
Abstract
Background
Semantic and short-term episodic memory are impaired in some brain disorders including Alzheimer's disease.
Objective
Development and validation of an almost self-administered, but cognitively demanding four-minute test identifying very mild cognitive impairment (vMCI).
Methods
The innovative hedgehog PICture Naming and Immediate Recall (PICNIR) consisted of two parts. The first task was to write down the names of 20 black-and-white pictures to evaluate long-term semantic memory and language. The second task involves immediate recall and writing the names of as many previously named pictures as possible in one minute. The PICNIR is assessed using the number of naming errors (NE) and correctly recalled picture names (PICR). The PICNIR and a neuropsychological battery were administered to 190 elderly individuals living independently in the community. They were divided into those with vMCI (n = 43 with Montreal Cognitive Assessment (MoCA) 24 ± 3 points) and sociodemographically matched cognitively normal (CN) individuals (n = 147 with MoCA 26 ± 3). Both subgroups had predicted mean Mini-Mental State Examination scores of 28–29 points.
Results
Compared to CN, vMCI participants made more NE (0.3 ± 0.6 versus 0.6 ± 0.9; p = 0.02) and recalled fewer PICR (8.9 ± 2.2 versus 6.8 ± 2.2; p < 0.000001). Discriminative validity was satisfactory using the area under the ROC curve (AUC): 0.76 for PICR, 0.74 for MoCA, 0.67 for MoCA-five-word recall, and 0.59 for NE. The AUCs of PICR and MoCA were comparable and larger than those of MoCA five-point recall or NE. Logical Memory scores, RAVLT scores, Digit symbol, and animal fluency correlated with PICR.
Conclusions
The picture-based PICNIR is an ultra-brief, sensitive cognitive test valid for assessing very mild cognitive impairment. Its effectiveness should be validated for other languages and cultures.
Keywords
Introduction
Long-term semantic and short-term episodic memory are two types of memory that are important for our everyday life. They are also used in the diagnostics of neurodegenerative dementias and other disorders.1–3 Semantic memory involves knowledge and facts that were intentionally learned. Short-term episodic memory refers to the ability to remember personal events that happened in the recent past, such as whether someone took a medication or remembered a traffic sign posted in front of an intersection. Both types of memory are impaired in some brain and other disorders.1,2 While a slow decline in episodic memory is common in limbic-predominant age-related TDP-43 encephalopathy (LATE), mild semantic memory deficits may also develop. 4 Cognitive impairment also affects various aspects of care for older adults with cancer or during a peri-operative period.5,6 Poor semantic memory is commonly observed in frontotemporal lobar degeneration (FTLD) and Alzheimer's disease (AD). Although deficits in short-term episodic memory are more typical in AD, they can also manifest in brain, neurodegenerative, psychiatric, and other disorders.1,7–10 Thus, both types of memory are non-specific, and their deficits cannot be used to predict neuropathological lesions. Recent evidence suggests that dementia and the underlying pathology are almost always mixed.11–13
Early detection of subtle cognitive changes is a challenge. Recognizing the disease in its early stages provides the opportunity for further diagnostics and a comprehensive management and treatment plan personalized for the patient. 14 It may help slow cognitive decline through the use of preventive measures such as cognitive, physical, and social intervention strategies. Initial deficits occur in individuals with mild cognitive impairment (MCI). It is a syndrome with heterogeneous underlying causes and different rates of disease progression. MCI is defined as a decline in cognitive abilities with objective evidence of impairment in standard memory or other cognitive tests but without the significant impairment in daily activities seen in conditions such as dementia.15,16 Memory is the most common domain involved among patients who subsequently progress to AD dementia. 15 Amnestic MCI can be classified as either early or late MCI according to the severity of memory impairment.17–19 This is usually determined by formal or bedside testing. 15
The level of specialist knowledge and experience required to administer and interpret many neuropsychological tests is high, which can limit patient access. A simpler, bedside screening test like the Mini-Mental State Examination (MMSE) has utility but may exhibit ceiling effects in those with the mildest levels of impairment or high pre-morbid cognitive function. 20 Episodic memory tests should be sufficiently challenging to identify patients with MCI, especially in the prodromal phases. If not, these tests may lack sensitivity to subtle cognitive dysfunction in the early stages of MCI, often yielding normal performance. The MMSE is the most commonly chosen cognitive tool in clinical practice.14,21 However, the MMSE is known to lack sensitivity at the earlier stages of dementia, making it an inappropriate screening tool for early detection. Additionally, the MMSE is copyrighted, meaning clinicians incur costs for its use in clinical practice. 14 More detailed and sensitive tests may help in early detection but are not always available. 20 The Montreal Cognitive Assessment (MoCA) is another screening test that has been shown to be better at detecting cognitive impairment in MCI. Relatively longer administration time (≥ 10 min) and interference by education levels (≤ 12 years of education) result in limitations of its application, particularly in initial screening of MCI in the community. 22 When selecting an initial cognitive tool for diagnostic evaluation of patients with suspected MCI and Alzheimer's disease, physicians prioritize characteristics such as speed and ease of administration, the ability to conduct the test without referral, and good sensitivity for detecting subtle problems. They also identified the time required to administer the tool as a significant barrier. 14 Thus, cognitive testing should be challenging enough for patients to reveal subtle impairments, yet brief and easy for clinicians to administer during an office visit to yield informative results suggestive of MCI.
Semantic memory, visual gnosia, or lexical access are quickly assessed by naming objects or pictures or by semantic questions as a standalone test23–27 or as part of a test battery.5,27–32 Written, oral, or typed picture naming tests can also be employed to evaluate language abilities.2,23–26,33,34
Short-term episodic memory can also be assessed using brief tests or as part of a test battery. An example of a recently developed option is our sensitive Amnesia Light and Brief Assessment (ALBA), which employs a three-minute evaluation of short-term episodic memory using sentence and gesture recall. The test is easy to use and implement into daily clinical practice.35–37 The ALBA uses 12 items to remember instead of the only three words used in the Mini-Cog test. 38 Short-term episodic memory is not assessed using the Clock Drawing Test, which is of little use when screening patients with very mild cognitive deficits. It is used to assess visuospatial, constructional, and executive functions. 39 Test batteries can include measurements of short-term episodic memory with items that differ from the semantic assessment. The number of such stimuli is relatively low, ranging from two to seven words or items. It usually takes 10 to 30 min to yield memory scores for the various cognitive tests.26,28,31,32,40–50 None of these test batteries simultaneously utilize semantic stimuli to assess short-term episodic memory. Dual use of the same items could reduce testing times.
Therefore, we developed the innovative PICture Naming and Immediate Recall (PICNIR) test. The test is very brief, easy to administer, and cognitively demanding, allowing it to detect mild cognitive deficits accurately. The PICNIR can be administered and quickly scored in about four minutes. Moreover, except for the simple instructions at the start and in the middle of the test, the PICNIR is self-administered, and the administrator is there for support, supervision, and to answer questions. The PICNIR test has been evaluated and approved as a certified method by the Ministry of Health of the Czech Republic. The PICNIR consists of two parts. It starts with the task of writing down the names of 20 black-and-white pictures, followed by the immediate recall and writing the names of as many previously named pictures as possible within one minute. 51 This allows PICNIR to assess semantic and short-term episodic memory in a single test simultaneously.
The first Czech study demonstrated a sensitivity of 100% and specificity of 97% for mild Alzheimer's dementia with a cut-off at ≤6 correctly recalled picture names. 51 The PICNIR is sensitive enough to identify subtle cognitive deficits in an offspring of a patient with dementia. 52 In the Czech Republic, the PICNIR and ALBA tests are used by physicians, speech therapists, social workers, and pharmacists to detect cognitive impairment in patients and clients. They have also been included in several research studies on probiotics, post-stroke cognitive impairment, and exercise alone or combined with omega-3 polyunsaturated fatty acid supplementation.53–56 Remote electronic administration results are comparable to in-person testing. 57 A self-administered online version has been developed and validated.58,59 The PICNIR test and brain SPECT were unexpectedly abnormal even in the grandson of a patient with dementia. At the age of 30, he recalled a relatively low number of picture names in the PICNIR test (seven). Brain SPECT activity accumulation was borderline or mildly reduced in the left hemisphere, unevenly affecting the frontal, parietal, and occipital lobes. 60 The current report introduces the PICNIR to the international community for the first time.
The objective of this study was to introduce and validate the PICNIR test, a newly developed original brief cognitive assessment. More specifically, we aimed to determine the known-group discriminant validity of the test by comparing scores of the PICNIR between cognitively normal individuals and those with very mild cognitive impairment. Additionally, we investigated the comparison of our results of the PICNIR with those of the MoCA, which is commonly used to detect mild cognitive impairment. This study also aimed to investigate convergent validity which was explored using correlations between scores of the PICNIR and the results of a neuropsychological battery and questionnaires assessing activities of daily living and depression.
Methods
Development and selection of unambiguously named uniform pictures for the hedgehog version of the PICture Naming and Immediate Recall (PICNIR) test
The cardinal component of the PICNIR test includes appropriately prepared pictures. Our special and original pictures were intentionally selected for the PICNIR test. We started the development of the PICNIR test with the specific purpose in mind, i.e., to identify cognitive or naming impairment by using a set of specially selected pictures that have been shown to be difficult to name by our patients with diagnosed dementia and cognitive disorders. Drawings were developed and sorted during our previous long-term picture research.
First, we prepared a list of potential candidate picture names, categorized into several semantic groups (e.g., animals, fruits, vegetables). Second, we drew the pictures and placed 35 of them on each page. We developed multiple picture sets for testing. The initial set included primitive pictures drawn by us and symbolizing only part of an object, such as the head of an animal. Over time, we achieved a consistent appearance with black-and-white, two-dimensional line drawings, with equally wide contours. The last set was drawn by a professional artist. As we refined the pictures, their number fluctuated, and their quality improved with new ideas and our experience in naming them. The number of objects in each picture set varied, ranging from 73, 67, 148, 147, and 119, to the final number of 66 in the last set. In total, we invented, drew, and tested 180 pictures. These pictures were presented for naming to both cognitively normal elderly individuals and cognitively impaired patients. Based on each round of testing, some pictures were eliminated for different reasons (ambiguous responses, synonyms, etc.), while new pictures were added. Simultaneously, the appearance of the pictures was modified. This iterative process aimed to identify pictures that could be correctly named with a single word by 90–100% of cognitively normal individuals while achieving the lowest possible correct naming percentage among cognitively impaired patients. Finally, 114 pictures were eliminated as described below and 66 pictures were used for further research.
What is special and original in pictures used in the PICNIR?
Firstly, they can be unambiguously named only with a single word in Czech. This is an important condition to avoid interpretation and scoring problems when using pictures without these characteristics.
We determined the name agreement of each picture since it is important in the development of a naming test. Name agreement in picture tests refers to the extent to which different people agree on a name for a particular picture. Native speakers of the Czech language were asked to view each picture in the sequential picture sets and provide the name that they think best describes it. This was done verbally in the first picture sets and then in writing in more advanced sets. The names were collected and coded. Responses were categorized based on their similarity to the target name.
Based on our experience, we have developed a system for evaluating the agreement between the expected and actual naming. We considered a name correct if it was either completely accurate (e.g., horse, bear, hammer) or a diminutive (e.g., a small ear, a lion cub, a baby hippopotamus, which are single words in Czech). By contrast, we did not accept superordinate terms (e.g., reptile, pastry, musical instrument, bird, tool, fish) or imprecise names (e.g., ram-sheep, hand-palm; organ-piano; broom-sweeper; socks-stockings). Other pictures were excluded due to a similar concept (e.g., cabbage-lettuce, bee-wasp, face-cheek), were hard to recognize when drawn in only two dimensions and with a black-and-white design (e.g., plum) or when they could be named with a synonym (e.g., sailboat/yacht, lorry/truck). Pictures were also excluded if a naming success rate was below 90% among healthy seniors (e.g., dolphin, organ). We calculated so called name agreement percentage which is the percentage of participants who provide the most frequently given name for each picture. This is calculated by dividing the number of participants who gave the most common name by the total number of participants and multiplying by 100. Then we compared name agreement between common people and cognitively impaired patients. The best pictures are those with the highest differences in name agreement between these two groups. Finally, we provided lists of pictures with their corresponding most common names and agreement rates. The number of pictures with high name agreement and unambiguous and one-word naming of animals was naturally and logically higher than those in other semantic categories (animals n = 32, clothing n = 7, working tools n = 6, fruit n = 5, parts of the body n = 3, plants n = 3, means of transport n = 2, food n = 2, musical instrument n = 1).
Secondly, the pictures have very high name agreement with the intended names, ranging from 91% to 100% in normal older adults. As a result, the PICNIR pictures are easily named by normal elderly people as shown in our first report. 51
Thirdly, on the other hand, patients with mild impairment of cognitive functions have difficulties correctly naming some of the specific pictures in the middle of the set. These items are difficult to name because of their characteristics and not because they are presented in the middle of the set. Their name agreement was between 44% to 77%. We designated these pictures as difficult ones. Examples of incorrectly named pictures are sock/stocking, lion/tiger, garlic/onion, pineapple/fruit, hippopotamus/pig, and zebra/donkey. Differences in name agreement between patients and normal elderly people ranged from 22% to 50%. All these features are a prerequisite for good differentiation between cognitively normal and impaired people. We are not aware of any picture sets created using similar principles and for this purpose. The choice of pictures used in the MoCA or in the Addenbrooke's Cognitive Examination was not justified by similar preceding evaluation of the pictures. Thus, the specific pictures were utilized for the assessment of semantic and long-term memory and lexical access in the first naming part of the PICNIR test.
Fourthly, the pictures belong to one of the following groups for semantic categorization: (1) animals, (2) working tools, (3) clothing, (4) fruit, (5) vegetables, (6) parts of the body, (7) plants, (8) means of transport, (9) food, and (10) musical instruments.
Finally, the pictures have an unambiguous and uniform appearance clearly visible for the elderly. The unambiguous appearance of the pictures was established through iterative modifications of the drawings during our previous research, as described earlier. This was confirmed by a high name agreement rate of over 90% among healthy elderly participants. The uniform appearance was achieved by having a professional artist draw the pictures in a consistent style which is clearly shown in Figure 1. They have good contrast (black lines on white paper) for visual perception even in people with some visual problems. The test form with black-and-white pictures can be printed out on any printer.
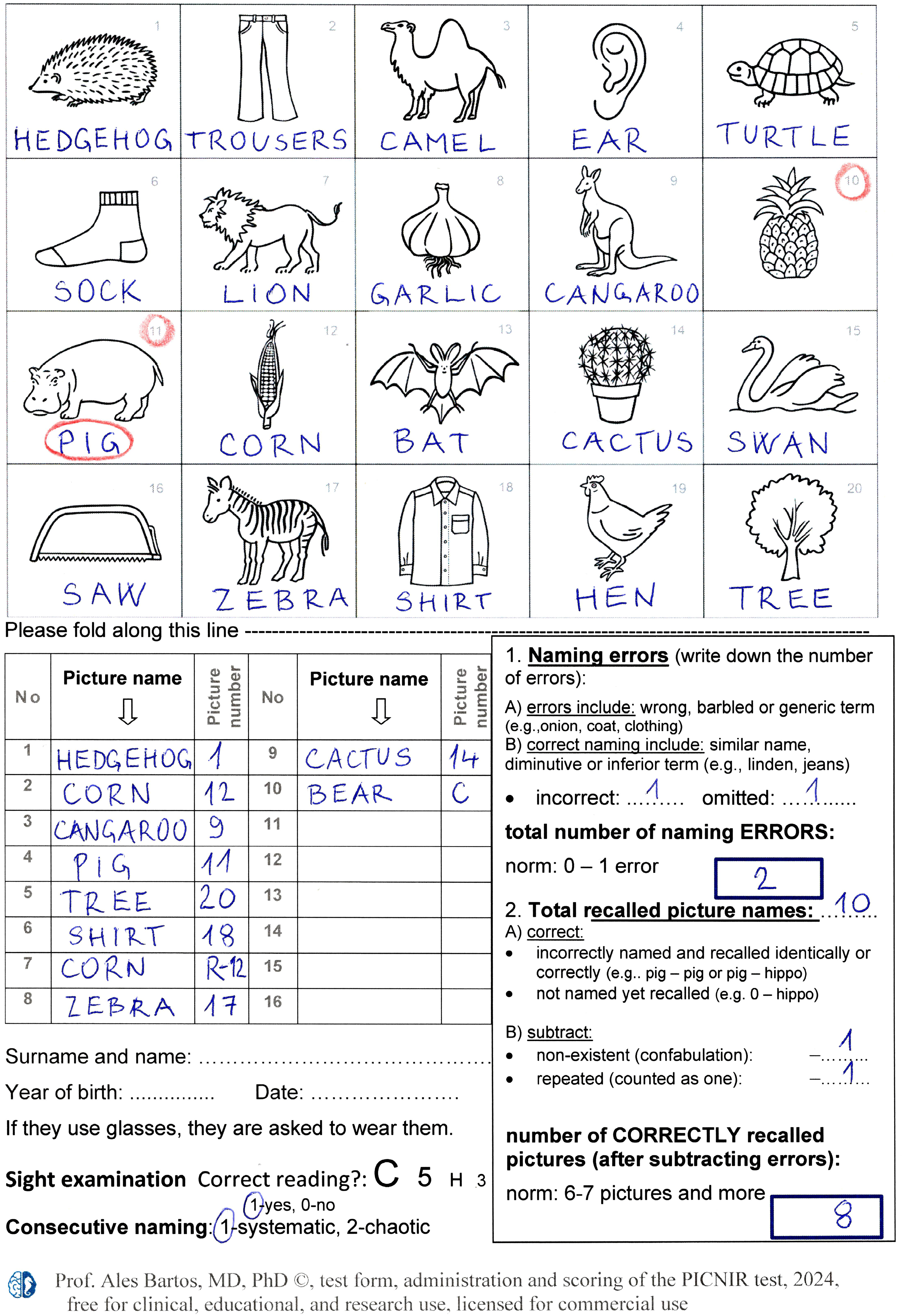
A filled-in test form of the PICture Naming and Immediate Recall (PICNIR) test form including brief administration and evaluation instructions
The arrangement of the pictures is original and intentional and occurs in a precisely determined order with an underlying rationale. The first and the last few pictures are easy to name by patients with mild Alzheimer's disease and other cognitive disorders. It allows recalling some of them. In contrast, pictures more difficult to name are placed in the middle part since it is generally more complicated to recall new information from the middle of an item set. Pictures of animals occupy all the odd positions, and pictures of other categories occupy the even positions (i.e., clothing, fruits, vegetables, parts of the human body, and tools). As described earlier, the number of animals in pictures significantly exceeded the number of pictures in other categories, ranging from fourfold (e.g., clothing) to several times (e.g., musical instruments). Thus, half of the pictures include animals while the remaining half consists of pictures from other categories. Additionally, this arrangement ensures that pictures from the same category are not placed adjacent to each other. The deliberate intention was to avoid facilitating memorization based on semantic or shape associations. 51
Correct naming includes intentional names, diminutive names (a small ear), and more specific names (e.g., a type of a tree – an apple tree). A list of acceptable alternative responses was established, based on the previous picture naming by 550 people (320 normal elderly and 230 patients with cognitive impairment). Since the pictures were carefully selected, it includes only a few of them: džíny (jeans), pantalóny (pants), dromedár (a dromedary), jednohrbý velbloud (a one-humped camel), lvice (lioness), lvíče (a lion cub), klokanice (a female kangaroo), hrošík (a baby hippopotamus), kukuřičný klas (a corn cub), pilka (a small saw), listnatý strom, lípa, dub, buk, jasan, javor, jabloň (deciduous tree, linden, oak, beech, ash, maple, apple tree).
Description of the hedgehog version of the PICture Naming and Immediate Recall (PICNIR) test
The PICNIR test consists of two parts and meets our criteria for developing a new test as outlined in Supplemental Table 1. In the first part, the examinee is asked to write a one-word name under each of 20 black-and-white pictures and simultaneously try to remember the picture names. This assesses long-term semantic memory, lexical access, language, and writing or spelling. The difficulty of the test is increased by this dual task of simultaneous naming and remembering. The second part follows without distraction. The examinee is then asked to recall and write down the names of as many previously named pictures as possible within one minute. This task assesses immediate short-term episodic memory. Based on initial experiments with this new paradigm, this timing was determined as the optimal compromise between the greatest number of written and recalled picture names and the shortest test duration. 51 In general, patients tended to stop recalling before the one-minute time limit. In contrast, normal elderly participants did not significantly add to the number of recalled picture names after the one-minute time limit (two on average). 51 The PICNIR is scored using the number of naming errors (NE) and picture names recalled correctly (PICR). Detailed instructions, administration procedures, and a scoring guide for using the “hedgehog” PICNIR test are provided in Supplemental Material 1. The term “hedgehog” PICNIR denotes the version of the test that starts with a picture of a hedgehog. The PICNIR test forms in English are in Supplemental Material 2 (Word) and Supplemental Material 3 (pdf) and the Czech version is in Supplemental Material 4.
The PICNIR test is original and innovative. Its distinctive features include a neatly organized test format that fits on a single page. Additionally, it is ultra-brief and straightforward, almost entirely self-administered, i.e., the test requires minimum input from or interaction with the test administrator. The PICNIR test uses original, easily recognized pictures and is quick and easy to score. Pictures and their arrangement in the PICNIR test were recognized as so-called industrial design.
The number of 20 pictures was intentionally chosen to exceed the capacity of short-term memory. This allows a wide range of memory performance on a scale of 0–20 pictures and detection of subtle deficits. A person with cognitive impairment may fail either in initial naming, memory recall, or both. Unnamed pictures also reduce the chance of recall, so the overall performance on the test is even worse. The written format of the PICNIR test allows a large degree of self-administration or even self-examination. A written test ensures appropriate registration of stimuli to remember. Examinees write the names of the pictures both during naming and recall without requiring much attention from the administrator whose role is largely supportive. The main job of the administrator is to provide instructions and turn over the folded test form after writing the name of the last picture, which effectively hides the pictures from examinees during the recall part of the test.
The front page of the test form consists of two parts which are shown in Figure 1. The upper half has 20 black-and-white special drawings organized in four rows and five columns. Each drawing is numbered and has adequate space underneath for writing the name of the picture. The lower part of the form consists of a blank table for use with the picture recall task. Additionally, there are brief scoring rules, a guide for test scores, and cut-off points. The back of the test form may contain more detailed instructions presented in Supplemental Material 1 or may be left blank, e.g., for a report about the patient.
The PICNIR test is convenient to administer. Everything needed is contained on a single page, which facilitates quick and efficient administration and scoring. An example of a PICNIR test form with results is depicted in Figure 1. Performance on the PICNIR is evaluated by determining the number of picture naming errors (Part 1) and the number of correctly recalled pictures (Part 2). The only value derived from the PICNIR test is the Recnam score, which is calculated as the number of correctly recalled picture names (Part 2) minus the number of picture naming errors (Part 1).
Neuropsychological assessment as a reference standard
As a reference standard, a comprehensive neuropsychological assessment was administered and scored by trained psychologists blinded to the final grouping and PICNIR results. The PICNIR test was administered by experienced nurses working in our Memory Clinic, research assistants, or students who had undergone PICNIR test training of administration and scoring prior to PICNIR testing. The neuropsychological assessment was performed, on average, within five months of the PICNIR test. PICNIR results were not used for diagnoses.
A neuropsychological battery was designed to include all cognitive domains, mood, and activities of daily living. The dataset of the battery results was used for subgroup categorization and exploring correlations between the battery of measures and PICNIR test scores. As part of the evaluation of general cognitive functions, participants completed the Czech version of the MoCA without education adjustment during scoring, which was consistent with the approach used in our validation study. 49 The battery of neuropsychological tests included immediate and delayed recall, verbal and visual memory, semantic memory, working memory, executive functions, language, visuospatial functions, psychomotor speed, attention, verbal reasoning, word knowledge and verbal concept formation. 61 The individual tests are described along with their correlations in the results section. Additionally, we assessed depression using the 15-item Geriatric Depression Scale (GDS) and the Beck depression inventory (2nd version (BDI-II). Anxiety was assessed using the Beck Anxiety Inventory (BAI). 61 A self-assessment of activities of daily living was conducted by the participants using our adapted Czech version of the Functional Assessment Questionnaire (FAQ). 62
Participants and eligibility criteria
This prospective study was conducted at the National Institute of Mental Health in Klecany near Prague, the Czech Republic. Volunteers were recruited from the community using advertisements and announcements at senior clubs, churches, etc. Participants met the following inclusion and exclusion criteria. We included Czech native speakers older than 50 years who lived independently in the community. Exclusion criteria involved a history of psychiatric or neurological brain disorders (e.g., stroke, trauma, tumor, alcohol abuse, and psychoactive medications). These criteria were consistent with those used in our previous normative and validation studies.35,49,50 All participants had normal near-vision acuity since they were able to correctly read all four characters (i.e., C 5 H, and 3) printed on the PICNIR form. The size of the characters gradually decreased in size down to Arial 10 points (Figure 1). Consequently, any instances of picture misnaming or anomia were attributed to impairments in visual perception, semantic processing, lexical access or language skills rather than visual impairment.
Thirty individuals were excluded due to high scores on the depression and anxiety questionnaires, specifically, GDS >6 points, BDI-II >19 points, or BAI >16 points. Based on the psychologists’ assessments, the remaining participants were categorized into two groups: (1) those with very mild neurocognitive impairment (vMCI) and (2) cognitively normal (CN) individuals.
Since vMCI is not a defined and recognized diagnostic label the inclusion criteria for vMCI group for this study were as follows: Czech native speakers older than 50 years who lived independently in the community, neuropsychological test scores lower than the 16th percentile according to Czech norms or those supplied by the companies offering Czech versions of the tests.63,64 This cut-off criterion of the 16th percentile was chosen to identify very mild and incipient deficits in accordance with international guidelines. 65 One of the primary purposes of this study was to determine whether the very brief and straightforward PICNIR test could differentiate between groups with only slight differences in neuropsychological test scores. Subjective views on memory were not taken into consideration since the cognitive state is not always accompanied by a subjective awareness of cognitive impairment. 20 Positive response to a question regarding memory problems was present in 75% of vMCI participants. However, these were not memory complaints since the volunteers were recruited by us to participate in our cognitive studies. They did not come with memory complaints to a physician´s office. The group division was based solely on objective neuropsychological scores. Exclusion criteria involved a history of psychiatric or neurological brain disorders (e.g., stroke, trauma, tumor, alcohol abuse, and psychoactive medications). Different types of MCI were included: amnestic single-domain (42%), non-amnestic single-domain (2%), multiple-domain (56%, amnestic component in 35%).
The cognitively normal (CN) elderly individuals in the control group had normal neuropsychological scores based on Czech norms, 63 normal GDS, BAI, and BDI scores, and met the previously described inclusion and exclusion criteria. To match the gender profile of the vMCI participants, 15% of cognitively normal women were randomly excluded from the sample.
All participants signed an informed consent. The research was approved by the Ethics Committees of the University Hospital Kralovske Vinohrady, Prague (EK-VP/03/02019) and the National Institute of Mental Health, Klecany near Prague (51/16), Czech Republic. The research was conducted in accordance with the Declaration of Helsinki.
Statistical analysis
We used nonparametric statistics since the data was not normally distributed in the Shapiro-Wilk test. Sociodemographic characteristics and test scores between the two groups of participants and between women and men were compared using the Mann-Whitney test or receiver operating characteristic (ROC) for continuous variables or the Chi-Square test for nominal variables. The optimal cut-off was chosen when the sum of sensitivity and specificity was high and sensitivity and specificity were well balanced in favor of sensitivity. The Spearman correlation was used to examine the relationship between PICNIR test scores and scores from the MoCA, neuropsychological tests, and questionnaires to assess convergent validity. Data analysis was performed using Statistica and MedCalc software with a significance level of p < 0.05.
Results
The average administration and scoring time of both tasks of the PICNIR test was 3.5 ± SD 0.7 min (median 3.5 min, min-max 2.5–5 min) in 66 random participants.
Discriminant validity of the PICture Naming and Immediate Recall (PICNIR)
The NC and vMCI groups were equivalent to each other in terms of age, education, and gender but differed in cognitive functions and activities of daily living (Table 1). Those with vMCI exhibited only very mild impairment, as evidenced by their MoCA and FAQ scores. Under these challenging conditions, the participants with vMCI made significantly more naming errors than the CN individuals. Conversely, those with vMCI recalled significantly fewer picture names than CN individuals. Detailed comparisons of PICNIR test scores between the two groups are presented in Table 2. The table also includes results of the areas under the receiver operating characteristic curves (AUC), cut-offs and sensitivities and specificities of the PICNIR test and its subtests, and the Recnam scores. Comparing the vMCI and NC groups using ROC analysis, we identified an optimal cut-off score of >0 for naming errors or ≤ 8 for correctly recalled picture names. The area under the ROC curve was 0.59 for naming and 0.76 for recall and the Recnam scores. For comparison, Table 2 also presents data showing comparable results for the MoCA and its subtest of delayed recall.
Participants’ characteristics and comparisons of socio-demographically matched groups.
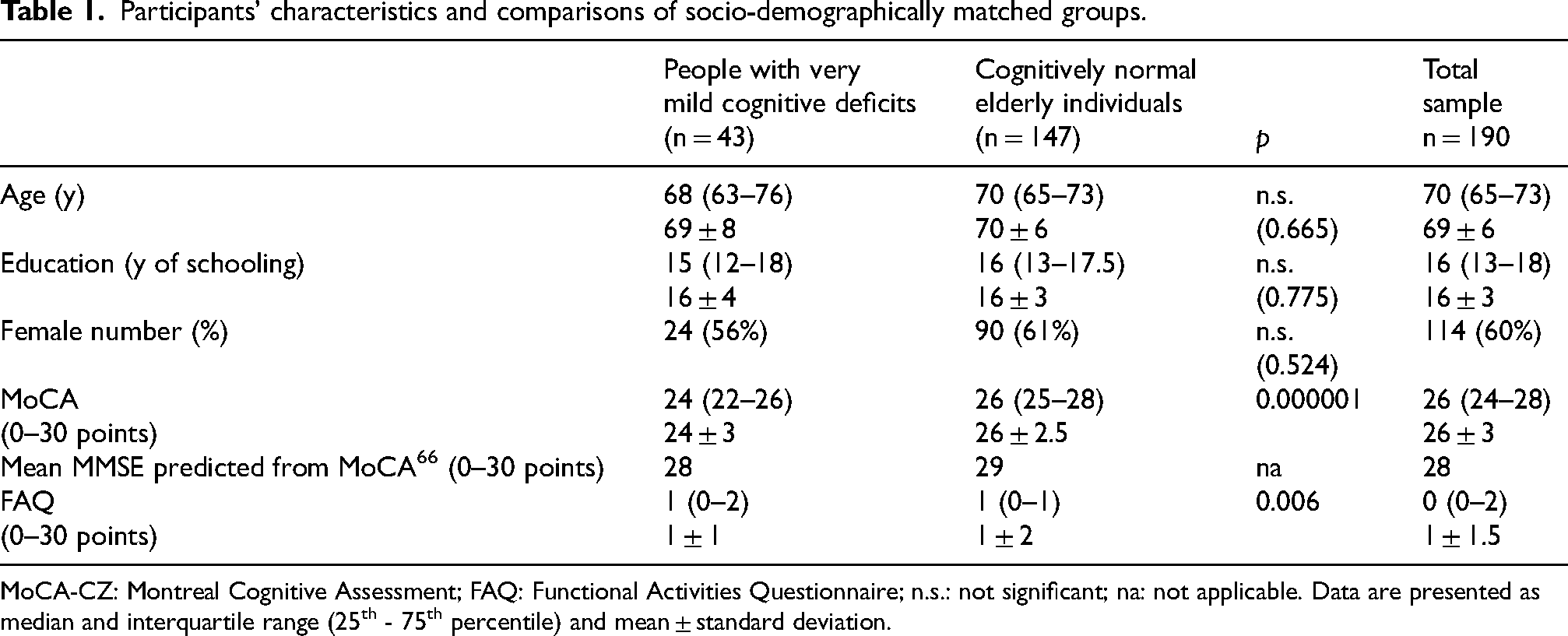
MoCA-CZ: Montreal Cognitive Assessment; FAQ: Functional Activities Questionnaire; n.s.: not significant; na: not applicable. Data are presented as median and interquartile range (25th - 75th percentile) and mean ± standard deviation.
Results of individual tasks of the hedgehog version of the PICNIR test, the MoCA and its memory recall, and their comparisons between those with very mild cognitive deficits and matched, cognitively normal elderly participants, using probability values, area under the receiver operating characteristic curve (AUC), sensitivities and specificities at optimal cut-offs.
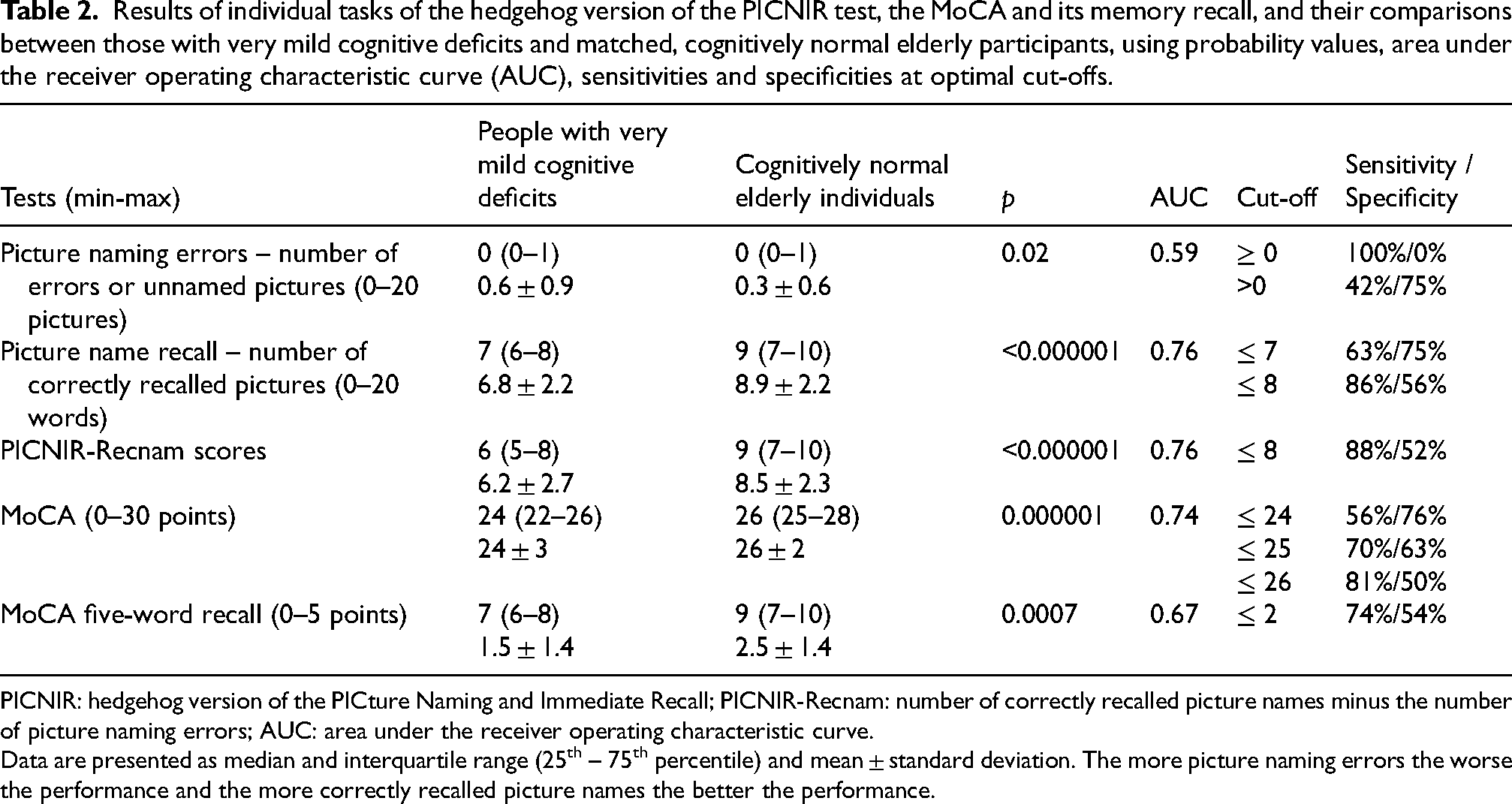
PICNIR: hedgehog version of the PICture Naming and Immediate Recall; PICNIR-Recnam: number of correctly recalled picture names minus the number of picture naming errors; AUC: area under the receiver operating characteristic curve.
Data are presented as median and interquartile range (25th – 75th percentile) and mean ± standard deviation. The more picture naming errors the worse the performance and the more correctly recalled picture names the better the performance.
The AUCs of the PICNIR picture name recall subtest, Recnam, and the MoCA were comparable and significantly greater than those of PICNIR naming errors and MoCA-delayed memory (Table 2). The AUC of the PICNIR naming errors subtest did not differ significantly from that of MoCA-delayed memory (p = 0.2). Graphic representations and comparisons of the ROC curves are provided in Figure 2.
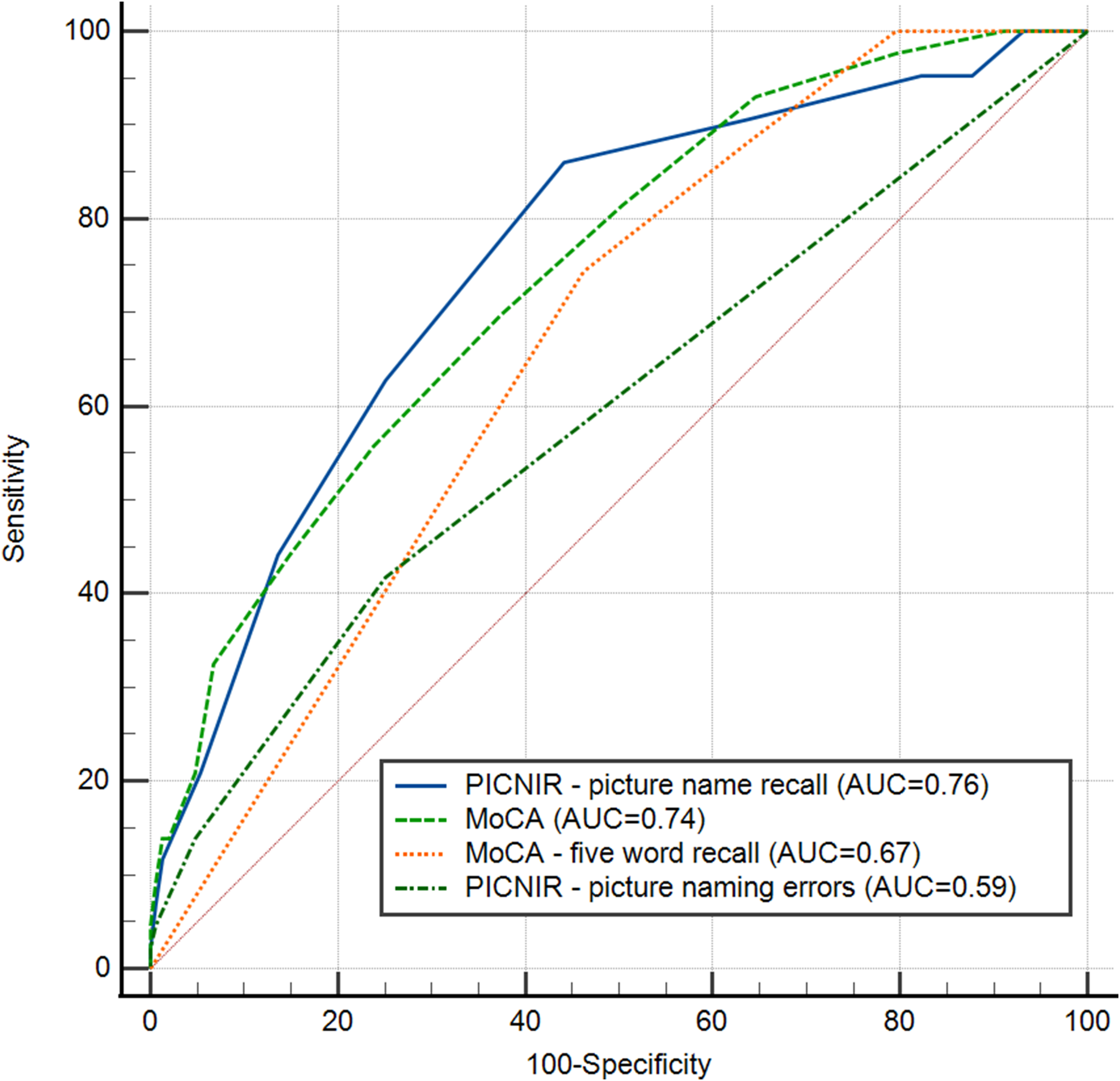
Receiver operating curve characterizes diagnostic yield based on the relationship between sensitivity and inverse specificity for the number of picture naming errors, picture naming recall in the PICNIR test, MoCA score, and MoCA five-word recall between people with very mild cognitive deficits and cognitively normal elderly individuals.
Convergent validity between the PICNIR and the MoCA, neuropsychological tests, and questionnaires
We examined correlations between the PICNIR test and the MoCA, traditional neuropsychological tests of memory and other cognitive functions, and questionnaire results. Selected neuropsychological findings for both groups are displayed in Supplemental Table 2. We did not observe correlations with picture naming errors (data not shown), possibly due to the narrow score range of this subtest (0–4) or due to assessing unique cognitive components. However, the second subtest, i.e., PICNIR picture name recall, exhibited significant correlations with MoCA scores (r = + 0.3; p < 0.0001), scores of all memory tests (Table 3A), scores of most non-memory tests (Table 3B), and FAQ questionnaire scores, but not with GDS, BAI, and BDI scores (Table 3C) in the total sample. A moderate relationship between the PICNIR recall and the MoCA was observed in the vMCI subgroup (r = 0.50; p = 0.0006).
Correlations between picture recall scores of the PICNIR (PICNIR-PICR) and scores of memory neuropsychological tests (A), non-memory neuropsychological tests (B), and questionnaires (C) ordered by correlation values in the total sample (n = 190).
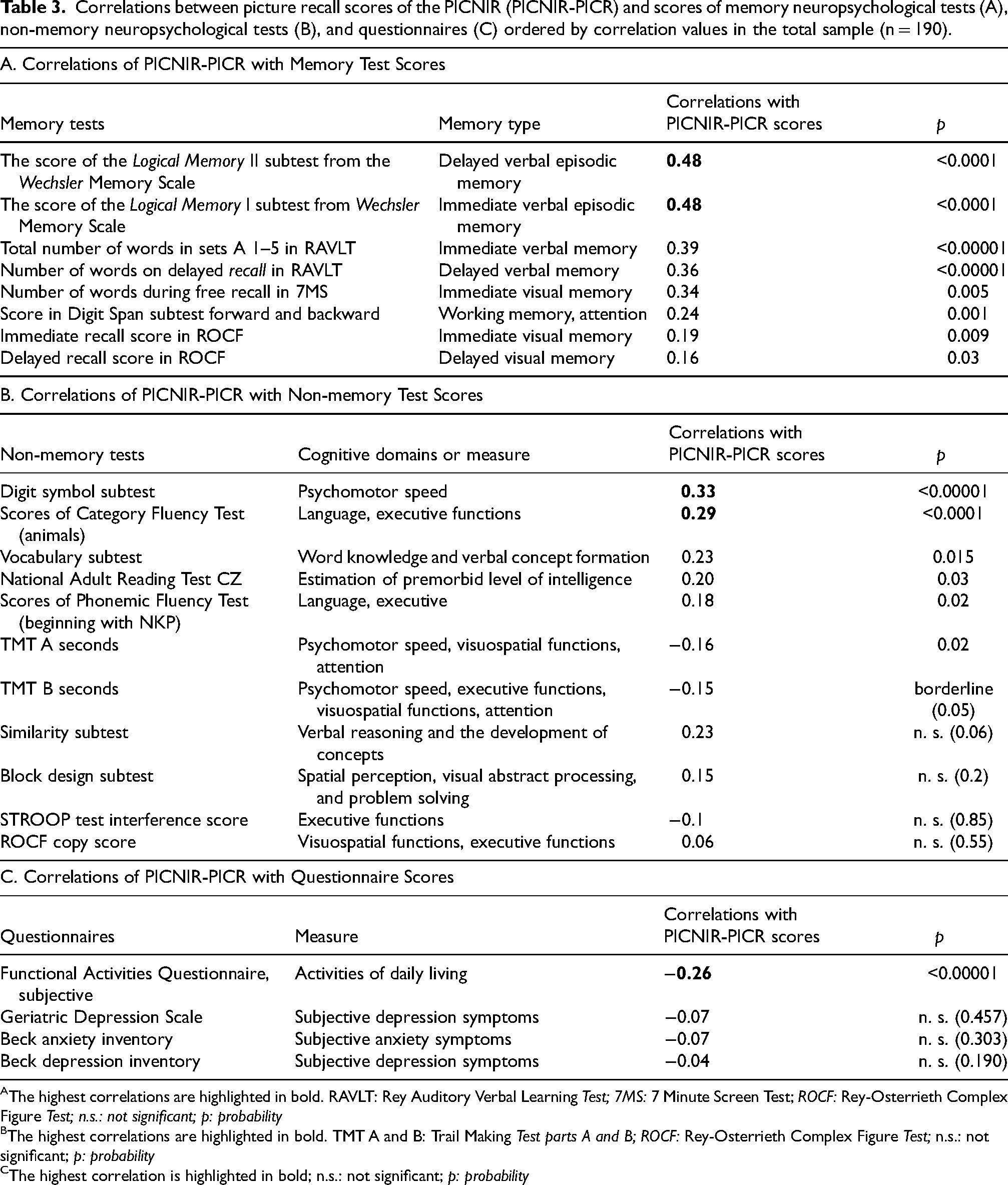
The highest correlations are highlighted in bold. RAVLT: Rey Auditory Verbal Learning Test; 7MS: 7 Minute Screen Test; ROCF: Rey-Osterrieth Complex Figure Test; n.s.: not significant; p: probability
The highest correlations are highlighted in bold. TMT A and B: Trail Making Test parts A and B; ROCF: Rey-Osterrieth Complex Figure Test; n.s.: not significant; p: probability
The highest correlation is highlighted in bold; n.s.: not significant; p: probability
Figure 3 shows the correlations between the number of correctly recalled picture names in the PICNIR test and MoCA scores within each subgroup. The MoCA scores varied slightly in cognitively normal individuals, while the PICNIR recall ranged from 3 to 14 picture names (r = 0.17; p = 0.04).
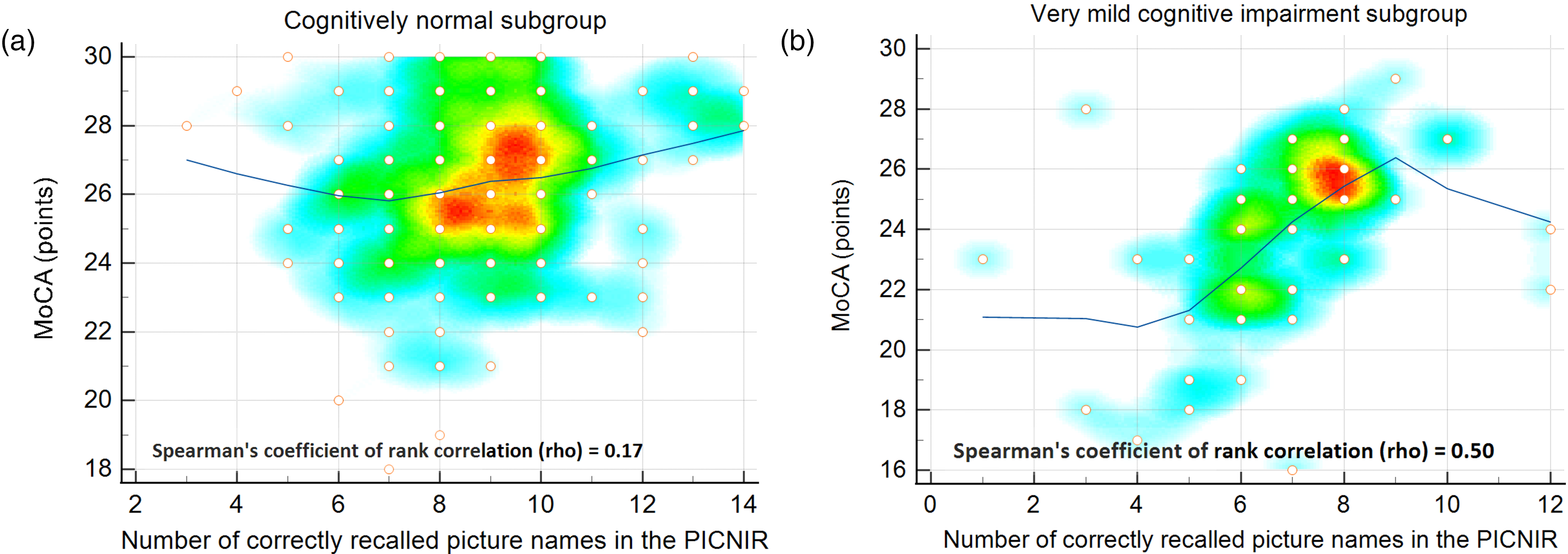
Correlations between the numbers of correctly recalled picture names in the PICNIR test and MoCA scores in cognitively normal elderly individuals (A) and people with very mild cognitive deficits (B).
Discussion
The newly developed innovative PICNIR test is an efficient and valid instrument offering several advantages for detecting subtle cognitive deficits. The unique feature of the PICNIR test is that it combines two cognitive tests, one for naming and one for recall, that use the same set of pictures to assess several cognitive functions simultaneously, i.e., handwriting, language, lexical access, long-term semantic memory, and short-term episodic memory. Even with two tasks in one instrument, the PICNIR is still very brief, only requiring about four minutes to administer and evaluate. The test is designed to be almost self-administered and uses a one-page test form. Moreover, administrators benefit from free time during participant´s writing of picture names in the naming and recall phase, which may be reminiscent of “picnic” in the acronym of the PICNIR. Meanwhile, administrators have an opportunity to observe the order of picture naming, which can provide additional qualitative information and insights into thinking organization and cognitive processing.
Healthy individuals follow a systematic procedure to name pictures from the left to the right and from the top to the bottom, similar to text reading. In contrast, some patients randomly skip from one picture to another in a chaotic manner. We can assume that this style indicates disordered or dysexecutive thinking.
The results of our study confirm the validity of the PICNIR in daily clinical practice across various medical disciplines and purposes. The validity of the PICNIR was demonstrated by the significant and discriminant differences detected between the two closely related groups (discriminant validity) and significant correlations with several neuropsychological tests and the FAQ assessments of activities of daily living (convergent validity) but not with depression questionnaires. Importantly, the PICNIR can effectively detect subtle cognitive deficits.
It is essential to point out that neither group consisted of patients. Both groups comprised volunteers who lived independently and were differentiated by a decline in neuropsychological test scores, with scores in one group being more than one standard deviation below the mean. Several indicators demonstrated a close relationship between the groups. The vMCI group achieved an average MoCA-CZ score of 24 points, indicating relatively high cognitive functioning. The difference between the two groups was only two points (Table 2). The average MoCA scores of both groups corresponded to approximately 28–29 points on the MMSE as shown in Table 2. 66 Their activities of daily living were normal, with only a minimal but significant difference of one point in FAQ scores between the two groups. Taken together, the participants were cognitively similar, i.e., the cognitive difference between the two groups was negligible.
The diagnostic properties of the PICNIR test were also compared with those of the MoCA, which is commonly used to detect MCI. Our data showed that the AUC of the PICNIR was numerically higher and statistically comparable to that of the MoCA. The sensitivities and specificities were also similar (Table 2, Figure 2). Diagnostic accuracy could have been improved if MCI patients had been used for comparison since the MoCA had better sensitivity and specificity in our previous study. 49 The PICNIR testing would also yield better results. Supplemental Table 3 shows the psychometric comparisons of the PICNIR with other very brief tests (i.e., less than 5 min), the MoCA, and the MMSE. Interestingly, all studies involving MoCA assessments of those with a Slavonic European background consistently report lower sensitivities and specificities for MCI detection compared to the original Canadian study (Supplemental Table 3). In scenarios involving dementia, the PICNIR demonstrated excellent sensitivity (100%) and specificity (97%). 51
We expected very few naming errors in both groups. The pictures were included in the PICNIR if CN individuals named them without any errors. The set contains pictures that are difficult to name by patients with more advanced cognitive impairment. Therefore, vMCI individuals (not patients), who are cognitively close to CN, also made minimum errors. The naming subtest of the PICNIR is useful for monitoring cognitive deterioration and early detection of language disorders in neurodegenerative diseases or stroke. Our long-term clinical experience and use of the PICNIR indicate that naming deficits increase and picture recall decreases during cognitive deterioration over follow-up periods. Thus, the importance of the naming part becomes more evident in patients. Naming errors on the PICNIR test or delayed recall of five words on the MoCA yielded equivalent results in differentiating between the two groups. This is a positive outcome for the PICNIR since picture naming is typically considered a less cognitively demanding task than memory. However, in our study, the two were comparable.
This is the first report to explore the convergent validity of traditional neuropsychological tests with the PICNIR. The number of correctly recalled picture names in the PICNIR correlated with the scores of several memory and non-memory tests and the FAQ. This suggests that the PICNIR primarily assesses immediate and delayed verbal episodic memory. To a lesser extent, the PICNIR was related to visual and working memory. It also has non-memory components, such as psychomotor speed, and language. The associations were logically lower than those with memory tests. Psychomotor speed tests reflected the timed recall phase of the PICNIR for one minute. Verbal fluency tests mirrored picture names in the recall part, similarly in limited time. Thus, the PICNIR covers several cognitive functions, including memory, which is the most important. The multi-domain cognitive nature of the PICNIR makes it particularly suitable for general use and diverse purposes. Furthermore, the correlation with functional assessments using the FAQ questionnaire demonstrates the ecological and practical validity of the PICNIR test and addresses real challenges faced by patients and their caregivers. On the other hand, performance on the PICNIR recall task (Subtest 2) was unaffected by anxiety and depression measured by the BAI, BDS, and GDS questionnaires.
The PICNIR offers several advantages. It combines two distinct tasks assessing writing and semantic and short-term episodic memory in about four minutes. In reality, it is even less because the majority of the PICNIR is self-administered by the examinees, i.e., the test requires very little input from test administrators. Additional benefits include easy administration, scoring, and interpretation for administrators while being relatively challenging for patients. The test is designed to be administered by individuals from various medical disciplines or caregivers. The test form is organized so that all necessary information for testing, administration, and scoring is on a single page. The clear, unambiguous drawings are intentionally in black and white for clear printing on any standard printer. The PICNIR is also suitable for individuals with impaired hearing since the instructions are short and straightforward, and the test itself is visual in nature (i.e., picture identification).
The main limitation of giving the PICNIR test is the need for the printed picture form. Additionally, patients or clients need vision, writing skills, and motor function of the writing hand appropriate for the test. In such cases, oral administration of the test is an option. It involves reducing the recall time to half a minute, as well as a few other minor adaptations for oral use. 57 Further studies are needed to confirm the usefulness of the PICNIR test by testing patients with confirmed MCI. The next step involves determining the cut-off values for the PICNIR test based on demographic characteristics. They are essential for interpreting the test results accurately.
In conclusion, the PICNIR is sensitive to the presence of vMCI and can be used in clinical settings where assessment time is often limited. Both discriminant and convergent validity were confirmed even in those with vMCI, particularly regarding deficits in long-term semantic memory, aphasia and dysgraphia, and short-term episodic memory. The PICNIR is especially useful for patients or clients with cognitive complaints but no functional impairment. Adaptations for use in other countries are encouraged so that the utility of PICNIR can be assessed in different clinical and research settings. Because of its brevity and sensitivity, we believe the PICNIR can be a valuable tool with diverse applications in busy clinical settings.
The English version of the PICNIR can be downloaded easily and free of charge from our website https://www.abadeco.cz/learn-and-download-tests/picture-naming-and-immediate-recall-picnir. An educational video with English subtitles demonstrates proper administration and scoring and is available on Ales Bartos's YouTube channel (https://www.youtube.com/watch?v = cbJGtPG-nVA). Ales Bartos holds the copyright and makes this test freely available for non-commercial use in clinical practice, education, and research. Other use requires permission from the corresponding author.
Supplemental Material
sj-docx-1-alz-10.1177_13872877241289385 - Supplemental material for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment
Supplemental material, sj-docx-1-alz-10.1177_13872877241289385 for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment by Ales Bartos and Sofie Diondet in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-2-alz-10.1177_13872877241289385 - Supplemental material for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment
Supplemental material, sj-docx-2-alz-10.1177_13872877241289385 for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment by Ales Bartos and Sofie Diondet in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-3-alz-10.1177_13872877241289385 - Supplemental material for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment
Supplemental material, sj-docx-3-alz-10.1177_13872877241289385 for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment by Ales Bartos and Sofie Diondet in Journal of Alzheimer's Disease
Supplemental Material
sj-docx-4-alz-10.1177_13872877241289385 - Supplemental material for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment
Supplemental material, sj-docx-4-alz-10.1177_13872877241289385 for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment by Ales Bartos and Sofie Diondet in Journal of Alzheimer's Disease
Supplemental Material
sj-pdf-5-alz-10.1177_13872877241289385 - Supplemental material for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment
Supplemental material, sj-pdf-5-alz-10.1177_13872877241289385 for Sensitive written hedgehog PICture Naming and Immediate Recall (PICNIR) as a valid and brief test of semantic and short-term episodic memory for very mild cognitive impairment by Ales Bartos and Sofie Diondet in Journal of Alzheimer's Disease
Footnotes
Acknowledgments
ChatGPT, version 3.5, a language model developed by OpenAI (https://www.openai.com) and DeepL (![]() ) were used for language refinement of this manuscript. The authors thank Thomas Secrest for editing the English version of the manuscript.
) were used for language refinement of this manuscript. The authors thank Thomas Secrest for editing the English version of the manuscript.
Statements and declarations
Author contributions
Ales Bartos, PhD, M.D. (Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Visualization; Writing – original draft; Writing – review & editing); Sofie Diondet (Data curation; Formal analysis; Writing – review & editing).
Funding
This study was supported by Neuroscience COOPERATIO [207038] from Charles University, Development of research organizations from the Ministry of Health [Kralovske Vinohrady University Hospital, 00064173], and the state support of the Technology Agency of the Czech Republic within the SIGMA Programme [the project TQ01000332 Telemedicine self-examination of speech and memory for rapid detection of cognitive impairments using machine learning methods].
Declaration of conflicting interests
Ales Bartos developed the PICNIR test
Data availability
The data supporting the findings of this study are within supplemental material of the article and available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.