
Abstract
Navigating through a child’s cancer treatment journey is challenging for a family. Understanding family members’ experiences helps identify their needs and how they can be supported during a child’s cancer treatment. This study aimed to explore parents’ perceptions of how their child’s cancer treatment impacts family members’ well-being and family dynamics. Semi-structured interviews with parents of children diagnosed with cancer (N = 18) were conducted to explore parental perceptions of family members’ experiences. Data were analysed using reflexive thematic analysis. Four themes were generated: disruption to daily life and relationships, impact on siblings, parents’ emotional and psychological impact and role changes, and navigating separation and family dynamics during treatment. This study provides important contributions to a broader understanding of how family members are affected, from a parental perspective, during childhood cancer treatment in the UK. Enforced separation of family units during hospital stay has an impact on family dynamics and family members’ well-being. This study highlights parents’ need for support and important considerations for healthcare professionals implementing family-based support during paediatric cancer treatment.
Introduction
Around 1600 children aged 14 and under receive a cancer diagnosis in the United Kingdom (UK) annually (NHS Digital, 2024). During treatment, children experience side-effects including lack of energy, pain, and nausea (Collins et al., 2000; Yeh et al., 2008). Patients experience many challenges when undergoing invasive treatments and procedures that have adverse side-effects (Ness and Gurney, 2007). These side-effects, along with long hospital stays, prevent patients from attending school, participating in activities, and seeing their friends (Gibson et al., 2010).
Impact of childhood cancer for family members
Parents face long-term psychological effects including anxiety, depression, and sleep disturbance (Hartley et al., 2021). Mothers have shown increased symptoms of anxiety, depression, distress, and poorer family functioning compared to fathers (Peterson et al., 2020). During treatment, parents report a greater need for social support to help them cope (Bretones Nieto et al., 2022; Maynard and Bennett, 2024). Yet during treatment, many parents’ social support network shrinks (Lundgren et al., 2023).
Studies involving siblings have shown mixed outcomes on their quality of life, post-diagnosis (Alderfer et al., 2010). Mean levels of anxiety and depression in siblings are similar to siblings in families unaffected by cancer (Long et al., 2018); however, a significant subgroup of siblings experience a poorer quality of life (especially in emotional, social, and family domains) (Alderfer et al., 2010). Importantly, in many families, siblings report a more detrimental impact on their well-being than their parents are aware of (Pariseau et al., 2020).
Most family units change to accommodate the treatment schedules, with one caregiver staying with their child in the hospital, whilst another caregiver or family member maintains the family home (Hjelmstedt et al., 2021). Parents often try to maintain normality and routine for their family whilst navigating through disruptions and turmoil during treatment (Moridi et al., 2018). Additionally, many parents are required to juggle caring responsibilities for their child with cancer, alongside paid work, and household and family responsibilities (Hjelmstedt et al., 2021).
Family functioning and relationships are affected following diagnosis (Rabineau et al., 2008). Although children living with cancer’s sibling and maternal relationships strengthen, parent-sibling relationships become strained (Winter et al., 2013). Additionally, parents’ increased caregiving demands during treatment leads to less attention on siblings, and difficulties in balancing the needs of all family members (Lewandowska, 2021; Long et al., 2018). Supporting family relationships during treatment can assist family functioning (Meyler et al., 2010).
Why this research is needed
Understanding parents’ experiences provides researchers with insight through the vivid retelling of the occurrence (Mapp, 2008). Siblings are a complex and poorly understood group who are under-prioritised in support services (Brosnan et al., 2022). Understanding parents’ perceived impact on family members and their approaches to managing the challenges of childhood cancer treatment can highlight families’ support needs (Darlington et al., 2021). Existing qualitative research within the paediatric oncology context has focused solely on experiences of individuals such as mothers (Davies & O’Connor, 2023; McEvoy and Creaner, 2021), fathers (Davies et al., 2023), or siblings (Van Schoors et al., 2018). Family-focused perspectives are key as a family is a complex system of interacting individuals (Bowen, 1978). Parents are uniquely placed to provide insights into family members’ experiences, their emotional and practical needs, and overall family functioning. Therefore, there is a need to explore parents’ perspectives of their family member’s experiences during treatment to understand the broader family impact, identify their family’s needs and design supportive interventions informed by lived experiences. Parents are key stakeholders whose input in designing support strategies for family members would increase the feasibility and effectiveness of support (Skivington et al., 2021).
Aim
To provide a holistic insight into the impact of childhood cancer on family members’ well-being and family dynamics during a child’s treatment for cancer. These insights from a parental perspective will inform the co-design of effective support.
Methods
Design
Semi-structured interviews with parents of children living with and beyond a cancer diagnosis in the UK were conducted. This was part of a wider study to research parents’ experiences of physical activity for family members during treatment (currently under review). The study was approved by Loughborough University Ethics Committee (approval: 2022-6811-9765). A patient and public involvement (PPI) group was established, consisting of two parents with lived experience of their child diagnosed with and treated for cancer. These individuals were known to the lead researcher, and they contributed to the research design.
Recruitment and screening
Parents who met the eligibility criteria were recruited. Eligible parents were (a) over 18 years old, (b) primary caregivers with parental responsibility, (c) able to communicate in English and (d) parents of a child diagnosed with cancer in the UK. The child must have been diagnosed between the ages of 3 and 16 years. At the time of recruitment, the child must have either completed treatment within the past 5 years or, if they were still undergoing treatment, it must have been at least 3 months since the diagnosis. Individuals who did not meet these inclusion criteria were excluded.
The age of three was chosen as at this age children typically develop their physical and communication skills and participate in physical activities such as walking, running, and jumping. Including children diagnosed from age three, allows exploration of disruptions to typically established family routines caused by illness, which is a topic of discussion in the interviews. To capture diverse experiences, parents of children undergoing treatment, those who had completed treatment and bereaved parents were included. Parents who had completed treatment may offer deeper reflections after time to process, while parents currently on treatment may have fresher, more vivid insights. Bereaved parents’ grief might affect recall, but their insights are valuable. If parents wanted to share information on their loss and grief, this was considered sensitively. The inclusion criteria were informed by discussions with the PPI group who supported the inclusion of bereaved parents. Parents were purposively recruited through social media posts shared by childhood-cancer-related charities. A snowball approach was directed towards reaching more fathers, through sharing recruitment material with networks supporting fathers and asking parents to share with other potentially eligible parents. Prior to the interview, participants provided written informed consent.
Due to the sensitive nature of this research, in an initial phone call between parents and the researcher, the eligibility and suitability of the parents were checked. Details about their child’s diagnosis and treatment were collected. Participants were encouraged to ask questions during this call and before the interview. Interviews were arranged at convenient times for participants. Study documents were emailed. Participant information and post-interview sheets included details of relevant support organisations. During the interview, participants were informed they could take a break or stop the interview at any point to reduce distress.
Data collection
Semi-structured interviews were conducted using an interview guide (Supplemental Material) with open questions focused on the impact on their own mental and physical health, as well as their whole family’s experience such as ‘How do you think the whole family’s physical and mental health has changed since your child’s diagnosis?’ Prompt questions further explored participants’ answers. The interview guide wording was informed by discussions with the PPI group to ensure there was the required sensitivity. The lead researcher has experience in talking with parents about sensitive topics as an experienced primary school teacher and with children diagnosed with cancer and their families through their role with a charity. She was not known to the participants. There were opportunities to debrief within the research team if the researcher needed support after the interview. Recruitment ceased when the research team decided saturation had been reached using information power to guide the decision. As the participant group was small, and more in-depth data were gained, fewer participants were needed (Malterud et al., 2016).
Data analysis
Data were analysed using reflexive thematic analysis (Braun and Clarke, 2019), a flexible approach to identify associations within and across accounts (Braun and Clarke, 2017). Interviews were transcribed verbatim by the lead researcher and anonymised with pseudonyms.
The lead researcher engaged inductively with data during interviews and transcription, reflecting on and becoming familiar with participants’ accounts before coding and theme development (Braun et al., 2016). Printed copies of transcripts were annotated for analysis, and NVivo software (Lumivero, v14.23.0) was used to organise analysis of interview data. Trustworthiness of the findings was ensured by considering credibility, dependability, and transferability, supported through peer debriefing and critical discussions during coding and theme development (Morse, 2015; Nowell et al., 2017). Within the research team, coding was discussed, assumptions challenged, and themes were explained and justified (Smith and McGannon, 2018). Final themes were agreed on by all authors. The lead researcher maintained a reflective log to document ideas and discussions, this formed part of an audit trail, including development diagrams and transcripts (Nowell et al., 2017).
Findings
There were 17 mothers and 1 father interviewed. The children had a median age at initial diagnosis of 4.5 years (IQR = 3). All the children received chemotherapy during treatment, alongside other treatments such as radiotherapy (including proton beam therapy) and surgery. The participants’ children were at different stages of treatment; 2 parents had children on treatment, 14 had completed treatment and 2 parents were bereaved. The first two interviews were supervised by another researcher.
Summary of demographic and clinical characteristics of participants. Includes the child’s sex, number of siblings, age at diagnosis, diagnosis type, and current treatment stage.
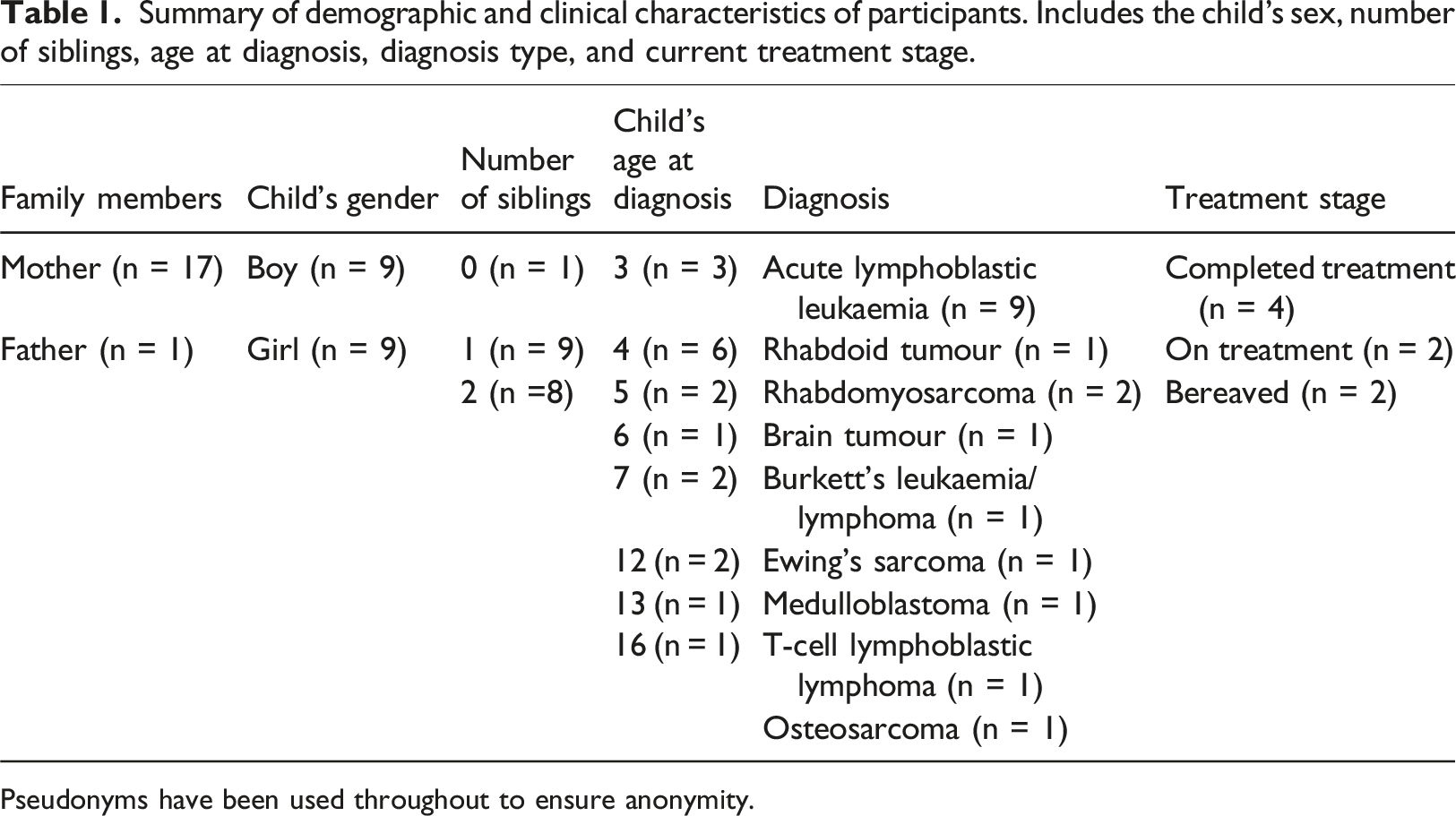
Pseudonyms have been used throughout to ensure anonymity.
Four main themes representing experiences of family members were generated: disruption to daily life and relationships, impact on siblings, parent emotional impact and role changes, and how parents navigated separation and family dynamics during treatment.
Disruption to daily life and relationships
From diagnosis, family routines and relationships were affected and family functioning was adversely impacted. Many participants felt like everything stopped after their child’s diagnosis. ‘…when you first are in treatment it…it's just knocks you off your feet. You know nothing was the same. Nothing. Nothing at all was the same…. She wasn't going to school. …You know you're trying to cope with everything. You're not going to work. Everything is completely different then’ (Ebony).
After diagnosis, the hospital became a central feature of their lives. Even when at home, parents were constantly vigilant for signs they may need to return to hospital. ‘…I just became totally institutionalised. Just lived in hospital. When we weren't in hospital, I've got my hospital bag packed. I could … check his temperature at any point day or night twenty-four seven and, and if you spike, I had an hour to get into hospital. Just life is on hold …’ (Bryony).
Parents experienced changes in their relationships. Whilst in hospital, many parents reported feeling trapped ‘inside a bubble’, confined to a small room with limited opportunities to access the outside world. ‘…so that was hard cause you’ve got no sort of like life outside…so you sort of go into this bubble where you are on your own basically’ (Alice).
Throughout treatment, parents described a shift in their priorities. For many, this involved deprioritising their own needs. ‘…we always focused on [child], …we always focused on what she needed and our, what we needed, came very much second’ (Iris).
Parents reported struggling in social situations. This meant they actively avoided interactions with their social circle. ‘…even doing the school run and things was like too difficult and you just kind of didn't wanna talk about it’ (Mary).
Impact on siblings
In the majority of families, siblings were living at home. Parents reported some siblings struggled with disruptions to family life and changes in family dynamics. In some families, siblings were confused when their sibling and a parent, usually the mother, would disappear for periods of time. This absence led to separation anxiety for some siblings. ‘She’s (sibling) just so frightened to not be in the same house as me, when she, when she falls asleep and I think that's because of her experience when she was two, three, four, five where at any point in the middle of the night she'd hear noises on the stairs and paramedics coming to whisk [child] and mummy off in an ambulance and she wouldn't see us for a fortnight’ (Bryony).
Parents shared that older siblings experienced anxiety and health concerns for their sibling. These feelings intensified around medical appointments. ‘…whenever she has appointments especially [eldest child], our eldest is autistic he really does go into a real heightened state of anxiety’ (Jasmine).
In addition to anxiety, some siblings expressed feelings of resentment for the perceived preferential treatment of the child with cancer. ‘Although it is not always his fault, they’ll probably think, “Oh, he got away with a lot” or “He spoke to mom and dad in a way that we never would or ever would be able to get away with!”’ (Mary).
Parents reported that processing these changes was challenging for siblings largely due to their limited understanding. This sometimes led to emotional outbursts towards their sibling, caused by jealousy, anger or frustration. ‘…they get very, very jealous and you can see it comes in a lot of anger comes out and aimed at [child] for kind of ruining things’ (Jasmine).
During the Coronavirus disease 2019 (COVID-19) pandemic, siblings’ feelings were enhanced as they were not allowed to visit the hospital. This meant it became a mysterious, forbidden location. ‘He’d find it hard to understand why we kept going off to this place and taking [child] with us and not him…’ (Grace).
Parent emotional impact and role changes
During treatment, parents found themselves having to quickly adapt to their new circumstances. Parents relied on much-valued support from other family members (mainly grandparents) to help with caring for siblings. ‘…without them (grandparents), we couldn’t have got through’ (Bryony).
Some parents found that they were often facing the trauma on their own with limited time with their co-parent as they needed to swap responsibilities or due to hospital rules. During the COVID-19 pandemic restrictions, encounters with their co-parent were even briefer. ‘I had to leave [child] in the room, run down the stairs, dad would pass me the car keys and then dad would run back up… so you didn’t get any time to sort of do a change-over so it was one in one out…. So, you sort of go into this bubble where you are on your own basically …We had literally 13 weeks of me and my husband passing car keys in reception that was it’ (Alice).
Whilst their child was an in-patient, parents struggled to function in their parental role as the hospital staff took over decision-making and care of their child. Upon their return home parents found it difficult to making decisions for their child again, as there were added responsibilities and no-one to advise. Parents also shared concerns they may unintentionally hurt their child. ‘…because you stop making any decisions for your own child. The hospital has to make all the decisions; to say, they take parental responsibility away from you. ... it was a really big shock to the system coming home after treatment… because you’ve got nobody. There’s no nurses to ask questions, there’s no doctors, there’s nobody. ...You are back on your own as a parent. …[dad] struggled a lot ...He was frightened of hurting him and frightened of pulling any of the wires or catching the wires’ (Alice).
Parents described a lack of control in the decision-making process. They were concerned about the consequences of their decisions. ‘… I found that really quite difficult. That I had no say in anything… And yet they still then ask you to make the decision. And you're like, “But you're the expert?” so, you always feel like you have no choice’ (Ebony).
Parents worried about prioritising time for themselves. They described feeling guilty if they left their children. ‘I felt really guilty that I was doing something for me...because I would see as a treat. As a nice thing to do as time for me I couldn't. I just felt guilty about it and I need to be doing something more productive. I can't just go off and do something for myself’ (Ebony).
Several mothers reported fathers struggled more mentally. They presumed this to be due to changes in childcare responsibilities, lack of routine and support, and stresses from work. ‘I think it's sort of affected my husband's mental health more and, and possibly that might have, you know he was at work every day and not kind of you know not able to kind of sort of help as much you know obviously he came to all of the hospital appointments and things but you know somebody had to go to work’ (Poppy).
Some parents reported strains on their wider relationships. ‘...you can't always completely offload to family and friends because it, it upsets them’ (Delphine).
This led to shifts in family and friend relationships that distanced parents further from their pre-diagnosis lives. In one case, their family support network dissipated completely under the stress of diagnosis and treatment. ‘… your support network disappears …’ (Ebony).
Navigating separation and family dynamics during treatment
Long hospital stays for the child receiving treatment and a parent (usually the mother) divided the family as the co-parent remained with any siblings at the family home, trying to maintain stability and routines. For some families, the hospital stays were the first time that parents had stayed in a separate location to their children. This was a challenging situation for all, and parents shared siblings struggled to adapt to their absence. ‘…although like you made the effort to kind of FaceTime every day and things like that. But it's just such an unnatural situation for a family for the mum to suddenly not be there and so I think she kind of struggled quite a lot really as well’ (Mary).
Enforced separation meant altered family relationships and dynamics. For some, this was intensified by the distance between home and the treatment centre. ‘Just simply just to be closer to home than stuck up, up in [Northern specialist centre], for us, you know, a four- or five-hour drive away’ (Fern).
Parents perceived normal family routines to be immensely important. When at home, the main priority was to maintain some normality for family members’ benefit. ‘…me and [dad] made the decision straight away, really, that as little as possible should change for them [child and siblings] and as we were quite worried about the impact it would have on their mental health’ (Mary).
Initially, maintaining normality may have been tricky but over time families found ways to facilitate this. Traditional, family activities such as dog walks and visiting nature reserves were activities parents actively facilitated to encourage family cohesion through activities during treatment. ‘We can't do long, strenuous days, but we make sure we always get out on the weekends and when the evenings are brighter, just scooters or bikes, with a dog and to the park and things like that’ (Grace).
Other strategies employed by parents, included choosing activities to create memories for their family members that did not revolve around hospitals and to counterbalance any challenges experienced. ‘These are things that the kids like talk about and they'll remember forever. It's just making sure that you’re making positive memories and as well to kind of combat the memories of OK, remember when [child] was in hospital?’ (Mary).
Parents also used technology to help bridge the separation and maintain connection between absent family members, for example with video calls uniting the distanced family during walks, family meals or even teeth brushing. ‘[Sister] would just carry me around to the bathroom and clean her teeth … sometimes they [father and sibling] will walk me on the school run, you know, on the phone. It's like you, like wave at everyone. But so that, I mean that, you know, obviously having that that I guess video calling connection, we used a lot’ (Fern).
Additionally, parents shared the importance of facilitating open conversations within the family unit. These conversations helped family members better understand the cancer treatment and process the events. ‘We’ve always been very open and honest with them which I think really helped so if they question, they will come to us, we will talk about things I think especially with kids if you don't talk about it then they'll just make a bigger drama of it in their head’ (Jasmine).
For parents, support accessed through pre-existing social networks played a valuable role in helping them cope. Additionally, new connections with other parents of children diagnosed with cancer provided valued support. These parents shared unique connections as they had similar lived experiences and a shared an understanding of their situation. ‘The most important thing for me throughout all of this, I think in terms of mental health, has been other oncology mums’ (Bryony).
Parents reported their needs, especially psychological needs, were not addressed during and after treatment completion. ‘…, when my wheels started falling off a little bit, I was like, I don't know, I have nowhere to turn. I don't know who to turn to, you know apart from professional support and there's a lag to get that on board’ (Fern).
Other parents experienced a struggle to access, or delays in accessing, support for family members. COVID-19 meant support services often did not meet family member’s needs as they stopped completely or could only be accessed virtually. ‘... we were then referred for like a family psychology, we had one session before lockdown hit and everything got pulled … anything virtual was just a no go for him so it's taken us a long time to get to the point where we are now, where he’s seeing somebody regularly and so we had to fight for that to be honest that was a shame’ (Jasmine).
This was reported during treatment as well as towards the end of treatment, which was challenging due to a lack of guidance for families to navigate their journey beyond cancer treatment. ‘…. when the treatment was finished…. I almost didn’t know quite what to do with myself, I felt quite low… [child]’s been very similar’ (Camile).
Discussion
This study aimed to explore parents’ perspectives of family members experiences during treatment for childhood cancer. It highlights the overwhelming impact on family members’ well-being and the shifts within the family dynamics during treatment. This study illustrates the COVID-19 pandemic added a layer of complexity to this challenging time.
The absence of family members during treatment stressed relationships within, and around, the family unit and negatively impacted family functioning and wellbeing, aligning with previous research (Long et al., 2018; Tay et al., 2022). Parents in this study showed an awareness of the challenges siblings experienced during treatment expressed through externalised behaviours such as jealous or angry outbursts as well as internally processed responses such as increased anxiety. However, this perception may underestimate the full extent of the burden, as Pariseau et al. (2020) found siblings often experience a greater impact on well-being than their parents recognise. Prior research identified that mothers experienced higher levels of anxiety and depression (Peterson et al., 2020), however mothers in this study perceived fathers to experience more psychological difficulties and greater barriers to accessing support. This divergence between parental perceptions and existing research highlights the need for studies that engage with family members to capture their lived experiences.
In line with previous research, this study found strategies used by parents to minimise disruptions and adverse impacts for siblings included encouraging open communication and maintaining normal family routines. These strategies have been linked to improved psychological adjustment and reduced anxiety, and behavioural problems for siblings and patients (Pariseau et al., 2020; Van Schoors et al., 2017, 2018). The findings from this study highlight that families would benefit from support throughout treatment to encourage communication, preserve a sense normality, and strengthen family cohesion between all family members.
During hospitalisation for treatment, parents described a loss of control over decision-making. In addition, they described redefining their identity, as identified in previous research (Gibbins et al., 2012; McEvoy and Creaner, 2021). Together, this highlights that parents need to be empowered with information and skills to maintain their own well-being through this transitional period to continue their care-coordinating and parenting roles. Support mechanisms need to be employed that would be acceptable and feasible in a hospital context. In a recent study, parents found the challenges they experienced during childhood cancer treatment were lessened and they felt valued by having a dedicated healthcare professional to support them and to provide informal psychosocial support (Murphy et al., 2025).
Support networks emerged as a key mechanism for supporting families coping with challenges. Social support has been shown to enhance parents’ adjustment and decrease parental stress (Maynard and Bennett, 2024; Melguizo-Garín et al., 2023). Yet our study showed that accessing social support was difficult, as strains appeared within some parents’ pre-existing support networks. Highlighted in this research is the support group self-identified as ‘oncology mums’, who were an important source of social support. This identification was not a stigma but instead was deemed as a uniting, supportive environment and agrees with other research where those with a shared experience can be an important source of hope for parents of a child affected by cancer (Barrera et al., 2013). This informal support group could also help parents as it would be a suitable context to share difficult moments, where their hopes could be shared, supported and sustained (Leite et al., 2019). Facilitating support networks outside the healthcare context could be beneficial for all family members.
This research highlights the difficulties parents found in accessing support for their family member’s needs throughout treatment, as shown in previous research (Robertson et al., 2024). In line with previous research, this study highlights more support is needed for caregivers, this could be through education or referral systems (Dionne-Odom et al., 2019; Young et al., 2023). Within hospital settings, healthcare professionals can signpost support for parents to unite family members in times of stress and increase their resilience so they can turn to one another for support and encouragement (Patterson, 1995). Previous research has suggested that healthcare professionals can support families navigate the childhood cancer journey (Murphy et al., 2025).
These findings offer broader insights from parents’ perspectives, which are essential as parents act as both gatekeepers and implementers of support during a child’s cancer treatment. Parents are required to facilitate external support and shape their family’s internal coping strategies. Unlike previous studies that focus on child patients or individual family members in isolation, this research reinforces the importance of viewing families as a dynamic, interactive system and highlights that support needs often extend beyond the patient. A more holistic, family-centred approach to care is needed that responds to all family members’ needs.
Limitations
This study focused on families with one to three children, so larger families’ experiences may not be fully represented and may differ in meaningful ways. Although efforts were made to include fathers, the majority of respondents were mothers. A more balanced representation of parental perspectives, particularly from more fathers, may have provided broader and richer understanding. Additionally, only English-speaking parents participated including non-English speakers could have added diverse, cultural perspectives potentially enriching the findings.
Implications for practice
This study underscores the importance of adopting a family-centred, holistic approach to care throughout a child’s cancer treatment. Healthcare professionals are uniquely positioned to play a pivotal role in supporting families during this challenging time. Proactive signposting to both formal services and informal support networks is essential to ensure families can access timely, appropriate, and sustained assistance. By collaborating with parents to co-design support to address their family’s need, healthcare professionals can deliver care to strengthen family relationships, bridge separation often experienced by families and alleviate the impact on family members’ well-being. By empowering parents to preserve a sense of normality and maintain balance within daily family life, professionals can help families better navigate the complex emotional, practical, and social demands of treatment. Thus, supporting not only the child receiving treatment but also their wider family unit.
Conclusion
This study highlights the importance of understanding family member’s experiences through parents’ perspectives. The experiences shared in this study highlight potential strategies to support families to mitigate the detrimental impact of childhood cancer on family member’s health and family functioning. Future research should adopt a family-centred approach, exploring the experiences of all family members within the context of the family unit. Support is needed to guide families through the challenges of treatment. To ensure this meets their needs, families along with healthcare professionals should be involved in co-designing support required to meet the unique needs of families during childhood cancer treatment.
Supplemental Material
Supplemental Material - A qualitative exploration of parents’ perspectives of family members’ well-being and family dynamics during childhood cancer treatment
Supplemental Material for A qualitative exploration of parents’ perspectives of family members’ well-being and family dynamics during childhood cancer treatment by Elizabeth Pharoah, Clare Stevinson, Silvia Costa and Elizabeth Stamp in Journal of Child Health Care.
Footnotes
Acknowledgements
The authors would like to thank the parents for participating in this study and sharing their experiences with us.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by Loughborough University Ethics Committee (approval: 2022-6811-9765).
Informed consent
Written informed consent was obtained from all participants before the participating in the study.
Data Availability Statement
The data underlying this article cannot be shared publicly due to ethical reasons as the participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research, supporting data is not available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.