
Abstract
Parent experiences of child health services can be used to understand their value and optimise the support provision to families during critical developmental periods. A gap in the literature exists regarding parental perspectives of linked child development supports, particularly in disadvantaged areas. This study examined parent experiences of the impact and value of a community paediatric clinic (Kidscope) with linked, multi-agency supports in a disadvantaged area of Ireland. Using a qualitative analysis design, 10 parents participated in one-to-one interviews. A Community Advisory Group consulted on interview schedules. Data was thematically analysed in line with Braun & Clarke’s Framework. Five themes and twenty-two sub-themes emerged. Kidscope’s linked, multi-agency approach was valuable for engaging families, addressing developmental delay, supporting readiness for education, and developing parent–child relationships. Relational working and a child and family centred model of care empowered parents to become active agents in children’s health. Coronavirus disease 2019, national deficits in healthcare, and staff turnover impeded service delivery. Kidscope and linked supports work in partnership to disrupt the impact exclusion from healthcare has on vulnerable children and families. This study provides evidence of an effective integrated paediatric service delivery model designed around vulnerable children and families and highlights areas for improvement.
Background
Children living in disadvantaged communities, areas which suffer most from a combination of economic, health, and environmental burdens (Ukpeh, 2009), are at greater risk of experiencing adverse childhood events which can negatively affect neurological development resulting in long-term impacts on developmental progress, self-regulation, and social-emotional functioning (Heckman and Masterov, 2007; Komro et al., 2013; Nicholson et al., 2012). A significant amount of developmental delay is avoidable (Buckley et al., 2022a). Research examining the impact of early detection and intervention initiatives show improved developmental trajectories and enhanced child outcomes (Komro et al., 2013; Nicholson et al., 2012; Shonkoff and Fischer, 2013). Lack of appropriate intervention within the critical period of development (conception to 6 years) can negatively impact children’s health, education, and psychosocial well-being (Nicholson et al., 2012).
Early intervention disability services in Ireland are delivered by both statutory and non-government agencies with wide variation and no national consistency in service provision (HSE, 2016). Attempts to reconfigure disability services from 2019 aimed to ensure children had fair and equitable access to services wherever they reside, however, significant issues remain in availability, access, wait times, communication with and quality of services (Inclusion Ireland, 2022). An ongoing issue exists whereby families from disadvantaged areas do not have the resources to pay for private assessment and intervention resulting in those from more affluent backgrounds accessing treatment and therapies faster (Carroll et al., 2013; Inclusion Ireland, 2022). A gap in the system therefore exists for disadvantaged families who do not have the means to access early intervention disability services (Buckley et al., 2022b).
Kidscope is a consultant-led community paediatric clinic set in a disadvantaged urban community in southern Ireland. Established in 2010, Kidscope is the only clinic of its kind in Ireland offering free health and developmental assessment and onward referral of vulnerable children aged zero to 6 years in their locality (Buckley et al., 2022b). Kidscope’s geographical catchment has a history of significant levels of deprivation (Pobal, 2019). Children are underachieving in developmental domains and experiencing poor educational and health outcomes (Buckley and Curtin, 2018). Kidscope is delivered in partnership with local child and family support agencies, utilising the strengths of existing services and their relationships with families. Kidscope’s inter-disciplinary team comprises of paediatricians, medical students, public health nurses (PHNs), speech and language therapists, and practitioners from local agencies: community public health nursing, NICHE, Let’s Grow Together, and Springboard. Through a linked multi-agency approach to supporting vulnerable children and their families, Kidscope aims to break the cycle of intergenerational poverty by disrupting the impact exclusion from healthcare has on child development (Buckley et al., 2022b). To do this, the clinic provides timely access to health and developmental assessment, onward referral to appropriate services, and a coordinated approach to follow-up care and support (Buckley et al., 2022c).
Previous studies have found that positive inter-personal communication from child healthcare providers effectively encourages engagement by vulnerable families (Lynam et al., 2010) and plays a key role in their management of child and family health (Wong et al., 2012). Findings also highlight the requirement for greater supports for parents in their attempt to engage with an often-arduous process of assessment, diagnosis, and intervention (Boulter and Rickwood, 2013). Boelsma et al. (2021) suggest parent experiences of child health services can be used to further understand the value of services and to contribute towards optimising the provision of supports to families during critical developmental periods. The need to further examine parent experiences of child developmental services was also highlighted (Boelsma et al., 2021). To date, very little has been reported on parent’s perspectives of engaging with a community paediatric clinic delivering health and developmental care in partnership with local services to vulnerable children and their families.
Aim
To examine parent experiences of engaging with a community paediatric clinic bolstered by local child and family services in a disadvantaged Irish community in order to: (1) Understand the perceived value of a linked multi-agency approach to supporting child development. (2) Contribute to the evidence base on optimising support provisions to vulnerable children and families during this critical developmental period.
Methods
Study design
Qualitative analysis of parent perspectives using one-to-one interviews.
Research question
The SPIDER Strategy tool (Sample, Phenomenon of Interest, Design, Evaluation, Research type) (Cooke et al., 2012) was used to construct research questions: • What are parent’s experiences of the impact and value of engaging with a paediatric outreach clinic bolstered by linked child and family supports in a disadvantaged Irish community?
Sub-questions
• How has engaging with Kidscope and linked services supported child development? • How has engaging with Kidscope and linked services benefitted families? • How has a linked multi-agency approach to supporting child development in the community encouraged the engagement of vulnerable children and families?
Reporting guidelines
The Consolidated Criteria for Reporting Qualitative Research Checklist (COREQ) (Tong et al., 2007) guided reporting.
Recruitment process
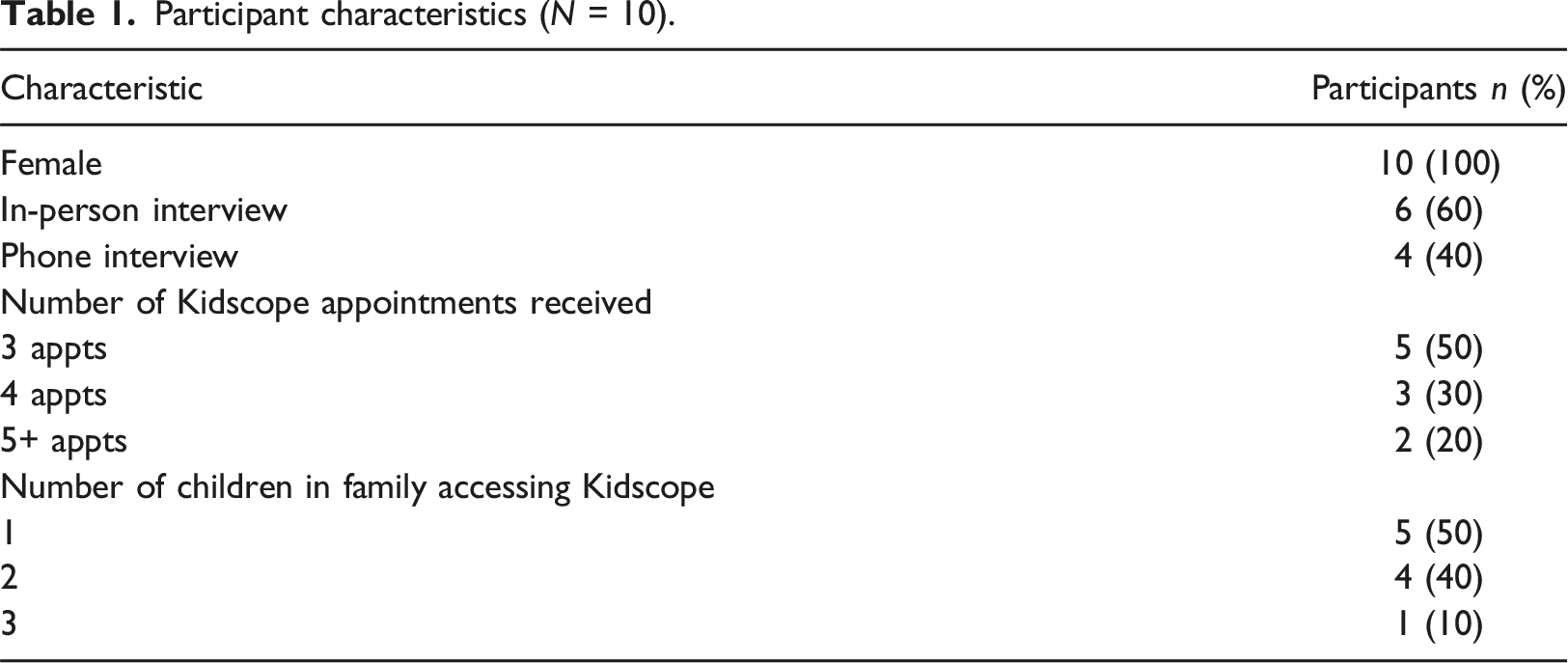
In a convenience sampling approach, parents who attended Kidscope between September 2021 and October 2022 received a study information sheet and were given the opportunity to ask questions. As this study was part of a larger research project examining Kidscope implementation, consent to follow-up and contact details was obtained for 50 parents interested in participating in project sub-studies. For this study, 10 parents were selected at random using ‘=RAND’ in Microsoft Excel. Selected parents were contacted, all agreed to participate, and a time and location for their interview was arranged. Fully informed consent was obtained in writing prior to interviews.
Inclusion and exclusion criteria
To ensure participants had sufficient knowledge and experience of Kidscope, participation was dependent on attending Kidscope on two or more occasions. Those who attended on one occasion were excluded from participation.
Data collection
Planning
A Patient and Public Involvement (PPI) Group, the Community Advisory Group (CAG), was developed to assist in research design, interview schedule development, interpretation of findings, and planning for knowledge sharing activities. The group consisted of the lead researcher and three community members. Two group members were parents living locally and the third was a family support practitioner working in the community. CAG members were not involved as research participants. Participant identities were protected at all times. To ensure adherence to best practice protocols for running a PPI group, the lead researcher completed relevant training.
Interview schedule development
The study’s main research questions guided the development of the semi-structured interview protocol (Supplementary file 1). Open-ended questions were supplemented by follow-up questions and probes allowing for increased dialogue between researcher and participant and elicitation of sometimes sensitive information. On completion of the first draft, mock interviews were set up with the CAG. Wording and meaning of questions were discussed as a group and the interview schedule was edited accordingly to create the final schedule. In addition, possible challenges during interview facilitation were discussed. CAG members highlighted possible issues with the wording of questions, willingness to answer certain questions, or potentially upsetting questions. Suggestions for eliminating and managing challenges were recorded and used by the researcher as an aid during interviews.
Interviews
Interviews were in-person at participants’ homes or at a secure and convenient community location. Phone interviews were offered to those unable to attend in-person; participants were asked to use a landline instead of mobile phone to limit signal issues and to position themselves in a quiet space with no distractions. Interviews were audio recorded and transcribed verbatim. In line with the guiding framework (Braun and Clarke, 2015), notes were developed alongside interviews. Reflections captured the researcher’s theoretical assumptions at pre-interview, during interview, and post-interview timepoints. Participant’s social cues were captured, focussing on verbal cues of those interviewed by telephone. A reflexivity statement was developed considering the researcher’s position within the research, questions asked, and interpretation of data. Being part of the interview’s social context, the statement included considerations of researcher positioning and approachability. The researcher being a parent also featured, and how this may influence responses to and interpretation of participant feedback.
Data analysis
NVivo (QSR International Pty Ltd, 2020) was used to collate data. Analysis was guided by Braun and Clarke, (2015) reflexive thematic analysis (RTA) framework and involved three phases. Phase 1: In an inductive approach, transcripts were coded to identify main themes and sub-themes. RTA assumes themes do not passively emerge from data; instead, they are creative and interpretive stories about data, produced at intersections between data, researchers’ theoretical assumptions, and their analytic resources and skill (Braun and Clarke, (2015). The lead author conducted line-by-line coding of individual transcripts, pooling codes, and developing overarching themes and sub-themes. Reflections documented during data collection aided engagement with and interpretation of data, and the CAG was consulted for assistance with interpretation, particularly meanings of colloquialisms and local sayings. Phase 2: In a two-reviewer process, a second author reviewed and provided input into themes and sub-themes, discussions took place during which differences of opinion were reconciled and definitions of themes agreed. Phase 3: Both reviewers completed a joint review and collapsing of overarching themes to develop a final set of themes and sub-themes. Quotations and sentiments were used to support findings and are denoted using pseudonyms.
Establishing trustworthiness
Trustworthiness of findings related to credibility, dependability, confirmability, and transferability (Connelly, 2016). Interview questions were tested with the CAG through pilot interviews. Feedback and suggested edits were incorporated to create final interview schedules. The CAG was consulted during data analysis to ensure accurate data interpretation, credibility, and dependability. To further enhance dependability, two reviewers engaged in transcript review and confirming themes and sub-themes. To achieve confirmability, excerpts were included to demonstrate how conclusions were drawn. Transferability was addressed by including a detailed description of findings to enable comparisons to be made.
Ethical considerations
Ethical approval was granted from the Clinical Research Ethics Committee, reference number ECM 03/2023 PUB.
Findings
Participant characteristics
Participant characteristics (N = 10).
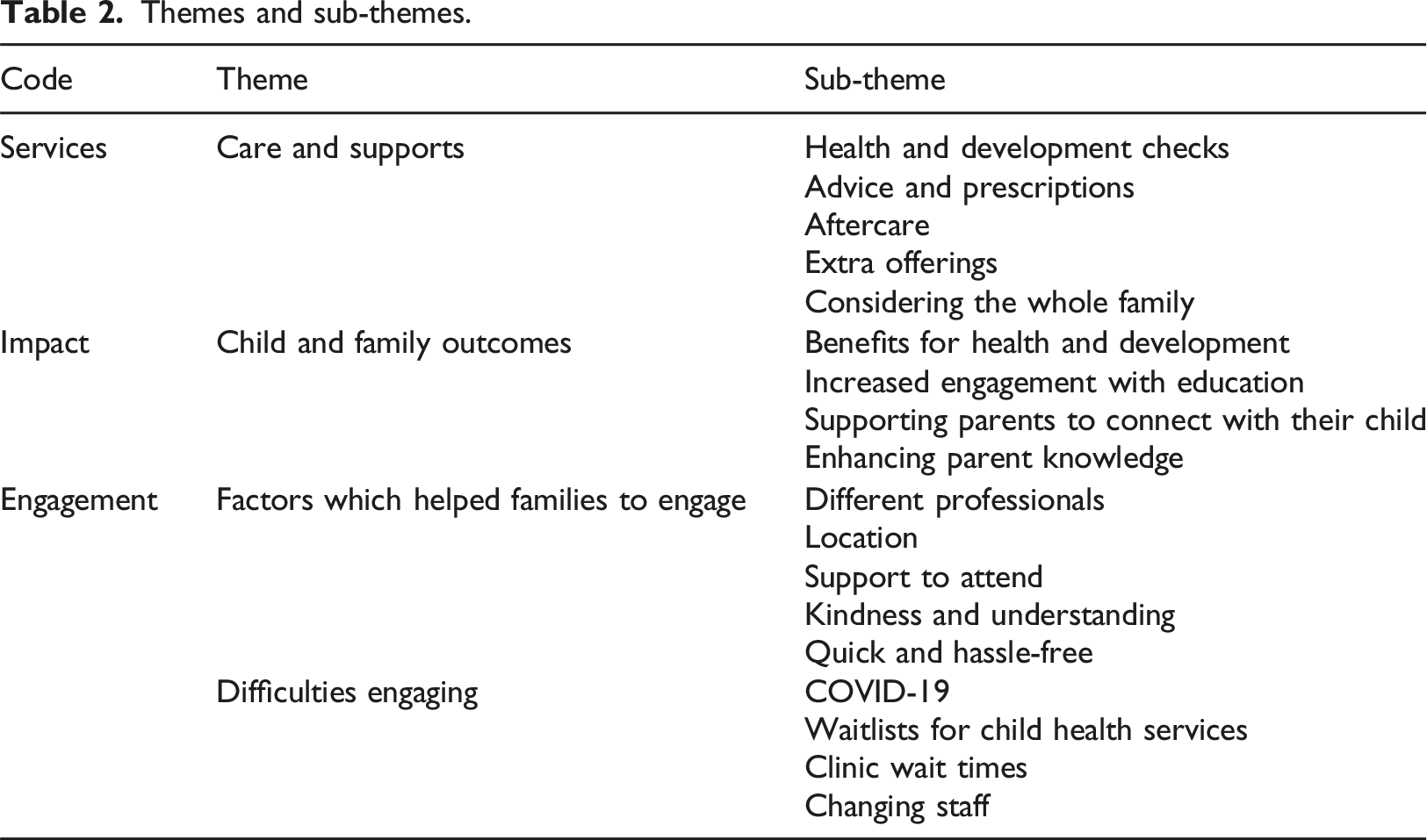
Thematic analysis
Themes and sub-themes.
Care and supports
A core theme emerging from the data centred on the value of care and supports delivered by Kidscope and linked services. Sub-themes included health and development checks, advice and prescriptions, aftercare, extra offerings, and a whole-family approach to delivering child health and developmental care.
Health and development checks
Receipt of detailed health and developmental checks as part of the Kidscope process was regarded as most valuable and beneficial for families, “they went through my son’s physical exam top to bottom, head to toe” (Janet).
The duration and thorough nature of consultations was useful for obtaining a comprehensive picture of children’s health and developmental status, “...they couldn’t have done any more for us. We were there for over two hours; they went through everything” (Liz).
Timely receipt of appointments was most valuable for participants who waited significantly longer for the same assessment by a Community Medical Doctor or hospital-based paediatrician, “we waited 2 to 3 weeks for our appointment at Kidscope. We got a letter recently to see the same doctor in the hospital… that appointment took two years to get” (Catherine).
Involvement of linked services in the Kidscope process provided an extra layer of support for families. In a whole community approach, Local PHNs posted Kidscope developmental questionnaires prior to appointments, community health workers assisted families with questionnaire completion, and Let’s Grow Together home visitors supported families to attend appointments, “she knew my child so well from the home visits, and she was able to help me explain what he struggles with and my concerns about his development” (Helena).
Advice and prescriptions
Participants received information and advice for several child health and development issues including gross and fine motor delay, speech, language, and communication delay, and social and emotional concerns. Guidance and support were also provided for toileting, feeding issues, and skin conditions. Sleep was found to be a common issue requiring advice and medications. Participants reported receiving prescriptions to help implement a sleep routine as part of the Kidscope care plan, “We couldn’t have done it without the Melatonin. It took a bit of time, but we eventually got him into a routine. He doesn’t need any [Melatonin] now, he only wakes once a night… the whole family is sleeping better now and he’s happier” (Helena).
Aftercare
As part of the Kidscope process, PHNs phoned families after consultations to discuss the care plan and to clarify advice or answer parent queries. Let’s Grow Together home visitors provided home-based support for toileting, feeding, social and emotional issues, and speech, language, and communication delay. Play therapy and parent counselling were provided by Springboard Family Support service. Participants noted the value of this aftercare, “we got advice from the doctor at the clinic but the PHN checked-in the following day and again about once a week after that to see how we were getting on” (Mary).
Extra offerings
Telehealth calls made by Kidscope’s paediatrician and linked services during Coronavirus disease 2019 (COVID-19) lockdown periods were valued by families who found it difficult to access healthcare during this time, “she was the only doctor we could talk to. We got two phone calls. She went through everything, and we got his sleep medications renewed” (Helena).
Receipt of clinic reports and letters of support were beneficial for families applying for social welfare supports, in particular social housing, “The doctor gave us a letter with everything in it… about my kids’ needs and the type of house we needed” (Janet).
Considering the whole family
Kidscope supported child development by considering the family as a whole. The paediatrician regularly supported parental health and well-being, “She would ask me how I was doing too. She would say “you need to mind yourself, your health is just as important”. She would ask about all the family” (Catherine).
Participants referenced the value of being able to bring their other children to Kidscope consultations. Lack of childcare often resulted in participants being unable to attend medical appointments where limits on numbers were enforced, “it was so important to us to have our other children there because our son is so loving to his baby brother…the doctors were able to see this and how well he can play with them” (Helena).
Ensuring consistency, linked services also adopted a whole-family approach when providing child health and developmental supports. This was found to contribute to parental health and well-being, particularly for parents of children with health and developmental challenges, “I cried after every group because I was so happy to see [my son] play with all the children. They would ask me ‘how are you doing?’, it was so lovely to be asked that” (Mary).
Child and family outcomes
Engagement with Kidscope and linked services resulted in several child and family outcomes including benefits for health and development, enhancing engagement with education, supporting parent–child connections, and parental encouragement.
Benefits for health and development
Kidscope and linked services provided essential monitoring and support for child health and development often not offered by other services, “without Let’s Grow Together my son’s sleep apnoea wouldn’t have been flagged, and without Kidscope we wouldn’t have been seen in the hospital and had the surgery he needed….without this my son might not be alive today” (Janet).
Kidscope provided an efficient pathway for referrals to primary care and early intervention services, “referral forms were completed for everything we needed” (Helena).
The range of disciplines available in Kidscope was beneficial for child development. Accessing specialists such as speech and language specialists was important for parents given the wait times to specialist services through the national disability system, “He was slow developing in all areas really… Kidscope referred him for every service he needed but he actually got to see speech and language therapist in Kidscope too” (Liz).
Parents regarded the advice and support offered in relation to sleep and diet as important for overall health and development but also for effectively managing child behavioural issues, “I thought he was just bold. His granny would say that his dad was the same. Since we changed his diet and got help for his sleep, he is like a different child now” (Jessica).
Increased engagement with education
Kidscope was found to help children’s engagement with education. As referrals to primary care and early intervention services were organised in a timelier manner, children were developmentally better able to engage in education because of the support received through Kidscope, “because of everything organised [in Kidscope], he is speaking more and he is calmer. He goes into preschool now and loves it, he is able to leave me at the gate without crying… he can talk and play with his friends without hitting or lashing out” (Mary).
Implementing recommended sleep routines resulted in improved child engagement with peers and school-based activities, “my kids were so tired, the preschool would ring saying my son lashed out at the other kids. The doctor gave us Melatonin and told me to put them to bed at the same time every night and give them a bath, to keep the same routine every night… they jump out of bed and love going into school now” (Catherine).
Guidance was offered to parents regarding local schools best suited to manage their child’s development. With assistance from linked service practitioners, the Kidscope team recommended schools which offered resources and facilities to best support children’s needs and requirements, “…his speech was improving slowly. The doctor explained that this might affect his reading later on. She recommended the school with the best resource unit” (Helena).
Supporting parents to connect with their child
Parent-child connections were encouraged and enhanced through guidance to parents regarding increased engagement in one-to-one activities with their children, “she was in the walker a lot, the doctor told me to get a rug for the floor and to do more tummy-time with her instead” (Catherine).
Referrals to local parenting programmes enhanced parent’s capacity to build relationships with their children. Learning about children’s behaviours empowered parents to better manage behavioural outbursts, “it opened my eyes to how I was dealing with his outbursts. Instead of giving out to him, I just ignore the bad things now and we focus and spend time on the good things he does” (Janet).
Receipt of books through Let’s Grow Together’s community book scheme organised through Kidscope created opportunities for parents and families to connect with their children through reading, “the speech and language therapist said I should use books with my son, even if he couldn’t read them. We read together now by looking at the colours and the pictures… we get a book every month in the post now too” (Helena).
Enhancing parent knowledge
Advice and knowledge provided by Kidscope and linked professionals improved parent’s understanding of child health, development, and well-being. Information acquired throughout the Kidscope process also helped parents to connect with other community services. Participants received advice about effectively linking with services, “They told me to keep a diary of her [my daughter’s] development so that I could bring it along to other appointments. This turned out to be really good because I have a record of everything now and I can tell them exactly about when her development went backwards” (Catherine).
Parents were encouraged to understand more about their child’s developmental strengths during Let’s Grow Together home visiting sessions, “She would say things to me about her that I hadn’t even spotted like “look at her now doing that and showing you this”, I was amazed. It opened my eyes to all the things my daughter does do” (Hannah).
Factors which helped families to engage
Parents regularly described elements of Kidscope and linked services that promoted engagement and helped to further support child health and development. The availability of practitioners from different disciplines, the kind and understanding approach of clinic staff, location, support to attend, and the quick and hassle-free nature of Kidscope were all found to facilitate engagement and promote continued attendance.
Different professionals
Delivery of child health and developmental care by a range of disciplines at Kidscope benefitted children and families. Participants valued the integrated approach of Kidscope’s inter-disciplinary team across the wider community, “…she did the assessment at Kidscope and about 3 months later we were called for our first community speech and language appointment in the primary care centre. Because she had done the first session at Kidscope and had all of my son’s information, we were able to start the therapy straight away” (Mary).
Parent and toddler groups facilitated by Let’s Grow Together speech and language therapists as part of Kidscope’s care plan effectively supported children’s speech, language and communication, “…she would stay back and give tips and handouts to work on his speech. She told us what to do to help him communicate and what not to do” (Helena).
Collaboration between Kidscope and linked services ensured families didn’t get ‘left behind’ (Helena) by any one service. This approach was most beneficial for parent’s who were previously overlooked by services, “…it’s not just one service, it’s the PHNs and all the others too. They make sure nothing is forgotten and that we aren’t forgotten” (Jane).
Medical students interacted and played with children which allowed parents to speak freely with clinicians and share sensitive information, “they were great to play with my daughter when I was trying to talk… They would try to find the area she liked to play in most and they would focus on playing with her there” (Hannah).
Location
Kidscope’s ‘relaxed’ and ‘homely’ atmosphere and its proximity to participants’ homes encouraged engagement, “it’s just down the road, it’s great. It was really welcoming and they [the staff] were so helpful. It didn’t feel like a normal doctor’s office or like a hospital appointment” (Laura).
The informal, calming nature of the centre positively affected children’s engagement with the service and the Kidscope team, “I definitely think this helped when my son was being examined… he didn’t become distressed waiting like he usually does… the doctor was able to examine him properly” (Laura).
Ease of access to centre staff outside of consultation hours was of benefit to parents who had questions about or required assistance with their child’s care plan, “I can call the centre anytime if I have questions in between appointments. They [community health workers] photocopy reports if I need them or send me out letters” (Jane).
Support to attend
Support to attend Kidscope was offered in a number of ways. Families were provided with a warm welcome by centre staff, “My son is autistic and doesn’t like some surroundings, but he never had a problem going into Kidscope. He liked the toys in the reception, and the lady behind the desk would always give him a biscuit” (Jane).
Reminder phone calls from community health workers in the days prior to appointments were found to be highly beneficial. Let’s Grow Together home visitors attended Kidscope appointments with families to corroborate parent's observations and concerns about their children and to help them articulate their experiences of their child during consultations, “She knows us so well and because I can’t always remember everything I should say in the appointments, she came to explain the problems we have with my daughter’s speech” (Jessica).
The ability to re-organise appointments also encouraged attendance. Parents described having to juggle various life commitments and the needs of their children and how this often meant they were unable to attend every clinical appointment, “Life just gets in the way or sometimes the kids might be sick, I would just ring down to them and ask for another appointment, there was never a problem they would offer another date and time” (Hannah).
Kindness and understanding
The kind and understating nature of Kidscope staff effectively encouraged the engagement of families. Parents recalled the value of this approach compared to their experiences of other services, “…they would say “there’s no late here, come anytime, you’re always welcome”, you don’t get that anywhere else” (Laura).
Kidscope practitioners also made efforts to understand families’ circumstances and to make parents feel comfortable, “they would remember our story and I wouldn’t have to go over everything at the next appointment” (Catherine).
Being ‘listened to’ (Jane) was valued by parents as it helped them to remember and share important information about their child’s health and development,
“they wait for you to tell your story instead of bombarding you with questions… you need that time to remember everything” (Janet).
By listening to parents and giving them time to tell their stories, participants reported feeling ‘respected’ (Mary) by Kidscope practitioners, “I never felt judged, I felt she was there just as much for me as she was for my kids” (Catherine).
Quick and hassle-free
Timely access to Kidscope was valued by parents who often struggled to access services for their children, “…we waited two to three weeks for our first appointment and then we were seen every 3 or 6 months. We don’t even get seen in our GP as quick as that” (Hannah).
Support provided by linked service practitioners between Kidscope consultations was found to be vital for continued family engagement and adherence to care plans, “they’re the ones who call to the house or who pick up the phone when you need support, they are always there” (Hannah).
The hassle-free nature of Kidscope’s referral process was also important for parents who often experienced onerous form-filling and lengthy wait times before acceptance by services, “we didn’t have to do anything, they organised everything… we got a phone call about a week later to ask if we wanted to sign up” (Liz).
Difficulties engaging
The fourth theme centred on the difficulties experienced by participants when engaging with the Kidscope process. Four sub-themes included COVID-19, significant national waitlists for child health services, the time spent waiting in reception prior to Kidscope consultations, and changing staff.
COVID-19
Closure of Kidscope and all child and family services as part of COVID-19 measures significantly impacted parent engagement with services and their efforts to advocate for children’s health and development, “we had no more speech and language therapy, no more occupational therapy, no more physiotherapy… everything stopped” (Helena).
Closure of Kidscope and linked services further exasperated child behavioural and developmental issues causing additional frustration for parents, “after a while in lockdown it got really hard to manage her at home without Kidscope and the supports we were used to” (Jessica).
Families encountered additional barriers in the aftermath of COVID-19 as many children had aged-out of child development programmes when services resumed, “it wasn’t their fault, but it was such a shame, he was too old for any groups or home visiting” (Helena).
Parents summarised the detrimental effects of the limited care and support available to children during and in the aftermath of COVID-19, “I’ve seen huge difference in my child. He totally went backwards, his speech got worse, his behaviour got worse, he’s anxious and doesn’t want to go into school now… he was never like that before” (Liz).
Waitlists for child health services
Lengthy wait times for primary care and early intervention services impacted the implementation of care plans, threatening potential benefits of Kidscope and linked services for vulnerable children and their families, “the only negative really was waiting for the different things organised through Kidscope. We’ve heard nothing back from the Community Network Disability Team and it’s been over a year. There’s only so much they can do for us in Kidscope, she [my daughter] needs an ASD assessment and the disability team are the only ones who can do it” (Hannah).
Wait times for early intervention services were also found to disrupt the Let’s Grow Together service as home visitors took time away from directly supporting families to prepare letters of complaint on a family’s behalf, “…we hadn’t received anything back after nearly a year so she [the home visitor] helped me write letters complaining. She spent so much time helping us pull everything together” (Laura).
Lack of responsiveness by national disability and early intervention services caused frustration for parents and negatively affected families’ engagement with Kidscope, “Kidscope was fantastic but it feels like we get so much help there and then it’s just a waiting game for other services. We have been waiting to hear from Community Psychology for nearly two years. There’s no point returning to Kidscope until he is seen there because they are the only ones who can assess him” (Jane).
Clinic wait times
In-clinic wait times were challenging for children with complex needs, “…I took her up and down the road a few times before they rang me to come back for the appointment” (Hannah).
Parents felt long wait times impacted children’s presentations within consultations, “We waited for over an hour at one appointment and he was upset going into the room and for a lot of the appointment” (Catherine).
Changing staff
Parents regularly mentioned how staff changes within linked services negatively impacted their engagement. Re-telling their complex social histories to new community professionals was difficult for parents and posed a barrier to their attendance at Kidscope, “we got to know her [local practitioner] really well, she got us into Kidscope. One day a new face showed up at the door, the other lady had left the area – I had to explain our story all over again” (Mary).
Discussion
By examining parent experiences of engaging with a paediatric outreach clinic bolstered by local child and family services in a disadvantaged Irish community, this study aimed to understand the perceived value of a linked multi-agency approach to supporting child development, and to contribute to the evidence on optimising support provisions to vulnerable families during this critical developmental period. Through a structured and integrated whole community approach, participants experienced a multitude of benefits to child health and development and improved family outcomes. Specifically, the multi-agency approach adopted by Kidscope and linked services engaged vulnerable families, supported parents and caregivers to manage and advocate for children’s health and development, provided supports to improve child readiness for education, and enhanced parent–child relationships. (Hallberg et al., 2001).
Findings parallel those of previous research. Evidence shows the provision of community paediatric healthcare services is an effective approach to improving child health and well-being (Komro et al., 2013; Shonkoff and Phillips, 2000). Literature highlights the importance of community-based initiatives in disadvantaged areas due to the many barriers vulnerable families encounter when accessing healthcare (Buckley et al., 2022a; Kearney and Fulbrook, 2012; Leventhal and Brooks-Gunn, 2000). A report addressing intentions of the National Model of Care for Paediatric Healthcare in Ireland to integrate services and adopt a more appropriate model of paediatric care states, ‘This has not yet been realised. At community level, there is still significant variation across regions’ (HSE, 2018, p.2). The Kidscope model of community paediatrics provides a template for effectively supporting children and families in their locality, particularly vulnerable populations.
Families living in disadvantaged communities have been found to disengage from health and developmental services more frequently than those from more affluent areas (Wallbank et al., 2013). Boshoff et al. (2018) show trusting and constructive relationships between health practitioners and parents of vulnerable children can have a lasting influence on future relationships with support services. Parents in this study offered valuable insights into the factors that enabled engagement. Relational working by practitioners who demonstrated kindness, understanding, and empathy encouraged openness and trust with families and their continued engagement with Kidscope and linked services. Lewing et al. (2018) highlight the importance of supportive and trusting practitioner-child relationships as a component of family centred interventions designed to support vulnerable children. Likewise, the World Health Organisation (2018) regards this approach as imperative for improving the quality of paediatric care.
Parent knowledge was sought and utilised through parent-completed questionnaires and in-depth consultations. Evidence shows early identification of developmental delay can be dramatically improved by utilising parental knowledge when treating children with subtle developmental delay; (Marshall, 2014; Williams and Holmes, 2004). Through a child and family centred model of care, parents felt respected and listened to. Parents found Kidscope to be a non-judgemental and safe space to share knowledge of their children’s strengths and challenges. As a result, practitioners were better able to understand and appropriately support child health and development. Findings therefore suggest the reported benefits of engaging with Kidscope and linked services relate to parental knowledge sharing and becoming partners in their child’s care. Reeder and Morris (2021) suggest that despite parents feeling empowered in children’s care, negative relational behaviours with health professionals can undermine their confidence and lead them to feel abandoned and unsupported. Our findings provide evidence of the impact of trusting parent-practitioner relationships for enhancing opportunities to empower parents and caregivers.
Findings demonstrate the value of building parental capacities to understand, manage, and advocate for their child’s needs. Educating parents on child health and development concepts empowered them to engage with other services and become advocates for their child’s care. Findings align with Pullon et al. (2015) who suggest a greater awareness of health issues and improved parenting education is essential for successful engagement of families with integrated child health services. Our findings show through joint knowledge sharing whereby parents provided knowledge of their child’s health and developmental context and professionals enhanced parents’ knowledge of child health, development, and well-being, Kidscope and linked services supported child development in a more effective and sustainable manner.
Adding to the evidence on optimising support provisions to vulnerable families, challenges experienced when accessing Kidscope and linked services were highlighted. Participants reported substantial wait times to mainstream child health services and the impacts of this on Kidscope care plans. Deficits in the Irish healthcare system pose substantial barriers to the provision of therapy and diagnostic assessment. Gaps in the system for disadvantaged families without the means to access private services are widening (Buckley et al., 2022a, Buckley et al., 2022b, Buckley et al., 2022c). By year end 2022, 18,000 children with disabilities in Ireland awaited initial contact by the Network Disability Team (Irish Examiner, 2022) and 110,000 children were waitlisted for primary care services (Irish Times, 2022). Our study exposes additional consequences of such significant deficits in the Irish healthcare system by highlighting the knock-on impact wait times can have on wider child and family supports such as Kidscope and linked services.
COVID-19 emerged as an additional challenge to engagement and continued participation. Service closures and restrictions enforced as part of efforts to curb the spread of the virus exacerbated an already growing national issue and resulted in increased wait times for primary care and early intervention services. Recent studies show crises such as COVID-19 have a disproportionate impact on vulnerable populations (Curtin et al., 2021).
Findings also highlight the issue of staff turnover and the impact this has on building relationships with and supporting vulnerable children and families. High levels of staff turnover is a real issue in health and social care professions, particularly in areas of disadvantage where practitioners support families experiencing significant levels of adversity (De Hert, 2020; Woltmann et al., 2008). Strategies to support and protect practitioners are essential to safeguard service provision and to ensure consistent, high-quality care for vulnerable children. In the context of significant challenges facing families in accessing therapies and assessment due to the recent pandemic and staff shortages, our study provides evidence that vulnerable families benefit greatly from inter-agency working close to home.
Strengths and limitations
The qualitative study design provided an opportunity to capture and share parent voices and to document findings that are internationally relevant to social determinants of health. Use of a PPI group in questionnaire development facilitated a more understandable and considered set of questions to effectively elicit information from participants. Consulting with PPI group members during analysis facilitated a more comprehensive and unbiased interpretation of the data. Several limitations also exist. The small number of participants may not permit generalisation of results; however, the sample size was sufficient to provide insight into parental experiences. Mothers only participated due to the frequency of lone mothers in this community. This is consistent with previous research (Kearney and Fulbrook, 2012). Different interview formats, in-person and telephone, may mean discussions were influenced by the approach used. A systematic review comparing the effectiveness of both interview methods confirmed both telephone and in-person methods of gathering data as equally effective for human qualitative research studies (Rahman, 2015).
Implications for practice, policy and research
This study generates important insights regarding healthcare supports valued by parents and caregivers which empower them to become active participants in child health and development. Findings support tackling health inequity via a child and family centred model whereby clinicians adopt a relational approach to working with families, facilitating a service that is accessible to all but capable of responding proportionately according to levels of need. Policy makers can utilise findings to tackle social and structural barriers to healthcare access for vulnerable families. Findings align with international literature underscoring the importance of universal access to high-quality and free community paediatric care, as well as parenting education, support, and empowerment (Buckley et al., 2022a; Redder and Morris, 2021; Ridgway et al., 2021; Stahmer et al., 2017). There remains a need for continued measurement of the impact of paediatric clinics supported by linked services in disadvantaged communities and to capture the voices of those accessing and delivering services to better understand their impact and value in order to optimise service provision.
Conclusion
Previous research called for additional investigations into parent experiences of child developmental supports. By examining parent experiences of a paediatric clinic bolstered by linked child development supports in a disadvantaged community, this study yields important insights on the impact and value of a multi-agency approach to supporting vulnerable children and families in their locality. Through an integrated child and family centred model of care, Kidscope engaged vulnerable families, supported child readiness for education, encouraged the development of parent–child relationships, and enhanced parental capacities to identify, manage, and advocate for children’s health and developmental needs. Kidscope and linked services successfully provided vulnerable families with high-quality and responsive health and developmental supports and empowered parents to become active agents in their child’s care. Overall, our findings add to the evidence on promoting child health and development through effective parental engagement and support of the family as a whole. This study generates important insights into the health needs and values of a vulnerable population which can be used to thoughtfully examine current models of care within contemporary child health practices in Ireland and further afield.
Supplemental Material
Supplemental Material - Parent perspectives of engaging with a community paediatric clinic with linked child development supports in a disadvantaged area of Ireland
Supplemental Material for Parent perspectives of engaging with a community paediatric clinic with linked child development supports in a disadvantaged area of Ireland by Lynn Buckley, Katherine Harford, Louise Gibson, Nicola Cornally, Margaret Curtin in Journal of Child Health Care
Footnotes
Acknowledgements
We wish to acknowledge the main funders of the study, the Irish Research Council (Project ID: EBPPG/2019/197) and Let’s Grow Together Infant & Childhood Partnerships CLG Ireland. This work was part of a PhD project conducted through University College Cork Ireland in conjunction with the Structured Population and Health-services Research Education (SPHeRE) Programme Ireland.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The Irish Research Council (Project ID: EBPPG/2019/197) and Let’s Grow Together Infant & Childhood Partnerships CLG Ireland.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.