
Abstract
Although stressors are common in group life, people cope better when group authorities treat them with care/concern. However, it remains unclear whether such treatment affects individuals’ physiological stress. In this experiment, individuals engaged in an interview known to increase cortisol (stress biomarker). Surrounding the interview, an ingroup supervisor treated them with standard professionalism (politeness [control]), explicit care/concern (high-quality treatment), or disregard (poor-quality treatment). While those in the control condition experienced a spike in cortisol, individuals in the high-quality treatment condition did not experience this physiological stress (cortisol). Those given poor-quality treatment also did not exhibit stress, suggesting the explicit disregard for them may have undermined the interview’s legitimacy, thereby removing social evaluative threat. Paralleling past research, self-reported stress did not reflect individuals’ physiological stress (cortisol). Overall, results suggest that to alleviate group members’ physiological stress, supervisors need to be more than polite and professional–also demonstrating care/concern for them as individuals.
Undergoing difficult interviews and evaluations is common in groups, including in work organizations and educational institutions. These can elicit stress (Dickerson & Kemeny, 2004), which with repeated exposure can potentially damage health over time (McEwen, 2004). Theory and research suggest, however, that individuals’ responses to these stressful events are affected by how well they are treated by other group members, especially members who are in positions of authority (Miedemam et al., 2006; Tyler & Lind, 1992; van den Bos et al., 1998). Indeed, evidence shows that the quality of treatment coming from group authorities affects individuals’ self-reported stress, health, and well-being. For instance, research has shown that when employees experienced a pay cut (stressor), their response depended on how they were treated by supervisors (Greenberg, 2006). Compared to a control group, employees in an experimental group whose supervisors underwent training on how to convey care and consideration for them reported less insomnia both immediately after the pay cut and 6 months later (see also Elovainio et al., 2002; Huo et al., 2010, 2015).
These beneficial effects likely occur because when individuals know that group authorities care about them, it enables them to better respond to stressors by communicating that they are valued group members (Tyler & Lind, 1992), and thus the group is likely to be a helpful resource to them during that stressful situation. This also aligns with other theorizing on the benefits afforded when group members are treated in ways that communicate concern for them (Greenberg, 2004; van den Bos et al., 1998; Vermunt & Steensma, 2001).
However, previous work on stress and intragroup treatment has relied heavily on self-reported stress and related outcomes (e.g., insomnia; Greenberg, 2006; Huo et al., 2015; cf. Vermunt et al., 2007). This is a notable limitation, given that self-reported stress does not always align with physiologically detectable stress (Kirschbaum et al., 1995; Maina et al., 2008; Townsend et al., 2011). Thus, regardless of whether individuals report feeling stressed, their body may be enduring it physiologically. This makes it critical to know what is happening “under the skin,” especially given that physiological stress is linked to various health outcomes (e.g., cardiovascular disease; Juster et al., 2010; McEwen, 1998).
Discerning What It Takes to Alleviate Physiological Stress
Moving beyond self-reported stress also provides an opportunity to start discerning what it really takes for group authorities to help members stave off physiological stress. One possibility is that it requires authorities to treat everyone with a clear level of professionalism—treatment that is generally polite and follows group norms/rules, with parallels to traditional notions of fairness (Leventhal, 1980) and equality-based respect (Honneth, 1996). Another possibility is that it requires something more. To alleviate physiological stress, group authorities might also have to show care and concern—reflecting the more interpersonal aspects of treatment quality highlighted in research on authority expressions of benevolence (Tyler & Lind, 1992). Thus, in moving beyond self-reported outcomes, there is an opportunity to probe an important and practical question: To prevent physiological stress, does it suffice for group authorities to treat everyone with a standard level of professionalism? Or does it require more? Indeed, authorities may need to take the time to show care and concern for group members’ particular needs, experiences, and well-being.
When considered from a biopsychosocial perspective (Blascovich, 2008; Jamieson, 2017; Mendes & Park, 2014; Seery, 2013; also see Haslam et al., 2019), treating group members in a professional manner (with politeness and following group norms) may convey that an event—such as a difficult and demanding interview—is a legitimate evaluative procedure. This sets the stage for potentially inducing social evaluative threat and a corresponding pattern of physiological reactivity, including increased cortisol. However, if group members feel that they also have adequate resources to cope with the demands of that interview, this should enable them to appraise it as a challenge rather than a threat, and avoid that increase in cortisol. Therefore, by demonstrating care and concern for the individual—going beyond mere professionalism—group authorities may be an important resource for enabling individuals to adequately cope with stressful events, and ultimately avoid increased cortisol.
Current Research
Here, we examine how group-based treatment coming from an ingroup supervisor impacts individuals’ physiological response to a stressful event. While using physiological methods is resource-intensive (regarding time, labor, cost), it allows us to go beyond how such treatment makes individuals feel “on the surface” to how it affects them “under the skin.”
The current research also extends work on social identity and health (Haslam & Reicher, 2006; Häusser et al., 2012) by integrating theories of intragroup relations to examine how the quality of treatment coming from group authorities affects physiological stress. It also extends work on social support and physiological stress (e.g., Heinrichs et al., 2003; Taylor et al., 2010; Uchino et al., 2011) by taking a pointedly intragroup approach. It assesses whether the capacity to buffer physiological stress extends beyond those with, for example, close relationships (family, friends) to include members of a shared social group. As we posit, even among those with more formal relationships in a group (e.g., supervisor and employee) and without any established rapport, the quality of their interactions has the potential to reduce physiological stress.
In this study, participants were exposed to a stressful interview procedure known to elevate cortisol (Trier Social Stress Task [TSST]; Kirschbaum et al., 1993). Cortisol is a biomarker of stress, a hormone regulated by the hypothalamic-pituitary-adrenocortical (HPA) axis that increases in situations that elicit social evaluative threat (Dickerson & Kemeny, 2004). Surrounding the interview, each participant was guided by an ingroup supervisor trained to act in one of three ways: treating the participant professionally (following politeness norms [control]), treating them with explicit care and concern (high-quality treatment), or with disinterest and lack of regard for the individual (poor-quality treatment).
We expected that undergoing a stressful event (TSST) guided by a supervisor who adheres to basic norms of professionalism (in line with general protocols for administering the TSST [control condition]) would elicit the typical stress response (elevated cortisol; Kirschbaum & Hellhammer, 2000). By comparison, we expected those guided by a supervisor who expresses care and concern for the individual to more effectively stave off this physiological stress—despite going through the same interview/social evaluative stressor. It was less clear how poor-quality treatment would affect individuals. One possibility is that overt expressions of disregard for the individual would exacerbate the stress induced by the interview procedure (e.g., by lowering perceived resources for coping). Another possibility, in line with some research (Schroth & Shah, 2000), is that poor treatment would reduce physiological stress by diminishing the perceived legitimacy of the evaluative procedure (Tyler & Lind, 1992). If the person overseeing the procedure fails to convey even a basic level of professionalism, the procedure’s credibility as a means of fairly assessing the individual might be degraded (van den Bos et al., 1999). This is important because in order for the interview to induce physiological stress it has to be a legitimate social evaluative procedure. Only then does it have the potential to induce social evaluative threat and elevated cortisol (Dickerson & Kemeny, 2004). Therefore, if the treatment surrounding the interview conveys disregard for the individual, it may feel like a burdensome procedure but may not induce physiological stress.
Trait Depressive Rumination
Past research indicates that physiological stress can be moderated by individual differences, including trait depressive rumination—that is, responding to depressive feelings by engaging in repetitive, unwanted thoughts on related negative content. This can produce a blunted or “flat” stress response (Zoccola & Dickerson, 2012). We therefore examine trait depressive rumination as a moderator of physiological stress. Those higher in trait depressive rumination should show a blunted, “flat” cortisol response across conditions. Those lower in trait depressive rumination should show differing responses across conditions, in line with anticipated treatment quality effects.
Methods
Participants and Design
Eighty-two university students completed the study, described as being about everyday social interactions (Mage = 19.98, SD = 1.76; 77.78% female; Mtrait depressive rumination = 3.15, SD = 0.82; one participant removed as cortisol values constituted an extreme outlier [approx. 9 SD from mean at baseline]; final n = 27/condition). While sample size was bounded by practical constraints (e.g., time, resources), sensitivity analyses showed the study was powered to detect effects of f ⩾ .34, α = .05, 1 – β = .80; key hypothesized effects were larger than this (Erdfelder et al., 1996). 1 Participation was limited to those aged 18+ absent of conditions and behaviors that can influence HPA axis functioning (e.g., clinical depression, taking female contraceptives). Participants were randomly assigned to one of three supervisor treatment conditions: control, high-quality treatment, poor-quality treatment.
Procedure
Pre-lab tasks
Participants first completed an online questionnaire, answering eligibility and demographic questions. Eligible participants were scheduled to complete an in-laboratory session. Prior to their session, they were instructed to avoid activities that may influence salivary cortisol levels (e.g., consuming alcohol 12 hours beforehand; Salimetrics, 2013). Participants completed their in-lab session individually in the afternoon to control for diurnal rhythm in cortisol levels (start time: from 2:00 to 4:00 p.m.).
Group context
In lab sessions, the shared university group membership of the participant, session supervisor, and interviewers was made salient, in part by (a) framing the interview procedure as an evaluation of the participant’s suitability for a selective university position; (b) making explicit that the session supervisor, interviewers, and principal investigators were all members of the university; (c) placing visual reminders of their shared group (institutional logos) at strategic locations in the lab and the online questionnaires.
Session supervisor
We also took steps to convey the session supervisor’s relative authority in relation to the participant. The supervisor was referred to by this distinguishing title in task instructions and in questionnaires. They wore business attire, had a designated full-sized desk, conveyed a distinct level of knowledge about the study as well as close affiliation with the principal investigators. Lastly, the supervisor (final-year undergraduate) was clearly in a position to lead the session and provide instructions, while the participant followed. 2
Acclimation period
Upon arrival to the lab, the participant was greeted by the session supervisor, who obtained consent to participate. During a 20-minute acclimation period, participants completed a questionnaire (e.g., health history) and rested quietly at a computer terminal in a private room. Next, participants returned to the main laboratory space and provided their first saliva sample (baseline).
Interview task
Participants then returned to the computer room where they received prerecorded audio instructions describing the main task (TSST; Kirschbaum et al., 1993), which was to deliver a speech to a panel of interviewers explaining why they would be an ideal candidate for a selective university position, and then complete a second task after the speech (backwards-counting task; the university-specific speech topic reflected a modification to the standard TSST). They then had 5 minutes to prepare their speech. After completing the speech and counting task in a separate room, they returned to the main laboratory space and provided another saliva sample. Shortly thereafter, participants returned to their computer terminal and completed measures assessing their perceptions of the supervisor (and research team—the principal investigators, who were represented in text and the prerecorded audio). Participants completed a measure of trait depressive rumination embedded among other measures. Afterwards, participants rested by watching a nature video and provided two more saliva samples. Finally, participants were debriefed.
Cortisol collection
We collected salivary cortisol at 4 time points (20-, 50-, 75-, and 100-minute marks), which were spaced to capture the typical quadratic trajectory in TSST-based research (Kirschbaum & Hellhammer, 2000).
Experimental Manipulation
Treatment quality (control, high-quality, poor-quality) was manipulated largely through supervisor–participant interactions. This included prescripted verbal instructions delivered by the supervisor at specific times, with corresponding demeanor (e.g., tone of voice, body language), starting after the acclimation period: (a) control condition: supervisor engaged with the participant only when necessary to provide instructions, made occasional eye contact, and rarely referred to them by name; (b) high-quality treatment condition: supervisor actively engaged with and listened to the participant, consistently made eye contact, and regularly referred to them by name; (c) poor-quality treatment condition: supervisor was disengaged from the participant, rarely made eye contact, and never referred to them by name.
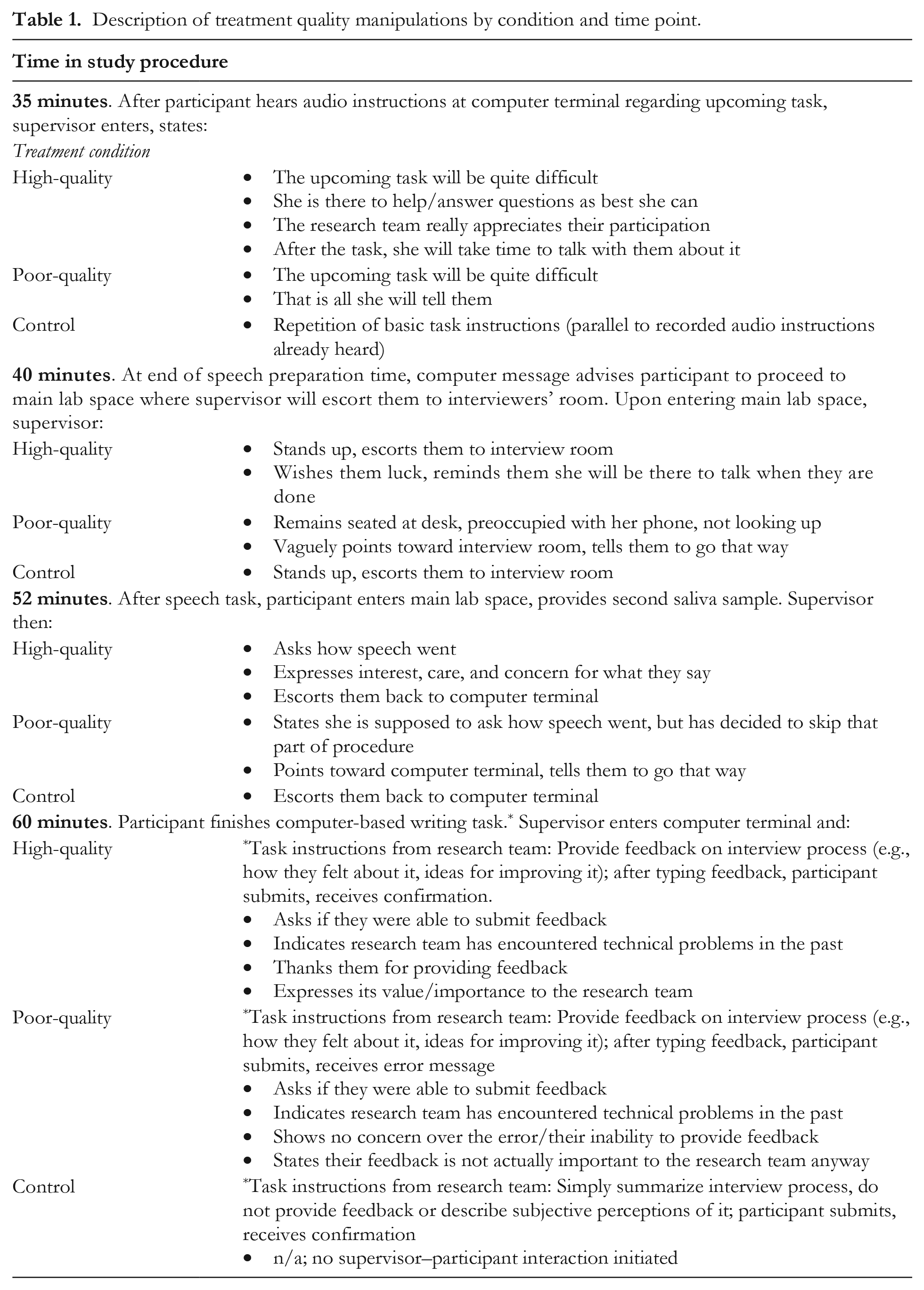
Table 1 outlines these manipulations in detail. In line with previous manipulations (Greenberg, 2006) and theory (Blader & Tyler, 2003; Tyler & Lind, 1992), in the high-quality treatment condition, the supervisor demonstrated clear concern for the individual (e.g., the individual’s particular needs and experiences during the lab session) in addition to conveying professionalism (e.g., being polite). In the poor-quality treatment condition, the supervisor explicitly deprived the individual of any expressions of care/concern nor did they show a general level of professionalism. In the control condition, the supervisor conveyed professionalism following politeness norms—in line with what one might typically expect from a lab supervisor—but did not provide any explicit indicators of care/concern.
Description of treatment quality manipulations by condition and time point.
Measures
Participants provided basic demographic information (age, sex, race/ethnicity). All multi-item measures were converted to item-averaged composites.
Cortisol
We collected salivary cortisol at four time points (T1–T4; passive drool technique; Salimetrics, 2013). Samples were stored at −20 °C and assayed in duplicate at a diagnostic company’s lab (Salimetrics; intra- and interassay coefficients of variation: 5.76% and 4.20%; sensitivity: 0.007 µg/dL). For ease of interpretation, we analyzed raw values (see multiverse analysis for analysis of log-transformed values).
Manipulation check: Professionalism
Treatment quality was assessed with regard to whether the supervisor first and foremost expressed professionalism toward the participant. Participants responded to five items assessing whether the supervisor seemed: polite, respectful, fair, competent, and objective (1 = not at all, 5 = extremely; α = .93). Participants were also asked about the research team as a whole: “The research team treated me with respect,” “The research team seems to treat participants fairly” (1 = strongly disagree, 7 = strongly agree; r = .77).
Manipulation check: Concern for the individual
Treatment quality was also assessed with regard to whether the supervisor expressed concern for the individual. Participants responded to five items assessing whether the supervisor seemed: caring, considerate, likable, nice, and intimidating (reverse-scored; 1 = not at all, 5 = extremely; α = .91). Participants also indicated whether the research team as a whole expressed care and concern for them as individuals: “The research team cares about me as a person,” “The research team conducting this study is interested in what I have to say” (1 = strongly disagree, 7 = strongly agree; r = .74). 3
To further assess perceptions of the supervisor’s concern for the individual specifically at the onset of the stressor—a potentially critical time to experience this—participants responded to the question, “When you were preparing to give your speech, was the session supervisor . . . ?”: “caring,” “considerate of your needs,” “supportive,” “helpful” (1 = not at all, 5 = extremely; α = .96).
Trait depressive rumination
Trait depressive rumination was assessed using five items from the Rumination Subscale of the Response Styles Questionnaire (Treynor et al., 2003): “When you are feeling sad, blue, or depressed, how often do you. . .?” Example: “. . . think about all your shortcomings, faults, and mistakes” (1 = never, 5 = very often; α = .75).
Self-reported stress
Participants reported their subjective stress levels immediately before and after the interview (near onset and peak of physiological stress). Before the interview, participants were asked, “How stressful do you expect the upcoming interview process to be (e.g., delivering your speech)?” (1 = not at all stressful, 7 = extremely stressful). Afterwards, they were asked, “To what extent was the interview stressful?” (1 = not at all, 5 = extremely).
Covariates
We made several efforts to control for other factors that might influence HPA axis functioning. This included prescreening prospective participants (not recruiting individuals with certain conditions or behaviors; e.g., clinical depression or anxiety, taking female contraceptives, smoking regularly), and instructing selected participants to avoid certain activities in the hours preceding participation (e.g., consuming alcohol 12 hours beforehand; Salimetrics, 2013).
Additionally, participants responded to questions that served as covariates in auxiliary analyses (see multiverse analysis). This included checks on whether they followed preparticipation instructions. Covariates included participant age, sex, and time in menstrual cycle. 4 Participants also indicated whether they had gained or lost 1 lb or more in the past week, or were trying to change their weight. They also indicated how many alcoholic drinks they had in the past 7 days (past 48 hours, past 24 hours), and how many hours it had been since they last ate. They also indicated, in the past 24 hours, if they had done any strenuous physical activity and how many caffeinated drinks they had. They also indicated if in the past 12 hours they had done any vigorous exercise or consumed any caffeine; if in the past 2 hours they had eaten any food; if in the past hour they had brushed their teeth, chewed gum, or consumed any candy/granulated sugar, or eaten a large meal. Participants also reported their overall health (1 = poor, 5 = excellent; from the Medical Outcomes Study, 36-Item Short Form Health Survey Ware & Sherbourne, 1992), and information about their sleep: how many hours it had been since waking up that day; how many hours they slept that night; whether it was a typical night of sleep. They also indicated whether they felt depressed that day (1 = no feelings of depression, 7 = frequent/severe feelings of depression), or were taking hormone replacement therapy. Participants also completed supplementary measures relating to general or interaction-related anxieties (or similar social phobias, needs, etc.), depression, or measures that were otherwise related to HPA axis functioning: trait anxiety (Spielberger, 1983), depressive symptoms (Kohout et al., 1993), interaction anxiousness (Leary & Kowalski, 1993), social phobia (Rapee et al., 1994), perceived social support (Zimet et al., 1988), need to belong (Leary et al., 2013), proneness to hurt feelings (in social contexts; Leary & Springer, 2001), blushing propensity (in social contexts; Leary & Meadows, 1991), and posttask rumination (Zoccola et al., 2008; all measures were reliable: α ⩾ .74).
Additional Measures
Participants also answered questions not examined as potential covariates, either because there was no variance (about consuming alcohol in the past 12 hours, how many cigarettes were smoked that day, or in the past hour) or because they focally served as filler items, given the necessity to keep participants in the lab for an extended period of time (measures of social dominance orientation, justice sensitivity, social desirability, life satisfaction, self-esteem, spheres of control, global stress, physical functioning, university-related questions [e.g., university identification, number of friends who are university students, general questions about the Ambassadors Program, which is related to the TSST speech topic—note that no participants were or had been part of this program]).
Results
Manipulation checks utilized one-way analyses of variance (ANOVA) with planned contrasts. Primary analyses of cortisol responses utilized a repeated measures ANOVA (GLM [WSFACTOR] [sub]command in SPSS) with planned contrasts (specified contrast matrices; factors: time [within-subjects, four measures], condition [between-subjects], trait depressive rumination [between-subjects, mean centered]). Anonymized data are available upon request from the first author.
It is important to reiterate that sample size was bounded by practical constraints for this time- and resource-intensive study. While our sample size was in line with similar physiological work (e.g., Creswell et al., 2005; Häusser et al., 2012; Zoccola et al., 2008), a larger sample size would have enabled us to more robustly detect effects, especially those involving moderation. As such, these results should be interpreted accordingly—as initial evidence, to be replicated and built upon in future work.
Manipulation Checks
Demonstrating professionalism
In both the high-quality treatment and control conditions, participants reported being shown professionalism to an equal degree. This appeared to hold true regarding their perceptions of the supervisor: high-quality (M = 4.47, SD = 0.81); control (M = 4.30, SD = 0.72), t(78) = 0.72, p = .47, d = 0.20 (Figure 1); and the research team as a whole: high-quality (M = 5.59, SD = 1.13); control (M = 5.39, SD = 1.01), t(78) = 0.65, p = .52, d = 0.18. By comparison, those in the poor-quality treatment condition did not seem to experience this same level of professionalism. This appeared to hold true regarding perceptions of the supervisor (M = 3.51, SD = 0.95); contrast with control, t(78) = 3.52, p < .001, d = 0.96; contrast with high-quality, t(78) = 4.24, p < .001, d = 1.16; omnibus, F(2, 80) = 10.30, p < .001, d = 1.03 (Figure 1); and the team as a whole (M = 4.48, SD = 1.31); contrast with control, t(78) = 2.88, p = .01, d = 0.78; contrast with high-quality, t(78) = 3.53, p < .001, d = 0.96; omnibus, F(2, 80) = 7.06, p = .002, d = 0.84. 5
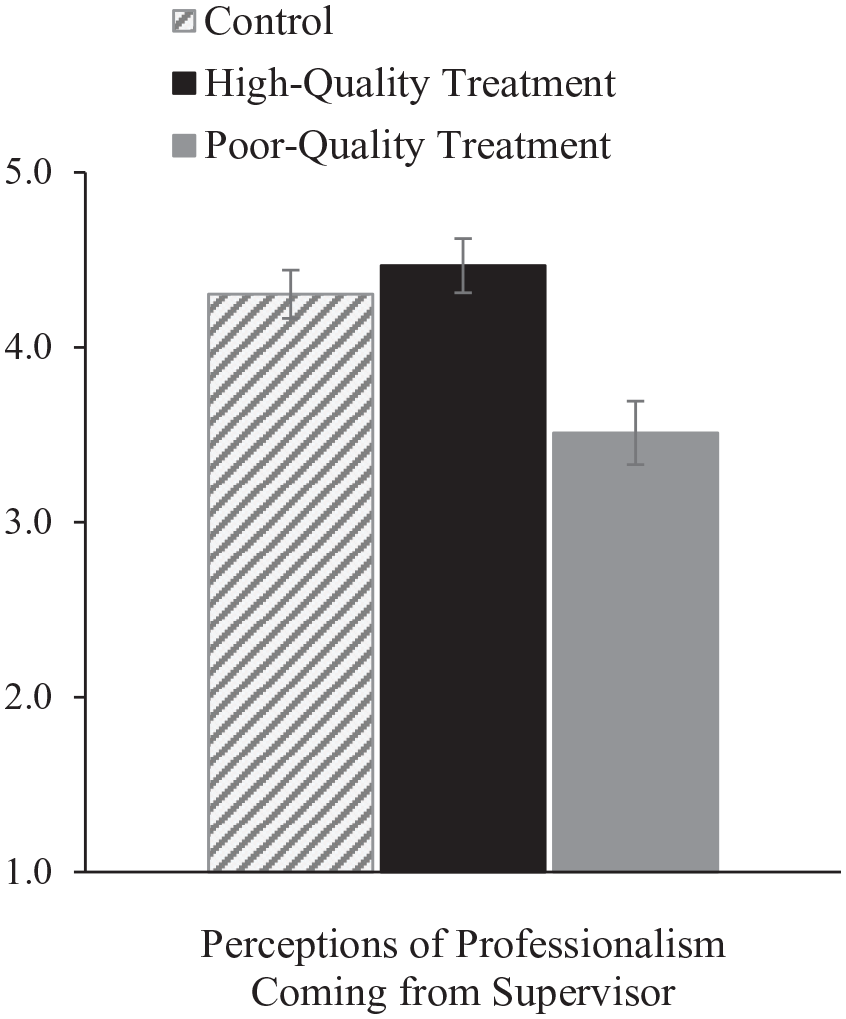
Effects of treatment condition on individuals’ perceptions that the supervisor demonstrated professionalism (meeting politeness norms).
Demonstrating concern for the individual
Despite the procedure seeming equally professional across the high-quality treatment and control conditions, participants in these two conditions differed on perceptions of being treated with care and concern. Compared to the control, those in the high-quality treatment condition seemed to experience being treated with greater care and concern both by the supervisor: high-quality (M = 4.59, SD = 0.78); control (M = 3.96, SD = 0.75), t(78) = 2.84, p = .01, d = 0.77; and the research team: high-quality (M = 5.57, SD = 1.12); control (M = 3.93, SD = 1.38), t(78) = 4.60, p < .001, d = 1.25. Similarly, at the onset of the stressor, those in the high-quality treatment condition perceived a higher level of concern being expressed by the supervisor (M = 4.25, SD = 0.88); control (M = 2.41, SD = 0.93), t(78) = 7.11, p < .001, d = 1.94 (Figure 2).
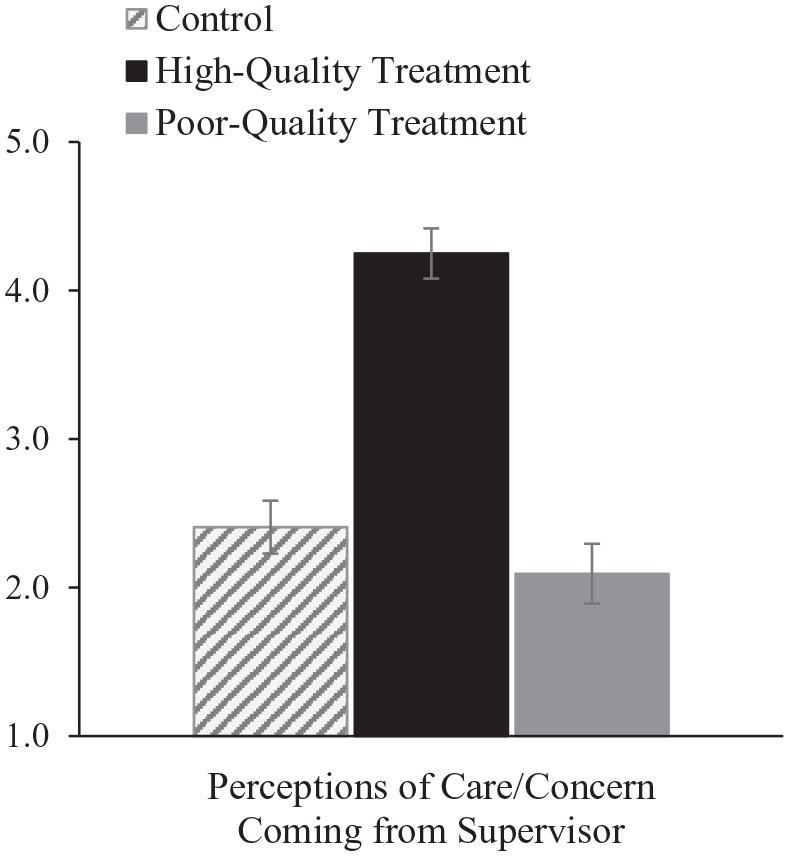
Effects of treatment condition on individuals’ perceptions that the supervisor demonstrated care/concern for them (at onset of physiological stressor).
Unsurprisingly, compared to these two conditions, those in the poor-quality treatment condition did not report being treated with much care/concern: perceptions of the supervisor (M = 3.10, SD = 0.91); contrast with control, t(78) = 3.87, p < .001, d = 1.05; contrast with high-quality, t(78) = 6.71, p < .001, d = 1.83; omnibus, F(2, 80) = 22.71, p < .001, d = 1.53. Perceptions of the research team (M = 3.02, SD = 1.43); contrast with control, t(78) = 2.53, p = .01, d = 0.69; contrast with high-quality, t(78) = 7.13, p < .001, d = 1.94; omnibus, F(2, 80) = 26.10, p < .001, d = 1.63. At the onset of the stressor, they also did not report being treated with much care/concern (M = 2.09, SD = 1.04); contrast with control, t(78) = 1.22, p = .23, d = 0.33; contrast with high-quality, t(78) = 8.33, p < .001, d = 2.27; omnibus, F(2, 80) = 40.48, p < .001, d = 2.04 (Figure 2).
Overall, these results suggest that conditions systematically varied in the experience of professionalism, and of being treated with care/concern. Participants in both the high-quality treatment and control conditions appeared to experience similar levels of professionalism. By comparison, those in the poor-quality treatment condition reported lower levels of professionalism (Figure 1). In contrast, participants in the high-quality treatment condition seemed to experience uniquely high levels of care/concern, compared to the control and poor-quality treatment conditions (Figure 2). 6
Cortisol Responses
We assessed whether participants’ cortisol levels varied as a function of time, condition, and trait depressive rumination. Because no potential covariates were significant (e.g., sex, hours since waking; p ⩾ .25), they were not included in primary analyses.
Consistent with predictions, the quadratic trajectory of cortisol appeared to vary as a function of both individuals’ experimental condition and trait depressive rumination: Time2 x Condition x Trait Depressive Rumination: F(2, 75) = 5.54, p = .01, f = .39; Time2 x Condition, F(2, 75) = 1.46, p = .24, f = .20; 7 Time2 x Trait Depressive Rumination, F(1, 75) = 3.85, p = .05, f = .23; Time2, F(1, 75) = 50.47, p < .001, f = .82. Test of between-subjects effects: condition, F(2, 75) = 1.21, p = .31, f = .18; tests of within-subjects effects with Greenhouse–Geisser correction (GGc): Mauchly’s test of sphericity, χ2(5) = 60.92, p < .001: Time x Condition, F(4.20, 157.53) = 1.12, p = .35, f = .18; Time x Trait Depressive Rumination, F(2.10, 157.53) = 5.49, p = .004, f = .27; Time x Condition x Trait Depressive Rumination, F(4.20, 157.53) = 4.18, p = .003, f = .33.
To probe this interaction, we assessed whether change in cortisol from one time point to the next (e.g., from T1 → T2) differed across the three conditions and among those who engaged in trait depressive rumination fairly often (+1 SD) versus rarely (−1 SD). We did so by examining contrasts in slopes from T1 (baseline) → T2 (emerging stress), T2 → T3 (peak stress), and T3 → T4 (recovery) by condition at ± 1 SD on trait depressive rumination. We also examined the magnitude of each slope and whether it significantly differed from zero.
Higher depressive rumination
As predicted, those with higher trait depressive rumination had a “flat” cortisol response across all conditions. The change in cortisol from T1 → T2, and from T2 → T3, for instance, did not appear to differ across conditions (all ps ⩾ .10). None of these slopes were significantly different from zero. 8
Lower depressive rumination
By comparison, those lower in trait depressive rumination (Figure 3) showed distinct response patterns by condition. Those in the control condition experienced a “classic” spike in cortisol. In contrast, those in the high-quality treatment condition seemed to show little change over time. Specifically, from T1 → T2, those in the control condition showed increases in cortisol (Mincrease = 0.13, p < .001), while those in the high-quality condition did not (Mincrease = 0.04, p = .18; Mcontrast = 0.09, p = .06). From T2 → T3 as well, those in the control condition showed continuing increases in cortisol (Mincrease = 0.16, p < .001), while those in the high-quality condition did not (Mincrease = 0.04, p = .22; Mcontrast = 0.13, p = .005). In the same vein, from T3 → T4 (recovery period), those in the control condition seemed to show a greater decline in cortisol (Mdecrease = −0.20, p < .001) compared to those in the high-quality treatment condition (Mdecrease = −0.05, p = .03; Mcontrast = −0.15, p < .001). Thus, results indicated support for predictions. While the evaluative process elicited a spike in physiological stress (cortisol) for those in the control condition, when that same evaluation was coupled with a caring and considerate supervisor, the typical stress response appeared to be wiped out.
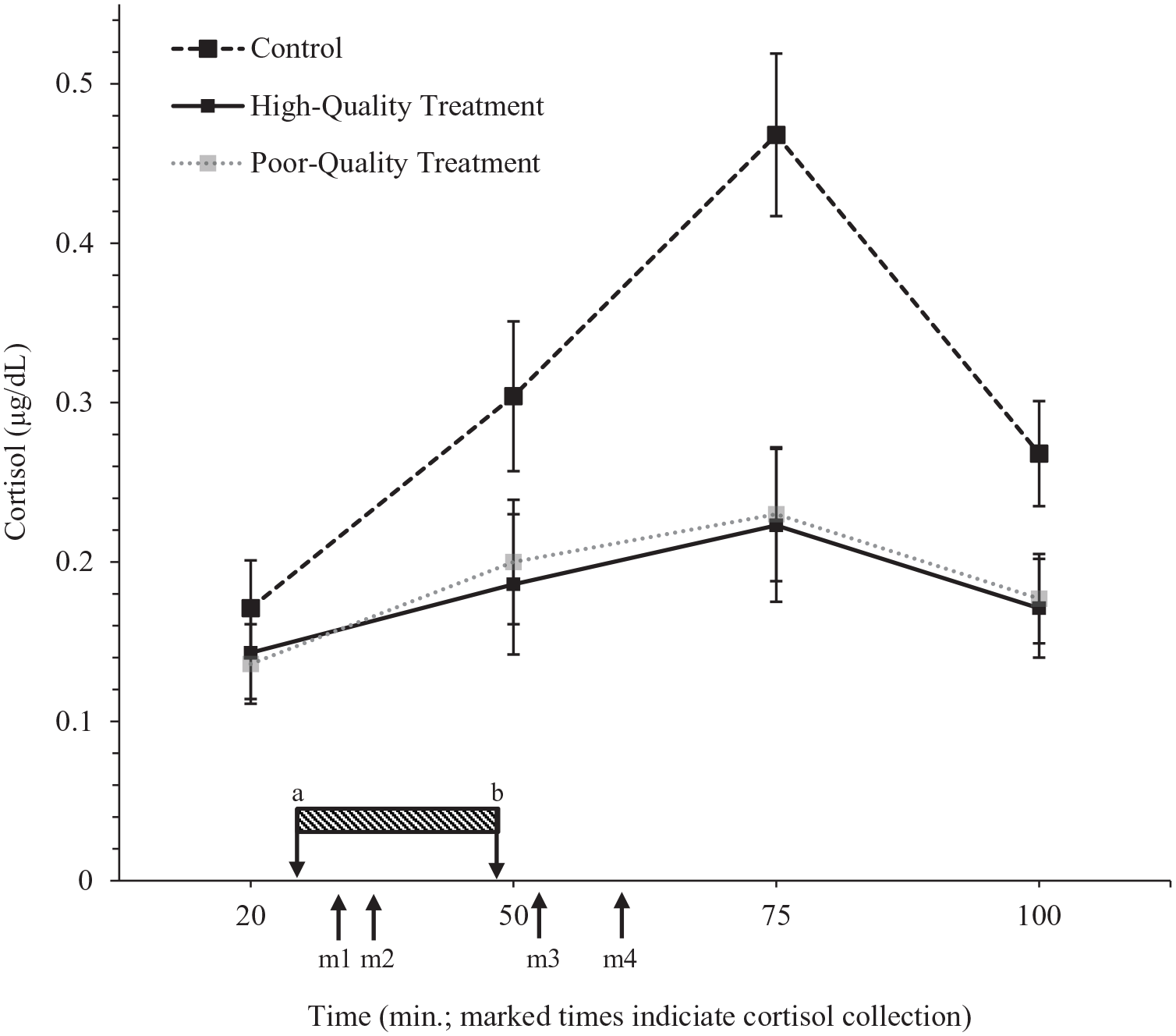
Change in cortisol across time by condition for participants low in trait depressive rumination.
When comparing the control and poor-quality treatment conditions, we found a similar pattern to those described before: poor-quality condition (contrasts with control), T1 → T2 Mincrease = 0.06, p = .03, Mcontrast = 0.07, p = .12; T2 → T3 Mincrease = 0.03, p = .26, Mcontrast = 0.13, p = .002; T3 → T4 Mdecrease = −0.05, p = .01, Mcontrast = −0.15, p < .001. Thus, again, while the evaluative process produced a “classic” spike in cortisol for those in the control condition, when it was carried out in a way that lacked that same level professionalism, individuals showed few signs of physiological stress.
Given the similarity in cortisol responses among those in the high- and poor-quality treatment conditions, when comparing these two conditions, unsurprisingly, there were no significant differences in slopes (all contrasts, p ⩾ .64).
Comparing Physiological and Self-Reported Stress
Overall, participants’ self-reported stress did not parallel physiological stress. While those in the control condition exhibited greater physiological stress than those in the high-quality treatment condition, they seemed to show no differences in self-reported stress: pre-TSST: control (M = 4.96, SD = 1.34), high-quality (M = 5.52, SD = 1.31), t(78) = 1.66, p = .10, d = 0.45; post-TSST: control (M = 5.07, SD = 1.52), high-quality (M = 5.33, SD = 1.54), t(78) = 0.61, p = .55, d = 0.17. Similarly, while those in the control showed higher levels of physiological stress than those in the poor-quality treatment condition, they appeared to show no consistent differences in self-reported stress: pre-TSST: poor-quality (M = 5.78, SD = 1.01); contrast with control, t(78) = 2.43, p = .02, d = 0.66; contrast with high-quality, t(78) = 0.77, p = .44, d = 0.21; omnibus, F(2, 80) = 3.08, p = .05, d = 0.55; post-TSST: poor-quality (M = 5.56, SD = 1.65); contrast with control, t(78) = 1.13, p = .26, d = 0.31; contrast with high-quality, t(78) = 0.52, p = .61, d = 0.14; omnibus, F(2, 80) = 0.64, p = .53, d = 0.29. Thus, individuals’ self-reported stress appeared largely disparate from what they experienced physiologically. 9
There were also no significant correlations between cortisol level (as assessed at any time point) and self-reported stress (either at pre- or post-TSST) in any conditions (all zero-order rs ⩽ .23, all ps ⩾ .25). This also held true when examining individuals lower in trait depressive rumination (below median).
Additional Analyses
To further probe key hypothesized effects, we conducted a multiverse analysis (Steegen et al., 2016) wherein we systematically changed various aspects of our primary analyses with reasonable alternatives (e.g., used by Creswell et al., 2005) to assess whether the same patterns of findings emerged. Table 2 outlines the systematic changes implemented, which cumulatively generated 256 unique p values for further probing effects across our two key conditions (control, high-quality treatment).
Structure of multiverse analysis.
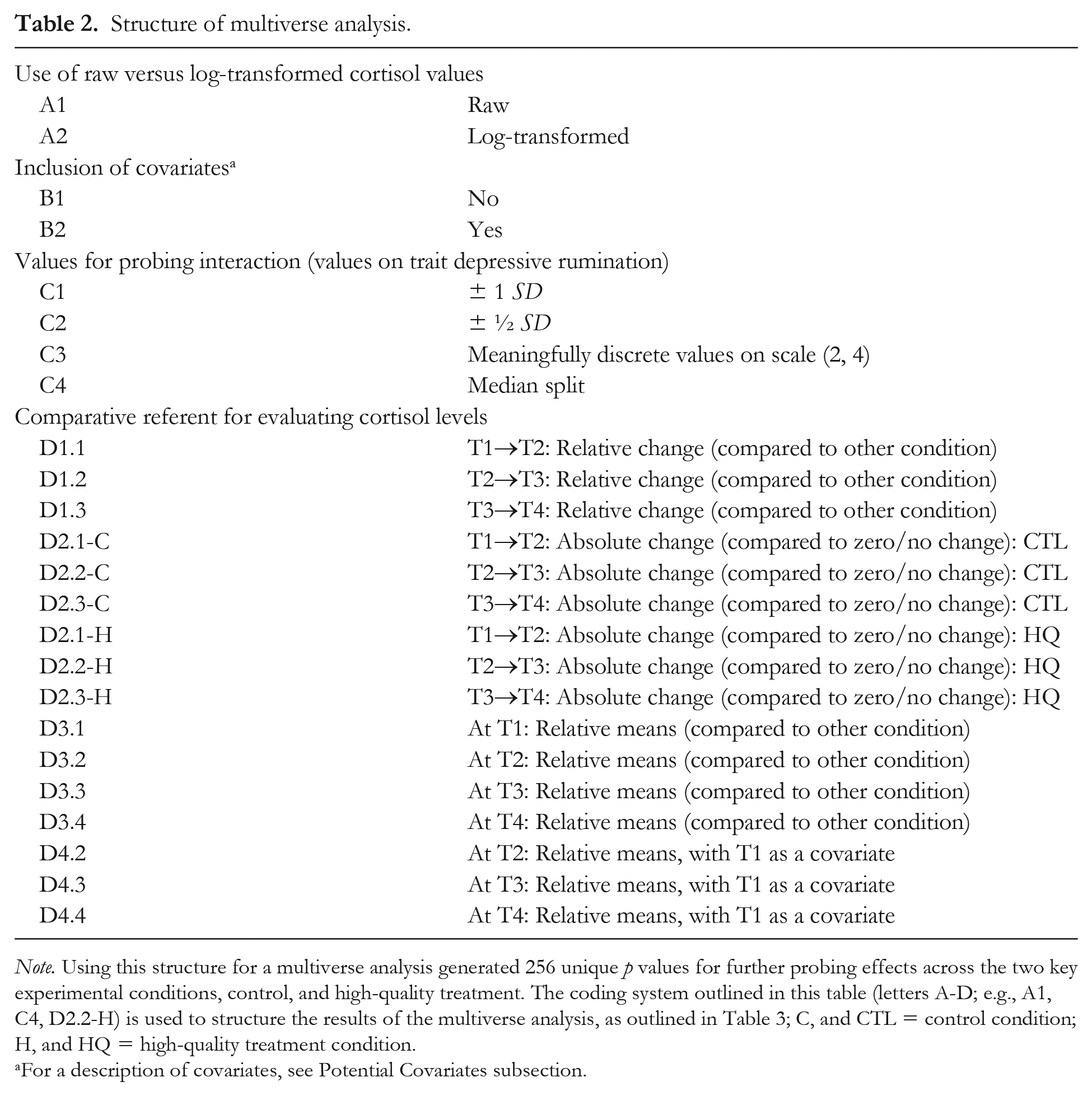
Note. Using this structure for a multiverse analysis generated 256 unique p values for further probing effects across the two key experimental conditions, control, and high-quality treatment. The coding system outlined in this table (letters A-D; e.g., A1, C4, D2.2-H) is used to structure the results of the multiverse analysis, as outlined in Table 3; C, and CTL = control condition; H, and HQ = high-quality treatment condition.
For a description of covariates, see Potential Covariates subsection.
Table 3 illustrates multiverse analysis results. Overall, support for hypothesized effects remained evident including when covariates were entered, alternate values were used to probe effects (on trait depressive rumination), and when using alternative comparative referents for evaluating differences in cortisol (e.g., comparing mean cortisol levels between conditions at a given time point). Notably, when using log-transformed cortisol values, there was a less consistent difference when directly comparing the magnitude of the control and high-quality treatment condition slopes from T2→T3 (Table 2, row D1.2). Nevertheless, analyses of log-transformed valued continued to evince consistent, significant increases in cortisol for the control condition (i.e., significant changes in absolute terms; T1→T2→T3; rows D2.1-C, D2.2-C), while any such evidence in the high-quality treatment condition was less consistent (rows D2.1-H, D2.2-H). Moreover, analyses of log-transformed values showed that the control and high-quality treatment conditions continued to consistently and significantly differ on their peak stress levels (row D3.3; also see D4.3). In fact, the evidence indicating that participants in the control condition experienced significantly higher levels of (peak) stress held true across nearly the whole multiverse analysis (16 separate tests of this effect). Overall, this suggests that those in the control condition exhibited a reliably distinct and particularly high level of stress compared to those in the high-quality treatment condition, further indicating that being guided by a caring and considerate supervisor helped mitigate physiological stress.
Results of multiverse analysis, comparing control and high-quality treatment conditions.
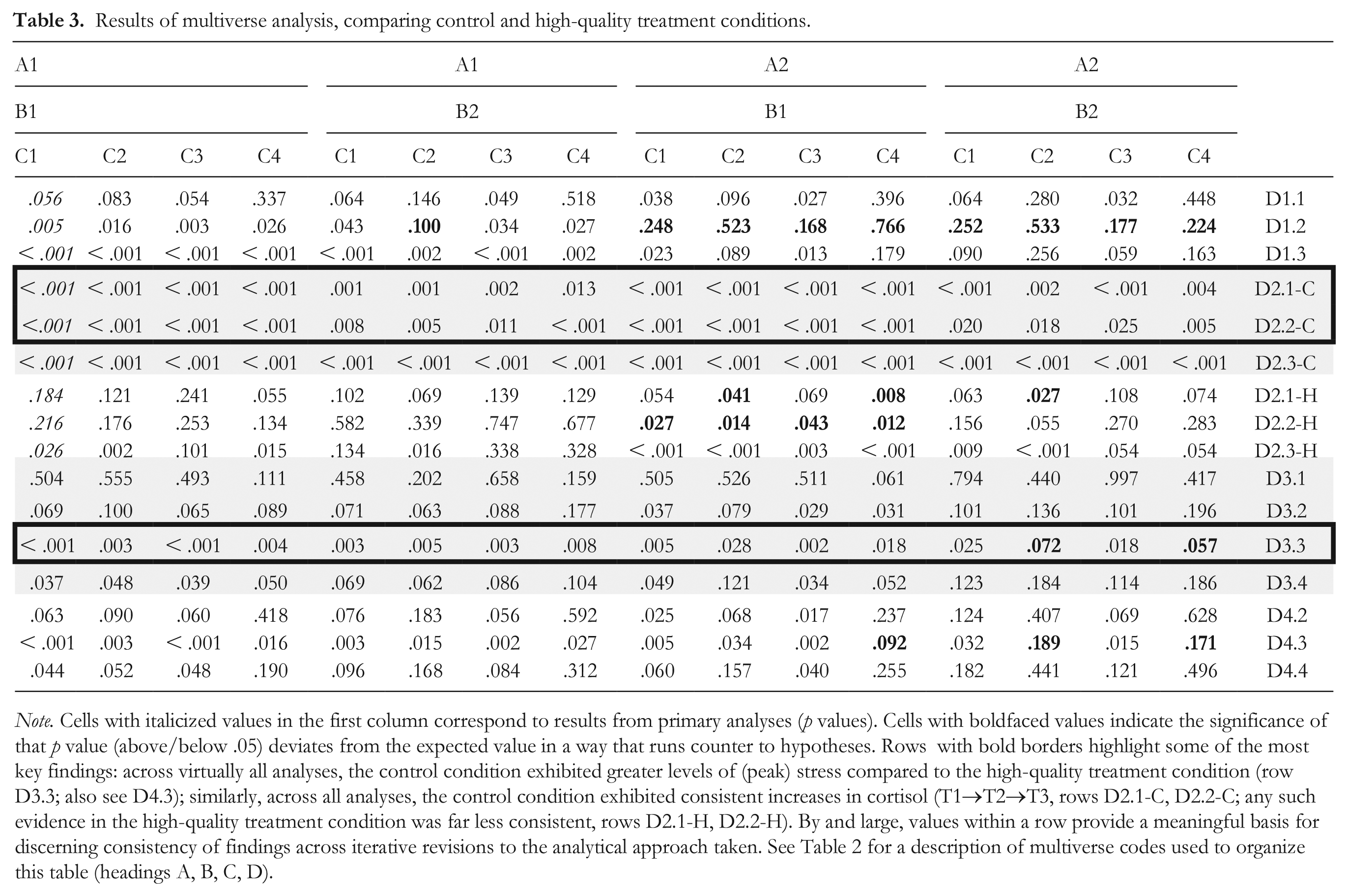
Note. Cells with italicized values in the first column correspond to results from primary analyses (p values). Cells with boldfaced values indicate the significance of that p value (above/below .05) deviates from the expected value in a way that runs counter to hypotheses. Rows with bold borders highlight some of the most key findings: across virtually all analyses, the control condition exhibited greater levels of (peak) stress compared to the high-quality treatment condition (row D3.3; also see D4.3); similarly, across all analyses, the control condition exhibited consistent increases in cortisol (T1→T2→T3, rows D2.1-C, D2.2-C; any such evidence in the high-quality treatment condition was far less consistent, rows D2.1-H, D2.2-H). By and large, values within a row provide a meaningful basis for discerning consistency of findings across iterative revisions to the analytical approach taken. See Table 2 for a description of multiverse codes used to organize this table (headings A, B, C, D).
In other analyses, we explored whether levels of posttask rumination (how often participants had negative thoughts about their performance following the TSST; e.g., “How bad my speech was,” “I must have looked stupid”; α = .94) differed across conditions, or moderated cortisol responses (as in Zoccola et al., 2008). Results indicated that posttask rumination levels did not differ across conditions: omnibus, F(2, 78) = 0.36, p = .70, d = 0.19; all condition contrasts: t(78) ⩽ 0.76, p ⩾ .45, d ⩽ 0.21. Results also indicated that individuals’ trajectory of cortisol was not moderated by posttask rumination: Time2 x Condition x Posttask Rumination, F(2, 75) = 0.67, p = .52, f = .14; Time2 x Posttask Rumination, F(1, 75) = 0.67, p = .42, f = .10; Time2 x Condition, F(2, 75) = 1.31, p = .28, f = .19; Time2, F(1, 75) = 47.90, p < .001, f = .80. Test of between-subjects effects: condition, F(2, 75) = 1.16, p = .32, f = .18; tests of within-subjects effects with GGc: Time x Condition x Posttask Rumination, F(3.97, 148.97) = 0.60, p = .66, f = .13; Time x Posttask Rumination, F(1.99, 148.97) = 0.29, p = .74, f = .06; Time x Condition, F(3.97, 148.97) = 1.36, p = .25, f = .19.
When examining both posttask rumination and trait depressive rumination (with corresponding interaction terms), results indicated: (a) regarding posttask rumination, the same null effects described in the preceding paragraph; (b) regarding trait depressive rumination, the same significant effects described in primary analyses, for example, Time2 x Condition x Trait Depressive Rumination, F(2, 69) = 5.12, p = .01, f = .38; (c) no significant interactions between them, for example, Time2 x Posttask Rumination x Trait Depressive Rumination, F(1, 69) = 0.68, p = .41, f = .10; Time2 x Condition x Posttask Rumination x Trait Depressive Rumination, F(2, 69) = 0.08, p = .92, f = .04.
Discussion
Past research indicates that when individuals are treated by fellow group members, including those in authority positions, in ways that communicate care and concern for them, they report fewer health issues (e.g., insomnia) and better well-being (Greenberg, 2006; Huo et al., 2010, 2015). Yet there is a relative lack of evidence about whether the actions of group authorities “sink in” deep enough to affect individuals physiologically. The current research helps fill this gap in the literature.
We specifically demonstrated that experiencing high-quality treatment from a group supervisor buffers individuals’ physiological stress response. All participants went through an interview procedure known to elicit physiological stress (cortisol; Kirschbaum et al., 1993), with parallels to what one might experience in a difficult interview or evaluation at work or school. While those in the control condition showed a clear spike in cortisol (among those low in trait depressive rumination), results indicated that being guided by a supervisor who demonstrated care and concern for them wiped out this stress response.
Additionally, despite these differences in physiological stress, individuals in the high-quality treatment and control conditions did not show a parallel pattern of self-reported stress. Thus, we not only demonstrated the beneficial physiological effects of high-quality treatment, but also that these effects cannot always be detected through self-reports.
Showing Concern for the Individual Is Key
This also provides insight into the particular aspects of high-quality treatment needed to mitigate physiological stress. Results indicated that those in the control condition experienced a level of professionalism equivalent to that experienced by those in the high-quality treatment condition. Yet, clearly this aspect of treatment alone did not stave off physiological stress, as indicated by the spike in cortisol among those in the control condition only. Rather, what differentiated those in the control and high-quality treatment conditions was the level of care and consideration that the supervisor, and the research team, showed for individuals. This suggests that simply being professional—being polite and following basic group norms/rules—is not sufficient to mitigate the physiological effects of a stressful situation. Something more is required. Specifically, it requires group authorities, including supervisors, to communicate care and concern for the particular needs and welfare of an individual.
These findings deepen our understanding of group processes and health in several ways. First, they advance past findings (e.g., Greenberg, 2006) where multiple elements of high-quality treatment have been conflated. The current research illustrates what may in fact be the most essential driver of these health-related effects—showing care for the individual as a group member. Second, these findings demonstrate that the capacity to buffer physiological stress is not limited to individuals with close interpersonal relationships (e.g., best friends; Heinrichs et al., 2003). Even among those in more formal relationships, including a supervisor and student (or employee), there is potential to reduce physiological stress.
On a practical level, these findings provide insight into how supervisors and other group authorities can more effectively alleviate group members’ physiological stress. It appears to require not only being polite and professional (e.g., treating people in line with established norms and protocols) but being truly considerate of individual members’ needs and experiences.
This distinction, between professionalism and that additional step of showing concern for the individual’s particular needs, has parallels to traditional conceptualizations of fairness (emphasizing consistency in how an authority treats all group members; Leventhal, 1980) versus more relational conceptualizations that recognize the importance of acting in ways that foster authority–member relationships and a shared group identity (Blader & Tyler, 2003; Huo, 2003; Tyler & Lind, 1992). In line with this distinction, group authorities might behave in ways that are generally polite and adhere to group rules/norms, but they can also provide a higher quality of treatment that conveys care for group members’ particular needs. In terms of physiological effects, the current evidence suggests the professional aspect of intragroup treatment may primarily function to signal whether a procedure or event (e.g., a difficult interview) is fair and legitimate. By comparison, the relational aspect of showing concern for the individual may function to signal the quality of the bond between the individual and the group, with a stronger bond signaling access to relevant resources to cope with the stress of that event. In future research using physiological measures, it will be important to further probe the role of treatment that emphasizes universal group norms (everyone being shown professionalism) and that which emphasizes the relationships among group members.
Poor-Quality Treatment
This research also explored the effects of being treated in explicitly negative ways—a supervisor conveying negligence and lack of care for the individual. We found that this resulted in an absence of detectable physiological stress. While this may seem counterintuitive, it fits with some previous work. In essence, being treated in this manner may undermine the credibility of the task (interview) as a legitimate social evaluative procedure (Tyler & Lind, 1992; van den Bos et al., 1999). As a result, the task or interview may be inconsequential at a physiological level because in order for it to induce social evaluative threat and physiological stress (cortisol), it has to be a seemingly legitimate social evaluative procedure (Dickerson & Kemeny, 2004). Thus, blatant disregard for the individual may take the “bite” out of what would otherwise be a situation that elicits social evaluative threat. This finding also aligns with evidence that persistent poor treatment may result in less stress “under the skin” (Matta et al., 2016). It is also informative that self-reported stress did not reflect physiological stress. Compared to the control condition, those in the poor-quality treatment condition showed no consistent differences in self-reported stress, despite having lower cortisol levels. This may be because while treatment that conveys utter disregard for the individual diminishes its potential to induce social evaluative threat and thus cortisol, having to carry on with the procedure may still feel unpleasant and thus stressful in self-report. In a similar vein, others have posited that self-reported and physiological stress may not parallel one another because they capture distinct aspects of an experience (Mendes et al., 2002; Townsend et al., 2011). Additionally, self-reported stress may have been shaped by demand characteristics—recognizing that the procedure was intended to be unpleasant. Overall, in future research, it will be important to further probe this poor-quality treatment effect.
Future Directions
Going forward, it will be important to probe mechanisms underpinning these patterns of stress reactivity (and to replicate the current study’s effects more generally). For instance, it will be important to empirically assess why both high-quality and poor-quality treatment result in little cortisol reactivity, and whether the mechanisms underpinning these similar outcomes are different. For instance, high-quality treatment may result in low cortisol reactivity because it prompts an approach-oriented response, which is characterized by low cortisol reactivity but elevated dehydroepiandrosterone-sulfate (DHEAS; Crum et al., 2017), if not also other indicators of approach-oriented task engagement (e.g., activation of the sympathetic-adrenal-medullary system, certain patterns of cardiovascular reactivity; see Jamieson, 2017; Mendes & Park, 2014; Seery, 2013). Experiencing poor-quality treatment may also result in low cortisol reactivity but for different reasons. For example, it may prompt individuals to view the task as illegitimate and thus not a personally meaningful social evaluative procedure. If so, individuals treated with such disregard might not only show low cortisol reactivity but also little reactivity in DHEAS, if not also few other physiological indices of motivated task engagement. Notably, given the potential incongruities between physiological and self-reported reactions to stressors (e.g., Kirschbaum et al., 1995; Townsend et al., 2011), relying on physiological evidence to probe these mechanisms seems valuable (e.g., differences in DHEAS; to avoid, for instance, the influence of demand characteristics on self-report mechanism measures).
Going forward, it will be valuable to test these processes in more applied, albeit less controlled, settings. This may include among members of an organization who have more established relationships. While the current research focused on less well-established relationships between members—perhaps paralleling relationships between an organizational supervisor and a new employee—future studies will enrich our understanding of these group-based processes by examining treatment effects between individuals with different “histories” (e.g., preexisting group relationships varying in length, quality).
In the current research, treatment quality manipulations encompassed variation in the supervisor’s engagement with the participant (e.g., wishing them luck on the interview) and the task itself (e.g., carrying out basic procedural steps appropriately). This is in line with previous manipulations (Greenberg, 2006) and related theory (Blader & Tyler, 2003; Tyler & Lind, 1992), and highlights that a supervisor’s engagement with the task is conceptually tethered to the quality of treatment received by the individual. This is because the individual is a central part of that task. When a supervisor overseeing the task demonstrates a willingness to ensure that it is carried out in an appropriately professional manner, this conveys fairness and respect for the individual and their experience with that task. In the current research, the supervisor demonstrated (appropriately professional) engagement with the task itself in both the control and high-quality treatment conditions. However, unique to the high-quality treatment condition, the supervisor also demonstrated (highly considerate) engagement with the participant (in the poor-quality treatment condition, the supervisor demonstrated neither appropriately professional nor highly considerate engagement). Going forward, it will be informative to examine stress reactivity and related processes (e.g., perceived legitimacy of task) under other conditions where, for instance, a supervisor’s engagement with the task versus the individual are more fully disaggregated (e.g., when a supervisor is disengaged from the task but highly engaged with the individual, or vice versa).
Conclusion
The current evidence helps fill an important gap in the literature on the social determinants of health and stress and, in particular, the role of intragroup treatment in shaping individuals’ physiological stress. It shows that supervisors and other group authorities have the capacity to affect individuals “under the skin.” Moreover, it provides practical insights into how supervisors can alleviate physiological stress—by not only being professional to fellow group members but also taking the time to show care and concern for their particular needs and experiences.
Footnotes
Acknowledgements
We would like to thank the Social Relations Lab research assistants for their invaluable support with recruitment and data collection. This research was approved by and carried out in compliance with standards for human research set forth by the University of California, Los Angeles Institutional Review Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support was provided by a UCLA Council on Research Grant awarded to Y.H. The funders had no role in study design, data collection, analysis, or manuscript preparation.