
Abstract
Repression has been linked to greater illness, somatic symptoms, and poorer physical health, both in adult and pediatric populations. The current study examined psychological and pain profiles of children with chronic pain who may under-report levels of psychological distress at a first interdisciplinary chronic pain assessment. Children and their caregiver completed measures of psychopathology and pain intensity, while clinicians rated their levels of disability. Based on self-report measures, children were classified as “repressors” (low anxiety/high social desirability) or as “true low anxious” (low anxiety/low social desirability). Groups were then compared on psychological and pain characteristics. Compared to children with true low anxiety, repressors reported lower levels of depressive and somatic symptoms but provided higher ratings on pain intensity, pain–unpleasantness, and self-oriented perfectionism. Caregivers of repressors rated their children as having higher levels of adaptability compared to caregivers of children in the true low anxious group. Groups did not differ on clinician-rated level of disability. Children classified as repressors exhibited different profiles than children classified as having true low anxiety on both psychological outcomes and pain characteristics. Repression may be an important factor to consider for those assessing and treating children with chronic pain.
The prevalence of chronic pain in children, defined as pain that lasts for more than 3 months, ranges from 11 to 38% (King et al., 2011). Chronic pain has been found to negatively impact many life domains including physical, emotional, and school attendance (Eccleston et al., 2004, 2008).
Given that psychological factors are known to contribute to and maintain chronic pain (Asmundson and Katz, 2009; Wojtowicz and Banez, 2015), clinical assessments of chronic pain often include administration of self-report questionnaires that assess emotional functioning. Indeed, there exist many well validated questionnaires to assess psychological distress in children (Reynolds, 2010). However, these questionnaires are primarily designed to detect psychopathology as denoted by scores in the distressed range of the continuum (Joiner et al., 1994). The validity of these self-report scales has been called into question for those who score in the healthy range of psychological functioning as scales may not differentiate between children who are truly psychologically healthy and those who minimize or suppress distress (Phipps and Steele, 2002). The possibility that some children may minimize emotional distress when using self-report formats (e.g., interviews or questionnaires) is problematic. Erroneously deeming a child as “functioning well” based on their report can have significant consequences for the child including reduced likelihood of referral to a specialist (e.g., mental health professional) and inadvertently missing psychological risk factors (e.g., coping by avoiding stressors), both of which may maintain a child’s pain and disability (Joiner et al., 1994; Myers, 2010; Shedler et al., 1993).
While children’s scores may be a genuine reflection of healthy psychological functioning, scores may also signal defensive processes, such as “socially desirable responding” (i.e., a tendency to minimize negative personality traits to portray a positive image to others; Helmes and Holden, 2003). In the handful of studies that have examined social desirability and chronic pain, social desirability has been found to influence self-report of psychological factors and pain characteristics in adult chronic pain patients (Haythornthwaite et al., 1991). For example, high levels of social desirability have been associated with lower levels of anxiety, but higher rates of disability and pain (Deshields et al., 1995). To date, only one study has been conducted to investigate the impact of social desirability on reporting of psychosocial factors and pain characteristics among children with chronic pain. Logan et al. (2008) showed that children with chronic pain who had higher levels of social desirability reported lower levels of depression and anxiety but that social desirability levels did not influence pain intensity or disability ratings. However, the authors of this study did not examine children who specifically may have under-reported their levels of distress based on socially desirable responding.
In comparison to research on social desirability, a more robust research literature investigating defensive responding exists on the phenomenon of repression (Myers, 2010). Repression has been most widely examined using Weinberger et al. (1979) paradigm. Using a measure of social desirability and a measure of psychological distress (e.g., anxiety), cutoff scores are used to create a four-quadrant table. Respondents are assigned to the following categories: high anxiety (high anxiety/low social desirability), true low anxiety (low anxiety, low social desirability), defensive high anxiety (high anxiety/high social desirability) and repressor (low anxiety/high social desirability). In laboratory research using adult samples, those classified as repressors show a significant discrepancy between their ratings of low anxiety on self-report measures, and high levels of anxiety on physiological indicators such as increased epidermal and cardiovascular responding (Derakshan et al., 2007; Furnham et al., 2002).
During objective physiological lab tasks, adult patients with chronic pain identified as repressors are found to experience “rebound effects” during cold-press tasks, meaning that they tend to deny pain during the experiment, but report significantly higher levels of pain after the experiment, compared to non-repressors (Burns et al., 2008). Wegner (1994) termed this coping style an “ironic process,” such that attempts to suppress unwanted experiences (physical or emotional) may have the paradoxical effect of making thoughts or sensations more salient. Denying or resisting negative thoughts, emotions, and sensations in the moment temporarily decreases feelings of anxiety; however, repression of emotions can have significant physical and psychological effects. Indeed, a review by Myers (2010) cites multiple negative health outcomes for adults identified as repressors versus non-repressors, such as complications following diagnosis and treatment for heart disease and cancer. Specifically, among chronic pain patients, there is evidence to show that repression is associated with poor long term adjustment, such as higher pain levels (Burns et al., 2001) and treatment resistance (Burns, 2000).
Although repression has been examined in adult chronic pain patients, relatively little has been done in pediatric populations. This lack of attention to pediatric populations is particularly concerning as age is known to be related to repression, such that younger children tend to be more susceptible to social desirability biases (Dadds et al., 1998). Several studies have been conducted to investigate repression among children with other health conditions, primarily cancer (Jurbergs et al., 2008; Phipps and Srivastava, 1997; Phipps and Steele, 2002). Studies show that children with cancer consistently report lower levels of psychological distress including anxiety, depression, and anger, compared to healthy controls (Canning et al., 1992; Jurbergs et al., 2008; Phipps et al., 2001; Phipps and Steele, 2002) and that their self-reported emotional function is strongly predicted by socially desirable responding. In general, these studies also find that the proportion of repressors is higher in children with cancer versus healthy controls, and that repressor status is the best predictor of scores on psychological measures. Arabiat et al. (2013) found a larger proportion of repressors amongst children with chronic illnesses in Jordan compared to healthy controls providing further cross-cultural evidence. No studies yet have examined the impact of repressor status in pediatric chronic pain.
The current study specifically focused on children with chronic pain who report low levels of distress on self-report questionnaires. This group was selected for study given concerns that repression of anxiety may be a risk factor for chronic pain and somatization (Jurbergs et al., 2007). We hypothesized that (1) compared to children with true low anxiety, children with repressed anxiety would report lower scores on measures that could be regarded as negative (e.g., anxiety, depression, stress) and higher scores on measures regarded as positive (e.g., social skills, perfectionism); and (2) children with repressed anxiety would report lower levels of pain and have lower levels of function than children with true low anxiety, as measured by pain intensity, disturbance, and disability. We also conducted exploratory analyses to compare caregiver-reported ratings of their children’s psychological distress to assess for possible differences in parental perceptions.
Aim
To explore how repression may influence children’s self-report of pain characteristics and emotional functioning within this pediatric chronic pain group.
Method
Setting and sample participants
The present study was conducted at a pediatric Chronic Pain Clinic in a large, tertiary care, urban hospital in Canada. The Chronic Pain Clinic is comprised of a multidisciplinary team, including a pain physician, a pain psychologist, a nurse and a physiotherapist. All children aged 8–18 years who received a pain focused psychology assessment between January 2011 and May 2015 were included in the study. In this assessment, the Pain Psychologist conducted a clinical interview to assess pain characteristics, functional impairment, and physical and emotional functioning. Both child and caregiver also completed questionnaires. Children younger than 8 years old were excluded as they were too young to complete questionnaires. Information and measures gathered for the current retrospective study are part of standard clinical care within our Chronic Pain Clinic. At the time of the psychological assessments, caregiver consent and child assent or consent (depending on capacity to consent) were received. Families also provided consent for deidentified data to be used for research purposes. The Hospital’s Institutional Review Board approved the project as a retrospective study (IRB # 1000046255).
Measures
Demographic information was obtained from health charts, including child’s age and sex, pain duration, and pain diagnosis. All questionnaires were administered as standard procedure in clinic psychology assessments, and were used with permission and following usage terms of the license where required.
Self-report
Crandall children’s social desirability scale
The Crandall Children’s Social Desirability (CSD) measures social desirability in children ages 8–17 (Crandall et al., 1965). The CSD is comprised of 46 True or False items such as “Are you always glad to cooperate with others?” and “Do you sometimes tell a lie?” Higher scores on the CSD indicate a higher tendency for socially desirable responding. Past research has found the CSD to have test–retest and split half reliability coefficients above 0.80 (Crandall et al., 1965). Sex-normed T-scores on the CSD were utilized (M = 50, SD = 10).
Behavior assessment for children-second edition
The behavior assessment for children-second edition (BASC-2) self-report of personality (SRP; Reynolds, 2010) is a standardized multidimensional self-report rating scale used to evaluate behaviors, emotional functioning and self-perception in children ages 8–11 (child form: SRP-C) and adolescents 12–21 (adolescent form: SRP-A). Both forms of the SRP are comprised of 16 subscales and three validity indices. Items are either scored using a True/False response rating or a 4-point Likert scale rating, from 1 (Never) to 4 (Always). The present study specifically looked at three clinical subscales: anxiety, depression, and somatization. T-scores were utilized (mean of 50, standard deviation of 10), allowing for direct comparison with normative data. The BASC-2 has shown excellent reliability and validity across numerous populations (Reynolds, 2010).
Numerical rating scale
The numerical rating scale (NRS) is a validated rating scale that is typically used in clinical pain assessment as a measure of pain intensity (Ruskin et al., 2014). Children are asked to rate their current, usual, lowest, and strongest levels of pain over the last week using any number between 0 (no pain) and 10 (strongest or worst pain you can imagine). For the purposes of this study, we only assessed children’s current pain score. Children are also asked to rate, based on their average pain rating, how much their pain “bugged” them (“on a scale of 0 = not bugged at all to 10 = bugged out of your mind”). The NRS has been validated in children and youth with chronic pain, showing good convergent and discriminant validity with previously validated pain scales such as the color analogue scale (Ruskin et al., 2014).
Pain catastrophizing scale-children
The pain catastrophizing scale-children (PSC-C) is a 13 item self-report measure assessing the extent to which a child worries, amplifies, and feels helpless about their current or anticipated pain experience (Sullivan et al., 1995). The PCS-C contains three scales, rumination, magnification, and helplessness. Item responses were scored on a 5-point Likert scale from 0 (not at all) to 4 (extremely). The PCS to has good internal reliability across scales (α = .91, .75 and .87, respectively’ Sullivan et al., 1995). The factor structure of the PCS-C has been replicated in several investigations (Sullivan et al., 1995).
Child-adolescent perfectionism scale
The child–adolescent perfectionism scale (CAPS) is a 22 item self-report scale based on the multidimensional perfectionism scale (Flett et al., 2016). The scale has two subscales measuring self-oriented perfectionism and socially prescribed perfectionism. Responses are scored on a 5-point Likert scale ranging from 1 (Not at all true of me) to 5 (Very true of me). The scale has good psychometric properties including good internal reliability for the self-oriented scale (α = .85) and social prescribed scale (α = .81; Flett et al., 2016).
Caregiver report
Behavior assessment for children-second edition parent rating scale
The BASC-2 parent rating scale (PRS) is a multidimensional parent-report rating scale used to evaluate behaviors, emotional functioning and adaptability in children ages 2–21 (Reynolds, 2010). The BASC-2 PRS is comprised of 16 subscales and three validity indices. Items are scored on a 4-point Likert scale rating, from 1 (Never) to 4 (Always). The present study specifically looked at the anxiety, depression, and somatization clinical subscales, as well as an adaptability scale (e.g., “Adjusts well to changes in family plans”). The BASC-2 PRS has shown excellent reliability and validity across numerous populations (Reynolds, 2010).
Clinician report
SickKids life disruption scale (SKDS)
The sickKids life disruption scale (SKDS) is an unpublished 4 item clinician-rated scale measuring the functional disability in children and adolescents with chronic pain (McGrath and Ruskin, 2007). The scale assesses difficulties with the child’s ability to sleep, attend school, socialize with friends, be physically active, and complete basic daily activities. Each item is rated on a 5-point scale, with descriptor rated from 0 (No disruption) to 4 (Severe disruption). Each level of disruption (0–4) is operationally defined by either the amount of disruption or the frequency of withdrawal from various activities. Levels of disruption are rated by the psychologist during the child’s interdisciplinary team appointment, as part of a semi-structured interview with the child and their family. The SKDS score is determined by summing the four items, which yields a score out of 16, with higher scores representing increased disruption or pain-related disability. Although this scale has not yet been empirically validated, it is used clinically to capture functional disability in this population.
Procedure
The majority of children’s ratings (all pain characteristics, BASC-2 data) were obtained at the initial interdisciplinary pain team intake. Children and caregivers completed the BASC-2 in the waiting room prior to seeing the interdisciplinary pain team. Children’s pain characteristics and functional disability scores were recorded in their hospital charts by the pain Psychologist at the interdisciplinary team intake.
Scores for perfectionism, social desirability, and pain catastrophizing were obtained at the pain psychology assessment. The CSD, NRS, PSC-C, CAPS were completed in the waiting room and scores were entered into psychology reports. Retrospective review of health charts were conducted to obtain the above data, including demographic information. Data were then entered into an SPSS database for analysis.
Analytic plan
Initial analysis of skewness and kurtosis were run to examine data distribution for continuous variables (i.e., normality, and missing data) in the full sample; assumptions of normality were met. Across variables, there was an average of 11.5% missing data. Listwise deletion was used in all analyses. The data were analyzed using IBM SPSS (version 27).
Coping group classification
Consistent with Weinberger’s paradigm (Weinberger et al., 1979) and prior pediatric research on repression, participant scores were first identified as either high or low on both anxiety (i.e., low = T-score of below or equal to the median score of 53 on the BASC-2 anxiety scale) and social desirability (i.e., high = T-score ≥ 60 on the CSD). Participants were then classified into two coping groups, “repressors” (i.e., low anxiety/high defensiveness) and “true low anxious” (i.e., low anxiety/low defensiveness). Classification was performed on the full sample, and individuals in the repressor and true low anxious groups were included for analysis.
Determination of covariates
Demographic differences (e.g., age, sex) between repressors and true low anxious groups have been identified in the literature (e.g., Phipps and Steele, 2002). Additionally, pain duration may importantly affect reporting of outcome variables. As such, group differences in age, pain duration and sex were examined using T-tests and Pearson Chi-Square. Variables that showed a statistically significant difference between groups were entered into subsequent models as covariates.
Primary analyses
To assess whether the repressor and true low anxious groups differ on pain characteristics and socioemotional functioning, analyses of covariance (ANCOVA) were performed. Models included patient-reported pain and socioemotional function as dependent variables while controlling for age. All prerequisite assumptions for ANCOVA were met; Levene’s test of equality of error variances yielded insignificant results for each model. Eta squared (η2) was used to measure the proportion of variation in outcome that is associated with group membership (η2 of .01, .06, .14 indicative of small, medium, large effects, respectively; Cohen, 1988).
Exploratory analyses
A second series of ANCOVA were conducted in the same manner to assess whether repressor and true low anxious groups differ on caregiver-reported socioemotional function, while controlling for age.
Results
Descriptive statistics for social desirability, internalizing symptoms, and pain characteristics: Analyzed sample (N = 57).
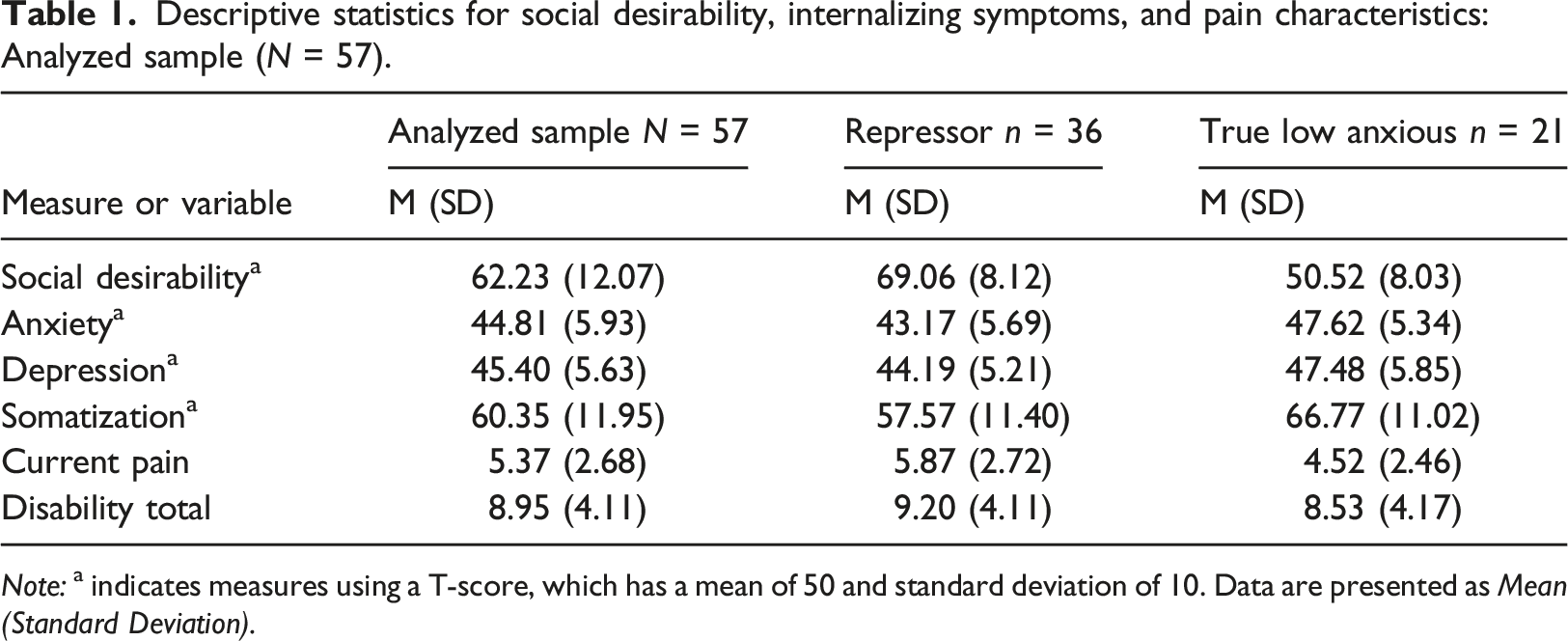
Note: a indicates measures using a T-score, which has a mean of 50 and standard deviation of 10. Data are presented as Mean (Standard Deviation).
Socio-demographic and pain characteristics across repressors and true low anxious groups.
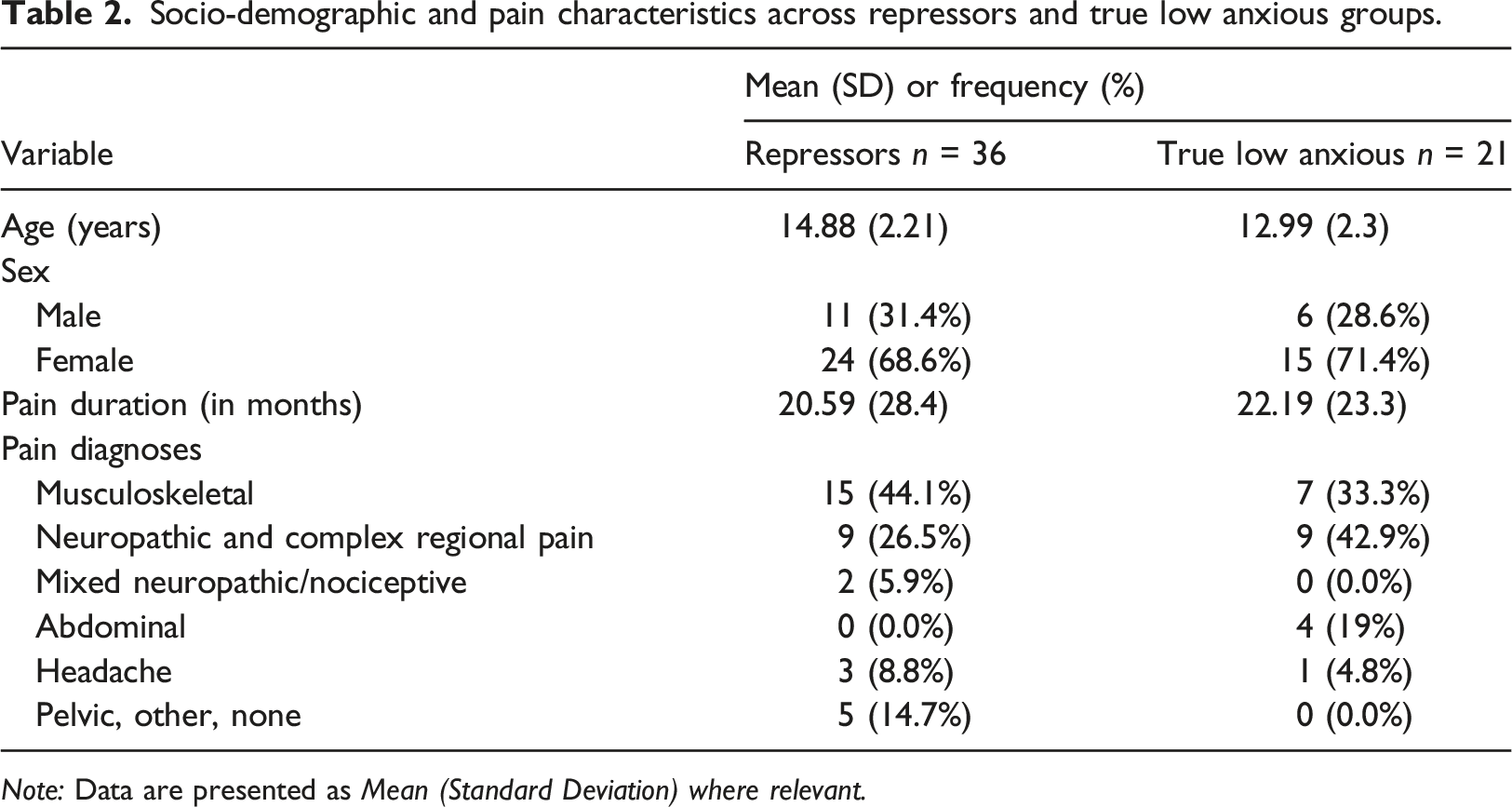
Note: Data are presented as Mean (Standard Deviation) where relevant.
Do repressors and true low anxious groups differ on how they report their pain characteristics and socioemotional functioning?
ANCOVA models comparing repressor and true low anxious groups on pain and socioemotional variables.
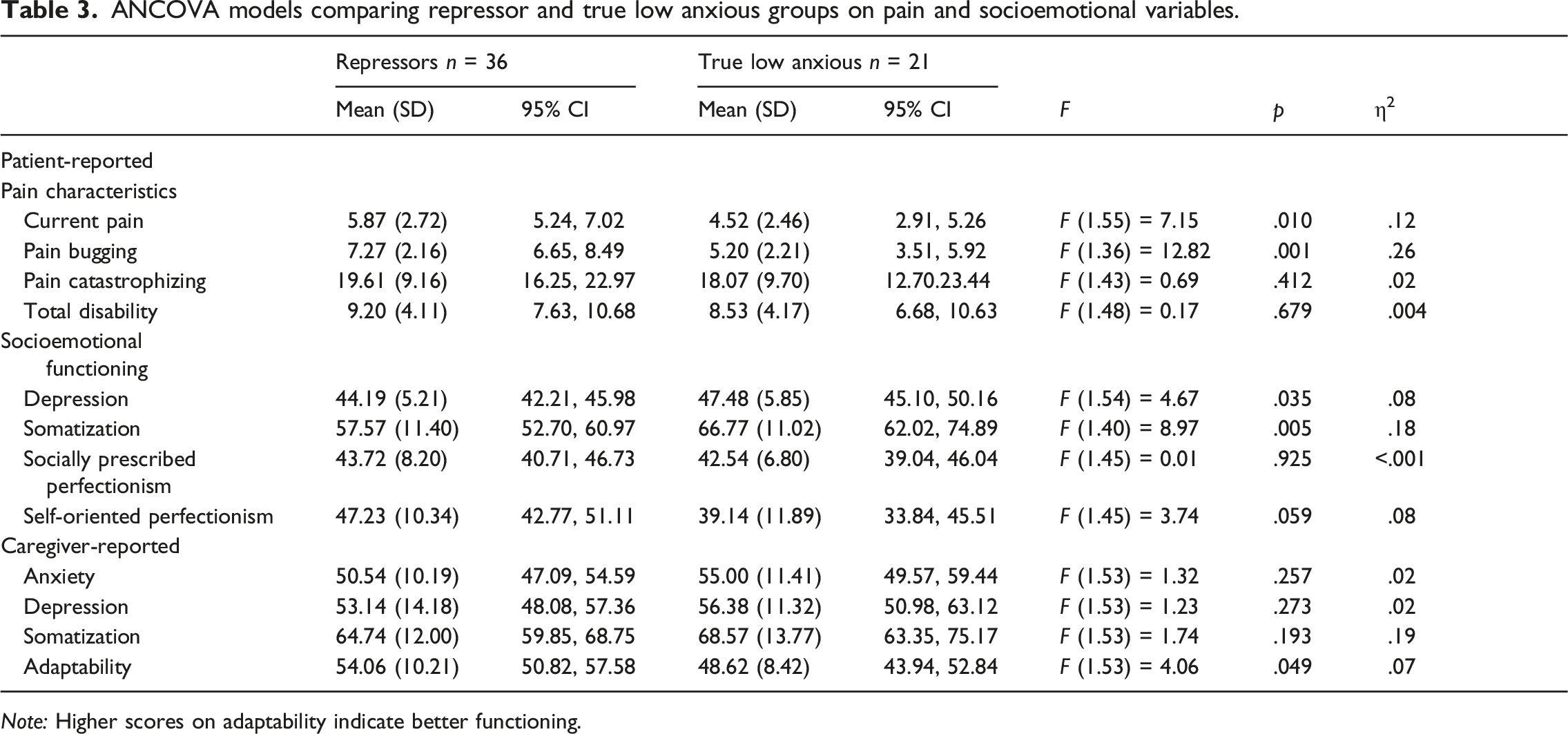
Note: Higher scores on adaptability indicate better functioning.
As predicted, repressors’ scores on the BASC-2 depression and somatization subscales were significantly lower as compared to scores of the true low anxious group, when controlling for age. Repressors reported significantly higher ratings of self-oriented perfectionism (F (1.45) = 3.74, p = 0.05, η2 = .08) than the true low anxious group, but not socially prescribed perfectionism (F (1.45) = .009, p = .93) on the CAPS.
Do caregivers of children in the repressor versus low anxious groups differ on how they report their child’s socioemotional functioning?
An examination of univariate effects (see Table 3) revealed that caregivers of repressors indicated fewer concerns with functional adaptability than caregivers of true low anxious reporters (F (1.53) = 4.06, p = 0.049, η2 = .07). No group differences were found on caregiver-reported scores on BASC-2 PRS anxiety, depression, or somatization subscales (ps > 0.05).
Discussion
The present study examined the profiles of children with chronic pain who report low psychological distress at their initial interdisciplinary pain assessment. This “low reporting group” was specifically selected for study given concerns that children’s self-report of psychological function may be a product of defensive responding, postulated by some to be a risk factor for chronic pain and somatization (Jurbergs et al., 2007). Using Weinberger’s et al. (1979) classification paradigm, this low reporting group was revealed to be heterogeneous in nature—with 34% of children within this group classified as repressors (low anxiety/high social desirability) and 19.8% classified as true low anxious (low anxiety/low social desirability). The remaining children did not meet criteria for classification in either the repressor or true low anxiety groups.
Further confirming the heterogeneity of this group, children in the repressor group exhibited different profiles than children in the true low anxious group not only on psychological outcomes but also on pain characteristics. Specifically, consistent with hypotheses and prior research, when compared to the true low anxious group, children in the repressor group reported significantly lower emotional symptoms including lower levels of depression and somatization but higher self-oriented perfectionism (i.e., perfectionism that is self-imposed versus imposed by others). This supports the notion that those with a repressive coping style are biased towards minimizing negative but endorsing positive personality characteristics (Jurbergs et al., 2008) with perfectionism arguably being an example of the latter. Caregivers’ ratings of their children’s positive traits followed a similar pattern in which caregivers of children in the repressor group scored their children higher than caregivers of children with true low anxiety on positive characteristics such as adaptability.
At face value, this suggests that children in the repressed group exhibit fewer complaints to their parents and more positive coping traits than children with true low anxiety; however, another interpretation is that children with repressed coping avoid complaining to their caregivers and thus appear to be doing well, termed the “illusion of mental health” by some (Phipps and Steele, 2002). Should this be the case, a concerning possibility is that appropriate health care may be delayed because children with repressed coping fail to voice concerns to their parents or to their health care providers. Indeed, one group recently showed that children with cancer with repressed coping are significantly less likely than non-repressors to report physical symptoms that could be late effects of cancer or signs of active disease to health care providers, possibly delaying needed treatment (Jurbergs et al., 2007).
The findings that repressors reported higher pain ratings and a trend towards higher pain–unpleasantness ratings compared to the true low anxious group were unexpected. This is especially so when considering that children in the repressor group reported far lower somatic complaints on the BASC-2 (1.5 standard deviations lower) than children in the true low anxiety group. While it is possible that this finding represents veritable differences such that children with repressed coping experience higher pain intensity but far lower somatic complaints than low anxious children another interpretation rests in the notion that children may be framing their pain ratings based on the sequence of experiences during their assessment appointment. Children’s ratings of their somatic symptoms are completed on the BASC-2 rating scale prior to seeing the pain team. As questions on this scale are of a psychological nature, children with repressed coping may be primed to minimize ratings on most questions given the psychological context. Upon being seen subsequently by our team, including an interview led by a pain physician, children may be more willing to emphasize pain ratings because they may want to underscore very real physical pain and reduce the likelihood of the team perceiving pain as having a connection to emotions. It is also possible that children with repressed coping experience their pain as more intense than children with low anxiety.
Results from the adult chronic pain literature on repression have been mixed. Some studies have found pain ratings to be higher in repressors compared to non-repressors, particularly levels of current pain (Burns et al., 2008), while other studies have found no significant differences (Franklin et al., 2014). Our finding of higher pain ratings amongst repressors is also consistent with several studies documenting higher levels of physiological reactivity to laboratory stress and greater likelihood of physical problems (e.g., tension headaches, ulcers, asthma and hypertension) in repressors versus non-repressors (Myers, 2010; Myers and Derakshan, 2015). Indeed, it is possible that higher physiological reactivity to pain may occur in children with repressed coping, presenting to pain clinics with pain that is more intense and bothersome than children with low anxiety.
Various theories have been posited to explain whether those with repressed coping are actively suppressing emotions or are unaware of their emotional experience so that this process is unconscious. It has been theorized by Derakshan et al. (2007) that those with repressor status experience negative emotional stimuli in two, contradicting, stages. First, the authors posit that repressors show an unconscious vigilance towards internal and external negative stimuli that pose a threat to their positive self-concept. This avoidance activates a physical response (e.g., increased heart rate). Cognitive avoidant strategies are then employed, allowing the individual to experience low levels of perceived anxiety. This results in high levels of physiological response to negative emotional stimuli, with low levels of perceived anxiety. The two-step process helps explain the low levels of reported anxiety on self-report measures with high levels of physiological reactivity on objective measures (e.g., skin conductance; Derakshan et al., 2007).
While differences between children in the repressor versus true low anxious group were not seen on measures of functional limitations, it is important to note that children’s level of disability in these groups is nonetheless in the moderate/moderate-severe range and does not differ substantially from full sample mean levels of disability. Thus, children’s low levels of psychological distress in these groups, regardless of being influenced by defensive responding, does not appear to protect against disability. More research is needed on functional impairment and repressor status in pediatric chronic pain populations to determine whether these children experience a different level of impairment compared to their low anxious counterparts.
Limitations
A number of limitations should be considered when interpreting findings. First, median split is not the most conservative method for determining low anxiety status. Although repressors and true low anxious children are labeled “low anxiety,” the median anxiety T score used to determine group membership was 53, which is considered “within normal limits.” Only 17.7% of the children identified as “low anxiety” had T scores 40 or below (which is the clinical cutoff). However, it should be noted that when levels of distress were examined (e.g., anxiety and depressive symptoms) both repressors and true low anxious children scored in the “low anxious” ranges (T-scores of 43 and 47 respectively). The median split approach was chosen over other methods for determining anxiety status based on what has typically been done in the literature (e.g., Myers, 2010; Jurbergs et al., 2007; Phipps and Steele, 2002).
Second, our sample may not be completely representative of all children who attend the chronic pain clinic. Children included in the current study were referred for a pain psychology assessment after their initial intake visit, which implies that even the children who report low levels of distress were thought to need additional psychological support. This is supported by the finding that the level of disability in both the repressor and low anxious group was in the moderate range (a score of 8 or more), and not significantly different from the rest of the sample.
Finally, several ANCOVAS were used to assess both hypothesis driven questions and exploratory analyses. With the number of ANCOVAS in addition to the low sample size, some caution must be used in interpreting results with a p-value of less than .05. Additionally, listwise deletion was used for all analyses. Complete case analysis is not without limitation, including the possibility for bias to be introduced by missingness.
Implications for practice
Clinical studies have found that adults with chronic pain who are identified as repressors are more likely to self-manage their pain and thus would not present to primary health care teams as often (Franklin et al., 2014). This is particularly concerning as repressive coping has been associated with an increased risk of somatic diseases, such as heart disease and cancer (Mund and Mitte, 2012). Given the risk of overlooking children with repression in primary health care teams, one could consider administering a brief social desirability scale as part of an overall evaluation to help identify children who respond in socially desirable ways. At minimum, social desirability indexes on established measures such as the Lie scale on the RCMAS, should be examined prior to interpreting psychosocial data.
Alternatively, objective measures of pain (e.g., Quantitative Sensory Testing, cold pressor) and distress in addition to self-reported levels of distress may help clinicians identify repressor children and address their psychological needs appropriately. This could be particularly important given that research has shown those with repressor status to be treatment resistant (Burns, 2000; Myers, 2010). Some research has also indicated the inclusion of projective measures such as drawings to better capture and understand emotional well-being in pediatric pain populations (Failo et al., 2018).
Given that many researchers in pediatric pain and behavioral medicine rely on self-report questionnaires to assess emotional function, the influence of socially desirable responding should be considered, as scores computed as averages may be artificially reduced because of socially desirable responding. In our sample, 34% of children were classified as repressors.
Children with repressor status might require targeted interventions as they may have difficulty in recognizing their own affective responses, particularly when it is negative (Myers, 2010). It is possible that children with repressor status may need additional supports and strategies to help them engage in treatment and increase their awareness of the connection between the mind and body. Psychological treatments that address acknowledging and accepting emotions, such as those targeted at improving psychological flexibility, may be beneficial for these children (Wallace et al., 2016).
Conclusion
Findings from the current study highlight the need for clinician and researchers alike to critically evaluate low levels of self-reported distress and consider the implication of social desirability on these scores. There exists some evidence from the adult literature that repression is related to increased risk for future physical health complications such as complications following diagnosis and treatment for heart disease and cancer. Longitudinal research is needed to determine whether repressed coping is associated with poor outcomes for children with chronic pain and whether children with repressed coping may benefit from targeted treatments that can address this coping style. Repression may be an important factor to consider for those assessing and treating children with chronic pain.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.