
Abstract
Background
Assessing consciousness might benefit the care for people with Alzheimer's disease and other types of dementia at the end of life by indicating distressing symptoms and moments of awareness. This could guide symptom control and increase interaction with the person with dementia.
Objective
This study aims to investigate the acceptability of a biosignal measurement of consciousness, the Bispectral Index monitoring (BIS), for persons with dementia at the end of life.
Methods
Qualitative study using focus groups and interviews with demonstrations of BIS monitoring, with 17 individuals with dementia and 24 family caregivers. Qualitative content analysis was based on the theoretical framework of acceptability.
Results
People with dementia did not find BIS monitoring bothersome, yet acceptability varied across participants and situations. Family caregivers considered BIS acceptable for medical situations such as palliative sedation and pain assessment. Perceived effectiveness, ethicality, and usefulness considerations underpinned reasons and concerns around acceptability.
Conclusions
Potential end-users expressed diverse attitudes towards BIS monitoring in dementia end-of-life care. If BIS or similar technologies are to be implemented in the future, care must be taken to ensure that the device has sufficient added value, that the person with dementia and family are well informed, and that the technology does not replace human care. Future research should investigate its efficacy and feasibility in the situations that were deemed acceptable.
Keywords
Introduction
Monitoring the level of consciousness of people with dementia may help maximize comfort and improve their quality of life at the end of life. End of life with dementia includes people in a comatose state and those with severely impaired decision-making, although controversy on this definition is ongoing.1,2 In this state, self-reporting of distressing symptoms is often no longer possible, while as many as 63% of people with dementia in palliative care and between 22% and 85% of people with dementia in nursing homes may be in pain.3,4 A change in consciousness may be used as an indicator of possible discomfort and guide symptom control. 5 Moreover, identifying moments of awareness, 6 which are often unexpected,7,8 may provide valuable opportunities to engage with people with advanced dementia. 7
Currently, evaluation of consciousness is mainly based on clinical observation. 9 Although observational scales are reliable in the end-of-life care context, 10 their validity is questioned. 11 For example, people in palliative care who are evaluated as being unconscious based on the rating of these scales, may actually still be conscious enough to experience discomfort. 12 Researchers question the accuracy and objectivity of observation because the signs of consciousness in this population are often subtle and unclear. 13 Objective, valid measurement of biosignals of consciousness using portable devices identified in a recent review 14 may provide an alternative option.
One potentially useful technology to measure consciousness is the Bispectral Index (BIS) monitor. BIS measures neuromuscular and superficial cortical activity through electrodes placed on the forehead. Its main variable, the BIS index, consists of a single number computed from a complex algorithmic equation based on the electroencephalography (EEG) data of a large sample of healthy adult subjects undergoing general anesthesia. 15 Its value can range from 0 (complete EEG suppression) to 100 (fully awake). This non-invasive, bedside technology is routinely used during surgery to monitor the depth of anesthesia and is found to be acceptable and potentially useful for palliative sedation to detect discomfort and help titrate the medication.16–18 The BIS index scores showed more variations in lower levels of consciousness compared to observational scales that had only one or two categories,19,20 indicating that BIS may be better at discriminating levels of consciousness in deeper sedation.
Research on the use of BIS monitoring with people with dementia is limited. One study showed that the baseline BIS level for people with dementia was lower, 21 but the effect of sedatives on the decline of BIS index was similar to people without dementia. 22 The feasibility of BIS monitoring has been demonstrated in people with severe dementia during dental treatment with sedation, 23 and it was generally tolerated by nursing home residents. 24 Thus, there is potential for the use of BIS monitoring in people with dementia.
However, it is not known whether people with dementia and their family caregivers are interested in, or would find it relevant or even acceptable, to apply BIS monitoring in end-of-life care for people with dementia. It is crucial to systematically examine the attitudes of stakeholders before deciding whether to devote more resources to validating and implementing the device in this setting.25–27 In this study, the theoretical framework of acceptability (TFA) developed by Sekhon and colleagues 25 was used to assess the acceptability of the application of BIS monitoring in various situations in end-of-life care for people with dementia. TFA is the first comprehensive framework for healthcare interventions developed based on an umbrella review. It consists of seven component constructs: 1) affective attitude, 2) burden, 3) perceived effectiveness, 4) ethicality, 5) intervention coherence, 6) opportunity costs, and 7) self-efficacy. According to TFA, acceptability can be examined before the person participates in an intervention (prospective), during the intervention (concurrent), and after going through the intervention (retrospective).
This study examines the prospective acceptability of BIS monitoring at the end of life of people with dementia from the perspective of people with dementia and their family caregivers. We investigate in which situations it is considered acceptable and why.
Methods
Study design
In this qualitative study, focus groups and interviews were conducted between August 2022 and January 2023 with family caregivers and people with dementia. Focus groups were chosen because the study aimed to gain an understanding of collective attitudes, and the group dynamic may stimulate more diversity in opinions.28,29 To maximize participation of people with dementia, a few people with dementia were interviewed individually or in pairs instead of collectively in the focus group setting. This research was grounded in a constructivist paradigm, aimed at understanding the subjective opinions of the participants and taking into account the situation and lens of the researchers. 30 The COREQ guideline was followed to report this study. 31
Participants
Participants were people with dementia, current family caregivers, and former family caregivers. All participants provided informed consent for this study. Current family caregivers were included because they represent the population that would be involved in decision-making regarding the actual implementation of BIS monitoring for people with dementia. Former family caregivers could contribute to the discussion with their experience of situations at the end of life, when the level of consciousness was not clear. All participants had decision-making capacity. In order to take part in the study, people with dementia needed to be aware of their dementia diagnosis and have enough language, memory and hearing abilities to participate in an interview or group discussion in Dutch. Current family caregivers had to provide care to a person living with dementia for at least two hours a month. Former family caregivers had to have provided care to a person with dementia who died within the past five years. These criteria were included in the informed consent form.
Family caregivers were recruited through the Dutch Alzheimer's Association and the University Network of the Care Sector South Holland (UNC-ZH) academic long-term care network. Current and former caregivers who were registered at the Dutch Alzheimer's Association panel received an invitation from the association asking their permission to be approached by the researchers. The researchers then sent an email about the study and the informed consent form to those who were interested, followed by a phone call to address any questions. Additionally, former family caregivers were approached by healthcare professionals affiliated with the long-term care network. Healthcare professionals contacted potential participants via phone or email and sent them the information letters with informed consent forms. For the recruitment of people with dementia, researchers first contacted healthcare professionals who worked at daycare programs of institutions associated with the long-term care network. People with dementia who attended these programs were approached in person by the researchers or healthcare professionals. Participants and healthcare professionals who helped with the recruitment were informed of the inclusion criteria in order to assess eligibility. All participants were encouraged to contact the research team if they had any questions. Recruitment stopped when the research team involved in data collection (XJ, HS, JTS, and students) agreed that no new information related to the research questions emerged from the last focus group. Data saturation on the code level was confirmed later during data analysis: 99% of the codes were generated before the last focus group, which was with persons with dementia. 32
Procedures
Each focus group had one main moderator and one researcher supporting the process. One focus group was conducted by a single researcher due to unforeseen circumstances. Focus groups were scheduled to last 90 min, including a short break. Individual or duo interviews were conducted by a single researcher and aimed to last no longer than 60 min. The moderators and interviewers included experienced female researchers with a background in psychology (HS, XJ) or epidemiology (JTS) and experience in qualitative research, female master students with a background in psychology, and a male master student in medicine. They all received training in conducting interviews and focus groups. Focus groups and interviews were performed face-to-face as much as possible, in long-term care facilities (n = 6), conference centers (n = 2), or the home of the person with dementia (n = 1). One focus group with family caregivers was conducted online to include participants who were not able to participate in face-to-face groups. In the majority of the focus groups and interviews, only the participants and researchers were present. In one interview a family member was present to support the person with dementia. During one focus group at a daycare center, a few other people with dementia and two staff members were in the same large room due to limited space. They conducted quiet activities on their own and did not participate in the focus group.
A semi-structured topic guide (Supplemental Material) and standard operating procedure (SOP) were developed. There were slight differences between the guide and SOP for people with dementia and those for family caregivers. In the initial plan, current and former caregivers were to participate in separate focus groups, so everyone could feel free to express their opinions to people in similar situations and so current caregivers would not be confronted with distressing experiences of former caregivers around the death of the relative with dementia. However, some groups were mixed due to a misunderstanding about whether the relative with dementia was still alive. Despite initial concerns, no negative experiences were reported from the first mixed group. Instead, the input from different perspectives led to lively discussion. As a result, the study team decided to no longer separate the two groups for easier logistics.
All focus groups and interviews started with an introduction round and the researchers explaining the aims of study and their roles within the meeting. Participants were asked whether there were situations in which they would like to know the consciousness level of people with dementia. The BIS device was then demonstrated, either live or with an instruction video. Researchers explained that the BIS device monitors brain activity, which indicates the level of consciousness. They also mentioned that it is already being used during surgery. In most face-to-face focus groups and interviews participants had the opportunity to try on the BIS monitor and share their experiences and first impressions of the device. If the device produced a beeping sound, researchers explained this indicated that the signal quality from the sensors was inadequate. For family caregivers, additional questions were asked about the advantages and disadvantages of BIS monitoring for people with dementia. Next, participants were asked in what situations they would find the use of BIS acceptable to monitor consciousness of people with dementia. The research team provided five standard situations, which were generated based on past research and the functionality of BIS monitors. The situations included during natural sleep of people with dementia, recovering from surgery in the hospital, severe dementia in the nursing home, the last days/hours of life, and palliative sedation. Participants were also encouraged to suggest other situations. To stimulate discussion, the proposed situations were not restricted to the end of life or a specific setting. In order to minimize experiences of failure, all situations proposed by the participants, no matter whether they were realistic for BIS monitors or not, were noted and subsequently discussed in the focus groups. Finally, each situation that was mentioned was displayed on one poster or screen and participants were invited to indicate whether they considered BIS monitoring acceptable by sticking colored post-it notes (red = not acceptable, green = acceptable) on the posters, voting online or replying verbally. After that, they elaborated on their opinions.
The focus groups and interviews were audio recorded and transcribed verbatim. Field notes were made by the assistants during the focus group and interview about the acceptability of the situations. Immediately afterwards, salient observations and reflections of the researchers on the interaction with participants were discussed between the moderator and assistant and added to the field notes. Member checking was not performed.
All participants completed a brief demographics questionnaire before or immediately after the focus group or interview. Care providers of the day centers helped complete the demographics for some participants with dementia. (Former) family caregivers also provided the demographic data of their (deceased) relatives with dementia.
Data analysis
The number of stickers or votes for each BIS monitoring situation were counted and recorded in the field notes. The opinions of people with dementia were derived from their answers in the transcripts, as they did not always manage to use sticky notes to indicate their preference. Situations proposed by the participants which were similar but phrased differently across the groups were combined during the analysis. Since many situations were generated, they were grouped into day-to-day and medical situations, depending on whether the situation was related to medical procedures, symptom assessment, and medical decision-making.
The transcripts were analyzed using combined inductive and deductive approaches of qualitative content analysis, addressing the question as to why participants considered BIS monitoring (not) acceptable.33,34 After open coding, the codes were grouped according to TFA. 25 An initial structure of the code tree was established based on the research questions and impressions from the data and observations. This was discussed between XJ, HS, JTS, and a female master student in medicine. Open coding was then conducted by XJ and the female master student to capture as much as possible the meanings conveyed by the participants. The two researchers independently coded one focus group of family caregivers and generated initial codes. They discussed any discrepancies and reached consensus on the code book. The codes were organized into groups such as pros, cons, and suggestions. The code book was checked by HS and JTS for clarity. XJ and YS independently coded the first focus group again based on this code book and reached consensus. They subsequently coded the other focus groups and interviews independently and held consensus meetings per two or three transcripts. During the consensus meetings, they discussed their differences in coding until they reached agreement and modified the codes and groups in the code book. Atlas.ti 22 (Scientific Software Development GmbH, Berlin) was used to support the coding. After all the data were coded, XJ grouped the codes in categories largely based on TFA. 25 When the theory did not fit the data, new categories were constructed, or the interpretation of existing categories was modified. This analysis was discussed with HS and JTS. The data from the field notes were also summarized under corresponding categories.
Ethical considerations
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and later amendments. All participants signed an informed consent form. People with dementia were encouraged to discuss participation in the study with healthcare professionals and their family caregivers before deciding whether to participate. All participants were informed that they would each receive a gift card of 20 euros. In practice, 13 people with dementia received gift cards worth 24 euros which were available at the time. The study was deemed exempt from the Dutch Medical Research Involving Human Subjects Act (WMO) by the ethics commission for non-WMO studies Leiden University Medical Center Division 3 (reference No. 22-3004, 04-04-2022).
Results
Demographics
Seventeen people with dementia participated in three face-to-face focus groups and two interviews. To overcome a language barrier, one participant was interviewed in the presence of his family caregiver for language support. Two other participants were interviewed together. Twelve current caregivers and 12 former caregivers participated in four face-to-face focus groups and one online focus group. An additional three current caregivers withdrew before the focus groups, due to personal issues (n = 2) or an unspecified reason (n = 1). Focus groups lasted between approximately 80 and 120 min. Focus groups with family caregivers took longer than those with people with dementia. Interviews lasted between 46 and 61 min. Table 1 presents the sample characteristics.
Sample characteristics.
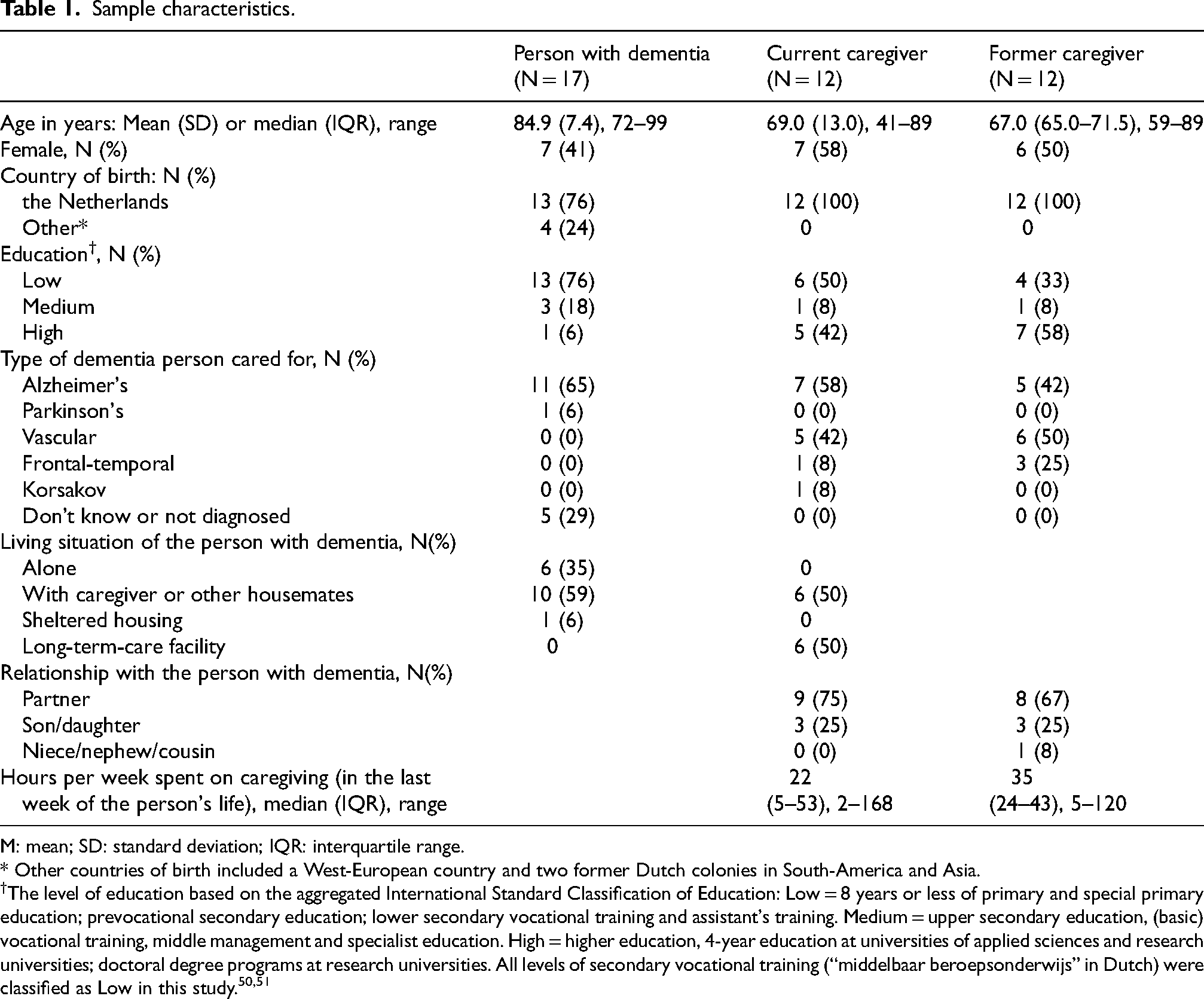
M: mean; SD: standard deviation; IQR: interquartile range.
* Other countries of birth included a West-European country and two former Dutch colonies in South-America and Asia.
The level of education based on the aggregated International Standard Classification of Education: Low = 8 years or less of primary and special primary education; prevocational secondary education; lower secondary vocational training and assistant's training. Medium = upper secondary education, (basic) vocational training, middle management and specialist education. High = higher education, 4-year education at universities of applied sciences and research universities; doctoral degree programs at research universities. All levels of secondary vocational training (“middelbaar beroepsonderwijs” in Dutch) were classified as Low in this study.50,51
The former family caregivers reported the death of the persons with dementia occurred on average 26.7 months before the study (SD 17.5, range 8–54 months). Three of the current caregivers were caring for a relative with dementia born outside the Netherlands (two from West-European countries, one from South Asia). Half of the current caregivers indicated the person with dementia was able to express pain or discomfort, and a third of former caregivers reported their ability to do so in the last week of life. Based on the remarks in the questionnaire, however, it is worth noting that not all caregivers were certain about the accuracy of their observation of discomfort in their relatives.
When BIS monitoring is considered acceptable
Situations for possible use of the BIS monitor in dementia care and their acceptability are presented in Table 2. A number of day-to-day and medical situations were suggested by participants. These suggested applications mostly aimed at ensuring the comfort of people with dementia, improving contact with them, and informing medical decisions. People with dementia suggested fewer applications than family caregivers.
Acceptability of bispectual Index monitoring in specific situations in palliative care for dementia.
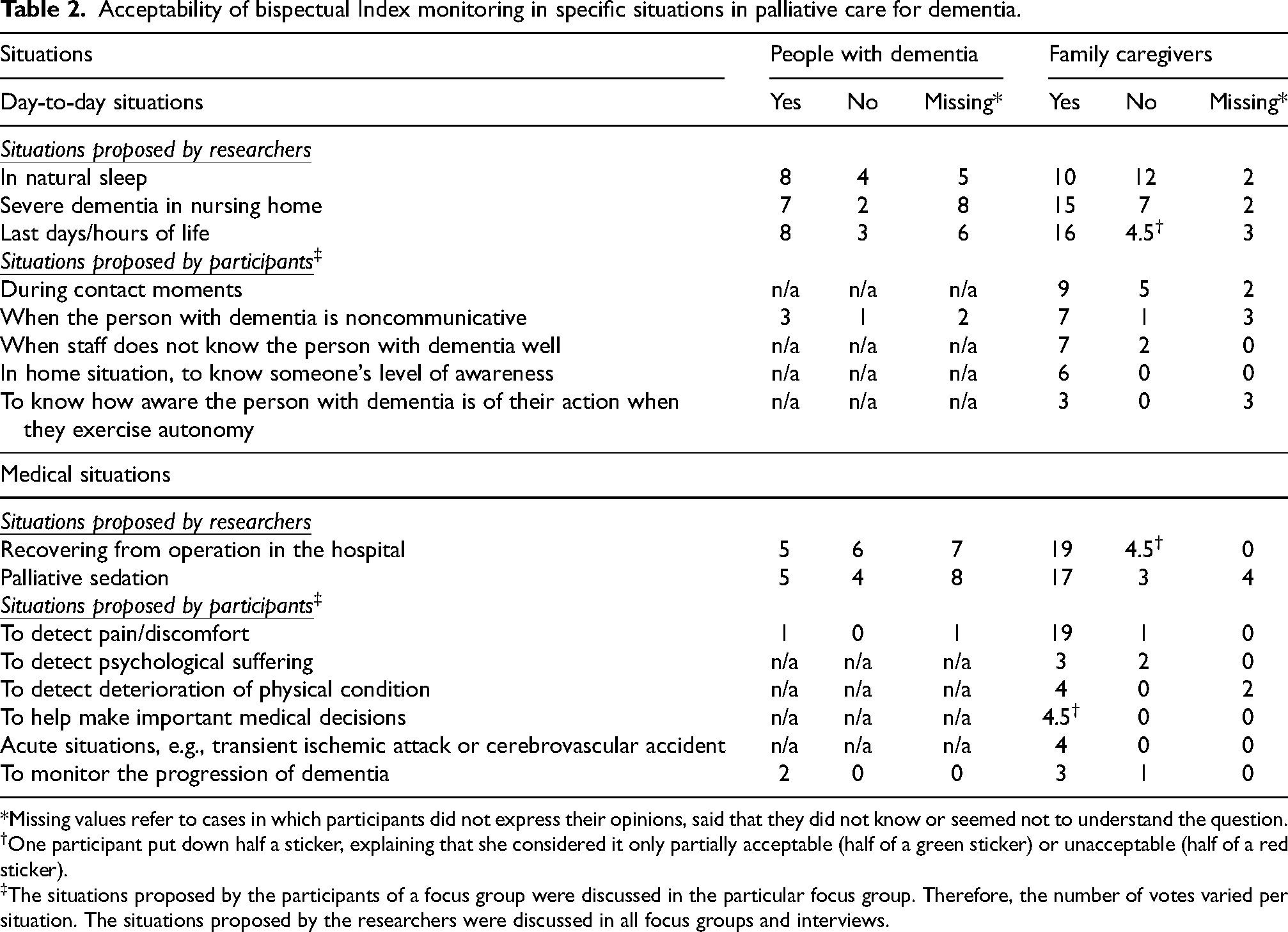
*Missing values refer to cases in which participants did not express their opinions, said that they did not know or seemed not to understand the question.
†One participant put down half a sticker, explaining that she considered it only partially acceptable (half of a green sticker) or unacceptable (half of a red sticker).
The situations proposed by the participants of a focus group were discussed in the particular focus group. Therefore, the number of votes varied per situation. The situations proposed by the researchers were discussed in all focus groups and interviews.
The acceptability of BIS monitoring differed depending on the situation. Around half of the people with dementia could not understand or imagine the situations or express an opinion on acceptability. The other participants with dementia had diverse opinions. The majority of participants considered BIS monitoring acceptable in day-to-day situations, while the acceptability was more controversial in medical situations. As for family caregivers, they generally considered BIS monitoring acceptable in most situations discussed, especially in medical situations such as when the person with dementia is recovering from surgery in the hospital or using the device to detect pain and discomfort. Opinions differed regarding the use of BIS in day-to-day situations, for example to monitor natural sleep or people with severe dementia in the nursing home. The situations proposed by other participants were deemed acceptable by a larger proportion of participants compared to those suggested by the researchers. In total, 39 (41%) votes by people with dementia across all situations were acceptable, 20 (21%) unacceptable, and 37 (39%) were missing. For family caregivers, the votes were 146.5 (70%) acceptable, 43 (20%) not acceptable, and 21 (10%) missing.
Why BIS monitoring is considered (not) acceptable
The opinions regarding the acceptability of BIS monitoring are summarized in Table 3. They were categorized according to the TFA domains, including affective attitude, burden, ethicality, intervention coherence, opportunity costs, and perceived effectiveness. Several modifications were made to the categories and their definitions to fit the data. Two inductive categories were generated, namely feasibility and usefulness. For the category “perceived effectiveness”, subcategories were generated to illustrate various aspects of effectiveness of BIS, including monitoring symptoms, facilitating communication, decision-making and improving care, and facilitating acceptance. The TFA category “self-efficacy” was not included in the analysis because no comments were related to it. This is probably because BIS does not require much action from the people with dementia or family caregivers themselves. The definition of the category “burden” was modified from “the perceived amount of effort that is required to participate in the intervention” to “perceived amount of difficulties, disturbance, and effort for the person with dementia, the family, and healthcare professionals”. The implementation of BIS does not require much effort from the receivers, but participants suggested that it may be burdensome in other ways and may affect other groups such as the family and professionals.
Acceptability of bispectral Index monitoring in palliative care for dementia – comments organized according to the theoretical framework of acceptability.
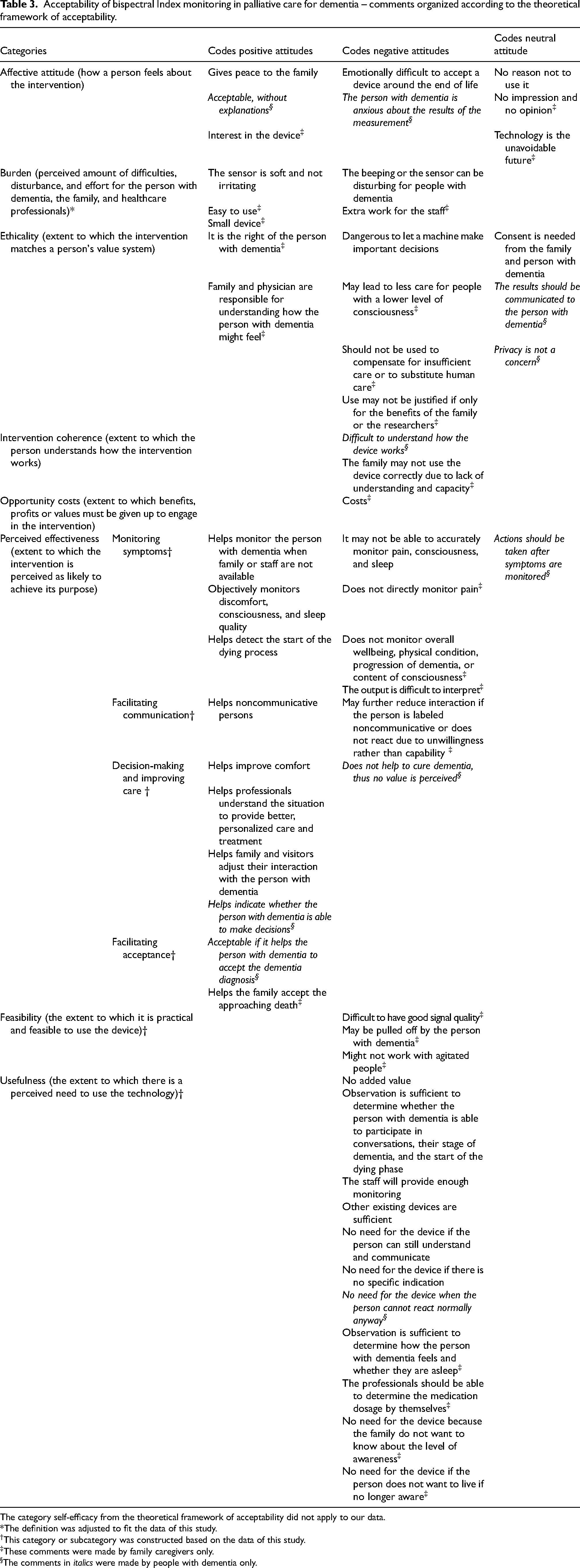
The category self-efficacy from the theoretical framework of acceptability did not apply to our data.
*The definition was adjusted to fit the data of this study.
†This category or subcategory was constructed based on the data of this study.
These comments were made by family caregivers only.
The comments in italics were made by people with dementia only.
We observed that the opinions of family caregivers and people with dementia largely overlapped, although those raised by family caregivers were more elaborate. While both groups made many comments about the effectiveness and usefulness of BIS, they expressed few concerns about opportunity costs. Some other comments made by people with dementia were more general, for example a negative attitude of seeing no added value, or a positive attitude towards the device without further elaboration: “Oh, look! How nice!” (Person with dementia, female, age 92). We observed that some people with dementia and a few family caregivers had difficulty understanding the questions and imagining the situations being discussed. Some were preoccupied by their immediate concerns, such as curing dementia or measuring its progression. “Yes, if it is really necessary, I would do it….to get better, you understand?” (Person with dementia, male, age 99).
Affective attitude
The participants mostly had a neutral or positive impression of BIS monitoring. They showed much interest in the device by asking questions, trying it on, or touching the sensors. Two participants with dementia were a bit anxious because they thought that the device would evaluate their cognitive functioning. The family elaborated on their attitudes towards BIS monitoring in palliative care for people with dementia. For some, BIS may give them peace of mind by providing more monitoring and information. “Some reassurance as well, you know. That it, well, that it's still there, the awareness.” (current caregiver, male, age 78). But for the end of life, some found it difficult to include the device. “I don’t want to see her hooked up to all sorts of tubes and stuff if it's not necessary …I don’t want that at that stage that is so intimate” (former family caregiver, male, age 78).
Burden
Many thought that the sensors of BIS monitors would not be burdensome for people with dementia, because they were soft and not painful to attach. Participants who attached the sensors kept them on their foreheads between a few seconds to a few minutes. They did not give the impression that the sensors bothered them, although temporary red marks were left on some participants’ foreheads after removing the sensors. “Well, I don’t really feel anything actually” (person with dementia, male, age 99).
Others raised the concern that the device may still be disturbing for people with dementia because of the extra stimuli. “Touching her head, that's absolutely not done. It would mean instant war, so to speak” (former caregiver, male, age 65). The beeping sound for inadequate signal quality, which occurred often during the demonstration, was perceived as annoying.
Some family caregivers also worried that BIS monitors in the current form, although small and relatively easy to use, would increase the workload for the staff and would not be welcomed in busy hospitals and nursing homes. Extra personnel might be needed to keep an eye on the monitors, to operate the device if less educated personnel were unable to do so, and to deliver care when the device showed that care might be needed. One of them suggested: “If you can use a final version, wirelessly, then you are also rid of that monitor… otherwise it won’t work. Then you'd still have to have someone there” (former caregiver, male, age 78).
Ethicality
The main ethical concern raised by the participants was that the device should be used for the benefit of the person with dementia, rather than for the family, researchers, or staff. Thus, it should not be used to substitute care that needs to be provided by healthcare professionals. “Yes you have to avoid that these kind of aids, ehm, well I don’t want to say laziness, but a kind of efficiency tool. […] if that's how it's going to work, well, then I have no desire to grow old” (current caregiver, female, age 56). If used improperly, participants worried that it might lead to people who have a constant lower level of consciousness receiving less attention and care.
Participants discussed ethical implications of using the BIS monitor to help medical decision-making. While some were enthusiastic, others stated that it would be dangerous to rely too heavily on a machine for important decisions. “- So maybe it's like extra support or something when you have to make a yes-or-no decision about euthanasia. I hope so, I certainly hope so. – It makes me nervous, a remark like that. I sincerely hope that no outside persons, based on a device like this, are ever allowed to arrive at a decision in a decision tree that this person has decreased awareness or no awareness, and we are either going to pull the plug now or we’ll start palliative sedation with death as the goal, the person dies.” (current caregivers, female, age 71 and 56 respectively).
Participants who considered BIS monitoring acceptable stated that proper monitoring is the right of the people with dementia as well as the responsibility of healthcare professionals. When implemented, it was considered important to share enough information with the stakeholders. Both people with dementia and family caregivers stated that they would want healthcare professionals to ask their consent about using BIS and share the monitoring results with them. Privacy was only mentioned by two persons with dementia, saying that it was not a concern. “- Oh everyone [is allowed to know how aware I am]. – Everyone yes. – Yes! I have no secrets from… It's my condition. So it is a good thing when people can know what my condition is” (persons with dementia, female, age 76, and male, age 72).
Intervention coherence
Concerns were raised by all groups of participants about adequate understanding of BIS monitoring. Some people with dementia thought that those being monitored would not understand how the device works and what it is used for. “But that wouldn’t help, you have to explain everything and people don’t understand you… They will shout ‘no!’” (person with dementia, male, age 73). A former family caregiver (female, age 65) worried that it might be implemented in the wrong way if this was done by caregivers at home who did not know enough about how to use it.
Opportunity costs
Few comments related to things that need to be given up in order to use BIS monitoring. Only two family caregivers mentioned that the cost could be a concern for healthcare institutions to implement it.
Perceived effectiveness
Monitoring symptoms
The expectation of the BIS device being able to monitor symptoms that are of interest to the participants was one of the main arguments for the acceptability of using it in dementia care. Those who considered BIS acceptable saw its potential for monitoring sleep, pain, and the onset of dying. However, others questioned whether the device was capable of monitoring these symptoms and events. A few participants were mainly interested in other measurements, such as the stage of dementia or the prognosis. They did not consider BIS monitoring acceptable because it would not provide such information.
Participants mentioned several advantages of BIS related to symptom monitoring, for instance, that it provides non-biased, objective information: “I think it's really helpful because one person says this and the other says that and well, the device measures exactly how it is.” (current caregiver, female, age 71), and that it can provide continuous monitoring when staff is not available, for example, at night. However, other participants did not agree with the latter, arguing that staff should be on standby to take action when symptoms are detected.
Facilitating communication
Participants saw the potential of BIS monitoring for helping noncommunicative people with dementia express their feelings or helping others in their interaction with the person with dementia. “Is it about that you know that it, your message, is received or not? Because I would really like that” (former caregiver, male, age 62). One former family caregiver (male, age 65), however, raised the concern that this would reduce the willingness to make the effort to interact with people who are identified as having reduced communication ability, or with people who are conscious and capable of communication, but reluctant to do so, for example, due to a bad mood.
Decision-making and improving care
Many participants hoped that BIS monitoring would improve care and medical decision-making for people with dementia. “If it's a device and it's in the hospital, and they can take action. Well great” (person with dementia, female, age 76).
This can especially be helpful for staff who do not know the person with dementia well enough to provide personalized care. The family can also adjust their behavior based on the monitoring results “What do and what don’t you say in this room. It would be very good to know if there is still awareness, so you can leave the room and discuss it outside” (former caregiver, male, age 65).
Facilitating acceptance
Participants suggested that BIS monitoring may provide more information and thus facilitate their acceptance of the situations they are in. Family caregivers indicated that BIS monitoring might help them accept the approaching death. “That it would do make it easier for me to let go if I… could see that the level of awareness is also drastically reduced in the person with dementia” (current caregiver, female, age 58). A person with dementia (female, age 82) said that the device would be valuable if it could help people with dementia accept their diagnosis, for example, by showing that their brain is not functioning well.
Feasibility
Several family caregivers raised concerns about the feasibility of the device due to problems with the signal quality and behavior of the people with dementia. As it was challenging to get good signal quality while there was good connection with the skin during the focus groups, the participants questioned whether it would work in practice. “If it is so difficult to put it on correctly, then I would have some reservations, especially for people with dementia in the final phase” (former caregiver, male, age 65). This may be of concern especially for people with dementia who are agitated. Family caregivers said that agitated people and those who do not want anything on their head, might pull the sensors off.
Usefulness
There were many comments questioning the usefulness of the device, in particular from persons who know about existing measures of communication, observation, and care and felt these sufficed. Based on the field notes, this may be partly related to difficulty imagining situations where communication or the observation of consciousness could be challenging. “When someone is in pain. You can see it” (former caregiver, female, age 59). When discussing the use of BIS monitoring to help titrate medication for palliative sedation, some participants expected healthcare professionals to be capable of doing that without the help of a monitoring device. One former family caregiver (male, age 78) even said that overmedication would be preferred to restless situations around the end of life. A current family caregiver (female, age 71) suggested that BIS monitoring would also not be necessary for people who would want to end their life before reaching the state of no longer being fully conscious.
The device would also not be useful if there is no need for extra information. For example, the device was not considered necessary if the person with dementia is in natural sleep and not experiencing any specific symptom that required attention and care. “I think, like the person before me just said, that using it would only be a good idea for people who are very restless during the night.” (person with dementia, male, age 92). Some family caregivers did not want to know about the level of awareness in certain situations, for instance at the end of life.
Suggestions
The participants made several suggestions on the use or further development of the device (Table 4). Participants suggested making the data more accessible for remote monitoring and later viewing. The sensors could be made more user-friendly, for example wireless, and be attached more securely to the head. Interestingly, there seemed to be discrepancies on how long BIS monitoring should be used in people with dementia, ranging from a maximum of 30 min to around-the-clock monitoring.
All suggestions on the use or possible future application and development of bispectural Index monitoring in palliative care for dementia.
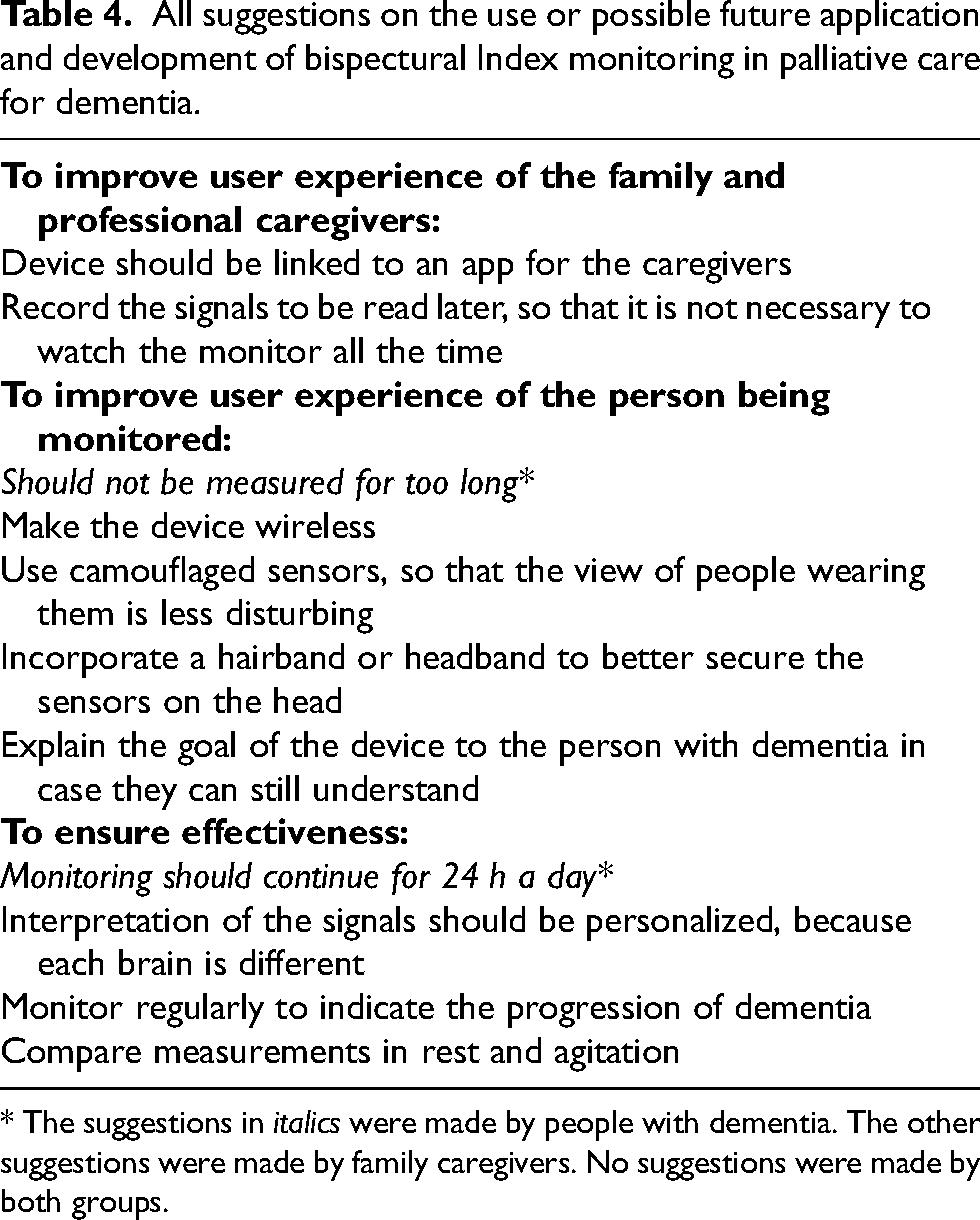
* The suggestions in italics were made by people with dementia. The other suggestions were made by family caregivers. No suggestions were made by both groups.
Discussion
This study examined when and why BIS monitoring is acceptable or unacceptable in end-of-life care for people with dementia. As for when BIS monitoring was acceptable, only a few people with dementia were able to evaluate the acceptability of BIS monitoring in specific situations, and their attitudes were diverse. Family caregivers were positive about its application in most situations discussed in the study, such as during palliative sedation and for pain monitoring. Its use was more controversial for them in non-medical situations, such as during natural sleep. Participants elaborated on different aspects of why they considered BIS monitoring (not) acceptable, including affective attitude, burden, ethicality, intervention coherence, opportunity costs, and perceived effectiveness, feasibility and usefulness. In general, BIS monitoring was not perceived as burdensome, and some participants saw its potential for monitoring symptoms, facilitating communication, facilitating acceptance, and helping with decision-making and improving care. However, its added value was not evident for some participants. Other participants also saw room for improvement in the user-friendliness of the device.
Although family caregivers and some people with dementia saw the potential of implementing BIS monitoring in a number of situations, only some of these situations would actually be realistic given current BIS technology. Based on the design of the BIS monitor and the literature, it is currently possible to apply BIS in palliative care to help titrate medication during palliative sedation,35,36 to monitor wakefulness during recovery in the hospital, to monitor natural sleep, 37 and to indicate periods of alertness in the home or nursing home setting. There might be potential for using BIS monitoring in the detection of acute pain, 38 to indicate emotional responsiveness during interaction, 39 and to identify the start of the dying phase. Currently, it is beyond the functionality of BIS monitors to indicate the contents of consciousness, the progression of dementia, the deterioration of physical condition, and decision-making capacity.
Even though some of the participants’ expectations may not be satisfied by the current possibilities of the BIS monitor, they may be indicative of other underlying needs that should be met. Family caregivers indicated the need for more information about the experience of their relative with dementia and support in decision-making. People with dementia expressed the need to be informed of the progression of their dementia. Measures need to be taken to address these needs, with or without the technology. For example, clinicians can ask whether there is a wish to periodically communicate the results of clinical observations on the stage of the disease to people with dementia and family caregivers. They can also provide information on what this stage would mean to the people with dementia and give advice to family caregivers on communicating with the person. If preferred, simple neurological tests could also be offered.
The results of this study demonstrate diverse opinions of people with dementia and family caregivers on BIS monitoring, and they shed light on issues to consider in the further development and implementation of monitoring technologies in end-of-life care for dementia, including BIS, if its effectiveness is demonstrated in the future. Stakeholders should be well-informed, and care must be taken that the technology does not replace human care. It is important to explain its use to people with dementia and family, and clarify misunderstandings before the implementation in order to minimize anxiety and manage expectations. Moreover, our participants with dementia expressed mixed attitudes towards the acceptability of BIS monitoring. This is in line with recent reviews reporting that people with dementia or mild cognitive impairment saw the benefits of monitoring technologies, but had reservations about acceptability.40,41 Healthcare professionals should therefore only implement such technologies after obtaining consent, or pay close attention to any signs of resistance during its application. Participants of our study also expressed ethical concerns that technologies should not substitute humans in medical decision-making, which coincides with a conclusion in a recent review. 42 Therefore, we should exercise caution regarding using input from the device to make important decisions, and healthcare institutions should ensure the quality of care provided by human professionals and avoid using the device as a substitute to compensate for substandard care.
This study has implications for the refinement of TFA framework when applied in studies on monitoring technology in dementia care, especially if the technology being researched requires minimal input from the person being monitored, as was the case for BIS monitors. The component constructs self-efficacy and opportunity costs may not be applicable, and the explanations of the constructs should be formulated not only from the perspective of the person receiving the intervention, but also the family and healthcare professionals as crucial stakeholders in dementia care. 43 For example, the construct “burden” was described in TFA as “the perceived amount of effort that is required to participate in the intervention”. 25 It could be modified into “the perceived amount of effort that is required for the person receiving the intervention, family caregivers, and healthcare professionals”. Moreover, concepts that are closely related to acceptability, such as feasibility and usefulness were frequently mentioned by our participants and could be added to the framework.
Future research is needed to further investigate the use of BIS monitoring in end-of-life care. Since effectiveness and purposefulness are essential when applying technology in palliative care, 42 future studies should evaluate the usefulness of BIS monitoring in situations deemed potentially acceptable by people with dementia and family caregivers in this study. Other crucial stakeholders, namely healthcare providers, should be involved. The device can also be improved to increase user-friendliness for a population outside the operation room and will need to be validated in people with dementia. Interestingly, the possible application of BIS monitoring to ensure unconsciousness in assisted dying 44 was not mentioned by our participants. This is worth future investigation because assisted dying is an important topic for end-of-life care in the Dutch context, 45 and the number of people with dementia receiving assisted dying has been increasing in recent years. 46 Moreover, feasibility and efficacy studies in palliative care for people with dementia should be conducted, for example a pilot study among nursing home residents with advanced dementia. 39 Concurrent and retrospective acceptability should be assessed if BIS is implemented after further development.
This research has several strengths and weaknesses. The involvement of people with dementia provided us with valuable information on their experience with the device, which is sometimes different from the perspectives of family caregivers. People with dementia are underrepresented in research, 47 while their voices are crucial in research aiming to improve their future care. The inclusion of both current and former family caregivers also contributed to the richness of the data. The sample included elements of cultural diversity. More than 23% of the participants with dementia were born in another country, which was more than in the general population. 48 At least one of the 12 family caregivers had a parent with a migration background, based on the information they gave about the person with dementia they cared for. A limitation was the use of abstract questions about imagined scenarios. We have simplified the questions and adjusted the procedure to make it less cognitively challenging for people with dementia. Previous research demonstrated the possibility of involving people with dementia in qualitative studies, 49 and we found that this is facilitated by limiting abstract questions and focusing on direct experience of real situations. However, some participants still did not fully understand the questions and the technology. Moreover, the group setting may have potentially led to social desirability bias. We recognize that the acceptability expressed by the participant may not be the same as their actual decision to use the technology when introduced by a healthcare professional. 27 Therefore, caution is needed when interpreting the results. Despite the limitations, this study was the first to illustrate the attitudes of people with dementia and family caregivers regarding a technology that monitors the level of consciousness of people with dementia in palliative care.
Conclusion
In conclusion, opinions on the acceptability of BIS monitoring differed among people with dementia. Family caregivers considered BIS acceptable in medical situations in palliative care for people with dementia, such as palliative sedation and pain detection. Reasons as to why BIS monitoring was deemed acceptable included its potential to improve care and that it was not perceived as burdensome. Skepticism was expressed concerning its added value compared to existing measures of symptom monitoring and the risk of replacing human care with the technology. Future research should validate and examine the acceptability of BIS monitoring in practice. If it is implemented in dementia care in the future, professionals should make sure that the stakeholders are well-informed and that the tool is only used as a supplement to human care.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241297147 - Supplemental material for Acceptability of bispectral Index monitoring in end-of-life care for dementia
Supplemental material, sj-docx-1-alz-10.1177_13872877241297147 for Acceptability of bispectral Index monitoring in end-of-life care for dementia by Jingyuan Xu (须静媛), Hanneke JA Smaling, Albert Dahan, Justin Chan and Jenny T van der Steen in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
We would like to thank our interns Gabriela M Sikorska BSc, Merve Çalışkan MSc, and Thijs J Huisman BSc for their help in the data collection, and Yara J. Schepen MD for her support with the coding of the data.
Author contributions
Jingyuan Xu (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Writing – original draft); Hanneke JA Smaling (Conceptualization; Investigation; Methodology; Project administration; Supervision; Writing – review & editing); Albert Dahan (Resources; Writing – review & editing); Justin Chan (Methodology; Resources; Writing – review & editing); Jenny T van der Steen (Conceptualization; Funding acquisition; Investigation; Methodology; Supervision; Writing – review & editing).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the European Research Council (ERC), grant number 771483. The financial sponsor did not play a role in the whole process of this study.
Declaration of conflicting interests
Jenny T. van der Steen is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor did she have access to any information regarding its peer-review.
The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are not publicly available due to privacy and ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.