
Abstract
Family-centred care (FCC) is central to care of children and families across healthcare settings. Research exploring FCC is increasing, so there is a need to identify clinical and research priority areas. This review aimed to describe FCC research for children and families in the 21st century. Studies were sourced from CINAHL, Ovid Medline, and Embase and underwent two-stage screening, guided by a published protocol. Data were extracted on study authorship, author discipline, funding, study methodology, study findings, and use of ‘FCC’. Analysis included descriptive statistics, Pearson’s Chi-Squared tests, and content analysis. Five hundred and seventy-nine articles were included. Most used quantitative methodologies and were published from 2010, predominantly by authors from nursing or medical disciplines. Most studies were conducted in acute care settings, typically in North America, and primarily included nurses or mothers as participants. FCC was typically defined using multiple references, with several key authors identified. Future research should focus on historically underrepresented clinical and geographical areas and include multidisciplinary team members. Increasing cultural and familial diversity in FCC research is also necessary to ensure inclusive FCC practices that are transferrable within and between clinical and geographical settings.
Introduction
Family-centred care (FCC) is a holistic, family-focused approach to providing care for infants and children and is widely used in acute, sub-acute, and community care paediatric settings worldwide (Foster, 2015; Kuo et al., 2012; O’Connor et al., 2019). There are multiple definitions of FCC, ranging from ‘an approach to the planning, delivery, and evaluation of health care that is grounded in mutually beneficial partnerships among health care providers, patients, and families’ (Institute for Patient and Family Centred Care, [IPFCC] n.d: 1) to ‘a way of caring for children and their families within health services which ensures that care is planned around the whole family, not just the individual child/person, and in which all family members are recognised as care recipients’. (Shields et al., 2006: 1318).
Foundations of FCC were established in the mid-20th century (Jolley and Shields, 2009; Kuo et al., 2012; Smith 2018). Before this, many hospitals, particularly in high-income countries, excluded parents from being with their children, sometimes for months at a time, due to fears of spreading disease and perceptions that parents were ill-equipped to care for their sick children (Jolley and Shields, 2009; Smith, 2018; Watts et al., 2014). However, seminal work by Bowlby (1951) and Robertson (1958) demonstrated significant negative psychological consequences for hospitalised children separated from their parents. Their works were published at a time when there was already increased focus on psychological wellbeing following widespread separation of children from their families during World War II (Jolley and Shields, 2009). Groups and organisations were established, such as the Association for Care of Children’s Health (established 1987) and Institute of Family Centred Care (established 1992) in the USA, the Platt Report (1959) and Action for Sick Children Movement (1961) in the United Kingdom (Jolley and Shields, 2009; Smith, 2018; Watts et al., 2014). These organisations and reports were pivotal in lobbying for improvements in hospitalised children’s care, including parents throughout a child’s hospital stay, and improving nursing training on child welfare (Jolley and Shields, 2009; Smith 2018).
Early models of FCC, such as ‘care-by-parent' and ‘partnership in care’ focused on involvement of a child’s parents, typically mothers, in providing physical and emotional care for children in hospital settings (Harrison, 2010; Jolley and Shields, 2009; Smith, 2018; Watts et al., 2014). A formal definition of FCC was first provided in 1987 by Shelton et al. (1987); however, disagreements remain regarding what FCC is, how to implement it, and whether it provides measurable benefits to children and their families (Coyne et al., 2018; Mikkelsen and Frederiksen, 2011; O’Connor et al., 2019; Uniacke et al., 2018). Several recent literature reviews and concept analyses identified common attributes of FCC in hospital and community-based healthcare settings: negotiation; trust; respect; open communication; collaboration and partnership between families and healthcare teams; parental empowerment and involvement; and recognising family units as a constant in children’s lives (Coyne et al., 2018; Foster, 2015; Kuo et al., 2012; Lor et al., 2016; Mikkelsen and Frederiksen, 2011; O’Connor et al., 2019; Shields et al., 2006; Smith, 2018; Watts et al., 2014). However, many of these common attributes are underpinned by Western cultural norms and ideals, with cross-cultural translation and acceptability of FCC into other cultures still unclear (Mikkelsen and Frederiksen, 2011).
Vast amounts of research explore the concept of FCC, with topics ranging from measuring family-centred outcomes (Davidson et al., 2017; Kuhlthau et al., 2011; Kuo et al., 2011; Watts et al., 2014), to investigating effects of family-centred rounds (Rea et al., 2018) and exploring staff and family experiences of FCC provision (Bellin et al., 2011; Goldfarb et al., 2017). Anecdotal evidence suggests that research into FCC is more prominent in some specialty areas and geographic locations than others (e.g. limited research from low- or middle-income countries), and that some research methods have been used more extensively than others, however, this has not been systematically explored. Mapping the current FCC landscape in paediatric acute, sub-acute and primary healthcare may guide future research and identify areas of priority focus.
Aim
To describe the extent and nature of research on child- and family-centred care for children and their families in the 21st century.
Methods
We developed and published a protocol to guide this review (Butler et al., 2021), informed by the Joanna Briggs Institute (JBI) methodology for scoping reviews (Peters et al., 2017, 2020; Pickering and Byrne, 2013; Pollock et al., 2023). We used the Preferred Reporting Guidelines for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR) checklist (Tricco et al., 2018). Scoping review methodology facilitated iterative searching and data extraction processes, as authors became familiar with the evidence base (Peters et al., 2017; Pollock et al., 2023).
Search strategy
We developed a search strategy to identify research on Population: infants, children, adolescents, parents, and extended family members; Phenomenon of interest: family-centred care and synonyms; and Context: hospital, acute care, community care, outpatient care, primary care, school care, and hospice care. We developed search strategies in collaboration with a Senior Research Librarian. Literature searches were conducted using the Cumulated Index to Nursing and Allied Health Literature (CINAHL), MEDLINE, and Embase in July 2021. Backwards searching was conducted using reference lists of identified FCC-related systematic reviews. Full search strategies, including FCC synonyms, can be viewed in Supplemental Material A.
Study selection process
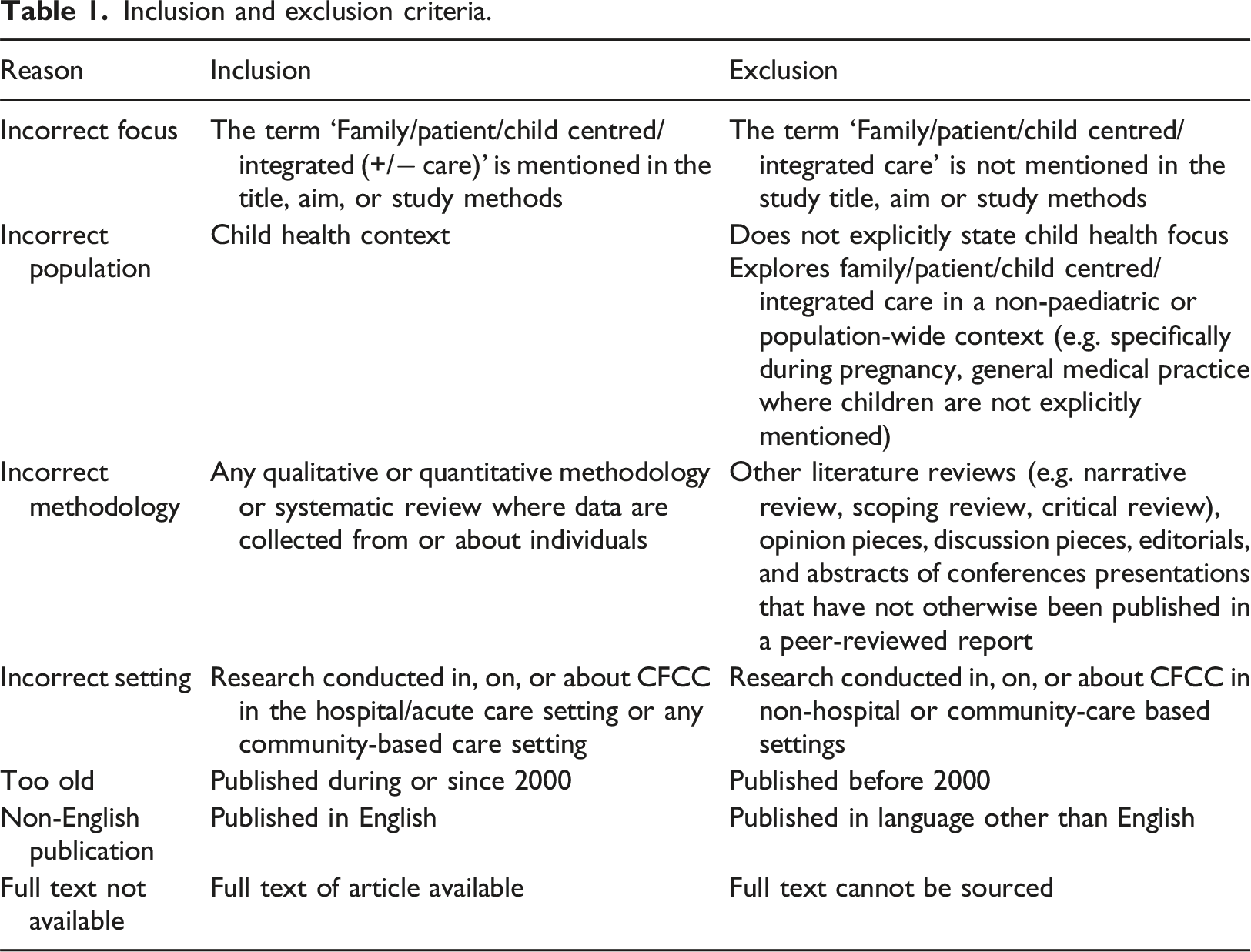
Inclusion and exclusion criteria.
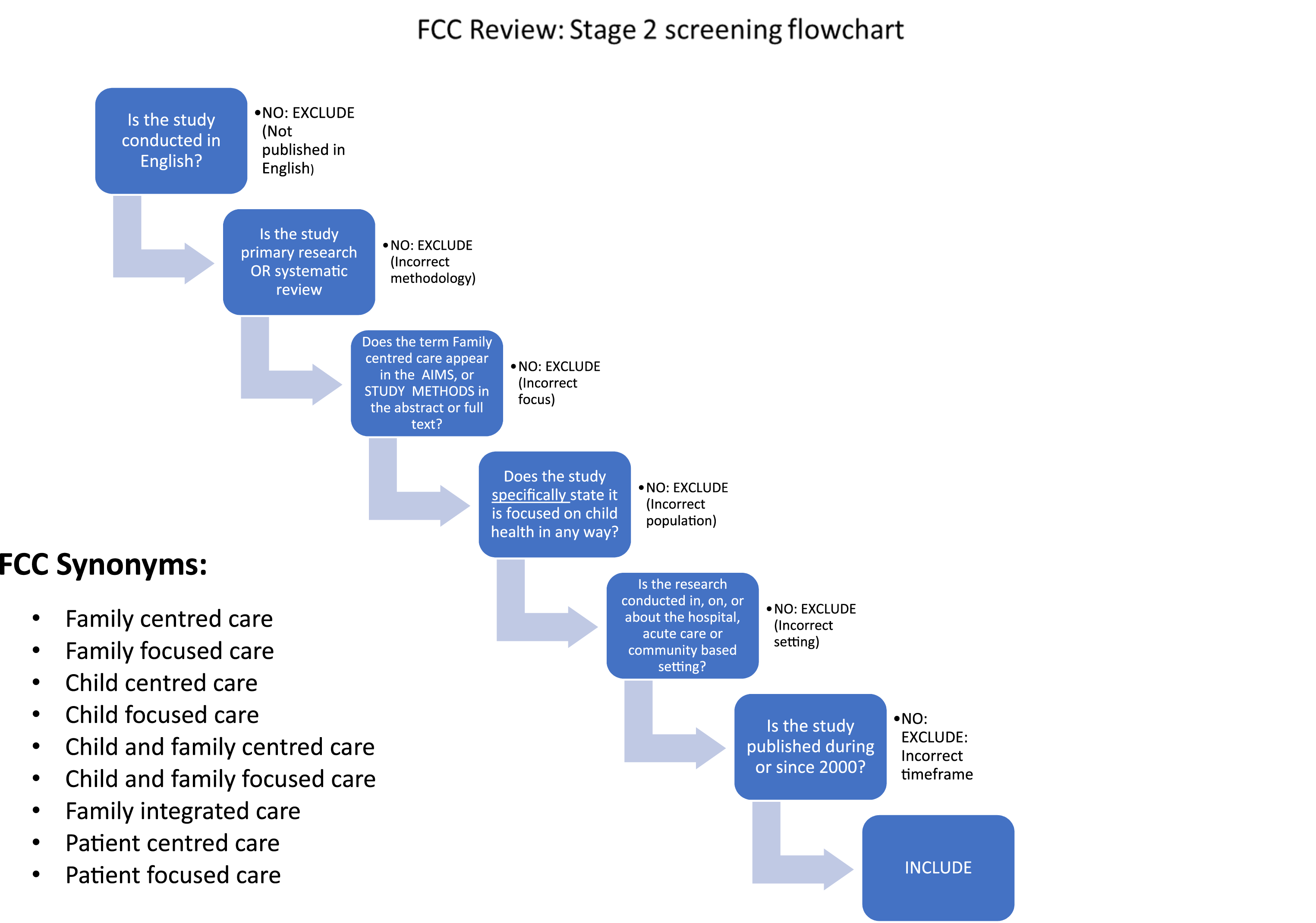
Stage 2 screening flowchart.
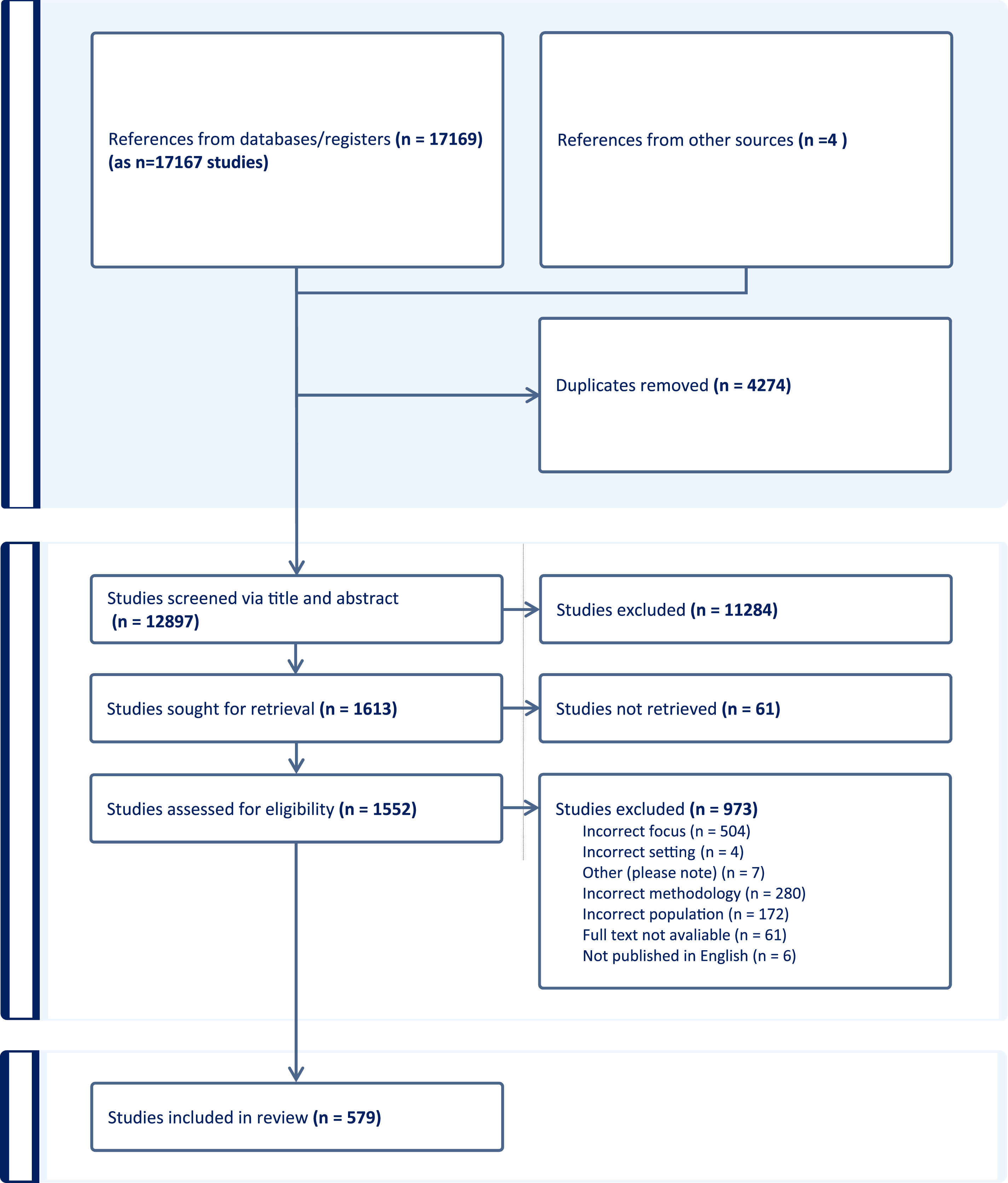
PRISMA diagram.
Data extraction
Based on the magnitude of articles included in this review, we split data extraction and analysis into two parts: Part one, a descriptive analysis of study characteristics, reported in this paper; and part two, a thematic analysis, planned as a subsequent publication. After full-text screening, the primary authors developed a data extraction tool. Pilot testing was conducted on a small number of included articles by (AEB, LR, EH, KE and CA). Extracted data included: article title, journal, publication year, discipline of lead and last authors, region of the study setting, aims, methods (i.e. recruitment, mode of data collection, and planned data analysis), study results, where FCC was mentioned in-text, and whether this included reference to a FCC definition. During extraction, we expanded on what was outlined in the protocol to include data related to individual study funding to enable an analysis of associations between funding and author discipline or study setting.
We undertook data extraction between September 2022 and January 2023. Five per cent of articles were reviewed by (AEB) for accuracy and consistency, with additional random spot checks undertaken throughout.
Data analysis and synthesis
Once data extraction was complete, quantitative results were exported into a Microsoft Excel (Version 2403) spreadsheet for quantitative analysis. Descriptive statistics were used to provide a quantitative overview of included articles, with Pearson Chi-Squared tests used to explore differences between studies. We were interested in the ways in which studies of FCC were funded. In order to explore this, we carried out three chi-square analyses exploring the role of study location and discipline and last author on funding for the study. FCC definition data were imported into NVivo 12 (QSR International, 2022) to facilitate a content analysis of terminology and references authors used to conceptualise FCC.
Results
Demographic and geographical findings
Overview of included studies.
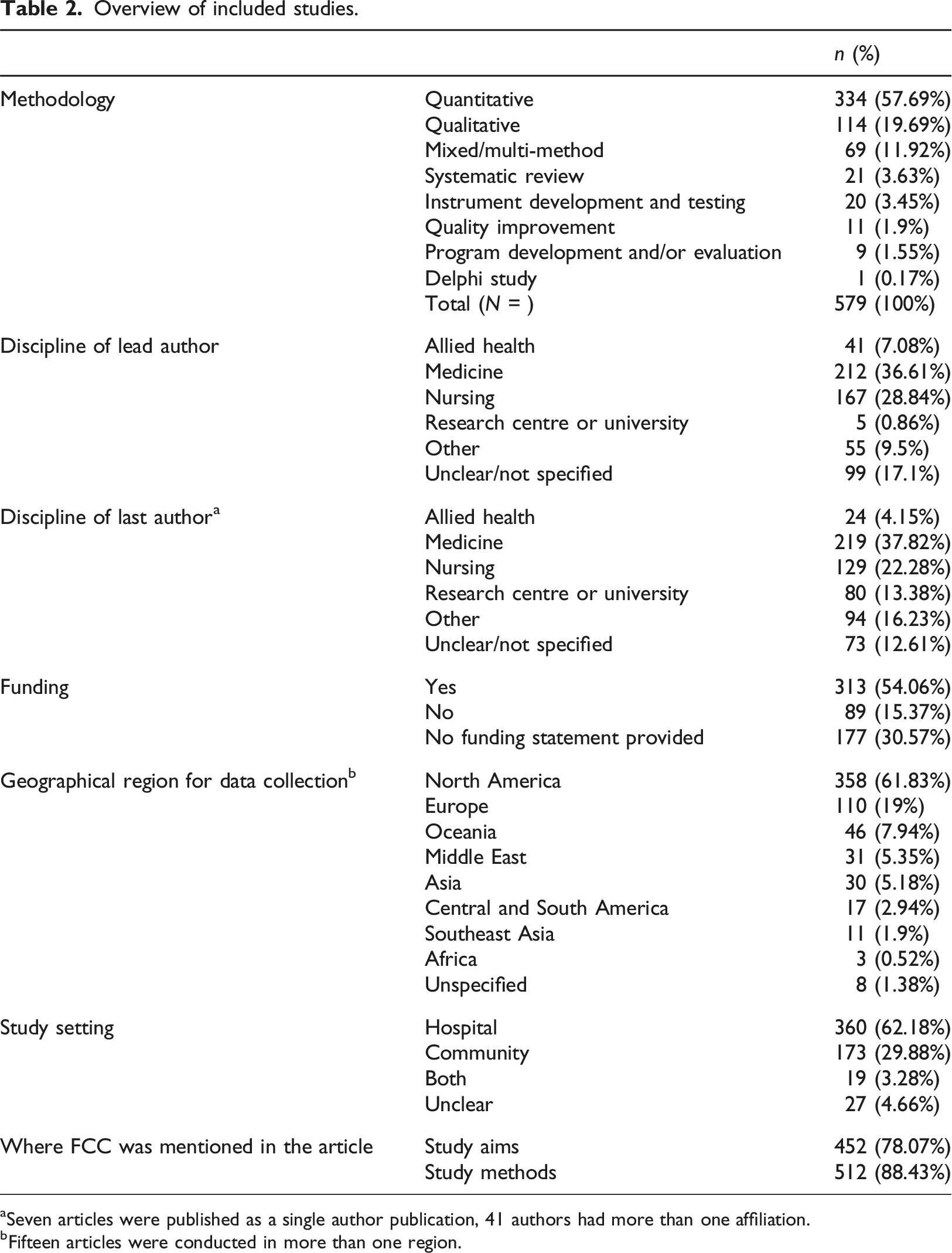
aSeven articles were published as a single author publication, 41 authors had more than one affiliation.
bFifteen articles were conducted in more than one region.
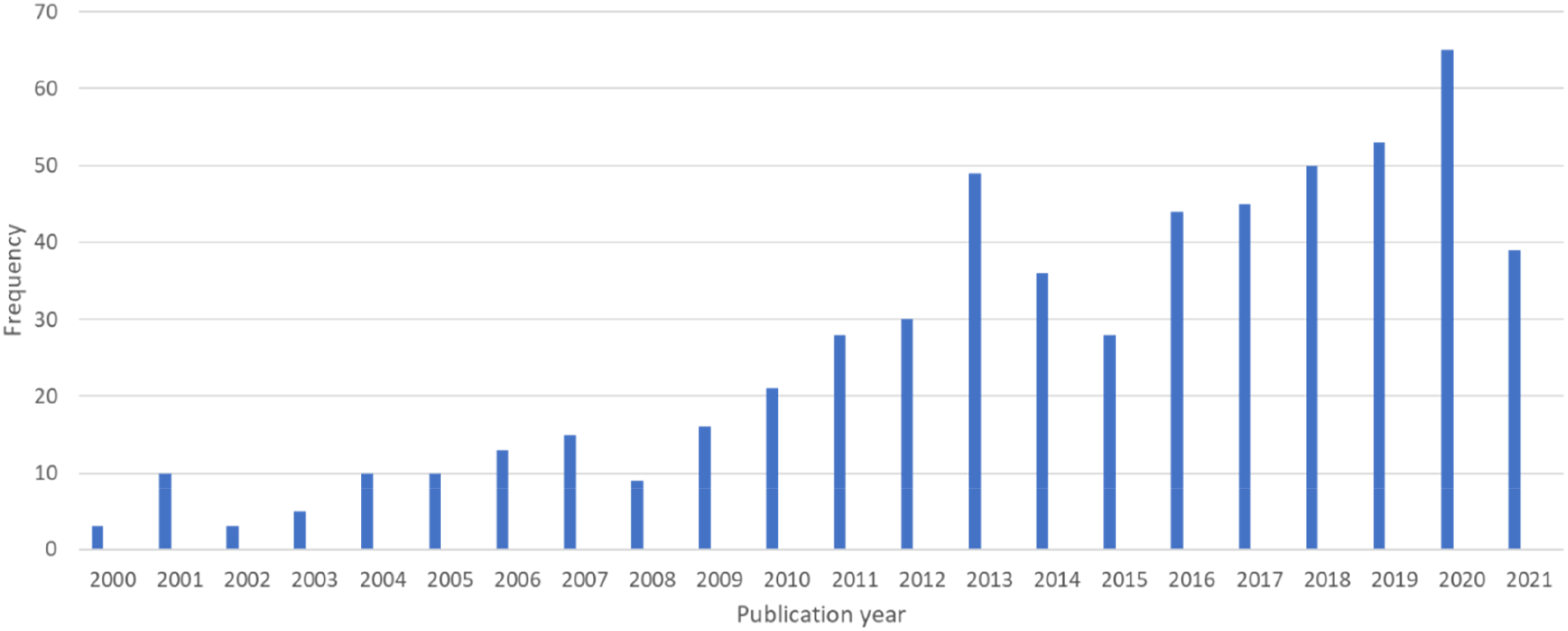
Publication frequency by year.
There was an association between discipline of first authors and study funding X2(14) = 32.654, 95% CI [0.002, 0.005]. Authors with a background in medicine were more likely to be part of a funded study. There was also an association between the discipline of last authors and study funding X2(18) = 30.156, 95% CI [0.028, 0.035], whereby authors from medicine were more likely to be funded.
Most FCC research was conducted in North America, with 314 of 579 studies (54.2%) conducted in the United States of America (Supplemental Material C). European FCC research was undertaken in the United Kingdom, The Netherlands, Italy, and the Nordic region, collectively making up 19.1% of included articles. In contrast, countries in Africa and Southeast Asia were least represented (0.5% and 1.9%, respectively).
Most research was conducted in hospital or acute care settings (n = 360; 62.2%), in neonatal intensive care units, general hospital wards, paediatric intensive care units, or included hospitals more broadly (Supplemental Material D). Community-based research accounted for 29.9% of included articles, and primarily focused on patient-centred medical homes, primary healthcare settings, community healthcare settings, and school-based health care. Remaining studies were conducted across both settings (3.3%) or were unclear (0.5%). There was no association between where studies were conducted and their funding X2(10) = 14.930, 95% CI [0.127, 0.141].
Overview of quantitative, qualitative, and mixed/multi-method articles
Quantitative study methods.
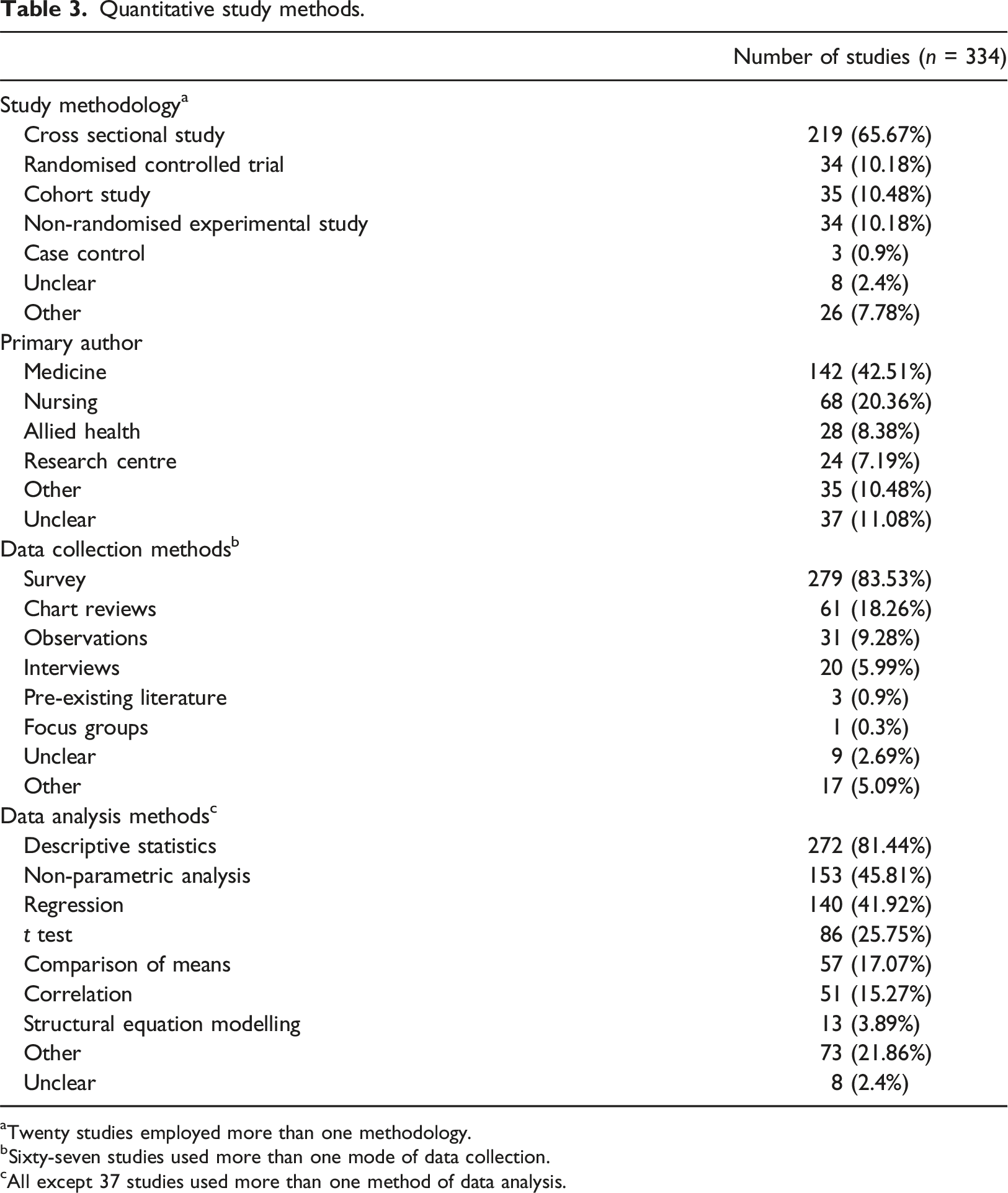
aTwenty studies employed more than one methodology.
bSixty-seven studies used more than one mode of data collection.
cAll except 37 studies used more than one method of data analysis.
Qualitative study methods.
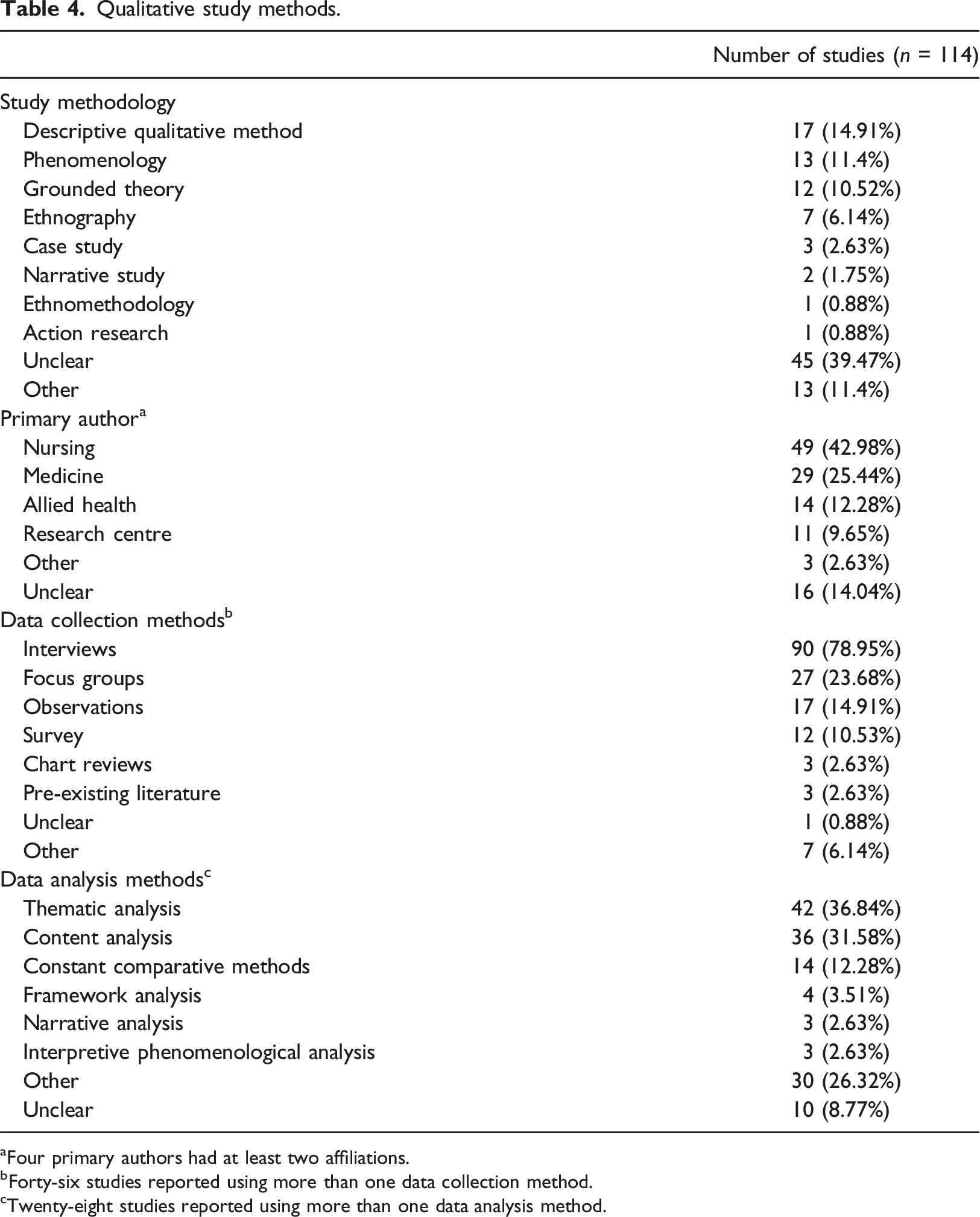
aFour primary authors had at least two affiliations.
bForty-six studies reported using more than one data collection method.
cTwenty-eight studies reported using more than one data analysis method.
Mixed or multi-methods articles accounted for 11.9% (n = 69) of included research. These were primarily led by authors with nursing (n = 21, 30.4%) or medical (n = 20, 29.0%) affiliations. Most mixed or multi-methods articles reported surveys (78.3%), interviews (55.1%) and focus groups (33.3%) as main methods of data collection, and content analysis (30.4%) and descriptive statistics (82.6%) as main data analysis methods.
Participants in quantitative, qualitative, and mixed/multi-method articles
Figure 4 provides an overview of participant groups identified in qualitative, quantitative, and mixed/multi-methods articles. Of those participants ‘receiving’ FCC (parents, children, and family members), the largest groups represented according to methodological approach were mothers for qualitative studies (40%), children receiving care for quantitative studies (41.6%), and parents for mixed/multi-methods studies (42%). Fathers were less frequently included than mothers in all three study types: qualitative 28.7% versus 40%; quantitative 11% versus 25.9%; and mixed/multi-methods 26.1% versus 33.3%. Siblings appeared in only 2.6% of qualitative studies, 0.9% of quantitative studies, and 1.4% of mixed/multi-method studies. Overview of participants in qualitative, quantitative, and mixed/muti-method studies.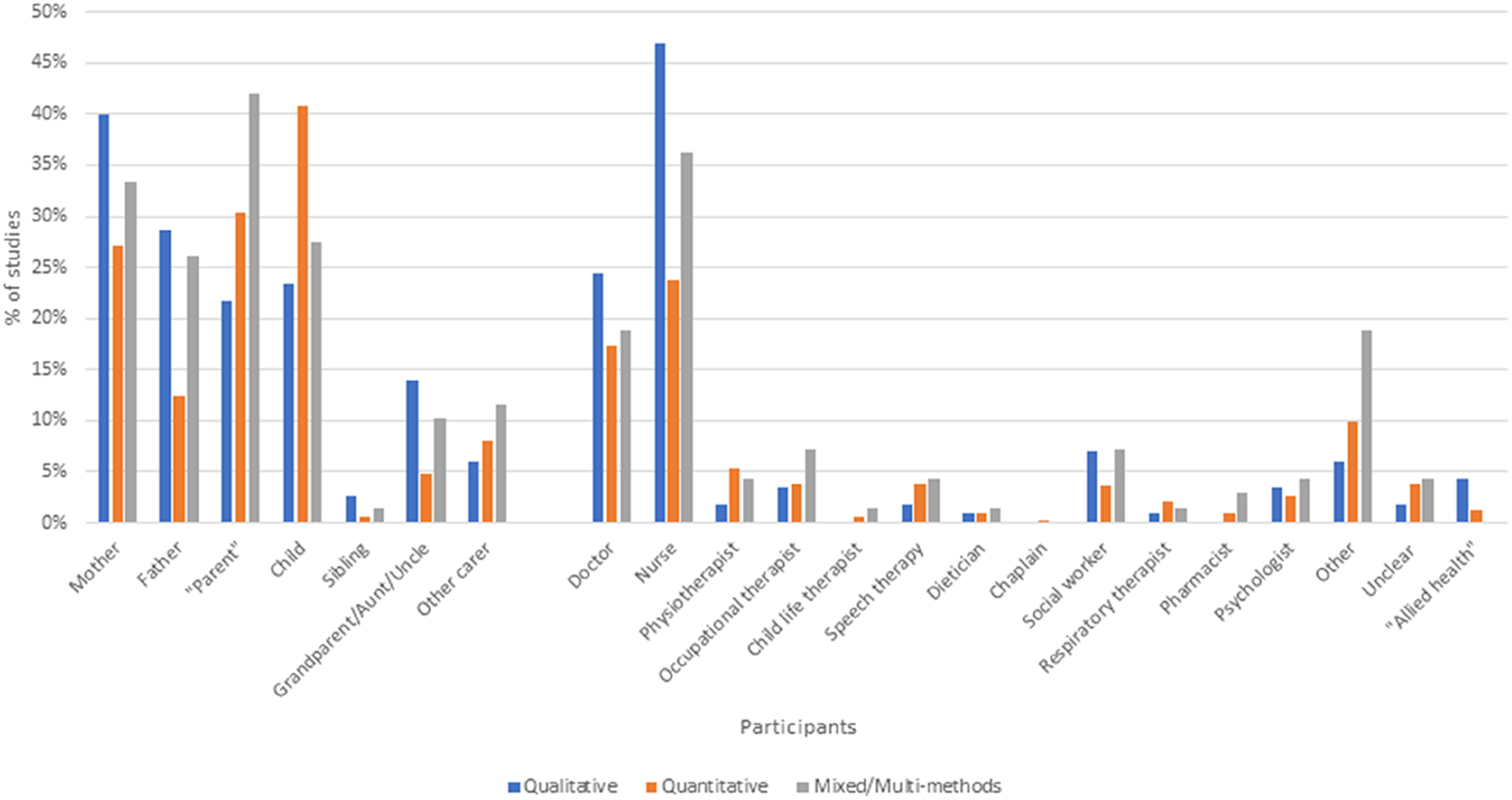
Of healthcare provider participants providing FCC, nurses were the largest group in all three study types: qualitative 47.8%; quantitative 23.5%; mixed/multi-methods 36.2% (Figure 4). In contrast, medical staff participated in 26.1% of qualitative studies, 16.7% of quantitative studies, and 18.8% of mixed/multi-method studies. Participation of allied health staff was limited overall, with each allied health specialty generally participating in less than 5% of studies overall. A notable exception was social workers, who participated in 7% of all qualitative studies and 7.2% of mixed/multi-method studies.
Participant exclusion criteria were noted in only 148 of 579 included articles (25.6%). Reasons for participant exclusion are listed in Supplemental Material E. Parents and family members were most often excluded from participation due to lack of proficiency in the primary language of the country where the research was conducted. Most commonly, this was listed as an inability to communicate sufficiently in English. Other reasons included being younger than 18 years of age or felt to be suffering from severe distress or mental health issues. Children and their families were typically excluded if children were deemed at risk of dying during the study, were ‘too unwell’, had significant additional co-morbid conditions, or when families had significant social or legal issues, for example, child protective services were involved.
Family-centred care frameworks and definitions
FCC (or a synonym) was mentioned in study aims of 454 articles, with 515 mentioning FCC in study methods. Of 579 studies, 313 defined FCC or a synonym (54.1%). Of these, 146 referred to one of six key authors to define this concept. The American Academy of Paediatrics (AAP), Institute for Patient- and Family-Centred Care (IPFCC), and/or Committee for Hospital Care were the most referenced sources used to define FCC, collectively cited in 82 articles. Others included works by Shields et al. (cited by 38 articles), Kuo et al. (n = 21), and Coyne (n = 13). However, most articles (n = 218 of 313; 69.6%) used alternative sources to define FCC. Over half of articles defining FCC cited more than one source (n = 166 of 313; 53.0%). Fifty articles defined FCC without citing any source.
Additional FCC-related terminologies were defined in 112 articles. Seven articles referred to Child-Centred Care (CCC), with Coyne et al. (2016) serving as a significant reference. Family-Centred Medical Homes were frequently cited, appearing in 65 articles, most of which referenced the AAP. Family-centred Rounding was also extensively discussed, with 37 articles and numerous other sources, including Foster (2015), Mittal (2010), and Sisterhen (2007).
Despite considerable references to FCC and its associated terms, 125 (21.5%) articles lacked definitions.
Discussion
This scoping review describes the extent and nature of research on family-centred care for children and their families in the 21st century. We identified 579 studies that explored FCC across a range of healthcare settings, most of which were published during or after 2010. Our findings demonstrate that FCC research has displayed a generally upward trajectory since the early 2000s, with a few notable exceptions. We found a decline in publications during 2008 and again in 2015; however, reasons for these declines are unclear. In addition, there was a notable increase in the number of publications in 2013. This increase may be a response to work published by FCC expert Linda Shields and colleagues between 2010 and 2012, calling for further research on FCC for children in hospitals (Shields, 2010; Shields et al., 2012a; Shields et al., 2012b). Of note, our review only included literature up to March 2021.
Although we included research published during the first year of the Coronavirus disease 2019 (COVID-19) pandemic, we suspect most of this will have been conducted and submitted for publication before or early in the pandemic. As noted by Foster and Blamires (2023), COVID-19 had a major impact on research activities in many parts of the world and substantially limited family access to many hospital and community settings for prolonged periods. An upward trend in publication numbers noted in our findings may not reflect research output in all areas. For example, whilst FCC research in acute care settings may have potentially declined due to pandemic-related visiting restrictions, it is possible that FCC research in community-based settings may have increased with additional use of telehealth consultations. Future reviews may uncover consequences of COVID-19 on both provision of and research into FCC.
Nursing and medical researchers led a substantial portion of FCC research included in this review. While this is not surprising, given that nurses and doctors typically account for the largest proportion of healthcare providers globally (World Health Organization, 2020), it is important to acknowledge that allied health providers also play a key role in delivering holistic, family-centred care to children and their families. Increasing support and involvement of allied health providers, such as physiotherapists, social workers, or psychologists, to lead and participate in FCC research studies would help to increase understanding and successful implementation of family-centred models of care.
We found three times as many quantitative studies than qualitative studies. Most quantitative studies used cross-sectional survey designs, which may be in response to frequent calls for more studies that measure outcomes related to FCC (Harrison, 2010; Jolley and Shields, 2009; O’Connor et al., 2019; Smith, 2018). However, Shields (2010) also called for more experimental studies on FCC, particularly randomised controlled trials. In our review, experimental studies (both randomised and quasi-experimental) only accounted for 20.4% of all quantitative studies, suggesting an ongoing need for more studies that directly measure multiple outcomes of FCC, including satisfaction with care, and health or care outcomes related to FCC provision. In addition, we found only 20 articles focusing on developing, translating, or validating new measurement tools since 2000. Further research is needed to identify whether tools developed before 2000 are fit-for-purpose in 21st century care, or whether, as noted by Kuo et al. (2012), more research is needed to develop and test outcome measurement tools for FCC.
Our review highlighted the predominance of studies conducted in North America and Europe (particularly Western Europe and the Nordic region). This may not be surprising in the context of traditionally Western-centric origins of FCC concepts. There are significant cultural and operational considerations related to appropriateness and implementation of FCC in low- or middle-income settings and for culturally and linguistically diverse populations in high-income countries (Al-Motlaq and Shields, 2017; Shields, 2010). Calls for FCC research in more culturally diverse populations have been present in the literature for many years (Dennis et al., 2017; O’Connor et al., 2019; Watts et al., 2014). Our review demonstrates that research is still needed, particularly exploring the relevance, applicability, and impacts of FCC in regions outside of North America and Europe.
We also found that most research on FCC was conducted in acute care settings rather than community-based settings, with a particular focus on FCC in neonatal intensive care units (ICUs). This finding is despite on-going recognition of the importance of families and FCC to the care of children with a variety of complex chronic conditions in both hospital and community settings (Al-Motlaq et al., 2019; McConkey et al., 2023; Watts et al., 2014) and in population-based preventative health care. We recommend researchers consider expanding their foci to include less-explored areas, particularly areas that traditionally have significant and prolonged family involvement, such as palliative care or neurology. We recommend a focus on research exploring FCC provision in community-based care services to understand and evaluate ongoing provision of FCC following discharge from acute care settings, as suggested by Harrison (2010) and Watts et al. (2014) .
This review highlights the role of organisations such as AAP, IPFCC, and Committee on Hospital Care in defining the concept of Family-Centred Care within research communities. Based on the frequency with which these organisations are cited, our findings indicate they are key contributors to FCC discourse. Despite these influential professional FCC sources, diverse citation sources, varying terminologies, and absent definitions demonstrate complexity and multiplicity of FCC as a concept. Over the past two decades, we have seen evolution and adaptation of FCC concepts: consensus about what constitutes FCC is yet to be realised.
Given that achieving a unified definition of FCC may not be possible or even desirable, it is vital that authors undertaking FCC research clearly identify the FCC definition used to underpin their study, to improve transparency and transferability of research findings into clinical practice.
We also examined which participants were or were not included in FCC studies. For those receiving FCC, participants were most commonly mothers (particularly for qualitative studies) or ill children (particularly for quantitative studies), with fathers also taking part in almost one-third of qualitative studies. Notably, other family members rarely participated in FCC studies, particularly those quantitative in nature. Our findings align well with those of both Mikkelsen and Frederiksen (2011) and Kokorelias et al. (2019), demonstrating that while family-centred care is espoused in clinical practice, our collective understandings of FCC as a concept are based on experiences of mothers, ill children and, to a lesser extent, fathers.
Potential participants were commonly excluded from FCC research because of their limited English language ability, because the clinical or research team felt they were too distressed, or because children were deemed to be too unwell for child and family to take part in research. However, only one-quarter of articles reported their exclusion criteria, so the true nature of participant exclusion in FCC research remains unknown. We strongly recommend future research focusses on including perspectives of underrepresented or excluded groups, such as siblings, extended family members and non-English speaking families, to ensure future FCC research is both family-centred and culturally safe (Lor et al., 2016).
Strengths and limitations
This review was strengthened by developing a review protocol prior to commencement. In addition, including diverse literature ensured a broad representation of different research contexts and contributed to a detailed and in-depth depiction of the current state of FCC research. As expected for a scoping review (Peters et al., 2017), iterative changes to the protocol were made due to the scale and scope of identified articles: transparency in reporting these changes supports the review’s rigour. Our review findings were limited by excluding articles published in languages other than English. This may have biased reporting of research conducted in countries that do not primarily speak or publish in English and limited our understandings of the scope of FCC research in culturally diverse settings. In addition, poorly or inconsistently described author data (particularly affiliations and funding) and study methods (particularly geographical location, data collection and analysis methods, and exclusion criteria) limited our ability to accurately extract and report data and may have led to underreporting of some study methods or locations. Although we only extracted affiliation data for first and last authors, this approach is unlikely to have impacted our ability to accurately report the interdisciplinary leadership of FCC research. Finally, we were limited by the information provided by study authors in their titles and abstracts. It is possible that relevant studies were not identified for inclusion in this review because of a lack of terms related to FCC mentioned in the title, aims, or study methods. Moving forward, we strongly recommend that authors carefully consider their titles and abstracts, to maximise identification and inclusion in future literature reviews.
Conclusion
Family-centred care is a core component of healthcare for children and their families, and an important focus for paediatric healthcare research. This review outlined the current state of FCC research in paediatrics, identifying clinical and geographical areas and methodologies that have received significant attention to date and highlighting areas for future focus. Our review’s findings may inform future research designs that consider multidisciplinary research teams, various study designs, and a range of clinical and geographical study locations. Such initiatives can promote provision of FCC that is equitable, inclusive, culturally safe, and appropriate across the range of settings and stages of children’s healthcare journeys.
Supplemental Material
Supplemental Material - Family-centred care research in paediatrics: A scoping review
Supplemental Material for Family-centred care research in paediatrics: A scoping review by Ashleigh E Butler, Lael Ridgway, Ellen M Henderson, Stacey Hokke, Kristina Edvardsson, Catina Adams, Elly Greenwood, Christine East, Kolsoom Safari, Noushin Arefadib, Lisa McKenna, and Beverley Copnell in Journal of Child Health Care.
Footnotes
Author contributions
Dr Ashleigh Butler conceptualized and designed the study, designed the data collection and screening instruments, collected, screened, and analysed the data, drafted the initial manuscript, and critically reviewed and revised the manuscript. Dr Ellen Henderson and Ms Lael Ridgway conceptualized and designed the study, designed the data collection and screening instruments, screened and analysed the data, and critically reviewed and revised the manuscript. Ms Elly Greenwood, Dr Stacey Hokke, Dr Catina Adams, Dr Kolsoom Safari and Dr Noushin Arefadib, Associate Professors Kristina Edvardsson and Bev Copnell, and Professors Christine East and Lisa McKenna designed the study, screened and analyzed the data, and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research assistance for this study was funded by La Trobe University.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.