
Abstract
In recent years, there has been growing recognition of the threats to health posed by loneliness. One of the main strategies that has been recommended to address this is social prescribing (SP). This typically involves general practitioners (GPs) and other health practitioners directing clients who are experiencing loneliness and related conditions to take part in social activities—typically in recreational and community contexts. However, evidence for the effectiveness of SP is mixed—leading some to suggest that enthusiasm for it might be misplaced. In this review, we argue that a core problem with most existing approaches to SP is that they lack a strong theoretical base. This has been a barrier to (a) understanding when SP will work and why, (b) designing optimally effective SP programmes, and (c) developing practitioner skills and appropriate infrastructure to support them. As a corrective to this state of affairs, this review outlines a three-tier social identity framework for SP and five associated hypotheses. These hypotheses predict that SP will be more effective when (a) clients join groups and (b) these groups are ones with which they identify, and when SP is supported by (c) social-identity-enhancing social infrastructure, (d) a social-identity-based therapeutic alliance, and (e) identity leadership that builds and shapes this alliance as well as clients’ identification with prescribed groups. This framework is supported by a range of evidence and provides an agenda for much-needed future research and practice.
The Scourge of Loneliness
Loneliness is the psychological experience of unwanted social isolation (C. Haslam et al., 2018; Hawkley & Cacioppo, 2010) and in recent years there has been growing recognition that it is a serious threat to health. For example, an influential meta-analysis of nearly 150 studies by Holt-Lunstad et al. (2010) found that when people lacked social support and were socially isolated (rather than socially integrated) this represented a risk of mortality equivalent to that associated with smoking and greater than that of many other well-known health risks (e.g., not exercising, high alcohol consumption, obesity). As well as compromising longevity, loneliness can also represent a more immediate threat to life in being associated with both suicidal ideation and death by suicide (McClelland et al., 2020; Shaw et al., 2021). At the same time, many people generally fail to recognise this threat. Illustrative of this, when members of the general public were asked to rank the 11 risk factors that were included in Holt-Lunstad et al.’s meta-analysis in terms of their importance as predictors of mortality, lacking social support and not being socially integrated were perceived to be the least important predictors when in fact they were the most important (S. A. Haslam et al., 2018).
There are several reasons why, historically, the threat of loneliness has largely flown under the health radar. A key one is that scientists’ understanding of health and the processes that compromise it is largely informed by a medical model of disease and treatment (C. Haslam et al., 2018). As loneliness is primarily a social condition (rather than a biological risk factor or disease), it is therefore not encompassed by this model and lies largely beyond its imagination (Engel, 1977; S. A. Haslam, Haslam, et al., 2019). And while it is recognised as a potential consequence of medical conditions (e.g., stroke, multiple sclerosis, cancer; Rokach, 2003), it is common for treatment to focus much more on those conditions than on their social consequences. In part, this is because loneliness is not amenable to medical treatment (although this has not stopped people from trying, for example, by prescribing oxytocin, β-blockers, or NOX inhibitors; Xia & Li, 2018).
All of this would not be a problem if loneliness were rare. But it is not. In the UK, for example, a 2018 survey of over 50,000 adults found that only a minority of people (42%) said they “rarely” or “never” felt lonely (Hammond, 2018). Very similar results emerged from similarly sized surveys in Australia, which found that only one third of people aged 18–24 years “rarely” or “never” felt lonely (S. A. Haslam et al., 2021) and that 1 in 6 people experienced severe loneliness (Ending Loneliness Together, 2023). As a result, it has been observed that loneliness is “the leprosy of the 21st century” (Bound Alberti, 2019, p. 1; see also Hertz, 2020) and that—at least in the Global North—there is something of a loneliness pandemic (Bound Alberti, 2018; Laranjeira, 2021).
As a result, in the last decade or so, there have been growing calls not only to recognise the seriousness and pervasiveness of loneliness, but also to do something about it (e.g., Gerst-Emerson & Jayawardhana, 2015; Hawkley & Cacioppo, 2010; Lim et al., 2020). In the scientific community, this has resulted in increased efforts to understand its causes, mechanisms, and consequences (e.g., Cacioppo et al., 2015; S. A. Haslam et al., 2022; Lim et al., 2020). Alongside this, governments, policy makers, and community agencies around the world have become increasingly concerned about tackling loneliness—and their concerns have been the stimulus for a raft of initiatives that differ in scale, focus, and ambition. Of these, the most influential are those that involve some form of social prescribing (SP), with 17 countries now having invested in formal social prescribing programmes and policies (Chatterjee et al., 2018; Dingle et al., 2022; Morse et al., 2022).
The Social Prescribing Landscape
Social prescribing (SP) is an umbrella term that broadly describes any intervention that involves general practitioners (GPs), health practitioners, or various other “social brokers” (e.g., volunteers, community workers; Blanchet et al., 2017) helping clients who are experiencing or are at risk of loneliness and other forms of social disconnection to take part in nonclinical activities that are designed primarily to increase their social connectedness and social integration (Muhl et al., 2023; World Health Organization [WHO], 2022). This typically involves connecting clients to existing organisations and services, particularly those associated with recreational and community activities. Typically, too, people engage in SP as part of a group (Brandling & House, 2009; Wakefield et al., 2022). And while this group-based delivery and the group dynamics that surround it are often treated as insignificant features of SP, as we will clarify below, they often prove pivotal to SP success or failure.
As Figure 1 indicates, it is possible to specify three tiers of the SP landscape that differ in their inclusivity and focus, and also in the degree to which SP itself is incidental (i.e., provided naturally as a by-product of life in a healthy society; Williams et al., 2019) or purposive (i.e., provided remedially to address identified health problems). Critically though, all three tiers can be seen to centre on group relations—although these too differ in their inclusivity and focus.
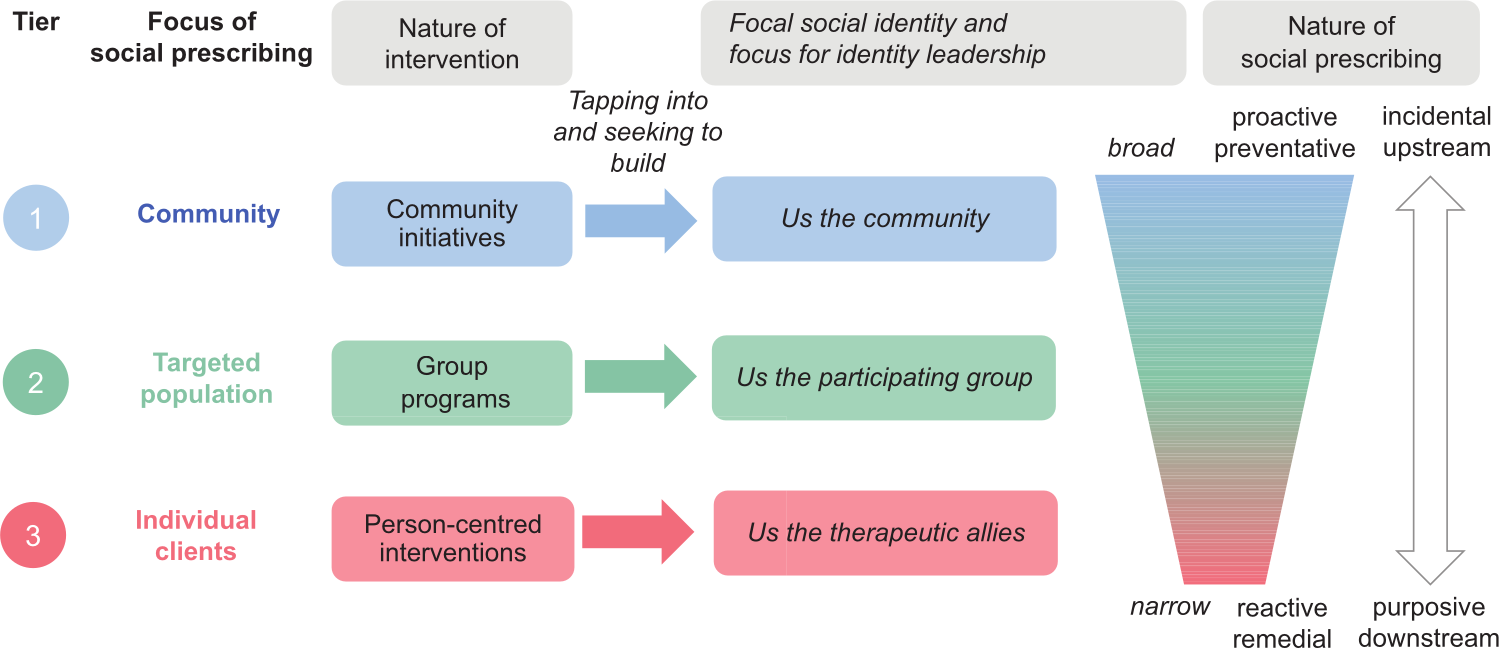
A three-tier social identity framework for social prescribing.
While these are often overlooked in discussions of SP (Brandling & House, 2009), at the most general and abstract level, Tier 1 SP practices centre on community initiatives that aim to provide support and resources for any member of the public. This support can come in a wide range of forms (material, informational, cognitive, emotional, or social), and be provided in a wide range of settings. For example, it may be provided by volunteers in a community centre, or by a church group that provides support to anyone who drops in (Bowe et al., 2020). Alternatively, large-scale programmes may seek to provide support across a broad community. For example, in Australia, Neighbours Every Day (formerly known as Neighbour Day) is a nationwide initiative that aims to help people organise activities in their own local neighbourhood, with a view to building social connectedness and making their residential community stronger (see Fong et al., 2021).
More generally, alongside such initiatives, SP involves people engaging with diverse forms of social infrastructure that provide a platform for them to connect with others. This function, for example, might be served by a library, a park, an art gallery, a community garden, or a sports facility (Brandling & House, 2009; Bungay & Clift, 2010; Poulos et al., 2019). Clearly, the primary purpose of facilities of this form is not to tackle social disconnection—and so the SP here is embedded within existing community facilities rather than bespoke services. As such, then, it is incidental rather than purposive. But insofar as these facilities provide opportunities for people to connect meaningfully with others, they can nevertheless be considered frontline resources in the battle against loneliness, and they are a critical part of the SP (and general health) terrain (Fong et al., 2020; Imrie, 2017). Indeed, Klinenberg (2016) and others (e.g., Becker et al., 2021; Crowe et al., 2024; Poole & Huxley, 2024) make the point that the decline in such infrastructure (e.g., due to government defunding and individualistic policy settings) is a key reason why we find ourselves needing to fight this battle.
At an intermediate level, Tier 2 SP is supported through group programmes in which relevant agencies, services, and health practices aim to address loneliness in targeted populations (e.g., veterans, people with a particular need or health condition, clients of a particular practice). For example, designated Link Workers associated with a medical centre or practice may direct their clients to different group activities that are available in the local community (e.g., a theatre group, a choir, or a community exercise program such as Parkrun). Alternatively, they may direct them to a group programme specifically designed to tackle loneliness (e.g., Groups 4 Health; Cruwys, Fong, et al., 2022; C. Haslam, Cruwys, et al., 2016, 2019). Organisations, too, may have a remit to support particular groups and thereby facilitate social connection. For example, Men’s Sheds (of which, there are over 750 in Australia) focus on providing facilities and activities that help men in local communities come together and collaborate on various projects (Milligan et al., 2016). Similarly, some charities (e.g., Reclink in Australia, the Marmalade Trust in the UK) specialise in delivering programmes that help people who are vulnerable (e.g., as a result of homelessness, unemployment, or a health condition) to join recreational groups (Cruwys et al., 2014, 2018; Marmalade Trust, 2023; Reclink, 2023).
Finally, in its most focused and prototypical form, Tier 3 SP involves person-centred interventions in which an individual prescriber works closely with an individual client. Ideally, the prescriber will have specialised knowledge about SP and community assets, and a job title that signals this (e.g., link worker, community navigator, or community connector; Drinkwater et al., 2019; Sharman et al., 2022). The client (or patient) will often present with profound and complex challenges that are associated with long-term loneliness and a range of comorbid problems (e.g., anxiety, depression; Dingle & Sharman, 2022). To help them overcome these, they will generally need a personalised social prescription, and will often need to be supported throughout this process (e.g., Cooper et al., 2022; Lim et al., 2020; Sharman et al., 2022; Smith et al., 2021).
As can be seen from Figure 1, SP differs across these three tiers of delivery in the degree to which it is broad and proactive rather than narrowly focused and remedial. Indeed, community initiatives generally have the latent (rather than explicit) function of tackling loneliness, and people often find their own way to them. As noted above, this means that they can be overlooked in discussions (and evaluations) of SP (and certainly are not prototypical exemplars of it). Nevertheless, we think it is important to recognise them as part of the SP landscape, not least because they constitute the most natural and sustainable form of social prescribing and are an important focus for efforts to change the upstream social determinants of mental health rather than just the downstream consequences of social atomisation (Williams et al., 2019). Moreover, in practice, distinctions between these tiers of service are somewhat blurred—in part because they are interdependent. Men’s Sheds and community centres, for example, are often both community initiatives and a site for group programmes. Such entities and the social infrastructure they are part of often also have a key role to play in the design and provision of personalised SP.
Practice in Need of Theory: Beyond Pathway Models of Social Prescribing
Cursory though it is, it is apparent from the foregoing overview that SP is not a clearly defined singular activity but rather a complex system of practices that relate in diverse ways to the multifaceted challenges of trying to tackle loneliness (Husk et al., 2019). Aside from the difficulties that this complexity causes when trying to define SP, this diversity has also hindered theoretical progress in the field. In line with this, Husk et al. (2020) note that the field is currently approached and understood through the lens of “if-then” referral models, which seek to describe optimal pathways for taking different types of clients through a process of SP (see e.g., Drinkwater et al., 2019).
There are at least three key problems with pathway models of this form. The first is that although they can provide a way for service providers to map out strategies for client management, they are (re)descriptive rather than explanatory. Second, as a result, they provide no basis for (a) understanding when and why SP will work, (b) designing optimally effective SP programmes, or (c) building practitioner capabilities and infrastructure to support them (Stevenson et al., 2019; Wakefield et al., 2022). Third, in the absence of a theory that might do these things, evidence to support these pathway models and the generalised efficacy of SP more broadly is very mixed. As Husk et al. (2020) conclude, the evidence base for SP is thus very “patchy” (p. 310). This has led some researchers and commentators to suggest that enthusiasm for it is misplaced (Poole & Huxley, 2024), or at least premature (e.g., Bickerdike et al., 2017; Husk et al., 2019).
Faced with this disappointing state of affairs, several researchers have argued that it is primarily an empirical issue that reflects a lack of high-quality controlled trials that rigorously evaluate the impact of SP interventions (e.g., Bickerdike et al., 2017; Husk et al., 2016, 2020; Rempel et al., 2017). This is certainly a problem, and studies of this form are very much needed (Chatterjee et al., 2018; Dingle et al., 2022). However, we would argue that, in order to progress, the field does not only need better trials and assessments, and more of them, it also needs a framework to inform and guide practice. As Stevenson et al. (2019) observe, a deeper and in many ways more fundamental problem for the field is that, as things stand, SP is very much “a practice in need of a theory” (see also Cooper et al., 2022; Halder et al., 2021).
Having contributed to a range of stakeholder events around the world in recent years (e.g., research symposia, practitioner conferences, policy summits, and government enquiries), this is certainly our experience of the realities of SP on the ground. Indeed, we believe that without good theory, the patchiness of support will leave service providers and policy makers confused and less willing to invest in SP. Drawing on the large corpus of health and organisational research informed by social identity theorising (after Tajfel & Turner, 1979), what follows is therefore an attempt to provide a theory-informed framework backed by empirical evidence that we might use to better understand, design, and build capacity around SP—while also providing a better appreciation of its limitations. Importantly, too, in contrast to dominant models of SP that focus on the dynamics of treatment alone, this social identity framework seeks to provide a coherent understanding of both treatment and the loneliness that it is primarily designed to treat.
Social Identity and Loneliness
In psychology, there is a general tendency for researchers and practitioners to understand and engage with people in singular terms—in terms of their personal identity associated with an understanding of the self as “I” and “me.” Moreover, this is the understanding that informs most psychological theories in which the self is a focal construct (e.g., theories of self-actualisation, self-esteem, and self-determination). As important as personal identity is, there are nevertheless a range of social contexts in which people’s sense of self is derived largely from their membership in one or more social groups—their social identity associated with a sense of the self as “we” and “us” (Tajfel & Turner, 1979). Homes, workplaces, sports grounds, social clubs, and neighbourhoods all provide examples of contexts in which people’s social identity is salient, and where it is at least as important as personal identity in shaping their cognition, emotions, and behaviour. This is primarily because these are all collective contexts in which—to varying degrees—people act, feel, and think as group members, and where social identity provides them with a sense of psychological connection to other members of a relevant ingroup (“us Smiths,” “us members of the Psychology Department,” “us Lions fans,” “us Grenfell residents,” etc.).
In the 5 decades that have passed since Tajfel and Turner (1979) first discussed the importance of social identity for social behaviour, a large of body of research has served to explore this point and, in particular, Turner’s (1982) core claim that social identity is what makes group behaviour and group life possible (Turner et al., 1987, 1994). In particular, this research has shown that social identity provides a basis for people (a) to align their thinking and behaviour with ingroup norms (Abrams & Hogg, 1990), (b) to trust and respect each other (Smith et al., 2003; Tanis & Postmes, 2005), (c) to influence and be influenced by each other (Turner, 1991), and (d) to work together to develop and achieve shared goals (van Knippenberg & Ellemers, 2003; Wegge & Haslam, 2003). As a result, social identity proves to be foundational to processes of leadership, motivation, and communication (S. A. Haslam, 2004). It is also important for health and well-being (C. Haslam et al., 2018; S. A. Haslam et al., 2009; Jetten et al., 2012, 2017). This is because a sense of social identity (where a person’s sense of self is defined in terms of “us” and not just “me”) proves to be foundational for self-esteem (Jetten et al., 2015) and for a sense of control, self-efficacy, meaning, and purpose (Cruwys et al., 2014; Greenaway et al., 2015; Junker et al., 2019; McNamara et al., 2013). Crucially, too, a sense that one shares social identity with fellow ingroup members is also a basis for people to provide and receive social support, and for that support to be effective (S. A. Haslam et al., 2012). Indeed, this sense of shared social identity is a defining feature of all communities—regardless of whether they are experienced face-to-face or virtually (Blanchard, 2024; S. A. Haslam et al., 2024).
A core point here, then, is that social identity is critical for the psychology of organisations and health because it allows people to participate productively in group life. For example, if Terry is a member of his local Men’s Shed, then identification with this group is a basis for him to find Shed activities meaningful, for him to engage in them enthusiastically, for him to benefit from interaction with fellow “shedders,” and for him to gain a sense of purpose and efficacy from the things that they do together (Barbagallo et al., 2023; Clarke et al., 2023; Ford et al., 2015). In short, social identity makes meaningful group-based connection possible in ways that have distinctive and generally positive consequences for health and well-being, as well as for organisational functioning (S. A. Haslam et al., 2022).
This is all well and good, but it also follows that if a person lacks or loses a sense of social identity, then this is likely to have problematic implications for their health due to a resulting lack of group-based social connection. This is a claim that is supported by another large body of evidence that includes studies of students transitioning to university (Iyer et al., 2009), new mothers (Seymour-Smith et al., 2017), retirees (C. Haslam, Steffens et al., 2019), veterans (Wakefield et al., 2024), and survivors of trauma (Muldoon et al., 2019; for a review, see C. Haslam et al., 2021). In particular, such research provides evidence that social identity change and loss are major catalysts not only for stress, anxiety, and depression (e.g., Cruwys et al., 2014; Junker et al., 2019), but also for loneliness (Becker et al., 2021; Evans et al., 2022; McIntyre et al., 2018).
More generally, then, such research speaks to three observations that are critical for the analysis of loneliness and SP (S. A. Haslam et al., 2022). First, the lack or loss of meaningful social group memberships (and the sense of social identity that they provide) is a major cause of loneliness (Hayes et al., 2022; Peterson, 2018; van Dick et al., 2023). Second, the toxic effects of loneliness (e.g., as a trigger for other health issues and suicidal ideation) can be seen, at least in part, to arise from the absence of this distinct form of social connection (Cruwys et al., 2018; C. Haslam et al., 2024). Third, SP should be effective in tackling loneliness to the extent that it serves to build, restore, and sustain social-identity-enhancing group-based connections (Dingle & Sharman, 2022; Këllezi et al., 2019; Wakefield et al., 2022). In the next section, we build on these three points to spell out more clearly the importance of social identity for SP.
A Social Identity Framework for Social Prescribing
As Stevenson et al. (2019) observe, the social identity approach set out in The New Psychology of Health (C. Haslam et al., 2018)—also known as the “social cure” approach (after Jetten et al., 2012)—provides a good starting point for a theoretical analysis of SP. A key reason for this is that, as we noted above, much of the practice of SP centres on efforts to help people join social groups (Wakefield et al., 2022), and we know from social identity research that, where these efforts are successful, this should generally have positive implications for people’s health. Research that supports this point shows, for example, that if a person is depressed, the likelihood of their depression relapsing 4 years later is halved (from 41% to 21%) if they join two community groups rather than none (when also controlling for health status and other relevant variables; Cruwys et al., 2013). Likewise, a retiree who is a member of two groups when they retire is at much lower risk of dying in the first 6 years of retirement if they continue to be a member of two groups rather than lose one group membership or both during this period (risk of mortality = 2%, 5%, and 12%, respectively, again while controlling for health status and other relevant variables; Steffens et al., 2016).
Importantly, too, the social identity approach also helps us to understand both when and why group memberships have a positive effect on health (see Figure 2). Formalising ideas that we have introduced in previous sections, it contends that group memberships are particularly important for health because they provide people with access to key social and psychological resources—particularly, self-esteem, a sense of control, meaning and purpose, as well as social support, belonging, and social connection (as suggested in the top portion of Figure 2; C. Haslam et al., 2018; Jetten et al., 2014, 2017). However, as we have argued, social identity theorising makes it clear that people will only be able to access these resources if the groups in question are ones that they (come to) identify with, so that they have been internalised as part of a valued social identity (in ways that lead groups and their members to be perceived and experienced as “us”; S. A. Haslam, 2014; S. A. Haslam et al., 2017). In the context of SP, these arguments can be formalised in the following two hypotheses:
H1: Social prescribing will be more beneficial for people’s health and well-being when it helps them to join social groups.
H2: In order for people’s health and well-being to benefit from social prescribing, the groups that they join need to be ones they will identify with—so that the groups provide them with a sense of social identity.
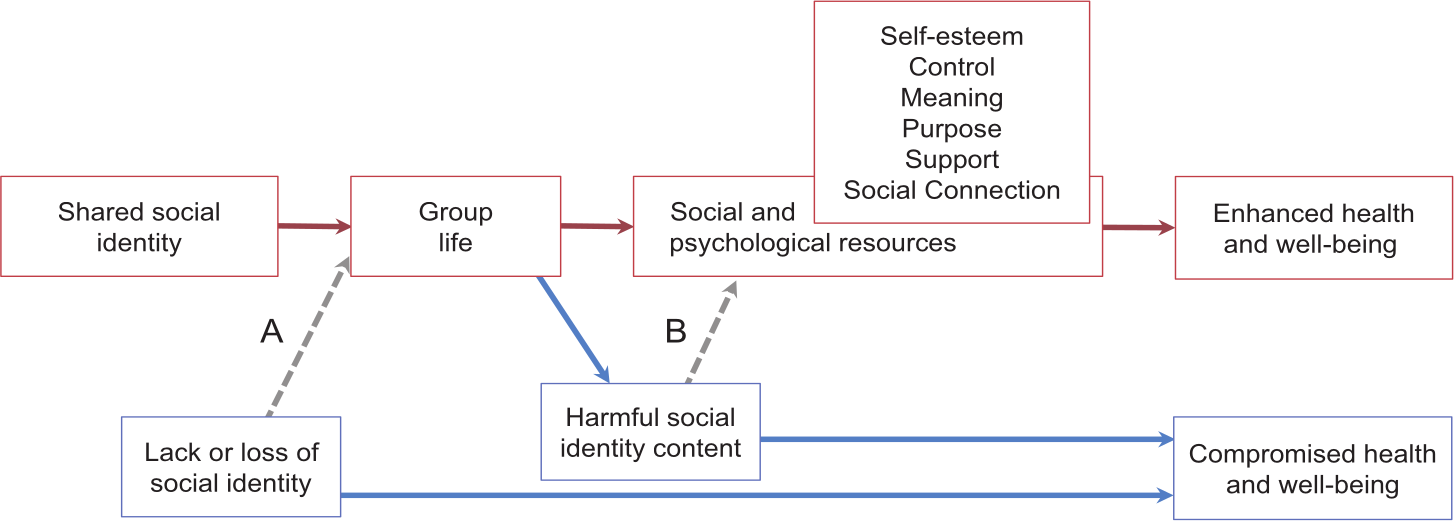
Social identity as a basis for group life, social and psychological resources, and health.
In many ways, these hypotheses simply formalise what practitioners typically try to achieve through SP—namely to connect people to groups in the community that they will find meaningful (Wakefield et al., 2022). At the same time, though, they alert us to several nuances in this process that SP needs to be attuned to. The first is that, in order for SP to be effective, what matters most is not that the group itself is inherently meaningful (although this may be important), but that the group is subjectively meaningful for would-be participants. It may be tempting, for example, to send a person off to a Men’s Shed or to take part in Parkrun because those groups are thriving in a local community; but if a client is not able to connect psychologically with the group and its activity—and ultimately sees their members as “them” rather than “us”—then the group is unlikely to provide a pathway to reduced loneliness or improved health. Indeed, on the contrary, the experience of being “forced,” or even encouraged, to join a group that you do not particularly like or do not see yourself to be a part of is likely to be alienating and counterproductive, and may ultimately result in disengagement or nonattendance (Stuart et al., 2022). Accordingly, if this is part of people’s experience of SP (which it sometimes is; see Stuart et al., 2022), then we would not expect it to be particularly effective.
A second nuance is that, while joining meaningful groups will generally increase a person’s sense of social connectedness, whether or not this has positive implications for their health and well-being will depend on the nature of the group itself (as suggested in the bottom portion of Figure 2; La Rue et al., 2023). In particular, if the content of the group’s identity is stigmatising (Crabtree et al., 2010) or centres on harmful or unhealthy norms (Dingle et al., 2015; Howell et al., 2014; Tarrant et al., 2011), then the group is less likely to provide a straightforward pathway to good health (although it may still be somewhat beneficial, for example, in providing support and a sense of agency and belonging; Postmes et al., 2019). In the former case, this is because the group has the capacity to amplify a person’s sense of rejection (e.g., as someone suffering from a mental health problem); in the latter, this is because the group may amplify unhealthy behaviour (e.g., excessive alcohol consumption, substance misuse, or excessive dieting). Sometimes, too, the group can become a target of problematic behaviour on the part of other groups (e.g., abuse; Këllezi et al., 2021).
A third nuance relates to the fact that, while H1 and H2 are relevant to all three tiers of SP (community interventions, targeted programmes, and facilitated interventions; see Figure 1), these social identity dynamics are likely to play out differently in each tier and to have different drivers—reflecting each tier’s status as incidental upstream processes or purposive downstream ones. This is the basis for two additional hypotheses that relate differentially to the three tiers.
Upstream, much will depend on how many preexisting groups there are in a given community for people to join—that is, whether the social infrastructure and the social identity capital that arises from it is abundant or depleted (Fried, 2020; C. Haslam, Steffens et al., 2019; Putnam, 2000). It will also depend on whether those groups are ongoing and nonstigmatising. An obvious point here, too, is that, in the event that this capital is depleted (e.g., as a result of social upheaval or policy change; Becker et al., 2021; Fong et al., 2019), then the downstream problems of loneliness and disconnection are likely to be more pronounced in ways that will increase demand for more personalised interventions and may place a strain on the resources needed to support them (Poole & Huxley, 2024). This is the basis for a third hypothesis:
H3. Incidental social prescribing will be effective (and reduce the need for purposive social prescribing) to the extent that people have ongoing access to social-identity-supporting and nonstigmatising social infrastructure within a given community.
In contrast, when it comes to downstream purposive forms of SP, much will depend on the nature not only of the groups that people join but also of the relationship that social prescribers have with their clients. As Husk et al. (2019) note, this reflects the fact that SP centres on “a series of relationships, between referrer and patient, patient and link worker, link worker and activity and patient and activity, all of which need to function to meet patient need” (p. 319; see also Brandling & House, 2009; Sharman et al., 2022). In this regard, a further contribution of the social identity approach is to recognise that, ideally, these relationships also have a sense of shared social identity at their core (S. A. Haslam, Steffens et al., 2019). More specifically, the therapeutic alliance between prescribers and clients can be seen to reflect an evolving sense of social identity that these parties come to share, and which is a basis for their mutual respect and trust as well as for productive engagement in the SP process (Cruwys, Lee et al., 2023; see also Lee et al., 2021; Robertson et al., 2023a, 2023b). Indeed, in psychotherapeutic contexts, Cruwys, Lee et al. (2023) found that social identification accounted for between 49% and 63% of the variance in therapeutic alliance. More formally, then, we can hypothesise that:
H4. Purposive social prescribing will be more effective to the extent that it is built around a social-identity-based therapeutic alliance between clients and prescribers.
Research relating to this fourth hypothesis alerts us to the fact that, as we noted above, social identity—and the sense of connection that it is a basis for—is relevant not only for health processes but also for organisational ones. This is an observation that has general relevance to SP as an organisational activity, but it alerts us to the fact that the processes described above are not simply “given,” but actively negotiated and managed. This means that social prescribers and those others who are broadly involved in SP (e.g., service providers, group facilitators) themselves need to engage in identity leadership in order to build and shape the social identities that give rise to positive SP outcomes (S. A. Haslam et al., 2011, 2023; Steffens et al., 2014).
As expounded in The New Psychology of Leadership (see Table 1; S. A. Haslam et al., 2011), this identity leadership has four main forms: (a) identity entrepreneurship in which the leader (i.e., the social prescriber) crafts a sense of shared identity with and for clients in ways that create “a sense of us” (Reicher et al., 2005); (2) identity prototypicality in which they embody a sense of shared social identity and are thereby seen as “one of us” (Hogg, 2001; Turner & Haslam, 2001; see also Davies et al., 2024); (3) identity advancement in which they promote the interests of shared identity and so are seen to be “doing it for us” (S. A. Haslam et al., 2001); and (4) identity impresarioship in which they devise structures and activities that sustain a sense of shared social identity and thereby “make us matter” (Haslam et al., 2011). Putting these things together, then, we hypothesise that:
H5. Social prescribing will be more effective to the extent that social prescribers engage in identity leadership to create, represent, advance, and embed group memberships that provide their clients with a sense of social identity.
Table 1 provides examples of what these different forms of identity leadership might look like at the three different tiers of SP. Again, we can see from this that the specific form that identity leadership will take (and need to take) depends very much on the particular form of SP that is being undertaken and the specific social identities in question. On the one hand, these relate to the nature of the intervention, targeted population, and treatment group; on the other hand, they relate to the nature of the groups that are being joined.
Examples of identity leadership at different tiers of the social prescribing landscape.
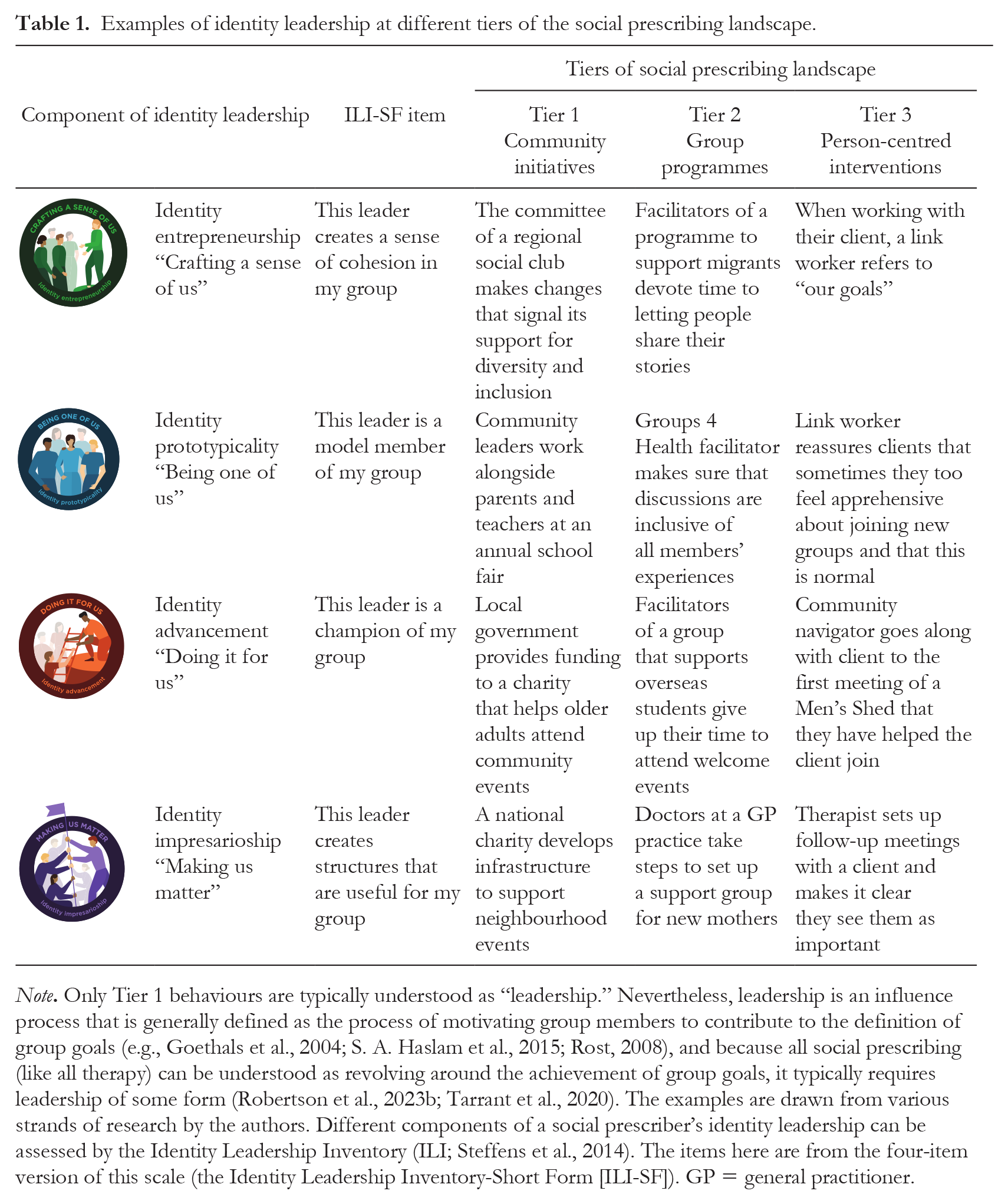
Note. Only Tier 1 behaviours are typically understood as “leadership.” Nevertheless, leadership is an influence process that is generally defined as the process of motivating group members to contribute to the definition of group goals (e.g., Goethals et al., 2004; S. A. Haslam et al., 2015; Rost, 2008), and because all social prescribing (like all therapy) can be understood as revolving around the achievement of group goals, it typically requires leadership of some form (Robertson et al., 2023b; Tarrant et al., 2020). The examples are drawn from various strands of research by the authors. Different components of a social prescriber’s identity leadership can be assessed by the Identity Leadership Inventory (ILI; Steffens et al., 2014). The items here are from the four-item version of this scale (the Identity Leadership Inventory-Short Form [ILI-SF]). GP = general practitioner.
Nevertheless, as indicated in Figure 1, there are two general ways in which identity leadership will vary across different tiers of SP. First, in higher (upstream, incidental) tiers of SP, the social identities that leaders need to build and work with will generally be broader and more inclusive than those in lower (downstream, purposive) tiers. More specifically, Tier 1 community initiatives will often involve leader–member alliances that encompass whole communities (Best et al., 2014; Dingle, Haslam et al., 2019), while Tier 2 programmes will often revolve around large- to medium-sized therapy and practitioner groups (Borek et al., 2019; Robertson et al., 2023a), and Tier 3 facilitated interventions may centre on two-person practitioner–client dyads (which will ideally still entail a sense of shared social identity; Cruwys, Lee et al., 2023).
Second, different aspects of identity leadership are likely to be more important at different tiers, and these will need to be performed by people who occupy different roles—although only Tier 1 roles may customarily involve people who are formally identified as “leaders” and be understood as requiring “leadership” (Morse et al., 2022). More specifically, at this tier, identity impresarioship and identity entrepreneurship are likely to be particularly important because there is a need for community and civic leaders to initiate structures and devise activities that bring large and often quite disparate groups of people together (see e.g., Këllezi et al., 2021). At Tier 2, structures and activities will often be predetermined (e.g., as manualised features of the programme being undertaken; C. Haslam et al., 2024), but, here, identity entrepreneurship and identity advancement are likely to be especially important as there is nevertheless a need for programme facilitators to make groups meaningful for participants and to ensure that they progress (Robertson et al., 2023a; Tarrant et al., 2020). Finally, at Tier 3, the identity advancement and identity prototypicality of individual social prescribers (e.g., link workers) will be particularly important because here there is a need for them to create a sense of psychological connection with individual clients and to win their trust (Bibic, 2023; Sharman et al., 2022; Stuart et al., 2022). That said, differences in the patterning of identity leadership across different tiers are likely to only be a matter of degree. Indeed, there is a good case for believing that all forms of identity leadership have an important role to play in all tiers of SP.
Support for the Social Identity Framework for Social Prescribing
Although SP research is in its infancy, there is already a large amount of empirical evidence that supports the above hypotheses either directly or indirectly. There is particularly strong support for H1 and H2—with a large number of studies finding both that people’s mental health is improved through interventions that serve to build a sense of social identity, and that these effects are more pronounced to the extent that participants come to identify with the groups at the heart of these interventions. This trend was observed in a meta-analysis of 27 intervention studies conducted by Steffens et al. (2021). Importantly, too, some of these studies were specifically focused on reducing loneliness. Primary amongst these were studies testing the efficacy of Groups 4 Health (G4H)—a five-module programme informed directly by social identity theorising and designed specifically to tackle problems of social disconnection and loneliness by helping people to build (or rebuild) meaningful group memberships and associated social identities (C. Haslam et al., 2024).
Three phases of clinical trials with people who are suffering from loneliness have confirmed the efficacy of G4H as a Tier 2 group programme. In particular, the programme has been shown to reduce participants’ loneliness (as well as their social anxiety and depression) relative to (a) a matched no-treatment control group (C. Haslam et al., 2016), (b) a randomised control group of people receiving treatment as usual for mental health conditions (C. Haslam, Steffens et al., 2019), and (c) a randomised control group taking part in a gold-standard clinical intervention for depression (group cognitive–behavioral therapy [CBT]; Cruwys, Haslam, Rathbone, Williams, et al., 2022). Speaking to the fact that group memberships are an enduring source of resilience (Muldoon et al., 2021), these benefits generally prove to be more sustained for
Providing further support for H1 and H2, there is evidence that Tier 1 community interventions are also more effective in reducing loneliness to the extent that they help people to participate in, and build social identification with, wider community groups. In Australia, for example, Fong et al. (2021) found that Neighbour Day activities that brought neighbours together to participate in community events, helped to build a sense of place-based social identification, which resulted in reduced loneliness and increased social cohesion. The study also found that the benefits of social-identity-based connection were sustained for at least 6 months after the intervention and protected residents who were isolated as a result of COVID-19 lockdowns (relative to residents in a no-intervention control; Cruwys, Fong, et al., 2022). Such findings accord with those of a host of studies pointing to the mental health benefits of community-based programmes that provide members of the general public—many of whom may be at risk of loneliness—with opportunities to participate in group activities (e.g., sport, music, and hobbies; Chatterjee et al., 2018) and thereby acquire new social identities (Dingle et al., 2013, Dingle, Clift et al., 2019; Ford et al., 2015).
Similar conclusions emerge from studies that have focused on Tier 3 forms of SP in which specialist social prescribers (e.g., link workers) work with individual clients to source group activities for them to take part in (e.g., Cruwys et al., 2018). In particular, studies by Këllezi et al. (2019), Wakefield et al. (2022), and Sharman et al. (2023) point consistently to the effectiveness of client-focused forms of SP that help people to join groups which they find meaningful. For example, in the largest of these studies, Wakefield et al. (2022) found that the effectiveness of SP in improving health-related quality of life was linked to its capacity to help participants become members of groups that provided them with a sense of community belonging, and thereby increased their access to social support while also reducing their loneliness. Importantly, too, within the same SP pathway, group memberships, community belonging, and associated reductions in loneliness also predicted reductions in primary care usage. As one of Këllezi et al.’s (2019) participants put it: You’re kind of helping each other, because I think for most people . . . you kind of feel that you’re the only person on the whole of Planet Earth, you know. . . So the fact that you can meet up with others is like, oh, there are other people that understand and know how it’s difficult . . . and so, you were able to give each other encouragement or copy each other or learn from each other. (Këllezi et al., 2019, p. 6)
These Tier 3 studies also provide support for H4 in showing that the relationships that clients and participants form with social prescribers are critical for programme success. In particular, this is a key conclusion of Sharman et al.’s (2023) SP research, which found that these emergent relationships were a significant positive predictor of both the strength of connection that clients reported having with the groups they were encouraged to join, and their reduced loneliness. Speaking to the fact that this relationship was bi-directional and centred on shared identity and understanding, link workers in this same programme of research also believed that their ability to forge bonds with clients was critical for the success of SP (Sharman et al., 2022; see also Këllezi et al., 2021).
In the context of making these observations, Sharman et al.’s Tier 3 research also supports H5—concerning the importance of identity leadership for SP—in suggesting that rather than just being given, identity-based relations between social prescribers and their clients are ones that those prescribers play an active role in building. Accordingly, the predictive power of these relationships was something that strengthened over the course of SP rather than something that was evident from the outset (Sharman et al., 2023). This conclusion is also supported by Clarke et al.’s (2023) and Guerrini et al.’s (2023) longitudinal investigations of Tier 2 SP associated with a large network of Men’s Sheds across Western Australia. In line with H1 and H2, these studies showed that members of Men’s Sheds who identified more strongly with their Shed enjoyed a stronger sense of social connectedness and higher levels of support giving, and, in turn, reported less loneliness as well as greater well-being and lower depression. In line with H5, Clarke et al. (2023) found that Shed leaders’ identity leadership (as assessed by the Identity ILI-SF) had a key role in cultivating social identification, which was associated with stronger social networks (close and supportive friends) within the shed and, in turn, higher well-being, lower depression, higher meaning in life, and lower loneliness. Similar conclusions emerge from research on the role that fitness instructors’ identity leadership plays in fostering the identification and engagement of gym attendees (Steffens et al., 2019; Stevens et al., 2020, 2022).
Yet, despite the fact that previous research provides reasonably good support for H4 and H5, it is clear that evidence supporting these hypotheses is not as extensive or robust as that which supports H1 and H2. As the gap in the above review of evidence suggests, it is apparent, too, that there is little or no research that has directly tested H3 (concerning the importance of social-identity-supporting social infrastructure for a given community). In part, as we noted earlier, this reflects the fact that most of the focus for SP is on Tier 2 and Tier 3 activities. Bringing this hypothesis into the frame is therefore an important way to broaden our understanding of SP and of the different ways in which communities might deliver it effectively. Indeed, we agree with Brandling and House that: On the face of it, empowering our communities to attend to some of our more intransigent health problems seems to be an obvious approach and is in line with stated government policy, including joint projects between health and social care. Building social capital and community cohesion is health-generating and so may help to create a virtuous circle. We could even take social prescribing to mean treating society as the patient for whom we prescribe. (Brandling & House, 2009, p. 455)
Yet, as with H4 and H5, H3 clearly needs to be fully and properly tested. It should be recognised, though, that our need for more evidence to support these hypotheses in part also reflects the challenging nature of SP research and the fact that high-powered, high-quality studies are extremely difficult to conduct, not least due to the inherent complexity of the SP programmes themselves (Cooper et al., 2022; Dingle et al., 2022). They are expensive too, but so are medical trials, and if we are serious about wanting to understand and unlock the life-saving health benefits of SP, then prioritising funding for this research is no less necessary.
Conclusion
SP has a long past as a general and incidental feature of the social and community landscape, but a short history as a specific purposive intervention with which to tackle loneliness and social disconnection (Husk et al., 2019). This means that, while there is a large corpus of research that provides general support for the hypotheses set out above (particularly H1 and H2; for reviews, see C. Haslam et al., 2018; S. A. Haslam et al., 2012), at present, there is only a relatively small amount of research that relates specifically to SP contexts. Nevertheless, as we have seen, this fledgling field already gives us good reason to believe not only that the social identity framework is theoretically and empirically sound, but also that it can be leveraged to design and deliver interventions that are feasible, appealing, and effective (Cruwys, Haslam et al., 2023), and to ensure the optimal utility of the entities and services that these interventions connect people to. At the same time, the framework can also inform muchneeded training both to deliver these interventions and services and to develop practitioner skills of identity leadership that shape and support clients’ social identities in ways that make all three tiers of SP more likely to be effective (e.g., S. A. Haslam et al., 2023).
Certainly, we might wish for a world in which these skills were not needed because SP would occur naturally as an incidental feature of a well-functioning and well-connected society. But that is a world that is increasingly distant for many people—particularly those who are economically and politically marginalised (Këllezi et al., 2021; Marmot, 2005, 2015; Wilkinson & Pickett, 2009). Accordingly, the need for SP is increasingly pressing, as is the need to ensure that we get this right. Indeed, unless we get this right, there is a strong possibility that SP could accentuate rather than ameliorate social disconnection and disadvantage—notably by offering only individual-focused solutions to what are often collective-level problems (Bingley et al., 2023; Chater & Loewenstein, 2023; Moscrop, 2023).
Having a strong theoretical framework to guide practical activity would seem to be a prerequisite for making progress in the design, delivery, and development of SP (Cooper et al., 2022; Stevenson et al., 2019). The principal contribution of the present paper is to provide a blueprint for such a framework. Although the details of this framework are very much in need of being tested and refined, this would therefore seem to be a step in the right direction. Ultimately, though, how big and how useful this proves to be is for others to discover and judge after having taken further steps along the same path. For now, our primary hope is that we have made the case that this is a good path to pursue—and one that we can all pursue together.
Footnotes
Correction (September 2024):
Article updated to correct the author byline to include author ‘Tarli Young’. Please see <https://doi.org/10.1177/13684302241284453> for more details.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.