
Abstract
Paediatric chronic health conditions are associated with poorer psychological wellbeing and quality of life for children and families. This study investigated differences in child and parent/family quality of life between families of children with asthma only, eczema only, or both asthma and eczema, and tested predictors of child and parent/family quality of life. A convenience sample of 106 families completed parent-report measures of child and parent/family quality of life, child emotional and behavioural difficulties, parent adjustment and parenting practices. Between-groups ANOVAs indicated no differences for child quality of life, whereas parent/family quality of life was worse for those with eczema only compared to asthma only. Multiple linear regression revealed that child emotional difficulties predicted worse child quality of life, whereas worse parent adjustment, child emotional difficulties and eczema only (compared to both asthma and eczema) predicted worse parent quality of life. Results suggest that families of children with eczema may be at particular risk for impaired parent/family quality of life. Interventions that take a family-centred approach to improving child and parent adjustment should be investigated as an adjunct to medical treatment to reduce the impact of chronic health conditions on quality of life for children and families.
Chronic childhood illnesses are a global concern, many can persist through life and have implications for children’s and families’ lives. Asthma and eczema are the most common chronic paediatric illnesses worldwide (Dharmage et al., 2019; Hay et al., 2014). The comorbidity between these conditions is high (Pols et al., 2015), with a meta-analysis indicating a 2.16 times greater risk of developing asthma for individuals with eczema (Li et al., 2022).
A substantial body of evidence suggests that having a chronic illness such as asthma or eczema is associated with diminished psychological wellbeing for both affected children and their parents, which in turn plays a role in illness severity and illness management. Children with these conditions experience significantly higher levels of internalising problems such as depression and anxiety (Budu-Aggrey et al., 2021; Hammer-Helmich et al., 2016; Huang et al., 2021) and externalising problems such as hyperactivity and inattention, conduct problems and peer problems (Hammer-Helmich et al., 2016; Huang et al., 2021; Keller et al., 2021).
Although there is considerable literature on the psychosocial factors associated with chronic childhood illnesses, by and large this research has focused on children diagnosed with a single illness. Early studies found that children’s psychological wellbeing, along with other health problems, worsened with every additional chronic illness (Newacheck and Stoddard, 1994; Newacheck et al., 1991). More recent studies suggest that multiple (cf. single) chronic health conditions are associated with elevated levels of depression in children (Wolock et al., 2020), increased school absenteeism (Patel et al., 2015) and greater family financial burden (Zhong et al., 2015). However, at this stage there is limited evidence about effects of comorbid childhood health conditions, interrelationships with condition type and severity and relationships with psychological wellbeing of parents and children.
Elevated levels of parenting stress are common among parents of children with a chronic health condition (Pinquart, 2018), including asthma (Foronda et al., 2020) and eczema (Yang et al., 2019). Moore et al. (2006) found that the depression scores of parents of children with eczema were two times higher than those of parents of children with asthma; however, this effect disappeared after controlling for parental sleep disturbances. Parental stress and depression have been implicated in child disease management and progression (Chan et al., 2018; Magnus et al., 2017; Wood et al., 2018). Hence, the evidence clearly illustrates that parent psychological wellbeing is lower compared to healthy children and is implicated in child health.
Children with asthma and eczema and their families have consistently been found to have poorer quality of life (Chamlin and Chren, 2010; Foronda et al., 2020; Lozier et al., 2019; Matterne et al., 2011; Meltzer and Booster, 2016; Yang et al., 2019). Parent quality of life is correlated with children’s internalising and externalising problems (Vila et al., 2003) and associated with disease management (Cano-Garcinuño et al., 2016). Importantly, research has shown that improvements in caregiver quality of life are correlated with better asthma control in children (Sheikh et al., 2017; Stelmach et al., 2012).
In summary, the existing research demonstrates that high levels of comorbidity and chronicity mean that asthma and eczema can have a great impact on multiple domains of a child’s and a family’s life. The quality of life of affected children and their families also appears to be significantly poorer than that of healthy children and their families. Quality of life is associated with other psychosocial factors in bidirectional, complex ways and clearer understanding of these interrelationships is important to intervention development and service provision. To our knowledge, studies to date have not examined interrelationships between quality of life and parent and child psychological wellbeing in children affected by both asthma and eczema, and any differences in these interrelationships between families of children with asthma only, eczema only, or both asthma and eczema are as yet unknown.
Aims
This study aimed to investigate differences in child and family quality of life between three groups: children with asthma only, children with eczema only and children with both conditions. We hypothesised that families of children with both asthma and eczema would report poorer child and parent/family quality of life compared to families of children with asthma or eczema alone. Further, we aimed to identify the domains of child and family quality of life most affected by each condition, investigate associations between child and family quality of life and several covariates (sociodemographic variables, health condition variables, child emotional and behavioural problems, parent adjustment and use of ineffective parenting practices) and to explore predictors of child and family quality of life across these three groups.
Methods
This study used a cross-sectional study design, drawing on baseline (pre-intervention) data from a randomised controlled trial of a brief parenting intervention for parents of children with asthma and/or eczema (Morawska et al., 2016, 2017). Parents were recruited via advertisements for the parenting intervention study placed in school newsletters and displayed in paediatric hospital emergency and outpatient departments and medical practice waiting areas in the metropolitan region of Brisbane, Australia, from June 2011 to June 2013. To be eligible to participate, parents needed to be (a) the primary caregiver for a 2- to 10-year-old child with a diagnosis of asthma and/or eczema, and (b) concerned about their child’s behaviour or emotions and/or illness management (yes/no). Parents were ineligible if (a) their child was diagnosed with a developmental disorder or disability, (b) parents were currently receiving professional assistance for their child’s behaviour problems or (c) parents were currently receiving psychological help or counselling for themselves.
Measures
Parents completed the following parent-report questionnaire measures online or in hardcopy (pen-and-paper) format, depending on parent preference.
Sociodemographic information
The 15-item Family Background Questionnaire (Sanders and Morawska, 2010) was used to collect sociodemographic information, including child and parent age and sex; parent relationship to child; parents' relationship status, education and employment; family type and composition; and the family’s ability to meet essential expenses.
Child quality of life
The Pediatric Quality of Life Inventory Version 4.0 (PedsQL 4.0; Varni et al., 2001) Generic Core Scales is a parent proxy measure of children’s quality of life. The appropriate parent-report measure for toddlers (ages 2–4), young children (ages 5–7), or children (ages 8–12) was administered depending on child age. Each scale assesses child quality of life across four dimensions: (1) Physical functioning (8 items), (2) Emotional functioning (5 items), (3) Social functioning (5 items) and (4) School functioning (3 items for toddlers who attend childcare, 5 items for young children and children). Items are rated on a 5-point scale on which 0 indicates ‘Never’ and 4 indicates ‘Almost Always’. The 5-point scale is transformed into a 0 to 100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0), where higher scores indicate better quality of life, and items are averaged to generate a total score (0–100). The PedsQL had good internal consistency in this study for toddlers (α = .87), young children (α = .90) and children (α = .82).
Family quality of life
The PedsQL Family Impact Module Version 2.0 (PedsQL-FIM; Varni et al., 2004) is a parent-report measure that assesses how much a child’s health is impacting on various aspects of parent and family quality of life and has eight dimensions. Four dimensions assess parent quality of life in terms of Physical functioning (6 items), Emotional functioning (5 items), Social functioning (4 items) and Cognitive functioning (5 items). Two dimensions assess parents’ difficulties with Communication (3 items) and Worry (5 items). Two dimensions relate to impact on the family’s Daily activities (3 items) and Family relationships (5 items). Items are rated on a 5-point scale on which 0 indicates ‘Never’ and 4 indicates ‘Almost Always’. The 5-point scale is transformed into a 0 to 100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0), where higher scores indicate better parent or family quality of life, and all items are averaged to generate a total Family Impact score (0–100). The PedsQL-FIM had high internal consistency in this study (α = .95).
Child behavioural difficulties
The Eyberg Child Behavior Inventory (ECBI; Eyberg and Pincus, 1999) is a 36-item scale assessing parental perceptions of disruptive child behaviours. Only the Intensity scale, assessing the frequency of disruptive behaviours, was used in this study. Items are rated on a 7-point scale ranging from 1 (never) to 7 (always). Item scores are summed to generate a total score (36–252) and higher scores indicate higher levels of child behavioural difficulties. The Intensity scale showed high internal consistency (α = .92) in this sample.
Child emotional difficulties
The Emotional Maladjustment subscale of the Child Adjustment and Parent Efficacy Scale (CAPES; Morawska et al., 2014) is a 4-item measure of child emotional adjustment. Emotional maladjustment items are rated on a 4-point scale ranging from 0 (not true of my child at all) to 3 (true of my child very much, or most of the time). Item scores are summed to generate an Emotional Maladjustment score (0–12), and higher scores indicate higher levels of child emotional adjustment difficulties. The Emotional Maladjustment subscale showed satisfactory internal consistency (α = .66) in this sample.
Parent adjustment
The Depression Anxiety Stress Scales–21 (DASS; Lovibond and Lovibond, 1995) is a 21-item measure of depression, anxiety and stress symptoms in adults. Items are rated on a 4-point scale ranging from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). Item scores are summed and then doubled to generate a total score that is directly comparable to the full 42-item scale, and higher scores indicate higher levels of distress. The scale showed high internal consistency (α = .94) in this study.
Parenting practices
The Parenting Scale (PS; Arnold et al., 1993) is a 30-item self-report questionnaire assessing use of ineffective parenting practices across the subscales of Laxness (permissive discipline), Overreactivity (authoritarian discipline, displays of anger) and Verbosity (overly long reprimands or reliance on talking). Items are rated on 7-point response scales with more effective and less effective anchors. Item scores are averaged to generate a total score, and higher scores indicate greater use of ineffective parenting practices. There was good internal consistency for the total score (α = .83) which was used in analyses.
Procedure
The University of Queensland Behavioural and Social Sciences Ethical Review Committee (2010001427) and the Royal Children’s Hospital (HREC/11/QRCH/86) and Mater Health Services Human Research Ethics Committees approved the study. Interested parents contacted the research team and were provided with detailed written study information and completed a telephone screening interview with the study coordinator to assess for eligibility. Eligible parents choosing to participate consented online and were directed to a secure online survey site (Qualtrics) to complete an online questionnaire, which took a mean 38 min (SD = 16) to complete. Hardcopy questionnaires and reply-paid envelopes were mailed to parents on request. Parents also consented for researchers to contact their child’s doctor (family doctor, paediatrician or dermatologist/respiratory physician) to confirm their diagnosis and collect information about currently prescribed asthma and eczema treatment.
Statistical analyses
All analyses were performed using IBM SPSS 25. A significance level of p < .05 was used. Descriptive statistics were used to summarise sample characteristics. Individual variable data distribution was examined to ensure parametric test assumptions were met. Between-groups ANOVAs were used to examine differences in child and parent/family quality of life between three groups (children with asthma only, eczema only and both conditions). Pearson’s and point biserial correlations examined relationships between child and family quality of life and demographic and child health condition variables, child and parent adjustment and use of ineffective parenting practices.
Hierarchical multiple regression analyses were used to test whether demographic and child health variables, child and parent adjustment and parenting indicators explained significant proportions of variation in child and family quality of life. Selection of variables for inclusion in the models was guided by an initial evaluation of the zero-order correlations between the variables. For analysis purposes, the child’s age at diagnosis was recoded into two categories (early diagnosis = 1 versus later diagnosis = 0) using a median split. Asthma diagnosis by 2 years of age (58.5%, n = 24) and/or eczema diagnosis by 6 months of age (63.3%, n = 50) was considered to represent an early diagnosis, and this variable was used in regression analyses to examine the effect of relatively early development of a chronic health condition on child and parent/family quality of life. Similarly, data on children’s treatment regimens (collected from treating doctors) was used to create a binary treatment intensity variable (high intensity = 1 versus low intensity = 0). Children who were not prescribed any corticosteroid or preventer medication for their asthma or eczema were considered to have low treatment intensity compared to those prescribed at least one corticosteroid or preventer medication.
Overall, 0.67% of data were missing, and the pattern of missing data was completely random. Pairwise deletion was used for bivariate analyses and listwise deletion was used for regression models. Analyses of standardised residuals and casewise diagnostics showed that there were no multivariate outliers and no cases exerting undue influence on the regression models.
Results
Participant characteristics
Demographic and clinical characteristics of participants by condition.
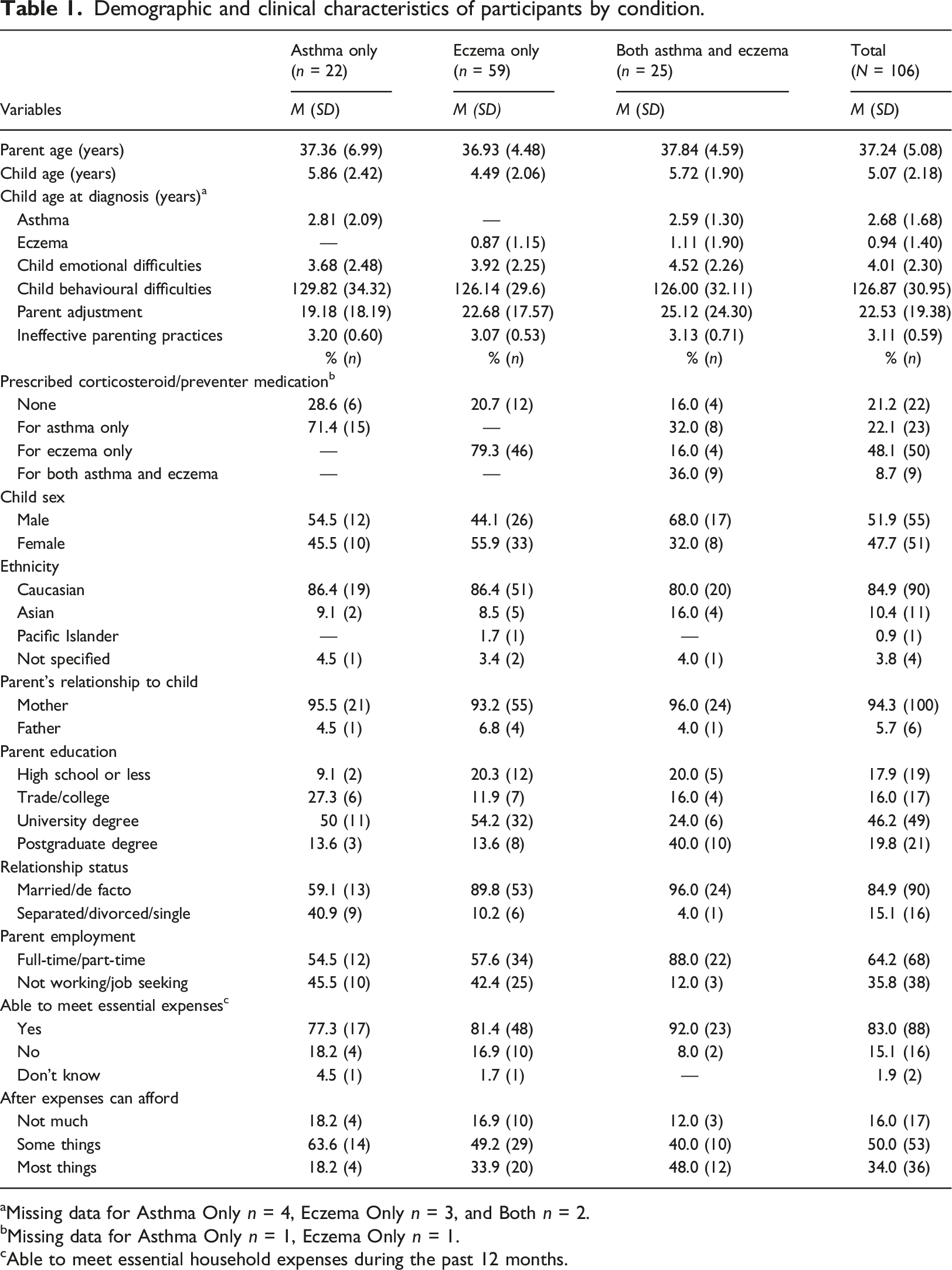
aMissing data for Asthma Only n = 4, Eczema Only n = 3, and Both n = 2.
bMissing data for Asthma Only n = 1, Eczema Only n = 1.
cAble to meet essential household expenses during the past 12 months.
Descriptive statistics for demographic and health condition variables and measures of child and parent adjustment and use of ineffective parenting practices are presented in Table 1. The vast majority of families of children with both asthma and eczema (92.0%, n = 23) reported meeting their essential expenses over the past 12 months, compared to 81.4% (n = 48) and 77.3% (n = 17) of families of children with eczema or asthma only. Similarly, almost half of families of children with both asthma and eczema were able to purchase most things they really wanted after meeting their essential expenses, compared to 33.9% (n = 20) and 18.2% (n = 4) of families of children with eczema or asthma only. A higher proportion of parents of children with asthma only were sole parents compared to families of children with eczema only or both asthma and eczema. There were no notable differences between the groups for other demographic variables.
Scale descriptives for child and parent/family quality of life dimensions by condition, and ANOVAs testing differences between groups (N = 106).
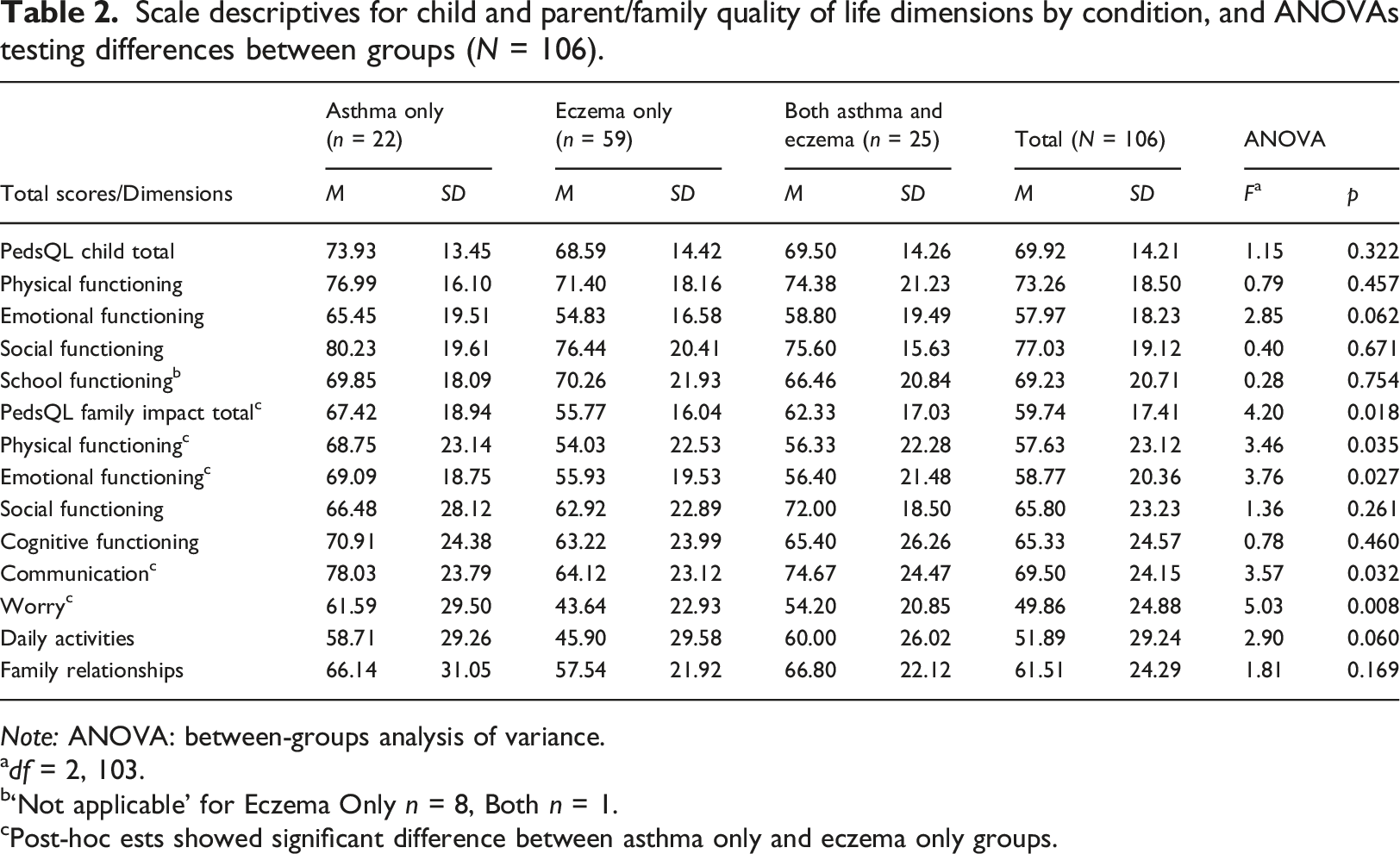
Note: ANOVA: between-groups analysis of variance.
adf = 2, 103.
b‘Not applicable’ for Eczema Only n = 8, Both n = 1.
cPost-hoc ests showed significant difference between asthma only and eczema only groups.
Between-groups ANOVAs indicated that mean child quality of life scores (dimension scores and total scores) did not differ between groups (see Table 2). On the other hand, parent/family quality of life scores showed significant differences across groups in terms of the total score as well as dimension scores for parent physical functioning, parent emotional functioning, communication and worry. Post-hoc analyses showed that families in the eczema only group scored significantly worse than families in the asthma only group in terms of total family impact (Mean difference = −11.66, 95% confidence interval (CI) [−21.61, −1.70]), parent physical functioning (Mean difference = −14.72, 95% CI [−28.03, −1.41]), parent emotional functioning (Mean difference = −13.16, 95% CI [−24.85, −1.47]), communication (Mean difference = −13.91, 95% CI [−27.79, −0.02]) and worry (Mean difference = −17.95, 95% CI [−32.07, −3.83]), indicating greater impact on multiple dimensions of parent/family quality of life. Scores for parents/families of children with both conditions did not differ significantly from those in the asthma only group or those in the eczema only group.
Predictors of child and parent/family quality of life
Pearson’s and point biserial correlations between child, parent, and family variables, and child and parent/family quality of life.
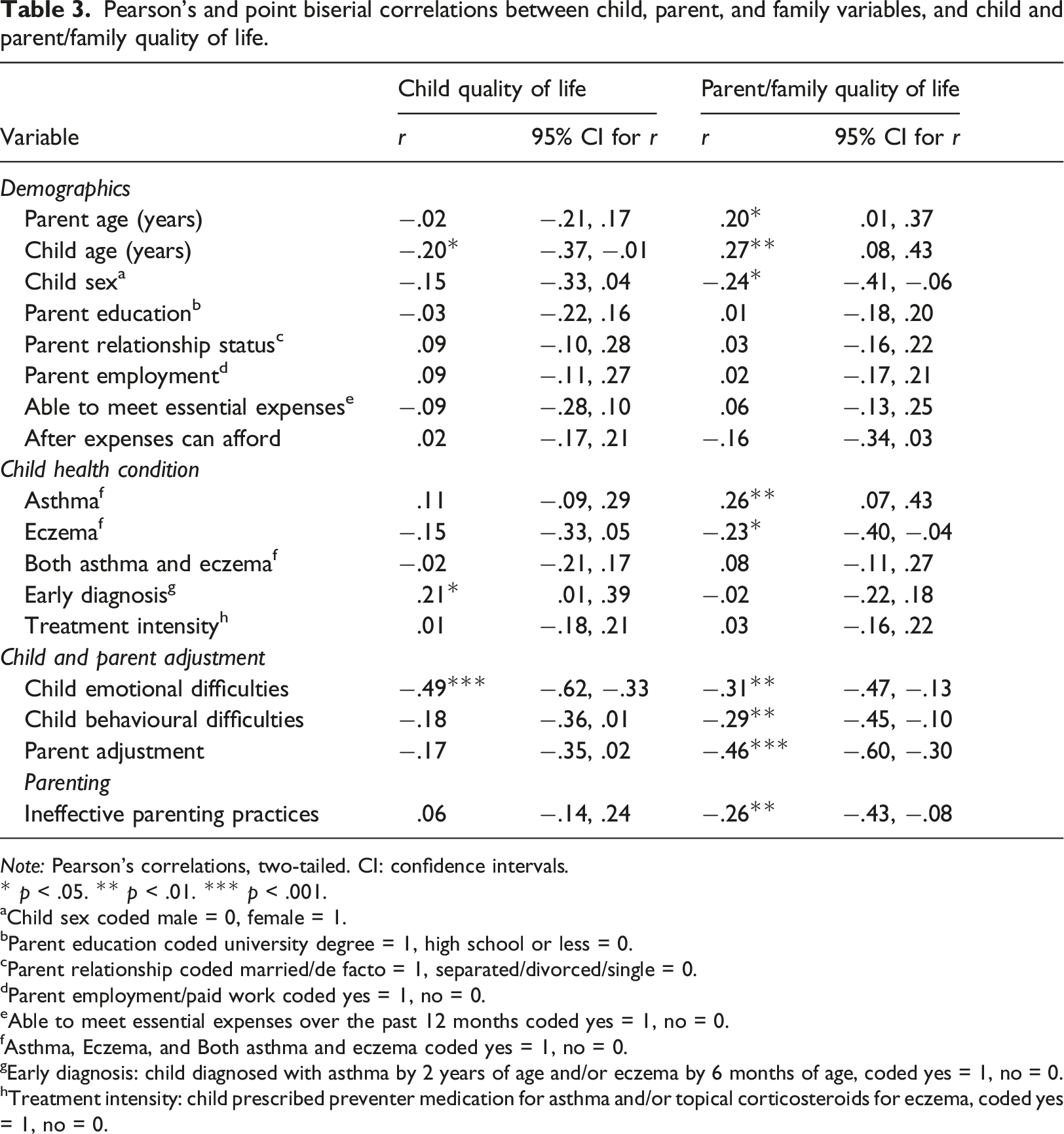
Note: Pearson’s correlations, two-tailed. CI: confidence intervals.
* p < .05. ** p < .01. *** p < .001.
aChild sex coded male = 0, female = 1.
bParent education coded university degree = 1, high school or less = 0.
cParent relationship coded married/de facto = 1, separated/divorced/single = 0.
dParent employment/paid work coded yes = 1, no = 0.
eAble to meet essential expenses over the past 12 months coded yes = 1, no = 0.
fAsthma, Eczema, and Both asthma and eczema coded yes = 1, no = 0.
gEarly diagnosis: child diagnosed with asthma by 2 years of age and/or eczema by 6 months of age, coded yes = 1, no = 0.
hTreatment intensity: child prescribed preventer medication for asthma and/or topical corticosteroids for eczema, coded yes = 1, no = 0.
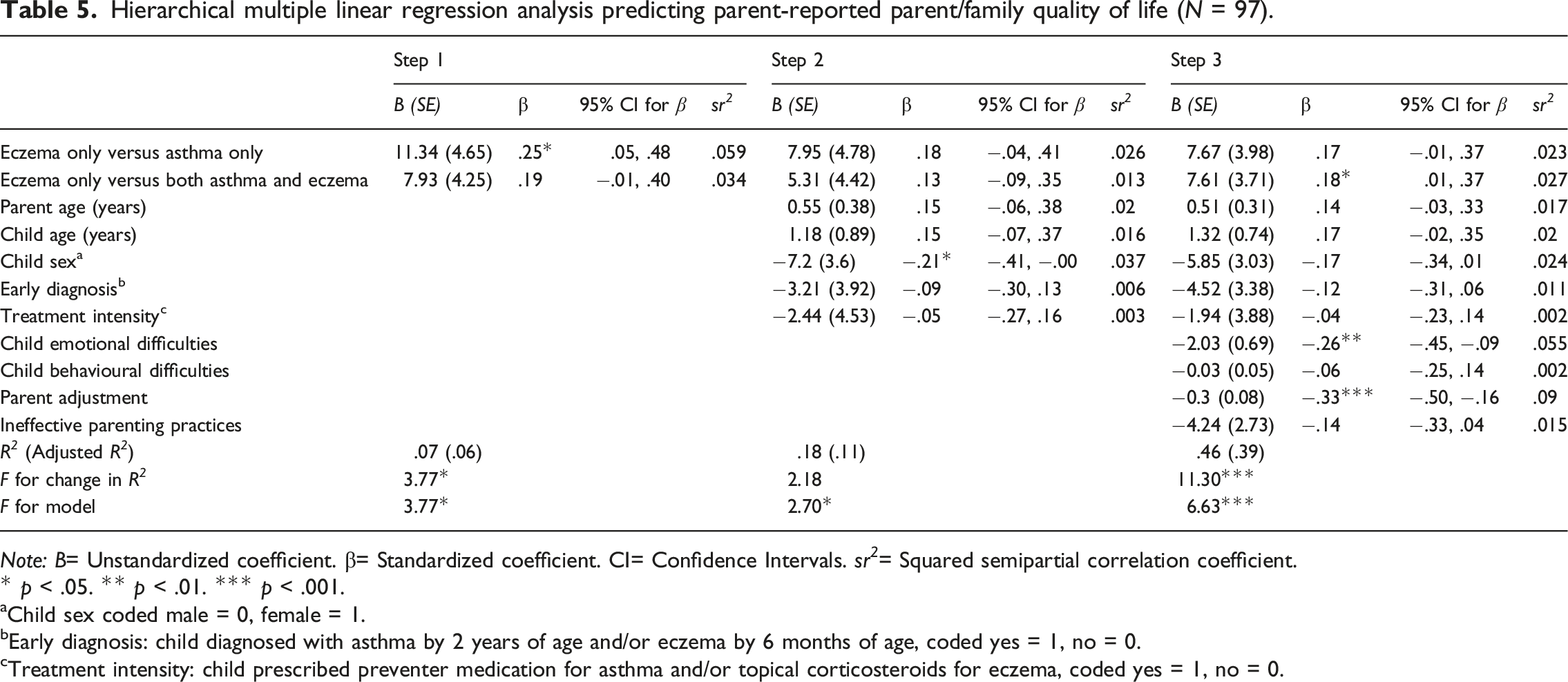
Hierarchical multiple regression analyses assessed the extent to which demographic and child health condition variables, child and parent adjustment, and parenting indicators explained variation in (1) child quality of life and (2) family quality of life. Considering the results of the between-group comparisons, the eczema only group was considered as a reference group and two dummy variables were entered into the equation in step 1: dummy 1 comparing the eczema only group (coded as 0) to the asthma only group (coded as 1), and dummy 2 comparing the eczema only group (coded as 0) to the asthma and eczema (both conditions) group (coded as 1). Child age, earlier diagnosis and treatment intensity were included in step 2, and child emotional and behavioural difficulties were included in step 3. For the model predicting family quality of life, parent age (r = .20, 95% CI [.01, .37]) and child sex (r = −.24, 95% CI [−.41, −.06]) were also included in step 2, and parent adjustment (r = −.46, 95% CI [−.60, −.30]) and use of ineffective parenting practices (r = −.26, 95% CI [−.43, −.08]) were also included in step 3 due to significant correlations with the outcome variable.
Hierarchical multiple linear regression analysis predicting parent-reported child quality of life (N = 97).
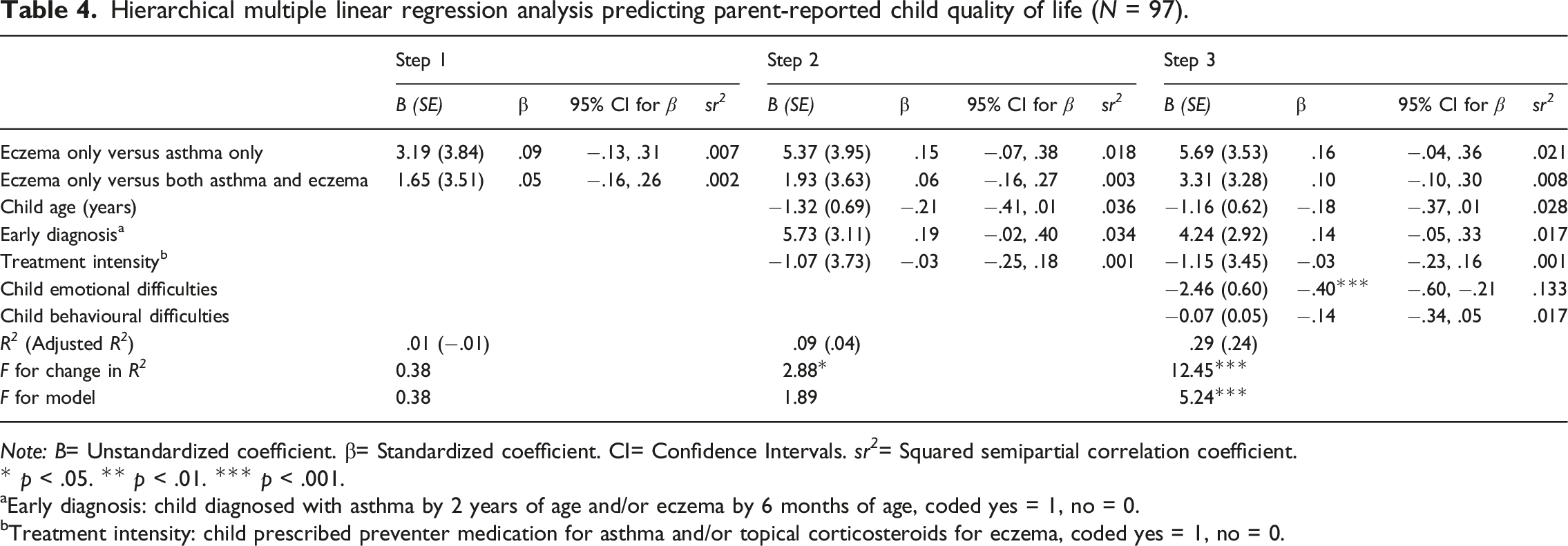
Note: B= Unstandardized coefficient. β= Standardized coefficient. CI= Confidence Intervals. sr 2 = Squared semipartial correlation coefficient.
* p < .05. ** p < .01. *** p < .001.
aEarly diagnosis: child diagnosed with asthma by 2 years of age and/or eczema by 6 months of age, coded yes = 1, no = 0.
bTreatment intensity: child prescribed preventer medication for asthma and/or topical corticosteroids for eczema, coded yes = 1, no = 0.
Hierarchical multiple linear regression analysis predicting parent-reported parent/family quality of life (N = 97).
Note: B= Unstandardized coefficient. β= Standardized coefficient. CI= Confidence Intervals. sr 2 = Squared semipartial correlation coefficient.
* p < .05. ** p < .01. *** p < .001.
aChild sex coded male = 0, female = 1.
bEarly diagnosis: child diagnosed with asthma by 2 years of age and/or eczema by 6 months of age, coded yes = 1, no = 0.
cTreatment intensity: child prescribed preventer medication for asthma and/or topical corticosteroids for eczema, coded yes = 1, no = 0.
Discussion
This study set out to examine relationships between child and parent/family quality of life and demographic and health condition variables, parent and child adjustment and parenting practices among families of children with asthma and/or eczema. We identified domains of child and parent/family quality of life most affected by each condition and found several unique predictors of child and parent/family quality of life. Although our results suggest no evidence of a cumulative effect of multiple health conditions on quality of life, the eczema only group did have significantly worse parent/family quality of life scores compared to the asthma only group. There was no difference between parent/family quality of life for the group with both asthma and eczema and either of the single-condition groups. At the most basic level, these results suggest that caring for a child with eczema has a greater impact on parent/family quality of life compared to asthma. This may reflect the high burden of caregiving reported by parents of children with eczema which includes time-consuming and distressing skin care regimens, sleep deprivation and restrictions on family activities (Chamlin and Chren, 2010; Moore et al., 2006).
The pattern of results for families of children with both asthma and eczema is harder to interpret and may be explained at least in part by subsample heterogeneity: some children had moderate-severe eczema but only mild asthma, whereas other children had more severe asthma but only mild eczema. Mean parent/family quality of life scores for this subsample fell between those of the single-condition groups and this may have resulted in no significant differences compared to either of the single-condition subsamples. In support of this notion, treatment intensity data revealed that a smaller proportion of children with both conditions were prescribed corticosteroid or preventer medication for their asthma (68.0%, n = 17) or eczema (52.0%, n = 13) compared to children with asthma only (71.4%, n = 15) or eczema only (79.3%, n = 46), suggesting greater heterogeneity in disease severity among families of children with both conditions.
Children’s emotional difficulties were the only significant predictor of child quality of life after controlling for health condition and other variables. These results are congruent with prior research identifying internalising symptoms, but not externalising symptoms, as an important predictor of quality of life for children in general (Stevanovic, 2013), as well as children with chronic health conditions (Stevanovic and Susic, 2013; Vila et al., 2003). This is particularly important considering the increased risk of internalising difficulties among children with chronic health conditions in general (Pinquart and Shen, 2011), and asthma and eczema in particular (Bussing et al., 1996; Vila et al., 2000; Yaghmaie et al., 2013). There is some evidence of a dose-dependent relationship between having multiple allergic diseases (e.g. asthma, eczema and allergic rhinitis) and increased risk of internalising problems (Nanda et al., 2016), and our results suggest that internalising difficulties were more important to children’s quality of life than the health condition/s they were diagnosed with.
Significant predictors of worse parent/family quality of life were poorer parent adjustment, child emotional difficulties and having eczema (but not asthma). These results are congruent with previous research identifying parental adjustment and children’s internalising difficulties (Toledano-Toledano et al., 2020; Vila et al., 2003) as predictors of worse quality of life among parents of children with chronic health conditions. Notably, the unadjusted bivariate relationship between eczema diagnosis and parents’ health-related quality of life persisted even after all other variables were accounted for in the linear regression model. This suggests that condition-specific factors such as the practical and emotional demands associated with caring for a child with eczema may contribute to variation in parents’ quality of life above and beyond what is explained by parent and child adjustment and the other variables examined in this study.
Although there is some degree of conceptual overlap between measures of parental adjustment and some parent quality of life domains, it is worth considering to what extent parents’ psychological wellbeing or distress may influence their responses to items within domains that are conceptually distinct from psychological functioning. There were statistically significant differences between groups for half of the parent/family quality of life domains. However, these differences were restricted to domains closely associated with parents’ personal psychological wellbeing – that is, physical functioning, emotional functioning, communication and worry – but not other domains of parent (i.e. cognitive functioning, social functioning) or family (daily activities, family relationships) functioning. There was no relationship between parents’ adjustment and their ratings of children’s quality of life. Overall, our data suggest that parent-report quality of life measures provide valuable information distinct from parental adjustment.
Limitations
Limitations are acknowledged. Data were collected at baseline in a randomised controlled trial of a parenting intervention for families of children with asthma and/or eczema between June 2011 to June 2013; since participating families all had concerns about their child emotions or behaviour and/or condition management, results may not be generalisable to the broader population. All psychosocial variables, including child quality of life, were measured using parent-report questionnaires. Use of proxy parent-report measures of children’s quality of life has inherent limitations in terms of differences between parental perceptions of children’s quality of life and the perspectives of children themselves. Studies examining relationships (agreement) between parent proxy- and child self-report have yielded inconsistent results that vary depending on the quality life measures used, the domains that were assessed and sample characteristics (Cox et al., 2019; Eiser and Morse, 2001). Regardless, quality of life is now considered a core outcome indicator in clinical trials for children with asthma (Sinha et al., 2012), eczema (Schmitt et al., 2015) and other chronic health conditions and use of proxy parent-report measures is still valuable, particularly when young age or other factors hinder children’s capacity to report for themselves.
Implications for practice
The importance of family-centred care in the paediatric health context is now well-established (Park et al., 2018), and there is a growing body of evidence to support the efficacy of family-based psychosocial interventions to improve chronic health condition management and child and family outcomes (Eccleston et al., 2015; Mitchell et al., 2020). Identifying factors that place families at increased risk of difficulties will help to inform intervention selection and service delivery. This study identifies child emotional symptoms and parent adjustment as key predictors of poorer child and parent/family quality of life among families of children with asthma and/or eczema, with families of children with eczema at particular risk of impaired quality of life. Multidisciplinary care approaches are needed to ensure that child and parent emotional health needs are addressed early and often to reduce impact on condition management and quality of life.
Conclusion
In conclusion, families of children with eczema only reported worse overall parent/family quality of life and greater impact on parents’ physical functioning, emotional functioning, communication and worry compared to families of children with asthma only. There was no evidence of a cumulative effect of having both asthma and eczema. Parent adjustment and children’s emotional difficulties were associated with worse parent/family quality of life, and child emotional difficulties were associated with worse parent-reported child quality of life. Interventions that take a family-centred approach to improving child and parent adjustment and parenting should be considered as an adjunct to medical treatment to reduce the impact of child chronic health conditions on the quality of life of children and their families.
Footnotes
Acknowledgements
Our sincere thanks to the families who participated in this study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Parenting and Family Support Centre is partly funded by royalties stemming from published resources of the Triple P – Positive Parenting Program, which is developed and owned by The University of Queensland (UQ). Royalties are also distributed to the Faculty of Health and Behavioural Sciences at UQ and contributory authors of published Triple P resources. Triple P International (TPI) Pty Ltd is a private company licensed by UQ, to publish and disseminate Triple P worldwide. The authors of this report have no share or ownership of TPI. Dr Morawska has received royalties from TPI. TPI had no involvement in the study design, collection, analysis or interpretation of data, or writing of this report. Dr Morawska is an employee at UQ. Dr Mitchell is an honorary research fellow at UQ. Drs Etel and Mitchell were employees at UQ at the time this research was conducted.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Research Council [grant number DP110102449]; and Children’s Hospital Foundation Early Career Fellowships [AEM; award ref. 50223, ECF0112020].