
Abstract
Interest in politics is a key indicator of citizens’ attitudes towards politics. Scholars disagree whether interest is a stable trait developed during adolescence, or if it changes over the life course. We hypothesise that deteriorating health can destabilise the stable sense of political interest because worsening health makes individuals more dependent on public healthcare and increase their attention to politics. Furthermore, we assume that the impact of health on interest is conditional on income as people with low incomes are dependent on public healthcare. Our results show only limited support for the first hypothesis. However, we found a negative relationship between declining health and increasing interest in the lowest income group. The results are consistent with the life-cycle theory, which presumes that important events in life have consequences even for the most endurable political attitudes. Deteriorating personal health can be a source of motivation to make persons more interested in politics.
Introduction
Political interest is perhaps the most fundamental factor in determining citizens’ attitudes towards politics, and it is widely regarded as the key characteristic of a democratic citizen (Prior, 2010; Strömbäck and Shehata, 2010). According to Van Deth and Elff (2004: 478), interest in political affairs makes it possible for citizens to defend their preferences in the democratic process, and it therefore marks the most important difference between citizenship under democratic or authoritarian rule. Still, as Prior (2010) notes, many political scientists admit that they do not fully understand the true nature of political interest as an analytical construct. This is perhaps most clearly evident in the conflicting evidence concerning the stability of political interest over the human life course. Early studies by Jennings and Niemi (1974) and Jennings and Markus (1984) concluded that political interest varies over time, while more recent findings have disputed these results (e.g. Prior, 2008, 2010; Shani, 2009). This disagreement is part of a much wider scholarly debate regarding the larger question whether political orientations are stable over an individual’s life course or if they change over time.
Scholars have sought answers to this dilemma by examining two competing hypotheses. According to the lifelong openness hypothesis, people update their political attitudes over their life course, especially if personal experiences provide a reason for change. The lifelong persistence hypothesis instead proposes that attitudes, which have been formed early on in life, typically during adolescence or early adulthood, tend to remain stable throughout life (see, for example, Lyons, 2016; Russo and Stattin, 2016; Sears, 1983). There is also a sort of middle-ground position suggesting that interest is susceptible to change during the formative years of adolescence and early adulthood, after which it stabilises (Neundorf et al., 2013). Political socialisation provides an important theoretical framework for all of these explanations. Klemmensen et al. (2012) have, however, recently shown that accounting for genetic influence considerably reduced the impact of the growth environment, thus casting some doubt over the ability of the socialisation paradigm to explain political interest. Klemmensen et al. also speculate that political interest might instead be more a part of an individual’s psychological profile, rather than determined by the socialisation experience quite as strongly as much of the previous scholarship has suggested.
In this study, also we investigate the possibility that political interest may not be as irrevocably determined through the process of political socialisation during adolescence and early adulthood. We examine the possibility that (in)stability could depend on motivational factors; if there is a significant enough reason for the individual to change their existing level of interest in politics, they might do so. Furthermore, we highlight the importance of context; motivational factors may be more significant for certain groups of people. For example, in this study, we ask if motivational factors are more strongly related to interest in politics among people who are more likely to depend on services provided by the public health care sector. For political behaviour scholarship, these issues are quite significant. If fundamental political attitudes, such as political interest, really are stable over a person’s life course, all effort should be directed towards understanding how they develop in the first place. But if they can and do change over time, we should instead look for contexts and situations where fluctuations occur also later in life.
We look at changes in personal health by considering them as a life-cycle event that changes the stakes people have in politics, thus also changing the way people will express interest in politics. We use the British Household Panel Survey (BHPS) data to test the assumption that declining health leads people to become more interested in politics. Our first hypothesis assumes that when people become more dependent on the public sector for healthcare services due to declining health, they also become more motivated to start paying more attention to politics. Our second hypothesis is an elaboration of the first one. It proposes that it is especially the less economically fortunate people whose levels of political interest are affected by their health condition, as they are in a more vulnerable position and hence more dependent on public services and transfers when their health deteriorates.
Our empirical analysis suggests that the relationship between declining health and increasing interest is strongest among low-income people and weaker or non-existent among people with mid-range or high income. This is the first research to show this contingent effect of health on political interest which is interesting in the context of the United Kingdom where private health care arrangements often complement the relatively strong services offered by the National Health System (NHS). We interpret the findings to be consistent with the assumption that personal hardship may in fact increase interest in politics and therefore even have a mobilising impact on political behaviour.
Political interest and self-interest
The individual-level manifestations of political interest are familiar to all political scientists. Politically interested citizens are usually well-informed (Delli Carpini and Keeter, 1996) and participate eagerly in politics (Verba et al., 1997). They are also keen to continuously learn from the news media to keep up-to-date with daily politics (Strömbäck and Shehata, 2010). In line with these observations, political scientists have typically associated political interest with active citizenship. Subsequently, political interest has been defined as the degree to which politics arouses a citizen’s curiosity (Van Deth, 1990: 275–278), the extent to which politics is attractive to someone (Dostie-Goulet, 2009: 406) or as a citizen’s willingness to pay attention to political phenomena at the possible expense of other topics (Lupia and Philbot, 2005: 1122).
According to these definitions, interest is intrinsic and people turn to politics because of pure pleasure, enjoyment and curiosity – simply because they find politics interesting in itself. While this is undoubtedly the case for many people, considering political interest to indicate curiosity about politics approaches a tautology.
Turning to psychology might offer a way forward to a better understanding of what political interest is all about. In psychological terms, political interest signifies motivation, which not only describes interest as, for example, curiosity, but also seeks to understand how it comes about (see also Colombo, 2018; Van Deth, 1990). In psychology, interest has been widely viewed as an emotion that is intimately tied to motivation (see also Robison, 2017; Silvia, 2008). The most enduring principle in psychological theories of motivation is that interest – in anything – involves a calculus, whereby a person seeks to maximise gains and minimise losses (Birch and Veroff, 1968: 3).
Political scientists recognise the same idea as the essence of self-interest theory. According to Sears and Funk (1990: 248), a basic psychological assumption in self-interest theory is the simple pain–pleasure principle of human motivation, that is, that the instinctive motivation in human action is the maximisation of personal gain. In this study, we apply this idea to examining changes over time in political interest. We expect political interest levels to respond to changes in a person’s motivation level, which, in turn, we expect to change as a function of self-interest. Therefore, if a person thinks he or she has more to gain from paying more attention to politics, his or her self-reported political interest should increase as a result.
Hence, we offer a slightly alternative view of political interest as simply being a matter of just finding politics curious or enjoyable. We feel that explaining interest as arising from (an inexplicable) feeling of curiosity is certainly useful, but insufficient to clarify how political interest as an analytical construct should be understood. Our suggestion is that at least under some circumstances, an expression of political interest could be tied to self-interest considerations, which, especially in psychological literature, are commonly referred to simply as motivation.
Theoretical expectations
Although the self-interest approach has been widely used, according to conventional wisdom, self-interest considerations only rarely guide the political actions of ordinary people (Lewis-Beck et al., 2008: 197). It therefore seems that a sense of personal motivation is not a particularly strong predictor of political behaviour. However, Weeden and Kurzban (2017) have recently challenged this view by arguing that there is in fact a considerable number of studies that have found evidence strongly suggesting support for self-interest theory. While self-interest may in most analyses yield non-significant results, it nevertheless seems to predict behaviour in policy issues with substantial, imminent and obvious effects for the well-being of the individual (e.g. Kinder, 1998: 802; see Weeden and Kurzban, 2017: 72 for a review). Healthcare, and social policy more broadly, are areas where self-interest seems to play a particularly salient role (Hacker et al., 2013; Margalit, 2013; Mattila and Rapeli, 2018; Owens and Pedulla, 2014). People who are concerned about medical costs also support more universal healthcare coverage (Henderson and Hillygus, 2011). As Soss (1999: 363) explains, welfare recipients have an unusually visible material stake in government policies. Their immediate fates depend on the actions of public officials, and this fact is routinely underscored by speeches delivered in electoral campaigns and legislative debates.
Moreover, for voting propensity, the impact of health is essentially on par with partisan strength, religious attendance and newspaper readership (Pacheco and Fletcher, 2015: 109), and its magnitude is about 10 percentage points in comparison between people in poor versus excellent health when age and education are controlled for (Mattila et al., 2013). Also, Burden et al. (2017) noted that health has a powerful effect on voting in the United States. The size of the health effect in their analysis was on par with traditional predictors of participation such as education.
Therefore, plenty of evidence suggests that self-interest could be important in shaping political behaviour when personal health is at stake. This underscores the increasing appreciation among scholars that health affects all aspects of the human experience, including political attitudes (Papageorgiou et al., 2019) and political behaviour (e.g. Mattila, 2019; Pacheco and Fletcher, 2015; Stockemer and Rapp, 2019). As such, a change in personal health potentially constitutes an important life event, which may have consequences for political interest, especially in the case of long-term health problems or other serious health conditions. According to life-cycle theory, individuals’ political behaviour responds to various life events, particularly to the transition from adolescence or early adulthood to adulthood. Getting an education, settling down and building a career and a family increase the stakes a person has in politics and society, thus also affecting their political behaviour (see, for example, Neundorf et al., 2013: 96ff.). Life-cycle events, such as entering the workforce, unemployment or family-related matters, do not, however, seem to affect interest levels after the impressionable years in (late) adolescence (Neundorf et al., 2013), suggesting considerable stability in interest after reaching adulthood.
By looking at changes in personal health, we test the theory in a new setting. Health, as we argue based on the reviewed literature, seems to have potential for a more concrete impact in people’s political behaviour than life-cycle events such as (un)employment and human relationships. Being such a fundamental aspect of human existence, health could create strong enough incentives for people to reconsider their relationship with politics. Personal health seems particularly likely to bring about changes even in attitudes that are typically resistant to change, as suggested by findings from studies on healthcare policy attitudes and health effects on voting. Deteriorating health could make a person suddenly more dependent on public healthcare services, thus increasing their need to know what is going on in politics, in order to affect the relevant policy decisions. 1 We therefore assume that health has a mobilising impact, because dependency on the surrounding society will lead to people perceiving politics as more salient to their daily lives as they are more likely to feel the concrete effects of policies. Rephrased as a hypothesis, we assume that the deterioration of personal health is associated with increased political interest (H1). We assume this relationship to hold even after controlling for several background variables, most notably age and education. Age and education are of particular importance, because the two are strongly linked with both health and interest. Due to natural reasons, health tends to deteriorate as a function of ageing, and education typically has a strong positive relationship with political interest.
Previous research also suggests an elaboration of H1. While health problems can plausibly be expected to increase a person’s motivation to start paying more attention to politics, the effect is likely to be strongest among people who are more dependent on public services or income transfers. Those with good income have more options and are economically more independent of public health services. Thus, among these people, the effect of health problems is likely to have a weaker impact on interest, at least through the motivational mechanism that we are examining. Thus, we assume that the deterioration of health is more strongly associated with increased political interest among low-income than mid-range and high-income citizens (H2). The second hypothesis therefore addresses a more rigorous test of the core idea that expressions of political interest could be understood through the maximisation of personal (economic) gain, as proposed by the self-interest paradigm.
Data
Our data come from the BHPS, which observed the same individuals over 18 waves during the period stretching from 3 September 1991 to 9 April 2009. The original BHPS respondents have been included in the more recent UK Household Longitudinal Study (UKHLS). However, and unfortunately for our case, the formulation of the self-reported health question is different in the currently running UKHLS, which means that we are unable to use these observations in our analysis.
The first BHPS wave included around 5500 households containing 10,300 individuals living in Great Britain. In the data we are using, interest in politics is captured by the standard item How interested would you say you are in politics? The possible answers are ordered as Not at all interested, Not very interested, Fairly interested and Very interested. Regrettably, there is no issue-specific question about interest in health-care policy is available in the BHPS data. However, general political interest is commonly understood to reflect an overall estimation of how much a person pays attention to politics, including different, specific policy areas.
Figure 1 shows the average levels of interest in politics stratified by wave in the BHPS data. There are no data available from Waves 7 to 10, because the question on political interest was not asked. The average scores seem rather stable, revolving around 2.28 (standard deviation: 0.91) with a high (2.49) in 1992 (second wave) and a low (2.19) in 2005 (16th wave). However, the average values do not tell us anything about how stable interest levels have been for the individual respondents over time.
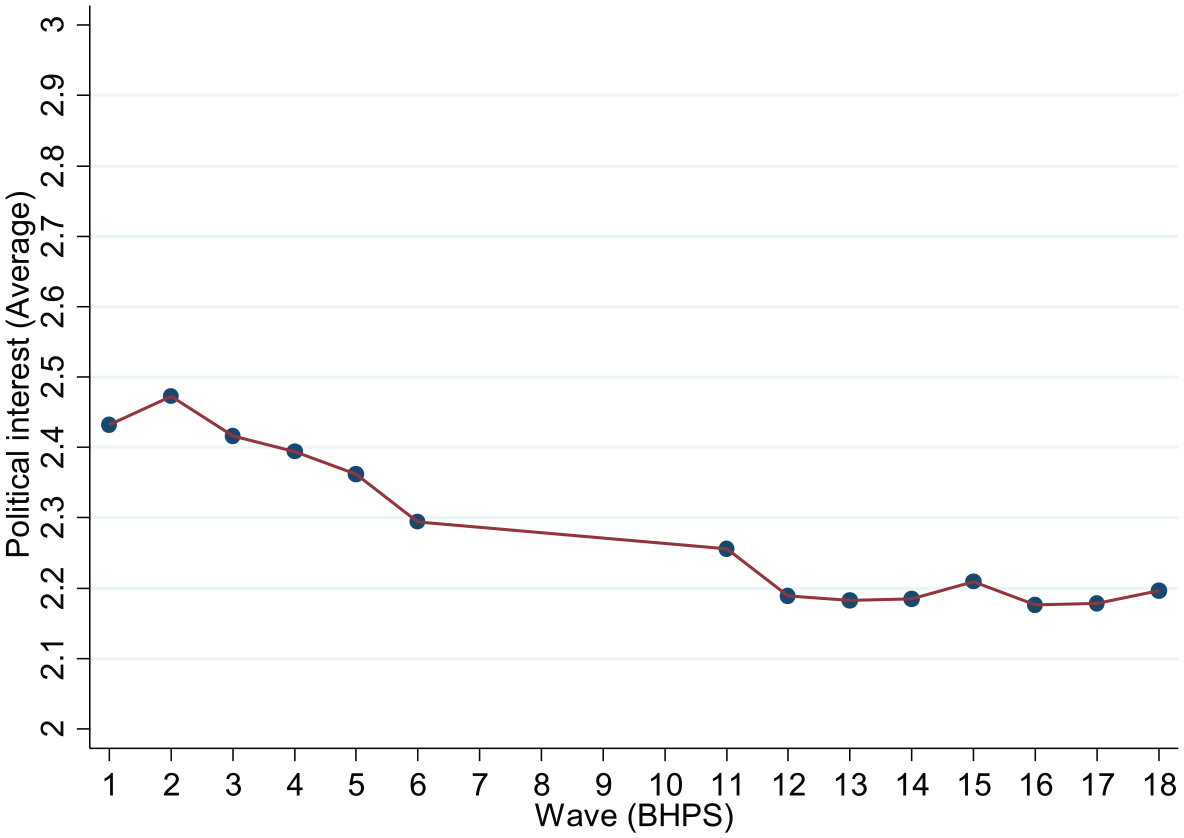
Interest in politics by wave (BHPS).
The effect of changes in health on political interest
In sociological medicine, self-rated health has been measured by a single item in surveys since the 1950s. Two different wordings have been used: the simple assessment of one’s personal health status or, as in the BHPS, an evaluation of personal health as a comparison with same-aged peers (Jylhä, 2009: 307): Please think back over the last 12 months about how your health has been. Compared to people of your own age, would you say that your health has on the whole been: Very poor, Poor, Fair, Good and Excellent. Such evaluations of self-rated health are considered to reliably condense a number of various health aspects and health-promoting behaviour into a personal assessment of one’s own health (e.g. Fylkesnes and Forde, 1992).
Since political interest is not a one-off act (such as, for example, turning out to vote) and is measured several times over the BHPS study period, in our models, we capture the effect of the lagged value of health on current political interest. By lagging health by one wave (year), the analysis allows for some time during which health can shape political interest, as we are mostly interested in chronic health conditions, which may have a gradual impact on interest. This may help to bypass part of the ‘noise’ or random fluctuations in political interest, capturing a more realistic variation of political interest along the time. Another good reason to employ the lagged value of health is presented by Pacheco and Fletcher (2015). According to the authors, self-rated health status may not be independent of the outcomes we wish to use them to explain (Pacheco and Fletcher, 2015: 106). For example, individuals may justify their lack of interest in politics by referring to a ‘legitimate’ reason such as health problems. Using the lagged value of health helps us to alleviate the potential endogeneity problem, which could lead to overestimated coefficient estimates. The reason that we do not use both current and lagged levels of health in the analysis is that using both of them would cancel out the main impetus behind using lagged levels of health in the first place. Using even longer lags could also mitigate the potential endogeneity problem mentioned above but the trade-off is that we would use self-rated health of more than 2 years ago to predict current levels of political interest.
Voters’ age is important as it affects both health and political interest. Taking into account that the relationship between political interest and age is not linear 2 (p < .000; F(3, 84685) = 13.64) and that a cubic spline function usually behaves poorly in the tails (Harrell, 2001), we assume a natural spline also known as restricted cubic spline (RCS). RCS is a function that is ‘a straight line before the first and after the last knot and continuous and smooth at the knot boundaries’ (Dupont, 2009: 135). We follow Harrell (2001) who recommends placing five 3 knots at equally spaced percentiles. The first knot is placed at the 5th (age = 20), the second one at the 27.5th (age = 33), the third one at the 50th (age = 44), the fourth one at the 72.5th (age = 58) and the fifth one at the 95th percentile (age = 78).
Below we discuss in detail two models that we use to analyse the relationship between health and interest. We start our analyses with a fixed effects model which we call static as it does not include the lagged value of the dependent variable as a regressor. The major advance of the fixed effects model is that it removes the potential effect of unobserved time-invariant variables from the analysis. Thus, it alleviates the problem of omitted variable bias. However, time series of attitudes, such as interest, often are affected by measurement error (Prior, 2010). This is why we also use a dynamic model where we let the previous values of interest to affect the current ones.
Static model
Our first model is a static linear fixed effects regression with a first-order autoregressive (AR1) disturbance term

The disturbance term is a first-order autoregressive
To deal with the endogeneity resulting from the correlation between the omitted (time-invariant) variables and the explanatory ones (Baltagi, 2008), we specify a fixed effect model (FE). The FE does not impose the strict assumption of the random effects model (RE) which is that the unit effect is a random variable unrelated to all other exogenous regressors (Gelman and Hill, 2007). Assuming, for example, an initial model of the form
Dynamic model
Drawing on the work by Prior (2010), we also consider a dynamic panel analysis. Our second model is dynamic, because it includes the dependent variable lagged by one and two 5 time units
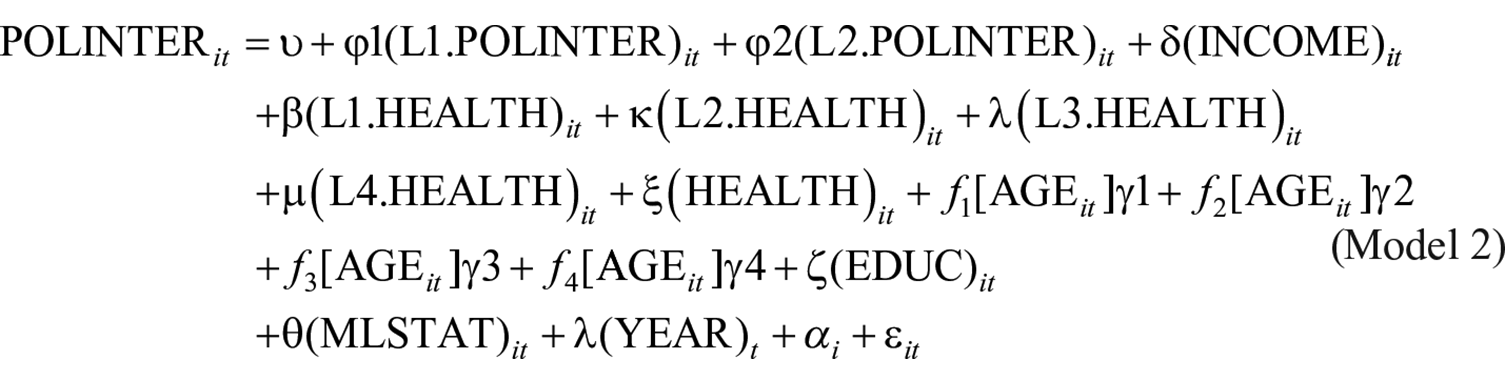
Model 2 assesses the impact of our main independent variable
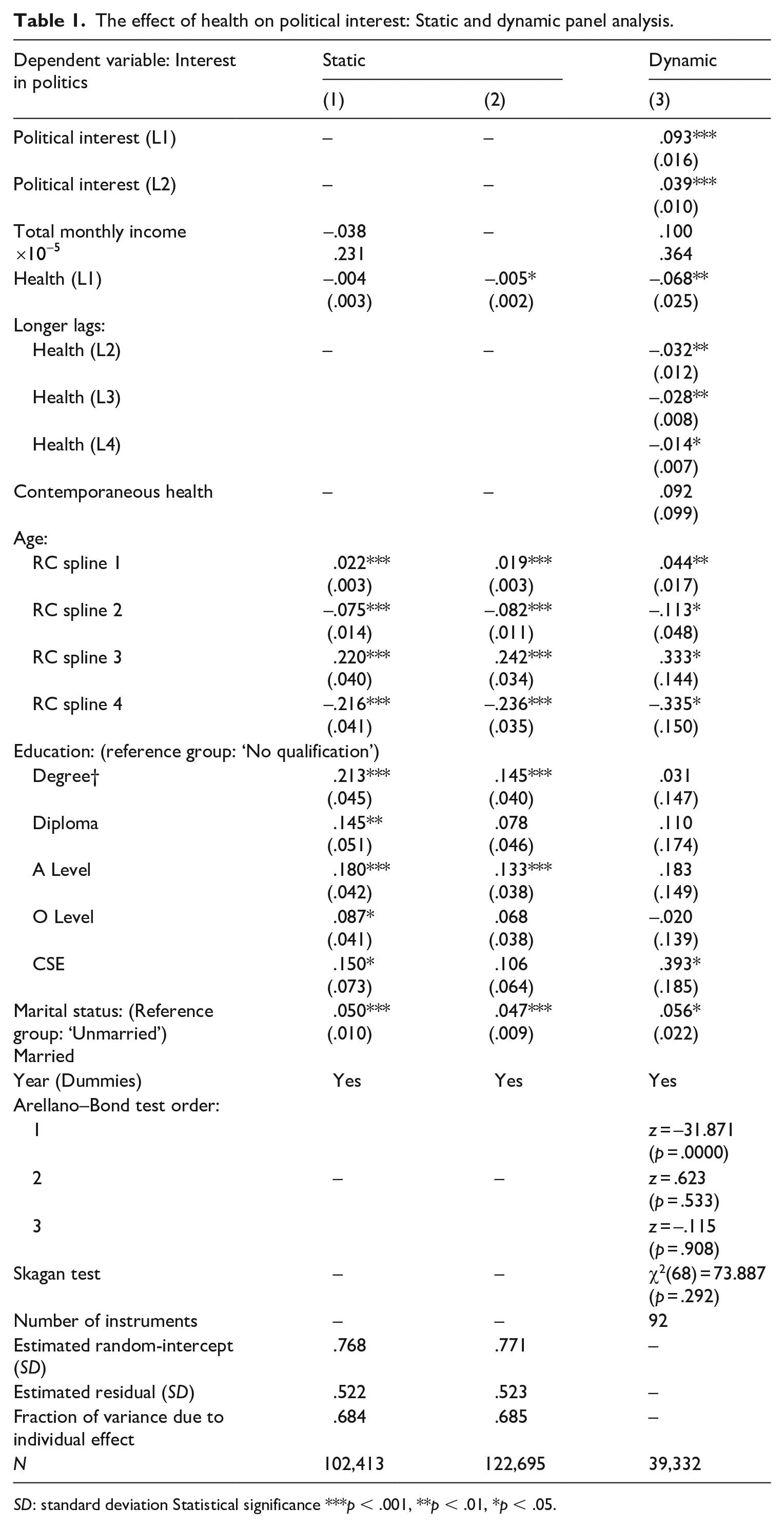
Column (1) of Table 1 presents results from the static fixed effects model. Although the FE specification cannot estimate the coefficients for time-invariant characteristics, such as gender, nevertheless the effects of such characteristics are controlled for by the fixed effects specification. Column (3) of Table 2 presents results from the dynamic model as estimated by the Arellano–Bond estimator.
The effect of health on political interest: Static and dynamic panel analysis.
SD: standard deviation Statistical significance ***p < .001, **p < .01, *p < .05.
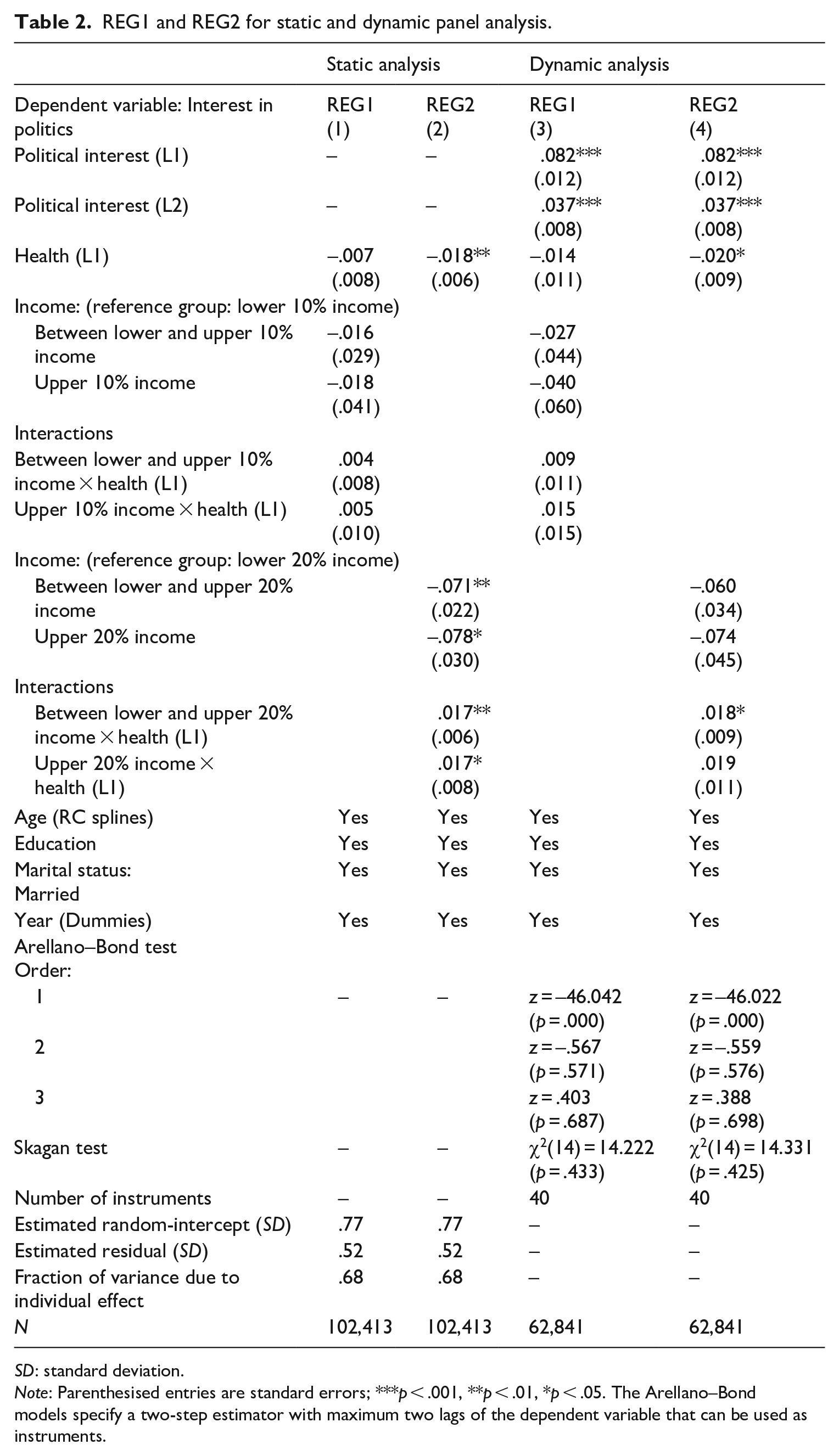
REG1 and REG2 for static and dynamic panel analysis.
SD: standard deviation.
Note: Parenthesised entries are standard errors; ***p < .001, **p < .01, *p < .05. The Arellano–Bond models specify a two-step estimator with maximum two lags of the dependent variable that can be used as instruments.
One important note should be in place regarding the FE estimator before moving to discuss the calculated estimates. In applications where the within variation is smaller in comparison to the between variation, 6 the standard errors of the fixed effects coefficients may be too large to tolerate (Allison, 2009: 8). However, the standard errors reported in Table 1 show that this is not a problem. As Cameron and Trivedi (2010: 227) note, a linear regression with AR1 errors is a better model than the i.i.d error model [. . .] and potentially will lead to more efficient parameter estimates.
In the fixed effects model, the control variables behave as expected. The results show that educated individuals are more interested in politics than individuals with no qualifications. Also married respondents are more interested in politics than unmarried ones. On the other hand, total monthly income does not appear to have a statistically significant effect. Regarding age, the estimate of RC spline 1 is positive; the estimate of RC spline 2 is negative; the estimate of RC spline 3 is positive; and the estimate of RC spline 4 is negative. Since RCSs cannot be interpreted in the same way as linear ones, Figure 2(a) pictures the relationship between age and political interest keeping all other independent variables stable at their mean. Figure 2(a) depicts a curvilinear relationship where political interest increases until the age of 70 and stabilises thereinafter. Figure 2(b) shows the marginal effect of the RCS. ‘In other words, it shows for each value of the spline variable how much the expected value of the explained variable changes for a unit change in the spline variable’ (Buis, 2009). The rate at which political interest changes with respect to the change of age is the highest for individuals between 20 and 40 years old. For individuals above 75, the change of political interest with respect to the change of age remains quite stable.
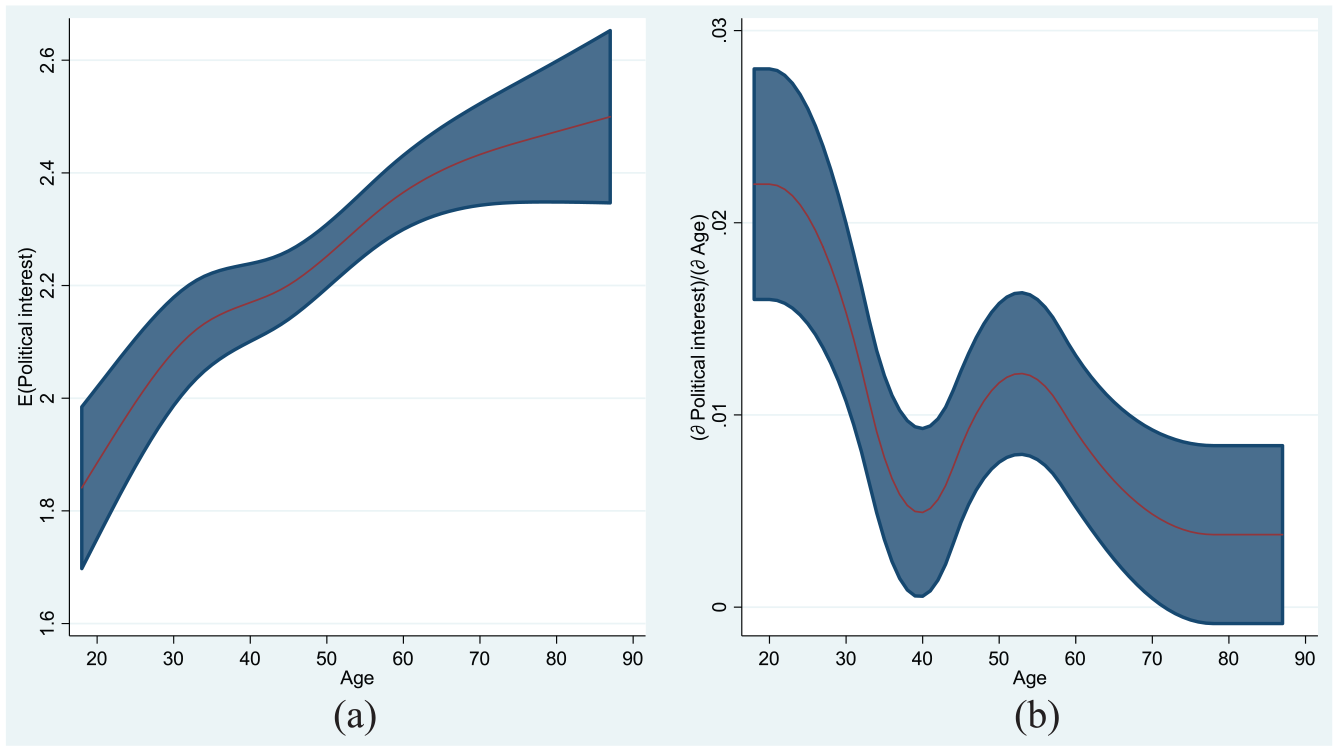
The relationship between political interest and age (a) and change of political interest with respect to change of age (b).
Finally, turning attention to our main independent variable, the coefficient estimate for Health (L1) in the linear FE model is negative but not statistically significant. When income is removed from the set of controls, the negative estimate of Health (L1) becomes statistically significant with p < .05 (Static (2)). In other words, results indicate that as health improves (deteriorates), political interest decreases (increases), yet it should be noted that the effect is rather miniscule. 7
The results from the dynamic Arellano–Bond models are shown in Table 1 in columns 4. As Arellano and Bond (1991: 278) argue, an estimator that uses lags as instruments under the assumption of white noise errors would lose its consistency if in fact the errors were serially correlated. It is therefore essential to satisfy oneself that this is not the case by reporting test statistics of the validity of the instrumental variables (that is, tests of lack of serial correlation) together with the parameter estimates.
So, we first check whether our dynamic model is correctly specified. We test for autocorrelation employing the Arellano–Bond test for zero autocorrelation in first-differenced errors. Results show that our dynamic model has been specified correctly. As expected, the z-statistic of the Arellano–Bond test is negative and significant for autocorrelation of order 1. Yet what matters is that we do not reject autocorrelation of order 2 (p = .533), not even of order 3 (p = .908), indicating thus that the Arellano–Bond model assumptions are satisfied. We also check whether the overidentifying restrictions of the model are valid. The Sargan test does not reject the null hypothesis that the overidentifying restrictions are valid with
Under the dynamic model (column 3), the first and second lag of the dependent variable are, as expected, both highly significant and positive indicating that last years and the last 2 years’ political interest affect current political interest ‘after accounting for a person’s long term interest [. . .] and the effect of contemporary disturbances’ (Prior, 2010: 758). Age and marital status appear to be more or less unaffected by the inclusion of lagged dependent variables; the estimates of education, retain mostly their positive signs yet they lose their explanatory power owing to the inclusion of lagged dependent variables. Also, income does not affect the outcome nor does contemporaneous health condition. In contrast, the estimate of our main independent variable, the first lag of health, is negative and statistically significant 8 with p < .01. Similarly, coefficient estimates of longer lags of health are also all negative and statistically significant. Our confidence in the robustness of the aforementioned findings is further enhanced by Prior’s (2019) recent book, which upon including two different types of health (physical and mental) in a dynamic model, also reports a negative effect of health on political interest.
Next, we turn to our second hypothesis, according to which we expect that the effect that health deterioration leads to an increase in political interest should be more evident among people with lower income. To test the hypothesis, we compute the percentiles of the income variable for each wave separately because income does not remain stable but changes with time (e.g. monthly income below the 10th percentile was £367 in 1991, while it was £542 in 2009 etc.) The reason for working with percentiles is that we are not able to specify a priori where the lines between low, middle and high income are drawn. The mean and median give the central income trends for each quantile in the period 1991–2009. For example, the average (middling) monthly income below the 10th percentile in the period 1991–2009, was £442 (£431); the average (middling) monthly income below the 90th percentile in the period 1991–2009 was £2423 (£2325) and so on. (see Supplementary Analyses, Appendix B). In the following analysis, we use interactions to assess the effect of health on political interest for individuals belonging to different income percentiles.
First, we add an interaction term in the static model. The reason to include interactions in the static model, although health appears not to significantly affect political interest when total monthly income is controlled for, is because the effect of health might nevertheless be significant for low-income groups as we hypothesised. The interaction is between the mean income percentile and health condition (lagged) but identical results are obtained when one considers median values as the latter are very similar to the mean ones (see Supplementary Analyses, Appendix B).
Two different linear regressions are then specified: In the first regression (REG1), the analysis considers as low-income group, individuals belonging below the 10th percentile; as high income group, individuals with income above the 90th percentile; and as middle income group, individuals with income between the 10th and the 90th percentile. The second regression (REG2) considers as individuals with low income those who fall below the 20th percentile and as individuals with high income those who are above the 80th percentile. Although the amounts corresponding to high monthly income in REG1 and REG2, 2423£ and 1836£, respectively, might not seem particularly large amounts in today’s standards, the one should bear in mind that our data go as back as 1991. Figure 3 shows the average political interest for income groups of REG1, whereas Figure 4 the average political interest for income groups of REG2.
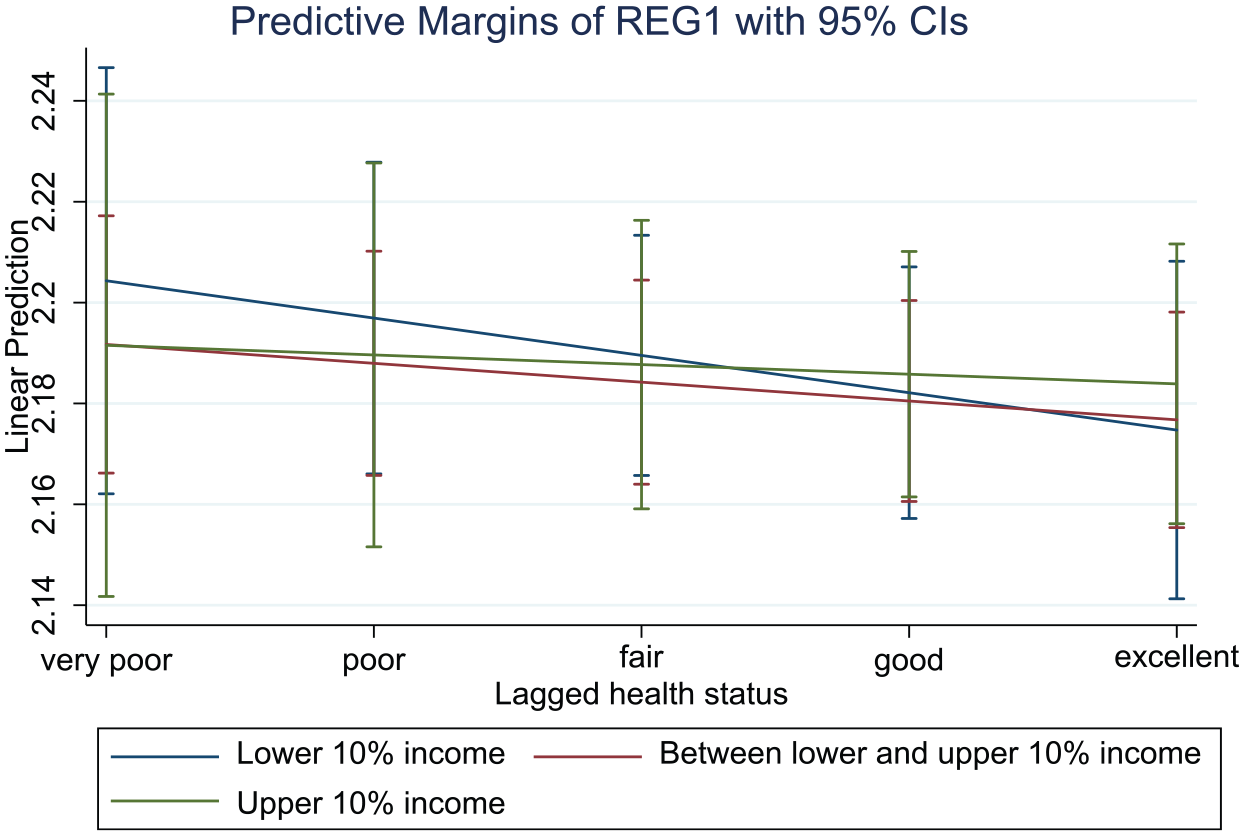
Margins with 95% CIs (REG1).
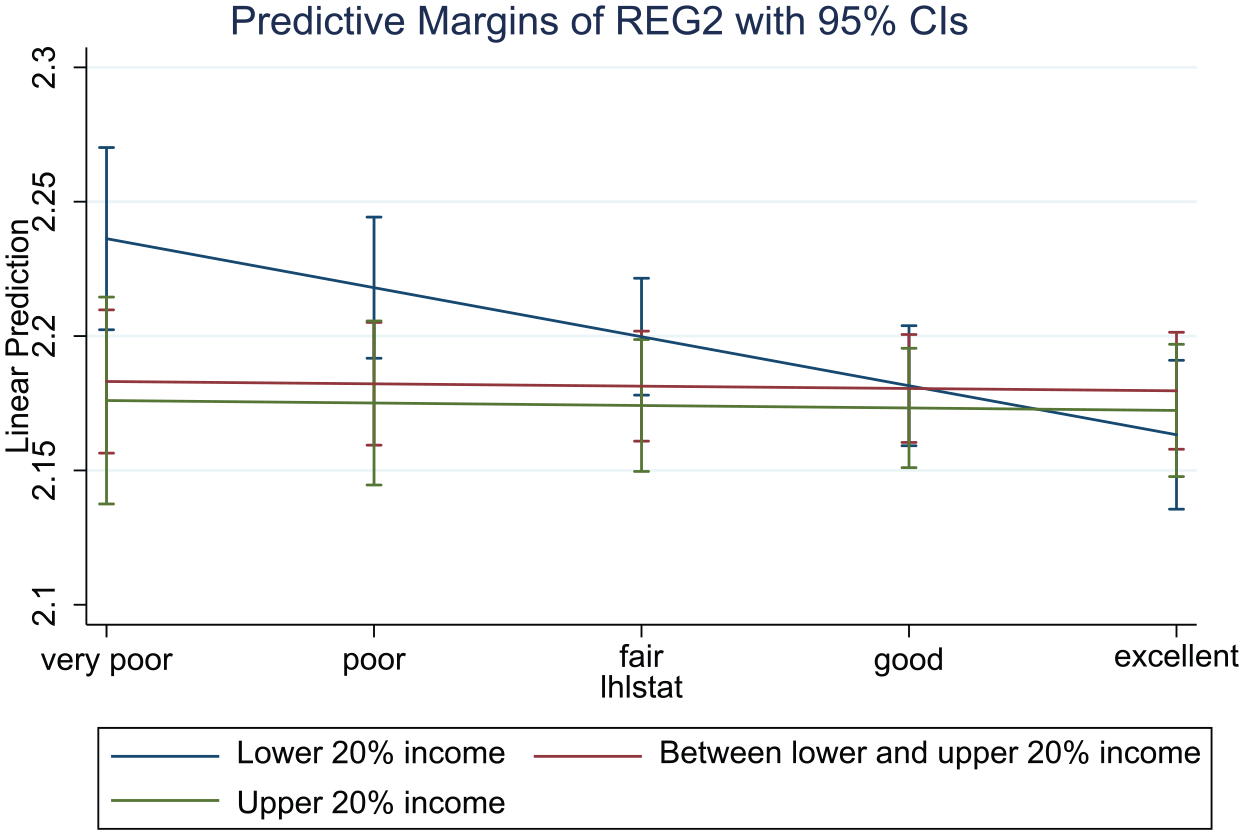
Margins with 95% CIs (REG2).
The slopes shown in Figures 3 and 4 are based on estimates from REG1 and REG2, respectively (Table 2). The interaction estimates in column (1) show whether the slope of the lower income group in REG1 (bottom 10%) is statistically different than the slopes for the middle and upper income groups. The results show that interactions are not statistically significant which was to be expected only by gazing the slopes in Figure 1. However, the interaction estimates in column (2) are both positive and statistically significant. In other words, the static analysis supports our hypothesis that the effect of changes in health on changes in political interest has more sizable effects for lower incomes (bottom 20%) compared to middle and upper incomes.
Column (3) and (4) of Table 2 repeat the interaction analyses, assuming this time dynamic models. 9 Under REG1 in column (3), the dynamic analysis reports similar findings as the fixed effects analysis, namely that the effect of health on political interest does not differ among different income groups. Yet, results from a dynamic analysis of REG2 in column (4) show that the interaction for the middle-income group is statistically significant, meaning that the effect of changes in health is more pronounced for respondents with low income (bottom 20%) than in the middle-income group. This implies that the non-significant estimate of health reported in the case of the dynamic model in Table 1, actually reflected the effect related to middle and top incomes (top 20%) suppressing thus the effect related to low incomes (bottom 20%). Also, the fact that there was no real difference in the effect of decline in health on political interest between the low and top incomes might be related to a ceiling effect: well-off people are already quite interested in politics and changes in their health conditions are less likely to increase their interest than among those with low starting levels of interest. However, this effect is probably limited as the average value for interest on the one to four scale is only 2.27 among the top 10% earners, leaving room for potential improvements.
Conclusion
Interest in politics is a key precursor of a citizen’s attitudes towards democratic politics. Yet, political science has not been able to fully reveal its nature, as scholars have offered opposing views and evidence concerning its stability during an individual’s life course. This is an important question for the study of political behaviour, because it determines whether or not we can examine political interest, and other fundamental attitudes, simply by looking at how they develop.
Since political interest is most often employed as an independent variable in analyses of political behaviour, scholarship has not adequately addressed it as a theoretically important and interesting dependent variable. However, a better understanding of what lies behind citizens’ self-expressed political interest levels is essential. In this study, we have suggested that the concept of political interest implies motivation, which typically manifests itself through political engagement. Based on psychological theories, we have put forth the idea that perhaps the motivational nature of political interest should be seen as signifying self-interest. Since human actions are driven by the motivation to maximise personal gain, also political interest could be understood essentially as a function of self-interest in political matters.
We have tested this idea by examining whether changes in motivation levels could cause instability in political interest. We argued that deteriorating health could plausibly constitute a strong enough question of self-interest to even destabilise the typically very stable subjective sense of interest in politics. We considered changes in personal health as a life event, as claimed by life-cycle theory, and hypothesised a negative relationship between health and interest: we assumed that the deterioration of personal health is associated with increased political interest, because worsening health makes a person more dependent on public healthcare and therefore increases their incentives to pay attention to politics.
We used both static and dynamic panel models to analyse the relationship between health and political interest. The results gave only partial support for our first hypothesis: results from our dynamic model show that a decline in health is associated with an increase in the interest in politics. However, results from the static panel model offer weaker support to the hypothesis, if at all. Furthermore, the effect size is rather small, showing that a decline in health leads only to a small increase in interest. These results, however, may be related to the differentiated effect of health in different income groups, a possibility examined by our second hypothesis.
Our second hypothesis elaborated the health-interest relationship. We assumed that the effect of changes in health on interest would be conditional on the income level of the respondents. This is because people with low income are often dependent on public healthcare, whereas people with high income are not. Therefore, we expected to see a stronger effect of growing political interest among low-income individuals as a result of declining health. The evidence showed some support for the second hypothesis, as we only found the expected negative relationship between health and interest in the lower income group, but not in other income groups.
On the whole, our analysis gives some support to the general idea that attitudes could be open to change even after the formative years, as we have identified a context where political interest fluctuates at the individual level as a result of a significant change in life circumstances. This observation lends some, although not overwhelming, support for the life-cycle theory, which presumes that important events during the life course have consequences even for the most endurable political attitudes. The magnitude of changes in interest produced by health differences should not be overdramatised, but it seems that deteriorating personal health is demonstrably a strong enough source of motivation to make a person more interested in politics. In addition, the relationship is contingent on the level of income. We therefore conclude that it seems that even the most fundamental of political attitudes, including political interest, can change over time.
We have reached this conclusion by arguing for a self-interest-centred view of political interest. More evidence from different contexts is, however, needed before we can feel confident that the political interest is sensitive to self-interest considerations and that the life-cycle theory can reliably predict fluctuations in political interest. Our analysis nevertheless suggests that for life-cycle theory to be useful for analysing changes in relatively stable attitudes, life events should be more dramatic – and perhaps sudden – than events such as the gradual transition to adulthood through acquiring a job and a family, something that typically takes several years. Moreover, political contexts are likely to affect the impact of health on political interest. The United Kingdom, where our data come from, is a case where policy choices can plausibly be expected to have an impact on healthcare services. In countries with a more privatised healthcare sector, people may not be equally likely to become politically interested due to changes in health, if they do not expect the political system to be able to affect health policy. Consequently, in addition to testing the robustness of our findings in other life event contexts, they should also be tested in different national contexts.
Supplemental Material
BPI912378_appendix – Supplemental material for Interest through necessity? The impact of personal health on the stability of political interest in the United Kingdom
Supplemental material, BPI912378_appendix for Interest through necessity? The impact of personal health on the stability of political interest in the United Kingdom by Mikko Mattila, Achillefs Papageorgiou and Lauri Rapeli in The British Journal of Politics and International Relations
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the following projects / financiers: Academy of Finland, grant numbers 266844 and 312676. The Åbo Akademi University Foundation, grant for the FutuDem centre of excellence.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.