
Abstract
Complex paediatric health conditions are increasingly associated with survival into adulthood resulting in more youth with complex care needs (CCN) transitioning from paediatric to adult healthcare. Current transition practices, when present, are disorganized, resulting in health status deterioration and complications due to unmet needs. The aim of this qualitative descriptive study is to develop a broader understanding of the current transition practices and experiences, as well as recommendations of care providers who support youth with CCN in the transition from paediatric to adult healthcare. Fifteen care providers from two Eastern Canadian provinces were interviewed using a semi-structured interview guide. The data collected were analyzed using inductive thematic analysis following the six phases outlined by Braun and Clarke (2006). The findings from this research demonstrate (1) a shortage of care providers, (2) inconsistent timing for transition initiation, and (3) lack of available community resources and services. Participant recommendations include (1) a designated transition coordinator; (2) transition policy implementation; (3) improved collaboration between and across care teams; and (4) the integration of virtual care to facilitate the transition process. The results of this study can potentially improve transition practices and policies and guide future research in this area.
Background
Youth with complex care needs (CCN) require significant health, educational, and/or social assistance beyond what is generally required by their peers (Canadian Association of Pediatric Health Centres [CAPHC], 2016). These youth, accounting for approximately 20% of children and youth in North America, experience complex chronic conditions (e.g., cystic fibrosis and cerebral palsy) that were once significantly life-limiting and are now surviving well into adulthood (Doucet e al., 2022, Peter et al., 2009, Scal and Blum, 2002, Young et al., 2018). As a result, more youth with CCN are transitioning from family-centered paediatric healthcare to individual-focused adult healthcare (Bolger et al., 2017). Healthcare transitions are often defined as planned, orderly, and purposeful processes of change from child- to adult-oriented models of healthcare, which is demonstrated to be a particularly difficult process for youth with CCN (Blum et al., 1993; Hart et al., 2017; Spaic et al., 2019).
When transferring to adult healthcare, current transition practices have been reported as disorganized and disjointed, resulting in health status deterioration and an increase in morbidity and mortality due to unmet health service needs for youth with CCN (Berens and Peacock, 2015, Burke et al., 2008, Doucet et al., 2022, Han et al., 2018, Peter et al., 2009, Reiss et al., 2005, Toulany et al., 2019). Consequences of poor transition include (1) an increase in emergency service utilization; (2) negative healthcare provider and patient experiences; and (3) poor access and fragmentation to care (Doucet et al., 2022). This has led instead to an aging-out phenomenon, where youth are discharged from care once they reach the upper age limit of the paediatric practice, rather than an integrated transition process to adult healthcare services (Burke et al., 2008).
Although transition practice has been a topic of interest for many years, few studies have looked directly at the transition practices and experiences of participants (e.g., patients, family members, and healthcare providers) outside of existing transition programs (Hart et al., 2017, Schraeder et al., 2021). Instead, a great number of studies focus on the structural factors of transition programs, such as how established or pilot programs are planned and implemented (Ciccarelli et al., 2015, Spaic et al., 2013, Telfair et al., 2004). Additionally, studies indicate that further exploration of the experiences and practices of healthcare providers is necessary (Bolger et al., 2017).
Aim
The focus of this study is on healthcare provider practices and experiences, as well as recommendations for future practice, as they support youth with CCN during the transition from paediatric to adult healthcare. To address these areas of focus, two research questions were posed: (1) What are the current practices and experiences of healthcare providers (primary care providers [PCPs], specialists, and subspecialists) who participate in the care of youth transitioning from paediatric to adult healthcare and (2) What are the recommendations of healthcare providers (PCPs, specialists, and subspecialists) to improve transition practices from paediatric to adult healthcare?
Methods
Design
This exploratory study used a qualitative descriptive design to understand the current practices, experiences, and recommendations of care providers in the support of youth with CCN as they transition from paediatric to adult healthcare. This descriptive design supports the study’s purpose as its intent is to stay close to the data generated from participants without significant interpretation and provide a straightforward comprehensive summary of experiences (LoBiondo-Weed et al., 2018). This study was conducted as part of a masters dissertation (Splane, 2021).
Ethical considerations
This study was reviewed and received ethics approval prior to commencement through the University of New Brunswick (REB#008-2020), Horizon Health Network (REB#100617), and Vitalité Health Network (REB#100864). Written or verbal consent from participants was obtained prior to participation in the study. Moreover, participants were given the right to withdraw from the study any time. Pseudonyms are used for participant quotes.
Population
The population of interest for this study included care providers in two Eastern Canadian provinces (New Brunswick [NB] and Nova Scotia [NS]) involved in supporting youth transitioning from paediatric to adult healthcare. Eligible participants included PCPs (physicians and nurse practitioners), paediatricians, paediatric subspecialists (physicians), and adult specialists (physicians) who are involved or have been involved in the transition process of youth between the ages of 14 and 30 from paediatric to adult healthcare. Subspecialists for this study included paediatricians trained and certified in a board-certifiable subspecialty (Canadian Medical Society, 2018).
Purposeful sampling was used to select participants. Specifically, maximum variation sampling was used to ensure representation across different practice areas (e.g., oncology and endocrinology), practice settings, and locations (Suri, 2011). Participants were identified through provincial organizations that provide health services to children and youth and were recruited through email using an ethics approved standard advertisement explaining the purpose and expectations of the study.
Data collection
To understand the transition process from the perspectives of healthcare providers supporting youth with CCN, this study explored two areas of focus: (1) current practices and experiences and (2) practice recommendations. Data were collected using semi-structured interviews, which serve to ensure participant-driven data in qualitative descriptive studies (Kim et al., 2017). A supplemental table is available online that outlines the interview guide and was piloted prior to study commencement. Interviews were conducted by an experienced nurse practitioner researcher (JS), and participants were probed for depth and clarification as needed to fully capture their experiences using motivational interviewing techniques (Miller and Rollnick, 2002). Participants had the option to be interviewed in either English or French and either by phone or over videoconference in keeping with coronavirus disease 2019 (COVID-19) public health protocols and restrictions. Methods proposed by Lincoln and Guba (1985) were used to address the four pillars of trustworthiness: credibility, transferability, dependability, and confirmability. To help ensure credibility of the findings, a summary of the study findings was presented to participants with an optional follow-up interview to clarify details. All data were stored on a secure, password-protected drive.
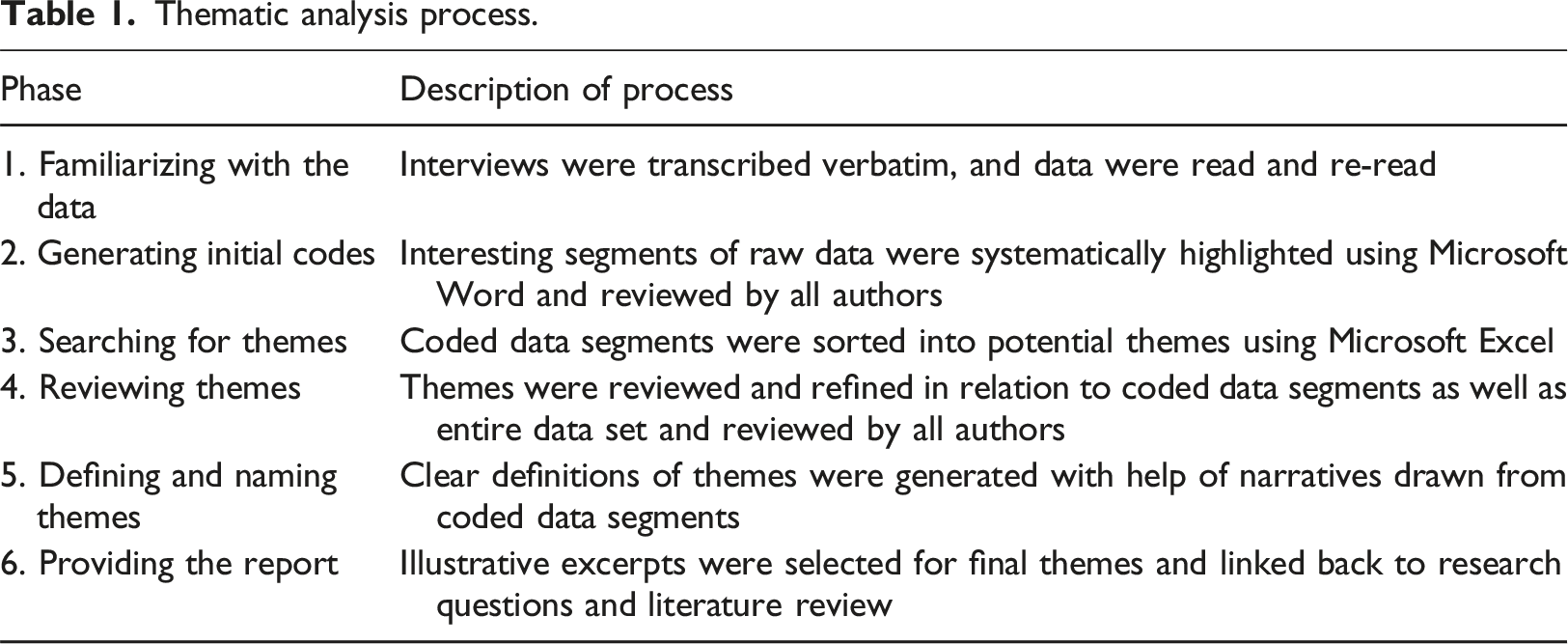
Data analysis
Thematic analysis process.
Findings
Participant characteristics.
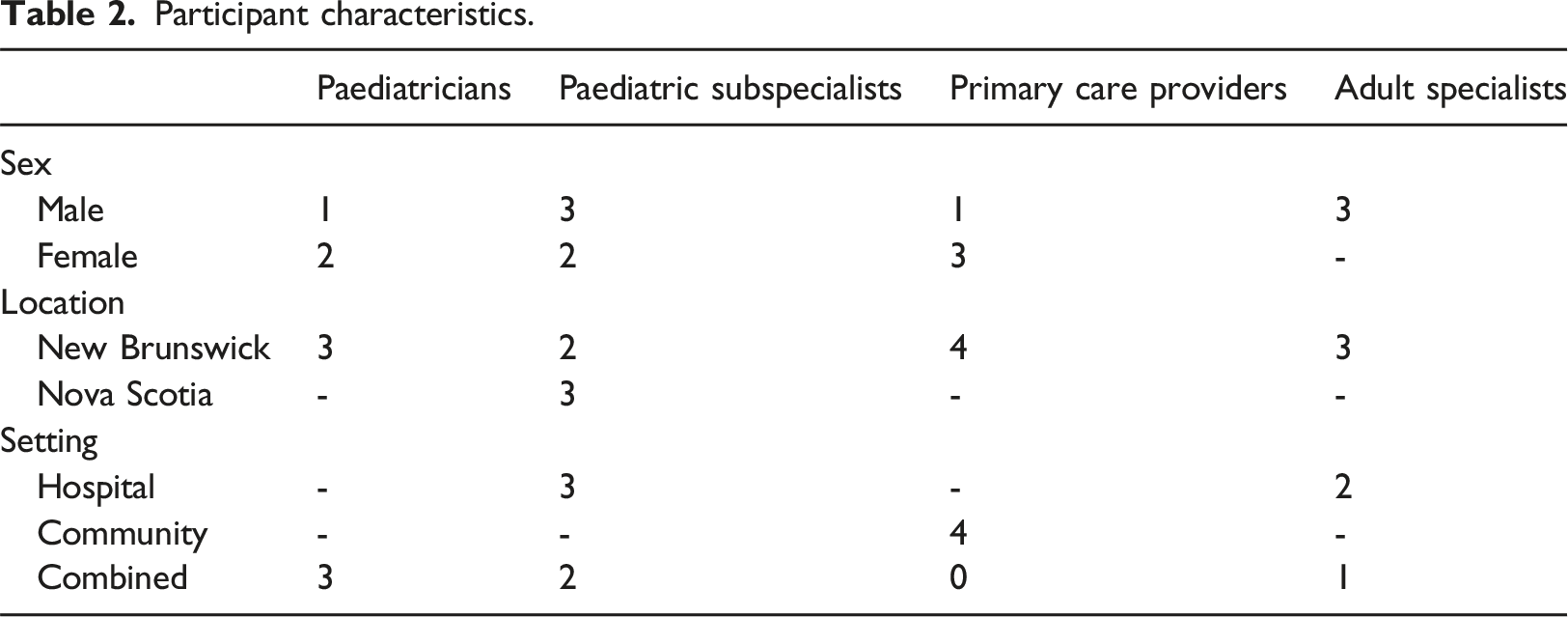
Care team composition was variable among the participants. Less than half of the participants indicated that they worked in a multidisciplinary setting, with the team members ranging from one to several members from various disciplines. Conversely, most participants worked independently when transitioning youth to adult healthcare services.
Study themes.
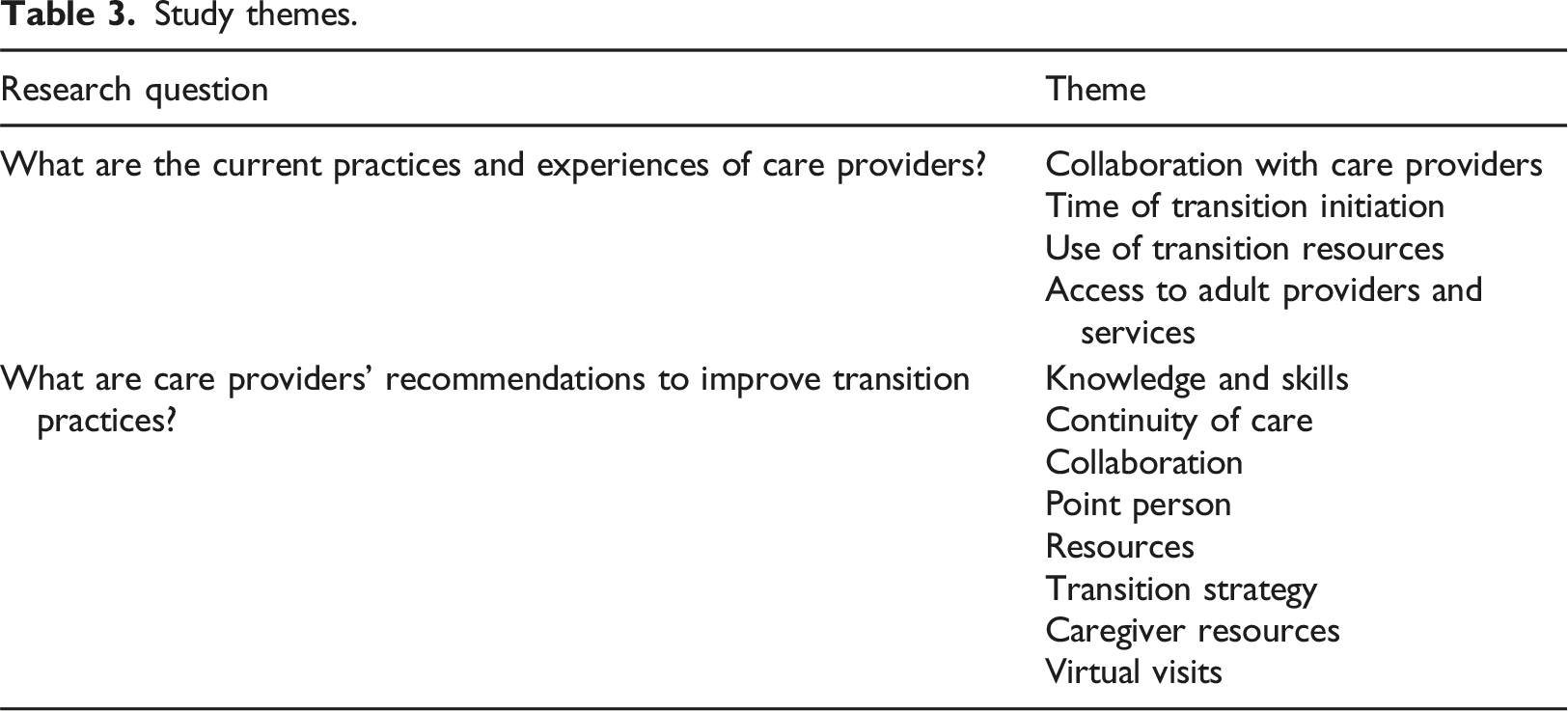
What are the current practices and experiences of care providers?
The first area of focus for this study was the current practices and experiences of care providers who support youth with CCN in the transition from paediatric to adult healthcare. Four themes were identified, including collaboration with care providers; time of transition initiation; use of transition resources; and access to adult providers and services.
Collaboration with care providers
This theme captures the experiences of participants in communicating and collaborating with stakeholders within or outside of their practice setting in the care and/or support of youth transitioning from paediatric to adult healthcare. Overall, participants reported that communication and collaboration with other care providers has been a positive experience, with one participant confirming, “I find it’s been positive so far for me” (John). Most of the communication and collaboration between care providers during the transition process is through written documentation. Additionally, participants also highlighted that dedication to thorough communication is an essential component to good collaboration when supporting the transfer of youth to adult healthcare: I think you just have to … be aware that you have to spend more effort. I don’t think anyone is less willing to communicate information or hand off transition care. I think you just have to be aware there’s more efforts required at that time. (Mary)
Being part of a multidisciplinary care team was a positive practice environment for many care providers with that opportunity. The importance and process of a comprehensive team approach when caring for youth with complex care needs as they transition from paediatric to adult healthcare was highlighted by one participant: I work in a fairly large interprofessional team, and various team members may take on different roles around transition. So typically, we have physiotherapy, occupational therapy, social work, nursing, dietitian, psychologists. And I think everybody takes on a bit of a role. It depends … on what the client and family’s goals are at the time, who happens to be working with the patients more directly. So, it can be anyone; social work and nursing team members do take on a bulk of … working on some of the specific issues related to life transition between adolescents and adulthood. But I’d say that everybody really takes that shared responsibility. (Heather)
Time of transition initiation
The second theme captures the age or life event when the participating clinicians begin to support their patients in the transition process and subsequently transfer youth from paediatric healthcare or receive youth into adult healthcare. The timing of transition initiation was variable among the participants ranging from “a month or two” (Eric) to several years before the actual transfer of care. Most paediatric-focused participants indicated that they see patients until 18 or 19 years of age, or until high school graduation. In keeping with this, adult-focused care provider participants indicated that they begin to see youth at age 18 in their practice.
Given the inconsistent age of transitioning youth to adult healthcare, a specific challenge that participants face is making the decision of when to begin the transition process: Do you wait until they’re close to it, because maybe then they won’t forget? But then they’re not prepared. Right? (Robert)
It was found that the end of some paediatric services does not align with the beginning of adult services, which is “problematic and led to some disjointed care” (Lisa). One participant captured this theme succinctly by trying to define the age at which they accept youth into adult care: So we will take them so around [pause], and that’s even just as simple as defining what is it, paediatric patient, versus what is not. So, is it 16? Is it 18, is it 19? Nobody seems to get along in terms of what should be the definition? (Eric)
Use of transition resources
The third theme captures the tools and resources used by participants to support and/or facilitate the transition from paediatric to adult healthcare. Additionally, this theme captured the participants’ awareness of tools, resources, programs, and/or policies available to support or facilitate transition. Participants shared that they seldom used tools or resources in their transition practice indicating “we don’t have any tools here” (Lisa) and “we just use our team” (Cathy).
It was noted that there are a few specialized local programs for youth who have specific diagnoses that assist youth in the transition from paediatric to adult healthcare. Otherwise, participants indicated that they “have not tapped into any community resources” (Michael) and “don’t know what’s there” (Robert) to support the transition process.
Access to adult providers and services
Participants often struggled during the transition process to identify and access adult providers and services for their transitioning youth either due to lack of resources or long waitlists. A challenge for both care providers and patients is the change in service delivery method when patients transition from paediatric to adult healthcare where: The supports that they may have had in, in childhood, which may or may not be sufficient, some of those don’t always roll over, or it’s very difficult to roll those over once somebody is an adult. (Rebecca)
For example, patients are often leaving a multidisciplinary approach to care and entering adult healthcare services that do not have the same resources. One participant captured this phenomenon with their experience: I can send them to a physician … I can usually find a physician to send them to. But then if let’s say, for example a bronchiectasis patient, I can send them to the physician, and I have a physiotherapist who sees them here. But then we find out that the physician I’m sending them to doesn’t have a regular physiotherapist to work with them. You see? So then, then we’re [stuck]. (Cathy)
When services and resources were identified in adult care, they were described as piecemeal and disjointed. Additionally, maintaining a current working knowledge of adult services and resources available for their patients tends to be a challenge as “it is ever changing” (Robert). When adult services and resources are available, participants identified that they may “have a two-year waitlist, then it’s hard to even start the conversation about transition” (Taylor).
Another challenge in accessing adult healthcare services as described by participants is the availability of services in a particular location. One participant indicated that their “biggest barrier is not having a certain [adult] specialty if needed” (Jack) in their region. For many patients from rural communities, travel is required to access available adult services leading to a sequence of challenges, such as financial barriers with patients finding it “difficult to absorb all those costs of traveling” (Daniel), and language barriers for Francophone patients travelling to predominantly English-speaking centers.
What are care providers’ recommendations to improve transition practice?
The second area of focus for this study was the recommendations from participants for future transition practice in supporting youth with CCN as they move from paediatric to adult healthcare. The three themes identified in this area include knowledge and skills; continuity of care; and resources.
Knowledge and skills
The first theme captures the knowledge and skills participants recommended care providers should possess when supporting youth transitioning to adult healthcare. Participants identified that understanding the differences between paediatric and adult healthcare delivery is important for care providers to support youth in their transition. So, for example, that on the adult side, by and large patients are expected to come by themselves and to be able in very short order to give the history of what’s happened since they were last seen. (Emma)
As identified earlier, resources in the adult healthcare system may be limited and lead to barriers in transition for youth. Some participants noted the importance of care providers having knowledge and familiarity with these limitations to help mitigate barriers and manage patient expectations. One participant highlighted that: Sometimes we get hung up on changing or fixing the adult healthcare system when there’s a lot of work that I think we can do as paediatric or childhood providers in setting kids and families up for success as they transition through adolescence to adulthood. (Rebecca)
Such suggestions included coaching and empowerment to aid youth in becoming effective advocates and navigators of the adult healthcare system.
Continuity of care
The importance of continuous care from paediatric to adult healthcare was emphasized by several participants. Two subthemes emerged from the accounts of participants in this study: collaboration and point person.
Collaboration
Recommendations to enhance transition practice included improved collaboration between providers and across teams who are invested in the care of youth to improve continuity of care. One participant stated: I think in an ideal world we’d have a greater opportunity to collaborate, provide capacity building to our primary care colleagues throughout the child’s journey. (John)
This is in keeping with findings that, due to the substantial amount of primary care general paediatricians provide, youth with CCN enter adult care without a PCP. This results in adult specialists being required to seek out a PCP for young adults who have recently transitioned into their care.
Additionally, improved collaboration includes “good documentation [and] good communication” (Taylor) with care providers who are “open to communication for quite some time to ensure that there’s any questions and things don’t get missed” (Jack).
A suggestion by one participant to facilitate collaboration included a directory of adult providers with whom they can collaborate. Participants also recommended a period of combined practice between paediatric and adult healthcare providers with an “overlap period between the care, between the transition from paediatrics to adult [care]” (Mary). This would allow an opportunity to bridge the transition gap for youth who are trepidatious of leaving the comfort of paediatric practice and entering adult care.
Point person
A recommendation provided by participants is the implementation of “a navigator” (Robert) or coordinator position for the transition of care for youth transitioning from paediatric to adult healthcare. Participants indicated that “having that person holding your chart, ensuring that things are getting done” (John) is a missing component of their current transition practices. A navigator or coordinator was described as someone overseeing all of the “moving pieces” (Sarah) in a transition event or transition program and subsequently “coordinating it, overseeing it, looking at the stats, looking at the data, looking at the feedback system” (Emma) to provide continuity of care and improve transitions. Suggestions for who would fulfill this role included registered nurses, social workers, occupational therapists, and healthcare students. Another participant emphasized the value of this role for patients with their statement: ‘Cause they would meet people where they’re at, right? So, people get, people get bothered because they don’t want to meet new people. And people who have complex illness have enough people in their lives, and so they get weird about it sometimes. But much like I would consult, I don’t know, a dietitian, it doesn’t have to be, you know “This is, you know, this is your transition coordinator. They’re not gonna be in your life forever, but they’re gonna make sure that it’s goes well”. And then, that would be brilliant. (Taylor)
Resources
The final theme for this area of focus captures recommendations by participants for resources, programs, or policies to facilitate the transition of youth with CCN from paediatric to adult healthcare. Although participants perceived it to be unrealistic, they indicated that “in a perfect world, we’d [paediatric and adult healthcare] have the same resources” (Eric) to lessen the contrast between paediatric and adult healthcare services. The subthemes identified include transition strategy, caregiver resources, and virtual healthcare.
Transition strategy
Participants recommended a province-wide strategy focused on the transition from paediatric to adult healthcare. Most participants, however, were unsure as to whether a disease-specific approach or an overarching transition policy would be most beneficial to youth and their families. Many participants emphasized that there is not a “one size fits all” (Jeremy) in terms of transition policy, but that, as one participant stated: Regardless of where in the province we're coming from, I think there needs to be some understanding of how we're transitioning them. So, do we transition them early on? Do we start that gradual transition from 16 to 18 in the preparation phase? Do we have the right people involved? Is there a psychologist involved on that team? (Jack)
Caregiver resources
It was identified that resources for caregivers of youth with CCN transitioning from paediatric to adult healthcare would be beneficial. This may take the form of informing the caregiver on what to expect for their youth in the adult healthcare system. A possible resource, as recommended by one participant, was “a handout maybe for the parents to help them, to share what's expected” (John). Specifically, this may include information “to help them understand the adult versus paediatric approach” (Jeremy). Other resources may assist the caregiver in transitioning away from being the central decision maker in their youth’s healthcare decisions: I’d be nice to have something for the parents. I think to help them. And I don't know what that would be if it would be like counseling or…I'm not sure. But that is a need. To help them to know when to step back. (Robert)
Recommendations were also made for resources to assist caregivers in understanding their new role in their young adult’s healthcare.
Virtual visits
The final recommendation was the use of virtual visits to facilitate transition care. For example, one participant stated: I think there's a lot to be said for virtual care. (Eric)
As a method of healthcare delivery highlighted during the COVID-19 pandemic, participants emphasized that with the use of virtual care appointments, “the gap closes more” (Jeremy).
By utilizing virtual care and e-visit opportunities, patients could benefit from resources that are otherwise unavailable in their region, further mitigating the challenge of location and travel.
Discussion
Findings from this study reveal healthcare provider practices and experiences, as well as recommendations for future practice, as they support youth with CCN during the transition from paediatric to adult healthcare. Beyond their complex care needs, youth are already in a vulnerable period of transition. Youth are not only transitioning from paediatric to adult healthcare, but they are also seeking independence from their parents and exploring education and vocational opportunities (Bhawra et al., 2016, Schraeder et al., 2021). It is a time when youth may drift away from the healthcare system without the close guidance from parents and caregivers despite their continued health and social care needs (CAPHC, 2016). Despite the attention transitions in care have received over the past three decades, findings demonstrate that the transition from paediatric to adult healthcare for youth with CCN continues to be fragmented, with the potential to cause an overall deterioration of health (Young et al., 2018). Understanding current practices and experiences is essential to improve and optimize transition practice (Maddux et al., 2015).
The findings of this study reveal current transition practices to be inconsistent and unpredictable. While most transitions to adult healthcare were perceived by study participants to be successful, the method of delivery was unguided and variable with each transfer having the potential for failure. Current transition practices of participants were conducted with little guidance and without an established transition program or policy. Although it is understood that transition for youth with CCN may require patient-specific adjustments due to the nature of their needs, without a formal transition process in place it becomes a time-consuming venture for all stakeholders with unreliable success.
Paediatricians and paediatric specialists were found to be the driving force behind transitions in care, acting as coordinators for the transition process to either primary care or an adult specialty. This is despite the fact that paediatric participants in this study found they lacked the necessary resources to facilitate a proper transition for youth with CCN, which is consistent with findings from previous studies (Berens and Peacock, 2015, Ciccarelli et al., 2014, Geenen et al., 2003). An additional finding was the sense that adult care providers could not meet patient expectations of care once transferred into their care. In keeping with previous research (Betz, 2018a, Kelly, 2015), adult care providers in this study feel like they are set up to fail due to the high-level of multidisciplinary care provided in paediatric healthcare, which is often unavailable in adult services.
Across all care provider types, a lack of knowledge about resources, along with gaps in services, to support the transition from paediatric to adult care was consistent with previous findings (Betz, 2018b, Young et al., 2009). Often, paediatric providers experience difficulties in supporting transitions due to the lack of similar healthcare services in the adult healthcare system, as well as a disparity in knowledge regarding existing services. Specifically, most difficult was identifying appropriate psychosocial support for youth, aligning with previous findings (Berens and Peacock, 2015, Peter et al., 2009). Of note, adult specialists and PCPs did not feel as though they have the knowledge and/or appropriate skill level to care for certain complex conditions (Berens and Peacock, 2015, Ciccarelli et al., 2014, Kelly, 2015, Peter et al., 2009, Reiss et al., 2005).
The importance of continuous care from paediatric to adult healthcare was emphasized by several participants in this study. Continuity of care is represented by increased information sharing and enhanced care coordination between care providers and stakeholders invested in a patient’s care as a result of strong and transparent relationships (Alberta Health Services, 2021). Previous findings have shown that care providers receiving youth in transfer, such as adult specialists or PCPs, encounter difficulties in receiving patients due to little or no health history (Wu et al., 2018); however, this study found that communication between providers did not serve as an obstacle in providing transition care. There were little to no barriers encountered when communication between providers and documentation was thorough as experienced by participants.
An essential facilitator for ensuring care continuity is the use of primary care services and providers who provide first-contact services and integrate care across systems (Government of Canada, 2012). Consistent with previous findings (Andrade et al., 2017; Chafe et al., 2019, Dewan and Cohen, 2013), paediatric provider participants in this study often provide substantial primary care services during childhood and adolescence. This has led to PCPs struggling to provide care post-transition when little adult specialist support is available (Schraeder et al., 2020). This lack of integration between primary and specialist care results in a lack of confidence and knowledge in PCPs’ ability to manage care when the time for transfer arrives, thus fragmenting care services (Kelly, 2015). Studies suggest that continuous primary care during the transition period may lower the risk of experiencing adverse outcomes for youth with CCN (Schraeder et al., 2020, Toulany et al., 2019).
Understanding the recommendations of care providers in their venture to transition youth with CCN from paediatric to adult healthcare is an important component to address needs and improve practice. All participants who support youth in the transition from paediatric to adult healthcare recommended enhancing their knowledge of available community and clinical resources. Furthermore, paediatric providers noted that they require training to help patients and families prepare for transition. An additional recommendation from paediatricians was to emphasize changes in service delivery that the patient and family may experience as they enter adult healthcare services. This recommendation addresses a need previously identified by patients and their families (Clarke et al., 2011) and mitigates a barrier identified in one study that showed that this conversation between providers and their patients took place only 2% of the time (Maddux et al., 2015).
A service delivery recommendation, consistent with previous research, supports a period of blended practice (Betz, 2018a, Crowley et al., 2011, Kyrana et al., 2016, Van Staa et al., 2011, Young et al., 2009). This includes shared care and decision-making during the transition period among paediatric, adult, and PCPs to co-manage the transition process (Schraeder et al., 2020). In this manner and with the comfort of familiarity, barriers to establishing a therapeutic relationship between youth and their adult providers can be removed and initial consultation may be facilitated.
The implementation of a care coordinator was another recommendation that was almost unanimously recommended by study participants. Previous findings have shown that this role, when implemented during the transition period, decreases inpatient and emergency utilization and costs, as well as increases family satisfaction ratings (Ciccarelli et al., 2015, Geenen et al., 2003, Kyrana et al., 2016).
Another recommendation from this study was the use of virtual care appointments for youth transitioning to adult services. With this method of healthcare delivery gaining increased prominence due to the COVID-19 pandemic, it has been found by participants to facilitate transition care and remove barriers due to limited resources and geographical location.
Study limitations
Understanding transition practices is a crucial first step to improving them (Maddux et al., 2015). Despite the strengths of this study, it is not without limitations. The first limitation included the geographical diversity of participants. Most participants were from the larger urban Anglophone centers in NB. There were few participants that represented the rural and Francophone locations in the province, limiting the experiences of this study. Additionally, there was representation from each care provider group; however, most participants were paediatric providers (generalists or subspecialists) and PCPs were primarily nurse practitioners. Finally, it is acknowledged that given the small sample size, the findings may not be generalizable to all care providers supporting youth with CCN as they transition from paediatric to adult healthcare. Nonetheless, having achieved data saturation and accounting for the four pillars of trustworthiness in qualitative studies, the broader themes may be transferable to similar settings.
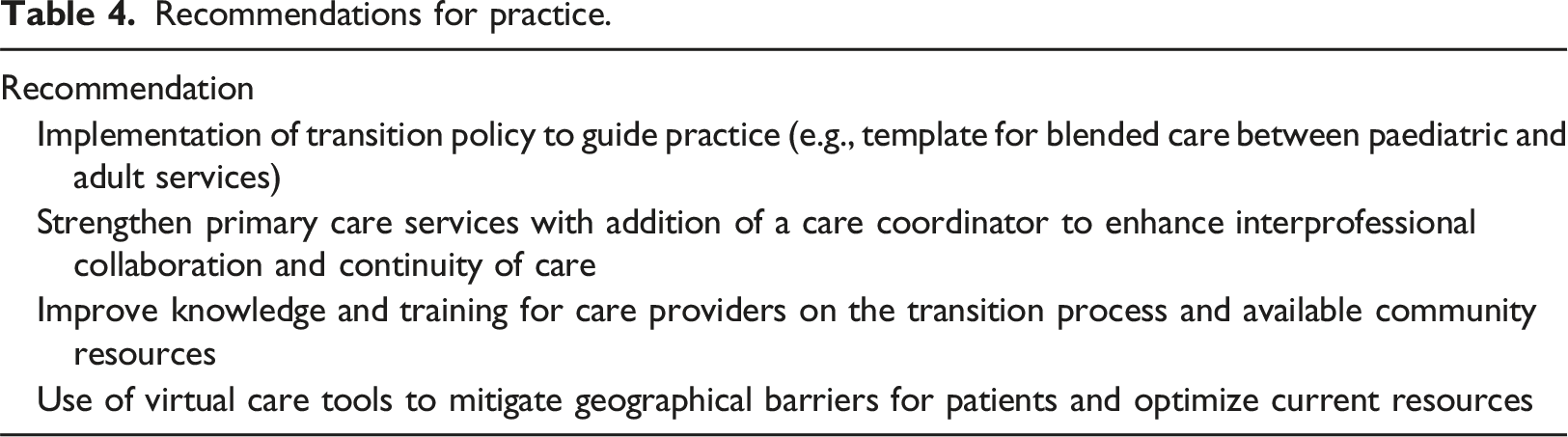
Implications for practice and research
Recommendations for practice.
Conclusion
It is well established that transition services for youth with CCN as they cross the chasm of paediatric to adult healthcare requires improvement. These services are found to be poorly managed and disjointed due to the complexity of care needs and maze of healthcare services. To improve transition practice, it must first be understood. This study is an initial step in understanding transition practices and recognizing care provider needs to inform the improvement of transition practice with future recommendations.
Supplemental Material
Supplemental Material - Transitioning from paediatric to adult healthcare: Exploring the practices and experiences of care providers
Supplemental Material for Transitioning from paediatric to adult healthcare: Exploring the practices and experiences of care providers by Jennifer Splane, Shelley Doucet, and Alison Luke in Journal of Child Health Care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the New Brunswick Innovation Foundation; 2020 008.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.