
Abstract
Identifying with a group can impact (positively) upon group members’ health. This can be explained (in part) through the social relations that a shared identity allows. We investigated the relationship between a shared identity and health in a longitudinal study of a month-long pilgrimage in north India. Questionnaire data (N = 416) showed that self-reported health (measured before, during, and after the event) was better at the event than before, and although it reduced on returning home, it remained higher than before the event. This trajectory was predicted by data concerning pilgrims’ perceptions of a shared identity with other pilgrims at the event. We also found evidence that a shared identity amongst pilgrims had an indirect effect on changes in self-assessed health via the belief one had closer relations with one’s fellow pilgrims. We discuss the implications of these data for our understandings of the role of shared identity in social relations and health.
Recent social psychological research highlights a link between the nature of our social relations and our health (Cohen, 2004; Helliwell & Putnam, 2004; Smith & Christakis, 2008). Particular emphasis has been paid to the finding that the number and quality of an individual’s social relationships affect health (the more, the better) and how these social relationships are bound up with our group memberships. Indeed, since we spend much of our time with others, it has been argued we should study health in group settings (Peterson, Park, & Sweeney, 2008).
Our research sought to do exactly this. We examined how participation in a large-scale collective event (a Hindu pilgrimage in north India) impacted participants’ (self-reported) health. As reported elsewhere (Tewari, Khan, Hopkins, Srinivasan, & Reicher, 2012), pilgrims reported better health after the event than a non-participating control group. In the current paper we address the social psychological mechanisms behind this effect of participation.
Group Processes and Health
The social identity perspective on group processes (Turner, Hogg, Oakes, Reicher, & Wetherell, 1987) argues that although we sometimes think of ourselves and others in terms of personal identities, we can also define ourselves in terms of our social group memberships (e.g., as a Catholic, as a Manchester United supporter, etc.). When we think about ourselves and others as members of a common group with a shared identity we are transformed from an aggregate of individuals into a psychological group (Hogg, 1992; Turner et al., 1987). This psychological transformation is consequential. A shared identity results in: greater trust, respect, and co-operation (Tyler & Blader, 2000), in mutual social influence (Abrams, Wetherell, Cochrane, Hogg, & Turner, 1990), and in greater support for each other (Levine, Prosser, Evans, & Reicher, 2005; Wakefield et al., 2011). It also shapes individuals’ expectations of support (Haslam, 2014; Haslam, Reicher, & Levine, 2012).
Drawing on this logic, social identity researchers argue that our health is affected by the degree to which we identify with others in terms of a shared social identity. This sense of “we-ness” with other group members leads us to see others as a source of support, which results in better health and well-being. In a phrase, shared social identity with others in groups constitutes a “social cure” (Jetten, Haslam, & Haslam, 2012). Illustrating this logic, Haslam, O’Brien, Jetten, Vormedal, and Penna (2005) showed that amongst those working in stressful jobs, the more individuals identified with their fellows, the more they felt they could cope, and the better their well-being (see too Wegge, van Dick, Fisher, Wecking, & Moltzen, 2006). Similar effects have been reported for the elderly living in residential care homes (Gleibs et al., 2011) and soldiers in army units (Sani, Hererra, Wakefield, Boroch, & Gulyas, 2012). Moreover, Sani et al. (2012) show it really is identification with the group as an entity (rather than the amount of contact with individuals in the group) that is important.
Although addressing a range of health outcomes (e.g., depression: Cruwys et al., 2014; stroke recovery: Haslam et al., 2008), for different demographics (e.g., the elderly: Gleibs et al., 2011), in different contexts (e.g., work teams: Haslam et al., 2005; theatre groups: Haslam, Jetten, & Waghorn, 2009), such research shares various characteristics. First, studies have concentrated on small face-to-face groups in which people develop intense interpersonal relationships. However, one of the strengths of the social identity approach is that it was developed to explain how members of large-scale social categories (e.g., a nation) can cohere (see Reicher, Spears, & Haslam, 2010). That is, it accounts for solidarities between strangers. This raises the question of whether participation in mass collective events, as well as small groups, could also be associated with positive health outcomes. If so, the theoretical significance of the concept of a shared social identity would be more clearly demonstrated.
Second, with some notable exceptions (e.g., Cruwys et al., 2014; Haslam et al., 2009), existing studies examining group identification and health are generally cross-sectional and rarely measure health change over time or how social identity-related processes are relevant to explaining that change. Moreover, if they do, the research either takes the form of an intervention designed to help people already experiencing difficulty (e.g., depression: Cruwys et al., 2014) or considers how people’s prior level of social identification with a group is relevant to well-being over a period of time (e.g., burnout in coworkers: Haslam et al., 2009). As far as we know there is no work that takes ordinary people at two time points and which considers how participation in group activities (and related social identity processes)—at a third time in-between these two other time points—explains any change in health and well-being from before participation to after participation.
Third, with only rare exceptions (e.g., Kellezi & Reicher, 2012; Khan et al., 2014) research has been conducted in Europe, Australia, and North America. This raises questions concerning the generalisability of social identity research in general to large areas of the world (Hopkins & Reicher, 2011).
Our previous research addressed some of these questions. Tewari et al. (2012) found that after attending a month-long pilgrimage event, pilgrims reported better self-reported health than a similar sample who did not participate. As there was no difference between these two groups prior to the event it appears that participation in the festival contributed to the post-event difference in health outcomes. This goes some way to addressing the first and third of our concerns listed before. However, the second concern remains. Analysing differences between two groups (pilgrims and nonpilgrim controls) before and after the event cannot address what aspects of collective participation are important and hence when collective participation will (or will not) have a positive health outcome. Indeed, it is conceivable that the pilgrims reported better health than controls because they were relieved to be home after a physically and psychologically demanding event (in which case group processes of whatever sort are irrelevant).
Accordingly, this paper addresses the social processes that could underlie the positive effect of mass gathering participation. This entails reporting data obtained from pilgrim participants whilst they were at the event concerning (a) their experience of a shared identity with other pilgrims, and (b) their social relations with other pilgrims (what we refer to as “relationality”). Specifically, we explored the degree to which between-individual variation in the experience of these two constructs explained between-individual differences in the longitudinal trajectory to participants’ self-reported health. That is, we report analyses of individual variation in the experience of social relations in the event to test a process model of collective participation and health outcomes.
Shared Identity at Mass Gatherings
There is much to be gained from investigating large-scale mass gatherings. The fact they bring together large numbers of people who have not met before allows investigation of the degree to which their social relations with each other are transformed through sharing a common social identity. The concept of a shared identity does not only entail a sense of identification with a group but also implies that crowd members view themselves and each other as identifying with the same social group and thus entails a sense of mutual recognition as common category members (Neville & Reicher, 2011). Evidence suggests such a shared identity may arise for various reasons. For example, although the behaviour of people in emergencies is often assumed to be selfish and individualistic, this can be misleading (Drury, Novelli, & Stott, 2013). Interview research with emergency survivors suggests that many experienced a shared social identity and that this resulted in mutual helping (Drury, Cocking, & Reicher, 2009).
However, a sense of shared identity at mass gathering events cannot be assumed and many empirical analyses of pilgrimage events show them to be characterised by sectarian division and factionalism (Messerschmidt & Sharma, 1981). This implies that the degree to which those attending a mass gathering actually experience a sense of shared identity is an empirical issue. So too, how such perceptions and experiences predict mass gathering participants’ well-being at the event (and after) is not known.
The Prayag Magh Mela
Our research was conducted at the Prayag Magh Mela in northern India. Several millions attend this event for a few days of its month-long duration. However, several hundred thousands remain for the full month. Known as Kalpwasis these latter pilgrims live in basic conditions exposed to various stressors (e.g., cold and noise: Pandey et al., 2014; Shankar et al., 2013). Kalpwasis are easily distinguishable (e.g., by their living area in the Mela site and their routines) and differentiate themselves from others attending the Mela for only a few days (Hopkins et al., in press). This provides a basis for Kalpwasis to see each other as sharing a social identity; and interview research (Hopkins et al., in press) reveals this shared identification can be manifested (for example) in their mutual greetings (for a discussion of the role of normatively prescribed greetings in the mutual recognition of identities, see Hopkins & Greenwood, 2013).
However, as noted before, such a sense of shared identity is not inevitable and we consider how variations in this are associated with participants’ reports of their social relations with others, and how these in turn are associated with their self-reported health at and after the event.
Hypotheses
We hypothesised that to the degree that Kalpwasi pilgrims perceived a shared identity amongst Kalpwasis, they would experience more supportive social relations and better self-reported health at and after the event (compared to before the event). Specifically, we predicted a curvilinear trajectory to participants’ self-reported health from before to after the event (with it peaking during the event), and that the more participants perceived a shared identity at the event: (a) the greater the pre-event to during-event health boost; (b) the greater the pre-event to post-event health boost; and (c) the greater the curvilinear trajectory in participants’ self-reported health.
Method
Sample
The sample conmprised 416 Kalpwasi pilgrims participating in the 2011 Magh Mela. On average they had attended the event on 10 previous occasions. Their age ranged between 28 and 92 years (M = 64.38, SD = 9.32 years); 237 (57.0%) were female; 384 (92.3%) belonged to the general caste (GC) category; and 32 (7.7%) to the other backward class (OBC) category (OBC is a categorisation referring to lower castes); 327 (78.6%) were married and 89 (21.4%) widowed; 177 were illiterate (42.5%), 192 (46.2%) held primary to intermediate education and 47 (11.3%) were university educated. Data were gathered at three time points: pre-event (T1), during the event (T2), and post-event (T3). 1
Measures
Data were gathered through an orally administered (Hindi) questionnaire. The scales were developed through extensive piloting and were translated and back-translated (English–Hindi–English) by two independent groups. Any differences in the translations were resolved by revising the items. The final items were piloted again to ensure intelligibility.
The questionnaires were administered by a team of 10 Hindi-speaking field investigators at three time points. On each occasion participants reported their health. During the event, they also reported on their perceptions of shared identity and inter-Kalpwasis relationships. Answers were obtained on a 5-point scale illustrated with drawings of five glasses containing increasing levels of water (ranging from empty to full). These were anchored: 1 = not at all and 5 = completely (which conceptually translates into English as a lot). The scale items were as follows:
Self-assessed health (SAH)
Participants completed three items based on the core module of the Centers for Disease Control and Prevention (2000) Health Related Quality of Life Measure (CDC HRQOL-14): “Over the last week, how would you describe your physical health”; “Over the last week, how would you describe your state of mind”; “Over the last week, how would you describe your energy levels?” 2
Symptoms of ill-health (SI-H)
Participants completed six items taken from a scale developed for use in the Indian subcontinent (Ruback, Pandey, & Begum, 1997) to capture something of the somatisation of stress believed to be particularly important in non-Western settings (Kirmayer & Young, 1998). Using the stem “Over the last week, to what extent have you…” the items included: “…felt anxious without any reason”; “…felt restless without any reason”; “…felt irritable without any reason?”; “…suffered from body-aches and pains”; “…suffered from breathlessness”; “…suffered from headaches?”
Shared identity
Five items measured the extent to which respondents perceived Kalpwasis attending the Magh Mela as having a shared identity. Using the stem “To what extent do you think that all Kalpwasis…” the items were: “…think of themselves as part of a single group?”; “…think of themselves as part of one large family?”; “…have a sense of ‘we-ness’ with other Kalpwasis?”; “…besides their differences, share the same identity?”; “…have a feeling of unity amongst each other?” These data were gathered during the event (T2).
Relationality
Five items measured the degree to which participants experienced their interactions and relations with other Kalpwasis to be respectful, understanding, and supportive. Using the stem “To what extent do other Kalpwasis…” the items were “…behave towards you in a respectful manner?”; “…behave towards you with understanding of your needs as a Kalpwasi?”; “…behave towards you in a way that allows you to fulfil your Kalpwas?”; “… demonstrate feelings of love to you?”; “… help you when you need it?” These data were gathered during the event (T2).
Procedure
Initially, participants were recruited through local contacts in the rural areas surrounding Allahabad. These then suggested others in the neighbourhood who could be approached.
The researchers identified themselves as coming from the University of Allahabad and as being interested in villagers’ lives and experiences. They then gave an overview of the questionnaire’s contents and addressed any questions that potential participants raised. After this, consent was sought (“Do we have your consent to participate in this survey study?”). The explanation of the research, the request for consent, and the giving of consent were all oral due to literacy issues (this was approved by the ethics committees of the universities of Allahabad and Dundee). No incentives were offered for participation.
The T1 survey was administered approximately one month before the beginning of the Magh Mela of 2011 (between the 1st and 15th of December, 2010). The T2 survey was administered at the height of the event (between the 26th of January and 9th of February, 2011). The T3 survey was administered to participants approximately one month after the event’s conclusion (between the 3rd and 15th of March, 2011). On average, the time difference between T1 and T2 ranged between 49 and 68 days (M = 55 days; SD = 4 days), between T2 and T3 it ranged between 24 and 43 days (M = 34 days; SD = 4 days), and between T1 and T3, it ranged between 83 and 99 days (M = 90 days; SD = 3 days). The data reported here are available at http://data-archive.ac.uk.
Results
Descriptive Statistics and Measurement Properties
The dimensionality of our T2 process variables (shared identity and relationality) was assessed using principal axis factoring (PAF) which is particularly suitable for measures that have not been used before (and as we were working in the distinctive cultural context of a Hindu pilgrimage event, our questionnaire items were necessarily created specifically for this study). PAF (with oblique rotation and explaining 64.46% of the total item variance) showed the items loaded onto two discrete variables corresponding to shared identity and relationality (eigenvalues: 5.17 and 1.97). The factor matrix appears in Table 1.
Factor structure of shared identity and relationality.
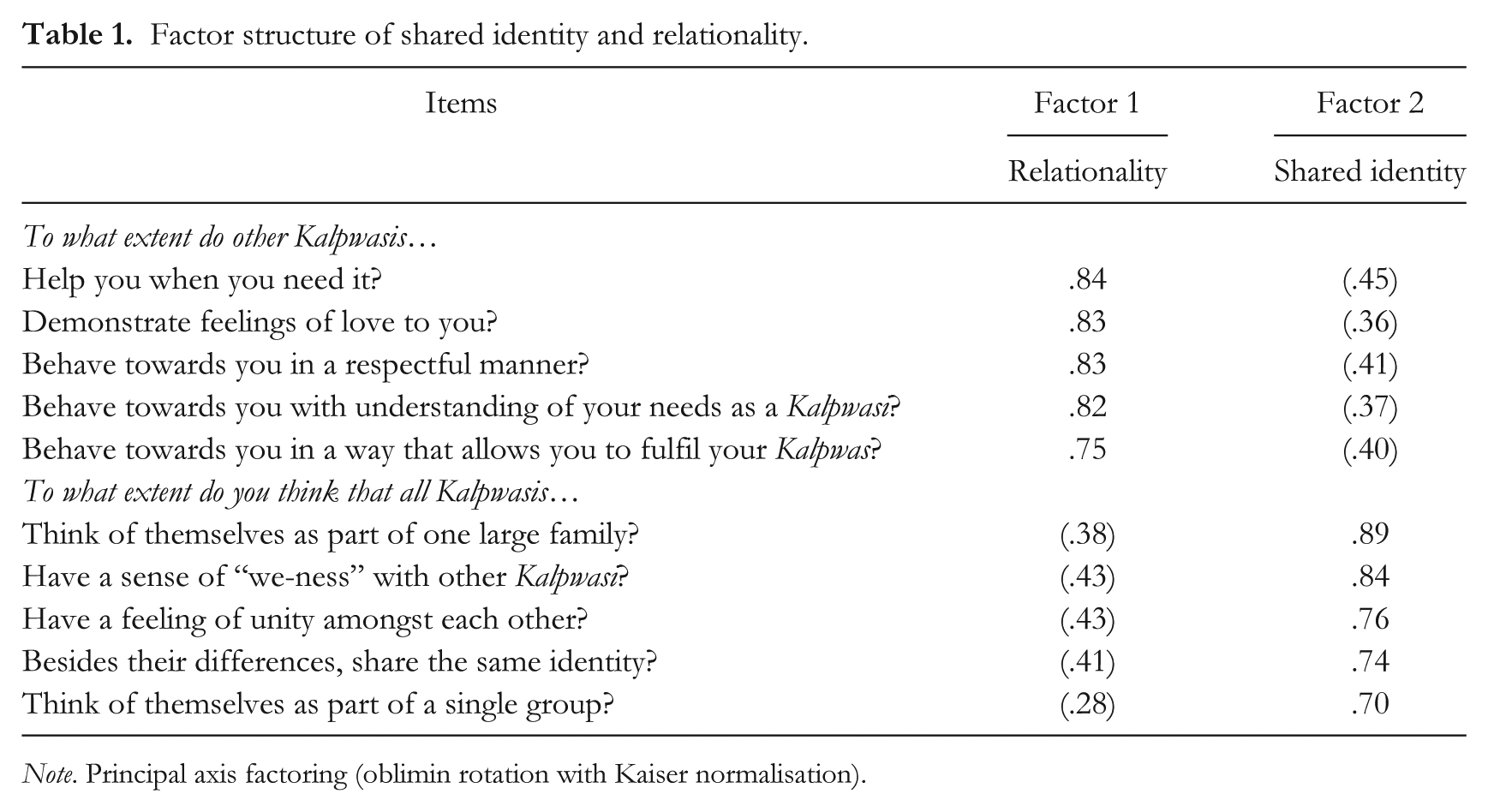
Note. Principal axis factoring (oblimin rotation with Kaiser normalisation).
The means, standard deviations, Cronbach’s alphas, and partial correlations between the measures (controlling for age, gender, caste and marital status, and education) are reported in Table 2. This shows that the reliabilities for all measures ranged between good and excellent across the three time points. It is also noteworthy that whereas the partial correlations revealed positive and significant bivariate relations between shared identity, relationality, and SAH at T2 and T3, neither shared identity nor relationality were correlated with SAH at T1. This indicates participants’ perceptions of social relations in the Mela were not contingent upon their prior (T1) SAH levels. In contrast, although T1 SI-H were not correlated with shared identity, T1 SI-H were correlated with relationality (which implies that one’s relations with others were affected by one’s symptomology).
Outcome and process variables: Estimated marginal means, standard deviations, Cronbach’s alphas and partial correlations.
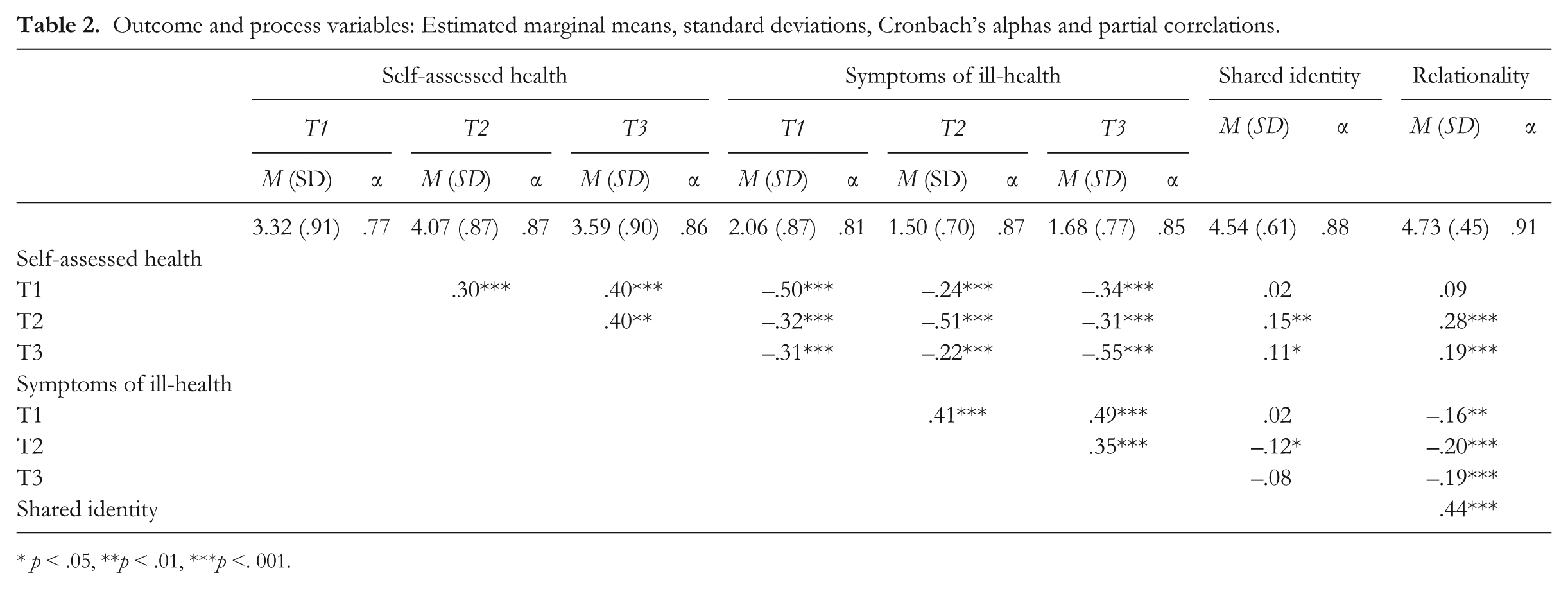
p < .05, ** p < .01, ***p <. 001.
Our analytic strategy had two stages. First, we examined the trajectory to participants’ self-reported health over T1, T2, and T3. Second, we examined the degree to which our process variables (shared identity and relationality) explained variation in this trajectory.
Self-Reported Health Over Time
Self-assessed health
Inspecting the data obtained at the three time points with a repeated-measures ANCOVA (controlling for age, gender, caste and marital status, and education) revealed no evidence of a linear trend, F(1, 409) = .08, p = .78, η p 2 = .00, but confirmed the data exhibited a quadratic (curvilinear) trend, F(1, 409) = 4.28, p = .04, η p 2 = .01 (T1 M = 3.32, SE = .004; T2 M = 4.07, SE = .004; T3 M = 3.59, SE = .004). Pairwise comparisons indicated significant differences between T1 and T2, t(415) = −14.40, p < .001, Cohen’s d = 1.41; between T2 and T3, t(415) = −5.59, p < .001, Cohen’s d = .55; and T1 and T3, t(415) = 9.89, p < .001, Cohen’s d = .97. Thus, SAH was better at T2 compared to both T1 and T3, and at T3 compared to T1.
Symptoms of ill-health
The data for the symptoms of ill-health revealed a similar pattern (T1: M = 2.06, SE = .04; T2: M = 1.50, SE = .03; T3: M = 1.68, SE = .04). Again there was no evidence of a linear trend, F(1, 409) = 0.33, p = .57, η p 2 = .00, but evidence for a quadratic trend F(1, 409) = 10.42, p = .001, η p 2 = .03. Pairwise comparisons indicated significant differences between T1 and T2, t(415) = 13.30, p < .001, Cohen’s d = 1.31; between T2 and T3, t(415) = −.4.30, p < .001, Cohen’s d = .42; and T1 and T3, t(415) = 9.20, p < .001, Cohen’s d = .90.
The Role of Shared Identity and Relationality: Regression Analyses
In order to investigate the role of our T2 process measures in explaining these health data we used hierarchical regression analyses. For both measures of health (SAH and SI-H) we explored how shared identity and relationality explained variation in (a) the T1–T2 health change and (b) the T1–T3 health change.
Self-assessed health: T1 to T2
Controlling for SAH at T1 and the sociodemographic variables (age, gender, caste and marital status, and education), we examined if shared identity and relationality explained variance in T2 SAH. For the analysis of the sociodemographic variables, the reference categories were: female, OBC (other backward classes or lower caste), widowed, and illiterate. The entry order of the variables in the model was as follows: Step 1: T1 SAH; Step 2: age, gender, caste and marital status; Step 3: education; Step 4: shared identity; and Step 5: relationality. The two process variables were entered separately in this order because theory and research shows shared identity to be a precursor of more supportive social relations between group members (Levine et al., 2005; Wakefield et al., 2011). The results are presented in Table 3.
Hierarchical regression model: Predicting self-assessed health at T2.
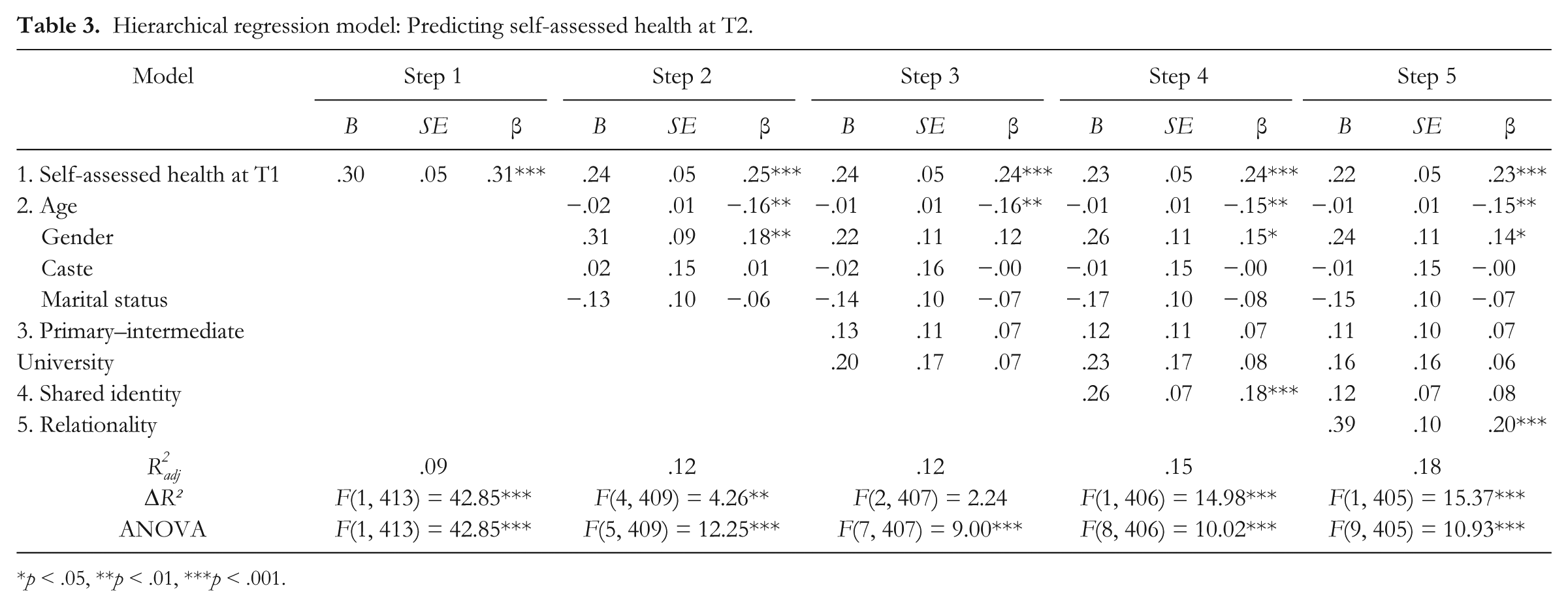
p < .05, **p < .01, ***p < .001.
The adjusted R2 values were significant at each step with the model as a whole explaining 18% of the variance in T2 SAH. The R2 change value was significant at all steps but the third, which indicates that the block consisting of the dummy-coded measures assessing education did not explain a significant proportion of variance in the model. Similarly, the standardised beta weights indicate that caste and marital status were non-significant at every step of the model that they were entered.
As expected, T1 SAH was the strongest predictor of T2 SAH, and was significant at every step of the model. Likewise, age was significant at every step, with younger participants experiencing greater levels of T2 SAH. Gender was significant at the second and fourth steps, with males experiencing significantly greater levels of T2 SAH than females. However, this effect was suppressed by the entry of education.
Shared identity and relationality were significant predictors at the fourth and fifth steps (respectively) and the effect of shared identity was suppressed by the entry of relationality. Shared identity and relationality were thus both found to predict a significant proportion of variance in T2 SAH, over and above the control variables. Besides the autoregressive effect of T1 SAH, the standardised beta weights for both shared identity and relationality in the fourth and fifth steps respectively showed the strongest effects.
Given that the introduction of relationality reduced the effect of shared identity on T2 SAH, we investigated whether shared identity had an indirect effect on T2 SAH via relationality. In this analysis shared identity was entered as the independent variable, relationality as the mediating variable, and T2 SAH as the dependent variable (and as before, T1 SAH and the sociodemographic variables were entered as covariates). Following recommendations by Aiken and West (1991) the predictor variables were standardised to avoid multicollinearity.
Using a bootstrapping procedure (PROCESS; Hayes, 2012) with 95% confidence intervals with 5,000 bootstrap samples, the bias-corrected and accelerated bootstrapped confidence intervals revealed an indirect effect of shared identity on T2 SAH via relationality (B = .08, 95% CI [.041, .137]). We also examined an alternative model. This investigated if the effect of relationality on T2 SAH was indirect via shared identity. This was not supported (B = .03, 95% CI [−.008, .084]).
Self-assessed health: T1 to T3
We examined the role of our process variables in explaining the T1 to T3 increase in SAH following the same analytic steps as mentioned. The results were very similar (Table 4). Shared identity and relationality were significant predictors at the fourth and fifth steps (respectively) and the effect of shared identity was suppressed by the entry of relationality. Again, the bias-corrected and accelerated bootstrapped confidence intervals revealed an indirect effect of shared identity on T3 SAH via relationality (B = .05, 95% CI [.009, .092]). We also examined an alternative model in which the effect of relationality on T3 SAH was indirect via shared identity. This received less support (B = .03, 95% CI [−.004, .072]).
Hierarchical regression model: Predicting self-assessed health at T3.
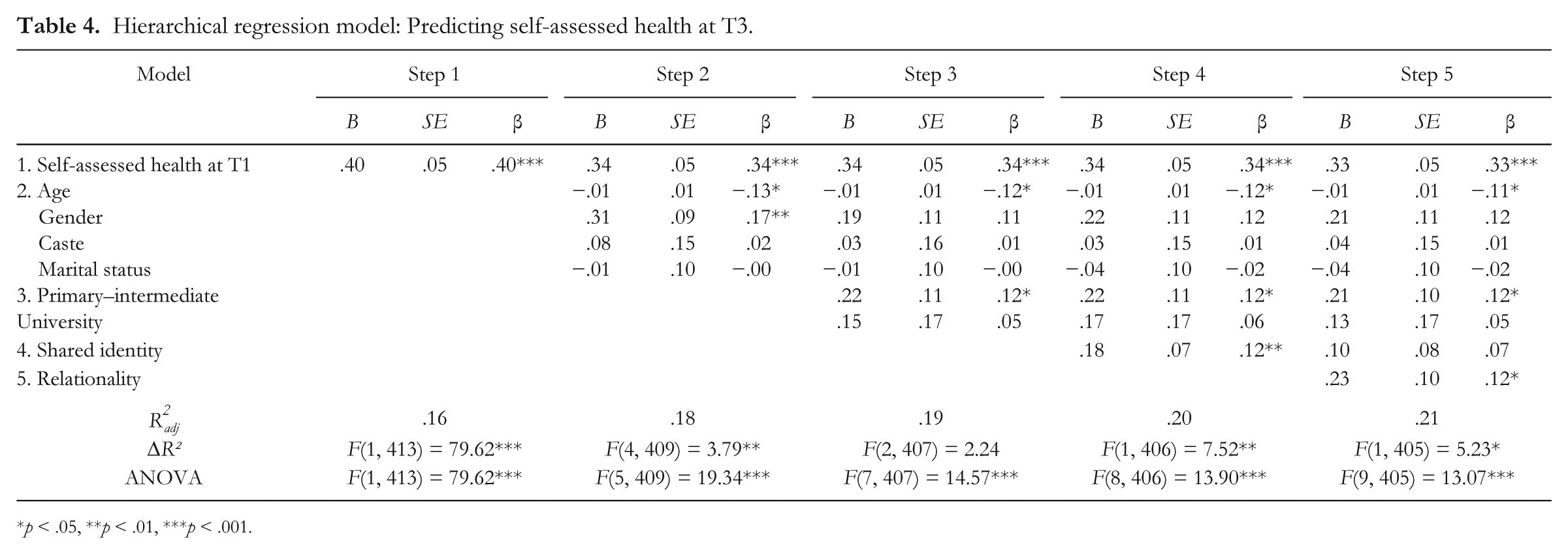
p < .05, **p < .01, ***p < .001.
Symptoms of ill-health: T1 to T2
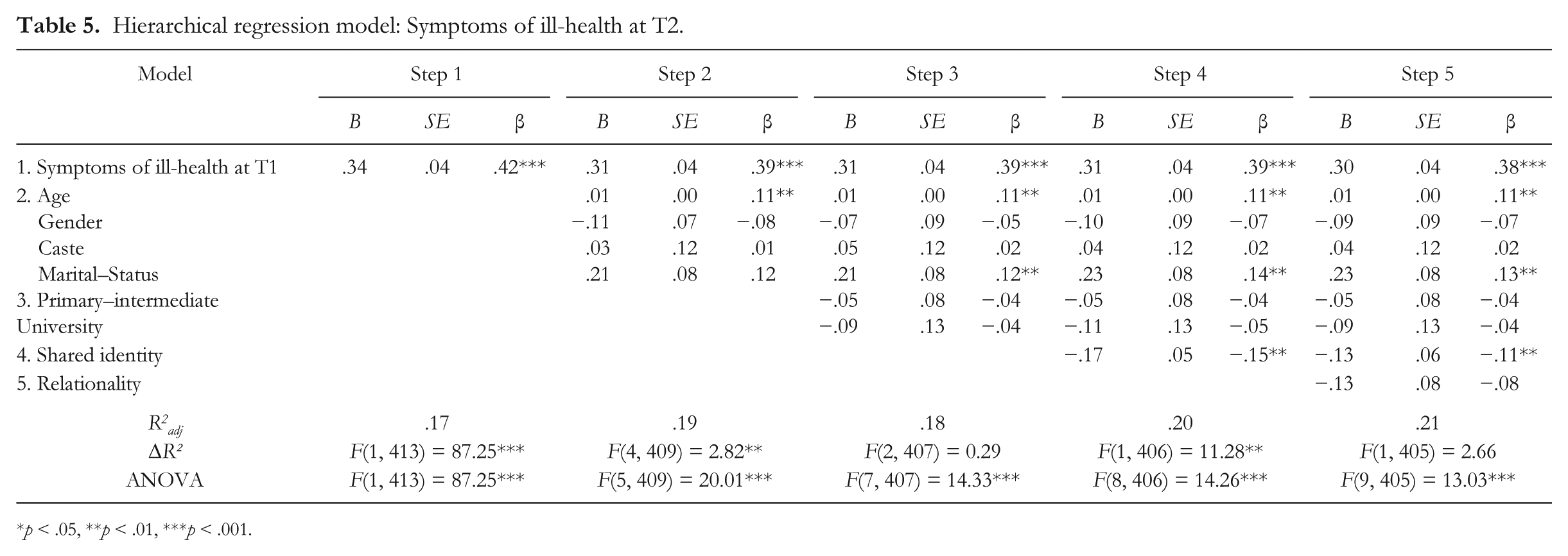
Repeating these analytic steps showed that shared identity was a significant predictor of T2 SI-H (Table 5), but that relationality added nothing.
Hierarchical regression model: Symptoms of ill-health at T2.
p < .05, **p < .01, ***p < .001.
Symptoms of ill-health: T1 to T3
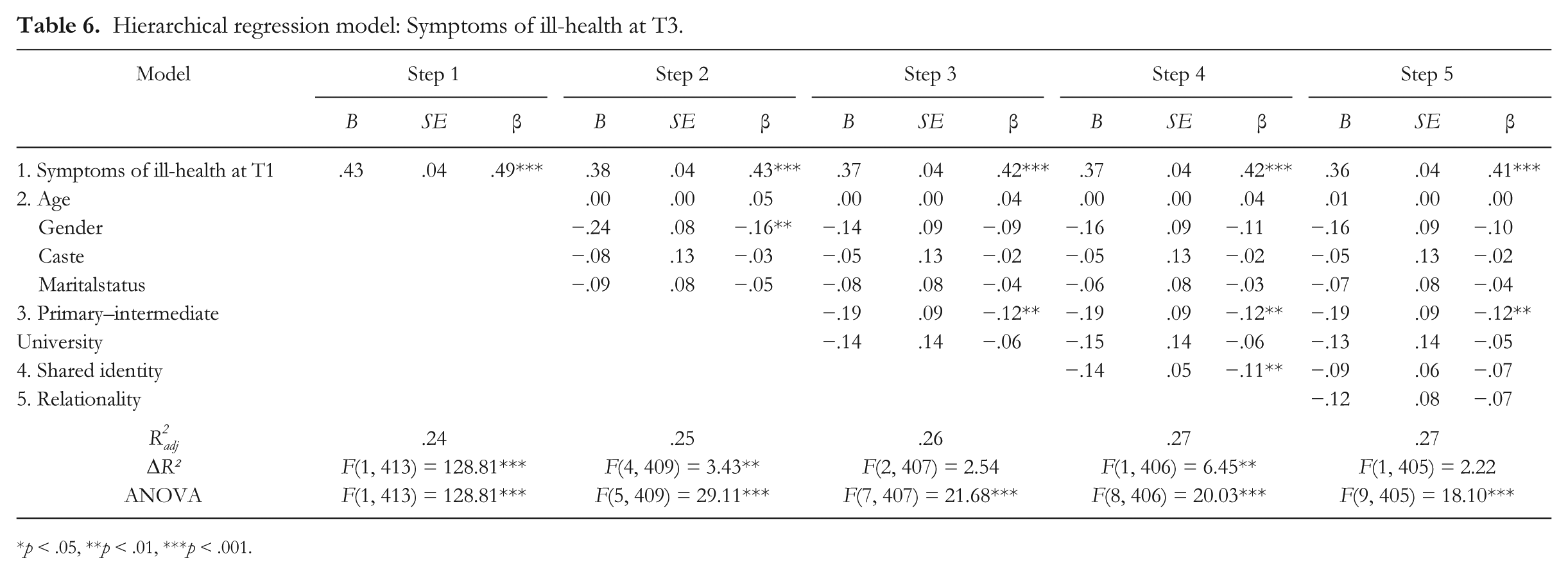
In similar vein, analyses of the T3 data showed that shared identity was a significant predictor of participants’ T3 SI-H (Table 6). Again relationality added nothing.
Hierarchical regression model: Symptoms of ill-health at T3.
p < .05, **p < .01, ***p < .001.
Thus far these four regressions provide good evidence for the role of shared identity in explaining both T1–T2 and T1–T3 health improvements (for both SAH and SI-H). With regard to SAH (but not SI-H) we also have evidence for the role of relationality in mediating this effect of shared identity.
Modelling the Curvilinear Trajectory to Health: Latent Growth Curve Analyses
Next, we examined the curvilinear trajectory to the SAH and SI-H data using latent growth curve modeling (LGCM; Duncan, Duncan, & Stoolmiller, 1994; McArdle & Epstein, 1987) in AMOS 17.0 (Arbuckle, 2008). We predicted that the curvilinear patterning to these data would be predicted by the T2 process variables. LGCM models are evaluated using the same criteria as for structural equation models (SEM). We used the comparative fit index (CFI), the root mean squared error of approximation (RMSEA), and the standardised root mean squared residual (SRMR) to evaluate model fit. Values of > .90 for the CFI and < .08 for the RMSEA and SRMR indicate acceptable fit between a specified model and observed data (Hu & Bentler, 1999; MacCallum, Browne, & Sugawara, 1996). Although we report the chi-square statistic for the models, we do not rely on it in evaluating model fit because of its sensitivity to large sample sizes (> 200; Kline, 2005). The Akaike information criterion (AIC; Akaike, 1987) is reported for the purpose of comparing nonnested models (Burnham & Anderson, 2004).
Self-assessed health
The LGCM analyses were conducted in two steps. First, a curvilinear growth curve model was constructed for SAH across the three time points of measurement (see Figure 1). This model had two latent factors. The first represented the intercept, corresponding to initial (i.e., T1) levels of SAH. This is a constant (and the loadings of the observed variables were thus constrained to 1). The second factor represented the slope (rate of change) in SAH from T1 to T3 (and the curvilinear change trajectory was specified by fitting a model with the slope factor loadings for T1, T2, and T3, being 0, 2, and 1, respectively).
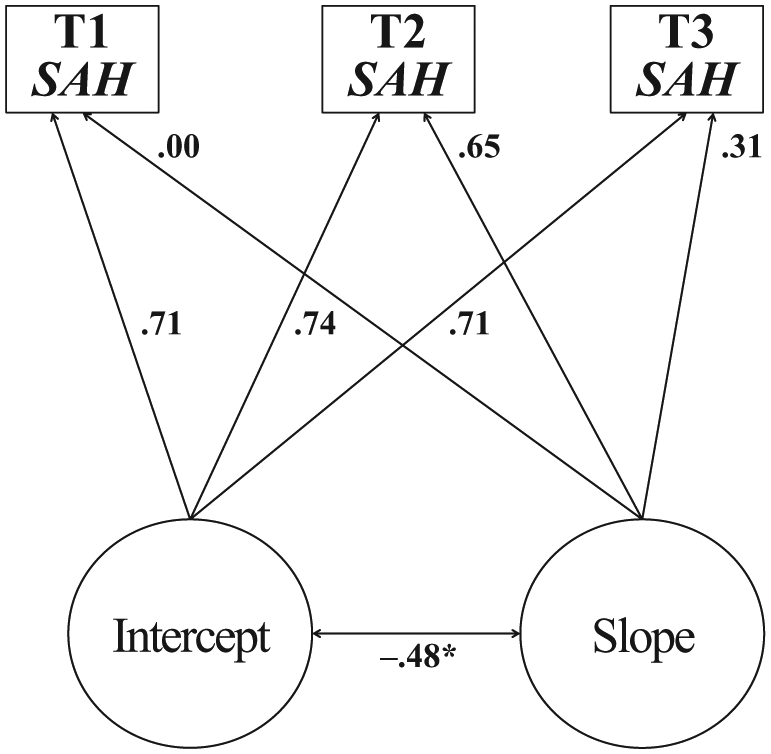
First LGC model: Estimating the change in self-assessed health across T1, T2, and T3.
Other than the relatively high RMSEA value (explicable in terms of the small number of degrees of freedom in the model: Kenny, Kaniskan, & McCoach, 2013), the fit indices indicated good model fit, χ2 = (34) 6.03, p < .001, χ2/df = 6.03, CFI = .97, RMSEA = .10, 90% CI [.040, .201], SRMR = .00. The estimates for the slope-variable paths corresponded to our curvilinear specification of the growth curve and the mean estimate for the slope was positive and significant (β = .37, p < .001), indicating that SAH increased curvilinearly from T1 to T3, reaching its highest levels at T2.
In the second step, we investigated the role played by our two process variables (shared identity and relationality) in explaining this trajectory. Shared identity was entered as an antecedent of relationality (see Figure 2).
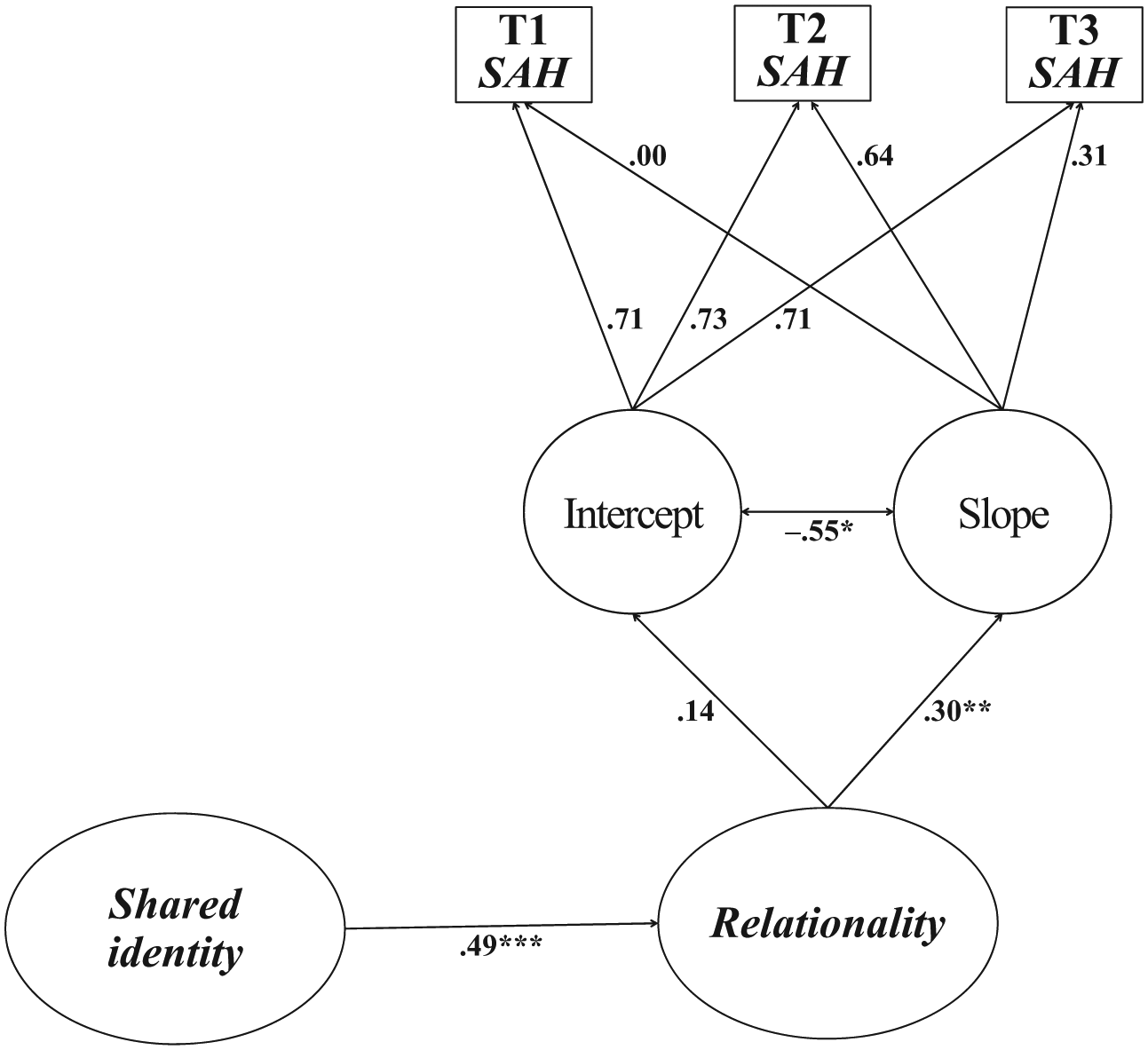
Second LGC model: Predicting the antecedents of the change in self-assessed health across T1, T2, and T3.
The model fit was again good, χ2= (62) 208.75, χ2/df = 3.31, CFI = .95, RMSEA = .07, 90% CI [.064, .086], SRMR = .04, AIC = 290.75. This model showed that shared identity was a (positive) predictor of relationality, and that relationality positively predicted the curvilinear growth in SAH from T1 to T3 (β = .30, p < .001; R2 = .09). This indicates that the curvilinear increase in SAH from T1 to T3 was a direct function of the degree to which participants experienced their interactions and relations with other Kalpwasi pilgrims to be respectful, understanding, and supportive, and that this latter was a function of participants’ perceptions of shared identity with other Kalpwasis. Furthermore, while not depicted in the model, the indirect effect of shared identity on the curvilinear increase in SAH from T1 to T3 via relationality was positive and significant (β = .15, p < .001). 3
We then examined if the role of shared identity and relationality identified in this second growth curve model remained after the sociodemographic variables (age, gender, caste and marital status, and education) were included as predictors of the intercept and slope. The results for this model also revealed a good fit, χ2 = (113) 289.50, p < .001, χ2/df = 2.56, CFI = .95, RMSEA = .06, 90% CI [.053, .070], SRMR = .05, AIC = 441.50. In addition to showing that age (β = −.28, p < .001) and gender (β = .36, p < .001) predicted initial levels of SAH (younger participants and males experienced better T1 SAH), the results confirmed the role of our process variables in explaining the curvilinear increase in SAH from T1 to T3. Specifically, relationality was the only significant direct predictor of the curvilinear increase in SAH from T1 to T3 (β = .31, p < .01; R2 = .13) with the effect of shared identity upon the curvilinear increase in SAH from T1 to T3 being indirect (β = .15, p < .001). 4
As in our earlier analyses we also investigated the adequacy of alternative models in which the ordering of the process variables was reversed. Specifically, we investigated if the effect of relationality on the curvilinear increase in SAH from T1 to T3 was indirect via shared identity. This alternative model exhibited a significantly poorer fit than the hypothesised model, χ2 = (63) 231.066, p < .001, χ2/df = 3.67, CFI = .94, RMSEA = .08, 90% CI [.069, .091], SRMR = .06, AIC = 313.07; ΔAIC = 22.32. This finding was repeated when the hypothesised model and the alternative model included the sociodemographic variables entered as predictors of the intercept and slope, χ2 = (113) 307.73, p < .001, χ2/df = 2.72, CFI = .94, RMSEA = .06, 90% CI [.056, .073], SRMR = .06, AIC = 459.73; ΔAIC = 18.23.
Symptoms of ill-health
As relationality did not add anything to the explanation of the T1–T2, nor the T1–T3 changes in SI-H, we investigated the symptom data with a simplified LGCM—one that only included shared identity as a predictor of an (inverted) curvilinear trajectory in symptoms. We obtained a good model fit whether or not we included the sociodemographic variables as predictors: without covariates: χ2= (19) 75.07, χ2/df =3.95, CFI = .96, RMSEA = .08, 90% CI [.065, .105], SRMR = .04, AIC = 125.07; with covariates: χ2 = (44) 119.40, χ2/df = 2.71, CFI = .96, RMSEA = .06, 90% CI [.051, .078], SRMR = .04, AIC = 239.40. With regard to the role of shared identity we found that without the covariates shared identity was a very marginal predictor of the slope (intercept: β = −.08, p = .24, slope: β = −.06, p = .10). However, with the covariates included in the model, the role of shared identity in predicting the slope was stronger and approached significance (intercept: β = −.02, p = .84, slope: β = −.08, p = .052).
Discussion
Our findings provide good support for our hypotheses. First, pilgrims’ self-assessed health (SAH) was higher during the event than before, and declined from during the event to after it was over. Yet it remained higher after than before. Similarly, participants reported reduced symptoms of ill-health (SI-H) at the event, and although these increased after the event, they remained less than before. This implies the improvement associated with participation in the mass gathering cannot be put down to a contrast effect (the Mela is so gruelling that, once home, people feel better as a result). It is rather the opposite: the Mela is experienced as invigorating and something that remains afterwards.
Second, we found that the improvement in SAH and in SI-H from before (T1) to during the event (T2), and from before (T1) to after the event (T3) were (partially) explained by participants’ sense of shared social identity during the event. Moreover, with regard to SAH we found that this effect of shared identity was mediated by our measure of relationality. This implies that the more those attending this mass gathering experienced a sense of shared identity, the more they experienced more intimate and supportive social relationships, and, compared to the T1 baseline, the better their T2 and their T3 SAH.
Third, considering the three time points together, the latent growth curve modelling of the SAH data confirmed the role of shared identity in explaining pilgrims’ health trajectories via relationality. For the SI-H data the role of shared identity in predicting the slope was marginal. Overall, then, these results complement and extend previous analyses of how mass gathering participation is associated with health benefits (Tewari et al., 2012). This is particularly clear with regard to the SAH data
Why relationality did not feature in the explanation of the SI-H data is unclear. We suspect that it may be because this measure has different properties. In this context it is noteworthy that the scales’ correlations ranged between −.50 and −.55 over the three time points (see Table 2). Whereas the SAH measure draws upon an internationally validated scale, the SI-H measure is an Indian scale designed to capture something of the somatisation of stress believed to be particularly important in non-Western settings. But it may also be sensitive to the physical difficulties posed by camp life (e.g., sleeping on the floor). Indeed, it is noteworthy that the effect of mass gathering participation on these scales reported by Tewari et al. (2012) differs in magnitude (greater on the internationally validated SAH measure). Yet, despite the likelihood that these two measures are sensitive to rather different aspects of health it is important to note that on both scales we obtain clear evidence from our regression analyses for the role of shared identity in explaining the T1 to T2 and the T1 to T3 improvements in health associated with participation.
Any extrapolation from this event to others must proceed with caution. Just as it is true that not all individuals in an event will have the same degree of shared identity (and so will not experience the same positive subjective health benefits), so it is true that shared identity may be harder to establish at some events than others (Messerschmidt & Sharma, 1981). Our case is not that all participants in all mass gatherings by the mere fact of being there experience a shared identity, a transformation of social relations, and improved health. Ours is a process account which stresses that to the degree a shared identity is perceived, and social relations experienced as more intimate and supportive, then subjective health can be enhanced.
Additionally, while we have shown that shared identity is associated with improved subjective health at and after the event, we do not suggest that this explains everything. For example, the fact the event is religious is important: religious belief can impact health through encouraging positive cognitions and meditative practices (James & Wells, 2003). However, it is also important to remember that religious belief can create a sense of group membership and shared identity with coreligionists (Graham & Haidt, 2010; Ysseldyk, Matheson, & Anisman, 2010). Indeed, there is evidence that this sense of collectivity (and the supportive social relationships that result) contributes to the health benefits associated with being religious (George, Ellison, & Larson, 2002; Lim & Putnam, 2010) and that a religious identification may be particularly beneficial because it may allow one to establish contacts with others that one does not know. For example, older adults who are religious may find a move into residential care easier because they more easily join and establish new face-to-face groups (Ysseldyk, Haslam, & Haslam, 2013).
All this means that any extrapolation to other events must attend to the characteristics of the events in question: A shared identity may be more readily achieved at some events than others. Also, it is important to attend to the behavioural norms associated with group membership. For example, Howell et al. (2014) found that amongst a student group, participants who were more central to the group reported positive health-related outcomes (e.g., feeling happier and more efficacious in dealing with stress). However, they also reported engaging in riskier behaviour (e.g., binge drinking). This mix of effects highlights the importance of attending to the social norms within the group for it is quite conceivable that the health benefits of shared identity brought by social support could be outweighed by the costs of unhealthy group practices.
Future work on mass gatherings could extend our own in various ways. Most obviously it is important to consider the benefits and processes operating in other types of events (e.g., music festivals). Furthermore, research could also employ more complex measures. Mass gatherings such as the Prayag Magh Mela entail a variety of interactions. Some involve previously known others (e.g., family members, friends). Others involve strangers for whom the only information available concerns their group membership (in this case whether they are a Kalpwasi). Our interview research (Hopkins et al., in press) suggests that a shared identity transforms unknown others from people with whom one has absolutely no psychological connection into people who (although one does not know them personally) are at another level one’s fellows. Future quantitative research could more directly investigate this with measures that differentiated between participants’ perceptions of their relationships with known and unknown others. Also, although self-report measures of health correlate with more objective measures (see Schnittker & Bacak, 2014), future research could also complement the use of self-report measures of health with physiological measures of health and examine the time course to such effects through gathering data at multiple (post-event) points.
With these qualifications in mind, our study suggests two broader lessons. One concerns the social bases to people’s sense of their health and well-being. We extend current understanding by showing that the benefits of social relations derive not just from social networks (e.g., Helliwell & Putnam, 2004; Lim & Putnam, 2010) and established small groups (e.g., Haslam et al., 2005), but can extend to mass gatherings. We also extend understanding by providing a clear idea of the processes involved: improvements are facilitated by shared identity. Our research also extends understanding through using a longitudinal design (pre-event, during event, and post-event), which allows us to show that the social identity processes we investigated during the event predicted participants’ self-reported health over time. This represents a significant addition to the existing research on identity and subjective health and well-being (which is typically cross-sectional). We also demonstrate that these processes apply outside the western world where most of the research on social relations and the “social cure” (Jetten et al., 2012) has been conducted (see too Khan et al., 2014).
The other lesson concerns the understanding of mass gatherings. Typically, these are seen as sites of irrationality where people act against their own best interests, and where, through panic, they are liable to harm themselves as well as others (e.g., Drury et al., 2009). Similar themes are apparent in medical approaches to mass gatherings which focus on the risks of infectious diseases, dehydration, exposure, crowding, stampedes, etc. (e.g., Steffen et al., 2012; Tam, Barbeschi, Shapovalova, Briand, & Memish, 2012). It would be reckless and foolish to suggest mass gatherings are risk-free (for data on the spread of diarrhoea and the risks associated with vibrio cholera at the site we studied, see Ayyagari et al., 2003). But not everyone will be affected and for those who aren’t, mass gatherings can be positive experiences with positive outcomes. Future research should therefore be sensitive to the mix of health benefits and risks associated with mass gathering participation. Indeed, it is likely that the benefits associated with shared group membership are important in attracting participants. Moreover, research could address how the experience of shared identity could impact upon mass gathering participants’ own health-related practices (for good or ill). For example, it is possible that the relational intimacy that benefits health could also lead individuals to lower their guard when it comes to sharing items that could facilitate infection transmission (e.g., sharing drinking utensils, razor blades, toothbrushes, etc.). Moreover, the subjective experience of improved health at the event could undermine the credibility of sound health advice (e.g., concerning mask-wearing or hand-washing; Gautret et al., 2011). Getting mass gathering participants to take official health-related warnings seriously can be difficult (Hutton, Roderick, & Munt, 2010) and this may be all the harder if participants themselves are experiencing heightened well-being at the event. By bringing together the medical and the social psychological analysis of mass gatherings we may achieve a far richer understanding of how groups are good for us, how they are bad for us, and even how what is good at one level can be bad at another.
Footnotes
Acknowledgements
We thank Kavita Pandey, Shail Shankar, Mark Levine, and Gozde Ozakinci for comments.
Funding
We thank the ESRC for funding (RES-062-23-1449).