
Abstract
Although a vast literature demonstrates that discrimination correlates negatively with health satisfaction, research has yet to examine whether within-person changes in perceptions of discrimination temporally precede declines in subjective health. Studies also overlook the possibility that the relationship between perceived discrimination and health satisfaction differs for structurally advantaged and disadvantaged groups. We address these oversights by utilizing 11 annual waves of data from a nationwide random sample of adults to examine the relationship between perceived discrimination and subjective health among Māori (N = 9,298) and New Zealand Europeans (N = 56,499). Results from a multi-group RI-CLPM reveal that perceived discrimination has a negative cross-lagged effect on within-person changes in health satisfaction for Māori, but not for New Zealand Europeans. These results highlight the asymmetrical consequences of discrimination between structurally advantaged and disadvantaged groups, underscoring the pervasive challenges minoritized communities continue to face.
Introduction
In 1946, the World Health Organization declared that all individuals should be able to achieve a high standard of health irrespective of their race, religion, political beliefs, or their economic and social circumstances (Whitehead & Dahlgren, 2006; World Health Organization, 1946). Despite making this declaration nearly 80 years ago, a life expectancy gap continues to persist across structurally advantaged and disadvantaged ethnic groups both globally (Arias et al., 2021; Australian Bureau of Statistics, 2020–2022; Dwyer-Lindgren et al., 2022), and locally here in Aotearoa/New Zealand (i.e., the location of the current study; Te Whatu Ora, 2024b). These enduring disparities are rooted in historical and structural forces that shape the distribution of social determinants of health, including access to healthcare, education, employment, and exposure to discrimination (Signal et al., 2008). Although considerable research demonstrates the negative impact of discrimination on health (Pascoe & Smart Richman, 2009), there remains a need to examine how these effects vary over time, between groups of differing social status, and across diverse geographical contexts.
The current study addresses these oversights by utilizing a multi-group random-intercept cross-lagged panel model (RI-CLPM) to assess the within-person associations between perceived discrimination and subjective health ratings in a nationwide random sample of structurally advantaged and disadvantaged adults. In doing so, we make an important theoretical contribution to the literature by testing whether the downstream effects of discrimination differ across groups of unequal status—a possibility that has received only limited attention (Harris et al., 2006b). We begin by reviewing the literature on the negative effects of perceived discrimination on well-being, acknowledging differences in outcomes across groups of different status. We then summarize the aims of the current study, as well as the rationale underlying our hypotheses. Finally, we provide an overview of the unique sociocultural context of Aotearoa and highlight how it has contributed to unequal health outcomes across structurally advantaged (i.e., Pākehā/New Zealand Europeans) and disadvantaged (i.e., Māori) groups (Ministry of Social Development, 2016).
Perceived Discrimination
Although persistent differences in various health outcomes exist across structurally advantaged and disadvantaged groups (Chen & Yang, 2014; Du Mont & Forte, 2016; Schulz et al., 2006; Schunck et al., 2015), theoretical approaches to intergroup relations emphasize that these inequities emerge from relations between groups. Group-based discrimination plays a central role in producing and maintaining these status-based differences in subjective health (Major et al., 2013; Paradies et al., 2015). Indeed, discrimination is harmful not only because it directly impacts individuals, but also because it communicates the relative position or status of one’s ingroup within a broader social hierarchy (Major et al., 2013). Because social identities are central to our self-concept and impact our self-esteem (e.g., see Tajfel & Turner, 1986), the perception that one’s ingroup is devalued in comparison to other groups—particularly due to systemic or interpersonal discrimination—can threaten one’s individual or collective sense of self (Major et al., 2013). Over time, such chronic experiences can increase vigilance to signals of exclusion (Murphy & Taylor, 2012), lead one to internalize the group’s devalued status (Vargas et al., 2020; Williams & Mohammed, 2009), and undermine one’s sense of social belonging (Baumeister & Leary, 1995).
Although ingroup identification among the structurally disadvantaged can buffer against the negative effects of discrimination by restoring a sense of belonging (Branscombe et al., 1999) and fostering access to social support to cope with prejudice (Jetten et al., 2012), these protective mechanisms may fail to fully counteract the toll of persistent discrimination. The benefits of ingroup identification may be limited if the unfair treatment is pervasively reinforced by broader structural inequities. Indeed, for structurally disadvantaged groups, ingroup status co-exists with ongoing exposure to exclusionary systems that shape health outcomes in harmful ways (Brown et al., 2025; Selvarajah et al., 2022). Thus, although group identification can provide an important source of resilience (Jetten et al., 2012), it must also be understood within a context where structural inequities continue to undermine health and well-being (Selvarajah et al., 2022).
Consistent with this perspective, perceptions of discrimination correlate with various adverse outcomes, including early substance use, psychosis, and anger (Williams et al., 2003), poorer collective well-being (Branscombe et al., 1999), psychological distress (Oates & DeMaris, 2022), anxiety, depression, and general lower well-being (Schmitt et al., 2014). Crucially, a growing literature also finds that perceived discrimination correlates negatively with physical health (for a review, see Pascoe & Smart Richman, 2009).
To understand why discrimination impacts physical health, it is important to consider the physiological mechanisms underpinning this link. According to the stress and coping framework, discrimination is a social stressor that triggers physiological responses that undermine physical health (Pascoe & Smart Richman, 2009). Indeed, repeated experiences of racism increase physiological stress responses through heightened cardiovascular activity (Guyll et al., 2001) and promote cardiovascular disease by disrupting nocturnal blood pressure recovery (Brondolo et al., 2008). Frequent experiences of racial discrimination are also associated with shorter telomere length (an indicator of aging), which is linked with early mortality (Chae et al., 2014; Lee et al., 2017). Experiences of discrimination can also impact health by increasing sleep problems (Fuller-Rowell et al., 2017), reducing self-control (Inzlicht et al., 2006), undermining capital resources, promoting distrust in healthcare systems, and bolstering engagement in unhealthy coping behaviours, such as smoking (Chen & Yang, 2014). Taken together, these physiological pathways illustrate how discrimination erodes physical health.
Although objective health measures are often seen as the gold standard in research, self-rated health is also an important indicator of well-being. Self-rated health is a consistent, reliable predictor of mortality that captures changes in bodily sensations indicative of health status, and the subjective evaluations affected by the broader sociocultural context (Jylhä, 2009). Given people’s inherent familiarity with their bodily states, people may detect subtle changes to their health that may otherwise be missed in a clinical examination. Indeed, people often evaluate their health by considering their current functioning compared to past states or may use social comparisons to assess what is “normal” for someone of their age, gender, or ethnicity (Benyamini, 2011). Because self-rated health reflects not only physical states, but also subjective and contextual interpretations, it may be particularly responsive to social stressors such as perceptions of discrimination. Indeed, perceived discrimination consistently undermines self-rated health across a range of groups, including immigrants (Schunck et al., 2015), women (Schulz et al., 2000), those with lower social capital (Chen & Yang, 2014), and those with disabilities (Du Mont & Forte, 2016).
Ethnic Group Asymmetries
Although perceptions of discrimination are consistently associated with poorer well-being, there may be asymmetries in this relationship across structurally advantaged and disadvantaged ethnic groups. Structural discrimination plays a central role in driving health inequities, as it limits access to factors that impact health (Talamaivao et al., 2020), and promotes inequities in the utilization and quality of medical care (Fowler-Brown et al., 2006). For example, despite having higher rates of heart failure, rates of cardiac intervention are substantially lower for Māori (i.e., the Indigenous peoples of New Zealand) than non-Māori (Westbrooke et al., 2001). Thus, structurally disadvantaged groups may be particularly likely to encounter health deficits following experiences of discrimination.
The cumulative nature of systemic discrimination (see Schmitt & Branscombe, 2002) further contributes to these asymmetries. Ethnic minority groups encounter more frequent and severe forms of discrimination on average than their ethnic majority counterparts (Ministry of Health, 2023; Statistics New Zealand, 2012). Moreover, these experiences persist across various contexts, including housing (Houkamau & Sibley, 2015), the workplace (Haar, 2023), in public spaces (Yeung & Crothers, 2016), and healthcare (Carter et al., 2019). When discrimination occurs repeatedly over time and across diverse contexts, it becomes a chronic stressor through prolonged activation of physiological pathways (Williams & Mohammed, 2009), thereby producing higher costs for health (Van Dyke et al., 2020). Consistent with a dose-response relationship between discrimination and health (i.e., more experiences of discrimination lead to greater declines in physical health), fewer experiences of discrimination should result in a weaker effect on well-being (Harris et al., 2012). Indeed, the negative relationship between perceived discrimination and well-being is stronger for several structurally disadvantaged ethnic groups, including those who identify as Māori (Harris et al., 2006b), Asian (Nicholson, 2020), Latino, and Black (Borrell & Dallo, 2008).
In summary, theoretical approaches to intergroup relations suggest that discrimination and health inequities arise from structural inequities between advantaged and disadvantaged groups. Inequities emerge through intergroup hierarchies and prejudice (Major et al., 2013), shaped by historical injustices such as colonization (Reid et al., 2019). In turn, the enduring legacy of colonization and resultant social hierarchies impact one’s quality of interpersonal interactions, exposure to stress and discrimination, and access to healthcare and other crucial coping resources (Major et al., 2013). These approaches align with Māori scholarship, which emphasizes that inequities are not inherent to Māori, but rather, stem from the positioning of Māori and Pākehā within a colonial and capitalist system that unequally distributes power, resources, and opportunities (Curtis et al., 2023; Reid et al., 2019).
Gaps in Existing Research
Despite a large body of research linking perceived discrimination to health outcomes, several gaps in the literature remain. First, existing research assessing group differences in the relationship between discrimination and well-being has largely (a) focused exclusively on structurally disadvantaged groups (Kapeli et al., 2020; Neblett, 2023), (b) explored the effects of discrimination outside the context of ethnic group relations (e.g., Schulz et al., 2000), (c) concentrated on mental well-being (Schmitt et al., 2014), or (d) relied on cross-sectional data (Harris et al., 2006a; Houkamau et al., 2017). As such, few—if any—studies to date have compared the longitudinal relationships between perceived ethnic discrimination and health satisfaction across structurally advantaged and disadvantaged ethnic groups.
In addition to overlooking structural asymmetries in this relationship, the few studies using longitudinal methods that do exist have mostly utilized cross-lagged panel modelling (CLPM) and similar approaches to examine the temporal ordering of the relationship between perceived discrimination and health outcomes (Gee & Walsemann, 2009; Liu & Yang, 2022; Schunck et al., 2015). However, this analytical approach confounds stable between-person differences and within-person change (see Berry & Willoughby, 2017; Hamaker et al., 2015; Osborne & Little, 2024). To accurately assess whether fluctuations in a person’s perceptions of discrimination at one time point predict subsequent changes in their health satisfaction, it is necessary to use an approach that distinguishes between enduring, trait-like differences and within-person effects.
The Present Study
To address these gaps in the literature, we utilize 11 annual waves of longitudinal panel data to examine the relationship between perceptions of ethnic discrimination and satisfaction with health among an ethnic minority group and an ethnic majority group in Aotearoa New Zealand. Importantly, we employ a multi-group RI-CLPM to address the limitations of past research using traditional CLPMs (namely, the confounding of between- and within-person processes). By incorporating random intercepts into the CLPM framework, we can disentangle the impact of trait-like differences and within-person change on health satisfaction. Prior research notes that there are a limited number of longitudinal studies that examine the direction of the pathways associated with discrimination and health (Pascoe & Smart Richman, 2009). Consequently, to the best of our knowledge, this is the first study to assess whether within-person departures from a person’s trait-level mean of perceived discrimination at one time point predict within-person changes in health satisfaction at the following assessment.
Because social identity impacts people’s sense of self and feelings of self-worth (see Tajfel & Turner, 1986), perceiving one’s ingroup to be the target of discrimination should undermine participants’ health. Indeed, as people are motivated to maintain a positive social identity, experiences of discrimination should act as a social stressor that takes a physiological toll on the body (Brondolo et al., 2008; Guyll et al., 2001) and, in turn, lead to declines in health satisfaction (Pascoe & Smart Richman, 2009). However, due to systematic differences in experiences of discrimination, we anticipate asymmetries to emerge between ethnic groups. Specifically, we expect perceptions of ethnic discrimination to undermine health satisfaction for Māori (Hypothesis 1)—a structurally disadvantaged ethnic group who experience frequent forms of discrimination (Ministry of Health, 2023). Conversely, we expect the association to be weaker or non-significant for Pākehā given their structurally advantaged position in society (Hypothesis 2).
The Context of Aotearoa
Although Aotearoa is often heralded internationally for its progressive approach towards intergroup relations, the enduring effects of colonialization continue to perpetuate extensive injustices for Māori, the Indigenous people of Aotearoa (Thom & Grimes, 2022). Shortly after the arrival of Pākehā colonizers from what is now the United Kingdom, a foundational document, Te Tiriti o Waitangi (i.e., The Treaty of Waitangi), was established to outline the rights and responsibilities of the Crown and Māori. Written in both English and Te Reo Māori, Te Tiriti articulated three guiding principles that granted the Crown limited governance over Pākehā residing in Aotearoa and permitted it to act as temporary custodians of the land. Crucially, the version of Te Tiriti written in Te Reo Māori affirmed Māori sovereignty and self-determination over their people and whenua (i.e., land; Berghan et al., 2017; Came et al., 2024), whereas the version written in English did not capture these important nuances.
Given the inconsistencies between the English and Te Reo Māori versions of the document, harmful and self-serving interpretations of Te Tiriti by Pākehā colonizers have led to ongoing disputes since its signing in 1840, with the English version being used to falsely justify claims that Māori ceded sovereignty (Came et al., 2024; Mutu, 2010). This misconstrual enabled illegal land acquisition through confiscation and other coercive means (Thom, 2022), producing a series of direct and downstream consequences that have privileged Pākehā at the expense of Māori (Curtis et al., 2023). Despite the Waitangi Tribunal identifying repeated violations of Te Tiriti (Came et al., 2020; Waitangi Tribunal, 2014), breaches continue into the present. Accordingly, many Māori report that colonization continues to affect their lives today (Dyall et al., 2014).
Many consequences operate invisibly, embedded within contemporary social, political and health structures (Curtis et al., 2023). Reflecting these systemic effects, Māori experience significant inequities across several domains (Houkamau et al., 2017), including lower levels of self-rated physical health, and higher rates of suicide, psychological distress and obesity, relative to Pākehā (Te Whatu Ora, 2024a). Given these persistent inequities, Aotearoa offers an ideal context to examine potential asymmetries in the temporal ordering of the relationship between perceptions of discrimination and health satisfaction.
Method
Data Access
The data described here are part of the New Zealand Attitudes and Values Study (NZAVS). Full copies of the NZAVS data files are held by all members of the NZAVS management team and advisory board. A de-identified dataset containing the variables analysed here is available upon request from the corresponding author or any NZAVS advisory board member to replicate or check any published study using NZAVS data. Surveys for each of the 11 annual waves of the study, as well as the Mplus syntax used to run these analyses, are also available on the OSF: https://osf.io/75snb/overview.
Sampling Procedure
Because our measure of satisfaction with health was first assessed at Time 5 in 2013, we analysed data from Times 5–15 of the NZAVS—a longitudinal national probability study of adults that began in 2009. Sampling for the NZAVS occurred on eight occasions. In 2009 (Time 1), a random sample of adults from the electoral roll were invited to participate in a projected 20-year longitudinal panel study. This first sampling occasion yielded 6,518 participants (response rate = 16.6%). By 2011, 3,918 participants remained in the study (60.1% retention from Time 1). To address sample attrition, a non-random booster sample was recruited from the website of a nationwide newspaper. This second sampling occasion yielded 2,966 new participants and increased the sample size at Time 3 to 6,884 participants.
To further increase the size and diversity of the sample, we conducted six additional booster samples by randomly sampling (without replacement) the electoral roll, oversampling hard-to-reach populations. The first of these six sampling occasions was in 2012 (Time 4) and used multiple sample frames to recruit 5,107 new participants into the study (response rate = 10.0%), plus an additional 265 unmatched participants or unsolicited opt-ins. The second sampling occasion occurred in 2013 (Time 5) and recruited 7,579 new participants into the study (response rate = 10.6%), whereas the third sampling occasion occurred in 2016 (Time 8) and recruited 7,667 new participants into the study (response rate = 9.6%). Thus, Time 8 included 21,936 participants (13,781 retained from a prior time point, 7,667 additions from booster sampling, and 488 unmatched or unsolicited opt-ins). By 2017 (Time 9), 17,072 participants remained in the study (retention rate from Time 8 = 72.0%). The fourth sampling occasion occurred at Time 10, which included both a random sample of the electoral roll and a paid Facebook promotion that recruited 29,293 (response rate = 9.2%) new participants into the study. A further 628 participants opted into the study, resulting in a sample size of 47,948 at Time 10. By Time 14, 33,722 participants were in the study, including 30,107 who were retained from one or more previous waves (with a 70.39% retention from Time 13 and a 29.35% retention from Time 1), 2,041 from a new cohort booster sample that randomly sampled 18–23-year-olds from the electoral roll (response rate = 5.83%), and 1,574 opt-ins. Time 15 included a final pair of booster samples that recruited 3,293 new participants into the study. In total, 76,409 participants completed at least one of the 15 annual waves of the study, 68,147 of whom identified as Māori or New Zealand European.
Participants
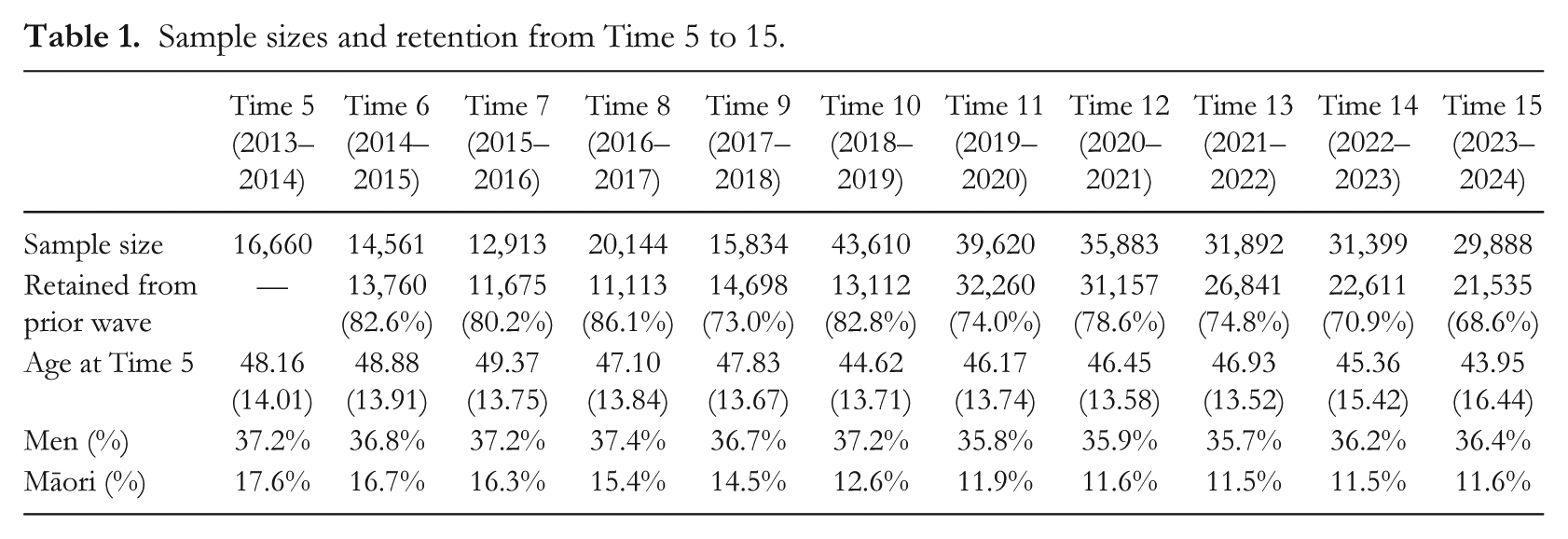
Of these 68,147 participants, 65,797 (i.e., 96.6% of the focal sample) completed our variables of interest at one or more waves and formed the basis of the sample for the current study (see Table 1 for an overview of the sample size and retention rate at each time point). To examine potential asymmetries across structurally advantaged and disadvantaged groups, analyses were grouped by ethnic majority group and ethnic minority group status. The ethnic majority group consisted of 56,499 New Zealand Europeans (Mage at Time 5 = 43.50, SD = 15.74; 61.8% women, 37.5% men, 1.1% gender diverse) who completed an average of 4.62 (SD = 2.86) waves, whereas the ethnic minority group consisted of 9,298 Māori (Mage at Time 5 = 40.30, SD = 15.50; 65.2% women, 33.3% men, 1.6% gender diverse) who completed an average of 4.19 (SD = 2.90) waves.
Sample sizes and retention from Time 5 to 15.
Measures
The current study measures perceived discrimination and self-rated health satisfaction at 11 consecutive annual waves.
Results
The present study aimed to examine the longitudinal relationship between perceived discrimination and health satisfaction across members of structurally disadvantaged and advantaged groups (for descriptive statistics and bivariate correlations, see Tables S1 and S2 in the supplemental material). Given that unfavourable social comparisons can undermine well-being by highlighting disparities in treatment and status (Baumeister & Leary, 1995; Tajfel & Turner, 1986), perceived discrimination should negatively impact individuals’ satisfaction with their health—particularly for members of structurally disadvantaged groups who chronically face unfair treatment. Indeed, these comparisons are situated within a broader context of historical and systemic inequalities for Māori which, due to their pervasive nature, may amplify the toll of discrimination on health over time. In contrast, Pākehā are a structurally advantaged group who report less frequent experiences of discrimination and, as a result, should be less affected by such comparisons (see Schmitt & Branscombe, 2002).
To test these hypotheses, we conducted a multi-group RI-CLPM. Because there was no theoretical reason to expect the size of the autoregressive and cross-lagged associations to differ between assessments, we estimated the model to be a stationary process (Orth et al., 2024; Osborne & Little, 2024). Specifically, we estimated a random intercept for both perceptions of discrimination and satisfaction with one’s health by constraining the corresponding factor loadings at each assessment occasion to 1. We then estimated within-person departures from these trait-level means by creating phantom variables at each assessment occasion and constraining the residual variance of the grand mean to 0. Accordingly, all the variance in our annually assessed measures of perceptions of discrimination and satisfaction with health was parsed into a stable, between-person component (i.e., the corresponding random intercepts) and time-specific, within-person departures from these trait-level means at each assessment occasion. Effect sizes are reported as unstandardized coefficients with corresponding 95% confidence intervals (CIs). Missing data were addressed by using full information maximum likelihood estimates (FIML; see Enders & Bandalos, 2001). Notably, FIML outperforms other approaches to missing data including both listwise and pairwise deletion by utilizing all the data available within the dataset (e.g., whereas listwise or pairwise deletion would delete participants from the booster samples, FIML allows for the inclusion of these participants; see Enders, 2022).
Results revealed that our multi-group RI-CLPM fit these data well, Σ2(426) = 6109.46, RMSEA = .020 [.020, .021], CFI = .981, SRMR = .045. Focusing on the model with Māori participants first (see Figure 1), the random intercepts for perceptions of discrimination and satisfaction with health correlated negatively (b = −0.32, 95% CI [−0.36, −0.28], p < .001). These results indicate that participants who had relatively high trait-level perceptions of discrimination across all 11 annual assessments tended to have relatively low levels of satisfaction with health over the same period. Notably, the within-person autoregressive effects for both perceptions of discrimination (b = 0.14, 95% CI [0.12, 0.16], p < .001) and satisfaction with one’s health (b = 0.19, 95% CI [0.18, 0.21], p < .001) were also significant. Whereas autoregressive effects in the traditional CLPM framework reflect the stability of constructs, they capture inertia in an RI-CLPM. Thus, a 1-unit departure from a person’s trait-level perceptions of discrimination at one assessment predicted a 0.14-unit departure from their trait-level mean at the subsequent assessment.
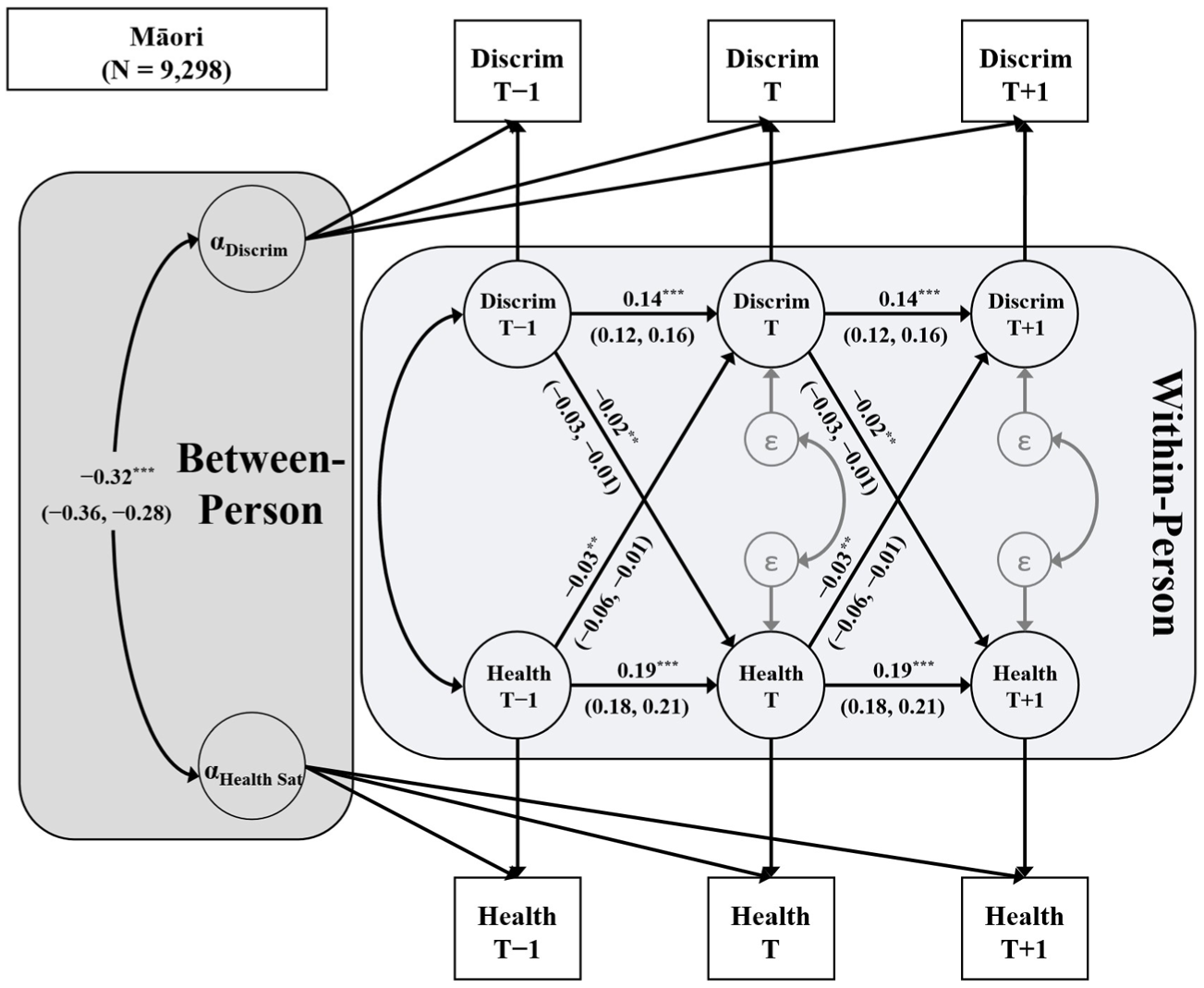
Multi-group RI-CLPM examining the associations between perceived discrimination and health satisfaction among Māori.
After adjusting for both the between-person effects and the within-person inertia, we found support for Hypothesis 1 amongst participants who identified as Māori. Specifically, an increase in one’s trait-level perception of discrimination at one assessment predicted later declines in health satisfaction (b = −0.02, 95% CI [−0.03, −0.01], p = .002). There was, however, evidence of a bi-directional association between health satisfaction and subsequent perceptions of discrimination (b = −0.03, 95% CI [−0.06, −0.01], p = .006). Follow-up analyses that constrained these two cross-lagged paths to equality did not significantly reduce model fit, ΔΣ2(1) = 1.97, p = .161, indicating they were of comparable size. Thus, departures from one’s trait-level perceptions of discrimination at one assessment predict decreases in health satisfaction a year later, and departures from one’s trait-level health satisfaction at one assessment predict comparably sized decreases in perceptions of discrimination the following year.
Turning to our results for New Zealand Europeans (see Figure 2), we once again see that trait-level perceptions of discrimination correlated negatively with average levels of health satisfaction across assessment occasions (b = −0.16, 95% CI [−0.17, −0.15], p < .001). Also replicating the results that emerged amongst participants who identified as Māori, the autoregressive effects for both perceptions of discrimination (b = 0.14, 95% CI [0.13, 0.15], p < .001) and satisfaction with health (b = 0.20, 95% CI [0.19, 0.21], p < .001) were significant. But in contrast to the results for Māori participants, neither the cross-lagged effects of perceptions of discrimination on satisfaction with health (b = −0.00, 95% CI [−0.01, 0.00], p = .459), nor the cross-lagged effects of health satisfaction on perceptions of discrimination (b = −0.00, 95% CI [−0.01, 0.00], p = .363), were significant. Subsequent analyses that constrained the cross-lagged effects of perceptions of discrimination on health satisfaction to equality across New Zealand European and Māori participants significantly reduced model fit (i.e., ΔΣ2(1) = 6.97, p = .008). Thus, consistent with Hypothesis 2, the cross-lagged effect of perceptions of discrimination on satisfaction with health was significantly larger for participants who identified as Māori vis-à-vis New Zealand Europeans.
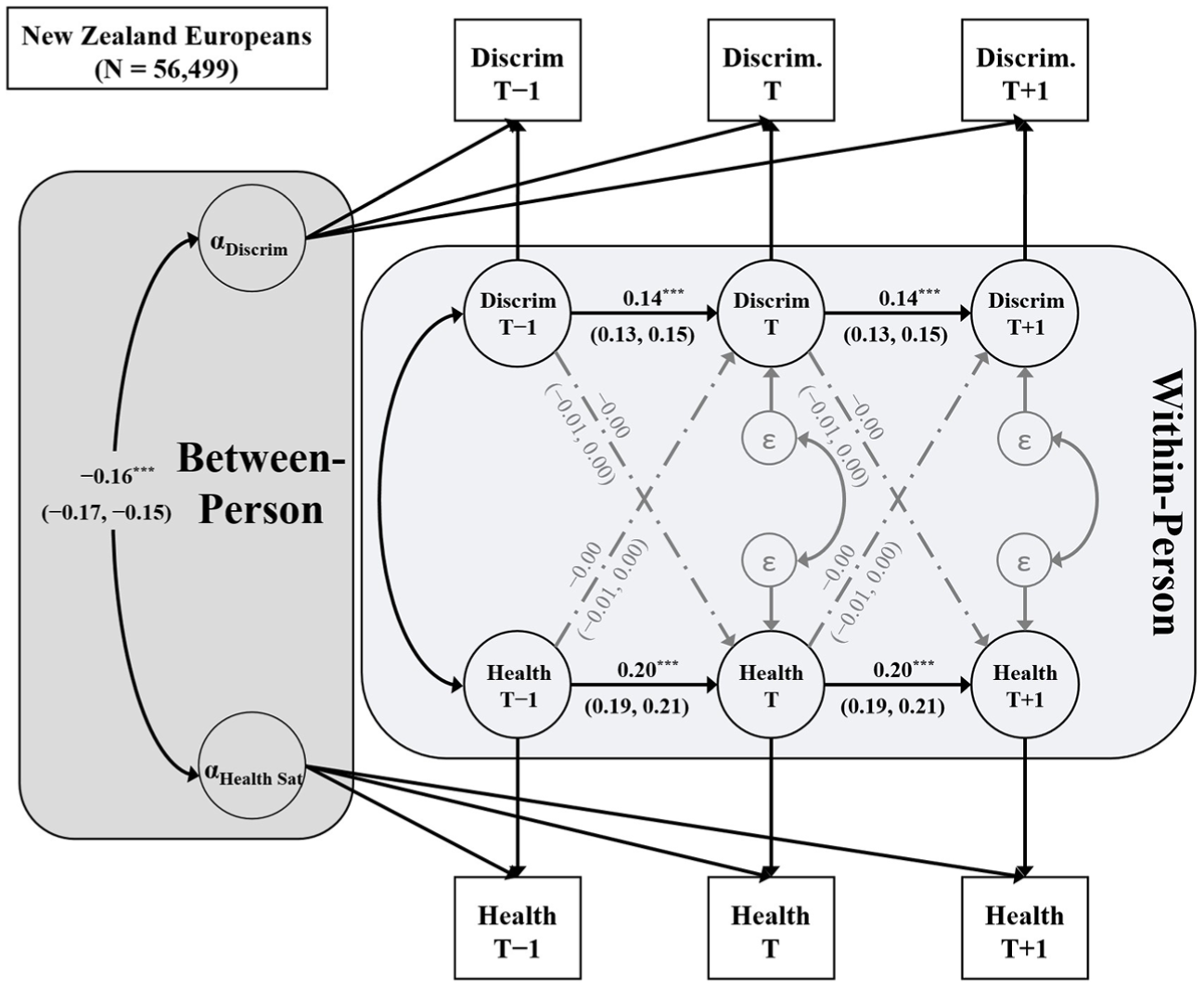
Multi-group RI-CLPM examining the associations between perceived discrimination and health satisfaction among New Zealand Europeans.
Discussion
Despite extensive cross-sectional research examining the association between perceived discrimination and health satisfaction (e.g., see Pascoe & Smart Richman, 2009), little work has investigated how these factors influence each other over time. Among the limited longitudinal studies conducted thus far, none have separated the stable between-person differences that persist over time from the within-person changes that form the core of psychological theory. Consequently, there is a dire need for research that decomposes trait-like, between-person stability, and within-person changes over time. Our study addresses this lacuna by utilizing a multi-group RI-CLPM to assess the within-person associations between perceived discrimination and health satisfaction, and to identify the temporal order of these variables. Building on this important methodological contribution, our study also examines the longitudinal effects of perceived discrimination on health satisfaction among both structurally advantaged and disadvantaged groups. Considering the enduring health disparities between groups (Te Whatu Ora, 2024b), it is imperative to identify the pivotal factors that contribute to these inequalities to develop effective interventions. As such, we examine these associations within the unique sociocultural context of Aotearoa New Zealand to contrast the patterns between Māori and New Zealand Europeans.
As expected, the between-person effects revealed a negative association between perceived discrimination and health satisfaction within structurally disadvantaged groups. Specifically, Māori who were higher in perceived discrimination across the 11 annual waves of data also tended to report lower levels of health satisfaction across time. These results build upon and extend the substantial body of work which finds a negative association between perceived discrimination and health satisfaction (e.g., see Pascoe & Smart Richman, 2009), by showing that these associations also emerge at the within-person level of analysis. Given the high levels of discrimination faced among ethnic minorities, understanding the consequences of unfair treatment on health and well-being is critical (Ministry of Health, 2023).
In contrast, we expected a weaker or non-significant association between these variables for structurally advantaged group members given the relative infrequency of their experiences with discrimination based on ethnicity (Ministry of Health, 2022). Indeed, the between-person effects revealed that perceived discrimination did correlate negatively with levels of health satisfaction; however, the effect was significantly weaker than was observed among Māori respondents. These results corroborate past research suggesting that members of structurally advantaged groups typically encounter isolated instances of discrimination instead of the systemic and frequent acts of discrimination that have a psychological toll on minoritized targets (Branscombe et al., 1999; Schmitt & Branscombe, 2002). Consequently, the smaller correlation between the random intercepts among members of the advantaged group likely reflects less frequent encounters that are perceived as ethnic discrimination.
Our results also build on cross-sectional work examining the correlates of perceived discrimination among Māori (Houkamau et al., 2017) by providing a longitudinal examination of this relationship. Specifically, our results demonstrate that perceptions of discrimination precede increases from one’s trait-level satisfaction with their health the next year. Because satisfaction with one’s health correlates strongly with mortality risk (Idler & Benyamini, 1997), this is an important proxy measure for physical health. Thus, our results help identify a likely contributor (namely, perceptions of discrimination) to persistent health disparities between structurally advantaged and disadvantaged groups.
Notably, previous research suggests that there is a dose-response relationship between experiences with discrimination and health: increases in the frequency of discrimination correlate with declines in physical health (see Harris et al., 2012). Although both groups may feel discriminated against, ethnic discrimination takes a particular toll on the health of ethnic minorities because of how often they experience unfair treatment (Ministry of Health, 2023). Our results thus help corroborate the stress and coping framework, which argues that repeated experiences of discrimination over time evolve into chronic stressors that undermine physical health (Pascoe & Smart Richman, 2009).
Although our results show that perceptions of discrimination preceded declines in satisfaction with health, there was evidence of a bidirectional relationship between perceived discrimination and health satisfaction at the within-person level of analysis for Māori. Specifically, departures from one’s trait-level health satisfaction at one assessment predict increases in perceptions of discrimination the following year among Māori. These results deviate from past research, suggesting that racial discrimination in job seeking is associated with health-related work limitations, but not vice versa (Gee & Walsemann, 2009). The current study does, however, focus on within-person changes in ethnic-based discrimination (as opposed to potentially chronic experiences of discrimination while job seeking), which may explain these discrepancies. Future research should aim to further understand this bi-directional relationship particularly within the healthcare domain. Indeed, previous research indicates that experiences of discrimination are associated with unmet healthcare needs among Māori (Harris et al., 2019).
In stark contrast to our results for Māori, neither of the cross-lagged effects between perceptions of discrimination and health satisfaction were significant among New Zealand Europeans (i.e., the structurally advantaged group). Subsequent analyses confirmed that the cross-lagged effects of perceived discrimination on satisfaction with health were significantly stronger for Māori compared to New Zealand Europeans. Although New Zealand Europeans may occasionally report instances of ethnic-based discrimination, these attributions do not capture systemic exclusion from mainstream society. Accordingly, such perceptions do not carry the same weight as when experienced by structurally disadvantaged groups (Schmitt & Branscombe, 2002). The relative infrequency of these perceptions of discrimination is also unlikely to evolve into a chronic stressor and, thus, may not impose a significant toll on New Zealand Europeans’ physical health over time.
Our results reveal important asymmetries between structurally advantaged and disadvantaged groups when it comes to the consequences of perceived discrimination on health satisfaction. Specifically, perceptions of discrimination precede decreases in health satisfaction over time for structurally disadvantaged groups, but not for their advantaged counterparts. Consequently, our results highlight the need for targeted initiatives that focus on improving health outcomes for disadvantaged groups to promote an equitable health system. In doing so, our results demonstrate the need for equity-focused initiatives, such as the recently disestablished Te Aka Whai Ora (i.e., the Māori Health Authority), which aimed to uplift the health of Māori by creating an equitable health system that reflects the principles of Te Tiriti o Waitangi (i.e., the treaty partnership between Māori and Pākehā). Furthermore, results shed light on health risk factors (i.e., discrimination) for preventative health interventions.
Finally, our results have important theoretical implications for our understanding of group-based processes underlying identity, given that they appear to operate differently across advantaged and disadvantaged groups. For structurally disadvantaged groups, identity can be both a potential vulnerability and a source of resilience (Jetten et al., 2012). Indeed, whereas the Identity-Deprivation-Efficacy-Action-Subjective Well-Being (IDEAS) model suggests that group identification may heighten the salience of discrimination and undermine well-being, a strong social identity can also foster beneficial group processes, such as engagement in collective action (Abrams et al., 2020; Van Zomeren et al., 2008). Research from the social cure perspective similarly reveals that group-based identities provide important psychological resources, including a sense of belonging and social support (Branscombe et al., 1999; Jetten et al., 2012). Although identity precedes feelings of injustice across both structurally advantaged and disadvantaged groups (Thomas et al., 2020), the formation of an identity is shaped by its relative position of power and ongoing intergroup relations (Schmitt & Branscombe, 2002). In turn, the relative position of the ingroup carries different implications, including differential exposure to systemic discrimination. Consequently, our results demonstrate that the association between perceived discrimination and health satisfaction unfolds differently across groups over time and reflect distinct group-based processes.
Strengths, Limitations and Future Directions
In conjunction with these theoretical implications, another strength of the current study is our use of a large-scale, nationwide random sample of adults across 11 annual assessments. Indeed, our large sample size and longitudinal data increases our confidence that these results generalize to the public and across time. An additional strength is our use of an RI-CLPM. Given that traditional CLPMs confound within- and between-person effects, the use of an RI-CLPM allows us to direct our focus to within-person effects and, thus, unravel the temporal ordering of constructs over time (see Berry & Willoughby, 2017; Hamaker et al., 2015; Osborne & Little, 2024). Specifically, after estimating random intercepts to adjust for the trait-like stability of perceived discrimination and health satisfaction, we reveal that within-person changes in perceptions of discrimination precede changes in health satisfaction over time among disadvantaged groups. Accordingly, it is important to keep in mind that our effect sizes were small but consistent with the nascent literature on RI-CLPMs (e.g., see Orth et al., 2024). Nevertheless, our study offers the most robust evidence to date for the within-person longitudinal association between perceived discrimination and health satisfaction.
Although the current study has numerous strengths, several limitations are also worth noting. For one, our measure of discrimination captures perceptions of both personal and group-based discrimination. Although this item enables us to capture individuals’ subjective perceptions of discrimination and, thus, account for the experiences of both advantaged and disadvantaged groups, differences in the interpretation of discrimination likely exist across groups. Past research reveals that individuals from disadvantaged groups often minimize personal discrimination relative to group-based discrimination (Taylor et al., 1990), whereas members of advantaged groups often overestimate ingroup discrimination (Bahamondes et al., 2020, 2022; Wilkins & Kaiser, 2014). Consequently, future research should distinguish between personal and group-based discrimination to provide a more nuanced understanding of these status-based asymmetries.
Relatedly, previous research identifies challenges in measuring subjective accounts of discrimination. Self-report measures may be unable to fully capture the nuances of racism, especially its subtle forms, and are subject to recall biases (Neblett, 2019). A large body of research does, however, continue to rely on self-reported experiences of discrimination to examine its effect on health, largely because there are few alternative methods capable of capturing discrimination in ways that are not dependent on subjective accounts (Lewis et al., 2015).
Reflecting its inclusion in a large omnibus survey, our perceived discrimination measure is based on a single item. Although the use of single-item measures in surveys enables the investigation of a broad range of variables, it also limits the depth at which any one construct can be examined. Nevertheless, this item has high face validity. An analysis of short-form scales included in the NZAVS also demonstrates that other single-item indicators have acceptable levels of reliability compared to their full-form counterparts (Sibley et al., 2024). These results suggest that single-item measures can adequately capture the constructs assessed in multi-item scales. Moreover, our single-item measure of perceived discrimination has been used to effectively predict other outcomes in several previous studies (Houkamau et al., 2017; Kapeli et al., 2020; Lilly et al., 2025). Finally, a systematic review of quantitative research shows that this item appears in 16.7% of the studies included on racism and health in Aotearoa (Talamaivao et al., 2020), thus demonstrating that it is a consistently used measure in the literature. Nevertheless, future research should utilize multi-item scales to capture the full depth of these nuanced experiences.
Due to the omnibus nature of our survey, we were also limited to a three-item measure of health satisfaction with low levels of reliability. Although it would have been ideal to include additional items to increase the reliability of the measure, survey space is often limited in large-scale population-based surveys like the NZAVS. A recent scale validation study does, however, reveal that our three-item measure is only slightly less reliable than the full five-item measure (see Sibley et al., 2024). That said, given the need to replicate across both samples and stimuli (see Westfall et al., 2015), future research should examine the generalizability of our results with different—and perhaps newer—measures of health satisfaction.
Another limitation of the current study is that (due to analytical constraints) we do not account for multiple ethnic identities in our analyses (i.e., participants who identify as both Māori and New Zealand European). This is important to note, as previous studies suggest that there may be differences in experiences of discrimination among those who identify with multiple ethnic groups as opposed to one (Houkamau & Sibley, 2014). Indeed, Māori who report being perceived as New Zealand Europeans (as opposed to those who are perceived as Māori) disclosed fewer experiences of discrimination and had better health and well-being outcomes (Harris et al., 2013). In contrast, individuals who identify solely as Māori report worse social, educational, and economic outcomes than do those who identify as both Māori and New Zealand European (Houkamau & Sibley, 2014). Consequently, future research should examine multiple ethnic identities to identify any nuances that we are unable to capture in the present study.
Although the current study focuses on only one ethnic minority group, other ethnic minority groups also experience discrimination frequently within New Zealand. Indeed, alongside Māori, Pacific and Asian adults are more likely than New Zealand Europeans to experience ethnic-based discrimination (Te Whatu Ora, 2024a). However, due to sample size limitations, we decided to focus exclusively on Māori and New Zealand Europeans (i.e., the two largest ethnic groups in New Zealand). This focused approach allows us to identify nuances specific to the contextually distinct relationship between settler-colonizers and the Indigenous peoples of New Zealand, which have drastically shaped health inequities (Moewaka Barnes & McCreanor, 2019). Nevertheless, future research should examine these associations among other ethnic minority groups.
Currently, global approaches to healthcare prioritize the needs of structurally advantaged group members and neglect holistic approaches of health management practised by Indigenous communities before the introduction of colonization. As such, current health models do not adequately address contextual needs among Indigenous populations (Barnabe, 2021), which ultimately contributed to their poorer health outcomes compared to non-Indigenous peoples (Durey & Thompson, 2012). Although we focus on the context of Aotearoa/New Zealand, the samples we utilize represent a cultural dynamic that resonates with patterns observed among colonized countries worldwide. Indeed, in recent decades, there has been a collective mobilization of Indigenous peoples advocating for the global recognition of Indigenous rights (see United Nations, 2007). There are, however, important nuances inherent to the socio-political histories of each geographical location (e.g., Moewaka Barnes & McCreanor, 2019). Consequently, future research should investigate the relationships identified here among Indigenous populations globally.
Conclusion
The overwhelming inequities in health outcomes observed between structurally advantaged and disadvantaged groups necessitates an investigation into the factors that contribute to these preventable issues. We meet this need by utilizing 11 annual waves of longitudinal panel data to investigate the temporal association between perceptions of discrimination and health satisfaction. Expanding on previous longitudinal work (e.g., see Paradies et al., 2015), the current study uses a multi-group RI-CLPM to distinguish between the within- and between-person effects of these associations. In doing so, we demonstrate that within-person increases in perceptions of discrimination precede decreases in health satisfaction (and vice versa) among a structurally disadvantaged group. Notably, these within-person effects failed to emerge among members of the advantaged group. Thus, the current study highlights the need to address the pervasive experiences of discrimination amongst the structurally disadvantaged in order to produce more equitable health outcomes across groups of varying social status.
Supplemental Material
sj-docx-1-gpi-10.1177_13684302261428465 – Supplemental material for Uncovering the toll: The impact of perceived discrimination on health among structurally advantaged and disadvantaged groups
Supplemental material, sj-docx-1-gpi-10.1177_13684302261428465 for Uncovering the toll: The impact of perceived discrimination on health among structurally advantaged and disadvantaged groups by Chantelle Kimberley, Zoe Bertenshaw, Chris G. Sibley and Danny Osborne in Group Processes & Intergroup Relations
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this manuscript was supported by a University of Auckland Doctoral Scholarship awarded to the first author, and a Templeton Religion Trust grant (No. 0196) awarded to the second author. The aforementioned funding sources had no role other than financial support.
Ethics Statement
The authors confirm that the data described in this paper stem from research conducted in adherence to the APA Code of Conduct.
Data Availability Statement
The data described in this paper are part of the New Zealand Attitudes and Values Study (NZAVS). Full copies of the NZAVS data files are held by all members of the NZAVS management team and advisory board. A de-identified dataset containing the variables analysed in this manuscript is available upon request for the purposes of replication or checking of any published study using the NZAVS data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.