
Abstract
Advocates for the use of specific labels to describe persons with disabilities presume that these labels fundamentally shape lay conceptions of persons with disabilities, and are thus critical targets for intervention. In two studies (N = 285) we test this presumption, by presenting participants with descriptions of persons with disabilities that use either person-first labels or condition-first labels; disability diagnoses were either made at birth or during the teenage years. For each description, participants judged how essential (consistent, deeply-rooted, broadly-ramifying) physical, sensory, or cognitive disability symptoms (Study 1) or diagnoses (Study 2) are to that person. Across both studies, participants judged disabilities to be equally essential to persons regardless of how they were labeled; this was robust whether diagnoses were made earlier or later in life. Although there may be other points of influence, these labels, which are primary targets of advocacy groups, do not seem to influence psychological essentialism of disabilities.
Persons with disabilities constitute the United States’ largest minority, including 26% of adults (Centers for Disease Control and Prevention [CDC], 2020a). According to the Centers for Disease Control and Prevention (CDC) Centers for Disease Control, a disability is “any condition of the body or mind (impairment) that makes it more difficult for the person with the condition to do certain activities (activity limitation) and interact with the world around them (participant restrictions)” (CDC, 2020b, para. 1). Persons with certain disabilities are often targets of discrimination (Equality and Human Rights Commission, 2020), which adds to the psychological toll that those disabilities already convey (National Alliance on Mental Illness, n.d.). Organizations interested in enhancing public understanding of and empathy towards persons with disabilities (e.g., Best Buddies International, National Association of Councils on Developmental Disabilities, Employer Assistance and Resource Network on Disability Inclusion) have for decades prescribed language to use when referring to folks with disabilities—namely, either person-first labels or condition-first labels—despite the type of disability or when it was diagnosed. Rules favoring one sort of label over another have been adopted by medical societies and the editors of writing style guides (Gernsbacher, 2017). Although recent work has identified how individuals with disabilities would personally like to be labeled (Darling & Heckert, 2010; Forber-Pratt & Zape, 2017; Hahn & Belt, 2004; Jones, 2012; Phelan & Kinsella, 2014), little work has examined how these same labels influence how laypersons conceptualize folks with disabilities. We examine how labels for persons with disabilities diagnosed early or later in life—containing either person-first or condition-first language—influence these lay conceptions.
Person-first Language and Condition-First Language Movements
Many in the disability community prefer to be identified by characteristics other than their disabilities (Forber-Pratt & Zape, 2017; Hahn & Belt, 2004; Jones, 2012; Phelan & Kinsella, 2014). Perhaps inspired by this, The “Person First Language” movement, originating in the 1980s, encourages others to think about people with disabilities as people first, and to reflect it in their language by putting the “person” before the disability; e.g., “person with Autism” (Texas Center for Disability Studies, 2017). Champions of this movement contend that person-first language should be a default (Collier, 2012). Prominent disability rights advocate, Emily Ladau (2015), explains: “Person-first language (PFL) was adopted as a general linguistic rule, moving from use by the people who initiated the movement towards heavy use by those in professional spheres . . . everyone was told that they should only use PFL” (para. 4).
Initial studies to examine the effects of person-first language have typically pitted it against de-humanized language—e.g., “person with psychosis” versus “psychotic”—in predicting treatment of those persons. There was little to no effect of person-first language on negative reactions (St. Louis, 1999), or inconsistent effects across subscales and participant pools (Granello & Gibbs, 2016). In contemporary parlance, de-humanizing labels are much less prominent and labels acknowledging personhood are much more common (Gernsbacher, 2017), but debate continues concerning where to place the “person” in disability labels—first (e.g., person with Autism) or last (e.g., Autistic person). Indeed, many individuals and communities—such as Blind, Deaf, or Autistic persons—have opposed the person-first movement (Brown, 2011; Vaughn, 1997), arguing instead for the use of condition-first language (e.g., “Blind person” or “Autistic person”) because it contributes to and reflects their group identity and belonging (Foreman, 2005). Prominent Autistic advocate, Lydia Brown (2011), explains: It is impossible to affirm the value and worth of an Autistic person without recognizing his or her identity as an Autistic person. Referring to me as a “person with Autism” or “an individual with ASD” demeans who I am. (para. 15)
Essentialism
One of the most likely ways in which labels might influence how persons with disabilities are conceptualized is in how essential their disabilities are believed to be. Essentialism is the idea that natural kinds have deep, hidden, unique essences that make them what they are and that distinguish those beings from other kinds (Gelman, 2003). Essentialism is implicated in much of our social categorization, where social groups (like categories of race and gender) are perceived as akin to natural kinds (Bogart et al., 2019; Gelman, 2003; Gelman et al., 2007). Disability—along with gender, race, and ethnicity—is one of the most essentialized of human categories (Prentice & Miller, 2007). Past work has found that traits and psychological characteristics are also essentialized, with the degree of essentializing influenced by a number of factors (Haslam et al., 2004; Haslam & Ernst, 2002; Haslam & Levy, 2006; Haslam et al., 2002). Labels can imply categorization, which can invoke essentialism (Gelman, 2004; Gelman & Heyman, 1999). The idea that labels might convey information about essences motivates person-first and condition-first language advocates: Person-first language seeks to acknowledge the inherent and equal value of every individual, before attaching any other descriptors or identities the person may view as secondary or not intrinsic . . . Some believe autism is inherent to their core identity and therefore find no exclusion in being called autistic. (Foley & Graff, 2018, paras. 2, 10)
Thus, we examine how language used to describe persons’ disabilities influences laypersons’ essentializing of those disabilities; in other words, lay beliefs about the extent to which disabilities are core to disabled persons. Based on past work (discussed earlier) on disability and identity, we selected three dimensions of essentialism to measure in the current studies: consistency (how consistently particular characteristics are displayed), inherence (how deeply-rooted particular characteristics are to identity), and informativeness (how broad the ramifications of particular characteristics are to identity). Given prior findings, these three dimensions seemed most susceptible to potential effects of disability label and timing (Bastian & Haslam, 2006; Haslam et al., 2000, 2002, 2004). Labels in which the defining feature comes first, as in condition-first labels, are more likely to suggest stability, an aspect of essentialism (Gelman, 2004; Gelman & Heyman, 1999). Moreover, Reynaert and Gelman (2007) found that references to novel illnesses using single nouns (“He is a baxtermic”) implied more permanence than illnesses referred to with possessive phrases (“He has baxtermia”). Thus, we hypothesize that disabilities described with condition-first labels (e.g., “Mike is a Daxic person”) will be essentialized more than disabilities described using person-first (possessive) labels (e.g., “Mike is a person with Daxism”).
Time of Diagnosis
We also investigate the effect of disability diagnosis timing on how laypeople essentialize disabilities. Language movements (discussed earlier) have not specifically focused on disability diagnoses acquired at birth vs. later in life, even though diagnosis timing may convey information about the inherence or informativeness of a disability and may make a difference in essentializing. Bogart et al. (2019) found that individuals with congenital disabilities (e.g., “born with paralysis from the waist down”) were essentialized more than those who acquired the same disability later in life (e.g., “became paralyzed from the waist down as a teenager”). In the current studies, we manipulate the timing of disability diagnoses—whether they were identified at birth or identified later in life. We chose to manipulate the timing of “diagnosis,” as opposed to “disability onset,” because “onset” is a more ambiguous term. Scientists and clinicians might disagree about when a disability “onset” occurs or how it manifests. For some, “onset” might begin with changes in behavior, cognition, or perception that are within the “typical” range; whereas others might consider “onset” the moment when one experiences trauma or experiences changes outside of the “typical” range. Laypersons might also have their own definitions of “onset,” and those definitions may vary. Drawing upon the findings of Bogart et al. (2019), we hypothesize that disability diagnoses identified at birth will be essentialized more than diagnoses identified in the teenage years. Manipulating timing also allows us to test for the robustness of any effects of label—whether such effects exist across disabilities identified earlier and later in life.
The Current Studies
The current studies examine whether person-first vs. condition-first labels differentially affect how people essentialize disabilities. Disabilities can be complex and multi-faceted—they may involve physical, sensory, and cognitive deficits. As well, different folks with a certain disability diagnosis may have different collections of symptoms. Past work (discussed earlier) suggests that individual disability symptoms may be essentialized to different extents. Thus, in Study 1, we evaluate the effects of labeling and diagnosis timing on how laypersons essentialize individual disability symptoms, including physical, sensory, and cognitive symptoms. We also evaluate labels’ influence on the breadth of essentializing: how labels used to introduce one disability (e.g., a physical disability) may influence participants’ essentializing of other abilities (e.g., sensory or cognitive) and personality characteristics (e.g., compassion and generosity). In Study 2, we evaluate how such labels influence laypersons’ essentializing of novel diagnoses for disabilities that primarily affect physical, sensory, or cognitive functioning. To control for participants’ knowledge of particular disabilities and to gauge how labels and diagnosis timing influence persons’ concepts of new disabilities, participants reasoned about disabilities with novel names. Use of novel names mimics circumstances in which persons are first encountering and coming to understand a disability.
Study 1
Method
All recruitment procedures, inclusion/exclusion criteria, and methods were pre-registered (https://aspredicted.org/2S6_W33).
Participants
Participants (N = 167, 95 men, 72 women) ranging from 22 to 70 years in age (M = 38.40 years) were recruited online through Amazon’s Mechanical Turk. Participants also had the option to identify with neither gender (n = 0). In accordance with our pre-registered plans, additional participants (n = 43) were excluded if one or more of the following was true: they completed the study in less than 5 minutes (it is exceptionally difficult to thoroughly read all of the instructions and questions in fewer than 5 minutes; n = 7), they took more than 45 minutes to complete the study (suggesting that they might have been distracted; n = 1), they did not correctly answer at least 3 of 4 basic reading/attention-check questions (suggesting that they were either not attentive or a bot; n = 32), or they did not pass any of three checks to ensure that they reside in the United States (n = 23). Unrelated to our pre-registration criteria, an additional 13 participants were excluded due to typographical errors in the Qualtrics form (later corrected). Ultimately, we recruited 3 participants beyond our initial goal, and we decided to retain, rather than discard, their data.
Research has demonstrated that samples recruited from Amazon’s Mechanical Turk are often more diverse than commonly recruited U.S. undergraduate samples (e.g., Burchmester et al., 2011). Of the participants in the final sample, 42.5% (n = 71) completed a Bachelor’s degree, 31.1% (n = 52) completed “some college,” 16.8% earned a high school diploma (n = 28), 7.8% earned a Master’s degree (n = 13), and 1.2% earned a Doctorate (n = 2). Most of the participants (85%; n = 142) identified as “White/Caucasian,” followed by 9.6% (n = 16) as “Black/African American,” 9% (n = 15) as “Latinx,” 4.8% (n = 8) as “Asian/Asian American,” 2.4% (n = 4) as “Native American,” and 1.2% (n = 2) as “Other.” These categories were not mutually exclusive; participants could select more than one. Participants were also asked about the frequency of their relationships with persons with disabilities: 45.5% (n = 76) of participants reported having “one or two” relationships, 37.7% (n = 63) reported no relationships, 15% (n = 25) reported “a few,” and 1.8% (n = 3) reported “a lot.” Participant recruitment, consent, and all study procedures were approved by Vanderbilt University’s Institutional Review Board (IRB #201401).
Our goal was to recruit a sample large enough to fulfill the requirements of an a priori power analysis (using G*Power 3.1; Faul et al., 2007) for ANOVAs that included label (2 levels, between-subjects), time of diagnosis (2 levels, between-subjects), and character disability type (3 levels, within-subjects). There is no between-between interaction option in G*Power 3.1, so we ran this analysis with 4 groups to estimate what that analysis might yield in a repeated-measures ANOVA. The analysis determined that we required a minimum of 164 participants to detect medium effect sizes (fs ⩾ .25; Cohen, 1992) with statistical power ⩾ .80 and α = .0125. We had planned to conduct four separate ANOVAS; as a conservative correction for potential Type 1 error, we divided the traditional alpha level (.05) by 4.
Procedure
The survey was delivered online; constructed and hosted using Qualtrics.com. Participants read a consent document in which the stated purpose of the survey was to understand how adults view personality and ability characteristics. They read that they would see brief descriptions of people and, following each description, answer questions about the impact of various personality or ability characteristics on that person’s life. Participants read that total participation time was typically 8 to 15 minutes (so that participants could opt to not proceed if they did not have that much time to afford). After participants read the consent document and reported demographic information, they were informed that the survey was available only to participants in the United States, and not to proceed if they do not live in the United States. Twenty-three non-U.S. participants still proceeded and were excluded on this basis later.
Before the presentation of the first description, participants were reminded that they would read about three different middle-aged people. We specified that the characters in the descriptions were “middle-aged” so that participants in the two diagnosis-timing conditions (infancy and the teenage years) would not hold systematically different assumptions about the current age of the characters. Participants read that, for each person, they would rate whether they agreed or disagreed with statements about that person’s characteristics, and were encouraged to read each description and question carefully. They were then prompted to check a box confirming that they agree to read each description and question carefully.
Participants were randomly assigned to one of four conditions: Person-first labels with diagnoses received at birth (n = 41), Person-first labels with diagnoses received during the teenage years (n = 45), Condition-first labels with diagnoses received at birth (n = 39), or Condition-first labels with diagnoses received during the teenage years (n = 42). Each participant proceeded through three blocks, presented in randomized order: a physical disability block, a sensory disability block, and a cognitive disability block. Each block began with a description of a person’s disability, according to the participant’s assigned condition. Disability descriptions can be found in the Supplemental Material. We created 8 novel diagnosis names by combining novel object names from the Novel Object and Unusual Name (NOUN) Database (Horst & Hout, 2015); these names can also be found in the Supplemental Material. For example, participants assigned to Person-first labels with diagnoses received at birth read the following about a character with a physical disability: “Chris is a person with Piskerism. People with Piskerism tend to experience challenges in their physical development, for example, their bodily strength and physical coordination. Chris has been diagnosed with Piskerism since birth.”
Below each vignette, participants were informed they would be asked about the person’s characteristics, one at a time. We reiterated the disability label and diagnosis timing to increase the salience of this information and participants’ retention of this information (e.g., “Remember, John is a Daxic person, diagnosed since birth”). For these reasons we also included the same diagnosis statements at the top of each page of questions; the purpose of the study was not to test participants’ memories and we did not want participants’ memories about the diagnoses to have faded by the time they rated later characteristics.
Participants read about one characteristic at a time. For example, after the diagnosis statement, they read, “Consider John’s EYESIGHT” and listed beneath were three statements that participants rated: 1) “John will display this characteristic consistently across very different situations” (Consistency), 2) “This characteristic is a deeply-rooted part of who John is as a person” (Inherence), and 3) “This characteristic has broad ramifications: it will influence many aspects of John’s life” (Informativeness). These measures were adapted from those used by Haslam et al. (2004), who studied personality characteristics; the language in the current study was simplified to avoid fatigue effects and modified so that it was appropriate to use in reference to personality and ability characteristics. Participants responded to each of these statements using a 5-item Likert scale ranging from strongly disagree (1) to strongly agree (5). Participants responded to these three statements for each of 8 characteristics: eyesight, hearing ability, bodily strength, physical coordination, comprehension, memory skills, compassion, and generosity.
Scoring
The key dependent variables are Physical Essentialism, Sensory Essentialism, Cognitive Essentialism, and Personality Essentialism. The Physical Essentialism variable was created by averaging across Consistency, Inherence, and Informativeness scores for Bodily Strength and Physical Coordination. The Sensory Essentialism variable was created by averaging across Consistency, Inherence, and Informativeness scores for Eyesight and Hearing Ability. The Cognitive Essentialism variable was created by averaging across Consistency, Inherence, and Informativeness scores for Comprehension and Memory Skills, and the Personality Essentialism score was created by averaging across Consistency, Inherence, and Informativeness scores for Compassion and Generosity. Each score could range from 1 to 5.
Results
Analyses were conducted to explore how the type of label used to describe a disability (person-first label vs. condition-first label), as well as the time of diagnosis (diagnosed since birth vs. the teenage years), influence the degree to which disability symptoms are essentialized. As well, analyses evaluate the breadth of essentializing: whether the type of label or the time of diagnosis used to describe a certain type of disability influence how people essentialize other abilities and personality characteristics. Descriptive data, per condition, are presented in Table 1.
Degree of essentializing physical, sensory, cognitive, and personality characteristics when a person-first (“Person”) vs. condition-first (“Condition”) label is used, and disability diagnoses are identified at birth (“Birth”) vs. in the teenage years (“Teen”).
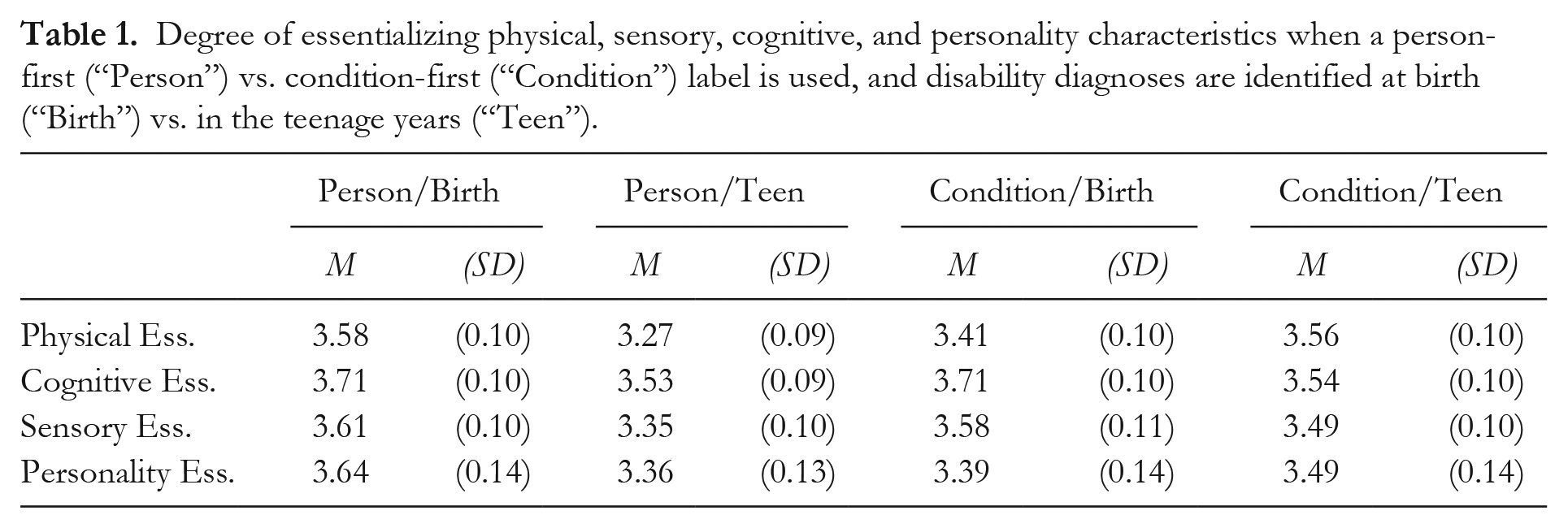
Four separate ANOVAs were conducted, one for each of the dependent variables: 1) Physical essentialism, 2) Sensory essentialism, 3) Cognitive essentialism, and 4) Personality essentialism. For the sake of conciseness and given that the results were consistent across all four analyses, we present them simultaneously. The 2 (LABEL: person-first label vs. condition-first label) × 2 (TIME OF DIAGNOSIS: since birth vs. teenage years) × 3 (DISABILITY: physical, sensory, cognitive) ANOVAs revealed no significant effects of Label (physical essentialism: F(1, 158) = 0.39, p = .53; sensory essentialism: F(1, 158) = 0.27, p = .60; cognitive essentialism: F(1, 158) = 0.01, p = .94; personality essentialism: F(1, 158) = 0.21, p = .65) or Time of Diagnosis (physical essentialism: F(1, 158) = 0.67, p = .41; sensory essentialism: F(1, 158) = 3.02, p = .08; cognitive essentialism: F(1, 158) = 3.25, p = .07; personality essentialism: F(1, 158) = 0.40, p = .53) on the degree to which participants essentialized characters’ disabilities. No significant interaction effects were found. Participants essentialized a disability to the same degree whether it was described with a person-first or condition-first label, and whether the diagnosis was identified at birth or in the teenage years. Additional analyses, located in the Supplemental Material, confirmed that this was the case for all three individual components of essentialism (Consistency, Inherence, and Informativeness).
There was, however, a significant effect of Disability on the degree to which participants essentialized characters’ disabilities for three of the four dependent variables: physical essentialism, sensory essentialism, and cognitive essentialism. Mauchly’s test indicated that the assumptions of sphericity had been violated (physical essentialism: χ2(2) = 27.52, p < .01; sensory essentialism: χ2(2) = 46.76, p < .01; cognitive essentialism: χ2(2) = 42.63, p < .01) so Greenhouse-Geisser corrections were used (physical essentialism: F(1.72, 158) = 32.45, p < .01, η2 p = .17; sensory essentialism: F(1.59, 158) = 25.51, p < .01, η2 p = .14. cognitive essentialism: F(1.62, 158) = 19.77, p <.01, η2 p = .11). As depicted in Figure 1, when participants read that a person had a disability diagnosis affecting their physical development, they essentialized physical characteristics (bodily strength and physical coordination) (M = 3.90, SE = 0.07) significantly more than when they read that a person had a diagnosis affecting sensory (M = 3.22, SE = 0.07) or cognitive development (M = 3.24, SE = 0.08), ps < .001. The same pattern emerged for sensory and cognitive disabilities. When a person had a disability diagnosis that affected their sensory development, sensory characteristics (vision and eyesight) (M = 3.96, SE = 0.07) were essentialized significantly more than when they had a diagnosis affecting physical (M = 3.27, SE = 0.08) or cognitive development (M = 3.29, SE = 0.09), ps < .001. Finally, when participants read a vignette where a person had a disability diagnosis affecting their cognitive development, they essentialized their cognitive characteristics (comprehension and memory skills) (M = 3.97, SE =0.07) significantly more than when a diagnosis affected sensory (M = 3.55, SE = 0.07) or physical development (M = 3.35, SE = 0.09), ps < .001. Thus, for all three types of disability (physical, sensory, cognitive), capacities directly compromised by that disability were judged to be more essential to disabled persons.
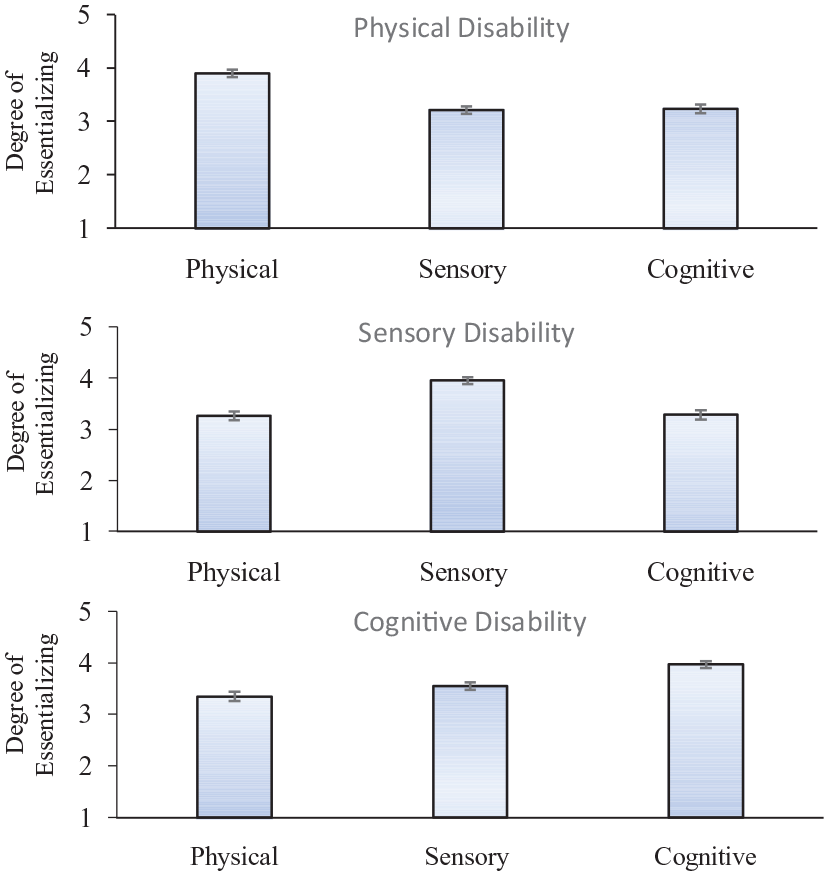
Degree of essentializing physical, sensory, and cognitive characteristics for a disability that affects either physical development, sensory development, or cognitive development.
Personality was essentialized to the same extent for all three disabilities, F(2, 158) = 1.58, p = .21. In sum, no disability was essentialized beyond its stated scope (i.e., physical disabilities affected essentializing of physical qualities, sensory disabilities affected essentializing of sensory qualities, and so on). There was no evidence of spillover.
Interim Discussion
In Study 1, the type of label used (condition-first vs. person-first) and the time at which a disability diagnosis was identified (at birth or as a teenager) did not significantly influence how laypersons essentialized disability symptoms. Additionally, we found no “spillover effects”—the capacities directly related to a particular type of disability (physical, cognitive, sensory) were essentialized significantly more than other capacities, regardless of which labels were used. Perhaps individual symptoms are interpreted as periphery to a person’s identity, whereas diagnoses are understood as more central (and thus essential) to people’s identities. If so, perhaps labels and timing might measurably influence how persons essentialize diagnoses; we test this possibility in Study 2. Our hypotheses regarding the effects of label and timing remained the same as in Study 1; however, hypotheses about breadth of essentializing were no longer relevant as we were no longer asking about individual symptoms.
Study 2
Method
All recruitment procedures, inclusion/exclusion criteria, and methods were pre-registered (https://aspredicted.org/VHJ_MBB).
Participants
Participants (N = 118, 67 men, 51 women) ranging from 21 to 64 years in age (M = 37.50 years) were recruited through Amazon’s Mechanical Turk; none had participated in Study 1. Participants also had the option to identify with neither gender (n = 0). In accordance with our pre-registered plans, additional participants (n = 9) were excluded if one or more of the following was true: they completed the study in more than 25 minutes (participants might have been distracted; n = 2), they did not correctly answer at least 3 of 4 basic reading/attention-check questions (suggesting that they were either not attentive or a bot; n = 5), or they did not pass any of three checks to ensure that they reside in the United States (n = 3). Ultimately, we recruited 2 participants beyond our initial goal, and we decided to retain, rather than discard, their data. Of the participants in the final sample, 47.5% (n = 56) earned a Bachelor’s degree, 25.4% (n = 30) completed “some college,” 16.1% (n = 19) earned a high school diploma, 5.9% (n = 7) earned a Master’s degree, and 3.4% (n = 4) earned a Doctorate. Most of the participants (79.7%; n = 94) identified as “White/Caucasian,” followed by 11% (n = 13) as “Latinx,” 10.2% (n = 12) as “Black/African American,” 10.2% (n = 12) as “Asian/Asian American,” 2.5% (n = 3) as “Native American,” and 3.4% (n = 4) as “Other.” These categories were not mutually exclusive; participants could select more than one. Participants were also asked about the frequency of their relationships with persons with disabilities: 53.4% (n = 63) of participants reported having “one or two” relationships, 31.4% (n = 37) reported no relationships, 12.7% (n = 15) reported “a few,” and 1.7% (n = 2) reported “a lot.” Participant recruitment, consent, and all study procedures were approved by Vanderbilt University’s Institutional Review Board (IRB #201401).
Our goal was to recruit a sample large enough to fulfill the requirements of an a priori power analysis for ANOVAs that included label (2 levels, between-subjects), time of diagnosis (2 levels, between-subjects), and character disability type (4 levels, within-subjects). The power analysis determined that we required a minimum of 116 participants to detect medium effect sizes (fs ⩾ .25; Cohen, 1992) with statistical power ⩾ .80 and α = .05.
Procedure
The procedure closely paralleled that of Study 1, with some key changes. The survey was again constructed and hosted using Qualtrics.com. Participants read a consent document in which the stated purpose of the survey was to understand how adults view diagnoses affecting ability. They read that they would later see a series of brief descriptions of people and, following each description, answer questions about the impact of various diagnoses on persons’ lives. Participants read that total participation time was typically 4 to 8 minutes (so one could opt to not proceed if they did not have time to afford). As in Study 1, after participants read the consent document and reported their demographic information, they were informed that the survey was available only to participants in the United States, and to not proceed if they do not live in the United States. Three non-U.S. participants still proceeded and were excluded on this basis later.
Before seeing the first description, participants were reminded that they would read about four different middle-aged people. Then, participants read that for each person, they would rate whether they agreed or disagreed with statements about that person’s diagnosis, and were encouraged to read each description and question carefully. They were then prompted to check a box confirming that they agree to read each description and question carefully.
Participants were assigned to one of four conditions: Person-first labels with diagnoses received at birth (n = 32), Person-first labels with diagnoses received during the teenage years (n = 29), Condition-first labels with diagnoses received at birth (n = 28), or Condition-first labels with diagnoses received during the teenage years (n = 29). Each participant proceeded through four blocks, presented in randomized order: a physical disability block, a sensory disability block, a cognitive disability block, and a block in which the type of disability was unspecified. We included an unspecified condition to investigate whether an effect of label or of timing exists when the “disability” in question is not constrained by a specific, limited set of symptoms. Each participant saw all four blocks, but the order in which the blocks were presented was randomized. Each block began by describing a person’s disability, according to the participant’s assigned condition. The physical disability, sensory disability, and cognitive disability descriptions were identical to those in Study 1. An example of the unspecified condition is as follows: “John is a person with Daxism. John has been diagnosed with Daxism since he was a teenager.”
As in Study 1, disability label and diagnosis timing were reiterated below each description and at the top of each page of questions. After the diagnosis statement in Study 2, participants were asked to, “Consider John’s diagnosis” (rather than a specific characteristic, such as eyesight). The same three essentialism measures/statements were used as in Study 1, but the “diagnosis” was referred to instead of the “characteristic”: 1) “John will display this diagnosis consistently across very different situations” (Consistency), 2) “This diagnosis is a deeply-rooted part of who John is as a person” (Inherence), and 3) “This diagnosis has broad ramifications: it will influence many aspects of John’s life” (Informativeness). Participants responded to each statement using a 5-item Likert scale ranging from strongly disagree (1) to strongly agree (5). In total, each participant responded to 12 questions, 3 per diagnosis.
Scoring
The key dependent variable is Disability Essentialism: an average of the Consistency, Inherence, and Informativeness scores for each of four vignettes (physical disability, sensory disability, cognitive disability, unspecified disability). Scores could range from 1 to 5.
Results
Analyses were conducted to examine how the type of label used to describe a disability (person-first label vs. condition-first label), as well as the time of diagnosis (since birth vs. the teenage years), influence the degree to which disability diagnoses are essentialized. Descriptive data, per condition, are presented in Table 2.
Degree of essentializing physical, sensory, cognitive, and unspecified disability diagnoses when a person-first (“Person”) vs. condition-first (“Condition”) label is used, and disability diagnoses are identified at birth (“Birth”) vs. in the teenage years (“Teen”).
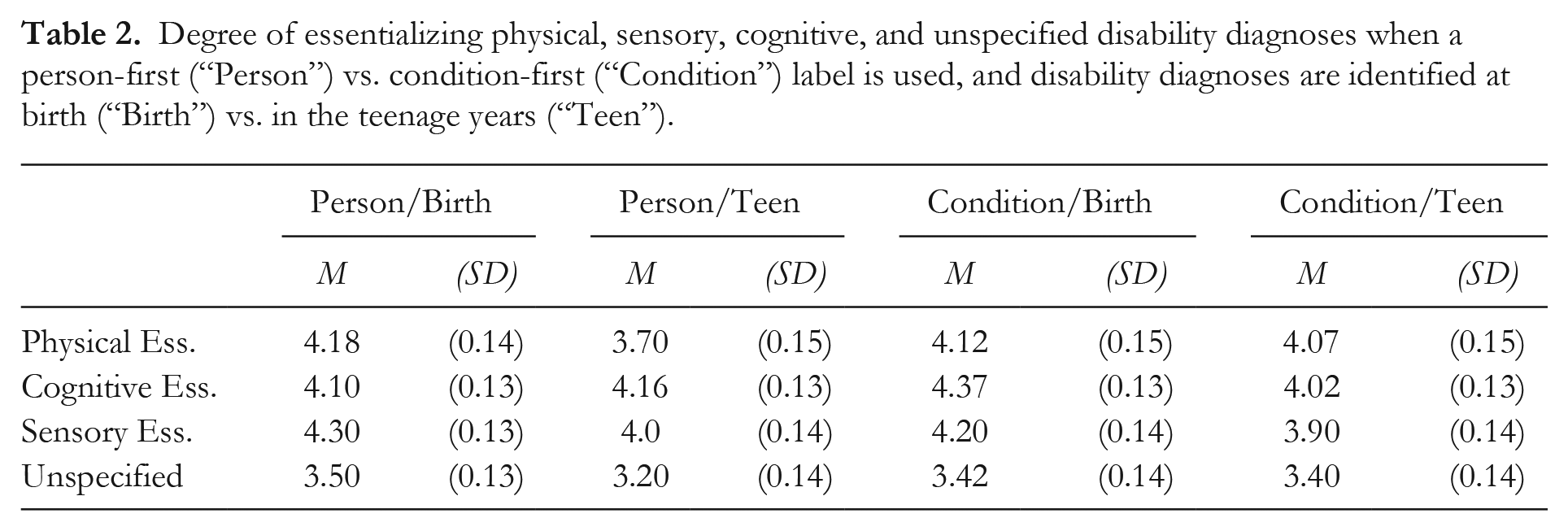
A 2 (LABEL (between-subjects): person-first label vs. condition-first label) × 2 (TIME OF DIAGNOSIS (between-subjects): since birth vs. teenage years) × 4 (DISABILITY (within-subjects): physical, sensory, cognitive, unspecified) ANOVA revealed no significant effects of Label, F(1, 114) = 0.45, p = .51., η2 p = .004, on the degree to which participants essentialized characters’ disabilities. Participants essentialized a disability to the same degree whether it was described with a person-first or condition-first label; this finding was consistent with that of Study 1. Additional analyses, located in the Supplemental Material, confirmed that this was the case for all three individual components of essentialism (Consistency, Inherence, and Informativeness).
There was, however, a significant effect of Time of Diagnosis, F(1, 114) = 5.41, p < .05, η2 p = .05, on the degree to which participants essentialized characters’ diagnoses; this finding was unique to Study 2. As depicted in Figure 2, when participants read that a disability diagnosis had been present since birth (M = 4.03, SE = 0.07), it was essentialized significantly more than when a disability diagnosis was identified in the teenage years (M = 3.80, SE = 0.08). That is, diagnoses present since birth were considered that much more “essential” (consistent, inherent, and informative) to a person’s being than diagnoses present since the teenage years. There were no significant interaction effects involving Label or Timing.
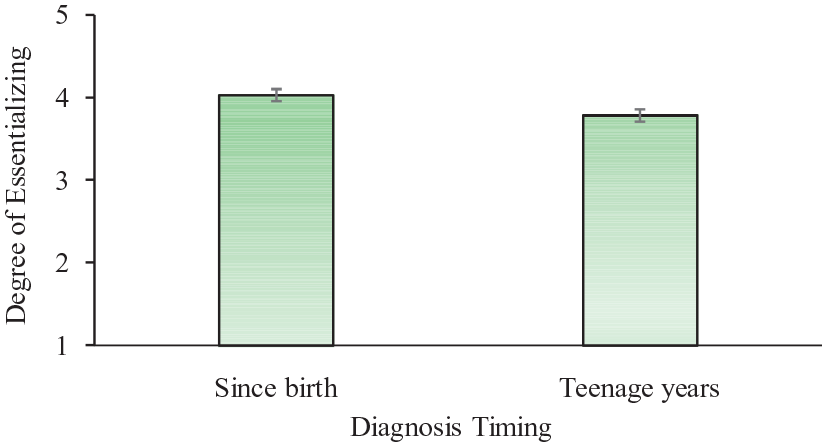
Degree of essentializing disabilities based on whether they were diagnosed since birth or in the teenage years.
Finally, as in Study 1, we found a significant effect of Disability. Mauchly’s test indicated that the assumption of sphericity had been violated, χ2(5)= 18.73, p < .001, so a Greenhouse-Geisser correction was used, F(2.73, 310.91) = 49.34, p < .001, η2 p = .30. As depicted in Figure 3, there was significantly less essentializing of “unspecified” disabilities (M = 3.36, SE =0.07) versus the three defined disability conditions (physical: M = 4.02, SE = 0.07, p < .001; sensory: M = 4.09, SE = 0.07, p < .001; cognitive: M = 4.15, SE =0.07, p < .001). Thus, when participants read a vignette in which no information was given pertaining to what a diagnosis affects, they judged the diagnosis as less “essential” to a person’s identity than when they were told that a diagnosis affects physical development, sensory development, or cognitive development.
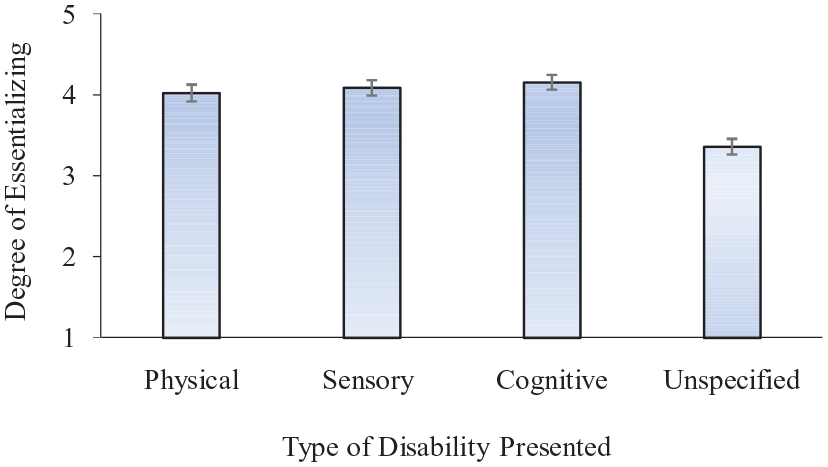
Degree of essentializing diagnoses of disabilities that have either physical, sensory, cognitive, or unspecified implications.
General Discussion
In these two studies, our primary goal was to investigate whether laypersons’ essentializing of disabilities differs depending on the labels used to describe disabilities; namely, person-first labels versus condition-first labels. Contrary to our predictions, participants’ essentializing of disabilities was unrelated to how those disabilities were labeled; participants judged persons’ disabilities to be just as consistent, inherent (deeply rooted), and informative to persons’ lives, regardless of what labels were used. This was true at the symptom level (Study 1) and at the diagnosis level (Study 2), and whether diagnoses were identified at birth or later in life. Interestingly, participants did essentialize specific characteristics more so when those characteristics were compromised by a disability (e.g., essentializing a person’s hearing more than other qualities when a person has a disability that affects their sensation), which suggests that non-normative capacities may be essentialized more so than typical capacities.
Our second goal was to investigate whether the time at which a disability diagnosis is identified (at birth vs. later in life) impacts the degree to which disabilities are essentialized. Diagnosis timing did not affect essentializing characteristics of disabilities (e.g., eyesight; Study 1), but timing did influence participants’ essentialism of diagnoses (Study 2)—diagnoses identified at birth were judged to be more essential than those identified later in life. These findings are consistent with other findings that earlier-identified diagnoses are more essentialized (e.g., Bogart et al., 2019). This effect of timing and the fact that disability-related qualities were essentialized more so than non-disability-related qualities make it unlikely that the null effects of labels are merely a function of participants’ potential inattentiveness or a function of the dependent variables lacking meaningful variability.
Medium effect sizes were the focus of our analyses because we were interested in practical, real-world effects of labeling. Hypothetically, had we detected minute effects of labeling, it is unclear how those effects would help to arbitrate the theoretical or practical issues at hand. Indeed, even medium or large effects found in controlled settings (such as the current studies) will typically amount to smaller effects in the real world where there are many other variables at play. We discuss some of these important variables in greater depth in the next section. Regardless, potential concerns about the current studies being under-powered should be alleviated by the fact that p-values for tests of Label were not remotely close to being significant at alpha levels of .0125 or .05—in Study 1, the p-values for the effects of Label were .53, .60, .94, and .65; in Study 2, the p-value was .51. In short, there is no evidence suggesting that a larger sample would have revealed significant effects of label in the current studies.
Future Directions
Essentialism was a feasible place to find differential effects of person-first versus condition-first language, and essentialism is often invoked by proponents of person-first and condition-first movements. Perhaps the use of these labels does influence other outcomes, such as disability-based bias or discrimination; topics that can be considered in future research. However, it is reasonable to predict that such labels would not influence these factors, given past work identifying essentialism as a mediator of bias and discrimination (Haslam et al., 2000; Lebowitz et al., 2014, 2016). It is conceivable that such labels influence inferences about other qualities of disabled persons, such as the breadth or richness of disabled persons’ lives—for example, perhaps person-first language (vs. condition-first language) induces greater consideration of qualities that are not closely tied to one’s disability (one’s individual personality, aptitudes, preferences, and so forth).
To limit the influence of participants’ existing knowledge of particular disabilities (and the extent to which they already essentialize those disabilities) we employed novel disability names in the current studies. Modeling the labels used for Autism Spectrum Disorder (ASD); “Person with Autism” vs. “Autistic person”, labels in the current studies were constructed in an “-ic” versus “-ism” format (i.e., “Person with Daxism” vs. “Daxic person”). Many disabilities will have unique person-first and condition-first constructions, and some disabilities will not have a “condition-first construction” (e.g., currently, we do not use the phrase “multiple sclerosis person”). Future work can explore whether other unique and subtle differences in label construction might matter in essentializing individual disabilities; for example, would persons essentialize a disability that affects communication more if a person is described as a “Nonverbal person” vs. a “Person who communicates with assistive technology”?
Conclusions
There is heated debate about whether person-first labels or condition-first labels should be the default when referring to persons with disabilities; with proponents on both sides highlighting how labels may shape social concepts. We found that participants in the current studies essentialized disability symptoms and disability diagnoses to the same extent whether disabilities were introduced with person-first labels or condition-first labels. This is not to say that labels cannot influence concepts of persons with disabilities in other ways—for example, it is still reasonable to hypothesize that de-personalized language once commonly used to refer to persons with disabilities (e.g., referring to someone as “an Autistic” vs. “an Autistic person”) influences concepts of disabled persons’ humanity. In the current studies, we had participants reason about novel disabilities, to minimize the influence of participants’ beliefs about real disabilities and labels. This method allowed for more precise comparisons of disability label format (person-first vs. condition-first), but it did not account for effects of the social contexts in which real disability labels are constructed and communicated. Real, existing disability labels may carry certain connotations and even new labels can acquire certain connotations over time. For example, if Daxism were to become a real disability, one label form (e.g., Daxic person) could culturally evolve to become derogatory and that label form may perpetuate negative conceptions of persons with that disability. However, our findings indicate that whether disability labels are condition-first or person-first does not, alone, influence the extent to which laypersons essentialize a newly-encountered disability.
Supplemental Material
sj-doc-1-gpi-10.1177_13684302231157990 – Supplemental material for Investigating the efficacy of prescribed labeling practices: Conceptualizing persons with disabilities
Supplemental material, sj-doc-1-gpi-10.1177_13684302231157990 for Investigating the efficacy of prescribed labeling practices: Conceptualizing persons with disabilities by Nicolette Granata and Jonathan D. Lane in Group Processes & Intergroup Relations
Footnotes
Ethical Approval
All study procedures were approved by Vanderbilt University’s Institutional Review Board (#201401).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.