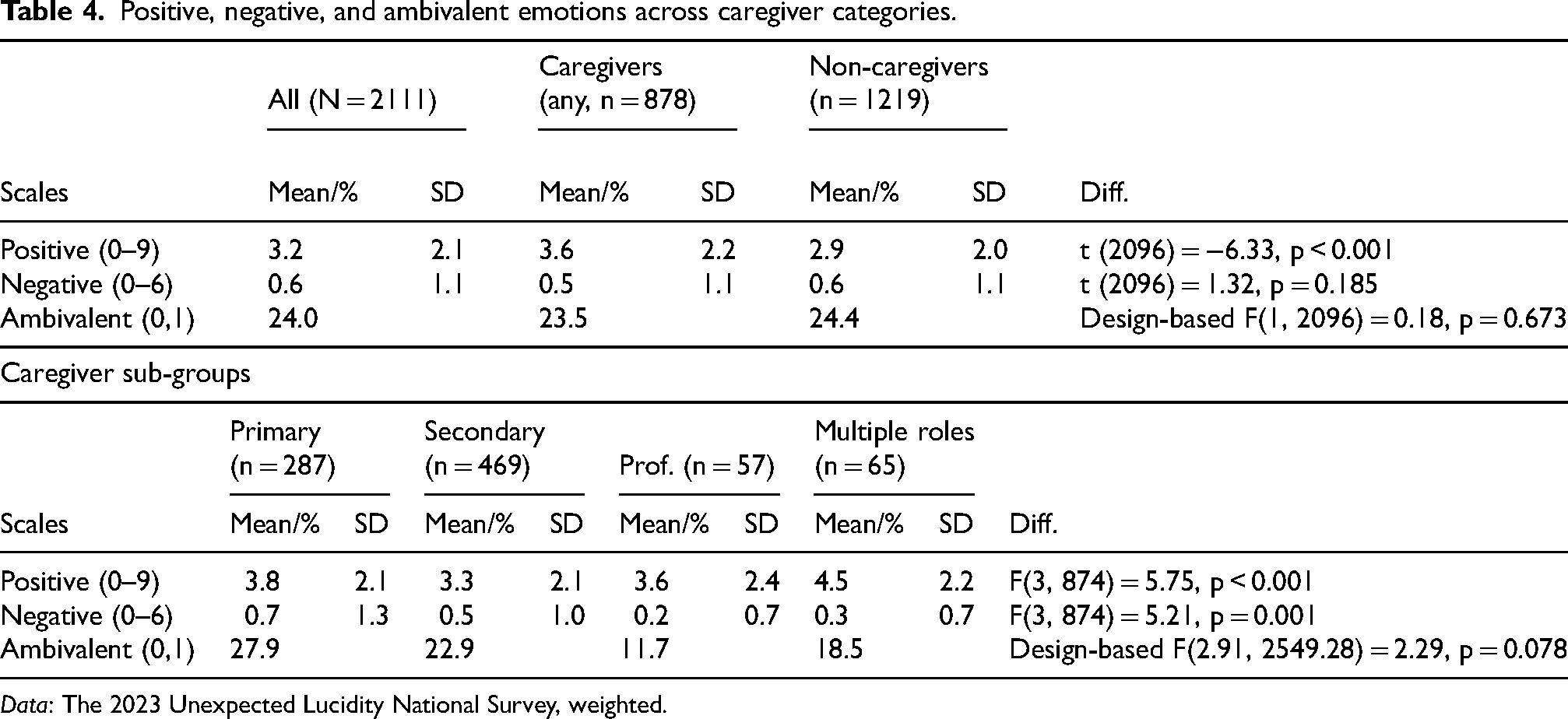
Data: The 2023 Unexpected Lucidity National Survey, weighted.
Experiences, insights, and reflections on unexpected lucidity
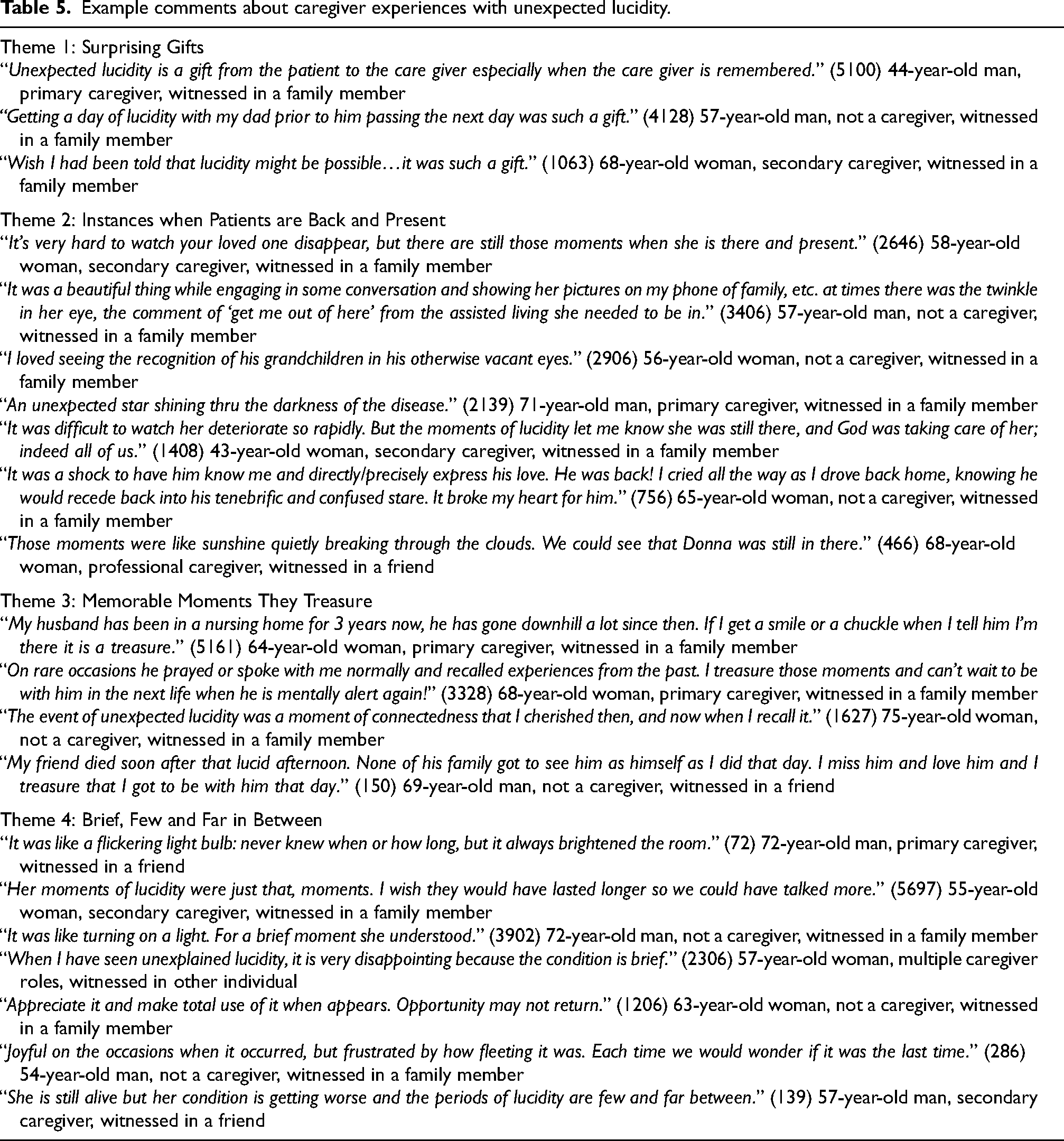
When asked to share additional comments and thoughts about their experiences with unexpected lucidity, four major themes were identified from the analysis of open-ended texts provided by the respondents. Overall, respondents perceived their unexpected lucidity experiences as: (a) surprising gifts, (b) instances when patients are back and present, (c) memorable moments they treasure, and (d) brief, few and far in between. The themes are illustrated with example comments in Table 5.
Example comments about caregiver experiences with unexpected lucidity.
Discussion
This paper draws on a national survey of U.S. adults that examined the lucidity phenomenon and the accompanying experiences of those who identify as caregivers, in whatever capacity. Caregivers for those with ADRD experience a variety of emotions in response to their witnessing episodes of surprising or unexpected lucidity in their loved one. The survey was administered by the Gallup Organization in mid-2023 but spans a full year in collaboration with Gallup as we developed a set of survey questions and pilot tested them over a period of several months. This project is shaped around the hypothesis that, for the most part, caregivers who witness such episodes of relative lucidity in loved ones — whom they may have considered to be entirely “gone” — may find hope and purpose in this renewal of the formerly known identity, however fleeting this experience. 11
The phenomenon of unexpected lucidity in ADRD
Anecdotally, these episodes of unexpected lucidity are quite common even very deep into the progression of something as severe as Alzheimer's disease. The National Institute on Aging of the NIH has supported research into these brief periods in the hopes of learning more about dementia and how to ameliorate it.12,13 This project continues the work at the interface of spirituality, meaning and caregiver morale or mindset as initiated in Post's book Dignity for Deeply Forgetful People: How Caregivers Can Meet the Challenges of Alzheimer's Disease (Johns Hopkins University Press, June 2022). 10 To our knowledge, this was the first national survey on the topic, and provides many insights into the prevalence, duration, nature, and meaning for these special moments of clarity, during which time the deeply forgetful person returns briefly to some degree of communication, verbal or non-verbal. Again, these moments can be unstimulated or occur spontaneously.
Caregiver applications
We have presented the self-reported emotional responses of caregivers to these episodes in the hope of understanding their effects on caregivers more fully, as this will help us develop an educational intervention that prepares future caregivers for these complex experiences. The main objective has been to inventory of emotional responses and investigate how this conveys an underlying continuity of the whole self–that may be relatively opaque most of the time–or may return either sporadically or by stimulation, and to teach the caregiver that their loved one is not gone, is not without value or dignity.
We acknowledge that caregiving is generally challenging and full of emotional adjustments. However, we propose that hope, meaning, and resilience are related to the sense of continuing underlying self. While episodes of lucidity in the context of moderate to severe dementia are brief, they clearly have an emotional impact on caregivers. By far the more common responses are emotionally positive. For example, the majority of caregivers are inspired by these episodes, however brief they may be (Figure 2). We assume that these positive responses sustain caregivers because they enhance their sense of purpose and meaning. In other words, they find hope in these surprising episodes of lucidity in the sense that the affected individual is not “gone,” “empty,” a “shell,” or a “husk,” to use metaphors that are commonly applied to individuals assumed to be otherwise obtunded.
There are a minority of caregivers who report negative emotions, such as stress and frustration associated with these episodes. These adverse reactions point both to the reality of lucid turnarounds and to the sense of loss that may be experienced by some caregivers, sometimes relating to a feeling of ‘whiplash’ as the generally brief episodes fade (see Table 5). A common theme this minority reports is that these experiences are fleeting and therefore somewhat frustrating. The inevitably transient nature of these lucid events is no reason to view them negatively, as most respondents indicate.
We think that the dignity with which these affected individuals are treated depends on caregivers being encouraged to notice these hints of continuing self-identity as exposed in these episodes. This is very significant for caregiver well-being because, as we learn about the emotional responses that caregivers have to these events, we can design educational interventions that will a) help them observe and appreciate continuing self-identity, b) include techniques to stimulate these episodes and thus maintain their sense of purpose and emotional wellbeing, and c) be mindful of how caregivers can be prepared for these events in such a way as not to be shocked by them, startled, or negatively affected by the inevitability of their fleeting nature, as some have reported. These experiences may be transient, but they are deeply meaningful to most caregivers, because they realize that the affected individual is not simply a useless husk or ‘life unworthy of life.’ Rather they can be included in a shared humanity and affirmed as such because despite the loss of communicative capacity and the opaqueness of this underlying identity, these individuals are still human beings with consciousness and can be appreciated as such. 14 Linear rationality, rationality found in action, may be gone; however, the more important form of rationality is symbolic, which is the rationality of realizing that one's self-identity is connected with certain symbols and artifacts that are meaningful over the course of a lifetime. 15 Ethically speaking, as Post has argued at length, symbolic rationality–which is the rationality not of “what I do” but of “who I am”–is what is most important. In a relatively “hypercognitive” culture, 11 one would expect more than a minority of respondents not to have experienced these episodes in a positive light.
Conclusion
The data for this study stem from a national survey of the American public and the American caregiver as implemented by the Gallup Organization, a paragon of excellence in large survey research. To our knowledge, nothing like this project has yet been conducted in research on the experience of deeply forgetful people as witnessed by their primary, secondary, and professional caregivers. The study at hand investigated how moments of unexpected lucidity as exhibited by deeply forgetful people are perceived emotionally by those who witness them, and especially whether primary caregivers may show stronger emotional responses compared to other caregivers or non-caregivers. What we have uncovered has great significance for the future of caregiving. We have established that, while caregiving may be burdensome and inevitably challenging, in most cases where episodes of lucidity are observed there is a dynamic of realistic hope because caregivers are able to see that their loved ones are more than husks, shells, empty and gone. Therefore, their actions of love and care are profoundly important as we seek to engage inclusively with our shared humanity. We aspire to use these findings to inform and educate both family and professional caregivers worldwide regarding the varied responses to episodes of lucidity as well as to encourage them to notice these moments with interest and appreciation. Because these episodes shape the emotional experiences of caregivers predominately in a positive way, further research is needed to understand how to educate caregivers to promote their wellbeing. We suggest that in-depth interviews of caregivers who have witnessed episodes of unexpected lucidity may be especially revealing.
Limitations
Despite garnering crucial new insights, we also want to note limitations to this study. First, survey respondents are subject to recall bias. The time since the lucid episode was witnessed differed between respondents, as does the level of closeness between the observer and the person with ADRD. This may have impacted the information respondents were able to provide. Second, this survey was fielded in the United States and results are not generalizable to other national contexts. For instance, attitudes toward individuals with ADRD and prevalence of caregiving by family members may differ between cultures. How lucid episodes are interpreted could also vary between cultures, which could influence subsequent emotional responses by witnesses. More research is needed in this area. Third, the survey's main aim was to gather in- depth information from one observer of lucidity about one individual with ADRD exhibiting lucid episodes. Some respondents may have known multiple individuals exhibiting lucid episodes (e.g., professional caregivers), but the survey made reference to only one individual who was identified by initials or a nickname chosen by the respondent. We did not provide the option to fill out the full survey in reference to multiple individuals, as this would have made the time to complete the assessment exceedingly long. Fourth, bias may have been introduced by listing more positive than negative emotions in the survey prompts, yet we hope that this may have been at least partially mitigated by the option to specify an “other” emotion and to clarify with a text response. More dialogue is needed to gather insights from family and professional caregivers, in order to properly understanding the significance and value of their perspectives.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241297149 - Supplemental material for Lucidity in deeply forgetful people: A national U.S. survey of caregivers’ reactions
Supplemental material, sj-docx-1-alz-10.1177_13872877241297149 for Lucidity in deeply forgetful people: A national U.S. survey of caregivers’ reactions by Stephen G Post, John Paul Ross, Rebecca Bonhag and Wei-Hsin Lu in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
The authors would like to thank our colleagues in the Center for Medical Humanities, Compassionate Care, & Bioethics at Stony Brook University, including April Bortzfield, MSEd. We would like to thank our colleagues at Baylor University as well, including Byron Johnson, PhD of the Institute for Studies of Religion, who contributed to the design of the study, and Jeff Levin, PhD, MPH, of the Medical Humanities Program at Baylor University and the Department of Psychiatry and Behavioral Sciences, Duke University School of Medicine. We would also like to thank Dr Rodney X. Sturdivant from the Statistical Consulting Center at Baylor University for his advice. Finally, we would like to express our gratitude to the tireless effort of the statisticians at the Gallup Organization for their preparation of the raw data and methodology report, and especially Luke Natzke and Drew Curtis for their consultative services.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors would like to thank an anonymous donor.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: John Ross is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available within the article and/or its supplemental material.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.