
Abstract
Parents and youth across Alberta were engaged to identify specific research questions that are a priority to them. Two lists, containing 27 topics were developed with local parent and youth advisory groups, and sent to participants via online questionnaires. Topics were rated from one (least important) to five (most important) and ranked in order of priority. Initial questionnaires were completed by 263 (46%) parents and 308 (54%) youth. Parents rated five topics (behaviour, learning, and developmental disorders; mental health; food, environment and lifestyle; quality of health care; and vaccines) and youth rated four topics (brain and nerve health; mental health; quality of health care; and vaccines) as a high priority. Research questions stemming from 4 parent (12 [5%]) and 6 youth (21 [7%]) focus group discussions were then ranked in a second questionnaire, completed by 43 (43%) parents and 56 (56%) youth. Parents’ highest ranked research question was ‘What is the effect of screen time on cognition and neurodevelopment for children and adolescents?’, while the highest ranked question from youth was ‘What are the early signs of anxiety and depression and when should an individual seek help?’. These topics highlight areas that are important to parents and youth where funding, research, and knowledge mobilization efforts should be directed.
Introduction
A growing body of literature supports the involvement of health care consumers (i.e. public, patients, patient advocates, or caregivers) in the design, prioritization, and dissemination of research and evidence based medicine (Wilson et al., 2015). This cultural shift, spurred by the phrase ‘nothing about me without me’, is changing the way in which policy makers, stakeholders, scientists and clinicians approach research (Chu et al., 2016). Seeking consumer input on the design, conduct, and translation of research can lead to research findings that are more pertinent to their needs (Domecq et al., 2014; Shen et al., 2017), create space for new ideas or innovations, provide a more holistic view of health, and increase the quality and relevance of the outcomes (Boote et al., 2010; Deverka et al., 2012; Kristine et al., 2017; Shippee et al., 2015)
Unfortunately, determining what health care topics are important for study is often determined by funding agencies and decided upon by researchers, whose priorities may differ from those of consumers (Crowe et al., 2015). It has been reported that this could lead to redundant and wasteful research findings, which do not inform real world decisions (Chalmers and Glasziou, 2009; Tallon et al., 2000). Although consumers are increasingly recognized as important research partners, a systematic map of priority setting research found that only 19% of over 250 studies involved both patients and clinicians in the process (Stewart and Oliver, 2008). Areas of potentially important research may be neglected, causing a mismatch between research being carried out and research evidence needed by consumers (Ioannidis, 2016). Ultimately this may impact health outcomes and health service use (Forsythe et al., 2019).
Engaging patients and families in setting research priorities (e.g. using Patient and Public Involvement approaches, where people with lived experience collaborate as research partners) may lead to funding of research that is of high relevance to them (Chalmers et al., 2014). For child health research, the perspectives of parents and children are rarely acknowledged. Two recently published Canadian studies used a modified James Lind Alliance (JLA) partnership with parents to identify unanswered research questions in paediatric preventative care (Lavigne et al., 2017), and for expectant parents and caregivers of children up to age 24 months (Brockway et al., 2021). However, much less is known about the priorities of youth in health research, and currently there is very little evidence linking youth priorities or experiences to health outcomes.
Involving patients and families in setting research priorities contributes to the growing emphasis on consumer-oriented health care (Canadian Institutes of Health Research, 2011). While previous paediatric priority setting partnerships have focussed on specific health topics, few have looked at prevention or general health priorities to set research and funding agendas (Modanloo et al., 2023). Further research exploring children’s, youth’s and families’ needs, and engaging with them to inform priority-setting research is needed.
Aim
The aim of the study was to identify health research priorities that are most relevant and important to parents and youth.
Methods
Design
The methodological approach was guided by components of a JLA Priority Setting Partnership (Nygaard et al., 2019), as well as common concepts for good priority setting practice (Viergever et al., 2010). Team members had prior experience with conducting priority setting exercises and were well-versed in qualitative methods, group facilitation and questionnaire design. The process consisted of four main phases: (1) stakeholder engagement (consumers, clinicians, researchers), (2) rating health research topics, (3) focus group interviews, and (4) establishing ‘top ten’ priority questions for future research in child and youth health.
The multi-methods study (questionnaires and focus group interviews) was conducted online (due to the SARS-CoV-2 pandemic and government mandated restrictions for in-person activities) in Alberta, Canada between March and June 2020 and is reported using the Reporting Guideline for Priority Setting of Health Research, where applicable (Tong et al., 2019).
Setting and population
A convenience sample of parents and youth were approached using a snowball sampling method (Berg, 2004), and utilizing a previously developed vast child health stakeholder network and organizational social media accounts.
Parents or legal guardians (>18 years) of a child (< 18 years) and youth (15 to <25 years, as defined by the United Nations) residing in the province of Alberta who could read and speak English, and had access to a computer, tablet or electronic device were eligible and invited to participate. Adults who did not have a child or youth under their care were ineligible to participate.
Ethical approval
The study received ethical approval from the University of Alberta Health Research Ethics Board (PRO 00088366) on March 21, 2019 and was conducted according to the Helsinki Declaration. All participants provided informed consent prior to data collection.
Approach
Phase 1 stakeholder engagement
Throughout the process, local parent and youth advisory groups were engaged, who acted as collaborators on all phases of the priority setting exercise, and provided vital input into the design, execution, and dissemination of the study (Hartling et al., 2021). Two youth advisory groups, the Stollery Children’s Hospital Youth Advisory Council (YAC) (n = 23) and the Alberta Children’s Hospital Child and Youth Advisory Council (CAYAC) (n = 25) were engaged as research partners. These groups are from the only two children’s hospitals in the province, and provide care for children across the province.
The objective of Phase 1 was to receive input on project design and generate an extensive list of health research topics for prioritization. The original list incorporated priority topics identified by Alberta Health and Alberta Health Services’ Maternal Newborn Child and Youth Strategic Clinical Network, representative of the main health authority for the province, as well as input from clinical colleagues.
A refined list for parents was then established after consultation with a parent advisory group (topic names were finalised, and two new categories were added). During consultations with the Stollery Children’s Hospital YAC and Alberta Children’s Hospital CAYAC, the topic list was further modified using terminology suitable for a youth audience, and examples were added for each topic (Supplementary Material 1).
Through consultation and pilot user testing with members of the parent and youth advisory groups, two online questionnaires were co-designed (format and delivery) with parents and youth, then programmed by Nooro Inc (Ontario, Canada). Advertisements for the project containing a link to the online questionnaires were then circulated via social media (Twitter and Facebook), and through local and provincial health networks, child care groups, youth community groups and community recreational centres.
Phase 2 rating child health research topics
The anonymous online questionnaires (available upon request) collected participant demographics (e.g. age, gender, ethnicity, geographic region) and asked parents and youth to rate the topics as either ‘high’, ‘medium’ or ‘low’ priority. Along with rating the pre-existing topic areas, an open response section allowed participants to write any additional health topics that were not included in the questionnaire.
At the end of the questionnaire, participants were invited to leave their contact details (separate from questionnaire submission) if they were interested in attending a focus group interview to discuss the highest-ranking topics. All participants were then entered (upon consent) into a draw to win an Apple iPad. The draw was governed by and construed, and enforced in accordance with the laws of the Province of Alberta and federal laws of Canada.
Phase 3 focus group interviews
Online focus group interviews using video conferencing software (Zoom Video Communications Inc. 2016, Version 3.6.5) were conducted with parents and youth, separately. Semi-structured interview guides were created with and piloted among youth and parent volunteers. Deliberative dialogue (Boyko et al., 2012) was used to facilitate discussions around the highly rated research topics, and to understand what specific aspects of those topics were most important and why (understanding information needs).
At the end of each focus group, participants were emailed a $10 Canadian dollars (CAD) electronic gift card to thank them for their time.
Phase 4 establishing parent and youth ‘top ten’ research questions
A second questionnaire (available upon request) containing research questions related to the parent and youth priority topics, were then sent to all parents and youth who completed questionnaire 1. Parents and youth were asked to rate the priority research questions on a 5-point Likert scale from 1 to 5; with 1 = not at all important, 2 = low importance, 3 = neutral, 4 = important, to 5 = very important. Participants were also asked to select their top two most important health research questions. Participants who completed the second questionnaire were emailed a $10 CAD electronic gift card to thank them for their time.
Analysis
Questionnaire data were downloaded and managed in Microsoft Excel 2016 (Microsoft Corporation). Descriptive statistics (means and standard deviations, as well as frequency counts) were calculated for parents and youth who responded to the online questionnaires.
Ratings and frequency counts were used to rank research topics and priority questions in Phase 2. All topics rated ‘high’ by ≥70% of respondents from Questionnaire 1 were retained for discussion in Phase 3. In Phase 4 (Questionnaire 2), the scores for all participants were merged illustrating which research questions were deemed most important (a score of 5) by the participants. Final rankings were determined by frequency counts related to questions selected by participants as their ‘top 2’ research questions.
Focus group interview discussions were audio recorded via Zoom, downloaded and transcribed verbatim by a third-party transcriptionist (Vanin Services) and analyzed using thematic analysis (Braun and Clarke, 2022). Resultant themes and subthemes were then used to produce representative research questions (Supplementary Material 2) for ranking. These were developed in consultation with members from the parent and youth advisory groups.
Focus group data collection and analysis occurred concurrently. Data management and analysis were facilitated using NVivo 12 Software (v.12, 2018 QSR International PTY Ltd). The analysis process was iterative, where each transcript was read through in its entirety, verbatim codes were assigned to topics in the transcript and codes were grouped into preliminary categories. These preliminary categories from all coded transcripts were compared and organized into themes. The common themes were reviewed and verified by all authors to promote analytic rigour and trustworthiness (Lincoln and Guba, 1986). Trustworthiness of the data was guided by four criteria: credibility (obtaining a broad sample), confirmability (maintaining a comprehensive audit trail, field notes, memos and interview tapes), dependability (keeping a detailed audit trail documenting decisions made throughout the research process) and transferability (while transferability is determined by the reader, the team developed thick descriptions of the parents’ and youth experiences and information needs related to priority topics to facilitate transferability) (Campbell et al., 2019). Facilitators wrote field notes during focus group interviews and regularly debriefed at the end of each focus group and throughout analysis to promote confirmability, reflexive practice, and rigorous research process (Johnson et al., 2020; Olmos-Vega et al., 2022; Rettke et al., 2018).
Results
Participant demographic characteristics.
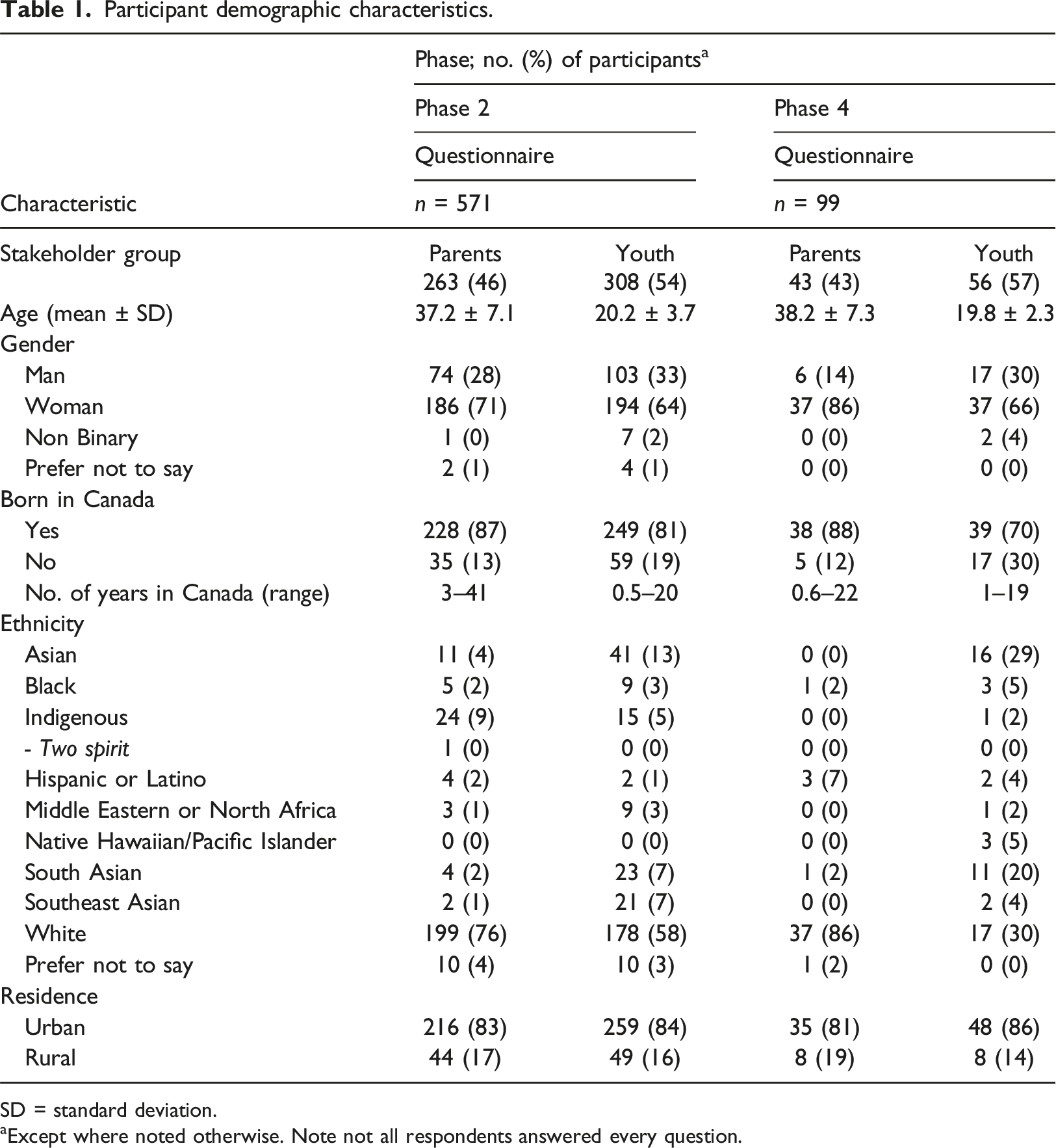
SD = standard deviation.
aExcept where noted otherwise. Note not all respondents answered every question.
In Phase 2, 571 (92%) participants completed the online questionnaire. 263 (46%) parents and 308 (54%) youth voted on 27 health topic areas. Parents rated five topic areas as a high priority (behaviour, learning and developmental disorders; mental health; food, environment and lifestyle; quality of health care; and vaccines). Youth rated four topic areas (brain and nerve health; mental health; quality of health care; and vaccines) as high priority. Additional topics listed by parents and youth included: poverty, sexual health, child health promotion, immune system health, preventative medicine, and health care system use.
In Phase 3, four focus groups with 12 (5%) parents generated themes and subthemes further describing their priorities and information needs highlighted in Phase 2. Although the interview guide was informed by prevalent topic areas from Phase 2, the semi-structured nature of the interview session allowed for creation of descriptive themes through an inductive process (Supplementary Material 2). Parents discussed how accessibility and continuity of care contributed to high quality of health care (especially around the need for supportive services and resources for behaviour, learning, and development), while emphasizing the importance of self-advocacy and credible information for making informed healthcare decisions. Parents described needing more information on teaching their children about the health effects of excessive screen time, nutrition, physical activity and climate change to improve their knowledge on environment and lifestyle. Notably, mental health was discussed in detail, as parents wanted to know the signs and symptoms of mental health conditions in their children, how to effectively foster self-confidence in their child, processes of seeking treatment for behavioural and mental health diagnoses and the impacts of parental mental health on their child’s mental health. In terms of vaccinations, parents discussed their struggles with keeping track of upcoming scheduled vaccines for their children, and wanted resources around how best to talk to children about vaccinations. From these findings, 24 research questions were generated (Supplementary Material 3). Lastly, parents expressed concern over the availability of health resources during to the Coronavirus disease 2019 (COVID-19) pandemic.
During six focus groups, 21 (7%) youth discussed their health information needs and priorities. Youth discussed their need for information about addictions, anxiety and depression, personality disorders, self-harm, stigma, and potential treatments for mental health concerns. Access to quality healthcare with accessible resources and navigating wait times was discussed, as well as the necessity to advocate for their health care preferences and patient satisfaction/quality of care. An additional topic previously described in Phase 2 was sexual health, which encompassed conversation points around trusting relationships, education, and sexual abuse. From these findings, 20 research questions related to their priority areas were developed (Supplementary Material 3). Interestingly, all youth focus groups discussed their concerns for helping their peers with mental health. Similar to the parent focus groups, COVID-19 was a topic of interest, where youth expressed concern about schooling disruptions, potential lack of socialization, accessing supports, and finding credible sources of information regarding the pandemic.
In Phase 4, 99 respondents (43 [43%] parents; 56 [56%] youth) completed the second questionnaire. Parents’ highest ranked question was ‘What is the effect of screen time on cognition and neurodevelopment for children and adolescents?’, while the highest ranked question from youth was ‘What are the early signs of anxiety and depression and when should an individual seek help?’. The final top 10 lists for parent and youth priorities are presented in Box 1 and 2, respectively.
What is the effect of screen time on cognition and neurodevelopment for children and adolescents? How does parental mental health impact a child’s mental health and behaviour? How can parents engage in and facilitate conversations with their children about self-confidence, self-efficacy and emotional regulation? What resources are available for parents and schools to recognize early signs and symptoms of behaviour disorders (e.g. attention deficit/hyperactivity disorder, oppositional defiant disorder, conduct disorder)? What resources are available to parents seeking assessment for and management of children with behaviour, learning and developmental disorders? What resources are available to parents to identify and manage anxiety in their child? How can a parent best advocate for their child's health care, ask questions, voice preferences, foster shared decision-making and engage healthcare provider in these conversations? What system-level changes can be made to reduce wait times for primary, emergency, and specialist care? How can support services for childhood and adolescent behaviour, learning, and developmental disorders be standardized and equally funded across the province? What resources are available to track vaccinations and remind individuals of upcoming vaccinations?
What are the early signs of anxiety and depression and when should an individual seek help? What are the effects of cannabis use among young people on long-term mental and physical health? What system-level changes can be made to reduce wait times for primary, emergency and specialist care? What role can peers take to recognize and support friends struggling with mental health issues? What does a young person need to know in order to advocate for one’s own health care? What are youth’s experiences and information needs regarding sexual health education? What educational resources are available to youth regarding what to do when someone has a seizure? What are the barriers to seeking care for youth (e.g. privacy concerns when parents attend appointments, access, familiarity with the system, cost)? What is the impact of social media use on anxiety levels in youth and when does social media use become unhealthy? How can the stigma of discussing mental health issues be reduced in youth?Top 10 parent priorities for child health research in Alberta, in order of importance
Top 10 youth priorities for child health research in Alberta, in order of importance
Dissemination and topic scoping
These findings were broadly disseminated using infographics (Supplementary Material 4) co-created with parents and youth via social media, as well as through online conference presentations, and direct contact with stakeholders via email (provincial health authority, women and children’s health research groups, funding agencies). All interested participants received the results in a summary email (including infographics) at the conclusion of the study.
To understand what research has already been conducted and what is currently known about the priority topics (whether the research question or topic had already been answered), two reviews were undertaken. The first was a scoping review which mapped the existing literature around the cognitive and neurological impacts of excessive screen time for children and youth, as well as identifying parent information needs (Wright et al., 2022). The second, a systematic environmental scan, set out to understand what information is currently available online for youth about the signs and symptoms of anxiety, what resources are available for self-assessment, and what are youth’s behaviours, experiences and information needs around seeking care for anxiety (Pohl et al., 2022).
Discussion
Utilizing the knowledge and experience of Albertan parents and youth, relevant lists of priority health topics were developed. Parents rated five topics (behaviour, learning, and developmental disorders; mental health; food, environment and lifestyle; quality of health care; and vaccines) and youth rated four topics (brain and nerve health; mental health; quality of health care; and vaccines) as a high priority. The corresponding priority research question lists (Box 1 and 2) highlight areas where funding, research, and knowledge mobilization efforts should be directed to improve child health outcomes that are important to parents and youth across Alberta, Canada.
Engaging parents and youth
Traditionally, deciding what health research topics should be explored has been done by researchers and clinicians, whose priorities often differ from those of consumers (patients, parents, and caregivers) (Tallon et al., 2000). There is now increasing awareness of the role consumers play in shaping research agendas (Pittens et al., 2014), and advocacy for including the perspectives of parents and youth (adolescents and young adults) in child health research (Postma et al., 2022). Previous paediatric priority setting studies have often used a JLA approach to either involve children in the identification of research questions, prioritization of research questions, or in the prioritization workshop (Odgers et al., 2018; Jongsma et al., 2020). While the most suitable method regarding involvement of parents and youth in priority setting exercises is unclear, parents and youth were engaged throughout the design, development, and dissemination of findings based on the principles of integrated knowledge translation (Kothari et al., 2017).
As stated by Postma et al., publishing a research agenda should be a tool and not a stand-alone goal of the research priority setting process (Postma et al., 2022). Engagement with local parent and youth advisory groups throughout the priority setting exercise, coupled with experiential knowledge mobilization efforts has supported the dissemination of findings during the post-prioritization phase. However, further evaluation on the uptake of the research agendas (priority questions) by relevant funding organizations is needed, as the impact on research funding and practice is currently unknown.
Priority topics
A recent systematic review identifying paediatric research priorities highlighted that while the majority of studies were focussed on specific childhood conditions, there was overlapping priorities identified (Modanloo et al., 2023). For example, improving access to health care services, early diagnosis, improving mental health care services and improving communication with health care providers, were identified across studies, and are reflective of current findings.
Similar to other recent priority setting exercises across Canada (Bialy et al., 2018; Brockway et al., 2021; Eaton A, 2022; Lavigne et al., 2017), the topic of mental health was found to be a general concern for both parents and youth. A number of top 10 priority topics centred around mental health, a finding shared by Eaton et al. (Eaton, 2022) and Brockway et al. (Brockway et al., 2021), who reported topics related to stress, emotional, and mental health as consistently a top concern for families and health care providers. These results provide more details within the broad topic of mental health, including specific conditions of interest as well issues around access to care, quality of care, and finding credible and supportive information and resources, the focus of which may be different to what clinicians or researchers might typically focus on.
With a rise in the prevalence of diagnosed mood and anxiety disorders in youth across Canada, it is no surprise to see mental health ranked as a priority topic. Current research agendas across Canada are working to fill this gap and have prioritized funding research in this area to respond to the rising demand for mental health services among youth (Wiens et al., 2020). Many parent priorities were centred around the need for resources to help them navigate health care management decisions. While topics such as ‘impact of screen time on neurodevelopment’ and ‘identifying and managing anxiety in children’ have been widely studied, findings highlight the need for knowledge mobilization resources to support parents in identifying and managing these health issues.
For both parents and youth, access to care in a safe and timely manner was important. A central tenet related to advocating for one’s healthcare preferences, and engaging with healthcare providers in conversations to foster shared decision-making. Shared decision-making is a widely studied and important part of implementing youth- and family-centred care (Boland et al., 2019); however, little is known how best to support this from a consumer’s perspective. Focussing on how to deliver care or resources to support self-management or information on when and what types of care to seek (Bombard et al., 2018; Nicholson et al., 2020b) may be needed.
The similarity or shared focus between consumers (the ones making the decision to seek care) and health service researchers is an important area to advance and engage consumers in, to support the implementation of shared decision-making in child health. To date, very little research has been done to understand parents’ and families’ priorities related to child health research (Modanloo et al.); yet, studies have highlighted a mismatch between parent and youth needs compared to clinicians and researchers. One recently published study conducted in Toronto, Ontario by Lavigne et al., (Lavigne et al., 2017) used a JLA partnership to identify the unanswered research questions in paediatric preventative care that are most important to parents of young children (0–5 years) and clinicians. They also reported on how the questions deemed important to parents differed from those of clinicians. Priority questions identified by parents were more focused on screen time, media exposure and environmental toxins, which differed from priorities put forth by clinicians. Parents also identified two topics that were not addressed by the US Preventative Services Task Force for child and adolescent preventative care, and two topics from the Task Force were not identified as priorities by parents (Lavigne et al., 2017). This highlights, once again, the difference between consumer priorities and those set by researchers and funding agencies who drive research agendas. Similarly, a study investigating health care preferences of adolescents with chronic illnesses found that similar to adults, participants rated aspects of interpersonal care (especially honesty, attention to pain, and items related to respect) as most important (Britto et al., 2004). They noted pain was a frequent topic discussed, and commented that regard for pain had not been a high ranking item in most surveys of adults, and was not even included as an item in many surveys (Britto et al., 2004). This draws attention to the need to engage with youth regarding these topics, and not assume their preferences are mirrored by adults. There is a growing field of patient engagement set to explore how best to involve youth in health related research, in a meaningful and ethical manner.
Pandemic implications
While not a focus of this priority setting exercise, it would be remiss not to acknowledge concerns raised by parents and youth related to the pandemic. Similar to what has been expressed by parents elsewhere (Nicholson et al., 2020a; Watson et al., 2021), the availability and accessibility of health care resources was a main concern. For youth, academic disruptions and concerns around lack of socialization were raised, which is consistent with findings from studies assessing the role of the pandemic in changes in emotional, social, and academic adjustment during adolescence (Branje and Morris, 2021). It was not surprising that youth discussed difficulty in finding credible sources of information regarding the pandemic. The ‘infodemic’ (Eysenbach, 2002) (used by the World Health Organization to describe the overabundance of information, including misinformation during the pandemic) resulted in many being confronted with conflicting information resulting in a high level of uncertainty. Resources have since been developed to support digital health literacy in youth, and reduce the spread of misinformation.
While this study unintentionally took place during the pandemic, the topics prioritized are relevant outside of the pandemic. Perhaps topics such as mental health and screen time were made more apparent or exacerbated as a result of public health safety measures (e.g. school closures, lockdowns, social distancing), but will likely remain priorities beyond the pandemic (Latoo et al., 2021).
Limitations
The findings from this study should be considered in context of its limitations. The majority of participants identified as white and well-educated from urban centres across the province of Alberta in Canada, and the priority topics may not be reflective of those from rural or diverse ethnic or cultural backgrounds. Due to the pandemic, methods used deviated from traditional JLA priority setting processes, and excluded those unable to participate online. However, using a co-designed approach with parents and youth ensured the recruitment strategy, questionnaire format and delivery were relevant to the target audience. Partnerships with local parent and youth advisory groups supported meaningful participation and ensured their voices were represented throughout the research process.
Implications for practice
Involving patients and families in setting research priorities is part of the growing emphasis on consumer-oriented health care. This is particularly important in paediatric research as youth are an under studied and vulnerable population. It is envisaged that the research priorities identified through this study will guide investigators and funding bodies in the development, planning, and funding of research as well as knowledge mobilization efforts, to improve care and outcomes for youth in Alberta.
Scoping the evidence around the identified topics to examine the extent, range, and nature of research activity in a topic area can identify research gaps in the existing literature (Pham et al., 2014). Identifying the key gaps where little or no evidence is available can be a useful tool for developing a strategic approach to building the evidence base and setting research priorities in a particular sector. Conversely, identifying where strong evidence exists can inform where effective knowledge mobilization strategies for parents and youth should be developed. By bringing these topics to the attention of funding agencies and researchers, studies which cater to the needs of patients and families can be designed and implemented.
Conclusion
Utilising the knowledge and experience of Albertan parents and youth, relevant lists of priority topics in child health research were developed. These lists highlight the areas where funding and research should be directed to improve child health outcomes and patient care experiences that are important to parents and youth. Parents’ highest ranked research topic was related to the effect of screen time on children’s neurodevelopment, while the highest ranked topic from youth was regarding early signs of anxiety and depression. Further research exploring whether a gap in the current evidence base related to these topics exits, or whether knowledge mobilization efforts are needed to communicate research findings and support parents and youth in these priority areas is warranted.
Supplemental Material
Supplemental Material - Establishing priorities in child health: Giving parents and youth a voice
Supplemental Material for Transitioning from paediatric to adult healthcare: Establishing priorities in child health: Giving parents and youth a voice by Sarah A Elliott, Shannon D Scott, Kelsey S Wright and Lisa Hartling in Journal of Child Health Care
Footnotes
Acknowledgements
We would like to thank our clinical experts and members of the Alberta Health Services’ Maternal Newborn Child and Youth Strategic Clinical Network for their input developing the original list of child health topics. We are thankful for the input and participation from our Pediatric Parent Advisory Group, as well as members from the Alberta Children’s Hospital Child and Youth Advisory Council and the Stollery Children’s Hospital Youth Advisory Council. Most importantly we thank the parents and youth who participated in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the generosity of the Stollery Children’s Hospital Foundation and the Alberta Women’s Health Foundation through the Women and Children’s Health Research Institute Innovation Grant (2550) awarded to Dr. Scott. The funder played no role in the study design, collection, analysis, and interpretation of data, writing of the report or decision to submit the manuscript for publication. Dr. Scott is supported by a Canada Research Chair in Knowledge Translation in Child Health. Dr. Hartling is supported by a Canada Research Chair in Knowledge Synthesis and Translation. Dr. Hartling and Dr. Scott are Distinguished Researchers with the Stollery Science Lab supported by the Stollery Children’s Hospital Foundation. The other authors received no external funding.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.