
Abstract
In 2017, the European Medicines Agency staged the first effort at democratic innovation within transnational European Union institutions directly influencing the transnational regulation of medicines. Alongside its public consultation on epilepsy drug Valproate, European Medicines Agency included a public hearing involving representatives of patients and testimony from those directly affected by the medicines. Using this critical case study, the article argues from a deliberative democratic perspective that although the hearing in many ways exhibited the traditional shortcomings of elite-driven deliberation, it also demonstrated unexpected and surprising deliberative qualities. Based on new quantitative analysis of the hearing using the Discourse Quality Index, and qualitative observation of over 4 hours of footage, the article argues European Medicines Agency’s hearing facilitated equitable access and influence of patients and members of the public who had previously been excluded from decision making on drug distribution. These findings provide important new evidence of the deliberative democratic value of public hearings.
Keywords
Independent regulatory agencies (IRAs) like the European Medicines Agency (EMA) and European Food Safety Authority (EFSA) have been touted since the 1990s as potentially important bodies for improving the European Union’s (EU) ‘democratic deficit’. Some have argued they provide ‘output legitimacy’ by ensuring the safety of consumer products distributed in the European Single Market (e.g. medicines and food), while others have added their democratic potential in ‘reaching out’ to a range of relevant societal and economic ‘stakeholders’ (Braun and Busuioc, 2020). The latter claim raises the expectation IRAs might contribute to open and inclusive public reasoning at a transnational level or ‘deliberative democracy’ (Maggetti, 2010). This prospect was raised by the European Commission in its 2001 White Paper on Governance (Parker, 2019) and has been hinted at by existing studies (Schmidt and Wood, 2019). However, IRAs’ engagement has generally been limited to relatively close groups of stakeholders in industry and non-governmental organisations, and to issue-based consultations (Pérez-Durán, 2019). While such constraints can be justified on functionalist grounds, they seem disappointing and ‘technocratic’ by ideal deliberative democratic standards. Is it possible that IRAs can really enable deliberative democracy in a way that squares with their regulatory functions? This article suggests it can, by applying the concept of democratic mending to a case study of IRA engagement activities, specifically the public hearing (Hendriks et al., 2020).
In 2017, EMA staged not only a public consultation on Valproate, an epilepsy medicine whose safety had come under question, but a public hearing involving representatives of patients and testimony from those directly affected by the medicine. The EMA promotes public hearings as opportunities for ‘working directly with people affected by [a] medicine’, which have real impact on Agency decisions: ‘Contribution(s) from the public at hearings will inform PRAC (Pharmacovigilance Risk Assessment Committee) decision making’ (EMA, 2018: 2). Public hearings are more ambitious than standard stakeholder engagement exercises. Any member of the public can apply to attend the hearing and individuals who have a specific interest in the policy issue being debated are encouraged to attend and report their experience in person. This procedure provides an important opportunity to understand how EU IRAs can undertake what Hendriks et al. (2020) call ‘democratic mending’ by enhancing deliberation between underrepresented groups and regulatory decision-making processes. It hence provides an unlikely, but potentially compelling, case study of an IRA enabling ‘connectivity’ between elite and non-elite groups in deliberating a key regulatory issue, thus potentially contributing to a wider ‘deliberative democratic system’ (Parkinson and Mansbridge, 2012).
This article assesses the extent to which the EMA’s public hearing was successful in achieving criteria for good democratic deliberation. Using the Discourse Quality Index (DQI), I coded 4 hours of a video of the hearing (https://www.youtube.com/watch?reload=9&v=CzeJSzkrygM#action=share). I complemented this with qualitative analysis interpreting the value and limits of the hearing. The core argument is EMA’s public hearing on Valproate-enabled deliberative democracy to the extent that it facilitated equitable access and influence of patients and members of the public who had previously been excluded from decision making on the distribution of the drug. I emphasise the way the hearing was set up in the style of a law court, with a democratic representative from the European Parliament (EP) present, and participants were allowed to use visual props to facilitate their argument. This allowed patients to tell profoundly powerful stories about the injustices they, and their families, had experienced. These stories compelled ‘elite’ actors, including industry and professional participants, to respect their demands and led to a transformation in how Valproate is regulated within the EU. The article shows how, when introduced in carefully curated ways, public hearings can facilitate moments of relatively ‘radical’ deliberation in IRAs usually defined by ‘output-oriented’ technical goals and ‘traditional’ stakeholder engagement (Pérez-Durán, 2019). In doing so, it identifies three methods of ‘democratic mending’ IRA officials can use during public hearings:
Demonstrating reflexivity by recognising the limits of the regulatory process;
Enabling storytelling by showing deference to non-elite actors to explain injustices they have experienced;
Embedding visual symbols of power to establish the importance of the hearing among all participants.
The article proceeds in five sections. First, it establishes the importance of ‘democratic mending’ for IRAs by conceptualising the value of performance in democracy and governance, and how ‘mending’ or ‘repair work’ involves performance within the policy makers’ day-to-day jobs. Second, it introduces the methodology, and details and justifies the Valproate case study, including the ‘puzzle’ of why the outcome of the process favoured non-elite actors, including Valproate patients, over pharmaceutical firms. Third, it analyses findings from a quantitative application of the DQI to the public hearing. Fourth, it presents qualitative observational analysis of the hearing video, highlighting three key methods of ‘repair work’ explaining why the public hearing was successful in extending the influence of non-elite groups over the regulatory decision. Fifth, the article discusses the conceptual implications of the findings for identifying methods of ‘democratic mending’. It concludes by suggesting that components of the DQI – storytelling and questioning – can enable non-elite actors to prompt other deliberative qualities in elite participants (respect for alternative groups and views).
Democratic mending, public hearings and IRAs
This article conceptualises the democratic value of public hearings within IRAs using the concept of ‘democratic mending’. It first outlines the problem that IRAs are constrained in how they can improve democratic governance in the EU, then shows the relevance of the ‘democratic mending’ concept in public and regulatory governance, and then points to the potential of IRAs engaging in democratic mending via public hearings.
IRAs and the EU’s ‘democratic deficit’
IRAs are unelected autonomous organisations responsible for authoring regulations that set quality standards of key commodities in the European Single Market, most prominently food, chemical substances, and medicines and health care products. Scholars have justified the creation of IRAs on the basis that they provide ‘credible commitment’ to long-term policy objectives, thus balancing alongside more explicitly ‘politicised’ aspects of the EU’s institutional order (Krapohl, 2004). The argument is that IRAs balance majoritarian institutions like the EP as part of a liberal, ‘Madisonian’ constitutional order (Miller, 2000). However, critical questions have long been raised about whether IRAs genuinely contribute to effective democratic governance (Papadopoulos, 2003). Stie (2021) argues that a growing range of crises show that the ‘input’ legitimacy of the EU cannot be divorced from ‘output’ legitimacy – just because IRAs are effective in regulating the quality of goods in the Single Market does not make the EU immune from allegations of a ‘democratic deficit’. Alter and Zürn (2020) and Zürn (2021) have even theorised that the growth of IRAs can be linked to the growth in electoral politics of authoritarian populism, via a ‘backlash’ against so-called ‘liberal elite’ unelected bodies.
Key questions have hence been raised about the practices of IRAs to promote democratic values of inclusion, diversity and engagement (Schmidt and Wood, 2019). How, and to what extent, can IRAs involve relevant ‘stakeholders’ and the wider public in their work? In what way could IRAs become responsive to the public? Recent studies have shown the relatively narrow range of stakeholders involved by IRAs in regulatory consultations and stakeholder inclusion in management boards (Beyers and Arras, 2020). This research shows that IRAs principally involve stakeholders from industry, although, interestingly, less so in ‘closed’ consultations than open ones (Arras and Beyers, 2020). This research primarily examines formal inclusion rather than delving into the actual procedures and processes of engagement, although research in Belgium does provide experimental survey evidence that IRA stakeholder inclusion positively influences the quality of decision making (Beyers and Arras, 2021).
Where research examines the breadth of stakeholder interactions with IRAs, it usually begins from theories of interest group influence (Pérez-Durán, 2019) and sociological legitimacy (Wood, 2018). These studies show IRAs are limited in the variety of actors they can engage by the formal requirements imposed upon them by their mandates from the EU’s core institutions. For example, while stakeholder engagement is required for the EFSA, its engagement is limited to ‘representative organisations that have an interest in its work or in the wider food and feed sector’ (EFSA, 2016). In practice, this includes a still relatively narrow range of potential groups identified by EFSA and of relevance to its core functions (Wood, 2018). How then is it possible for IRAs to enable the EU to respond more effectively to the democratic deficit? My argument is that they may do so through the relatively mundane, yet democratically powerful, practice of democratic mending.
Democratic performance and democratic mending
The role of ‘mending’, and its potential for IRAs, can be seen once the broader importance of performance in democracy, and its intersection with public governance, is understood. First, this article follows Parkinson in defining democracy as ‘decisive public reasoning on common issues among all affected interests’ (Parkinson, 2012: 47). Parkinson uses this definition to make the case that such public reasoning requires performance from those tasked with doing it: narration is an essential first step in any democracy that aims at solving real problems, and . . . performance is necessary to bring narratives to the attention of fellow citizens. (Parkinson, 2012: 47–48)
Bringing those ‘issues to the attention of fellow citizens’ means that actors in a democracy can (and do) play different ‘roles’ within the public reasoning (deliberation) process. Their identities shift regularly – for example, a politician can play the political campaigner speaking to potential voters, the international statesman speaking to other world leaders, or the consoling and diligent ‘social worker’ helping constituents going through hard times (Crewe, 2015). In all cases, they make ‘claims’ about how to solve this or that problem, all in service of bringing their understanding of the problem – their narrative about its cause and solution – to the attention of their audience.
How is this notion of democracy as ‘performance’ relevant for public governance? Maarten Hajer (2009) makes a similar argument to Parkinson but emphasises how policy makers ‘perform’ their authority is crucial for that authority having effect. Hajer and Uitermark argue through a series of case studies that ‘those who have politico-administrative functions cannot rely on the rational-legal authority they derive from the institutional position they have been given’ (Hajer and Uitermark, 2008: 21). Instead, Hajer argues in Authoritative Governance, they have to ‘create de facto authority by acting out their role in a sequence of situations . . . authority is a relational notion’ (Hajer, 2009: 21). While this position may make it seem more difficult for policy makers in their jobs – emphasising the constant need for them to ‘perform’ for their ‘stakeholders’ to be perceived as legitimate authorities and do their jobs effectively – it also gives them a certain remit to creatively ‘innovate’ their role. So again, just as the politician acts as a statesperson, campaigner or ‘glorified social worker’, so the civil servant or bureaucrat can perform as the independent expert, the diligent and neutral agent serving the public, or the ‘innovative’ entrepreneur (Ebinger et al., 2021). Bureaucrats working within IRAs do not simply carry out a predefined job. As Littoz-Monnet (2014) argues, IRAs can use ambiguities in their formal roles to ‘make policy’, as well as implement regulations. Particularly once it is recognised that the power of IRAs is to make authoritative decisions with consequences for millions of people, it becomes clear that the way they use this autonomy to perform these roles may also have significant implications for democracy. It is here that we can see an intersection between the democratic and regulatory potential of bureaucrats in IRAs ‘performing’ the role of ‘democratic mending’.
In Mending Democracy, Hendriks et al. (2020) chart a novel way of conceptualising how policy makers can improve democracy through ‘everyday action’ within the boundaries of their day-to-day jobs. ‘Mending’ democracy involves a performance of one’s public duty, in the role of the metaphorical repair worker or ‘healer’. Performing democratic mending involves identifying points of systemic weakness between public institutions and the communities they serve. It then involves deliberately – performatively – creating ways of involving those who have experienced unfair or unjust outcomes, or feel disconnected from those institutions to improve their institutional influence – the work of ‘democratic mending’ in practice. Democratic mending can involve the establishment of distinct practices or procedures to enable the mending process, but it does not have to. Democratic mending can be conducted by public sector professionals in their everyday jobs within the boundaries of established procedure. Moreover, those practices or procedures do not have to be ‘innovative’ in the sense of being entirely novel. They do not have to meet the high, arguably unrealistic, bar set by the widely popular ‘democratic innovation’ concept (Smith, 2009). Nevertheless, in practice, democratic mending does similar work to democratic innovations. Hendriks et al. (2020) conceptualise mending as an important part of what Parkinson and Mansbridge (2012: 4–5) called the ‘deliberative system’, that is, a ‘set of distinguishable, differentiated, but to some degree interdependent parts, often with distributed functions and a division of labour’, which is deliberative, or ‘encompasses a talk-based approach to political conflict and problem-solving – through arguing, demonstrating, expressing, and persuading’. This idea translates the classic normative ideal of deliberative democracy, into a programme for systematically planning for liberal democratic societies to democratise by enhancing deliberation in structured institutional spaces in those societies. Within deliberative systems, there are key institutional sites of power where deliberation is particularly important and can ‘connect’ informal political networks to structured sites where deliberation can be ‘staged’ with elite experts (Hendriks, 2016).
Democratic mending in IRAs through public hearings
How, then, can officials in IRAs engage in democratic mending? IRAs are well known to be constrained by the regulatory remits provided to them by their founding mandates, and their accountability to the European Commission, Parliament and Council. This article suggests that, for IRAs at the EU level, public hearings may be important opportunities for ‘democratic mending’. Public hearings are an old democratic practice, dating back at least to Ancient Athens. They are also widespread internationally, particularly in local governance (Adams, 2004). However, scholarship on democracy has not looked upon them positively. In his study of public hearings in the United States, Karpowitz (2006: 5) notes that ‘on those rare occasions when scholars have looked closely at local public hearings and town hall meetings, their responses have been, for the most part, witheringly critical’. These sites are far from ‘ideally’ deliberative. As Karpowitz (2006: 5) notes, ‘Not only can [public hearing] meetings be long, difficult, and boring, but they are also, most say, poor examples of deliberation because they rarely allow for effective give-and-talk among those present’. Scholars note significant limitations, particularly due to the dominance of elite decision makers: ‘For many, such meetings come across as frustratingly non-responsive because decisionmakers seem often to arrive with their minds already made up’ (Karpowitz, 2006: 5). Scholars have been sceptical that elite projects of ‘deliberation’ through consultations with ‘stakeholders’ and the wider public run the risk of what Fung and Wright (2003: 265) call ‘participatory window-dressing’, essentially legitimating pre-existing elite consensus with inadequate ‘consultation’ – deliberation in name only. Simone Chambers (2017: 266) worries that such partitioning of ‘epistemic quality’ and ‘equal participation’ ‘flirt(s) with elitist theories of democracy . . . violat[ing] an essential defining feature of deliberative democracy, namely that epistemic quality and equal participation are tightly linked’.
Nevertheless, some scholars suggest public hearings can add value by allowing citizens to make their voices heard to powerful elites, and provide a ‘tool that citizens can use to achieve political objectives’ (Adams, 2004). Karpowitz and Mansbridge (2005) defend public hearings as ‘deliberative in the minimal sense that they [represent] an opportunity for citizens to give public reasons for their opinions and to hear the opinions of others’. Wider literature shows that how elites conduct themselves in designing or facilitating democratic processes has been highlighted as key to their success (Escobar, 2019). Bureaucrats and experts can be ‘boundary spanners’ in collaborative initiatives with citizens (Sørensen et al., 2020); they can stimulate deliberation with citizens to evaluate policy during implementation (Boswell and Corbett, 2018), or encouraging participation from diverse groups to enhance capacity in legislative select committees (Hendriks et al., 2019). As an elite-led process, public hearings are not necessarily problematic. Moreover, when viewed through the conceptual lens of ‘mending’, public hearings are opportunities for policy makers keen on enhancing the democratic quality of policy making to take on the performative role of ‘mending’ in the context of their everyday jobs. They do not require entirely new institutional processes, as is required in democratic ‘innovation’ (Smith, 2009), and can work through the day-to-day processes of engagement public policy makers are required to undertake.
In our case, legislation has made provisions for EU institutions to use public hearings, under Article 20 of Regulation (EC) 726/2004, Article 31 or Article 107i of Directive 2001/83/EC (EMA, 2017: 2). Public policy makers at the EU level are allowed to use public hearings on the basis that these are used in connection with ‘safety referrals’. Hence, European policy makers can have agency in their everyday jobs to use public forums as advisory tools for decision making on the safety of products in the European Single Market. This power enables opportunities for them to use their discretion to seek to use forums as tools for ‘mending’ relationships between IRAs and communities who are distrustful of regulatory institutions and the process of regulation.
Moreover, because these public hearings are tied to ‘elite’ regulatory decision-making sites, they may contain the potential to be effective in shaping outcomes, because of their close proximity to the levers of institutional power. In particular, this article suggests that public hearings, when conducted effectively, may present genuine moments for radical deliberation within the acknowledged confines of elite-led, expert decision making. Deliberation here is ‘radical’ in the sense that individuals are ‘empowered, especially in the institutions that affect their everyday lives’ (Warren, 1996: 241). The experiences and understandings of marginalised groups are heard directly by those making the relevant decisions that will affect their lives, in a specific and targeted way that means the ‘staging’ of those experiences exercises a direct influence on the regulatory decision elites are tasked with. Moreover, because public hearings are directly linked into policy-making processes (because they are designed and controlled by elites), these events have disproportionately greater power and resonance with the wider political system, if they maximise the quality of deliberation within their forum (Papadopoulos, 2012).
Case selection and methodology
This article analyses the case of the EMA’s public hearing on Valproate in 2017. This hearing was designed as a democratic experiment. It was directly linked into a regulatory decision-making process; the hearing was included as one phase of a process of re-evaluating regulatory requirements for a medicine whose safety had come under question. The EMA stated the hearing was intended to ‘enrich the available scientific evidence’ (EMA, 2018) and public hearings more generally are described as going ‘beyond existing channels or stakeholder engagement’ (EMA, 2019). Moreover, the hearing was designed to give patients directly affected by Valproate ‘a voice’ in the process going much deeper than standard written submissions. As such, it could be argued that the Valproate hearing provided the opportunity for democratic mending, because of (1) its direct link to substantive regulatory decision making, and (2) the explicit attempt to ‘add value’ in terms of the depth of engagement of those communities who would not usually have a voice in EMA decision making.
This article uses the Valproate hearing as a ‘paradigmatic case’ of the potential of democratic mending in IRAs (Flyvbjerg, 2006). The Valproate hearing was the first attempt at institutionalising a physical public hearing within an established EU institution, with a self-professed direct impact on that institution’s policy. Most attempts at democratic ‘innovation’ at the transnational level, like the European Citizens Initiative, ‘failed to have any effect on the decision making process’ (Smith, 2013: 211). By contrast, in the Valproate hearing, patients and members of the public had a direct say in a regulatory decision-making process, while being subject to all the administrative, social, economic and political factors that would make reform likely to fail. Investigating the intricacies of how this reform played out as an opportunity for ‘democratic mending’ in detail will yield important insights into how, and through which methods, democratic mending can take place in IRAs.
The hearing was live streamed by video link with multiple camera angles showing participants speaking and the layout of the room, and an official summary was made available along with written submissions. This is useful both in terms of reinforcing how significant the agency itself viewed the hearing as an innovative exercise, and in providing a data source from which to evaluate it. It was possible to track and replay every minute of the hearing and make reflective notes. As such, the author watched and coded the full 4-hour hearing, both quantitatively and qualitatively, and referred back to the hearing transcript for clarifications. EMA also provided several supporting documents with detailed analysis of the problem, written feedback from stakeholder consultation and a detailed report of the final regulatory recommendation.
The case: Valproate
Understanding the context of public controversy around the public hearing is crucial for further explicating the importance of the EMA’s public hearing as an opportunity for democratic mending through deliberation. Valproate is a medicine used to treat epilepsy, bipolar disorder and sometimes migraine in EU member states. For some patients with severe cases, there are no other treatments available other than Valproate and similar substances (valproic acid, sodium valproate, valproate semisodium and valpromide). Valproate is not a new medicine – having been available by prescription in France since 1967. It has been approved for prescription in all EU member states. However, Valproate become known during the 2000s for significant side-effects among pregnant women, leading to abnormalities in new-born babies, particularly severe learning disabilities. Despite knowing its side-effects, some doctors prescribed Valproate to pregnant women without informing them of the full implications of its use, and many continued using it because of no known alternative treatment. In March 2017, at the request of the French medicines regulator, the Agence Nationale de Sécurité du Médicament et des Produits de Santé (ANSM), EMA began a Europe-wide review of Valproate and its effects, with the aim of strengthening regulatory guidelines for practitioners around the conditions under which Valproate can be prescribed.
The severe learning disabilities some Valproate patients found their children experiencing are serious issues of equity and justice. Campaigners argued pregnant women were not given enough information to make a balanced decision, by doctors who knew of the likely consequences for their children. Moreover, severe learning disabilities often suffered by children born from Valproate patients have implications for the entire life of those children, their mothers and families. Nevertheless, the freedom of patients with severe bipolar disorder or epilepsy to take Valproate must be taken into account when deciding on whether to place restrictions, or an outright prohibition, on its prescription to pregnant women. Some women refuse to be taken off the medicine despite knowing its likely side-effects, because it prevents severe pain they experience from epileptic attacks, bipolar episodes or migraines. Medical studies – for example, by the US Food and Drug Administration – suggest taking patients off Valproate suddenly can also have serious health impacts (https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-children-born-mothers-who-took-valproate-products-while-pregnant-may). The EMA’s consultation was thus conducted in a highly contestable field, both ethically and scientifically. Deliberation is particularly apt here, because the issue is contestable, with significant implications for equity and justice across the whole of Europe (Dryzek, 2002). EMA’s work is also used as a template for other smaller countries globally, so its review could arguably be said to have implications for regulatory policies focused on Valproate around the world.
A policy puzzle
What makes the Valproate case particularly interesting is the outcome unexpectedly favoured non-elite patients and the wider public, and imposed greater accountability on the pharmaceutical industry. The most powerful suggestion that the hearing was a ‘successful’ deliberative exercise is that it helped shape an eventual policy outcome that transformed the regulatory controls over the provision of Valproate in a way that demonstrates (or at least heavily implies) the influence of those who had started out in the debate as disadvantaged and receiving injustice in its provision. Such influence, or ‘consequentiality’, is an important deliberative democratic quality (Dryzek, 2002). This makes it a case particularly ripe for investigation into what led to this outcome.
In 2018, the PRAC announced its final decision to introduce stringent new controls on the provision and marketing of Valproate. These are summarised as follows:
Where licensed for migraine or bipolar disorder: In pregnancy – Valproate must not be used. In female patients from the time they become able to have children – Valproate must not be used unless the conditions of a new pregnancy prevention programme are met.
For epilepsy: In pregnancy – Valproate must not be used. However, it is recognised that for some women with epilepsy it may not be possible to stop Valproate and they may have to continue treatment (with appropriate specialist care) in pregnancy. In female patients from the time they become able to have children – Valproate must not be used unless the conditions of the new pregnancy prevention programme are met.
The PRAC has also recommended that the outer packaging of all Valproate medicines must include a visual warning about the risks in pregnancy. In addition to boxed text, this may include a symbol/pictogram, with the details to be adapted at national level.
A patient reminder card will also be attached to the outer package for pharmacists to discuss with the patient each time the medicine is dispensed.
Companies that market Valproate should also provide updated educational materials in the form of guides for health care professionals and patients (EMA, 2018).
These controls impose new obligations on pharmaceutical companies against the demands those companies made within the hearing. The manufacturer Sanofi argued for more communication by governments in providing Valproate, but demanded that Valproate not be banned for pregnant women with the relevant syndromes. The PRAC recommendation goes explicitly against this stated demand. Moreover, demands by patient/public participants were met in full, particularly demands to introduce new visual warnings on packaging and require pharmaceutical firms to produce and disseminate educational materials about the effects of Valproate. These recommendations then became legally binding as PRAC’s recommendations were validated by the Coordination Group for Mutual Recognition and Decentralised Procedures (Human) in March 2018, and adopted in full by the European Commission.
This outcome was not only a result of the public hearing nor was the result only an outcome of privileging the emotive arguments of patient representatives. The hearing was one part of a review encompassing ‘written submissions, expert meetings, meetings with stakeholders including healthcare professionals, patients’ organisations, patients and their families’ (EMA, 2018: 2). The PRAC’s recommendation, moreover, could not legally have relied on patients’ testimonies alone, but had to be justified on the basis of a balanced consideration of the range of evidence provided to come to a ‘scientific’ decision. However, crucially from our perspective, the hearing allowed representatives of those suffering from Valproate to exercise a particular kind of influence within the process that would not have been possible otherwise. One of the key requirements of deliberation is that participants should exercise ‘equal (or fair) influence over the outcomes of discourse’ (Beauvais and Bächtiger, 2016: 2).
How was this influence enabled in this particular instance against the odds of a heavily invested pharmaceutical corporation? This is the central puzzle that a mixed-method analysis of the hearing video enables this research to answer.
A mixed-method approach
This article assesses democratic mending through a mixed-method approach, first using the quantitative DQI and then qualitative visual observation. The DQI was used initially to map the contribution of each participant to the public hearing. This mapping shows how different contributors to the hearing exhibited deliberative democratic qualities, hence providing an overall assessment of how the exercise ‘scored’ in common indicators of deliberative democracy, and inequalities between groups in fulfilling these indicators. The findings of this analysis contrast with the outcome of the regulatory process, which unexpectedly favoured non-elite groups including patients and the public, despite them exhibiting lower qualities on the DQI. Qualitative visual observation is hence used to explain how the hearing was organised as an exercise in democratic ‘mending’, and to identify the methods of ‘repair’ through which this mending occurred. Combining these methods enables the article to show both the actors’ overall deliberative ‘qualities’, and to show how the curious outcome of the hearing can be explained through the agency of EMA officials doing ‘democratic mending’.
DQI
The DQI was developed by Steenbergen et al. (2003) and Steiner et al. (2004) to quantify how closely purportedly ‘deliberative’ discussions in political arenas got to the ‘ideal speech situation’ posited by Habermas. The DQI is criticised about the criteria it uses and assumptions it makes (Jaramillo and Steiner, 2014; King, 2009). Even if it were possible to quantify an ‘ideal’ outcome, the DQI does not cover all of the criteria that would need to be covered for assessing a case. Hence, King (2009: 4) argues, ‘Steenbergen et al’s attempt to operationalise the theory produces conceptions that distort, reduce and omit vital notions of the ideals it aims to measure’. On balance, because it evaluates speeches within a ‘debate’ as individual units, Steenbergen et al.’s index has been successfully applied to evaluating set-piece political speeches (Lord and Tamvaki, 2013), but has proved more difficult for assessing small group debates (Jaramillo and Steiner, 2014). For our purposes of analysing a public hearing, the DQI is useful as it is explicitly set up to code (and thus privilege) the quality of individual speakers’ contributions. As suggested above, public hearings are ‘minimally deliberative’ involving staged interventions regulated by a chair.
I watched the Valproate public hearing three times on YouTube in January and June 2019, and March 2020. I followed Steenbergen et al.’s (2003) original DQI coding scheme in the first two exercises, adding Gerber et al.’s (2018) adapted scheme, with two extra codes, in the third exercise to account for storytelling and questioning as deliberative criteria. I also adapted the coding scheme to the public hearing context (see Appendix 3 for details). After the first viewing and coding exercise, in light of reading and theoretical reflection, I recoded the hearing twice using DQI (and incorporating Gerber et al.’s added codes of storytelling and questioning the third time).
Visual observation
Alongside coding to the DQI, I conducted qualitative visual observation of the Valproate hearing, which was then analysed interpretively (Ercan et al., 2017). In advance of the research, I anticipated that explaining power dynamics within the hearing – a micro-scale event with a small number of actors involved – would require detailed qualitative data collection and interpretive analysis, going beyond the descriptive numerical data provided through the DQI to identify the importance of ‘people, experiences, actions and objects’ through which the public hearing gained meaning in the regulatory process (Ercan et al., 2017: 198). This interpretive element of the research allows me to supplement the quantitative mapping exercise, with a method for explaining the outcome that ‘opens up’ the hearing to explore the contextual elements of the hearing that empowered non-elite groups. ‘Opening up’ in practice means (1) paying careful attention to the ‘audiovisual’ data provided by the 4-hour video of the hearing that were not directly captured by the DQI, (2) summarising these elements ‘thematically’ with reference to relevant literature and (3) positing a ‘narrative’ that weaves these themes into an explanation of power dynamics (Bevir, 2006).
I hence made handwritten reflective notes on the video of the hearing during each coding session, identifying and naming ‘themes’ (e.g. storytelling, visual symbols) in an inductive way, highlighting elements of the hearing that appeared of significance during the observation. This note taking allowed me to develop a narrative, based on the themes identified, that explains the patterns found in the quantitative data. The narrative identifies three ‘methods of repair’ used by policy makers in the public hearing to empower non-elite groups. Importantly, the ‘methods of repair’ identified rely on my own interpretation – so I do not and cannot claim they are the definitive or objectively ‘correct’ interpretation. Rather, the aim is that the evidence provided for this interpretation ‘resonates’ with other researchers, and provides a useful contribution to debate and contestation over the ideal methods for ‘mending democracy’.
DQI: Results and analysis
Codes were applied to each ‘speech’ by a scheduled speaker in the public hearing. This included patients taking Valproate with epilepsy, bipolar disorder and migraine; victims of Valproate-related post-birth abnormalities; the pharmaceutical company Sanofi that sells Valproate; and professional representatives including pharmacists, medical scientists and authors of prominent academic studies of Valproate’s effects. Overall, there were 17 participants who were introduced as ‘speakers’ in the main part of the public hearing (3 hours 45 minutes). Two participants spoke twice making substantively different ‘demands’ (as Steenbergen et al. call them) and are thus coded as separate ‘speeches’ within the ‘debate’. Appendix 1 details all the speakers and their affiliations as described by EMA in its public documents. The coded speeches are not directly referenced for each participant to protect anonymity; however, these may be replicated by other researchers by coding the hearing manually using the project codebook (see Appendix 2).
One key problem with elite public hearings, existing research suggests, is that they privilege educated elite speakers who are invited ‘to the table’. The EMA hearing sought to overcome this by inviting public and patient representatives, who outnumbered elite industry/professional representatives. How did deliberation compare between them? Table 1 compares scores for patients and members of the public, with participants from industry and professional associations.
DQI scores for patient/public and industry professional participants in Valproate hearing. a
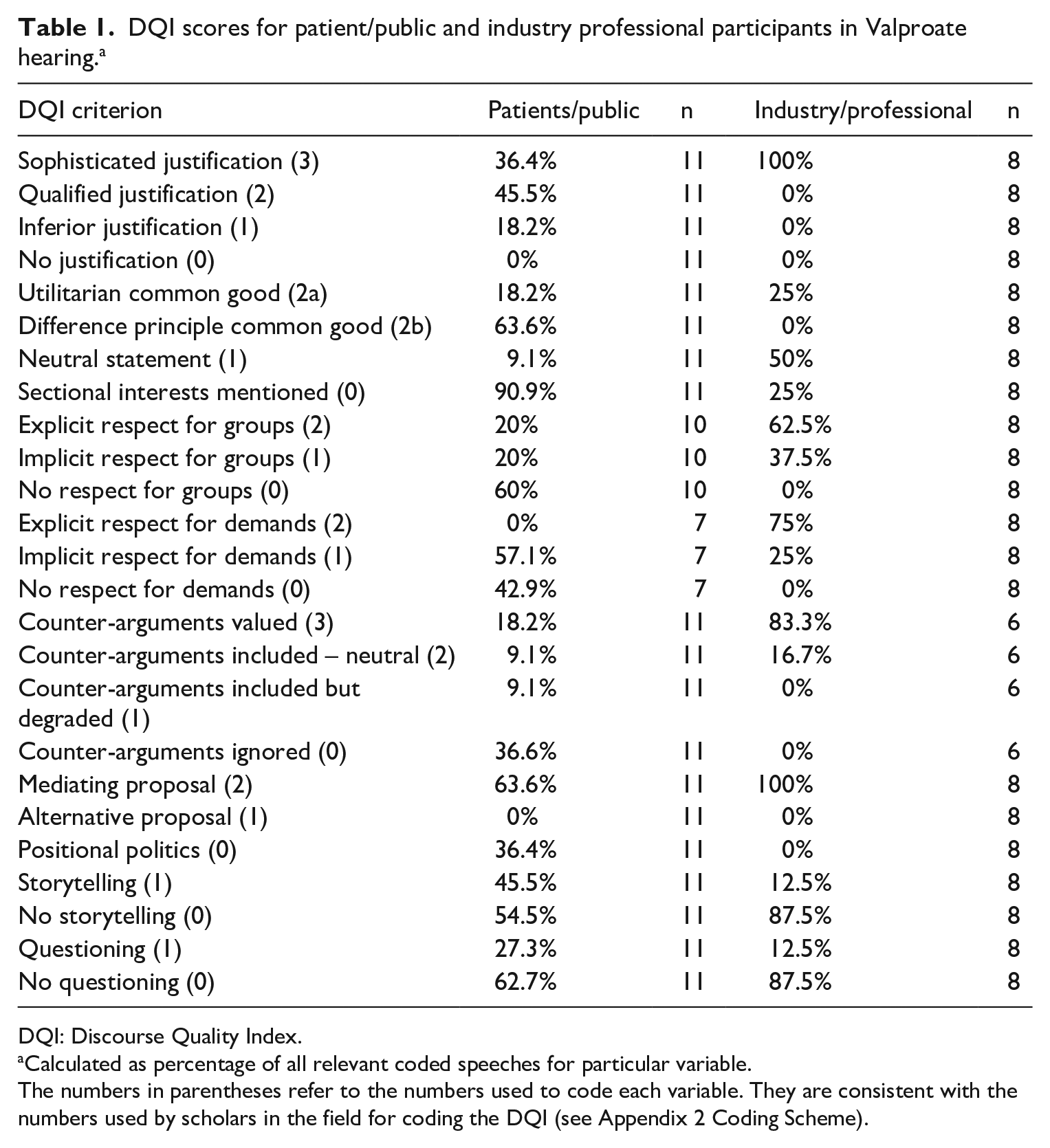
DQI: Discourse Quality Index.
Calculated as percentage of all relevant coded speeches for particular variable.
The numbers in parentheses refer to the numbers used to code each variable. They are consistent with the numbers used by scholars in the field for coding the DQI (see Appendix 2 Coding Scheme).
The scores demonstrate stark differences between groups in line with existing research on differential capacities to deliberate among elite and non-elite participants (Escobar, 2019). Industry and professional groups score higher on the majority of DQI components. Particularly striking are standards of justification, where 100% of industry/professional speakers scored the maximum of 3, compared with only 36.4% of patient/public participants. Similarly stark are differences between respect for groups and demands among industry/professionals (62.5% and 75% of speeches explicitly showed respect for groups and demands, respectively) compared with public/patients (20% and 0%, respectively). Industry representatives/professionals consistently recognised demands of public participants for improved communication between doctors and patients on Valproate risks, clear labelling on boxes and introducing mandatory controls ensuring doctors inform patients. By contrast, patients often ‘degraded’ (in Steenbergen et al.’s, 2003, words) industry efforts, suggesting they were at best negligent in explaining Valproate’s side-effects and at worst actively profiteering. There are also clear differences in terms of ‘constructive politics’ – the extent to which participants attempt to compromise or suggest solutions; 100% of representatives from industry sought mediating proposals, such as improving communication through pharmacists and intermediary professional bodies. By contrast, appeals by patient/public participants were emotive and often uncompromising, driven by individual experience and hostile to public information programmes they described as ineffective.
There were only three indicators where patient/public participants scored higher: reference to the common good; storytelling and questioning. First, industry/professional participants couched demands using scientific evidence, best practice, complexities around different types of epilepsy and the evidence base surrounding patient withdrawal from Valproate provision. These arguments, while sympathetic to equity claims and interests, focused neither on asserting group interests nor on conceptions of the common good. Patient/public participants, by contrast, focused almost exclusively on both their interests as representatives of Valproate patients and victims, and on issues of justice related to helping the disadvantaged. Speakers demanded mandatory clear pictures on packaging to ensure communication to parents about risk. Moreover, they told detailed stories of their own personal struggles with Valproate as emotive context for the hearing (although, as one speaker put it, ‘not evidential’). Third, and relatedly, patient/public participants were more likely to question the basis of the public hearing itself by, for example, voicing scepticism over the motives of the hearing and whether it would have any impact on the PRAC’s assessment process. The qualitative analysis below unpacks these differences and their implications in more detail.
Visual observation: Methods of ‘democratic repair work’
Quantitative analysis suggests EMA’s Valproate hearing fell into the same trap as many elite-driven forms of democratic innovation. Those supported by corporate pharmaceutical resources, or elite scientific education, were more articulate and exhibited ‘better’ discursive quality than members of the public and patients, who told emotional personal stories, openly disparaged elite actors and questioned the overall process. However, the DQI gives only a descriptive account of apparent inequalities between elite and non-elite groups in this public hearing. Interpretive analysis suggests not all components of deliberative quality need to be present for non-elite actors to be empowered. Rather, some elements, particularly storytelling and questioning, coupled with the symbolic ‘staging’ of the deliberation by PRAC, contributed towards empowering non-elites and rhetorically forcing non-elites to increase the ‘respect’ afforded to non-elite views. This, I suggest, shows us methods of ‘repair’ at work during the public hearing.
Demonstrating reflexivity
Hammond (2019) argues that deliberative democracy ought to be ‘an innately inclusive, itself reflexive and self-reflexive project’ rather than ‘a theory to be implemented’. As such, democratic ‘repair work’ must be conducted in a way that allows and appreciates the shortcomings and contradictions in engagement processes. The first moment during the discussion where contradictions are acknowledged is in the introductory remarks by EMA Head of Public Engagement, Juan Garcia Burgos, who notes that there is ‘no time for the specific debate’ during the hearing, and that the aims are constrained to allowing the PRAC to hear participants’ evidence and ask ‘clarification’ questions.
As the DQI analysis of ‘questioning’ showed, the process allowed reflexive remarks by non-elite participants about whether the hearing was simply a talking shop. As the first participant wryly noted, ‘if nothing comes from this the whole hearing will have been a waste of everyone’s time’. At several points, patients directly sought to expose power relations within the process. Two patients noted the presence of Sanofi in the room and called on them to stop ‘profit-making’ activities. One patient noted sarcastically that if Sanofi had been marketing a new drug, they would be enthusiastically giving information out, while others berated national governments for ‘doing nothing’ and that ‘neither Sanofi, nor anyone else, has been held accountable’.
While these statements were only tangentially related to the matter at hand, by allowing them to take place the PRAC enabled reflexivity during the public hearing in a way that exposed and allowed reflection on its shortcomings. In response to patients, the Chair of the PRAC mentioned on several occasions that the panel was ‘listening very carefully’ to their recommendations and reiterated the purpose of the hearing as enabling those who do not ‘usually’ have a say in such processes to have their ‘voice heard’.
Enabling storytelling
Storytelling has occupied an increasingly vital role within deliberative democratic theory. Where disadvantaged communities are given a ‘stage’ from which to tell, in detail, the extent and intensity of their suffering, this can have powerful effects on the deliberative process. Elite actors are forced to respond to the basic human tragedy they tell and put themselves in the positions of those who experience suffering (Mansbridge et al., 2010). The DQI analysis shows non-elite participants were more likely to engage in storytelling. This section unpacks how this had a rhetorical impact, which was enabled and amplified by EMA officials, hence the second ‘method’ of repair.
In the public hearing, patients and victims of Valproate were given the floor from the start of proceedings to tell their stories. One patient told of how she and others she knew had received their medicine in a plastic bag with no information or warnings on it. She described how because she was not made sufficiently aware of the risks of taking the drug, her children suffered: Behind the statistics are real human stories, and mine is that I am a mother of three adult children [states names], who have all been affected by the exposure of Valproate. We are living evidence of the risks and devastating impact of this drug. Two of my three boys require lifelong care and will never be able to have a normal life. They will never be able to get married. They will never be able to have children. They have been robbed of all the joys of life. (Author’s notes)
The Chair responded appreciatively to this story, stating that the PRAC ‘greatly appreciate your courage in bringing your own [long pause] issues into a situation of constructive proposals’. A young participant with Valproate syndrome told the story of her family’s experience dealing with her disease: ‘As a family we have been through hell. Called liars. Told we are fabricating our daughter’s condition. It’s ridiculous. The ignorance surrounding the rare disease is as bad as the disease itself’ (Author’s notes). The Chair again thanked her for ‘courageously sharing your thoughts which are extremely valuable to us’. Another woman with bipolar disorder related her own problems with taking Valproate and its effect on her mental health: I stand here as an individual woman with bipolar who has not received any input from any organisation. My thoughts are mine and mine alone and aren’t evidential. As a woman with bipolar I battle with feelings of shame, inadequacy and guilt, therefore I was terrified of getting pregnant while taking Valproate due to its proof of toxicity . . . I have always had a strong desire to have children and continue to express this to my mental health teams. However, for a number of years I had an unsympathetic psychiatrist who refused to stop providing Valproate despite my concerns and requests. I was actually told ‘perhaps, given your illness, you shouldn’t have children’, although I have never been detained under any mental health act. (Author’s notes)
This story about the unsympathetic psychiatrist had a visibly powerful effect on the rest of the room. Women in the audience behind the speaker can be seen shaking their heads, and at the end of her speech the room breaks into applause, despite there not being any applause for previous speakers. The Chair praises the speech as ‘tremendous and very altruistic’.
These stories exercised power in at least two ways. First, their rhetorical force demanded recognition from subsequent professional speakers from industry and academia. I noted down twice how speakers later in the hearing seemed to spontaneously make reference to, and express deference towards, the experiences of patients quoted above at the start of their own speeches. In the DQI, this creates the impression that industry and professional speakers made more of an effort at recognising groups and demands. Interpreting their speeches carefully, however, suggests that by recounting the injustices they faced, patients forced recognition of injustice in a way that would not otherwise have happened. In this respect, it could be argued that allowing a space for storytelling contributed directly to the deliberative quality of the hearing by pressurising elite speakers to recognise them. Of course, we cannot know the counter-factual here, whether if patients had not recounted their stories, elite speakers would not have recognised the importance of their experiences. Based on my interpretation of the video – the way subsequent speakers framed and made reference to those speeches – it seems unlikely.
Second, the power of these stories was enhanced by the Chair giving recognition to the stories and testimony of participants. By praising the impact of their stories and their ‘courageous’, ‘brave’ and ‘altruistic’ motives, the Chair not only reinforces the rhetorical power of those stories by breaking out of her neutral role, she emphasises the relevance of the stories to the PRAC’s overall assessment and the functional and epistemic demands it must also fulfil. This observation is in line with existing research showing the importance of ‘facilitation’ in deliberative exercises. Facilitators, who can range from trained conveners of mini-publics to moderators of online deliberative forums, play a crucial role in determining the internal quality of deliberation. In this instance, the PRAC Chair did so by elevating personal stories and projecting their value to the decision-making process as a whole, thus counteracting bias towards statistical data and scientific studies. Given the makeup of PRAC is almost exclusively trained medical scientists, this is a crucial mediating role.
Embedding visual symbols of power
Facilitating the influence of marginalised and vulnerable groups in elite arenas is a delicate process, particularly enabling them to recount powerful stories of deeply personal injustice. What methods of ‘repair’ helped enable those who gave personal stories to the PRAC present them in such a compelling way? Here, I suggest the embedding of visual symbols in the room of the hearing enabled the expression of these powerful stories. I identify three in particular: the layout of the room, the presence of a democratic representative and the use of visual props. These are symbols generating and expressing power, and enhancing the equity of the decision-making process.
First, the layout of the room creates a powerful atmosphere similar to a law court. The ‘robust argumentative capacity and privileged perspective’ of law courts, particularly constitutional courts, gives them significant authority in the public imagination (Mendes, 2013: 2). The video shows a long room (described by one elite actor as making things seem ‘a bit far away’) with EMA officials at one end, members of PRAC sat at adjacent tables with a space in the middle, leading to a plinth to which speakers were called. A translator sat alongside non-English speakers, also pouring speakers’ water. Behind the speakers, there were several rows where both other speakers and members of the public were sat. The seats were full for most of the hearing. This testimonial, set-piece, atmosphere can be both daunting and facilitating for deliberative quality. On one hand, non-elite patients in particular struggled with nerves for the occasion. However, the way in which this setup gave an impression of participants being called as ‘witnesses’ created a feeling of drama and importance to the occasion. There is a sense, particularly at the start of proceedings, of the audience hanging on the words of participants as they ‘testify’ to their views and experiences. The court-like atmosphere is reinforced by the line-up of participants. Eleven public and patient demands were presented first, before eight industry and professional opinions were presented. This programme, which one professional representative lamented for only allowing him limited space because he was ‘twelfth on the bill’, mimics a ‘prosecution versus defence’ scheduling common in court rooms. The patients and public representatives are framed as those ‘on the attack’ while industry and professional representatives are framed as giving mitigating circumstances.
Second, the hearing also appears an empowered space because of the presence of democratic representation. An elected Member of European Parliament (MEP), Linda McAvan, sat at the front of the room next to the PRAC Chair, and explained at the beginning how the hearing had come about through EP legislation designed to require regulatory reviews in the field of medicines to be conducted via engagement with the public, and that she was there to report on its effectiveness. This gave a clear rationale – the hearing had been sanctioned, and was being monitored, by an elected democratic institution. McAvan’s presence was never directly referred to as an indicator of democratic legitimacy, but there were points her presence was noted in relation to the process as a whole. One participant noted they were glad McAvan was present given the work of her EP committee in the area of health, and several other participants expressed hope the hearing might have implications for practice on the basis it was a ‘serious’ decision-making venue.
Third, and finally, allowing participants to use visual symbols enhanced the power of patients and members of the public. One French participant leading a campaign to introduce a visual warning on the side of Valproate packaging spoke via the translator, but showed PRAC members an enlarged version of the warning sign (a black outline of a pregnant woman in a red circle with a cross). Another participant held up a plastic bag for PRAC members to see, which she claimed was one of the unmarked bags she had received her medication in with no description on the side of health warnings. I interpreted these as powerful symbols because they became objects of sustained questioning by PRAC members. They asked the speakers to elaborate further on the points the symbols were used to illustrate and then returned to them in questioning elite participants. As the final recommendations to include clear visual risk markers on packaging suggest, they may also have stuck in the minds of PRAC members as they went away to discuss their final recommendations privately.
The methods of ‘mending democracy’ in IRAs
This article shows public hearings can enable non-elite influence within IRAs by empowering disadvantaged actors through methods of democratic mending. In doing so, it responds to Hendriks et al.’s (2020: 31) call for an approach to democratic reform ‘that focuses analytic attention on “real life” actors, their practices, and the way they make sense of and navigate the complexities of social and political life’. A ‘grounded’ approach, they suggest, ‘enables us to see how citizens and other political actors are making connections and doing repair work in practice’ (Hendriks et al., 2020: 31). This article contributes to an understanding of what this ‘repair work’ actually involves in a particular regulatory scenario where there is an opportunity for such ‘repair’ to generate meaningful connections between elite and non-elite actors involved with the medicines regulatory system in the EU. Using the DQI, this article first showed how actors involved in EMA’s public hearing on Valproate measured up in terms of ‘deliberative quality’. This showed commonly acknowledged shortcomings, most prominently that elite actors scored higher on most facets of deliberative quality than non-elite patient and public representatives. However, visual observation and interpretive analysis enabled the study to identify some ‘methods’ that allowed the public hearing to empower non-elite actors to influence the overall decision. This ‘repair work’ includes demonstrating reflexivity, enabling storytelling and embedding visual symbols of power.
Theoretically, this article contributes to our understanding of democratic mending by identifying how these methods combine to empower non-elite actors in regulatory governance processes through ‘performance’ (Hajer, 2009; Parkinson, 2012). First, in this case study, reflexivity is performed to prompt self-awareness about how stakeholder engagement processes that claim to expand the range of involved actors in fact risk legitimating unequal power relationships between elite and non-elite actors. This method can be deployed by administrators organising engagement processes when non-elite actors express how they lack trust in those processes. In this case, the EMA’s administrators not only noted they were ‘listening closely’ and ‘taking note’ but also recognised the limitations of the public hearing to provoke a sustained ‘debate’ on the issue. This is a first step in the democratic mending process – performatively noticing the inadequacy of existing processes while nevertheless suggesting how those organising the process can respond to the views and demands of marginalised actors. Second, storytelling is a tool for democratic mending in the sense that the stories of non-elite actors are encouraged by administrators, and given space alongside data produced by elite actors, within the process. The non-elite actors involved in the process are given space to express their stories, and are encouraged and thanked for telling those stories. Third, mending can also involve carefully and attentively ‘setting the stage’ for deliberation by organising the physical setting of the room in which the public hearing is held. The room layout as equivalent to a court hearing, the presence of Linda McAvan MEP in a monitoring role, and allowing participants to use visual props to make relevant demands, created an equitable space giving non-elite participants opportunity to influence the process through powerful storytelling. This ‘staging’ is crucial for dramatising the importance of the hearing (Parkinson, 2012).
Beyond these conceptual contributions to the study of ‘democratic mending’, this article suggests two broader insights, for the application of the DQI and for broader debates about the prospects for democratising EU regulatory governance. First, as Beauvais and Bächtiger (2016: 9) argue, ‘not every civic forum needs to achieve every deliberative goal simultaneously’. Which deliberative goals may be given preference depends on the type of outcome envisaged, who is running the deliberation and how ‘maximally deliberative’ the forum needs to be. In this case, I argue public hearings can have a deliberative democratic function by giving non-elites a facilitated platform for powerful personal storytelling and questioning the process itself, which give rhetorical force to their group demands. The qualitative analysis picked out how the structure and framing of the hearing empowered patients and public representatives, despite the DQI seemingly showing they scored ‘lower’ on deliberative quality than the industry and professional participants. Future assessment using DQI might consider measures that incorporate temporal sequencing of deliberative scores to highlight where participants raise powerful points to prompt other participants to meet deliberative standards they may not otherwise have done.
Second, this article suggests that elite efforts at democratising regulatory governance processes in their everyday jobs need not be mere tools of ‘technocratic’ legitimation. Much recent literature has been critical of efforts at stakeholder engagement in IRAs as strategies of ‘legitimation’ (Braun and Busuioc, 2020). In this case, however, one can hardly see how the EMA received any public legitimation for the hearing at all. As of 14 September 2020, the YouTube video of the hearing has only been watched 2330 times worldwide in just short of three years since it was first uploaded on 29 September 2017. While EMA went on to hold another hearing in 2018 on a similar medicine safety review, public coverage of the debate has been, as with many EU institutional processes, minimal. It could be argued to this extent, then, that the hearing was relatively removed from any ambitions EMA had to publicly legitimate its regulatory processes, and instead view it as an exercise in promoting a slow-moving, everyday process of democratisation. One may go further to argue, contentiously perhaps, that EMA’s public hearing was even a ‘critical’ exercise in deliberative democracy, because it ‘promote[d] emancipation against domination’ (Hammond, 2019) to the extent that the outcome of the hearing was:
to introduce new burdensome requirements upon those with power (the pharmaceutical company Sanofi) to invest resources in informing Valproate users about risk;
providing those without power (pregnant women with epilepsy or bipolar disorder without knowledge of the adverse side-effects of the drug they are reliant upon) with important relevant information about its use; and
to introduce mandatory requirements upon mediating authorities (national governments) to bar any exercise of non-legitimate domination through the continued prescription of Valproate to pregnant women who were being harmed by taking it without their knowledge or active consent.
Again, it is difficult to think of the counter-factual here – whether the PRAC would have recommended something different, and more suited to the demands of Sanofi, had patients not had the opportunity to testify. Nevertheless, the EMA case should offer pause for thought for those insistent that elite bodies cannot do ‘meaningful’ deliberation.
Footnotes
Appendix 1
Appendix 2
Appendix 3
Acknowledgements
The author would like to thanks the reviewers for their insightful comments, and to all participants in the European Consortium for Political Research Annual General Conference 2019 Panel “Elite Governance and Democratic Innovation”.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Funding is gratefully acknowledged from two Economic and Social Research Council grants ES/L010925/1 and ES/S00730X/1.