
Abstract
Exercise interventions are identified as effective treatments for children not meeting developmental milestones. This systematic review synthesizes research regarding exercise interventions that involved social participatory elements, for children with complex developmental needs. Academic Search Complete, CINAHL, Emcare, Proquest Theses and Dissertations, MEDLINE, and Google Scholar were searched systematically for relevant studies. Peer-reviewed studies meeting the review aim and published between 2000 and 2021 in English, were included. Methodological quality of 49 eligible studies (47 controlled trials, two mixed methods, total of 2355 participants) was appraised using the Mixed Methods Appraisal Tool. Narrative synthesis identified two groups of studies: Group 1 incorporated intentional social participatory elements; Group 2 likely involved incidental social participation. Most studies were of moderate to low methodological quality. Few measured impacts of interventions upon total physical activity levels. Short-term improvements in physical outcomes – particularly motor skills – were most frequently reported and were the main benefit of social exercise interventions for children with complex developmental needs, for which evidence exists. Further rigorous, longitudinal research is needed to assess social, psychological, and executive function outcomes of social exercise interventions in this population. Such interventions should incorporate booster sessions to provide children with greater opportunity to meet developmental milestones.
Introduction
Participation in regular physical activity (PA) helps maintain physical and mental wellbeing (Lubans et al., 2016). Physical activity with social participatory elements such as active play during school recess, team sports or family-based PA, provides children with opportunities to practice prosocial skills including communication skills, taking turns, and conflict resolution and gaining these skills may contribute to children’s enjoyment and participation in PA (O’Connor et al., 2014). The World Health Organisation recommends that children accrue a minimum of 60 min of moderate-to-vigorous PA (MVPA) per day but globally many children are not meeting those guidelines (Tremblay, 2014). Cross-sectional studies have found that children’s levels of PA are positively correlated to their ability to perform fundamental motor skills (FMS), whereby those more proficient in FMS have higher levels of PA; and those with less proficiency participate in less PA (Lubans et al., 2010). This association is not surprising as FMS provide foundational skills, such as locomotor, object-control, and stability skills, to participate in many different types of PA, including sport-related activities (Lubans et al., 2010). It is important for children to gain proficiency in these skills as early as possible as the relationship between ability and participation in PA may strengthen over time (Stodden et al., 2008). However, directionality of this relationship and its many probable mediators aren’t fully understood (Barnett et al., 2011). Children who have complex developmental needs are a particular group who are at greater risk of inactivity and reduced FMS (Ferguson et al., 2015).
Children with complex developmental needs may have a single identified developmental disorder, or in a substantial number of children, they may experience concurrent developmental conditions (Kadesjo and Gillberg, 1999). Conditions may impact their physical ability, for example, Developmental Coordination Disorder (DCD) which is a broad diagnosis encompassing motor difficulties from immaturity and developmental delay (McWhirter et al., 2022). Other conditions may also impact them behaviourally and socially including autism spectrum disorder (ASD), which impacts social and communication skills, repetitive behaviours, and narrow interests across a wide spectrum (Bremer et al., 2015); and attention deficit hyperactivity disorder (ADHD), characterised by inattention, hyperactivity, and impulsive behaviours (O’Connor et al., 2014). Some children who are not meeting their developmental milestones have no formal diagnosis (Weitzman and Wegner, 2015). Management of these complex developmental presentations are important to reduce the risk of secondary health and psychosocial complications (Piek et al., 2008). Physical activity has been identified as an effective treatment, due to the physical, socio-emotional, behavioural, and cognitive benefits that it provides (Den Heijer et al., 2017). Exercise is PA, that is, structured and planned (Dasso, 2018). Recent systematic reviews have focussed upon using exercise to manage ADHD, (Cerrillo-Urbina et al., 2015; Den Heijer et al., 2017) rather than contextual elements of exercise interventions.
Aim
To identify, critically appraise, and synthesise findings from published studies of exercise interventions that involved social participatory elements, in children with complex developmental needs.
Methods
The protocol for this systematic review was registered with PROSPERO (CRD42020188327). Methods and findings are reported using the PRISMA 2020 statement (Page et al., 2021) as a guide.
Identification of studies
Systematic searches for relevant articles were completed in February 2021 via the following databases and search engine: Academic Search Complete, Cumulative Index to Nursing and Allied Health Literature, Emcare, Proquest Theses and Dissertations, MEDLINE, and Google Scholar. Key search words and subject headings, related to PA, exercise and the relevant population, in conjunction with appropriate Boolean operators, were identified by reviewers. Search terms included: PA, exercise, sports, recreation, developmental vulnerability, motor skills, child, intervention, and program. Specific search strategies, adapted for each database by the librarian, are reported in supplementary material.
Inclusion/exclusion criteria
All identified citations, from searches, were uploaded to EndNote X9 (Clarivate Analytics, 2013) and duplicates removed. Title and abstract of each remaining report were screened against inclusion and exclusion criteria by one reviewer and clearly ineligible articles were removed.
Inclusion criteria included studies which included children aged 2–18 years who were identified as not meeting their developmental milestones, studies that evaluated an exercise intervention which included social participatory elements, research published between 2000 and 2021 in English language, and peer reviewed published research including quantitative, qualitative, and mixed methods studies, theses.
Exclusion criteria included were studies that did not evaluate an exercise intervention or described an exercise intervention with no social elements, and review articles, conference proceedings and posters; non-peer-reviewed research, including grey literature and opinion papers.
Reports were retained, and full text retrieved, if they appeared to be potentially eligible or if there was any uncertainty regarding eligibility, and all decisions were recorded. Full texts of these articles were then assessed for eligibility by two reviewers, independently. Disagreements were resolved by a third reviewer and excluded reports were removed from further consideration, with reasons for exclusion recorded. Reference lists of all reports selected for inclusion, based on eligibility criteria, were screened to identify additional eligible studies.
Assessment of methodological quality
Methodological quality of included studies was appraised using the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). This tool allows assessment of five different types of study using a single tool. Two reviewers independently scored each study against five quality criteria and disagreements were resolved by a third reviewer. As recommended by Hong et al. (2018), no studies were excluded from this study because of their methodological quality assessment results.
Data extraction and synthesis
Information extracted from each study included: authors, year of publication, study design, setting, participant characteristics (gender, age, developmental needs), intervention description, comparator (if any), sample size, study duration, analysis method, main outcome measure(s), secondary outcome measure(s), quantitative results, and qualitative findings. Extracted data were documented in standardised tables which had been piloted by all reviewers using a small number of studies, to ensure consistency between reviewers in data extraction. Data extraction was completed by two review authors independently and then combined into one table. Differences were resolved through discussion and consensus.
Data were synthesised using a narrative approach (Popay et al., 2006). Meta-analysis was not conducted because the studies were not sufficiently homogenous for a meaningful analysis due to diversity of participants, interventions, and outcomes, as well as lack of sufficient data. Findings from individual studies were tabulated and sorted, guided by the results of the MMAT methodological quality appraisals.
Results
Identification and selection of studies
Figure 1 summarises results of identification, screening, and selection of studies in a PRISMA flow diagram (Page et al., 2021). After duplicate removal, 2063 studies remained for screening. Title and abstract screening resulted in 1795 papers being excluded and 268 full texts of studies were obtained for review. Full text reviewing excluded 219 studies, leaving 49 eligible studies. PRISMA flow diagram (Page et al., 2021) depicting literature search, screening and selection processes.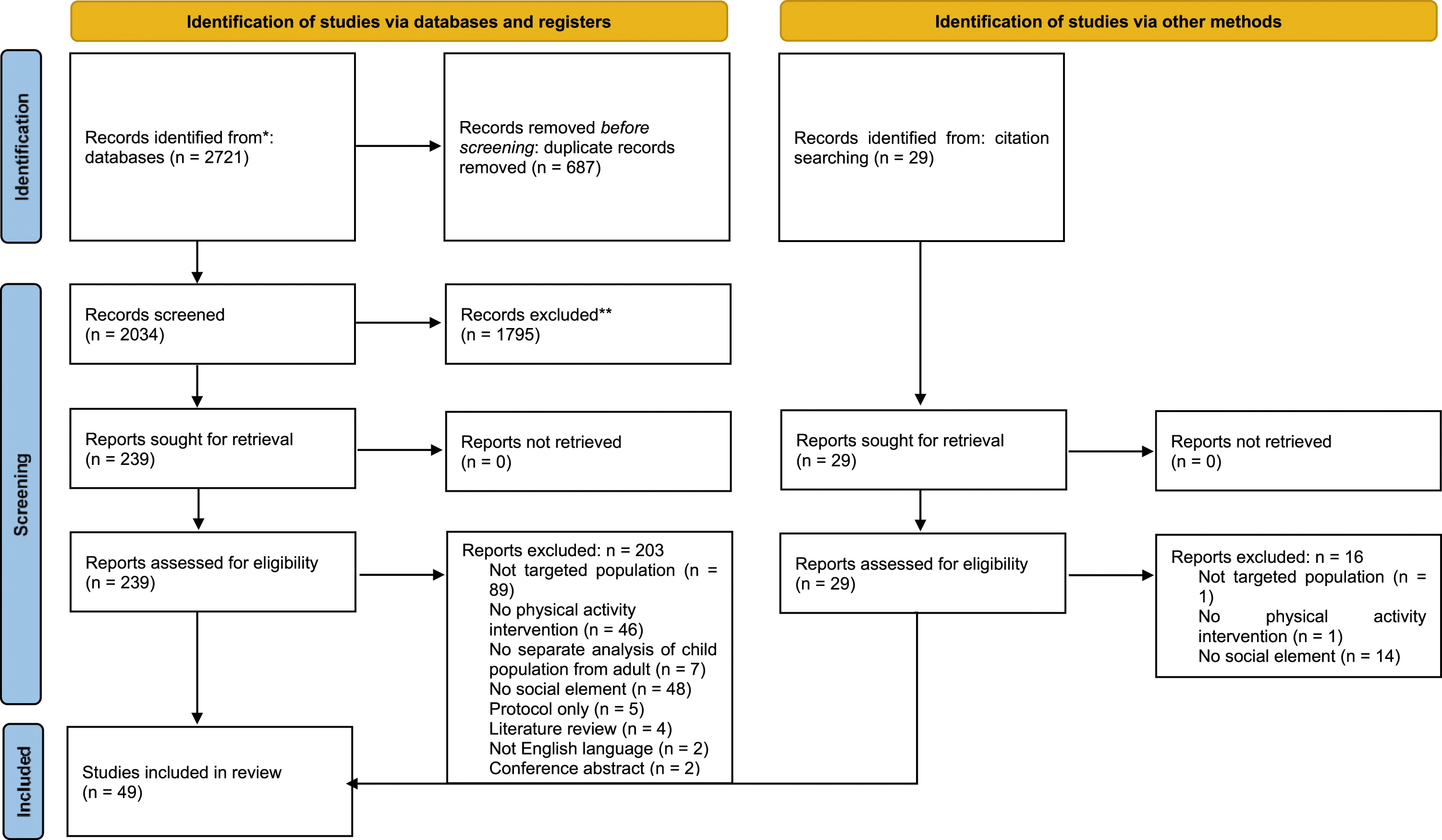
Characteristics of included studies
Characteristics of included studies.

Notes: CG: control group; CP: cerebral palsy; ID: intellectual disability; IG: intervention group; NI: no intervention; NR: not reported; NTT: Neuromotor Task Training; TD: typically developing.
Numbers of participants in intervention groups ranged from five to one hundred and twenty-one participants. Nearly three quarters of studies (n = 36, 73%) included less than 20 participants in their intervention group. Fourteen studies (29%) included pre-schoolers (aged 3–5 years), forty-three (88%) included children aged six to 12 years and twelve (24%) included children aged 13 years and older. Children with a range of developmental conditions were included in the studies, including ADHD (n = 14, 29%), ASD (n = 10, 21%), DCD (n = 9, 18%), mixed developmental conditions (n = 5, 10%), and intellectual disability (ID) (n = 5, 10%).
Quality screening
Of the included studies, twenty (41%) were quantitative randomised controlled trials (RCT), twenty-seven (55%) were quantitative non-randomised controlled trials (NRCT) and two were mixed method studies (supplementary material). Methodological quality of studies varied, with 11 (22%) of studies deemed high quality (scoring 5 on MMAT), 20 (41%) medium quality (scoring 3 or four on MMAT), and 18 (37%) low quality (scoring ≤2 on MMAT). Nearly three quarters (n = 13, 72%) of those evaluated as low quality used a RCT methodology. Quality assessment of RCT studies found that 15 (75%) did not randomise the population adequately, in 14 (70%) outcome assessors were not blinded to type of interventions, and eight (40%) indicated poor participant adherence to assigned intervention. A third (n = 9, 33%) of NRCT studies were deemed high quality. Among all NRCT studies, information on conduct of intervention or exposure was not provided by 12 (44%) and nine (33%) did not account for confounders in the design and analysis. Neither mixed method study met criterion of achieving specific quality standards for each method utilised in their design.
Synthesis
Overview
Group one: studies which incorporated social participation with other participants as an integral part of their group intervention.

Notes: BOT: Bruininks–Oseretsky test of motor proficiency; CBCL: child behaviour checklist; CG: control group; EF: executive function; HEP: home exercise program; ID: intellectual disability; IG: intervention group; MABC: movement assessment battery for children; MVPA: moderate to vigorous physical activity; NR: not reported; OTH: other; PA: physical activity; PE: physical education; PHY: physical; PSY: psychological; SOC: social; TD: typically developing; TGMD: test of gross motor development.
Group two: studies where social participation between participants were likely an incidental part of the group context.

Notes: BOT: Bruininks–Oseretsky test of motor proficiency; CG: control group; DCD: developmental coordination disorder; EF: executive function; HEP: home exercise program; ID: intellectual disability; IG: intervention group; MABC: movement assessment battery for children; MVPA: moderate to vigorous physical activity; NR: not reported; OTH: other; PA: physical activity; PDMS: Peabody developmental motor scales; PHY: physical outcome measures; PSY: psychological; SCQ: social communication questionnaire; SOC: social outcome measures; TD: typically developing; TGMD: test of gross motor development.
Group one: Studies which incorporated social participation as an integral part of exercise intervention
High quality studies which incorporated social participation as an integral part of exercise intervention described interventions that included motor skills training or skills training for specific collaborative sports, targeting children aged 5–14 years (n = 3, 12.5%). Two studies (O’Connor et al., 2014; Pan et al., 2017a) utilised the Bruininks–Oseretsky Test of Motor Proficiency (BOT-2) to assess participants’ motor skills, while Smith (2015) used The Test of Gross Motor Development (TGMD-2). Pan et al. (2017a) found significant improvement in BOT-2 scores, cardiovascular endurance, and flexibility post intervention. Their intervention included a simulated developmental horse-riding program, ball games and exercise stations; and finished with cool down activities focused on ‘prosocial behaviour and engagement’ (Pan et al., 2017a: 786). Pan et al. (2017a) only assessed physical outcome measures, despite their goal of providing an intervention that was suitable for children with ADHD and which included social elements. O’Connor et al. (2014) evaluated effect of sports training as part of an intensive behavioural modification program for children with ADHD and found significant improvements in motor and sports skills (performance and knowledge of game rules). They asked parents to rate their child’s improvement in ‘sports skills’ and ‘good sportsmanship’ using a Likert scale (O’Connor et al., 2014: 1010) and found that parents of children in the intervention group reported significantly larger improvement than parents of children in the no-intervention control group.
Smith (2015) used outcome measures assessing four domains to evaluate a one-week intensive, multi-sport, skills camp for girls with ASD (n = 13). They found significant improvement in TGMD-2 scores but no improvement in total PA levels immediately post program or at 8 weeks post-program. Improvements found in social and psychological domains, using questionnaires that were completed by both children (Children’s Self-Perceptions of Adequacy in and Predilection for Physical Activity) and guardians (The Social Skills Improvement System (SSIS), Vineland adaptive behaviour scale (VABS-2)), were not statistically significant. Children also completed the Children and Youth Self Perception Profile and reported significant improvements in sub-domains of physical self-perceptions, sport/athletic competence, and social skills. Significant correlations between motor skills and physical self-perceptions were also found, suggesting that as a child’s motor skills improved, their self-efficacy for PA and sport competence also increased.
Synthesis of findings from lower quality studies from Group One, listed in Table 2 (n = 21, 87.5%), identified that only two studies measured PA levels and found no significant change in PA levels post intervention (Kane and Staples, 2016; Rubin et al., 2018). Kane and Staples (2016) reported a non-significant improvement of 10-min of MVPA per day, but their small sample size (n = 10) is likely to have contributed to the null finding. Sixteen (76%) lower quality studies assessed motor skills and eleven (69%) of them found significant improvement in at least one aspect of participants’ motor skills. No discernible pattern was identified in social, psychological, or executive function outcome measures. However, it is worth noting the wide variation in measures and focus upon physical outcomes, as only nine (37.5%) studies assessed social outcomes, seven (29%) studies executive function outcomes, and four (17%) studies psychological outcomes.
Group two: Studies where social participation was likely to have been an incidental part of group context
High quality studies in Group Two, in which social participation was likely to have been an incidental part of group context, described exercise interventions that included motor skills training (n = 4, 50%) and obstacle courses (n = 3, 37.5%). Six (76%) high-quality studies in this group focused on only one domain of their participants’ development; specifically, four (50%) focused on physical outcomes, one (12.5%) on psychological outcomes, and one (12.5%) on executive function outcomes. Three (60%) of the five studies in Group Two that assessed motor skills utilised the Movement Assessment Battery for Children-2 and significant improvements in motor skills were found in all five studies. Three (37.5%) studies utilised other physical outcome measures, including Fong et al. (2012), who found significant improvements in sensory organisation and unilateral stance tests in 16 children with DCD following 3 months of Taekwondo training. No high-quality studies in Group Two assessed total PA levels post intervention.
Bremer et al. (2015) used parent questionnaires to assess social skills (SSIS) and adaptive behaviours (VABS-2), and behavioural video of free play, which was analysed by researchers; they found non-significant improvements across these measures in their sample of eight children with ASD. Angeli et al. (2019) used The Self Perception Profile for Children to assess self-concept following a 10-week community running program for children and young adults with disability (n = 19). Participants significantly improved their self-perception in domains of scholastic competence, athletic ability, and physical appearance but no significant improvements occurred in their self-perception of social competence and behavioural conduct. Chou and Huang (2017) found significant improvements in attention and discrimination function in children with ADHD following an 8-week yoga program.
Synthesis of findings from lower quality studies from Group Two (Table 3) (n = 17, 68%), identified that four (23.5%) studies assessed PA levels via accelerometer data, and none found significant improvements in PA levels post intervention. Most studies (n = 12, 70.5%) that investigated physical outcomes reported significant improvements in one or more outcome measure. Six (35%) studies examined social outcomes with mixed results; three (50%) reported significant improvements in at least one social outcome measure, including social and play skills. Three (18%) studies assessed a range of psychological attributes, with significant improvements found in self-concept, depression, and stress. Five (30%) studies investigated executive function post intervention, with significant improvements found for attention, cognitive flexibility, and response inhibition.
Adverse findings across both groups
Two (4%) lower quality studies reported adverse findings. Caçola et al. (2016) examined two interventions, both involving motor skills training; one was focussed on task orientated activities and another on goal directed activities. They found that anxiety increased, and enjoyment decreased in the task orientated group post intervention. The authors acknowledged that it was difficult to draw conclusions on whether this was an intervention effect because of confounding factors, in particular differences in group sizes. The task orientated group performed their intervention in one group (n = 11) whilst goal directed activities were conducted in three smaller groups of four-to-five participants.
Ninot et al. (2005) assessed social outcomes for adolescent females with ID, across four groups: a swimming group for participants with ID only, a mixed swimming group of children with ID and children who were typically developing (TD), a physical education group, and a control group (no intervention). They found no change in perceived self-worth across the four groups but children with ID in the mixed swimming group had a significantly lower self-perception of athletic competence post intervention, despite an increase in their performance.
Barriers and facilitators
Seven (28%) studies reported 11 facilitators, and three (12.5%) studies reported six barriers to implementing interventions which incorporated social participation with other participants as an integral part of exercise interventions (Group One; Table 2). Facilitators included incentivising attendance with money and a chart depicting participants’ attendance (Pan et al., 2017a); and parents facilitating carry-over from intervention to home environments (Kane and Staples, 2016). Enjoyment or fun was the most frequently mentioned facilitator (n = 3, 27%), whilst engagement barriers (n = 5, 83%) were the most frequently reported barriers. For example, Caçola et al. (2016) noted that the varying abilities of children with DCD limited engagement of some in group interventions.
Seven (28%) studies reported 11 facilitators, and seven (28%) studies reported 10 barriers to implementing interventions where social participation between participants were likely to be an incidental part of group context (Group Two; Table 3). Most of the identified facilitators related to engagement (n = 7, 64%), including: enjoyment of the intervention (Dickinson and Place, 2014) and the dynamics of small groups providing opportunities for social participation (Bremer et al. 2015). Barriers relating to engagement were most frequently reported (n = 5, 50%) and included children shifting to motor skills in which they had greater proficiency, which limited their practice time of motor skills in which they were less adept (Valentini et al., 2017).
Discussion
The aim of this review was to synthesise current evidence relating to exercise interventions involving social participatory elements, for children who have complex developmental needs. Two broad groups of studies were identified: studies that incorporated social participation as an integral part of exercise intervention (Group One), and studies where social participation between participants were likely an incidental part of group context (Group Two). However, differences between these exercise intervention types in physical outcomes are currently unclear, as both groups of studies focussed predominantly upon physical outcomes, particularly motor skills. Intervention influence upon total PA levels is largely unknown, as only seven of the 49 included studies assessed total PA levels post intervention. Furthermore, the review identified aspects of social, psychological, and executive function domains that would benefit from additional investigation in future studies of group exercise interventions in this population. Finally, adverse findings, albeit identified in only two lower quality studies, highlight that group context may be an influential factor in a child’s experience of group exercise interventions.
This review found short-term improvements across many different physical outcomes following exercise interventions with social participatory elements, particularly in motor skills, but long-term implications of these improvements have not been studied. Future studies should consider longitudinal designs so that physical and psychosocial outcome persistence is investigated. It is also worth noting that although short-term improvements in motor skills were found, in many cases, these improvements did not allow children to meet their developmental motor milestones (Pan et al., 2017a, 2017b; Tsai et al., 2012). This finding suggests that future studies should not only consider longitudinal designs but also repeated intervention or booster sessions (Gearing et al., 2013). Booster sessions are now incorporated into behaviour change practices, acknowledging that enthusiasm and routines can fade over time, leading to relapses (Gearing et al., 2013). Gaining insights into both longitudinal outcome persistence and impacts of booster sessions would provide clinicians and families with more useful information from which to plan interventions.
All included studies utilised an exercise intervention, but only seven (14%) studies assessed short-term total PA levels post intervention. None of these studies found significant increases in total PA levels but their findings may have been impacted by small sample sizes. Thus, the influence of these interventions on total PA levels, both short- and long-term, is largely unknown and a significant gap in this area. Omission of total PA levels as an outcome measure is inconsistent with current understanding of a dynamic relationship between motor skills and PA (Barnett et al., 2011), and appears short-sighted considering potential health benefits and current low levels of total PA in this population (Lubans et al., 2010; O’Connor et al., 2014).
It seemed a reasonable hypothesis that high quality studies which integrated social elements into exercise interventions would observe greater improvements across multiple domains than those where social participation was incidental to the exercise. However, few studies assessed outcomes across multiple domains so limited insight was gained about impacts of group exercise interventions upon the social domain and other aspects of a child’s development. However, the review has identified several outcome areas that would benefit from further investigation, including sport skills and sportsmanship (O’Connor et al., 2014), social and play skills (Smith, 2015), adaptive behaviours (Bremer et al., 2015), self-concept (Angeli et al., 2019), self-perception (Smith, 2015), depression (Da Silva et al., 2020), stress (Da Silva et al., 2020), attention (Ahmed and Mohamed, 2011), cognitive flexibility (Da Silva et al., 2020), and response inhibition (Verret et al., 2012). It is important that further research is done to highlight which contexts influence these outcomes within this population, both positively and negatively. For example, Barnett et al. (2011) has recommended targeting sports competence alongside PA levels and skill development because of its influence on active lifestyles of children who are TD. The complexity of an individual’s exercise experience and social context was highlighted by Ninot et al.’s (2005) adverse finding of significantly lower athletic self-perception in children with ID who trained and competed against children who are TD in swimming. Children with ID reported lower athletic self-perception despite an improvement in their own swimming times indicating comparative aspects of exercise contexts can impact a child’s self-perception, enjoyment (Ninot et al., 2005); and ultimately their engagement in exercise.
Child engagement was facilitated in some studies through parent involvement. Home exercise programs may play an important role in facilitating carryover of exercise interventions into a child’s home environment (Huang and Pang, 2010; Kane and Staples, 2016). They may also provide both children and parents with ideas and experiences of successful and sustainable exercise at home. In addition, studies of children who are TD have found that doing exercise together with their parents provides opportunities for parental role modelling of exercise (Yao and Rhodes, 2015), bonding and connecting experiences, and opportunities for children to practice their developing skills in a safe environment (Freire et al., 2019). It was disappointing how little attention was given to assessing and evaluating potential benefits of home exercise programs of the included studies. Future studies should focus on how to evaluate this aspect, beyond engagement levels.
Social ecological models of health describe the complex interplay between children, families, their communities, and society (Bronfenbrenner, 1989). Importantly, they acknowledge that children influence their parents and their environment (James et al., 1998). Adopting a social ecological approach may increase the number of studies taking a holistic approach to child outcome measures (physical, social, psychological). This approach would also increase the number of studies involving parent with interventions and seeking the child’s view of exercise interventions. Finally, social ecological models of health would likely increase the number of studies utilising exercise interventions that were also available at home or in their community. A small number of studies in this review included novel exercise interventions that were unlikely to have been available in a child’s home or community or focused upon skills that children may not be able to utilise at home; for example, using a simulated developmental horse-riding machine (Pan et al., 2017a) and interventions focussed upon table tennis skills (Pan et al., 2016). Researchers should use exercise interventions that are relevant to the child’s community context, to increase the possibility of exercise interventions having long-term positive impacts upon total PA levels and health.
Limitations of included studies
Limitations of studies included moderate (n = 20, 41%) or low (n = 18, 37%) methodological quality of studies, which suggests high risk of bias. Design limitations, in particular small sample sizes, may have contributed to some of the null findings. Lack of a control group or utilisation of a no-intervention control group was another common limitation, whilst in contrast other studies used a waitlist design, which arguably seems a more ethically acceptable approach with this vulnerable population whilst also benefiting sample sizes. Confounding factors, such as comparing two different interventions with two different group sizes (which may have affected group interactions), were found. Additionally, the influence of the social element of the intervention or group context was often not adequately considered, with many studies (n = 18, 37%) making no attempt to measure impact upon other, non-physical aspects of a child’s development, either positive or negative. This limitation is underlined by some adverse findings, which may have been related to group context.
Parent and teacher voices were sought across a small number of studies but only one study, by Siu and Lo (2020), sought to gain the child’s perspective on a family rugby intervention. They found that children felt they had better self-control post intervention. The absence of children’s voices is an important gap in the research and future studies should consider ways to elicit children’s opinions of exercise interventions. Seeking child and family input into exercise interventions, prior to implementing them, via participatory approaches, would also increase the relevance of exercise interventions to target populations (Freire et al., 2022).
Limitations of review
The review is limited by likely publication bias and inclusion of only studies published in English between years of 2000 and 2021. Also, heterogeneity and low methodological quality of most of the included studies made it difficult to compare across studies. These factors limited analyses to narrative review, increasing the risk of reviewer bias, but comprehensive tables providing details of studies and extracted data have been compiled to increase review transparency (Munn et al., 2014). In addition, absence of, or insufficient description of the exercise interventions was a limitation in some studies and may have also erroneous grouping within this systematic review.
Implications for practice
Findings of this review suggest that group exercise intervention contexts influence children’s experiences and holistic development positively or negatively highlighting the importance of planning and evaluating the psychosocial impact of group exercise interventions upon this population. Although short-term improvements in motor skills were found following group interventions, many of the interventions did not support children to meet their developmental motor milestones, suggesting that longer interventions or booster sessions are required to provide children who are not meeting their developmental milestones with greater opportunities to thrive.
Conclusion
This review found that group exercise interventions with a social element for children who are not meeting their developmental milestones, may improve more than children’s motor skills. However, current evidence is of poor quality. Few studies took a comprehensive and holistic approach to assessing children’s developmental outcomes. Thus, further robust research is needed to establish the full impact of group exercise interventions upon social, psychological, executive function outcomes and total PA levels. Future research and exercise interventions should include longitudinal intervention studies or booster sessions to ensure that children are given greater opportunities to thrive and meet their developmental milestones.
Supplemental Material
Supplemental Material - Social exercise interventions for children who have complex developmental needs: A systematic review
Supplemental Material for Social exercise interventions for children who have complex developmental needs: A systematic review by Kate Freire, Rod Pope, Isabella Size, Kristen Andrews, Emma Fitz-Gerald and Tricia Bowman in Journal of Child Health Care
Footnotes
Author contributions
Professor Darryl Maybery, Monash University Department of Rural Health, who contributed to early stages of planning and conduct of the review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Three Rivers Department of Rural Health, Charles Sturt University. Three Rivers is funded by the Australian Government Under the Rural Health Multidisciplinary Training Program.
Supplemental Material
Supplementary material for this article is available on the online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.