
Abstract
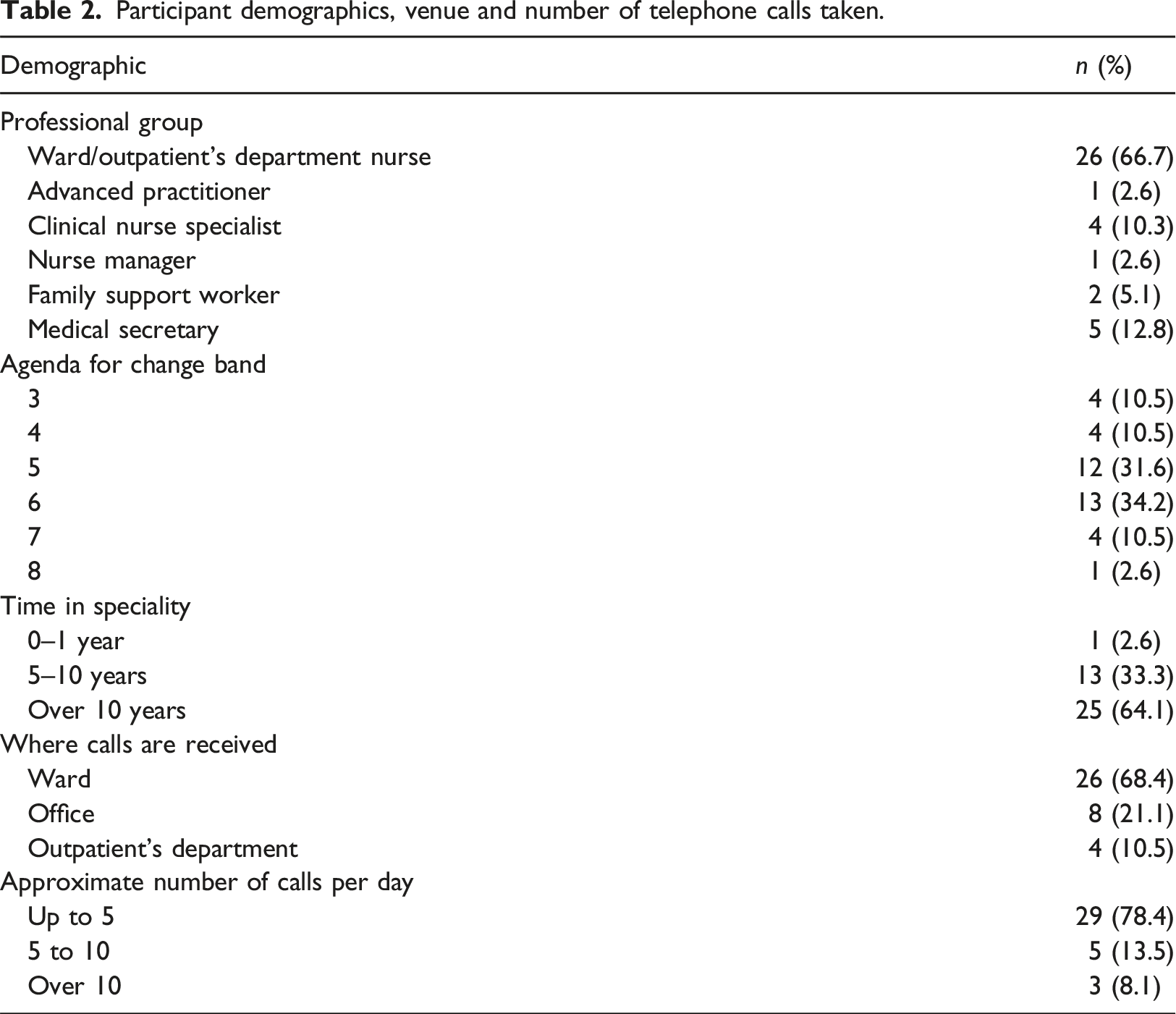
The Congenital Heart Disease Standards for England indicate that parents and children should have access to a 24-h telephone advice service, however, little is known about existing services. This paper presents phase two of a mixed-methods service evaluation, which aimed to evaluate staff experiences of telephone communication with these parents. All nursing and support staff in a single specialist children’s cardiac surgical centre were invited to participate in an online survey during July–November 2019. Data were descriptively and thematically analysed. Participants (N = 39) were predominantly nurses (n = 32, 82%) with 64.1% (n = 25) working in the speciality >10 years. Positive experiences included: signposting and preventing further deterioration; supporting families to get expert advice quickly; providing reassurance. Challenging experiences included: offering advice without being able to see the child, dealing with telephone calls alongside busy workload; and parents running out of medications and telephoning out of hours. In conclusion, taking telephone calls were perceived to be time consuming and are potentially high risk. A standardised approach to assessment, intervention and documentation was deemed necessary. Implementation of an updated parental early warning tool was recommended, along with staff and parental education.
Introduction
Up to nine babies per 1000 are born annually in the United Kingdom (UK) with congenital heart disease (CHD) (Pandya et al., 2016). Over 3000 cardiac surgical procedures were conducted in children during 2021–2022, approximately 2000 of these were on infants during their first year of life (National Institute for Cardiovascular Outcomes Research, 2023a, 2023b).
Many of these infants require ongoing medical and surgical support, and detailed parental involvement at home following hospital discharge, which for some parents includes daily monitoring, administering multiple medications and tube feeding their infant (Brown and Smith, 2018; Gaskin et al., 2018).
To address the gap in parents’ understanding of signs of deterioration, a parental early warning tool called the Congenital Heart Assessment Tool (CHAT) was developed by Gaskin et al. (2016) enabling appropriate contact and earlier management by clinicians. CHAT feasibility was evaluated (Gaskin et al., 2018) and demonstrated the importance of providing parents with information about when and who to call for management advice and support. CHAT was subsequently further evaluated in a multicentre quality improvement project, resulting in a second updated version called the CHAT2 (Gaskin et al., 2022; Smith et al., 2022).
The project site nursing team stopped using CHAT, as some staff were concerned that it would generate an increase in telephone calls from parents, resulting in an increase in their workload. In 2019, the ward manager, surgical and medical team were keen to implement CHAT2 for patient safety but wanted to understand the type of telephone calls being received and ascertain staff experience of taking telephone calls prior to implementation.
Availability of a telephone advice service is a specification for children’s cardiac networks in England (National Health Service England, NHSE, 2016). Furthermore, ‘each Specialist Children’s Surgical Centre must provide a 24/7 emergency telephone advice service for patients and their families with urgent concerns about deteriorating health’ (NHSE, 2016: 149). There is currently a dearth of evidence evaluating telephone services, nature of calls taken, clinical risk relating to management of concerns, associated workload, and experiences of healthcare professionals (HCPs) and other staff (medical secretaries) who take these calls. To enhance patient safety, we need a shared understanding of the context of telephone calls to ensure timely escalation of parental and HCPs concerns (National Health Service Employers, 2022; NHSE, 2021).
Aim
To evaluate the existing telephone service at the project site, identifying ways in which service effectiveness could be improved to enhance patient safety through patient and/or carer involvement.
Methods
This mixed-methods service evaluation, of the existing telephone service, followed the plan, do, study, act cycle (PDSA) (National Health Service England and NHS Improvement, 2022) and was undertaken during May–November 2019 (Figure 1). After planning the service evaluation, phase one [‘do/study’ stages] (reported elsewhere) prospectively evaluated: number of telephone calls received by HCPs from parents after their child had been discharged home; nature of parent’s concerns or queries and advice given to parents by HCPs. Phase two [‘do/study’ stages], a cross-sectional online survey, explored staff experiences of taking telephone calls from parents of children who had been discharged home under cardiac services care. Phase three was to ‘act’ on the findings and implement recommendations. This paper reports on phase two of the service evaluation and follows the Standards for Quality Improvement Reporting Excellence guidelines (Ogrinc et al., 2016). PDSA cycle.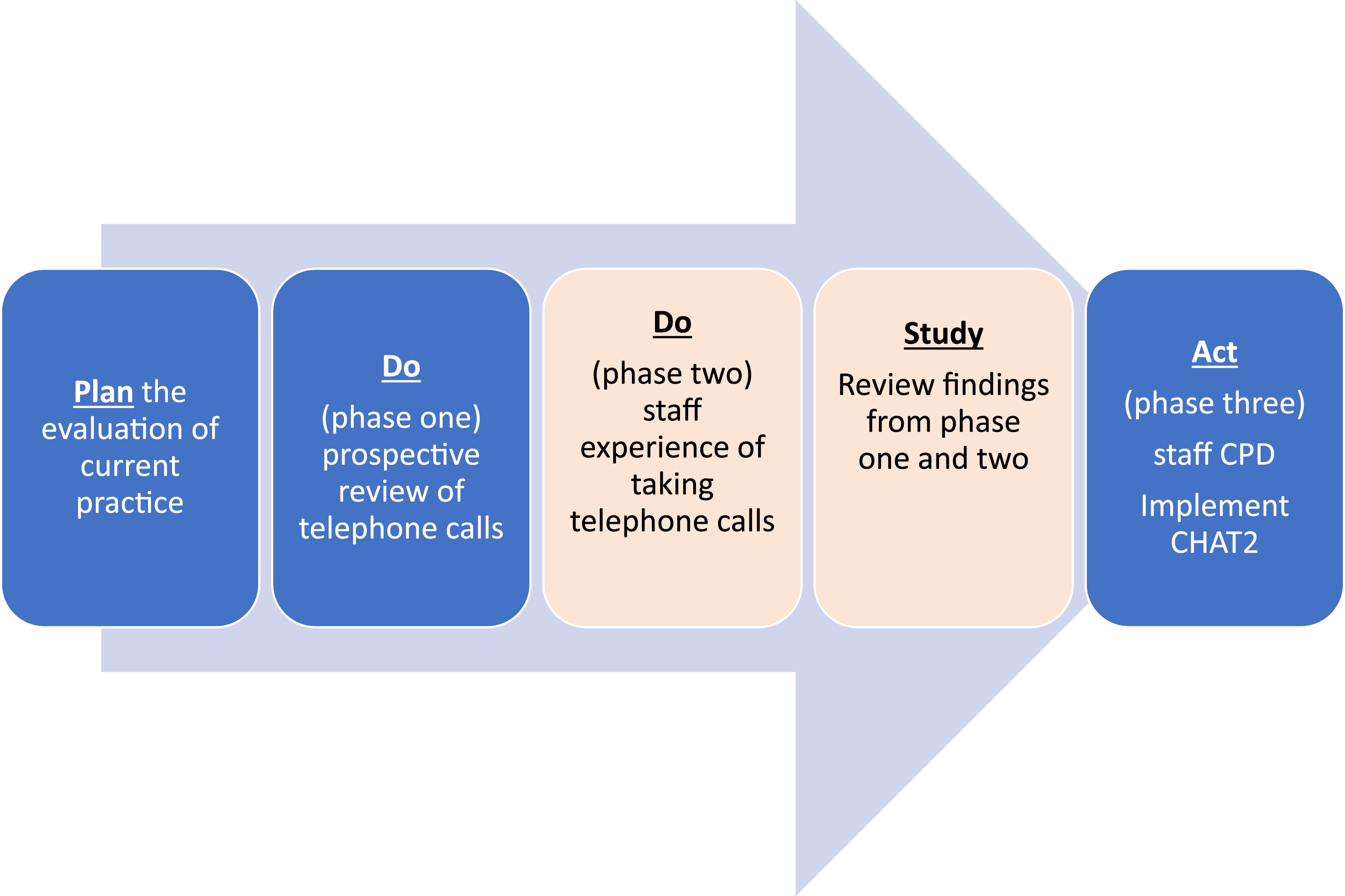
Figure 1 The Plan, Do, Study, Act cycle.
Setting
A tertiary level specialist children’s cardiac surgical centre in England.
Sample
All nurses, family support workers and medical secretaries (N = 86) employed in the children’s cardiac unit at the project site. There were no exclusion criteria.
Recruitment
The two ward managers invited staff to participate via an email. Additionally, invitation posters were displayed in the two staffrooms.
Ethics
Ethical approval was obtained from the University of Worcester, Health, Life And Environmental Sciences Research Ethics Panel (CHLES18190028) and the project was registered as a service evaluation on the Trust Clinical Audit Registration and Governance System. To fulfil requirements of this approval, participants completed a mandatory online consent question before proceeding to questions.
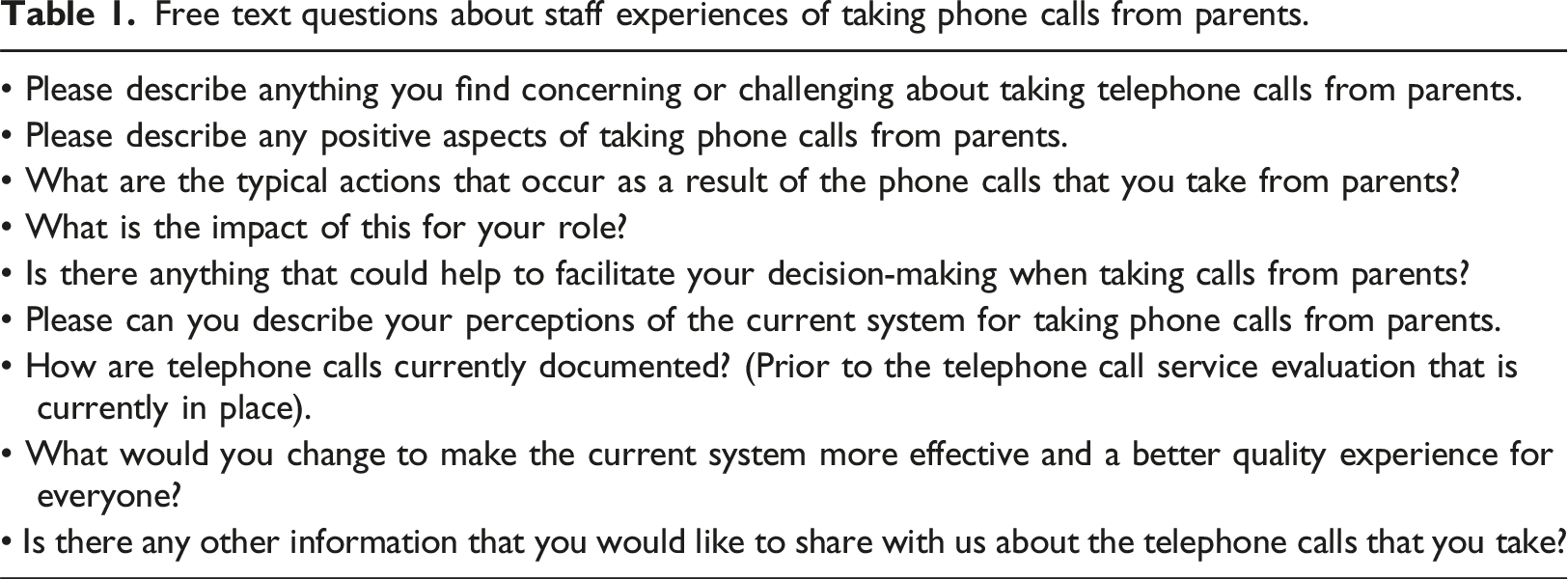
Data collection instrument
Free text questions about staff experiences of taking phone calls from parents.
Data collection procedure
For speed, flexibility and accessibility, the questionnaire was made available online, accessed via JISC online survey software (JISC.ac.uk), and paper copies were made available upon request.
Data analysis
Descriptive statistical analysis of quantitative data was undertaken using Microsoft Excel (v2101) and JISC Online Surveys (JISC.ac.uk). The qualitative responses to questions were thematically analysed according to Braun and Clarke (2006). Thematic analysis proceeded as follows: anonymous individual responses were downloaded from JISC.ac.uk and imported into QRS International NVivo12 (NVivo), and the project was then shared via NVivo with the project team. The team, an honorary nurse researcher (academic), nurse researcher (Paediatric Intensive Care) and a Consultant Cardiologist (working in the service), familiarised themselves with the data by individually reading responses, making notes and initial codes. These started as free nodes (stand-alone nodes that had no clear connection with other nodes). Creation of free nodes occurred less frequently as the coding progressed because references in the data began to fit into existing free nodes. The NVivo project was shared so that we could review each other’s coding. The number of free nodes varied and at this stage some of the free nodes were combined to make parent and child nodes. The team met to discuss the nodes for each question, their meanings and to search for generic themes across the whole data set. These generic themes were reviewed, refined and renamed by the whole team.
Findings
Participant demographics, venue and number of telephone calls taken.
Participants were asked to recall the most common types of queries that parents called to discuss and could choose multiple items. The most common were perceived as: ‘concern about child’s condition/deterioration (cardiac related) - asking for advice’ (n = 37/39, 94.9%); ‘medication/prescription checks/updates’ (n = 33/39, 84.6%) and ‘wound care’ (n = 22/39, 56.4%). Interestingly, n = 4 (80%) of medical secretaries also received calls about cardiac condition and medications. Examples of ‘other’ included insurance and holiday advice, next follow-up appointments, surgery and fit to fly queries.
Participants were asked to rate their confidence with taking telephone calls on a scale of no confidence (n = 0), slight confidence (n = 1/38, 2.6%), moderate confidence (n = 17/38, 44.7%) and high confidence (n = 20/38, 52.6%).
Five statements were provided, asking participants what they would do if they were unsure about how to answer a parent’s query. Only three statements were chosen: ‘I am unsure but will find someone who knows the answer’ n = 23/38 (59%); ‘take the parents details and offer to call them back’ n = 11/38 (28.2%) or ‘redirect the call and ask another colleague to take over’ n = 4/38 (10.3%). ‘Tell the caller that I am too busy at the moment and that I will call them back so that I can find an answer’ and ‘avoid answering the telephone when I can’ had no responses. Two participants provided an answer in the ‘other’ box: ‘I would take both the parents details and offer to call back after discussing this with a colleague if I was unsure’. And ‘Ask another colleague and call back’.
Qualitative themes
Three themes emerged relating to areas for quality improvement: safety, challenges (workload and communication) and educational requirements (role expectations, staff education and training, parent discharge preparation and expectations). These themes are presented with anonymised salient quotes. All quotes are written verbatim and labelled with the participant’s role and number, and role as either ‘nurse’ or ‘medical secretary’. Advanced practitioners were included in the nurse category to ensure anonymity.
Safety
Safety related to the complexity of giving advice over the phone and the risks involved with doing so. Almost a third of the respondents (n = 11/39, 28%) described it was not possible to assess a child visually over the phone; this increased their concern and created anxiety, for example:
“[I] Can’t see child over the phone and worry how serious they could be” (Nurse, 11)
Some suggested that not seeing the child, made them have a lower threshold for advising parents to seek review, for example:
“[I am] Unable to see [the] child so always ask parents to go to GP or A & E if concerns” (Nurse, 23)
Another participant clearly summarised the range of safety issues arising from a telephone call relating to a deteriorating clinical condition, including the level of responsibility for nurses and their concerns about being to blame for a child becoming critically unwell: “Some parents want you to assess their children over the phone, which you cannot do with 100% confidence as you can’t see them. Therefore, if they are describing their child’s deteriorating clinical condition, 9 times out of 10 you have to encourage them to get their child seen by a health care professional as ascertaining the severity of their child’s illness can be difficult to assess (the parents may not know what a ‘sick child’ looks like or may not have the ability to recognize this; they may not have been educated as to worrying signs and symptoms to look for). You need to clearly signpost them in the right direction for further help and clarify that they have understood that they need to seek more urgent help. This can cause increased anxiety or increase attendances to the ED, but nurses feel that they need to cover themselves with advice given and want to make sure that they do not ‘get the blame’ if something goes wrong [and] a child becomes critically ill at home or worse and they have not advised parents to take their child to be seen at time of phone call” (Nurse, 34)
The second key safety issue related to telephone calls about medications, particularly when parents contacted cardiac services out of office hours. Many staff found this a stressful situation, for example: “[It is] Stressful when parents phone at 10pm when they have run out of medication” (Nurse, 28)
or when the pharmacy was closed: “If [it is] to do with medications being needed and pharmacy [is] shut, usually bank holidays or Friday evening/weekend” (Nurse, 20)
The third safety issue, related to telephone calls, was where the query could not be answered by the person taking the call, because there was no-one available to ask for advice, for example: “When I am unsure of the answer, and it is needed urgently and there is no one available who knows the answer” (Nurse, 32)
Another participant explained: “it’s a lot of responsibility providing information or advice to parents. They may not like or want to hear the advice given” (Nurse, 12)
Challenges (workload and communication)
The perceived challenges and impact of taking telephone calls for most participants was the effect of taking telephone calls on their workload, such as taking telephone calls that had been directed to the wrong person or the time it took to arrange prescriptions or deal with medication enquiries, for example: “[And] parents phone out of hours for medicines as they have run out which is difficult to organise on top of my patient workload” (Nurse, 4)
Another challenge to workload was the difficulty trying to access patient information to answer the query: “Difficult [when read doctor’s advice] or to get up details of patient on [system] as nurses can’t access it” (Nurse, 16)
and this participant agreed: “Parent’s demand prescriptions. No details / weight on patient. Unable to get on [system] to find patient details” (Nurse, 24)
Communication challenges included language barriers, but also having to talk to a parent they felt was angry or patronising or a parent that they felt disliked the advice that they were being given: “Some of the parents can be patronising” (Medical secretary, 36)
and “Challenging is sometimes a language barrier and poor reception on the phone. Angry parent” (Nurse 2)
Challenges – proposed solutions
Some participants proposed solutions to facilitate a better experience for staff and to help manage these challenges, such as ensuring that all staff have access to patient details: “[as long as we have] access to patient details and current care and medical plans” (Nurse, 33)
and ensuring that parents are given information before discharge that guided them to the right person: “Giving [parents the] correct contact details when discharged. Switchboard /call centre asking correct questions, so call is put through to correct person rather than just putting through to the secs” (Medical secretary, 39)
Several participants suggested having a structured checklist that staff could refer to with guidelines about how to answer specific queries would be beneficial, for example: “Maybe an algorithm online” (Nurse, 21)
A solution to the workload impact of telephone calls was to have a designated phone line, dedicated times and a designated role or person to answer the calls and that the medical staff should also contribute. One participant suggested that they: “Could do with doctors sometimes taking calls too” (Nurse, 16)
Educational requirements
Educational and training requirements related to both staff and parents, with the key elements being consistency, education in assessing a child remotely and having access to senior support. From a staff perspective, educational needs related to ensuring consistency in the advice given to parents “[there are] not very clear guidelines, what to say to parents” (Nurse, 24)
This was deemed especially important for junior staff. The responses in theme one (safety) also indicate that there is potentially an educational requirement in relation to safely assessing the condition of a child over the telephone. Responses relating to consistency of advice included the suggestion of having: “A system in which we have guidelines to follow, so we all provide the same advice” (Nurse, 18)
as per theme two (Challenges). Participants also indicated that obtaining advice from senior colleagues or nurse in charge helped them in their decision-making when taking telephone calls.
There was also a perception that using a standardised method of recording notes from a telephone consultation was necessary. Some participants said there was nowhere to document, whilst others reported using a ‘ward book or communication book’. However, whilst indicating the need for a standardised method of documentation, several participants suggested that this would add to their workload; there was no description of the safety of accurate documentation in these responses: “Some form of record system would be beneficial; however, this is adding on our current workload!” (Nurse, 17)
The data suggested that education was required to ensure that everyone was using the same approach for documentation.
The educational requirements of parents perceived by staff related primarily to parents: “Knowing who can specifically help with what type of query” (Medical secretary, 37)
and being given the “Correct contact details when discharged” (Medical secretary, 39)
Additionally, theme one (safety) suggests that there may be educational and discharge preparation needs for parents in relation to their child’s clinical condition, medication and wound care.
Discussion
This project evaluated the telephone service in a tertiary level specialist children’s cardiac surgical centre in England, through exploration of staff experiences of taking telephone calls. The project identified issues relating to patient and staff safety, workload and communication challenges, and education needs that could be improved to enhance patient safety through parent involvement.
The CHD Standards indicate that the purpose of a telephone service for children, discharged home with a confirmed cardiac abnormality, their families and carers is to provide 24-h access to expert advice and support (NHSE, 2016). Access to specialist expert advice is important for the safety of these vulnerable children at home. Furthermore, robust parental discharge preparation is needed to accurately recognise signs of deterioration in their child with CHD (Crowe et al., 2016; Gaskin et al., 2016, 2018; Gaskin, 2018; March and Keim-Malpass, 2018; Tregay et al., 2016a, 2016b, 2017).
Crowe et al. (2016) recommended discharge and post-discharge care improvements including developing structured discharge documentation, enhanced home monitoring for patients with high-risk cardiac diagnoses and early warning tool for parents and community HCPs.
Around the same time, another team was developing a parental early warning tool, called the Congenital Heart Assessment Tool (CHAT), to address the gap in parents’ understanding of signs of deterioration (Gaskin et al., 2016). Created predominantly for parental use after discharge home from hospital following the first of three stages of cardiac surgery for functionally univentricular hearts, the CHAT gives parents action indicators depending on whether their baby is in the green category (continue as normal), amber category (telephone call to ward for advice) or in the red category (emergency telephone call for an ambulance) (Gaskin et al., 2016).
The CHAT empowers parents to articulate their infant’s needs clearly and in a timely manner (Gaskin et al., 2018). Further evaluation has demonstrated the usefulness of the CHAT early warning tool for tertiary and community HCPs working with parents to escalate their concerns, effectively indicating amber and red triggers and the action required (Smith et al., 2022).
Staff not using a tool and not being appropriately trained to structure their assessment, decision-making and documentation undertaken during telephone calls potentially creates safety and quality risks (Car and Sheikh, 2003). UK nurses are bound by the Nursing and Midwifery Council (NMC) Code (NMC, 2018), which puts the interests of people first ensuring that care and safety is the nurse’s main concern.
Nurses have a legal ‘duty of care’ (Dowie, 2017) to their patients and must practise effectively and preserve safety in line with best available evidence, keeping clear and accurate records (NMC, 2018). A duty of care exists when giving telephone advice to an advice-seeker, whether that is a parent, patient, family member of another HCP and the advice-giver or their employer may be found liable to negligence where the duty of care owed is breached and the patient harmed as a result (Devlin, 2014).
Furthermore, professional and ethical obligations to ‘practice effectively’ and work within their level of competence when giving advice, means any advice given must, as far as reasonably possible, be accurate (Devlin, 2014; NMC, 2018). It is, therefore, understandable that participants in this project identified anxiety, fear of blame and level of responsibility bestowed upon them when taking telephone calls from parents and giving advice.
Complexity and volume of telephone calls may leave parents and staff susceptible to errors (Haimi et al., 2020). Interruption from other work activities, can directly affect performance, compromise decision-making processes and work efficiency; particularly if the interruptions occur during the performance of complex activities that necessitate greater concentration (Monteiro et al., 2015).
Some studies have associated interruptions with the increased incidence of errors in the administration of medication (Colligan and Bass, 2012; Tomieto et al., 2012). Conversely one study suggested that interruptions may contribute to increased safety, increased comfort of patients and help nurses to be more accurate in their tasks (McGillis Hall et al., 2010). There was, however, only a small percentage of improvement to safety identified and as such the results should be considered with caution. The advantage for some children at home, whose parents are calling to escalate a concern, could indeed be one of safety if a structured early warning tool is used to rapidly assess, escalate and treat concerns (Gaskin et al., 2016, 2018; Smith et al., 2022).
Participants in this project also identified safety concerns about medications and the process for supporting parents on the telephone to obtain repeat prescriptions out of hours. Within children’s cardiac services, medicines are regularly prescribed that are termed ‘off-label’ or ‘unlicensed’; however, these have been associated with a greater incidence of medication errors, adverse drug reactions and unplanned hospital admissions when compared with licenced medicines (Bellis et al., 2014; Conroy, 2011; Horen et al., 2002).
Whilst this treatment is typically initiated in secondary or tertiary care, the responsibility for repeat prescriptions lies with the General Practitioner (GP) or community pharmacist. However, there is evidence to suggest that GPs and community pharmacists have a poor understanding of the licencing process and the implications of supplying unlicensed or off-label medicines to children (Chisholm, 2012; Mukattash et al., 2011; Venables et al., 2012). This may explain why parents experience problems obtaining these medications (Husain et al., 2017) and are often reliant on obtaining their child’s medication through their cardiac centre at short notice. Further work is needed to address the nature of these issues at home (Dahmash et al., 2020).
We believe this is the first paper to specifically report on staff experiences of taking telephone calls from parents of children with CHD in the UK and there is a lack of research considering staff experiences of telephone calls in other diseases also. Gischler et al. (2008) evaluated how often and for what reason parents of children born with congenital abnormalities (not including CHD) used a 24-h telephone helpline.
The most common call typology was about feeding problems (23.7%), but the study did not ascertain the nurses’ experiences of taking those calls. Sandelius and Wahlberg (2020) considered telenurses experiences, but these were nurses making planned monitoring calls to parents of children with gastroenteritis, versus unplanned telephone calls being taken by the staff in our project. Sandelius and Wahlberg (2020) found that nurses aimed to provide self-care at home in a patient safe way, focussing on increasing parents’ feelings of security, and monitoring calls provided a learning opportunity for nurses and parents as well as potentially relieving pressure on services.
Finally, there are studies exploring the benefit of telemedicine and teleconferencing with parents and children with CHD as part of a home monitoring programme, and these have demonstrated some success in terms of feasibility, accessibility and acceptability of the technology and decreasing parental anxiety (Morgan et al., 2008; McCrossan et al., 2008). Given the rapid changes to delivery of services required during the Coronavirus disease 2019 pandemic, other digital methods of communication with parents (such as videoconferencing) used during this time could be further explored.
Limitations
This was a small single centre service evaluation of staff experiences of taking telephone calls at one timepoint and, therefore, the findings cannot be generalised. The response rate (45%) was also potentially a limitation as more than half of invited staff did not participate. A recent meta-analysis of online surveys identified that an average online survey response rate is 44.1% (Wu et al., 2022). The sample did not include doctors and allied health professionals who also take telephone calls and, therefore, the findings were not fully representative of all staff in this cardiac unit. The responses also reflected what staff perceived that they did, rather than reflections on observed practice. This inaccurate recall is a recognised limitation of surveys (Safdar et al., 2016). The survey did facilitate staff completion as it was convenient, anonymous and relatively quick to complete, however, a limitation was that we were unable to follow up with participants to clarify responses or probe further (Safdar et al., 2016).
Implications for clinical practice
Safety, training, education, and service delivery implications for staff and parents regarding provision and receipt of consistent specialist information and advice were identified. Utilising a standardised model for assessment, communication, decision-making and documentation and clear signposting for parents about who to call for which query were recommended. Furthermore, the current telephone system could be safer and more effective by creating a dedicated telephone line, with a designated person to take the calls and designated medical staff availability for advice and support. Debrief support for staff from the Medical Consultants after taking complex telephone calls, would enable staff to talk through and reflect on their decision and advice in a supportive developmental way.
The results of this project, and highlighted risks, were presented at the cardiac audit meeting in November 2019. The Cardiac Surgeons and Cardiologists agreed with recommendations to improve service effectiveness during phase three (‘Act’). These being, firstly, to provide continuing professional development to all nursing staff in the cardiac unit during 2020. All nursing staff were given a 7.5-h study day to complete the free e-learning resource for the CHAT2, available via the Congenital Cardiac Nurses’ Association website https://www.ccn-a.co.uk/. Secondly, implementation of CHAT2 to provide a structured method for preparing parents pre-discharge, for parental assessment and early escalation of a child’s clinical deterioration at home. Implementing the tool would also assist staff assessment, decision-making and documentation when taking telephone calls from parents. Thirdly, further monitoring of risks and evaluation of impact of CHAT2 implementation and education will follow, repeating the PDSA cycle.
Conclusion
Whilst there were some positives identified of taking telephone calls, this project identified that taking telephone calls was perceived as high risk and staff felt in a vulnerable position when they could not see the child. Taking calls can be time consuming alongside the daily clinical workload of staff and systematic assessment and recording processes were deemed necessary. Implementation of the updated early warning tool CHAT2 (Gaskin et al., 2022) was recommended, along with staff and parental education to enhance safety through structured communication, assessment, decision-making and documentation of parents worries and concerns.
Footnotes
Acknowledgements
Amanda Daniels, Associate Lecturer, University of Worcester supported recruitment and data collection. Thank you to all members of staff that participated in this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.