
Abstract
Transgender and gender-diverse (TGD) populations are identified as high-risk for negative healthcare outcomes. Limited data exists on experiences of TGD youths in healthcare. The review aim is to systematically review literature on healthcare experiences of TGD youths. Seven electronic databases were systematically searched for relevant studies. Pre-determined eligibility criteria were used for inclusion with a double-screening approach. Sixteen studies were included. Studies included were quality appraised, data were extracted, and findings were synthesized narratively. Four narratives were identified including experiences of: accessing care, healthcare settings and services, healthcare providers, and healthcare interventions. Long waiting times, lack of competent providers, and fear were reported as challenges to accessing gender-affirming care. Negative experiences occurred in mental health services and primary care, while school counseling and gender clinics were affirming. Puberty blockers and hormone-replacement therapy were identified as protective factors. TGD youths are at risk of negative health outcomes due to an under resourced healthcare system. Further research is needed to assess interventions implemented to improve TGD youth’s experiences.
Introduction
Health disparities are health differences experienced by populations, commonly reported in the context of a perceived advantaged group, and are linked to economic, social, and environmental disadvantage (Carter-Pokras and Baquet, 2002). Health equity aims to reduce and subsequently eliminate health disparities in society (Braveman, 2014; Gerlach and Varcoe, 2021).
Transgender and gender-diverse (TGD) youths experience significant health related disparities such as limited and delayed access to care (Bauer et al., 2009; Bradford et al., 2013). TGD individuals are those whose sex assigned at birth is incongruent with their experienced gender identity (Lindqvist et al., 2021). Estimations of the TGD youth population range from 1.3% to 2.7% of the gross population which is a marked increase compared to the TGD adult range of 0.1% to 2% (Goodman et al., 2019). TGD population reports higher rates of suicidality, not only in comparison to cisgender counterparts but also Lesbian, Gay, and Bisexual (LGB) peers, with a greater prevalence within younger age groupings (Hunt et al., 2020).
Johns et al. (2019) reported TGD youths are more likely than cisgender peers to report violence victimization, suicide risk, and substance use. Although it is known youth from the general population experience delays in accessing health care (MacDonald et al., 2018) and poor health outcomes (Marie-Mitchell & O’Connor, 2013), recent evidence suggests that TGD youths’ experiences are more challenging owing to invalidating environments (Call et al., 2021). TGD identity is linked to intrapersonal, interpersonal, and societal stressors that are seldom experienced by cisgender counterparts (Hunt et al., 2020).
Gender dysphoria, according to American Psychiatric Association (2022), is a clinically marked distress related to an individual’s lack of congruence between assigned gender and experienced gender identity. TGD adolescents with gender dysphoria are likely to experience co-morbidities such as anxiety and depression (De Vries et al., 2011). A retrospective cohort study identified a two-to-threefold increase in risk of negative mental health outcomes for transgender youth (Reisner et al., 2015). A significant disparity relating to perceived general health amongst TGD youths was reported, with 62.1% rating their general health as poor, fair, or good (Rider et al., 2018). TGD youth who obtain early and evidence-based intervention for dysphoria are less likely to experience negative health outcomes (De Vries et al., 2014).
Evidently TGD youths require more input from mental health and general healthcare providers. On average, LGBT + education accounts for 2.2–5 h of healthcare provider’s education, with TGD-specific education absent from almost all developed curricula (Hana et al., 2021). Rowe et al. (2017) explored primary care providers’ knowledge of LGBT + health noting further education is required to increase cultural competency of providers. An understanding of experiences of TGD youth across healthcare, and factors impacting experiences is imperative to enhance and ensure equitable healthcare delivery.
Aim
To identify and synthesize qualitative research on healthcare experiences of TGD youths. Review objectives include: (i) identifying healthcare experiences of TGD youths; (ii) identifying factors impacting healthcare experiences of TGD youths; and (iii) exploring recommendations by TGD youths to improve healthcare experiences.
Methods
Review methods and reporting were based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (Page et al., 2021). Authors of this review are from various professional backgrounds including higher education, mental health nursing, general nursing, and senior research. Authors also identify across the spectrum of sex, gender, sexuality, and ethnicity. Regular reflexive conversations occurred among all authors which helped minimize potential biases and ensured representation of the TGD youths voice in synthesis and reporting of results.
Eligibility criteria
Eligibility criteria were pre-defined according to review aim and objectives. The Sample, Phenomenon of Interest, Design, Evaluation and Research framework underpinned eligibility criteria (Cooke et al., 2012). Studies focusing on healthcare experiences of TGD youths under 18 years were included to capture experiences of those under the age of consent. Studies focusing on cisgender, or TGD experiences outside of healthcare were excluded. Qualitative research and mixed-methods research with isolated qualitative findings were included; other research designs were excluded. Full eligibility criteria can be found in Supplemental Table S1.
Search
First author conducted a scoping search of Academic Search Complete, Cumulative Index of Nursing and Allied Health Literature plus with Full Text, American Psychological Association PsycInfo, SocINDEX with Full Text, MEDLINE, Social Sciences Full Text (H.W. Wilson), and American Psychological Association PsycArticles to identify relevant keywords used in research on TGD youths. Subject headings were sought from each electronic database and a single search strategy devised, in agreement with all authors. A systematic search of mentioned electronic databases was completed in 2021 and updated in 2022.
Synonyms of key terms “Experience,” “Transgender,” and “Healthcare” were used. Boolean operators “AND” and “OR” were used. Smart searching tools such as phrase searching, and truncation were employed. Limits included, studies published in English between January 2016 and July 2022. The five-year limit was employed following the introduction of the Yogyakarta Principles Plus 10 (International Commission of Jurists, 2017), which identified 10 additional human rights principles for sexual and gender diverse individuals. A hand search of reference lists of included studies and published systematic reviews (Brown et al., 2016; Chong et al., 2021; Heng et al., 2018; Wilson and Cariola, 2020) was conducted. An overview of the search is available in Supplemental Table S2.
Study selection
Covidence, the primary screening software for Cochrane authors, was used to screen records (Veritas Health Innovation, 2022). Duplicates were removed automatically in Covidence. A review of titles and abstracts, followed by a full-text review of remaining studies was completed. A conventional double screening approach was used. Conflicts were resolved by a third author. Articles identified during hand searching were also screened.
Critical appraisal
The Joanna Briggs Institute critical appraisal tool for qualitative research was used (Lockwood et al., 2015). This tool comprises 10 items to assess congruity between research methodology and philosophical perspective, research questions, data collection methods, representation and analysis of data, and interpretation of results (Lockwood et al., 2015). Further appraisal included locating researchers’ positions culturally or theoretically and their influence on the research, ethical approval, whether participants were adequately represented, and if conclusions drawn are consistent with analysis and interpretation of data (Lockwood et al., 2015). A conventional double screening approach was used during quality assessment whereby two authors voted “Yes” (Y), “No” (N), or “Unclear” (U) for each of the 10 items. Conflicts were resolved by a third author.
Data extraction
Data from included studies were extracted using a standardized table (Goodwin et al., 2021). Data extracted included: authors; country and setting; aim; number of participants; participants’ age range and identity descriptor; design of studies including data collection methods and data analysis; and key findings. Data were extracted by first author and cross-checked by remaining authors to ensure accuracy. A condensed data extraction table is presented in Table 2 and a comprehensive data extraction table found Supplemental Table S3.
Synthesis methods
A narrative synthesis was conducted in accordance with Popay et al.’s (2006) guidelines. This approach relies on the use of words and text to summarize, present, and explain findings from multiple studies. Data relating to TGD youths’ healthcare experiences were extracted into the data extraction table, creating a preliminary synthesis. Relationships within and between studies were explored to identify reoccurring concepts in line with current review aim and objectives. Narratives were constructed by condensing reoccurring concepts. Each narrative comprised illustrative stories from participants.
Identity descriptors were extracted from each included study and categorized into masculine presenting, feminine presenting, and gender diverse identities for ease of comparison. All narratives and gender identity descriptors were constructed by the first author and agreed by all authors.
Results
Study selection
A total of 3503 articles were identified within databases and 1294 duplicates were removed. The remaining 2209 articles titles’ and abstracts’ were screened for eligibility resulting in exclusion of 1726 studies. A full text review followed for 483 records. Of those, 469 records were excluded, and 14 studies included for review. Hand searching yielded two additional studies. In total, 16 studies were included in this systematic review. Study selection is presented in Figure 1. Preferred reporting items for systematic reviews and meta-analysis flow chart identifying results from the search strategy.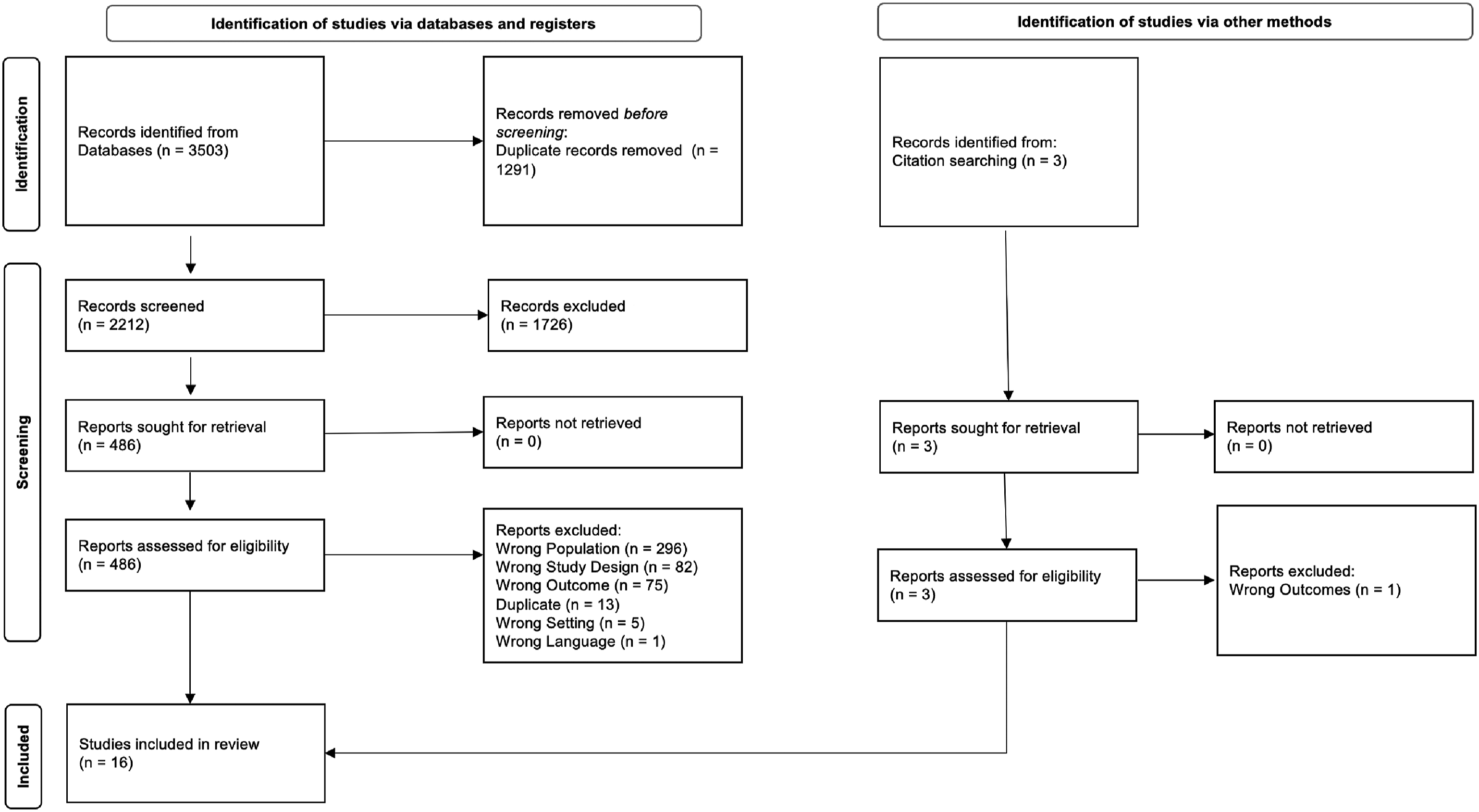
Study characteristics
Thirteen studies were qualitative and three were mixed-methods. Seven studies were conducted within the USA, with Australia, Canada, and the United Kingdom (UK) representing three additional studies each.
Study characteristics of included studies (n = 16).
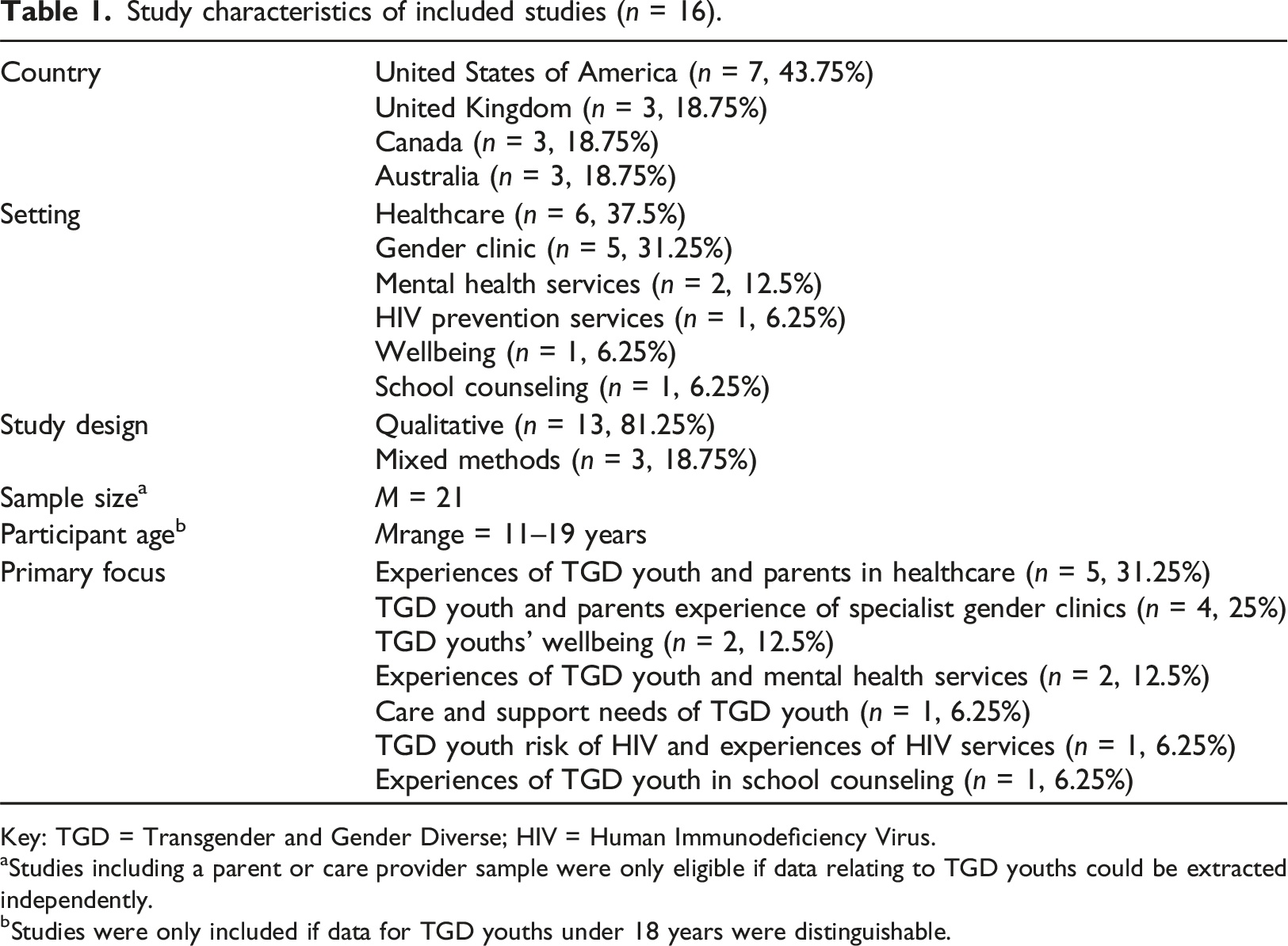
Key: TGD = Transgender and Gender Diverse; HIV = Human Immunodeficiency Virus.
aStudies including a parent or care provider sample were only eligible if data relating to TGD youths could be extracted independently.
bStudies were only included if data for TGD youths under 18 years were distinguishable.
A condensed data extraction table for the included studies (n = 16)
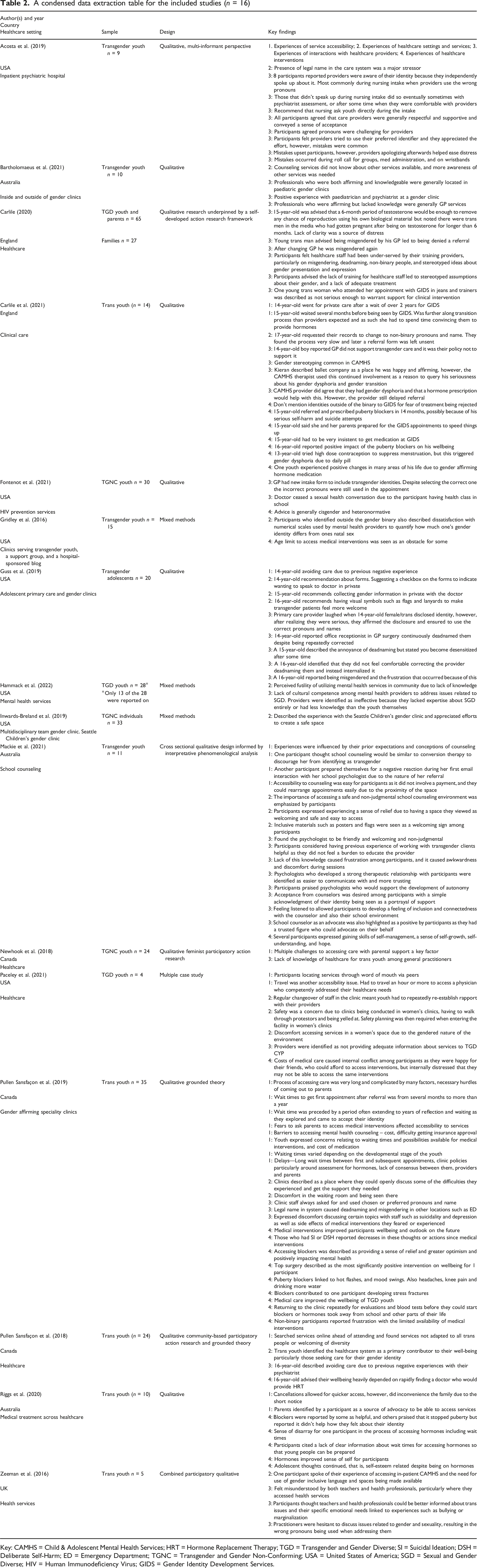
Key: CAMHS = Child & Adolescent Mental Health Services; HRT = Hormone Replacement Therapy; TGD = Transgender and Gender Diverse; SI = Suicidal Ideation; DSH = Deliberate Self-Harm; ED = Emergency Department; TGNC = Transgender and Gender Non-Conforming; USA = United States of America; SGD = Sexual and Gender Diverse; HIV = Human Immunodeficiency Virus; GIDS = Gender Identity Development Services.
Critical appraisal
All studies appropriately drew conclusions from analysis of data and established congruity between research methodology and interpretation of results. All but two studies (Mackie et al., 2021; Newhook et al., 2018) had congruity between the research methodology and research question. Newhook et al. (2018) utilized a participatory action research framework, employing a pre-determined questionnaire limiting congruity between methodology and data collection. Guss et al. (2019) utilized a qualitative approach but a mixed-methods program for analysis, limiting congruity between methodology and analysis. Three studies aimed to identify experiences of TGD youths and parents; however, appeared to underrepresent TGD youths in results (Bartholomaeus et al., 2021; Inwards-Breland et al., 2019; Newhook et al., 2018). These three studies also missed reporting the influence of researcher on the research and vice versa (Bartholomaeus et al., 2021; Inwards-Breland et al., 2019; Newhook et al., 2018). Quality assessment results are available in Table S4.
Four narratives were identified through data synthesis: (i) experiences of service accessibility, (ii) experiences of healthcare settings and services, (iii) experiences of interactions with healthcare providers, and (iv) experiences of healthcare interventions. An overview of narratives and quotes can be found in Supplemental Table S5.
Experiences of service accessibility
Factors influencing service accessibility were explored in nine studies. These primarily related to care avoidance due to fear of negative reactions from providers or parents (Guss et al., 2019; Mackie et al., 2021; Pullen-Sansfacon et al., 2019), identification of gender-affirming services, (Bartholomaeus et al., 2021; Pullen-Sansfaçon et al., 2018; Paceley et al., 2021; Riggs et al., 2020), disparity of access (Mackie et al., 2021; Newhook et al., 2018; Paceley et al., 2021; Pullen-Sansfacon et al., 2019), and delays accessing services (Carlile et al., 2021; Pullen-Sansfaçon et al., 2019; Riggs et al., 2020).
A 14-year-old participant reported avoiding care, despite being unwell, due to fear of healthcare providers’ reactions (Guss et al., 2019). Youth’s healthcare engagement was impacted by expectations of negative reactions, with some expecting counseling to be a form of conversion therapy (Mackie et al., 2021).
Fear of negative parental reaction prevented youths accessing services early (Pullen-Sansfaçon et al., 2019). Fear delayed youths accessing medical interventions like puberty blockers, and hormone replacement therapy (HRT). Other participants identified parents as advocates who assisted them in accessing treatment in hospitals (Riggs et al., 2020).
Participants used LGBT + peers to identify TGD affirming services (Paceley et al., 2021). Online searches were also used to identify if services were affirming (Pullen-Sansfaçon et al., 2018). Service providers’ insular view of care affected their ability to signpost effectively (Bartholomaeus et al., 2021).
Cost of gender-affirming care was noted as a distinct disparity. One participant reported cost impacted their ability to access gender-affirming interventions such as top surgery (removal of breast tissue) (Paceley et al., 2021). Another participant worried about their ability to afford gender-affirming medication, however, identified parents as a source of financial support (Pullen-Sansfaçon et al., 2019). Not all participants had financial or emotional support of parents (Newhook et al., 2018). Access to school counseling was more frequent due to the lack of cost involved (Mackie et al., 2021).
Lack of geographically accessible gender-competent resources was highlighted as an issue. Participants traveled over 2 hours to find physicians that competently met healthcare needs (Paceley et al., 2021). School-based counseling was geographically beneficial to participants (Mackie et al., 2021).
Waiting times to access gender-affirming services was identified as another barrier to service accessibility (Carlile et al., 2021; Pullen-Sansfaçon et al., 2019; Riggs et al., 2020). Delays were common with participants waiting several months to 2 years for first appointment with Gender Identity Development Services (GIDS) (Carlile et al., 2021; Pullen-Sansfaçon et al., 2019). Due to waiting times, a 15-year-old participant advised their transition was advanced which impacted care due to confusion within GIDS (Carlile et al., 2021). Another participant reported accessing private healthcare due to delays in receiving an appointment (Carlile et al., 2021). Instances of swift accessibility were also identified. One participant was able to access care due to a cancellation, however, this caused inconvenience due to short notice (Riggs et al., 2020). A 15-year-old participant was able to access puberty blockers in 14 months, due to ongoing mental health factors (Carlile et al., 2021).
Experiences of healthcare setting and service
Factors influencing TGD youths’ experiences of healthcare settings and services related to experiences of gender clinics (Inwards-Breland et al., 2019; Paceley et al., 2021; Pullen-Sansfaçon et al., 2019), mental health services, (Acosta et al., 2019; Carlile et al., 2021; Gridley et al., 2016; Hammack et al., 2022; Mackie et al., 2021) and recommendations to improve healthcare services (Guss et al., 2019; Mackie et al., 2021).
Gender clinics were identified as a safe space where participants could be open and not feel judged (Inwards-Breland et al., 2019; Pullen-Sansfaçon et al., 2019). Participants acknowledged the setting of gender clinics impacted their sense of safety (Paceley et al., 2021). Gender-affirming care within women’s clinics was noted as potentially unsafe and uncomfortable due to the gendered nature of the service (Paceley et al., 2021).
Child and Adolescent Mental Health Services (CAMHS) were described as futile due to a perceived lack of support for the queer community (Hammack et al., 2022). Gender stereotyping was reported as commonplace within CAMHS (Carlile et al., 2021). Individuals’ assigned name within the care system caused instances of deadnaming (use of birth name instead of chosen name) and misgendering (use of incorrect pronouns or incorrect assumption of gender identity) in inpatient mental health settings (Acosta et al., 2019). Non-Binary participants also reported frustration with mental health numerical scales to quantify dysphoria (Gridley et al., 2016).
Recommendations by participants included spaces that are safe, inclusive, and gender-affirming. Using LGBT + material such as lanyards as a visual symbol of acceptance within healthcare (Guss et al., 2019). Participants in school counseling praised the availability of LGBT + material (Mackie et al., 2021). Youths in this environment also recommended a need for improved confidentiality (Mackie et al., 2021).
Experiences of service provider interaction
Factors impacting experiences of service provider interactions were discussed across 13 studies predominantly focusing on deadnaming and misgendering (Acosta et al., 2019; Carlile, 2020; Fontenot et al., 2020; Guss et al., 2019; Zeeman et al., 2017), lack of provider knowledge or experience (Bartholomaeus et al., 2021; Carlile, 2020; Hammack et al., 2022; Mackie et al., 2021; Newhook et al., 2018; Zeeman et al., 2017), and service providers being accepting or judgmental (Acosta et al., 2019; Carlile, 2020; Carlile et al., 2021; Mackie et al., 2021; Pullen-Sansfacon et al., 2019; Zeeman et al., 2017).
Identity disclosure to healthcare providers was perceived by participants as difficult and uncomfortable. Disclosure commonly occurred during admission, with nursing staff, however, some participants waited till trust was established (Acosta et al., 2019). During a participant’s disclosure to their GP, the provider initially “chuckled” but realized the participant was serious and sought to establish correct pronouns and chosen name (Guss et al., 2019: 346).
Deadnaming was commonly reported by participants in primary care settings, even when gender identity was highlighted (Guss et al., 2019). Repeated deadnaming by a primary care office receptionist resulted in one participant feeling unsafe (Guss et al., 2019). A 15-year-old participant internalized their discomfort with deadnaming and accepted it as a part of transitioning (Guss et al., 2019).
Misgendering was reported by participants across services resulting in feeling anxious and frustrated with service providers (Acosta et al., 2019). Participants advised apologizing after a mistake is made can alleviate a lot of discomfort (Acosta et al., 2019). One participant recounted a frustrating incident of misgendering with their doctor whereby they selected their pronouns, and incorrect ones were still used (Fontenot et al., 2020). Misgendering by one participant’s GP resulted in denial of a referral and a decline in mental health (Carlile, 2020). Misgendering reoccurred when this participant changed GPs, resulting in feelings of judgement and worthlessness (Carlile, 2020). Participants agreed that providers were reluctant to discuss gender and sexuality, which resulted in instances of misgendering (Zeeman et al., 2017). Participants recommended healthcare providers, specifically nurses, explore aspects of gender identity during admission (Acosta et al., 2019).
Lack of TGD healthcare education was noted across primary care settings (Bartholomaeus et al., 2021; Newhook et al., 2018). One GP was affirming but lacked knowledge of medical interventions such as Hormone Replacement Therapy (HRT) (Newhook et al., 2018). Discussions around sexual health were discontinued by GPs upon learning TGD youths had sexual health education in school (Fontenot et al., 2020). One participant felt let down by their doctor for not providing adequate education on the transition process (Paceley et al., 2021). Lack of timely information from healthcare providers relating to delays accessing hormones was detrimental, as youths felt they had no time to prepare (Riggs et al., 2020).
Mental health providers were also identified as lacking knowledge about TGD healthcare, additional needs of the population, and cultural competence (Hammack et al., 2022; Zeeman et al., 2017). Knowledgeable professionals were identified in paediatric gender clinics (Bartholomaeus et al., 2021). Lack of knowledge and experience had negative impacts on participants within school counseling (Mackie et al., 2021). School counselors who had previous experience with TGD clients were perceived as knowledgeable and sensitive, and created an effective therapeutic relationship (Mackie et al., 2021). Participants expressed relief about not having to educate counselors about TGD health in this case (Mackie et al., 2021). Participants recommend providers be educated comprehensively about TGD healthcare to ensure a knowledgeable gender-affirming service (Bartholomaeus et al., 2021; Carlile, 2020; Hammack et al., 2022; Mackie et al., 2021; Newhook et al., 2018; Zeeman et al., 2017).
Feeling judged or accepted by healthcare providers was a common experience explored by participants (Acosta et al., 2019; Carlile, 2020; Carlile et al., 2021; Mackie et al., 2021; Pullen-Sansfacon et al., 2019; Zeeman et al., 2017). One participant was denied access to TGD healthcare because it was against policy to support it (Carlile et al., 2021). Another participant had their gender dysphoria and desire to transition queried because of involvement in ballet (Carlile et al., 2021). Participants reported feeling judged by nurses for the bathroom they chose within CAMHS (Zeeman et al., 2017). A trans woman was denied further clinical intervention in GIDS because of their outfit (Carlile, 2020).
Experiences of acceptance were also reported by participants (Acosta et al., 2019; Mackie et al., 2021). Participants agreed care providers were generally respectful and supportive and strived to create a sense of acceptance (Acosta et al., 2019). School counseling was identified as an accepting space (Mackie et al., 2021). The school counselor reacted to participants in a supportive and non-judgmental manner impacting participants’ sense of inclusion and connectedness with the service and school (Mackie et al., 2021).
Experiences of healthcare interventions
Experiences of healthcare interventions (e.g., puberty blockers, HRT, and surgery) and factors associated with these experiences were noted across six studies. Provision of interventions was described as frustrating and disorganized (Carlile et al., 2021; Riggs et al., 2020). Convincing providers of the need for interventions was described as frustrating (Carlile et al., 2021).
One TGD youth was advised 6 months of HRT would remove their ability to reproduce; however, they saw other TGD people reproduce, causing confusion (Carlile, 2020). After being diagnosed with gender dysphoria, a participant was left without a referral to gender specialist services despite serious mental health issues related to their dysphoria (Carlile et al., 2021).
Non-binary participants were disappointed with lack of medical interventions available (Pullen-Sansfaçon et al., 2019). Transgender non-binary participants hid their non-binary identity from providers due to fears of interventions being stopped (Carlile et al., 2021).
Participants’ mental health was positively affected by interventions. Accessing hormone therapy resulted in positive outcomes to wellbeing (Carlile et al., 2021). Medical interventions reduced the prevalence of suicidal ideation and self-harm (Pullen-Sansfaçon et al., 2019). Interventions instilled a sense of relief, greater optimism for the future, and positively impacted overall wellbeing (Pullen-Sansfaçon et al., 2019).
Negative effects of medical interventions were also explored. Gender dysphoria increased for one participant taking a daily high-dose contraceptive (Carlile et al., 2021) with other youth developing stress fractures which were attributed to puberty blockers (Pullen-Sansfaçon et al., 2019). Puberty blockers caused several physical symptoms such as hot flushes and excessive sweating (Pullen-Sansfaçon et al., 2019). Some participants’ gender identity was not affirmed by puberty blockers (Riggs et al., 2020). Attending clinics for blood tests and assessments took away from other aspects of participants’ lives (Pullen-Sansfaçon et al., 2019). Despite potential negative effects of interventions, participants expressed they would not consider discontinuing them (Pullen-Sansfaçon et al., 2019).
Discussion
This review aimed to identify and synthesize qualitative research on healthcare experiences of TGD youths in healthcare settings. Care avoidance was reported by several TGD youths citing fear of no parental support, and discriminatory experiences within healthcare services and with providers. While TGD youths are at higher risk of negative physical and mental health outcomes, barriers to help-seeking exist which do not allow engagement with healthcare, including discrimination and lack of sensitivity (Safer et al., 2016). Parental support of TGD youths positively impacted mental health and life satisfaction (Simons et al., 2013). Therefore, to improve help-seeking behaviors among youths, supportive and non-judgmental parents and providers would be beneficial.
Cost and geographical location were frequently reported as challenges to accessing gender-affirming care. TGD youths identified feelings of guilt and worry about the cost treatments placed on their households (Kearns et al., 2021). Cost was directly impacted by disparities within insurance plans, particularly in countries such as the USA where universal healthcare is not available (Kearns et al., 2021). The geographical distribution of clinical care for TGD youths was examined in the USA and was found to affect provision of TGD care negatively (Weixel and Wildman, 2022). In the UK, the need for de-centralized gender identity services was highlighted with recommendations for localized gender services (Cass, 2022).
A need for services that are safe, gender-affirming, and knowledgeable was identified. Experiences of participants varied across healthcare services, with particularly positive experiences noted in gender clinics and school counseling. Experiences in primary care services and mental health services, however, were primarily negative. Similar findings were noted within the TransPULSE study which highlighted poor competency among providers, resulting in one-third of participants having unmet healthcare needs (Giblon and Bauer, 2017). Lack of competent providers is also identified within primary care settings, resulting in TGD youths taking an active role in their care provision (Vermeir et al., 2017). Gender clinics were noted for their gender-affirming approach with positive experiences being linked with level of competence (Wright et al., 2021). A lack of competency exists among healthcare providers and responsibility is being placed on TGD youths to address this issue. A standardized gender-affirming approach delivered by competent providers has the potential to positively impact experiences of TGD youths within healthcare.
A lack of adequate TGD healthcare knowledge among healthcare providers and recommendations for additional training needs is regularly acknowledged. To aid in provision of gender-affirming care, the World Professional Association of Transgender Health (WPATH) released version 8 of the Standards of Care for the Health of Transgender and Gender Diverse People (Coleman et al., 2022). This incorporates a need for providers working with TGD youths to have additional training and expertise on gender identity development theory across childhood and adolescence (Coleman et al., 2022). A systematic review of current education provision amongst medical curricula worldwide found that, at undergraduate level, medical staff received between an hour to half a day of TGD specific education (Van Heesewijk et al., 2022). The Cass Report (Cass, 2022), which assessed current provision of gender specialist care in the UK, noted to provide a safe, viable long-term service, a multi-specialist provider approach including equal access to interventions for TGD youths is required. Further education provision and a review of current service provision are required to meet the standards and recommendations outlined by WPATH (Coleman et al., 2022).
Misgendering and deadnaming were reported frequently. Many linked misgendering and deadnaming to lack of provider knowledge of TGD healthcare. Of note, Stroumsa et al. (2019) posited a lack of correlation between increased knowledge and reduction in transphobia among healthcare providers. Using regression analysis, no reduction in transphobia was identified when TGD healthcare knowledge was increased. Discrimination is experienced frequently within primary care by TGD youths (Vermeir et al., 2017). Despite barriers of current educational programs such as lack of TGD healthcare resources, it is imperative that undercurrents of transphobia are addressed (Van Heesewijk et al., 2022).
Positive physical and mental health benefits of healthcare interventions were explored. Participants reported their desire to remain on treatments despite side-effects. A 60% and 73% reduction in odds of depression and suicidality, respectively, among TGD individuals who utilized healthcare interventions was identified (Tordoff et al., 2022). Lengthy waiting time and assessment period reduced participants’ ability to access medical interventions. Additional forms of appointment provision, including telehealth, and online video calls are being utilized in healthcare (Haleem et al., 2021). Telehealth was identified as a tool that would benefit the overall impact of cost and productivity (du Toit et al., 2021; Frye et al., 2022; Snoswell et al., 2022). The First Assessment Single-Session Triage (FASST) system was found to improve levels of depression, anxiety, and quality of life by reaching TGD youths earlier (Dahlgren Allen et al., 2021). A review of current waitlist systems and incorporation of additional methods of communication could reduce wait times of TGD youths resulting in faster access to medical interventions.
Limitations
Results from this review must be considered in the context of some limitations. While included studies met most critical appraisal criteria, almost half did not report on positionality of researchers, therefore reducing trustworthiness. Reviewed studies were conducted in countries which are classified as higher income countries and with majority Caucasian populations. As such, results may not be generalizable to TGD youths in lower income countries or indigenous or minority racial groupings. Gender specialist services, mental health services, and primary care settings were overrepresented. It is therefore difficult to generalize experiences of TGD youths across other healthcare settings.
At the level of the current review, the search was limited to seven electronic databases and did not include records from Grey literature. Limits also included English language and timeframe, leading to omission of non-English studies and studies published prior to 2016, possibly increasing a risk of study selection bias.
Implications
This review has several implications for healthcare services. To ensure gender-affirming care, services need to engage fully with WPATH standards of care (Coleman et al., 2022). Informed by the Cass report (Cass, 2022), national healthcare services should review sustainability of current models of care employed for gender services. Gender-affirming approaches and TGD competent providers should be adopted across healthcare. Resolving existing transphobia within healthcare should be prioritized in parallel with interventions to increase provider knowledge. Although most studies were conducted within Western countries including the USA, Canada, and UK, the cultural environment of healthcare settings ought to be considered when exploring experiences of TGD youths accessing these facilities. Factors like unconscious bias and diversity within the workforce within these settings should be addressed in future research as this might influence experiences of access.
Reviewing healthcare curricula in higher education and including TGD healthcare would benefit future providers. Reviewing TGD healthcare interventions would benefit future intervention creation.
Conclusion
TGD youths are likely to identify negative experiences within primary care, mental health settings and occasionally gender clinics. While some positive experiences were identified, this was within services that were affirming or were willing to self-educate. Parents and providers can impact help-seeking behaviors of TGD youths, as such a gender-affirming approach should be used. Care disparities were identified across healthcare settings. Parity is necessary to ensure TGD youths avail of the same standard of healthcare services as their counterparts. Using alternative technology to access care, such as telehealth could reduce waiting times and allow quicker access to comprehensive care.
Supplemental Material
Supplemental Material - Transgender and gender diverse youths’ experiences of healthcare: A systematic review of qualitative studies
Supplemental Material for Transgender and gender diverse youths’ experiences of healthcare: A systematic review of qualitative studies by Ryan Goulding, John Goodwin, Aine O’Donovan and Mohamad M Saab in Journal of Child Health Care.
Footnotes
Acknowledgements
All individuals who have contributed significantly to this work are listed above as authors. There are no further acknowledgements necessary.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is carried out as part of a PhD which has been funded through scholarship by the Catherine McAuley School of Nursing & Midwifery, University College Cork, Ireland.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.