
Abstract
Providing quality end-of-life care to a child who is dying in hospital can be stressful and challenging, and health professionals often feel ill-prepared and require additional support. End-of-Life Essentials offers online education modules for health professionals working in acute hospitals, including one on end-of-life care in pediatric settings. This study aimed to evaluate this module and explore learners’ views on challenges faced when caring for a dying child and their family in a hospital setting. Learners comprised nurses, doctors, and allied health professionals. A quantitative pre-/post-evaluation analysis was conducted using learner data (n = 552) on knowledge and skills gained from engagement with the module, along with a qualitative thematic content analysis on learner responses (n = 395) to a post-evaluation free-text response question, between May 2019 and May 2020. Learners’ post-evaluation ranks of perceived knowledge, skill, attitude, and confidence were significantly higher than pre-evaluation ranks (p < 0.001). Effect sizes were small to medium, ranging from 0.31 to 0.38 (95% confidence intervals from 0.23 to 0.45). Emerging themes from the qualitative data were dealing with emotions, and communicating effectively. This evaluation suggests that the Pediatrics module could be a useful online learning resource for health professionals. A planned longitudinal study will further investigate practice change.
Keywords
Introduction
Many child deaths in hospitals occur in neonatal, pediatric, and intensive care settings (Bloomer et al., 2016; Mu et al., 2019). Infants and children who are dying can be supported at home as well as hospital, with many factors contributing to the location of death (Coombs et al., 2020). As the death of an infant or child is relatively uncommon, health care professionals’ end-of-life clinical skills are not often practiced, and clinicians can feel poorly trained and ill-prepared (Korzeniewska-Eksterowicz et al., 2013; Price et al., 2017). Dying in an acute care setting brings its own unique challenges, where fast-paced environments with a focus on curative care, may translate to clinicians’ viewing dying as a failure (Rawlings et al,. 2021; Muskat et al., 2020). There are enormous challenges to clinical practice when providing pediatric end-of-life care, such as decision-making for starting or withdrawing treatments, discussing goals of care with minors, and sensitively ascertaining the hopes and worries of a family who may not share expectations or wishes (Streuli et al., 2019). As a result, many health care professionals require support in the care of children who are dying (Atout, 2019), as this is an area that can be both stressful and challenging (Bergsträsser et al., 2017; Bloomer et al., 2016).
In 2015 the Australian Government Department of Health funded the End-of-Life Essentials (EOLE) project, which provides evidence-based, online education and implementation toolkits for doctors, nurses, and allied health professionals who work in acute hospitals (End-of-Life Essentials, 2022a). The EOLE education is delivered online as a response to the requirements of a nationally delivered program, with over 25,000 learners enrolled to date, who can engage with the education in their own time. There is also the impracticality of delivering multiple cross-jurisdictional and geographically dispersed face-to-face sessions across Australia (Rawlings et al., 2019a).
EOLE aims to strengthen the knowledge base and drive practice change in end-of-life-care, and is based on the ACSQHC National Consensus Statement: essential elements for safe and high-quality end-of-life care (Australian Commission on Safety and Quality in Health Care, 2015). The project translates the five processes of care elements from the statement: patient centred care; teamwork; goals of care; using triggers; responding to concerns, directly into a suite of education modules, each developed following consultation with industry and clinical partners (Rawlings et al., 2019b) “Paediatric End-of-Life Care” (hereafter referred to as the Pediatrics module) features in the suite of EOLE modules, and includes education around end-of-life care for children in hospital settings (e.g., the importance of families in all aspects of care, applying a critical approach to symptom management, and responding to moral distress) (End-of-Life Essentials, 2022b).
Aim
To evaluate the EOLE Pediatrics module, and to explore learners’ views on challenges faced when caring for a dying child and their family in a hospital setting.
Methods
The EOLE modules
The suite of EOLE education modules are freely available online, and are designed to build capacity of doctors, nurses and allied health professionals working in acute hospitals in delivering end-of-life care (https://www.endoflifeessentials.com.au/). Each module focusses on a specific aspect of clinical care, with learning delivered via problem-based learning instruction, graphics, and videos demonstrating practical care scenarios (Rawlings et al., 2019b). The pedagogy is a mix of case-based learning, critical self-reflection tools, and adult learning principles (e.g., where the learners’ prior experience is sought and integrated into building new knowledge, and where learning is relevant and self-directed) (Lee et al., 2020). Simulations (film) were created and employed to provide educational content around communication responses. Peer-reviewed dialogue and scripts were developed in partnership with a National Advisory Group (NAG) to provide simulated health professional responses to families’ and child questions concerning end of life. Examples of questions to elicit simulated responses include Why am I not having any more chemo? Why are the lumps on my arms getting bigger? Is my brother going to die this time? Why are mum and dad so sad? Why is my baby brother not coming home? Have I done something wrong? Topics such as empowering families, moral distress, staff support, self-awareness, and mindfulness are included in the education, woven around the case-based learning, with evidence-based resources to provide varied opportunities for acquisition of new understandings and knowledge. There is also an accompanying and downloadable implementation toolkit, which provides resources and tailored checklists that learners can take away from the education and use in their own clinical practice, reinforcing learning and behaviour change in the workplace (Hutchinson et al., 2018). Learners who register are given access to all modules and can choose to engage with any or all of them. The modules are self-paced, taking anywhere from thirty minutes to one and a half hours to complete, depending on how deeply the learner chooses to delve into the learning resources (End-of-Life Essentials, 2022b).
Targeted to health professionals working within pediatric hospital settings, the learning outcomes of the Pediatrics module are as follows: • Identify causes of expected deaths in Australian children. • Identify the centrality of families and the intricacy of decision-making in pediatric end-of-life care. • Develop an awareness of your own attitudes to the death of a child. • Analyse and adopt communication responses to common questions in pediatric end-of-life care. • Apply a critical approach to symptom management in children who are living with life limiting conditions. • Recognize that compassion in fast paced environments is possible. • Recognize the most helpful responses to moral distress. • Locate best professional responses and resources to grief, loss and bereavement (End-of-Life Essentials, 2022b).
The Pediatrics module was developed through consultation with the NAG, along with experts from Palliative Care Australia, Paediatric Palliative Care Australia and New Zealand (PaPCANZ), and the pediatric palliative care project “Quality of Care Collaborative Australia” (QuoCCA). As part of ongoing quality processes, the module was also peer-reviewed, and user-tested by doctors, nurses, and allied health professionals working in Pediatric settings.
Evaluation framework
The EOLE project has so far carried out a range of data collection techniques to explore and describe changes in the perceived knowledge, skills, and behaviors of health professionals who engage with the online modules and resources (Rawlings et al,. 2020a, 2021). Evaluation of all EOLE modules is ongoing, with two discrete evaluation components embedded into each module, considered a multi-methods approach (Anguera et al., 2018): 1. A quantitative pre-test/post-test evaluation related to learners’ perceived knowledge, skill, attitude, and confidence. 2. A qualitative thematic analysis on learner responses to a free-text question (relevant to the module content) that invites them to reflect on what they have taken away from the education or on their own practice.
These evaluation components are captured in two different platforms, providing different mechanisms by which to consider how the education modules help to improve knowledge, and whether they are useful in practice (Rawlings et al., 2021).
The education takes approximately 35 min to complete online. The strengths of online education include flexibility of access, its ability to overcome geographical boundaries, being time efficient (Reeves et al., 2017), and its ‘potential for … rich and effective construction of knowledge’ (Russell et al., 2006: 496). Furthermore, virtual learning allows the learner to critically reflect on providing care to a dying child and there is evidence that transformative learning and professional empowerment can be attained from online learning (Sim and Radloff, 2008). Certainly, there is scope to use the online education as a foundation for face-to-face education, where interprofessional collaboration and group learning can happen (Reeves et al., 2017).
Sampling
The participants in this evaluation were learners (doctors, nurses, allied health professionals) who had accessed the EOLE website and engaged with the Pediatrics module. Learners are self-selected in that they register on the EOLE website and choose which modules to engage with.
Ethics
Ethics approval was obtained from the Flinders University Research Ethics Committee (Project 7012). Learners are invited to complete pre-test and post-test questions within each module, and consent is implied with completion of the evaluation questions. Participation is voluntary with no forced answers; learners can choose to engage with the modules without participating in the evaluation. Learning about pediatric end-of-life care can be an emotional trigger for health professionals. Throughout the education, learners are invited to consider their own reactions, feelings, and emotions and to prepare for kind and compassionate care.
Data collection
Data (both quantitative and qualitative) were extracted for a 12-month period, May 6, 2019–May 6, 2020.
Quantitative data
Quantitative evaluation questionnaires were embedded in the EOLE learning management system. The pre-evaluation questionnaire was set out at the beginning of the Pediatrics module, under the header “In thinking about providing end-of-life care to paediatric patients….” Learners were asked to select “strongly disagree,” “disagree,” “neutral,” “agree,” or “strongly agree” for four statements: I have sufficient knowledge in providing end-of-life care; I am skilled in providing end-of-life care; I have a positive attitude towards end-of-life care; I am confident in my ability to provide good end-of-life care. At the end of the Pediatrics module, learners were asked to again respond to the same four statements about end-of-life care knowledge, skill, attitude, and confidence under the header “Since completing this module, in thinking about providing paediatric end-of-life care….”
Learners who did not provide any responses were deleted and excluded from data analysis. The pre- and post-evaluation responses were deidentified and imported into SPSS separately, then merged using the SPSS merge function with the key variable userID. In total, data from 552 learners were included for data analysis.
Qualitative data
A question (individual to each module) was developed by the researchers to seek feedback on challenges in care provision, to consider resources for the implementation toolkits (Hutchinson et al., 2018). The question for the Pediatrics module was derived and developed from the module learning outcomes and key literature (Cherny et al., 2015; Children’ s Health Queensland Hospital and Health Service, 2014), with learning outcomes developed in consultation with a National Advisory Group of Pediatric palliative care doctors, nurses, and allied health professionals. Learner statements (one statement per learner) responding to the free-text response question posed at the end of the module: “What is your biggest challenge when engaging with a dying child and supporting families and friends?” were extracted from the EOLE learning platform. The data were cleaned, de-identified, and imported into NVivo version 12 software package (QSR International).
Data analysis
Quantitative data
Data were analysed using IBM SPSS Statistics version 25. Categorical data were summarized using frequency and percentages. Each variable (perceived knowledge, skill, attitude, and confidence) was measured using a single 5-point Likert item (strongly disagree = 1, disagree = 2, neutral = 3, agree = 4, strongly agree = 5). Data were ordinal, therefore the Wilcoxon signed-rank test was used for comparison of pre and post evaluation data. Effect size (r = z/
Qualitative data
Data were analysed using NVivo version 12 (QSR International). Thematic content analysis was conducted to identify key themes emerging from the data (Green and Thorogood, 2018; Vaismoradi et al., 2013), a method chosen due to its suitability for analysing complex healthcare data (Vaismoradi et al., 2013). Author MW completed coding for all data and created a coding scheme. An inductive, open approach was used to code the participant statements line-by-line, conceptually grouping similar words and sections of text, and adding new codes when new concepts emerged (Saldana, 2016; Vaismoradi et al., 2013). Axial coding was then used to organize the codes into overarching categories, and to develop and refine the themes (Saldana, 2016). To enhance rigor and improve reliability of the analytical approach (Vaismoradi et al., 2013), authors MW and DR reviewed and discussed the analysis process and coding schema in detail, with minor modifications made. MW and DR then consulted with a third author, KD, to discuss and refine the themes further. In considering reflexivity (Ramani et al., 2018), author MW led the analysis from a neutral position, having no clinical background, and no previous involvement in module development. All authors were conscious of the need for the learners’ own words and voices to drive the analysis, rather than their own experiences or pre-conceptions (Ramani et al., 2018; Vaismoradi et al., 2013).
Results and findings
Results
In total, 591 learners accessed the pre-evaluation questionnaire, and 545 learners responded to at least one question, the response rate was 92.2%. A total of 552 learners accessed the post-evaluation questionnaire, 507 learners answered at least one question, the response rate was 91.8%.
Demographics
Of the 552 learners, 426 (77.2%) were nurses, 64 (11.6%) were doctors, and 62 (11.2%) were allied health professionals. The majority of learners (70.8%, n = 391) were from acute hospitals. This sample of learner professions mostly represented the proportion of healthcare professionals in Australian public hospitals (Australian Institute of Health and Welfare, 2019), similar to previous studies by the authors (Rawlings et al,. 2020a, 2021).
Impact on learners’ perceived knowledge, skill, attitude, and confidence
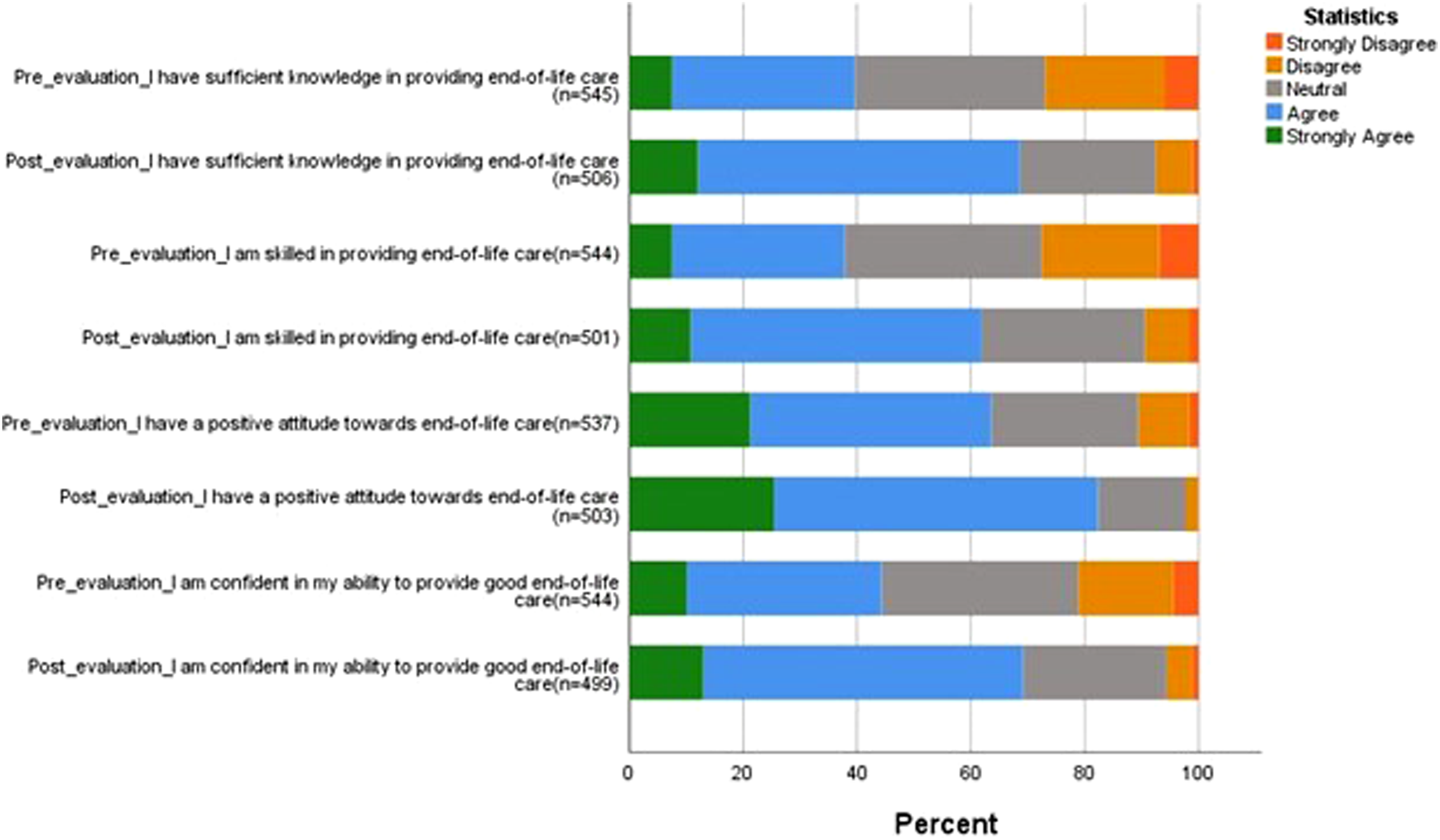
Learners’ perceived knowledge, skill, attitude, and confidence in providing end-of-life care to pediatric patients.
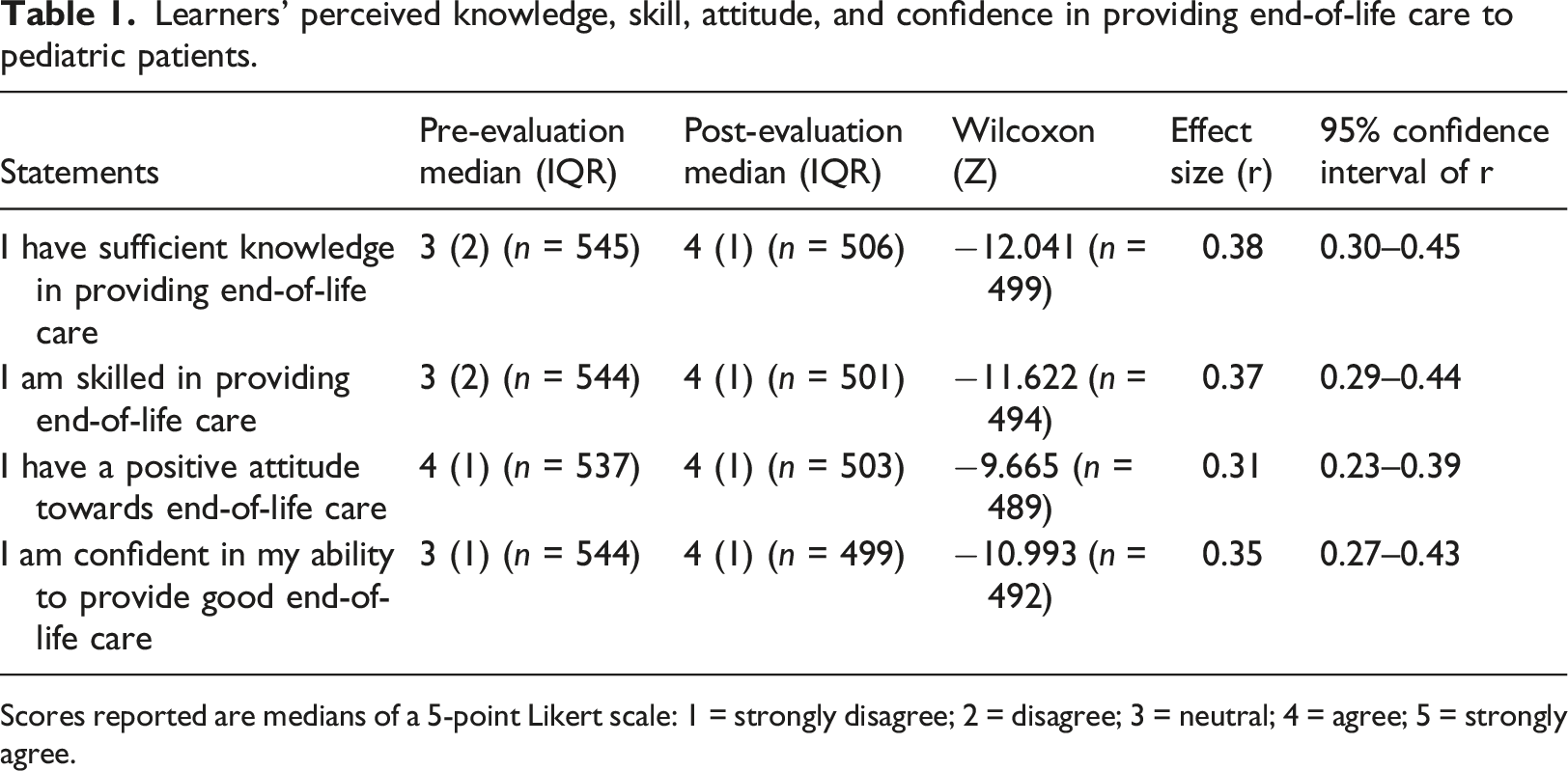
Scores reported are medians of a 5-point Likert scale: 1 = strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree.
Learners’ perceived knowledge, skill, attitude, and confidence in providing end-of-life care to pediatric patients.
Qualitative findings
A total of 395 learner statements (one statement per learner) responding to the free-text response question were thematically analyzed. Nine emerging themes were organized in to two overarching categories: Dealing with emotions and Communicating effectively. Descriptions of each theme, along with quantitative summaries (number and percentage of learner statements which related to each category and theme) and exemplar learner quotes, are presented below.
Dealing with emotions
Managing own emotions
More than one third of learners (n = 135; 34.2%) discussed the challenge of managing their own emotions, including not becoming overwhelmed, or letting their own feelings of sadness get in the way of their ability to provide adequate care as a health care professional. “Biggest challenge is keeping own emotions in check” (L35) “emotions and not having a courage to deal with it” (L79) “My emotions getting the better of me when having to face the patient and their family/friends” (L224)
Providing adequate emotional support and comfort
Less than one fifth of learners (n = 68; 17.2%) discussed the challenge of being able to provide the right level of emotional support and comfort to the child and family, for example, offering empathy, compassion, and meeting their needs. “consoling the family is difficult for me” (L45) “knowing when the right time may be to approach the family, wanting to provide space to allow for grieving, though also wanting to assure my presence and if there are any needs or requests they can be fulfilled.” (L199) “Providing comfort to the child in a way that is fun and engaging.” (L272)
Witnessing the emotions and grief of families
The biggest challenge for around one seventh of learners (n = 55; 13.9%) was witnessing the emotions of grieving families, for example, seeing parents upset, scared, or angry. “some families become angry and need to vent, I find this difficult” (L290) “When a child dies emotions are particularly heightened, there can be sometimes feelings of guilt, anger, overwhelming loss and to sit in those situations is extremely hard.” (L367) “Seeing the devastating fear in parents’ eyes” (L283)
Unfairness and unnaturalness of the death of a child
The biggest challenge for 28 learners (7.1%) was the sense of unfairness of the death of a child; that they have died too soon. “the injustice of a child passing” (L216) “My biggest challenge is the simple fact that it is a child and on many moral levels, parents are not to bury their children.” (L217) “That they haven't lived their lives yet. The death seems far too soon” (L303)
Identifying as a parent
For 26 learners (6.6%), being a parent themselves and identifying as a parent was the biggest challenge to their professional role, for example, thinking of their own children and what it would be like to lose them. “That it seems so unfair and as a mother myself how would you ever recover” (L302) “Since having children I find it difficult not to put myself in the parents situation.” (L288)
Feeling helpless or inadequate
The biggest challenge for 15 learners (3.8%) was feeling helpless or inadequate in these situations, for example, that nothing they could do would make a difference, or that they have not done enough to help. “I feel so inadequate because I cannot change the outcome” (L129) “helplessness in not being able to fix the situation or save the child” (L329) “The intense feelings of helplessness and unfairness with regards to the situation” (L330)
Communicating effectively
Answering questions, not knowing what to say
More than one quarter of learners (n = 107; 27.1%) discussed the challenge of effectively answering patients’ or family members’ questions, for example, knowing the right words to use or ways of responding in these situations. “my fear of saying or doing something wrong” (L225) “not knowing what to say to the parents” (L254)
Being honest about the child’s prognosis
For 25 learners (6.3%), the biggest challenge was talking to the child and their family about dying and being upfront and honest about the child’s prognosis. “Explaining to parents” (L86) “Understanding how to communicate with a child when telling them about their condition” (L257)
Discuss goals of care, respect and incorporate family’s needs and wishes
Thirteen learners (3.3%) discussed the challenge of initiating discussion around end-of-life care goals and needs, making sure to involve the family in this and respect their wishes. “supporting a/or parents’ decisions that I don’t necessarily agree with.” (L253) “Depending on the age of the child identifying what is important to them, what is important to the families and friends may not always be the same. trying to find and offer a perspective on how they experience illness and treatment options.” (L60)
Discussion
This study aimed to evaluate the EOLE Pediatrics module and explored learners’ views on challenges faced when caring for a dying child and their family in a hospital setting. The quantitative results of this study have shown that learners demonstrated a statistically significant increase in perceived knowledge, skill, attitude, and confidence in providing end-of-life care to pediatric patients compared to pre-evaluation ranks. This is consistent with evaluations undertaken on the Chronic Complex Illness module (Rawlings et al., 2020a) and the Emergency Department module (Rawlings et al., 2021). The qualitative results revealed two overarching themes of: “dealing with emotions” and “communicating effectively,” with communication featured as a theme in earlier work (Rawlings et al., 2019b, 2020a, 2021).
Excellent communication is vital to provision of good end-of-life care for children but is insufficient and/or lacking in many cases (Mu et al., 2019), and can be delayed until death is imminent (Marsac et al., 2018). Education and training for health professionals on communication skills related to death and dying and having challenging conversations, tends to vary across countries and within professional groups (Beaune et al., 2018), although Ekberg and colleagues state that “Effective communication is crucial for high-quality pediatric palliative care” (Ekberg et al., 2018: 1518). One barrier to excellent end-of-life communication though is a lack of experience, as many health care professionals (outside of intensive care units) may not have been present for the death of a child (Midson and Carter, 2010).
A further barrier to good quality care, is a lack of education in pediatric palliative care (Bergsträsser et al., 2017). Atout (2019) cited communication as the highest educational need by nurses who work with children with palliative care needs, leaving them “unprepared to act” or “at a loss for words” (2019: 4). Learners in the current study mentioned the challenge of effectively answering patients’ or family members’ questions, for example knowing the right words to use or ways of responding in these situations. Communication also covers concepts of truth telling, prognostication, honesty and discussing goals of care, all of which are stressors for staff (Dryden-Palmer et al., 2018). In a systematic review of parents’ needs in pediatric palliative care, communication and choice were rated highly (Gill et al., 2021), and in a study by Midson and Carter (2010), communication that prepares parents for the death of a child (as well as decision-making) was identified as a major issue.
Moral distress in pediatric end-of-life care can be seen as encompassing uncertainty of treatment effectiveness, awareness of potential poor outcomes, consideration of pain and suffering in life-limiting illness, and conflict over decision-making and conflicting values (Brandon et al., 2014). Many of these concepts are found within the results of this study, identified by learners as emotionally challenging. Therefore, an important consideration for clinicians in end-of-life care is managing their own emotions and emotional responses (Grimston et al., 2018), with Bergsträsser and colleagues describing the work as requiring high emotional involvement, consisting of emotionally draining tasks, and evoking emotional distress such as related to decision-making (Bergsträsser et al., 2017). Curcio (2017) supported this in relating incidences where nurses are required to act against their own beliefs (e.g., treatment versus non treatment). This author also mentioned concepts around compartmentalising emotions and emotional distancing behaviour (self-preservation) to help with the multiple emotional demands of the work, including understanding and compassion for families (Curcio, 2017).
Emotional burden, moral distress, and the need to strengthen resilience, was also identified by Mu and colleagues in their systematic review of nurses caring for children in a pediatric intensive care unit (Mu et al., 2019). However, heightened emotions cannot always be easily managed, and staff resilience can be exhausted (Boyle and Bush, 2018; Sisk et al., 2020), with some learners in the current study speaking about the moral distress of recognising and understanding the right thing to do, and then being unable to implement it. If moral distress remains unaddressed, there is the potential for adverse psychological distress and physical symptoms in health professionals, as well as an overall loss of workforce due to burnout (Brandon et al., 2014).
In addition, results from the current study showed that some learners identified that their role was to communicate with a family who may no longer share expectations of their child’s illness and life; coupled with themes of not knowing what to say, as well as identifying strongly as a parent who is supporting another in sorrow, grief, and loss. Chan and colleagues wrote about the perceived challenges in providing pediatric palliative care, one being the vulnerabilities of being a parent while also providing end-of-life care to children (Chan et al., 2019).
What also resonated with some learners and in the literature was that children are not supposed to die (Curcio, 2017), that a death in one so young is unfair, and that it disrupts the natural order of things (Muskat et al., 2020). This was described as difficult by those learners who are parents (Curcio, 2017), who are of a similar age to parents of a dying child or have a child of a similar age (Muskat et al., 2020). For some there was a blurring between their personal and professional self (Grimston et al., 2018), with Muskat and colleagues reporting impacts on clinicians’ own personal relationships (Muskat et al., 2020).
In contrast to this, however, the literature also reported factors of both personal growth (Beaune et al., 2018), and professional growth for those working with dying children (Muskat et al., 2020). Also, important to consider, is the need for self-awareness and proactive self-care (Dryden-Palmer et al., 2018; Muskat et al., 2020), a must for any health professional working in a setting where they experience death and dying. Organizations must be attentive to this (Rawlings et al., 2020b), and offer staff the opportunity and time for self-care (Beaune et al., 2018) and team building (Dryden-Palmer et al., 2018). Strategies that can help to retain staff working in these areas include formalized support mechanisms, such as Employee Assistance Programs (EAPs) and clinical supervision, as well as education and professional development (Whiting et al., 2020).
Some learners also reported feeling helpless in view of imminent death (Grimston et al., 2018), with challenges noted in talking to the child and their family about dying, and in prognosticating. It is important to recognize however, that care of the family is as important as care of the dying person and this is especially true in pediatrics (Bloomer et al., 2016). Ekberg and colleagues go further in saying that the principles of family centred care underpin pediatrics (Ekberg et al., 2018), although it should be noted that there are challenges to developing such relationships (Muskat et al., 2020). Working and communication with (and between) family members was also highlighted as important (Grimston et al., 2018; Marsac et al., 2018).
Strengths and limitations
Learners were self-selecting in registering to the EOLE education and then engaging with the Pediatrics module, therefore there is a tendency towards acquiescence, with their responses likely to differ from those who elect not to do this (Weijters and Baumgartner, 2012). Numbers of learners in this topic are lower than others due to the specialized nature of the content, however there are also strengths in that learners could be more motivated. The self-report nature of the evaluation, which is a feature of the EOLE education, does present limitations around gaining an understanding of the full impact of the education in practice. For example, measuring ones’ own knowledge, attitudes, and confidence as a result of e-learning is in itself problematic, and by nature subjective. It can be seen as an example of indirect assessment of cognitive learning (Benbunan-Fich, 2010), as opposed to direct assessment by, for example, direct observation of whether, and to what extent behaviour/practice change actually took place, with self-assessment not always correlating with objective measures (Dickson et al., 2012). However, a strength of this is that learners have considered their practice and looked at what could be changed to improve end-of-life care for children. A longitudinal study is planned which will aim to provide real data on both intended and actual changes in practice.
Regarding the qualitative data, learner responses to the open-ended question varied in length from one or two words, to multiple paragraphs. Learners were not probed further on their answers, potentially reducing the richness of the data; however, a strength lies in the fact that the authors have heard the voices of those who are caring for dying children, even if not expansive, and can now look to address the challenges that they face in this area.
Another limitation is that the qualitative and quantitative data were collected in two different platforms and cannot be linked, which may have provided a more comprehensive picture of learners’ experiences. A further limitation is that more detailed demographics data were not captured (e.g., role, length of service), thereby limiting a more in-depth analysis of learner characteristics.
Implications for practice
More education is needed in relation to pediatric end-of-life care, especially around communication skills and discussing goals of care. Examples from participants include “Answering the ‘will I die?’ question” (L9), and “Having to provide honest answers which involve sharing the reality of the child’s condition” (L108). Communication plays an important part in improving end-of-life care (Rawlings et al., 2019b).
It is also important to acknowledge that care of the family is as important as care of the dying child. Examples from participants include: “setting goals of care. Family to be involved. Encourage siblings to voice their concerns” (L286). Person-centred care, and here family-centred care, should always be the aim in care at the end of life (Rawlings et al., 2020a).
An important consideration for clinicians is in managing their own emotions and emotional responses (especially as a parent), and to acknowledge that professional and personal boundaries can become blurred. Examples from learners who identified as parents included: “trying to be professional while holding back my own emotions” (L336), and “My biggest challenge is not thinking ‘how would I cope if this was my child’” (L120). Self-preservation and preventing burnout are important considerations in this work (Curcio, 2017) which makes self-awareness and proactive self-care a priority. While debriefing with colleagues is helpful, formalized and structured organizational support, such as employee assistance programs and clinical supervision, is also important. The EOLE Pediatrics module includes reflection opportunities, further reading and references on self-care, and examples of self-care in practice such as “The Pause” following a death in the Emergency Department (Cunningham and Ducar, 2019).
Conclusion
This study has shown that learners can and do increase their perceived knowledge, skill, attitudes, and confidence in providing end-of-life care to pediatric patients in a hospital setting, following engagement with the EOLE Pediatrics module. Learners also tend to consider and reflect on the challenges that they face in providing this care. Communication is vital from the perspectives of learners, with the literature emphasizing the need for this in education programs. It is also important to recognize the emotional burden that this type of care places on health professionals, and to acknowledge that lines can be blurred between the personal and professional, with self-care vital in building resilience and maintaining strength in the face of dying.
Footnotes
Acknowledgements
The authors thank the EOLE module learners for their contribution to this research.
Author contributions
All authors contributed to the study conception and design and data analysis and/or drafting and writing of the manuscript. All authors have read and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: EOLE is funded by the Australian Government Department of Health. Education evaluation is a funding requirement. Some authors (KD, MW and HY) are part or wholly funded to conduct the EOLE project.
Ethical approval
Ethics approval was obtained from the Flinders University Research Ethics Committee (Project 7012). Learners are invited to complete pre-test and post-test questions within each module, and consent is implied with completion of the evaluation questions. Participation is voluntary with no forced answers; learners can choose to engage with the modules without participating in the evaluation.