
Abstract
The objective of this study was to assess the burden of disease and prevalence of lifestyle factors for adolescents and young adults with frequent episodic migraine. We conducted a secondary comparative analysis of data collected during two previous studies. Inclusion criteria for this analysis were age 15–35 years, 15 to 44 migraine episodes within 12 weeks, and completeness of Migraine Disability Assessment and lifestyle questionnaire data. Datasets of 37 adults (median age [interquartile range]: 25 [6]) and 27 adolescents (median age [interquartile range]: 15 [1]) were analyzed. 81% (n = 30) of adults reported severe disability (16% [n = 3] of adolescents; p < 0.001). Headache frequency (24 vs. 17 days; p = 0.005) and prevalence of regular analgesic use (60% [n = 22] vs. 18% [n = 5]; p = 0.002) were significantly higher in adults. In adults, sleep duration on weekdays was significantly lower (8.5 vs. 10 h; p < 0.001). Any consumption of caffeine tended to be higher in adolescents and alcohol consumption tended to be higher in adults (p > 0.05). This study underlines the importance of educating adolescents and young adults with migraine about lifestyle habits that are likely to interfere with the condition.
Introduction
Migraine belongs to the group of primary headache disorders as classified by the International Classification of Headache Disorders (IHS, 2018). This condition is caused by a complex interplay of central and peripheral pathophysiological mechanisms that lead to a variety of symptoms (Eller and Goadsby, 2020). A typical migraine headache is characterized by recurrent episodes of unilateral, pulsating headaches of moderate to severe intensity. In general, migraine headache is aggravated by routine or physical activity and can be accompanied by symptoms like nausea, photo-, or phonophobia. If transient focal neurological symptoms (i.e., visual or sensory) precede a migraine attack, a migraine with aura is diagnosed. Often, a pro- or postdromal phase is associated with a migraine episode with patients complaining of fatigue, as well as cognitive, emotional, or behavioral symptoms, less or more appetite, and others (IHS, 2018). Migraine is a relevant and common neurological disorder affecting all age-groups including children and adolescents. The disorder leads to a restricted participation in social and everyday activities, to a considerable fraction of “years lived with disability,” and holds the risk of chronification (Philipp et al., 2019; Sillanpaa and Saarinen, 2018; Torres-Ferrus et al., 2019; Woldeamanuel and Cowan, 2017). Overall, more than a billion people worldwide suffer from migraine according to a recent systematic analysis of the Global Burden of Disease Study (Saylor and Steiner, 2018).
In the acute treatment of migraine attacks, the evidence-based approach is to establish an effective pharmacological treatment strategy (Marmura et al., 2015; Oskoui et al., 2019b). A tailored, individual, and multimodal approach combining education, non-pharmacological interventions, and, in case that those actions stay insufficient, pharmacoprophylaxis represents the gold standard in preventing migraine attacks (Eller and Goadsby, 2020; Oskoui et al., 2019a).
Epidemiological studies identified a variety of risk factors relevant for primary headache disorders in adults and adolescents (Albers et al., 2013; Hagen et al., 2018; Milde-Busch et al., 2010, 2011; Roy et al., 2019; Torres-Ferrus et al., 2019). Besides determinants that cannot be influenced (i.e., genetics and climate conditions), several publications highlight the importance of lifestyle factors (i.e., diet, alcohol and nicotine use, sleep habit, or physical activity) regarding their effect on the frequency and intensity and/or duration of headache episodes, particularly in migraine patients (Albers et al., 2013; Fernandez-de-Las-Penas et al., 2010; Le et al., 2011; Robberstad et al., 2010).
Lifestyle factors are supposed to be most easily amenable in the context of interventions (Marmura, 2018; Lehmann et al., 2013). Therefore, thoroughly reflecting everyday activities is recommended. A headache diary—paper-based or by use of electronic applications—is an efficient way of supporting this process. There upon, an appropriate individual education on a biopsychosocial basis supported by written or digital information constitutes an effective as well as economic approach for the management and prevention of migraine attacks (Park et al., 2016; Peris et al., 2017; Woldeamanuel and Cowan, 2016). Prevalence and population-attributable risk of dietary and lifestyle factors in the light of impact on migraine supposedly increase with age. In this context, a rise in consumption of alcohol and nicotine as well as a decrease in physical activity have been documented in prior epidemiological adolescent studies at different age-groups up to age 19 (Albers et al., 2013).
So far, only very limited data exist that specifically focus on the burden of disease and prevalence of lifestyle factors considered relevant for migraine in young adult patients in their twenties up to their first thirties (Dzoljic et al., 2014). From a child neurologist’s perspective, there is an important need to fill this gap by closely focusing on this subgroup. As brain maturation continues after reaching majority, young adulthood may be a period as vulnerable as adolescence in terms of frequently experiencing pain and coping strategies. Particularly, when considering highly dynamically changing demands in every aspect of life during young adulthood (Tamnes et al., 2010; Vijayakumar et al., 2018). Adolescence and young adulthood represent a period in which way could be given to prevent long-term (up to lifelong) and (over time) increasing impairment of quality of life and loss of productivity. Further, early appropriate management may contribute to prevent the evolution to chronic migraine (Burch et al., 2019; Orr et al., 2019; Sillanpaa and Saarinen, 2018).
We are scoping at revealing relevant topics for educating adolescent and young adult migraine patients in terms of lifestyle habits that may interfere with their condition. In particular, data of young adults are descriptively compared to data of adolescents suffering frequent episodic migraine as well. Based on the knowledge about habits of patients in that age, responsible healthcare providers can provide an informed education. The closer the recommendations fit everyday experiences and challenges young patients are facing, the better their compliance may be.
Aim
The aim of this study was to report on the burden of migraine and the prevalence of several lifestyle factors in a cohort of young adults diagnosed with frequent episodic migraine.
Methods
Study population
This article presents data collected during two different studies previously conducted by our research group. The first study enrolled students in grade eight to 10 from 12 grammar schools (highest level of school education in Germany) in the greater Munich area during a prospective study called Muenchner Untersuchung zu Kopfschmerzen bei Gymnasiasten—Interventionsstudie (MUKIS). All students in the respective grades were asked to fill in a paper-based survey if students and legal guardians gave informed written consent. During November 2011 and January 2012, 1674 participants aged 12–19 years completed the questionnaire during a regular school lesson in their classroom (n = 937 [56%] women). Aim of this previous study was to assess the effects of a 60-min educational intervention on the prevalence of primary headaches. Therefore, classes were randomly assigned to a control or an intervention arm. Students in the intervention group received an educational lecture on lifestyle risk factors for headaches, instructions for stress management, and physiotherapeutic exercises for relaxation of neck and shoulder muscles. Headache cessation was assessed 7 months later on behalf of a re-survey (Albers et al., 2015a).
The second study represents a clinical study evaluating effects of repetitive peripheral magnetic stimulation (rPMS) applied to myofascial trigger points (mTrPs) in the upper trapezius muscle in a cohort of young adults suffering episodic migraine (all students, recruited via the University of Munich, Germany) (Renner et al., 2020). During this study, 37 patients (19–35 years of age, n = 36 [97%] women) have been asked to answer a subset of the questions of the MUKIS study. Inclusion criteria applied during this rPMS study were (1) age between 18 and 35 years, (2) migraine (according to the German version of the headache questionnaire modified according to the ICHD, 3rd edition (IHS, 2018)), (3) at least one active mTrP in one of the upper trapezius muscles (identified by a physiotherapist specialized in manual palpation of mTrPs), and (4) no metallic implants (e.g., pacemaker and cochlear implants). Exclusion criteria were (1) any neurological disorder except for migraine, (2) intake of any medication for migraine prophylaxis, and (3) pregnancy.
In this article, the results of comparative secondary post hoc analyses are reported. Inclusion criteria for these analyses were age between 15 and 19 years for the group of adolescents retrieved from the MUKIS study and diagnosis of migraine with a frequency of 15–44 headache days during the last 3 months prior to participation in one of the above described studies. Exclusion criteria for this analysis were incompleteness of data available on lifestyle habits and burden of migraine in the paper-based questionnaires.
Ethics
The above described previous studies had been conducted according to the World Medical Association Declaration of Helsinki. Both studies had been approved by the local Ethics Committees (MUKIS study: 356/2011 [ethics committee of the LMU Munich], rPMS study: 313-16 [ethics committee of the LMU Munich] and 152/16 S [ethics committee of the TU Munich]). The rPMS study participants, parents, and all students older than 14 years of the MUKIS trial had given written consent to participate in the former studies. Both studies had been registered to the German Clinical Trial Register: MUKIS DRKS00003308 and rPMS study DRKS00019870.
Assessment of migraine, burden of migraine, and lifestyle factors
To assess for the type of headache, the German version of the Headache Questionnaire modified according to the ICHD was applied in the two previous studies. The individual burden of migraine was studied based on migraine frequency and intensity as well as the disability due to migraine on a 3-month basis (assessed by the Pediatric Migraine Disability Assessment [PedMIDAS] in MUKIS and the Migraine Disability Assessment [MIDAS] in the rPMS trial) (Albers et al., 2015a; Renner et al., 2020). Disability grading scores were determined separately for both age-groups (as described previously). Questions to assess lifestyle factors (consumption of coffee, caffeinated drinks, and alcohol; smoking; physical and athletic activity; and sleeping habits) and their dichotomization have been published previously (Albers et al., 2015a). This questionnaire is available as supplemental file.
Statistical analysis
Characteristics of the study sample were calculated for adolescents and young adults, including median with interquartile range (IQR), median differences and 95% confidence intervals of differences, or proportions with absolute numbers and risk differences with 95% confidence intervals. Post hoc analyses of differences between age-groups were conducted using appropriate statistical tests including Wilcoxon–Mann–Whitney tests, chi-squared tests, or Fisher exact tests. R (https://www.r-project.org/, version 3.6.2) and SAS, version 9.4 (SAS Institute Inc., Cary, North Carolina), were used for calculations. p-values < 0.05 were assumed as statistically significant. As this is the first exploratory analysis of its kind, no established point estimates could be referred to when setting up the statistical protocol. The proforma null hypothesis was that there is no difference regarding burden of migraine and prevalence of lifestyle factors between the two age-groups, respectively.
Results
Study population
Data of 27 adolescent participants of the MUKIS study and 37 young adult participants of the rPMS study could be included in these comparative secondary analyses. The median age (IQR) of adolescents was 15 (1) years, and 82% (n = 22) of adolescents were female. The group of young adults included 97% (n = 36) women and the median age (IQR) in this group was 25 (6) years.
Burden of disease
Characteristics of the study sample and migraine-associated disability assessed by the Pediatric Migraine Disability Assessment (PedMIDAS; adolescents) and Migraine Disability Assessment (MIDAS; young adults). Disability grade by total scores was rated as Pediatric Migraine Disability Assessment: 0–10, none to little; 11–30, mild; 31–50, moderate; and > 50, severe and MIDAS: 0–10, none to little; 6–10, mild; 11–20, moderate; and >20, severe. Statistical analysis aimed to assess for statistically significant differences with regard to the burden of migraine perceived by adolescents compared to young adults suffering from the disorder.
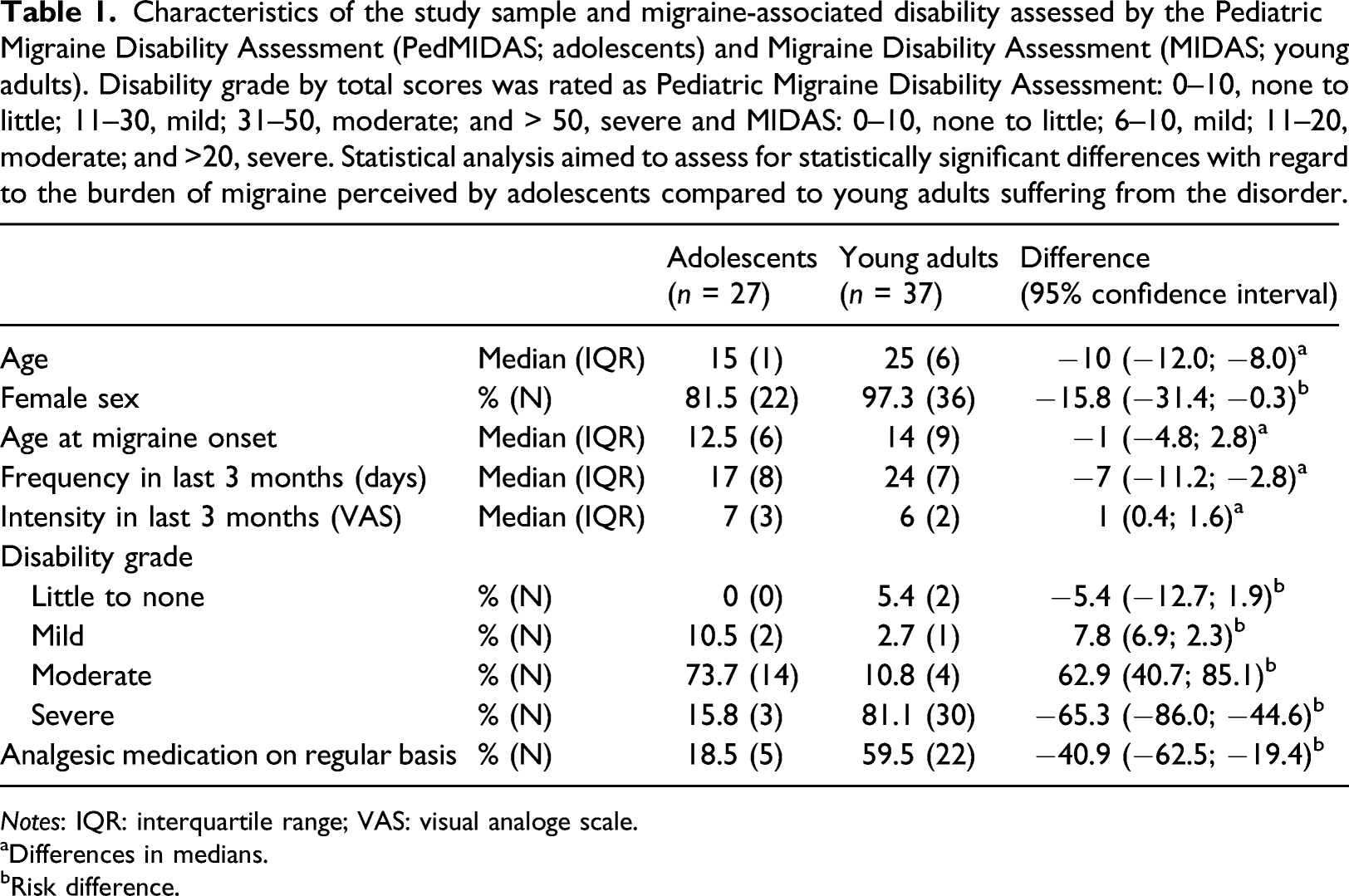
Notes: IQR: interquartile range; VAS: visual analoge scale.
aDifferences in medians.
bRisk difference.
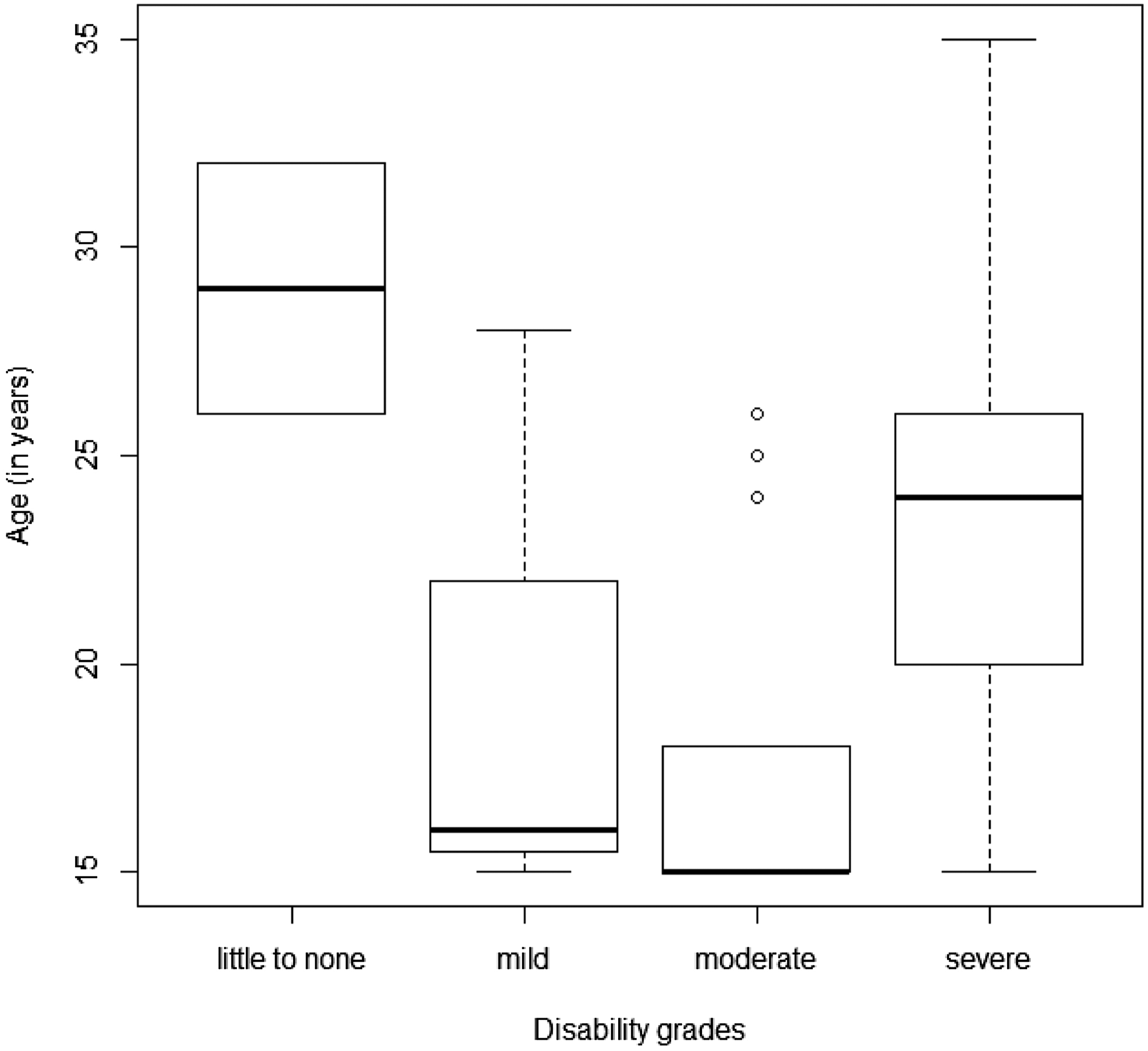
Age distribution of disability grades assessed by PedMIDAS (MUKIS; adolescents) and MIDAS (rPMS trial; young adults). Group none to little N = 2 (mean age 29 ± 4.2), mild N = 3 (mean age 19.7 ± 7.2), moderate N = 18 (mean age 17.6 ± 4.2), and severe N = 33 (mean age 23.9 ± 4.8); ANOVA p > 0.05. Disability grade by total scores was rated as PedMIDAS: 0–10, none to little; 11–30, mild; 31–50, moderate; and > 50, severe and MIDAS: 0–10, none to little; 6–10, mild; 11–20, moderate; and >20, severe. Notes: PedMIDAS: Pediatric Migraine Disability Assessment; MIDAS: Migraine Disability Assessment; MUKIS: Muenchner Untersuchung zu Kopfschmerzen bei Gymnasiasten—Interventionsstudie; rPMS: repetitive peripheral magnetic stimulation.
Medication on a regular basis
A threefold higher proportion of adults reported intake of analgesics on a regular basis (19% [n = 5] of adolescents vs. 60% [n = 22] of adults; p = 0.002; Table 1).
Lifestyle habits
Lifestyle factors in adolescents and young adults with migraine. Physical activity was rated low in case of less than 2 days physical activity of at least 60 min. Statistical analysis aimed to assess for statistically significant differences in the prevalence of the different lifestyle factors between the two age-groups.
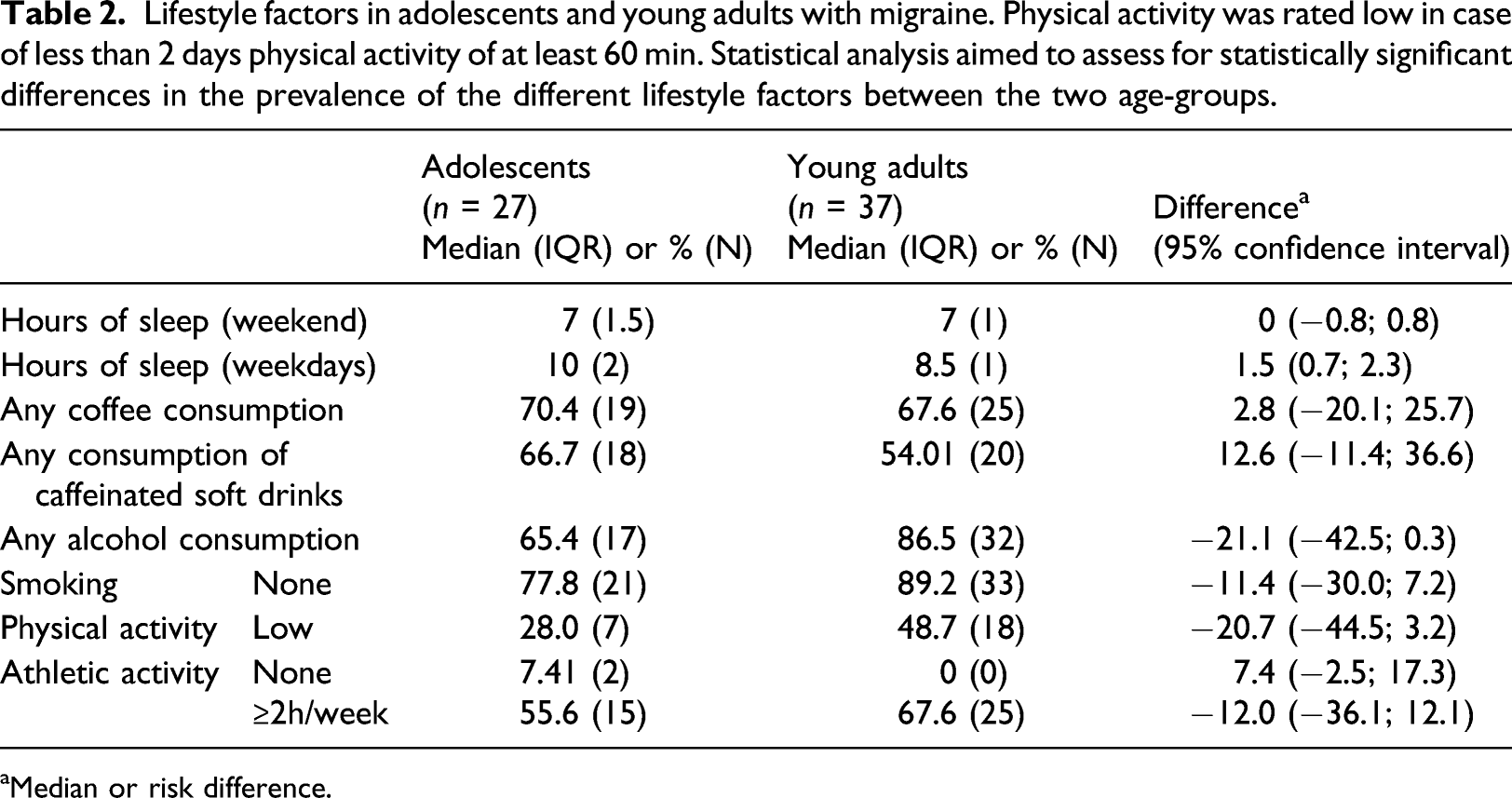
aMedian or risk difference.
Discussion
In this study, the burden of migraine and several lifestyle factors in a cohort of young adults diagnosed with frequent episodic migraine have been reported and descriptively compared to data of adolescents who suffer frequent episodic migraine as well. Young adults experienced a higher burden of migraine assessed by the disability grade and a higher frequency of headache days but a lower intensity level compared to adolescents. Furthermore, a significantly higher proportion of young adults reported regular intake of analgesics than adolescents suffering from migraine. With regard to lifestyle habits, adults slept less during the week. The likelihood of a low general physical activity was higher in adults. Weekly athletic training yielded at least 2 h in a higher proportion in adults. In addition, a higher proportion of adults reported daily caffeine consumption as well as alcohol consumption. In literature concerning primary headache disorders, the age-group of young adult patients is so far underrepresented. The results presented on behalf of this study are a first step to start filling this gap.
The young adults report a more frequent analgesic intake than the adolescents. On the one hand, this could reflect a more defensive pharmaco-management in the pediatric cohort or even a lack of healthcare utilization (Foiadelli et al., 2018). However, there exists broad consent that acute migraine attacks should be treated by effective medication in any age-group (Marmura et al., 2015; Oskoui et al., 2019b). On the other hand, young adults may treat headache attacks more offensively to limit absenteeism from school, studies, or work. Hereby, they may avoid restricted participation in social and everyday activities.
Despite a higher rate of medication, the reported migraine-associated disability is still high in the adult group. This may reflect a rather unspecific use of analgesics in terms of substance, preparation, method of application, dosage, and time point of intake in line with high rates of self-medication reported previously in adult headache patients (Brusa et al., 2019; Katsarava et al., 2018). These results highlight the importance for young adults suffering from migraine to be sufficiently educated and supported by a healthcare specialist. Consequently, young adults should be as closely in touch with the healthcare provider as migraine patients of other age-groups. Young patients should not hesitate to seek medical advice.
Through all age-groups, lifestyle habits play an important role in migraine (Albers et al., 2013; Hagen et al., 2018; Le et al., 2011; Lehmann et al., 2013; Marmura, 2018; Milde-Busch et al., 2010, 2011). The risk of developing chronic migraine is higher in patients not following recommendations on lifestyle behavior (Burch et al., 2019; Buse et al., 2019; Woldeamanuel and Cowan, 2016). This study reflects a lower duration of sleep during weekdays and a lower level of general physical activity in the adult group. Sleep hygiene (i.e., regular sleeping patterns and adequate duration of sleep [in general >8 h per night]) and general physical activity strongly correlate with the burden of headache disorders and are an integral part of any migraine education program (Fernandez-de-Las-Penas et al., 2010; Fernandez-de-Las-Penas et al., 2018; Klausen et al., 2019; Molarius et al., 2008; Pavkovic and Kothare, 2020; Robberstad et al., 2010; Rosenberg et al., 2018; Roy et al., 2019; Solotareff et al., 2017; Torres-Ferrus et al., 2019).
As daily demands rise during education and early work life, basic self-behavior strategies may get quickly lost of sight or may no longer be feasible. Longer sleep duration on weekends suggests that reduction during weeks is not solely due to maturation processes but may need to be compensated for during weekends. Compared to the KIGSS (German Health Interview and Examination Survey for Children and Adolescents) and DEGSS (German Health Interview and Examination Survey for Adults) data, less adolescents but more adults were physically active than reported by the representative data sets with regard to general activity (Finger et al., 2018; Krug et al., 2013). Athletic activities are still regularly followed by a relevant number of adult patients. In this analysis, both groups reported a higher active proportion than the population-based reports (Finger et al., 2018; Krug et al., 2013).
A higher proportion of young adults occasionally consume coffee and alcoholic beverages. The level of coffee consumption has been associated to migraine symptoms in adolescents (Milde-Busch et al., 2010). Alcohol is usually perceived as an important migraine trigger and to become diagnosed with migraine has been associated with reduced or even stopped alcohol consumption. However, its trigger potential tends to be overestimated (Onderwater et al., 2019). Comparison of alcohol consumption to the above quoted German population-based surveys is not possible as alcohol consumption is documented using the Alcohol Use Disorder Identification Test-Consumption (Zeiher et al., 2018), a measure that was not used in our trials.
Previous studies in adolescent students found no significant correlation between time spent with electronic media and headache prevalence (Milde-Busch et al., 2010). However, as habits have significantly changed in terms of availability of portable devices, access to internet, and utilization of social media, an up-to-date assessment of daily electronic media consume would be reasonable.
Prospective observational cohort data analyses including the transition period from adolescence to young adulthood are warranted to assess unmet needs of young adults suffering from migraine—a subgroup of patients not at all adequately addressed in the literature so far. To fill this gap even faster, available data from some previous population-based studies could be reanalyzed in the light of information collected in groups of young adults (i.e., (Fernandez-de-Las-Penas et al., 2010; Hagen et al., 2018; Le et al., 2011; Molarius et al., 2008; Roy et al., 2019).
Study limitations
Some limitations account to this study. First, small sample sizes and possible selection biases do not allow for a broad generalization of our results. As we intentionally screened for participants with frequent episodic migraine, these results may not comply with findings in patients with less frequent attacks or chronic migraine. Whereas adolescents were derived from a population-based survey study, young adults were intentionally recruited for an interventional trial to treat frequent episodic migraine by rPMS. However, circumstances and lifestyle habits can be considered to be comparable as both studies recruited participants of the highest academic level and in the same region of Germany (students at grammar schools and university). Yet, as both groups are prone to a highly academic background, results might not be generalizable to patients in different socioeconomic and educational settings.
All variables have been assessed by completion of questionnaires by participants on a retrospective basis. This approach reflects common clinical practice in the migraine care setting and has proven to be a reliable measure (Solotareff et al., 2017; Zebenholzer et al., 2016).
In both groups, migraine started in early adolescence; however, we do not dispose of any data on its evolution over time. Furthermore, there are no data available on family history of headache disorders, which reflects a factor that may contribute to lifestyle behavior. We have not asked about sleep disorders; therefore, no assumption can be made in this study about their contribution to the burden of disease. In context of being a common comorbidity in migraine patients and the link to a worse trajectory, this information would be valuable (Barmherzig et al., 2019; Lipton et al., 2019; Solotareff et al., 2017). Finally, more recently emerged lifestyle habits, that is, smart device and social media adherence, should be assessed in forthcoming studies.
Implications for practice
Despite a high relevance of headache disorders in the pediatric population, a considerably high number of patients still do not seek medical advice nor receive gold-standard multimodal care (Albers et al., 2015b). In addition, patients who “grow out” of the pediatric care setting are not only dependent on the continuation of neurological care but are confronted with constantly increasing demands with regard to their graduation, the start of training or academic studies, a change in their life situation (i.e., moving out of the parental home and new social environment), and possibly simultaneous changes in living habits with regard to sleep, meals, physical activity, sport, and caffeine, alcohol, and tobacco consumption.
Lifestyle factors may contribute to changes in migraine susceptibility during this period of life. Adolescents should be prepared as optimal as possible concerning those meaningful stressors, and young adults should have easy access to comprehensive migraine care programs specifically aligned to their needs (i.e., offering telemedicine, remote electronic diaries, smart device applications for lifestyle management, and measure to cope with stress) (Barmherzig et al., 2019; Bougea et al., 2018; Kroon Van Diest et al., 2016; Ramsey et al., 2018). Education on lifestyle habits that interfere with the migraine condition is considered as one of the key features of such multimodal regimens. Therefore, it is important to be aware of pattern of risk factors that apply to the patients’ age-group a healthcare provider is taking care of. The recommendations given are more likely to be effective and taken seriously if they reflect everyday experiences of young adults instead of a “one fits all” strategy.
A comprehensive migraine program specifically designed for adolescent and young adult migraine patients may promote adherence to recommendations and healthcare utilization. Mutual outpatient hours held by child neurologists together with neurologists for patients in their late teen and early twen years could ease transition to adult neurology. Appealingly designed educational material and distribution of information via different kinds of media may represent further key features (Albers et al., 2015a; Klausen et al., 2019; Kroon Van Diest et al., 2016). With regard to lifestyle management, the significance of a well-balanced diet, sleep habits, and physical activity should be addressed. Offers of sports activities together with other migraine patients may foster athletic activity. (Virtual) meetings with peers affected by migraine as well as a kind of tandem setting of adolescent and adult patients may reasonably complement such migraine transition program.
Conclusion
This is a first report focusing on the burden of disease and lifestyle habits in young adults suffering from frequent episodic migraine. It highlights the importance of sustaining medical care longer than the time point growing out of the child neurologist’s care zone. Young adulthood should be perceived as a very vulnerable period as it comes along with many changes to everyday life. Educating those patients on an individual basis, considering as many aspects of their everyday life as possible, should be the goal of any healthcare provider in charge. Comprehensive medical programs for young adults suffering from migraine may achieve a high level of adherence by innovative approaches (i.e., telemedicine, remote electronic diaries, and smart device applications for lifestyle management).
Supplemental Material
sj-pdf-1-chc-10.1177_13674935211008712 – Supplemental Material for Burden of disease and lifestyle habits in adolescents and young adults prone to frequent episodic migraine: A secondary comparative analysis
Supplemental Material, sj-pdf-1-chc-10.1177_13674935211008712 for Burden of disease and lifestyle habits in adolescents and young adults prone to frequent episodic migraine: A secondary comparative analysis by Michaela V Bonfert, Nico Sollmann, Tabea Renner, Corinna Börner, Giada Urban, Paul Schandelmaier, Iris Hannibal, Kristina Huβ, Carmen Parisi, Lucia Gerstl, Katharina Vill, Astrid Blaschek, Helene Koenig, Birgit Klose, Florian Heinen, Mirjam N Landgraf and Lucia Albers in Journal of Child Health Care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MVB’s work is supported by a scholarship by the Bavarian Gender Equality Grant. MNL and FH receive funding by the Federal Ministry of Education and Research for the project Innovationsfonds—project for early intervention of migraine in children. The MUKIS study had been supported by an unrestricted fund of the German Headache Society (DMKG).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.