
Abstract
Mental health problems are highly prevalent in childhood and adolescence and may be associated with nutritional intake. It has recently been shown that a high percentage of infants and children consume large amounts of free sugars. In this paper, we analyse the relationship between free sugar consumption at 12 and 30 months and the risk of developing psychological problems at 30 months in a community sample of 86 children evaluated longitudinally. Socio-family and anthropometric data, and the amount of free sugars consumed were collected at both ages. At 30 months, the Child Behavior Checklist 1.5–5 was administered to parents and an interview was conducted to identify psychological disorders in accordance with DC: 0–3’s classification. We report a relationship between high free sugar consumption at 30 months and the concurrent presence of sleeping problems, ADHD and anxiety symptoms. However, no significant association was observed between free sugar consumption at 12 months and the subsequent development of psychological problems. Early detection of emotional and behavioural manifestations and high sugar consumption in children may help to prevent the persistence of psychological problems.
Introduction
Mental health problems, many of which appear at early stages of development, affect 10–20% of children and adolescents (Kieling et al., 2011). These problems may appear early, persist throughout life and become a risk factor for other problems in the long term (Forbes et al., 2017; Lahey et al., 2014). Early childhood (from birth to 3 years) is an important period in which children gradually acquire basic skills that enable them to interact effectively with their environment (McCoy et al., 2016). Although this is a period of vulnerability to adverse factors, it is also one in which synaptic plasticity enables our brain to modify its organisation and functions, and provide the best responses (Belsky, 2005; Hensch, 2004; Shonkoff et al., 2012). Earlier studies have reported that dietary intake and nutritional status are environmental factors behind early brain development and children’s mental health (Wachs et al., 2014). However, although the effects of nutritional aspects on overweight and metabolic disorders have been extensively investigated, their effects on development and mental health require further study (Adan et al., 2019).
Both globally and in westernised environments, the quality of the diet consumed by children and adolescents has deteriorated in recent years (Arcila-Agudelo et al., 2019; Dunford et al., 2020), while the incidence of psychopathological disorders in these age groups has increased (Danielson et al., 2021; Vasileva et al., 2021). Poor nutrition in the early stages of life can affect growth and development not only physiologically but also in terms of cognitive functions and optimal brain development, which increases the risk of psychological problems (Cusick and Georgieff, 2016; Wachs et al., 2014).
Previous research has focused not only on general dietary quality but also on the link between the consumption of certain macronutrients or dietary patterns and mental health problems (Aparicio et al., 2017a; Dimov et al., 2021). Some studies have indicated that certain nutritional deficiencies or unhealthy dietary patterns – particularly the high consumption of free sugars (FS) – may be associated with a risk of developing attention deficit hyperactivity disorder (ADHD) (Rios-Hernandez et al., 2017; Woo et al., 2014; Yu et al., 2016).
Sugary beverages (the consumption of which has increased significantly and one of the main sources of FS intake) can stimulate insulin secretion and boost reactive hypoglycaemia, functions which are related to manifestations of ADHD (Dykman and Dykman, 1998). Moreover, certain neurobiological mechanisms explain how the consumption of obesogenic factors such as FS or saturated fatty acids is associated with early memory problems and dysfunctions in the hippocampus, which can compromise a child’s learning ability (Noble and Kanoski, 2016). In addition to influencing cognitive function, a high sugar diet has also been associated with emotional disorders such as depression and anxiety (Aparicio et al., 2017b; Kim et al., 2018). A recent review by Jacques et al. (2019) concluded that negative emotions can increase sugar consumption, just as high sugar consumption can alter emotion processing. In this context, some studies have related a lack of emotional regulation strategies with childhood obesity (Aparicio et al., 2016), while others have reported that conduct problems are related to an increase in sugar intake. Jansen et al. (2017), for example, observed that baseline-externalising behaviour was positively associated with added sugar intake at follow-up among boys. It is important, therefore, to identify those nutritional risk factors that may compromise mental health at a young age, and ensure that psychological problems are detected early.
Aim
To investigate the relationship between FS intake at 12 and 30 months (m) and psychological problems at 30 m in a community sample of children. We hypothesise that a high consumption of sugars (above the level recommended by World Health Organization (WHO), that is, >10% of total energy intake) at 12 m, irrespective of total energy and other covariates, may be a risk factor in the development of psychological problems at 30m.
Material and methods
Study design and population
All subjects were participants in the DeFensas project (Jardí et al., 2018, 2019), a longitudinal study in which children of mothers recruited during pregnancy were assessed from birth to 30 m during visits made 48–72 h after birth and at 6 m, 12 m and 30 m. A total of 86 children completed the study up to 30 m. Of these, 57 (32 boys and 25 girls) participated in psychological assessment in all study phases and nutritional assessment at 12 m, while 78 (39 boys and 39 girls) participated in psychological assessment in all study phases and nutritional assessment at 30 m. Mothers were included as participants if they had been pregnant for no more than 11 weeks at the study’s beginning and they had to be over 18 years old. Mothers were excluded if they suffered from an illness such as type II diabetes, Crohn’s disease or celiac disease, had a multiple pregnancy, or intended to give birth in a different hospital. Infants were included if they were Caucasian, born as from week 37 with a weight ≥2500 grams, and from a family that understood Catalan or Spanish. Infants were excluded if they had birth defects or suffered from hypothyroidism, immunodeficiency, or any disease related to iron metabolism or that required intensive care. According to Granmo, a program for calculating sample sizes (Version 7.12) (Marrugat, 2012), with an alpha risk of 0.05 and a beta risk of less than 0.2 in a one-sided contrast, 66 subjects were needed in the first group and 13 in the second group to detect a difference equal to or greater than 15 units. Common standard deviation was assumed to be 20.
Procedure
This project was approved by the Ethics Committee of the Sant Joan University Hospital in Reus (Tarragona, Spain) and all families provided their informed consent. The sample was recruited in the hospital between 2006 and 2009.
In the various phases, the clinical and obstetric data of mothers and babies were recorded, as were their sociodemographic, anthropometric, nutritional and psychopathological data. Paediatricians and nutritionists collected anthropometric and feeding data, while psychologists conducted psychological assessment. All professionals were trained in collecting the project variables.
Psychological assessment
Child Behavior Checklist 1, 5–5 (CBCL 1, 5–5) (Achenbach and Rescorla, 2000) is a 110-item questionnaire that is completed by parents and used to assess the presence of emotional and behavioural problems. Items are rated on a 3-point Likert scale (0 = not true, 1 = somewhat or sometimes true, and 2 = very true or often true). It has seven subscales: that is, emotional reactivity, anxiety/depression, somatic complaints, withdrawal (internalised problems), aggressive behaviour and attention problems (externalised problems), and sleep problems. The sum of the scores on the subscales provides a total score. This questionnaire also provides five DSM-oriented scales: depression, anxiety, autism spectrum disorders, attention deficit hyperactivity disorders and opposition defiant disorder. For this study, each parent answered the questionnaire separately during the 30 m visit and the average T-score of their responses was used (in seven cases, however, only the mother’s response could be used). These scores were classified as normal, borderline or clinical in accordance with the questionnaire’s standardised criteria. For statistical analyses, we considered borderline + clinical as a psychological problem. The internal consistency of the Spanish version is 0.65–0.86 (De la Osa et al., 2016). In this study, CBCL showed a Cronbach’s alpha of .96 for mothers and .91 for father ones.
General Health Questionnaire (GHQ-28) (Goldberg and Hillier, 1979) is a 28-item self-administered instrument for determining general health status. Items are rated on a 4-point Likert scale (0 = better than usual, 1 = same as usual, 2 = worse than usual, 3 = much worse than usual). It has four scales, and the Spanish version has acceptable psychometric properties (Lobo et al., 1986). GHQ-28 was completed by mothers and fathers during the 30m visit.
An ad-hoc interview based on the Diagnostic Classification of Mental Health and Developmental Disorders of Infancy and Early Childhood (Zero To Three, 2005) was administered to the parents to assess anxiety, sleep, regulation and adaptive and eating disorders.
Socioeconomic status (SES) (Hollingshead, 2011) was determined using the Hollingshead index. Both parents were asked about their level of studies (divided into seven categories – from having completed primary school to having completed higher education) and occupation (divided into nine categories – from having an unskilled job to having a highly qualified job). Accordingly, three categories of SES were established (i.e. low, medium and high).
Anthropometric assessment
At 12 m and 30 m visits, weight and length were recorded. At 12 m, weight was measured using a SECA electronic weighing machine (Vogel and Halke GmbH & Co, Hamburg, Germany) to an accuracy of 5 grams and length was measured using a length rod to an accuracy of 0.1 cm (model PE-RILB -STND). At 30 m, weight and length were measured using an electronic weighing machine with a stadiometer (SECA 764). Child growth indicators – that is, weight for length at 12 m and weight for length at 30 m z-score – were measured using the LMS method (Cole et al., 1995; De Onis et al., 2006).
Infant feeding assessment
A 24-h dietary recall was administered via interviews with parents at 12 and 30 m visits. Amounts of food and drink were expressed in grams/person/day. The REGAL food composition table ‘Répertoire général des Aliments’ (Favier et al., 1997) and the Spanish food composition table ‘Mataix Verdú’ (Mataix Verdú, 2009) were used to calculate nutrient intake. A percentage of total energy provided by macronutrients was calculated. From simple carbohydrates, the following two variables were created: natural sugars, that is, sugars from fruits (whole fruit pieces), vegetables, milk and cereals such as bread, flour, rice and pasta; and FS, that is, from sugary dairy desserts, sugary beverages (natural and commercial fruit juices and soft drinks), sugary breakfast cereals, cookies, pastries, chocolate, sugar and honey, in accordance with 2015 WHO’s definition of FS (monosaccharides and disaccharides added to foods and beverages by manufacturers, cooks and consumers, as well as sugars naturally present in honey, syrups, fruit juices and fruit juice concentrates).
Statistical analyses
All the analyses were performed using SPSS Software (IBM Corp. Released, 2017. IBM SPSS Statistics for Windows, Version 25.0). The data were first tested for normality using the Kolmogorov–Smirnov test and, when the distribution was not normal, the U-Mann–Whitney test for independent samples.
To analyse the relationship between percentage of energy from FS (at 12 m and 30 m) as the independent variable and psychological problems at 30 m as the dependent variable, we created a regression model adjusted for the following covariates: sex (1: boy; 2: girl), socioeconomic level (total score), weight-for-length z-score at 30m (total score), amount of energy at 12 m or 30 m (total score, kcal), breastfeeding (total score, months), smoking in pregnancy (0: non-smoker; 1: smoker) and scores on mother’s and father’s GHQ-28 questionnaires (total scores). Specifically, dependent variables for each model were T scores of CBCL subscales 1.5–5, on the one hand, and variables of the diagnoses made with DC: 0–3 interview on the other (0 = no diagnosis and 1 = diagnosis). In the first case, we performed multiple linear regressions, while in the second case we performed logistic regressions by introducing the independent variables with the ENTER method. The level of significance was set at p < .05.
Results
Mean weight at birth of infants was 3304.9 grams (SD = 429.5), mean gestational age was 39.6 weeks (SD = 1.3) and average Apgar score at 10 min was 10 (SD = 0.1). Ninety-three percent of families were of a mid-to-high socioeconomic level. Supplementary Table 1 shows more descriptive data of this study sample (of mothers and their infants). Note that at 12 m of age 40.4% of infants consumed >10% of their total energy intake as FS, as did 50% of the infants at 30m of age. Moreover, at 30 m 26.7% had internalising problems (borderline+clinical) and 36.0% had externalising problems (borderline+clinical).
Bivariate analysis of the relationship between the amount of free sugars consumed at 12 and 30 months (in grams), and CBCL scores 1.5–5 by ranges (normal and borderline/clinical) and DC diagnoses: 0–3.
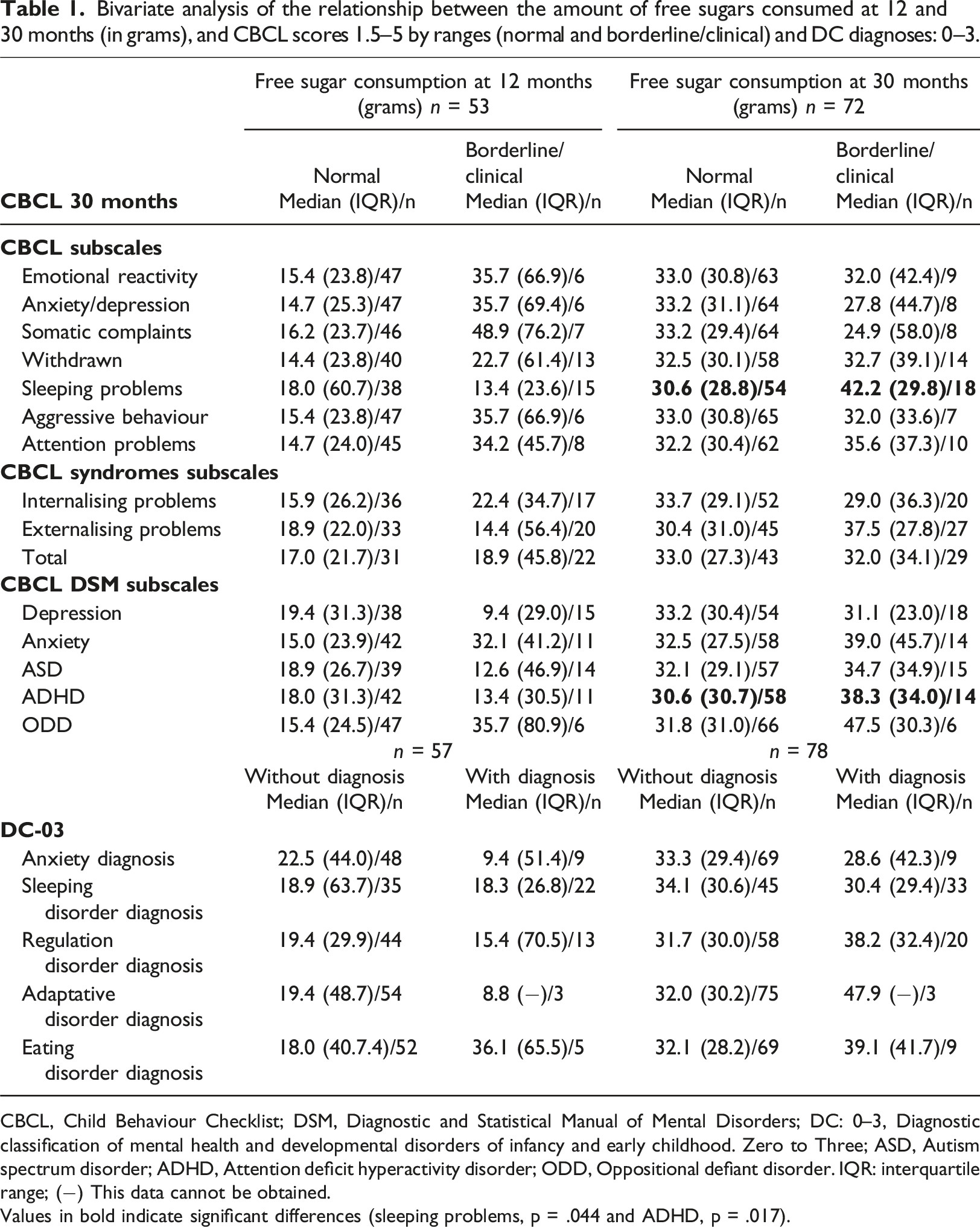
CBCL, Child Behaviour Checklist; DSM, Diagnostic and Statistical Manual of Mental Disorders; DC: 0–3, Diagnostic classification of mental health and developmental disorders of infancy and early childhood. Zero to Three; ASD, Autism spectrum disorder; ADHD, Attention deficit hyperactivity disorder; ODD, Oppositional defiant disorder. IQR: interquartile range; (−) This data cannot be obtained.
Values in bold indicate significant differences (sleeping problems, p = .044 and ADHD, p = .017).
Relationship between the percentage of energy provided by free sugars (at 12 and 30 months) and the presence of psychological problems at 30 months of age adjusted for several covariates.
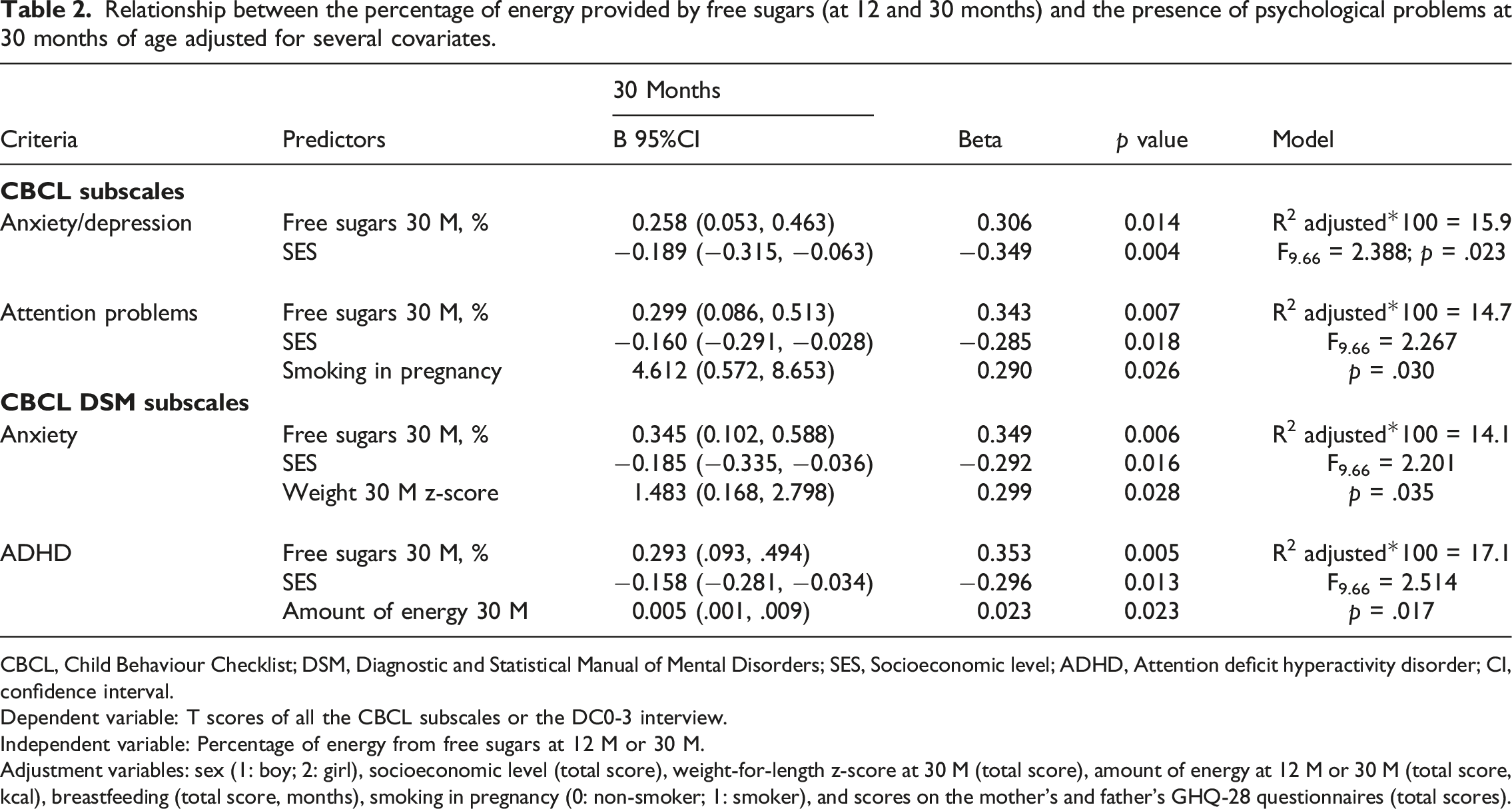
CBCL, Child Behaviour Checklist; DSM, Diagnostic and Statistical Manual of Mental Disorders; SES, Socioeconomic level; ADHD, Attention deficit hyperactivity disorder; CI, confidence interval.
Dependent variable: T scores of all the CBCL subscales or the DC0-3 interview.
Independent variable: Percentage of energy from free sugars at 12 M or 30 M.
Adjustment variables: sex (1: boy; 2: girl), socioeconomic level (total score), weight-for-length z-score at 30 M (total score), amount of energy at 12 M or 30 M (total score, kcal), breastfeeding (total score, months), smoking in pregnancy (0: non-smoker; 1: smoker), and scores on the mother’s and father’s GHQ-28 questionnaires (total scores).
Discussion
This study’s aim was to evaluate the effect of FS intake on the mental health of a community sample of children assessed at various periods from birth to 30 m. To our knowledge, no studies have assessed the consequences of high FS consumption on mental health in early childhood.
Results did not support our hypothesis since FS consumption at 12 months was not a risk factor for the subsequent development of psychopathological problems at 30 m. In general, at 12 m complementary feeding is not fully established, and this may be the reason why we do not observe this longitudinal relationship. However, our data support a relationship between high FS consumption at 30 m and concurrent sleeping problems, ADHD and emotional symptoms. In this context, we found that participants generally consumed high amounts of FS in their diet, and that between 40% (12 m) and 50% (30 m) of participants consumed over 10% more than WHO recommendations.
An unhealthy diet in the early stages of life could alter brain function in children and adolescents (Georgieff et al., 2018; Noble and Kanoski, 2016). Many highly prevalent behaviour disorders in childhood (such as ADHD) are influenced by dietary factors (Del-Ponte et al., 2019; Millichap and Yee, 2012). In this regard, bivariate analyses indicate that participants at 30 m whose scores on the ADHD subscale were within the borderline/clinical range had consumed a significantly higher amount of FS than participants without risk scores. Although some studies suggest that diet in the early stages of life may be related to the aetiology of ADHD (Del-Ponte et al., 2019; Rios-Hernandez et al., 2017), evidence is still weak and further longitudinal studies are required. Overall, our results seem to be in line with those of previous studies that found that obese children who consumed a poor quality diet performed worse on tasks related to executive functions and attention (Cagigal et al., 2019; Khan et al., 2015). As far as physiological aspects are concerned, sugar may be related to hyperactivity since it quickly passes into the bloodstream (glucose levels are increased) and adrenaline is released. In turn, changes in adrenaline levels are associated with symptoms such as anxiety and attention problems (Jones et al., 1995; Paglia et al., 2019).
In line with the results of bivariate analyses, regressions showed that a high consumption of FS at 30 m, a low socioeconomic environment and a high total amount of energy at 30 m were associated with ADHD symptoms (17.1%) and a high percentage of energy from FS together with a low socioeconomic level and to smoke during pregnancy, was associated with attention problems (14.7%). As we have mentioned above, evidence is still weak and, although some studies suggest there may be a positive association between the consumption of sugar-rich foods and ADHD (Azadbakht and Esmaillzadeh, 2012; Rios-Hernandez et al., 2017), others have found no association (Kim and Chang, 2011; Peacock et al., 2011). Note also that few studies have been conducted with preschool samples. However, in this context, a cross-sectional study conducted in a Chinese city with a sample of children (3–6 years old) suggested that a dietary pattern with a higher consumption of processed foods and unhealthy snacks was related to a higher prevalence of ADHD symptoms, unlike studies in which participants adhered to a dietary pattern with a high consumption of vegetables (Yan et al., 2018). Accordingly, it has been observed that children and adolescents with ADHD symptoms have a less healthy lifestyle, low adherence to the Mediterranean diet, high levels of inactivity, and a greater tendency to obesity (Cagigal et al., 2019; San Mauro Martin et al., 2019; Tong et al., 2016). On the other hand, the relationship between maternal smoking in pregnancy and attention problems in children found in the current study are in line with data from the meta-analyses of He et al. (2020).
The findings also showed that at 30 m a high FS consumption was cross-sectionally associated with emotional symptoms (anxiety and depression) and sleeping problems. Our results, therefore, suggest that either these kinds of manifestation lead children to consume high amounts of sugars, or that the consumption of high amounts of sugars leads to these kinds of manifestation. Regressions indicated that consuming a high percentage of FS, being from a disadvantaged socioeconomic family and weighing more at 30 m, explains between 14.1% and 15.9% of anxious and depressive symptoms at that age. However, we did not find that children from disadvantaged families consume significantly more FS than those from families with higher socioeconomic levels. In contrast, Bolt-Evensen et al. (2018) found that participants from high socioeconomic environments generally consumed less sugar-sweetened beverages. In line with our results, a multi-ethnic cohort study of adults conducted in Amsterdam concluded that a dietary pattern high in saturated fat and sugar was related to high levels of depressive symptoms and a depressed mood (Vermeulen et al., 2017). Previous evidence indicates that consuming sucrose (common sugar) activates the mesocortilimbic system, which leads to alterations in processing emotions and behaviour. Furthermore, a high consumption of sugars can reduce the ability to control impulses and resist consuming products high in fats and sugars that produce immediate reward (Jacques et al., 2019). Consuming high amounts of sucrose during critical periods of brain development is known to be linked to the aetiology of depression or anxiety (Baker et al., 2017; Gueye et al., 2018).
In reference to the result indicating a relationship between free sugar consumption and sleep problems, several studies found similar results (Blunden et al., 2011; Pelsser et al., 2011; Peuhkuri et al., 2012). In this regard, some studies revealed that higher soft drink consumption is associated with less sleep in adolescents (Al-Haifi et al., 2016) and children (Franckle et al., 2015; Kjeldsen et al., 2014). These beverages, specially caffeinated ones, are known to affect the physiological circadian rhythm and sleep-related features (Godos et al., 2021). In their study of overweight children aged 2–9 years, Hunsberger et al. (2015) found that short sleep was associated with less total sugar intake at midday, but higher intake in the evening. In contrast, Watson et al. (2018) suggested that although a high proportion of children consumed more than the recommended amount of daily total sugar, total sugar consumption was not related to behavioural or sleep problems. It should be pointed out, however, that children in that sample were older (8–12 years) than the participants in our study. Thus, as was concluded in a recent meta-analysis, several studies indicate that a higher intake of processed and FS rich foods is associated with worse quality of sleep in children, adolescents and adults, but further studies are needed to corroborate these findings. Despite a certain consistency observed between studies, many had cross-sectional designs so no conclusions as to causal relation can be drawn (Godos et al., 2021).
Study limitations and strengths
The main limitation of our study is sample size, which may be responsible for the lack of significant findings. However, the longitudinal design provides a unique insight into the relationship between free sugar intake and psychopathological problems in early childhood because most previous studies were conducted among older children, adolescents or adults. Besides, many of them had cross-sectional designs, so no conclusions as to cause can be drawn. Additionally, many studies consider that sugar consumption means consuming table sugar or focus only on sugary drinks, whereas it is important to consider the WHO’s definition of free sugar and also their recommendations. On the other hand, another limitation we should point out is that we do not have specific information on whether either parent has a mental health diagnosis. However, we did have information about parent’s mental health status from the GHQ-28 and we used it as an adjustment variable in the analyses.
Implications for practice
FS consumption is much higher than that recommended in 12 m or 30 m infants. Thus, our results reveal that it is important to inform and raise awareness in society of the need to follow a healthy and balanced diet from the beginning of life. This issue is important for both physical health and psychological health. Much more information on this important issue needs to be made available to both families and professionals. This study may help to improve existing dietary guidelines that can be implemented by primary care professionals such as paediatricians and paediatric nurses.
Schools can also play a leading role as early as nursery levels. Children spend many hours in schools, so it is important to offer healthy food and a balanced diet supervised by nutritionists. The importance of a healthy lifestyle should be part of a child’s education so that they can learn to discriminate between those foods that are healthy and those that are not.
Conclusion
Free sugars intake is associated with the presence of psychological problems early in life. Specifically, a high free sugar consumption at 30 months was related with sleeping problems, and ADHD and anxiety symptoms. It is important to ensure that families follow dietary recommendations so that the nutritional status of their children is optimal and they are in good physical and mental health.
Emotional and behavioural problems, and high FS consumption in sensitive growth and development periods need to be detected early to prevent physiological and psychological problems.
Supplemental Material
Supplemental Material - Association between free sugars intake and early psychopathological problems
Supplemental Material for Association between free sugars intake and early psychopathological problems by Núria Voltas, Cristina Jardíb, Carmen Hernández-Martínez, Victoria Arija and Josefa Canalsa in Journal of Child Health Care
Footnotes
Acknowledgements
We would like to thank the children and their parents for participating in this study as well as the entire DeFensas project research team.
Author contributions
Núria Voltas: participated in the data collection, planning the manuscript, searched the articles to write the manuscript, conducted and interpreted the results and wrote the manuscript.
Cristina Jardí: participated in the data collection and in the planning of the manuscript.
Carmen Hernández: participated in the data collection and in the planning of the manuscript.
Victoria Arija: designed the study, planned and directed the execution of the study, contributed in the search of articles, interpreted the results, and supervised and reviewed all the manuscript.
Josefa Canals: designed the study, planned and directed the execution of the study, contributed in the search of articles, interpreted the results, and supervised and reviewed all the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The project was approved by the Ethics Committee of the Sant Joan University Hospital in Reus (Tarragona, Spain) and all families provided their informed consent. The sample was recruited at the Sant Joan University Hospital between 2006 and 2009.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.