
Abstract
Facilitating children’s understanding of their medical condition can improve health outcomes and psychosocial well-being. To inform how medical information is delivered, an interpretive qualitative approach was used to explore children’s understanding of their brachial plexus birth injury. In-depth interviews of children with brachial plexus birth injuries (n = 8) and their caregivers (n = 10) were conducted individually and as a child-caregiver dyad. Thematic analysis of interview data found that children primarily understood their injury through lived experiences of functional and psychosocial concerns related to movement and appearance of the affected limb, rather than medical information. Children’s ability to learn about diagnostic and prognostic information was influenced by age, emotional readiness, and background knowledge. In receiving information about their medical condition, children needed greater support in understanding their prognosis and its implications on their future. These narratives indicate the importance of addressing the primary functional and psychosocial concerns to contextualize medical information and ascertain the emotional readiness of children with brachial plexus birth injuries in information delivery approaches.
Keywords
Introduction
Brachial plexus birth injury (BPBI) occurs in approximately 1–3/1000 childbirths in which the nerves that supply upper limb motor and sensory control is injured (Pondaag et al., 2004). Although most infants achieve full neurological recovery, the other 20–30% experience lifelong impairments in the affected limb which often require intensive treatment plans (Pondaag et al., 2004). As interventions cannot restore complete physical function, families ideally engage in shared decision-making to ascertain how treatment options, along with their risks and benefits, align with their preferences and values (Ho et al., 2021).
Children have a basic right to participate in medical decisions and be heard (United Nations, 2002). Their desired level of involvement may differ according to their medical needs, competence, developmental age, and the type of decision that needs to be made (Coyne and Harder, 2011). Receiving better education regarding their medical condition can help children form accurate expectations for treatment (Rushforth, 1999; Veldtman et al., 2000). It is critical that they are given opportunities to best understand their medical condition, express their desired level of involvement (Kelly et al., 2017), and support with making decisions that aligns well with them.
Literature on active participation of children with BPBI during information delivery regarding their medical and rehabilitation management is limited (Ho et al., 2021). Studies have typically focused on parents’ health literacy and understanding of the diagnosis. Bellew and Kay (2003) demonstrated that information imparted to parents at the time of diagnosis is limited due to lack of BPBI knowledge by staff at the birthing hospital. The possibility of irreversible limb impairment and potential need for medical and rehabilitation treatments also causes significant stress to parents at the time of diagnosis. As a result of these factors at the time of birth, many parents seek initial information via the Internet (Bellew & Kay, 2003). Consequently, there is relatively more literature on medical education about BPBI using online platforms than traditional settings. BPBI information on the Internet is often inconsistent, inadequate, and misinformed (Winship et al., 2014). Accuracy of information parents receive prior to their specialist BPBI visit is uncertain (Shah et al., 2006). Good parental health education is important as studies show that health literacy in parents/caregivers is linked to their child’s health literacy. Low health literacy in both or either parents and/or children are associated with worse child health behaviors and outcomes (DeWalt and Hink, 2009).
While there are studies demonstrating how parental understanding affects that of their child (DeWalt and Hink, 2009), there is no known research that directly explores health literacy in children with BPBI or the family unit. In elucidating the decisional needs of children and adolescents with BPBI in shared decision-making, Ho et al. (2021) describe the importance of the relational processes involved in medical education and decision-making. The influence of clinician–family relationships and interpersonal connections plays a role in how information is delivered, understood, and how shared decisions are made. In this way, healthcare and family contexts are important considerations of the child’s understanding of their health condition. Further, families tend to target multiple sources of medical information beyond the information provided by their health care team including conversations with people in their social network and online health information which can help or hinder their understanding of medical information (Edwards et al., 2015).
Aim
To explore children’s understanding of their BPBI to inform how medical information is delivered to the child and family in an outpatient clinic setting.
Methods
This study was approved by the Research Ethics Board at the Hospital for Sick Children (SickKids) and the University of Toronto. An interpretive qualitative approach informed by a social constructionist epistemology was used to explore children’s understanding of their BPBI. Interpretive approaches focus on individuals’ interpretations of the world and what meaning they prescribe to certain phenomena. A social constructionist approach assumes that reality is a socially constructed outcome of human processes and recognizes that meanings are co-constructed and deeply embedded in context (Green and Thorogood, 2004b). The context of our research is the outpatient clinic setting where children and parents receive information about their BPBI together. By focusing on the children’s points of view and the meanings behind their experiences, rather than making assumptions and generalizations about the diagnosis itself, we may gain a deeper understanding of their unique perspectives.
Population
This study used maximal variation purposive sampling used to recruit children with a BPBI more broadly, emphasize the unique experiences of each child, and identify patterns connecting these experiences (Patton, 2002). Eligible child participants met the following inclusion criteria: 6–18 years old, have a BPBI diagnosis, are a client of the SickKids BPBI clinic, and are English-speaking. Children with upper and total BPBI were included in the study. Children were also required to have a caregiver that is English-speaking who were also interviewed. Exclusion criteria included children with a developmental delay.
Child participant demographics.
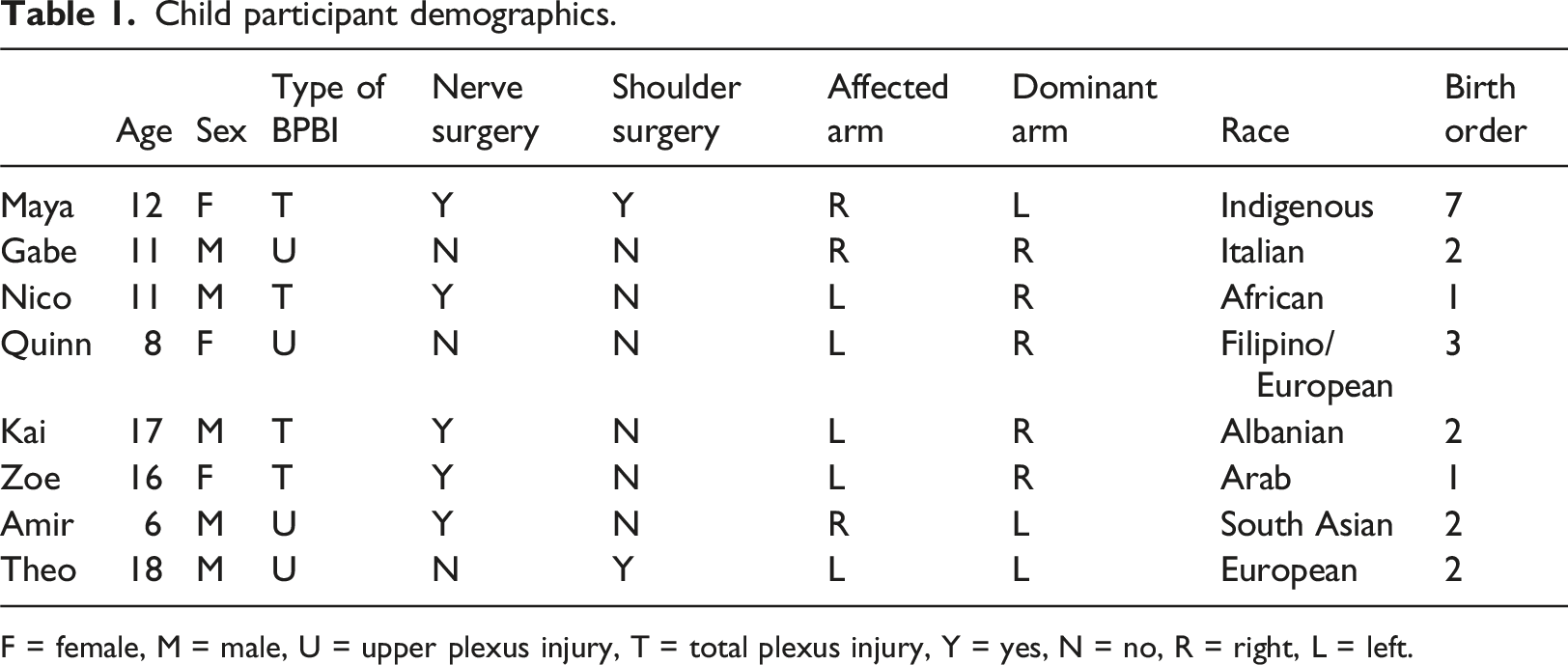
F = female, M = male, U = upper plexus injury, T = total plexus injury, Y = yes, N = no, R = right, L = left.
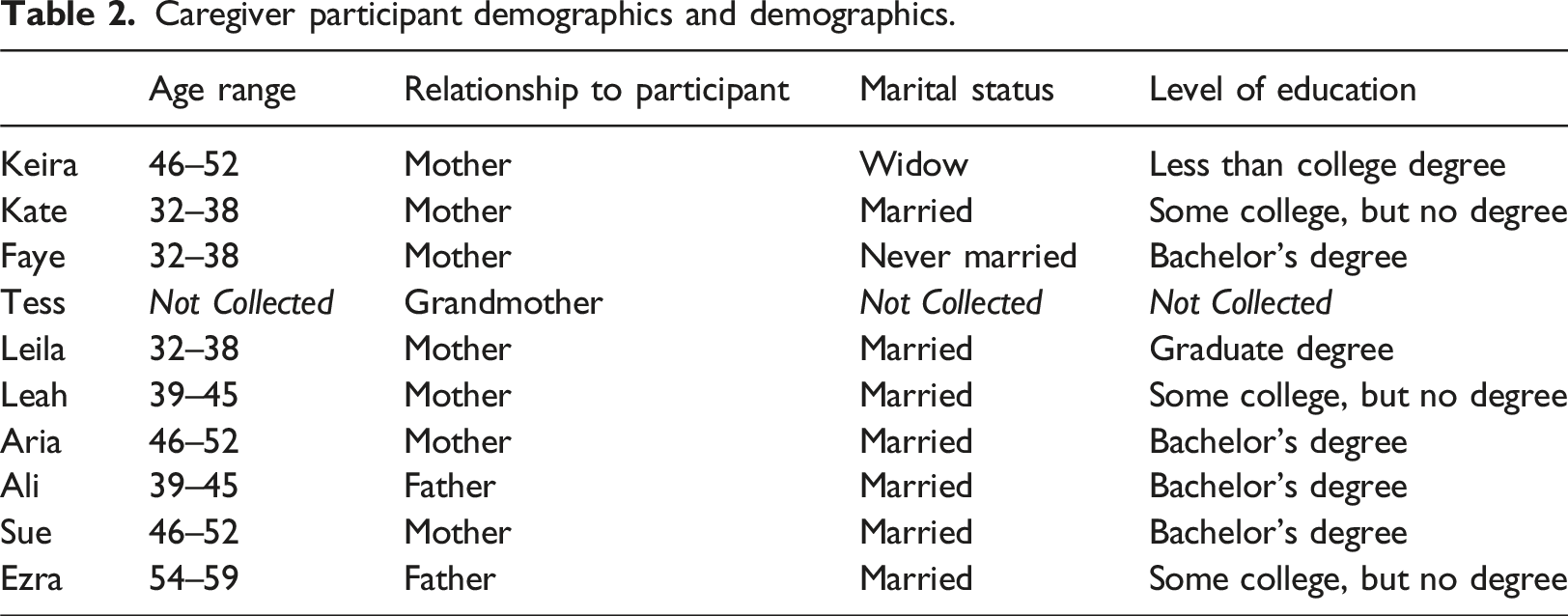
Caregiver participant demographics and demographics.
Data collection
Demographic data such as age, injury severity, race, and birth order were collected through each child’s electronic health record system. Caregiver age range, level of education, and marital status was collected through a demographic questionnaire.
Child interviews were co-conducted by the first authors on this paper, two graduate students, while caregiver interviews were conducted separately by another pair of graduate students. All graduate students were trained in qualitative interviewing by the principal investigator (PI). The child and caregiver interviews were conducted independently to ensure that the child’s voice was heard and to address the power differential (Holstein and Gubrium, 2003). In the clinic setting, children’s knowledge is shaped and expressed alongside their parents; therefore, it was important to hear their voices separately and together. At the end of each interview, children and caregiver(s) were invited to share in a collective debriefing interview to consolidate their understanding, facilitate further discussion, and close the interview. A child–caregiver dyad approach was used to triangulate data sources as caregivers were asked to add their perceptions to their child’s voice (Ungar et al., 2006). Interviewing the family members together also aligns with a social constructionist approach of interpreting children’s experiences in the context of their lived reality of information delivery in the clinic setting (Green and Thorogood, 2004b). The interviews were conducted in-person in two adjacent private offices, while debriefing sessions were held in a private conference room. Consent and assent, when appropriate, was revisited prior to the debriefing and children were given opportunity to choose what they wish to disclose.
{kind=link}
{kind=link}
Interview guide.
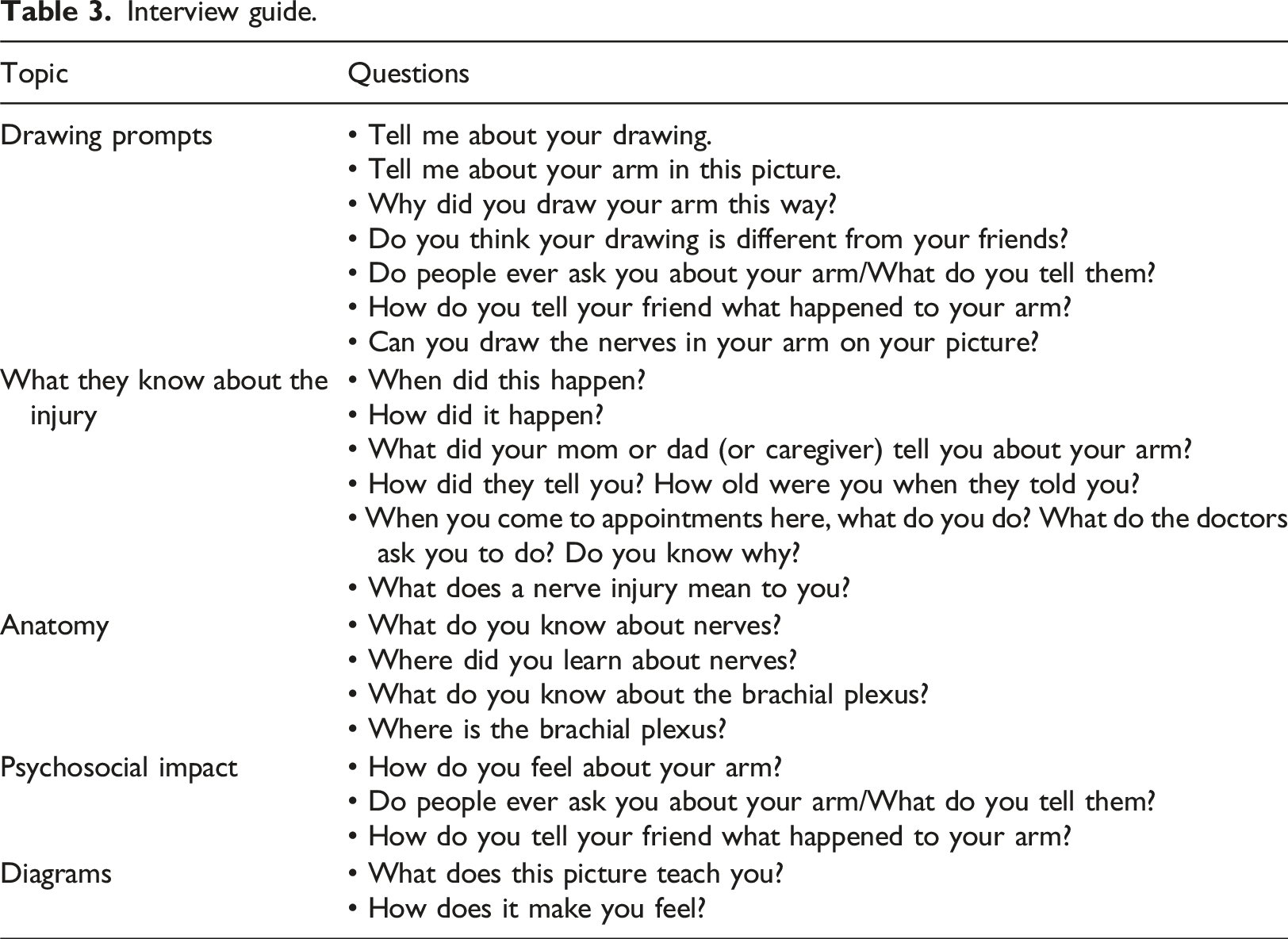
Caregiver interviews lasted approximately 1 hour. Caregiver interviews were framed to gather the caregiver’s perspective of their child’s understanding of BPBI and followed the same open-ended approach using a predetermined interview guide (Supplementary Material).
Data analysis
Each interview was transcribed and uploaded to NVivo 12 (QSR International Pty Ltd, 2018). Data were analyzed as outlined by Braun and Clarke’s (2006) six phases of thematic analysis. Initially, first authors engaged in independent repeated reading/listening and made preliminary notes to identify emerging codes in the child interview and debriefing session transcripts, alongside fieldnotes. To maintain trustworthiness, the researchers independently generated initial codes for several transcripts then came together to revise the codebook until consistency was reached. Initial codes were then organized into meaningful groups and analyzed to generate broader categories or themes. Next, the drawings were thematically analyzed as a data set in relation to the interviews. Following, the caregiver interview transcripts were independently coded by the researchers and integrated into the collaborative codebook. Emerging themes were reviewed against the interview coded extracts and then the entire data set to generate a thematic map. Themes were then defined and named as the overall story of the analysis was refined. During the final phase, meaningful extracts were selected, and findings were related back to the research question and existing literature (Clarke’s (2006)). Saturation was achieved when the researchers (four graduate students and PI) agreed that there was a redundancy of concepts in the data. This was an iterative process of constant comparison of the emerging ideas and themes from individual transcripts with the larger data set to integrate or confirm its uniqueness (Bowen, 2008). In representing these data, all participants were given pseudonyms that were linked to their participant identification code.
Rigor was maintained in several ways. The first authors kept a reflexive research journal to build awareness of their assumptions and potential biases. Researchers also continuously discussed all stages of the research process with the PI and engaged in reflexivity together, along with the pair of graduate students who interviewed the caregivers. Triangulation was applied through the use of multiple methods of data collection including observations, interviews with children/caregivers, debriefing after interviews, drawings, and fieldnotes (Miles et al., 2014). Having multiple investigators and consulting with the investigators of the parallel study also offered different perspectives on the phenomenon of interest. An audit trail was maintained to document the research process and monitor methodological and theoretical decisions.
Findings
The transcripts of eight sets of child, caregiver, and child–caregiver dyad interviews were analyzed alongside fieldnotes and eight children’s self-portraits. The analysis of participants’ understanding of their BPBI derived from the interpretation of drawings and interviews were grouped into three main themes and two subthemes: (1) Knowing versus Living: (i) medical knowledge and (ii) lived experiences, (2) Readiness to Learn, and (3) Looking Forward. These themes are discussed below alongside quotes that are denoted with pseudonyms.
Knowing versus living
By immersing ourselves in the narratives of the children and their caregivers, the intersection of our assumptions as clinicians and their lived reality regarding what it means to understand the medical diagnosis of BPBI became apparent. This theme elucidates the insights that contrast the role of children’s medical knowledge and their lived experiences in understanding their BPBI.
Medical knowledge
In the context of understanding the anatomical nature of their BPBI and its sequelae, children reported receiving medical knowledge from their parents, clinicians from SickKids, school, or the Internet. Aligning with the developmental age represented, gaps and diversity in children’s medical knowledge were identified. Older children and teenagers (>8 years) knew that nerves help with movement and were related to the brain. In reference to the term brachial plexus, some teenagers knew what it meant, others recognized the term but knew nothing further about the term, and some had never heard of it. Comparatively, younger children (6–8 years) had less understanding of the medical context of their BPBI. Nerves are “when you’re angry or upset,” Quinn explained.
Misunderstandings about BPBI were also expressed, but irrespective of age. Nico (age 11 years) shared how the “the green stuff,” referring to his nerves, while pointing to the veins in his forearm, was damaged at birth which caused his affected arm not to grow, “as fast as the other arm.” With further probing about his knowledge of nerves, he added, “Blood, I think it’s for blood.” Similarly, Kai, tried to appease with medical terms, but was uncertain and inaccurate: “I think it’s something that broke in my shoulder ... I don’t want to say cells, I don’t think cells is the right word ... it can’t really connect with ... my bones ... or whatever, so it doesn’t really register what I want it to do?” Kai
Misunderstandings of medical terminology and structure and function of the brachial plexus were common. Yet, the need and desire to impart understanding of BPBI using medical terminology was expressed by caregivers. Nico’s mother stated: “If anyone asks, he will just tell them what the injury is called - brachial plexus injury ...” Consequently, his confusion with medical terms were unknown to her. The educational diagrams presented to the children that illustrated where nerves are located and how they were injured at birth (see AboutKidsHealth website: Brachial Plexus Injury) also created confusion. Irrespective of age, most children were unable to relate the diagrams to their own bodies or to their BPBI. This was demonstrated by use of third person language when describing the nerves or the baby in the diagram, as if it were a science lesson.
One thing that appeared certain was that children understood that their injury occurred during birth. Their responses about how their BPBI happened seemed to be a regurgitation of their parents’ explanation to them. Quinn described why her left arm is different than her right arm: “Cause when I was a baby, [the doctor] had to pull my left arm to get me out.” Concurrently, in a separate neighboring office, her mother described how she explained BPBI: “Mommy had difficulty giving birth with you and so the doctors had to do what they needed … you suffered in a sense because … some of your brachial plexus nerves were damaged.” Leila
This “birth story” had common references to being “stuck” and that damage occurred to the nerves. There were occasional references to being a large baby and the doctor’s role in the injury.
All children answered medical questions related to their BPBI when asked directly, but their responses were short and succinct, varied in accuracy and depth, and appeared disconnected from their personal experiences. In contrast, how their injury affects their daily life was clearly prioritized in the children’s description of their understanding of their BPBI.
Lived experiences
Narratives around physical functioning were prioritized in the expression of ideas from all interviewees. Caregivers communicated how functional situations were often the catalysts to the occasional, but naturally occurring BPBI-related conversations between parent and child. Both parties shared that functional difficulties were expressed as the initial context that children understood their BPBI. At age six, Amir noticed pain, discomfort, and negative impacts on his engagement in activities related to his BPBI. Amir’s father explained that BPBI is raised by Amir in the context of this functional limitations and how he is unable to do the things they ask of him. Similarly, Kai described how motor impairments and pain interfered with his ability to do things: “I couldn’t hold the hockey stick properly and that would bother me, and it would kind of hurt too ... I went to Laser Quest, and holding the gun was hard. And, it hurt.” Kai
Children expressed their knowledge and understanding of their BPBI through the negative impacts experienced when participating in various activities including hockey, football, basketball, gym class, rock climbing, running, doing their hair, putting on jewelry, and typing.
The functional impact of BPBI also interacted with social impacts of having a physical impairment in their arm. Gabe (age 11 years) explained how his peers notice that he’s in pain and ask, “Is your arm hurting?” which would lead to the need to disclose information about his arm. As a visual attribute, the physical difference in the affected limb could lead to discredited stigma, a trait that is clearly seen by others and considered undesirable or unfavorable which can set the individual apart and may lead to perceived or actual negative social interactions (Goffman, 1963). Many children received unwanted attention regarding the appearance of their arm. They were frequently asked about the difference between their arms or splints they wore when they were young. Maya expressed that she often wore baggy clothing or long sleeves in an attempt to hide that her affected limb is shorter, and her mom shared the impact the visible nature of the BPBI has on her daughter’s self-image, as seen by her discomfort in her body: “Even if we were walking and I try to hold her hand, she won’t let me. She’s very self-conscious. I don’t know if she’s embarrassed because her right arm is smaller than her left arm, but she doesn't allow anyone to touch her hand.” Keira
In their lives, discredited stigma experienced by Maya also affected her mother and these feelings may have also negatively affect her psychological well-being (Bos, 2013). Unwanted attention because of their BPBI brought increased awareness of their arm differences; demonstrating an interaction between the visible nature of BPBI and the social impacts of BPBI.
Of the children interviewed, Theo more readily shared how social impacts of BPBI affects his self-concept, as demonstrated by his internalization of feeling different: “I’m always thinking about it. Not even talking to anyone, nobody’s around me, I’m adjusting my shirt on this side of my body and trying to make it look more normal.” Theo
Further, of self-portraits drawn, Theo, was also the only teen who drew his affected arm differently and explained that the asymmetry of his arms is a key attribute of his appearance. He expressed that he thinks of his arm often and feels self-conscious about it. In contrast, the other teenagers, Kai and Zoe, chose not to draw their arms differently and expressed that they do not like to think about it, or that they wanted to draw it like a “normal person.”
Collectively, children expressed various social implications brought by their BPBI, including comparison to peers and social exclusion that brought a range of strong emotional responses including sadness, exasperation, embarrassment, anger, resentfulness, frustration, indifference, annoyance, discomfort, and helplessness. At school entry, children expressed beginning to compare themselves to their peers and recognizing the difference in the appearance and function of their affected arm. Kai recalled how his viewpoint changed: “When I was two years old, I would be dribbling a basketball and older people would look at me like ‘oh, it’s a little baby is dribbling a basketball!’ and [then] I went to school and all of a sudden, I was like, wait, I’m not doing this the same way everyone else is. And now people are calling me out.” Kai
Children also recalled times when they sat out of gym class or had to do activities differently from their peers and how this was perceived negatively. Zoe reflected: “In my drama class, they looked at me and when I told them [about my BPBI], they were like, “oh I thought you were lazy!” I don’t want people to think I'm lazy and I just don’t want to move my arm up.” Zoe
To emotionally cope with their impairments, some children bargained with their diagnosis. Theo stated, “at least it’s better than being born with no hand,” or, “at least I’m not blind.”
Overall, in contrast to knowledge shared regarding the anatomical nature of their injury, the depth expressed to explicate the physical, social, and emotional consequences of BPBI demonstrated that the lived reality of children with BPBI is how their diagnosis is understood.
Readiness to learn
Children often discussed major milestones in the development of their understanding of BPBI. Teenagers and their parents reflected back and recognized how developmental maturity influenced the process of understanding BPBI. Zoe’s mom stated, “When she was five or six years old and she goes, ‘why can't I do the monkey bars?', I'm not going to go and draw a diagram of the nerves and all the stuff.” Aria
The importance of developmental readiness to understand medical terminology and the context of BPBI was expressed. Nico’s mom shared, “When they’re younger, you don’t really want to go into details about how babies are born.” Now that Nico is 11 years old, she remarked that he would know that “it happened at birth and ... he knows it’s connected to the nerve.”
The collective voice of the children and caregivers elucidated understanding regarding the general milestones in children’s understanding of BPBI (Figure 1). Around 4–5 years old, children noticed their arm felt different. This coincided with the age children first enter school and when they began comparing the appearance and function of their arm with their peers. During this time, children had a very shallow understanding of their arm; certain children remember explaining to their peers why their arm was “broken.” Developmental age: Timeline of understanding.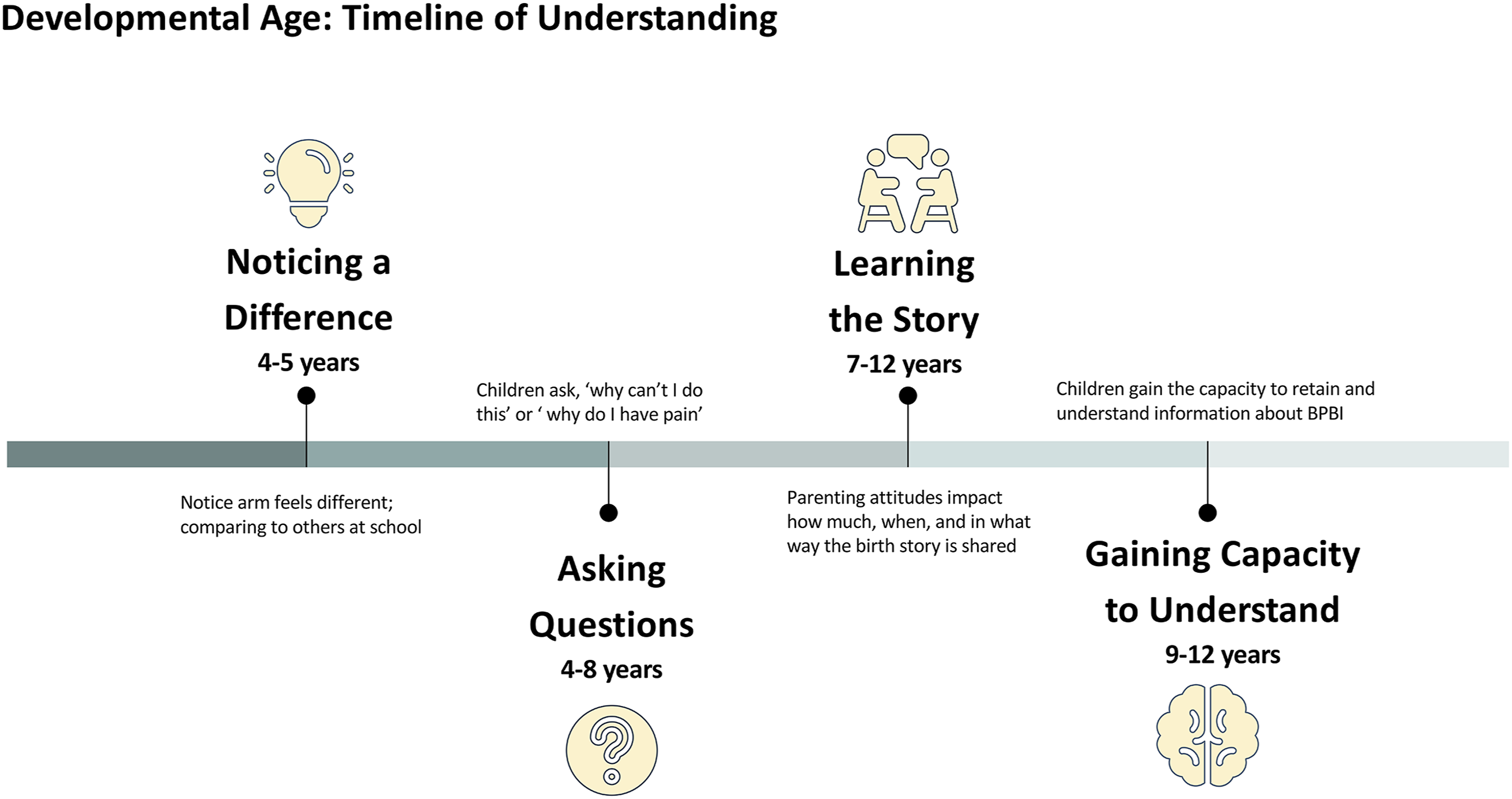
Arising after 4 years of age, children typically began asking their parents questions about the function of their affected limb. Often, these inquires arose in search of answers about physical observations about BPBI or discomfort in the limb. Zoe reflected back, “I would ask my mom a lot about what happened ... about the scars and the surgery.” While Gabe and his mother recalled the contexts of their early discussions: “I remember it hurting sometimes and I asked them why, and then they told me.” Similarly, his mother spoke of when and how their conversations about BPBI arose: “Really, it’s only when he has a few complaints about the arm, or he’ll ask questions...it hasn't been often.” Kate
Between 7 and 12 years, caregivers typically expressed spending time explaining to their children how their injury occurred or shared the story of their birth. Nico describes how he was much younger when he noticed the difference in his arm, but it was not until 7 or 8 years of age that his mom “told me the story.” When reflecting back, teenagers noticed an increase in their capacity to retain and understand medical information beyond a basic explanation after 8 years of age. This increased capacity also appeared to correspond with the age that children learn about the nervous system in school. Zoe’s mom explained: “At school when they learned the nerve system and stuff, this is my opportunity to go, ‘you know what, you have five nerves...’ She learned more about her nerves in school.” Aria
Children’s emotional readiness/acceptance was a precursor to being able to talk about their BPBI, having a desire to learn, or ability to process information. Theo’s reflections regarding his experience of readiness with searching BPBI on the Internet: “I haven’t, which is really weird because I like to learn things. I have barely any knowledge about this thing that’s so inherent to me and my whole life, I haven’t gone into it. And I don’t know why. I don’t know if it’s because, I’m scared of what I’ll find? [I think about it] all the time, every night I’m in my bed like, ‘I could literally research this and find out what’s wrong with my arm.’ But I never do it. And I don’t know why.” Theo
Once readiness was attained, having sufficient background knowledge made seeking and receiving information less overwhelming. This gave children the power to search for information independently should they wish to. For example, Zoe shared the importance of the moment she learned the name of her injury, as it enabled her to seek out information on the Internet independently.
Looking forward
BPBI encompasses a wide spectrum of sequelae, leading to many uncertainties surrounding prognosis and future outlook (Buterbaugh and Shah, 2016). Since rapid progression in motor recovery occurs during infancy and toddlerhood, parents experience hopes for improvements during these early years. At school-age, neurological recovery plateaus and surgical/rehabilitation interventions may be offered to help with physical function. Therefore, clinicians face the challenge of setting functional goals or expectations with children and caregivers that may still hope for full motor recovery, while other families accept the long-term impairment, but have many questions about how their BPBI will impact them now and in the future.
Kai’s story surrounding disappointment with functional improvements in his arm provides insight on how these feelings may affect how information is received. When an infant is diagnosed with BPBI, doctors track nerve recovery through frequent routine clinic visits, looking for movement and gathering information to make informed decisions about surgery. This medical and curative nature of their early care later transforms into prevention, maintenance, and adaption. However, for Kai, the ideas of fixing and curing persisted. Kai recalled coming to clinic visits as a young child, “As a kid, I thought it was to like fix my arm, I thought it would get fixed.” He recounted that his therapist jotted down numbers during his clinic visits and described his assessments: “... do this ... do that with your arm. And they touch it; say a bunch of fancy words.” Then, he described the hopelessness he felt in understanding the meaning of the assessment data collected and the disappointment of the lack of a cure: “I do wish it would get better. But all surgery or physio options won’t get me to having two normal functioning arms ... [surgery] gives me one thing but then I'm like what’s the catch, it’s going to limit something else.” Kai
Kai’s narrative illustrates that for some children with BPBI, hoping to be “fixed” or for a cure can be troubling, and how information is conveyed about their progress or BPBI can lead to feelings of defeat and hopelessness.
Discussion
This study explores children’s understanding of their BPBI, a medical condition that affects their health outcomes and psychosocial well-being. These findings highlight that a child’s lived experience is their understanding. The current biomedical approach emphasizes medical knowledge; by shifting this emphasis towards children’s lived experiences, and explaining information in this context, children may be more able to internalize this information as it relates to their own body. In this way, a better understanding of their medical diagnosis and prognosis may be achieved. Second, the experiences of the participants in this study illustrate the impact of mental wellbeing on children’s ability to receive medical information, as participants’ emotional readiness was found to be a precursor to their learning.
Children are active seekers of their medical information and want to be informed enough to contribute to shared medical decisions (Coyne, 2006). A main focus on children’s understanding of information has been on health care provider attitudes and communication skills (Coyne, 2008; Moore and Kirk, 2010). While numerous studies have emphasized the approach and value to educating children about their illness, literature on the content that provides the best avenue to education is unknown. In this study, participants understood their injury through their lived experiences, which helps to inform what educational content would be meaningful to children with BPBI.
The experiences of the participants in this study also illustrate the impact of mental wellbeing on children’s ability to receive medical information, as participants’ emotional readiness was found to be a precursor to their learning. Teenagers in this study had the developmental capacity to understand their BPBI; however, if they were not emotionally ready to accept the injury, they appeared more reluctant or unable to receive or process information. As such, what appears important is for health care providers to evaluate the child’s emotional readiness by attending to their psychosocial and emotional adjustment in order to determine if it is affecting their ability to receive health information (Gallo et al., 2008).
Strengths and limitations
The findings provide a rich description of participants’ experiences with, and understanding of, their BPBI, although they do not intend to explain lived experiences of all children with this diagnosis. The use of in-depth interviewing with children, caregivers, and child-caregiver dyads, demonstrated that children can provide a unique perspective on their condition that can be meaningfully applied to practice such as in family-centered information delivery approaches.
Several limitations of this study are noted. Although maximal variation sampling informed our understanding of the impact of developmental age, older children provided richer descriptions of their experiences. Further studies would benefit from a targeted sample of older children and teenagers. It is also important to note that timelines outlined in Figure 1 are only reflective of the participants in our sample, not the population as a whole. We also encountered challenges with applying arts-based data collection methods. In our experience, drawing a self-portrait did not elicit rich or deep responses from younger participants to elucidate ideas around body-image and self-concept related to the BPBI. Arts-based methods seemed more developmentally appropriate for older children, as they were able to explain their thought process behind their drawings in the context of their BPBI.
Implications for practice
Facilitation of change towards a more evidence-based, family-centered model of information delivery is supported by the study findings. It is important for clinicians to take a strengths-based approach, focusing on client-centered goals (King, 2009). Their diagnosis/health condition can then be explained within the context of achieving their goals, taking into consideration each child’s unique lived experience in education delivery (Rushforth, 1999). Children’s needs and concerns change as they grow up (Rushforth, 1999), suggesting that ongoing conversations about the functional and psychosocial aspects of BPBI are needed, despite being in a physical health setting. Health care providers can facilitate children’s understanding of their diagnosis and better prepare them for the mental and physical health consequences of BPBI and the emotional responses they bring.
Conclusion
The findings of this study highlight a gap in current information delivery approaches, as they poorly address the primary concerns of children, namely, their lived experiences of BPBI, or the diagnosis as they know it. Mental health and emotional readiness were found to be a precursor for fostering a deeper understanding of BPBI. For many participants in this study, mental health and emotional readiness acted as a barrier to this understanding, suggesting that these factors are poorly addressed in current information delivery and practice approaches and highlighting the importance of addressing this more adequately in the future.
Supplemental Material
Supplemental Material - Elucidating children’s understanding of brachial plexus birth injury
Supplemental Material for Elucidating children’s understanding of brachial plexus birth injury by Michelle Goldsand, Kathleen Lai, Kristen Davidge, and Emily S. Ho in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The authors of this study verify that the medical research was conducted according to the World Medical Association Declaration of Helsinki. The methods section met the relevant ethical consideration of the local institutional Research Ethics Board and informed consent was obtained from all participants of the study. Informed consent to participate in the quality assurance project was received from participants verbally and documented by the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.