
Abstract
Retention of staff presents major challenges within children’s palliative care; this has substantial implications for children, families and the nursing workforce. To address this, a programme was undertaken that provided pathways of professional development for senior nurses working in this field. This study reports the views of nurses completing this programme, the overall project manager (PM) and the day-to-day programme lead (PL) as well as factors that influence nurse retention within children’s palliative care nursing. The study drew on an Appreciative Inquiry approach that comprised of interviews with the PM and PL as well as focus groups and questionnaires with senior nurses from the children’s palliative care sector, who participated in the training programme. Thematic analysis of data from interviews and focus groups revealed factors influencing nurse retention: speciality, positivity and making a difference, support, provision of adequate resources, tailored education/professional development and resilience. These themes were supported by the questionnaire findings. The programme was perceived as having a positive influence on nurse retention within the children’s palliative care workforce. In addition, it was felt to be very beneficial in terms of shared learning and development. Participants highlighted the need for similar opportunities in the future.
Background
Palliative care aims to enhance quality of life for patients, who have life-limiting illnesses, and for their families (World Health Organization, 2020); it is based on a holistic approach which includes areas such as pain management and psychosocial support. Palliative care is provided in a range of settings including home, acute hospital wards and hospices – the latter now having become one of the most recognised areas for its provision.
Children’s palliative care services have grown considerably since the establishment of the first hospice (Helen House, United Kingdom [UK]) in 1982, with the UK now having 54 children’s hospice services; these provide care for children with life-limiting and life-threatening conditions, including in-house respite, community outreach and palliative/end of life care. Delivery of safe and effective care is dependent on several factors, not least an ability to recruit and retain staff with appropriate skills; however, palliative care services, including hospices, are facing serious challenges in terms of recruiting and retaining staff (Together for Short Lives [TfSL], 2017).
In 2017, the UK’s nursing regulatory body undertook a survey of former nurses, who had left the register between June 2016 and May 2017; they were invited to indicate their decisions for leaving, other than retirement (UK Nursing and Midwifery Council, 2017). Three top reasons were: working conditions, for example, staffing levels and workload, a change in personal circumstances, such as ill health and/or childcare responsibilities, and disillusionment with care quality provided to patients. In 2016, Together for Short Lives (2017) undertook a survey of nurse vacancies within the UK children’s hospice sector (undertaken because of concerns about the children’s palliative care workforce). Twenty four (62%) of the organisations responded, identifying that the average vacancy rate was over 11%, of which nearly two-thirds were described as ‘hard to fill’. Fourteen (58%) children’s hospices stated that vacancies were having a negative impact including reductions in care allocations to children and families. Overall, this report found that vacancy rates were higher in the children’s hospice sector than other areas of healthcare and that recruitment and retention were becoming more difficult. Together for Short Lives (2017) identified factors that affected recruitment, including workforce issues related to shortages of registered children’s nurses, challenges in matching pay, terms and conditions, geographical locations of inpatient hospice services (giving rise to transport difficulties), shift patterns and challenges in convincing potential applicants to work with children at the end of life.
Several studies have explored nurses’ experiences of working in palliative care and have highlighted factors that may influence job satisfaction and retention and which may lead to workplace stress and burnout (Cope et al., 2016 [Western Australia]; McConnell and Porter, 2017 [Northern Ireland, UK]; Pattison et al., 2019 [UK]); these include workload, leadership/management style, professional conflict and the emotional cost of caring. The impact of workplace stress on recruitment and retention of staff is noted by Kavalieratos et al. (2017) who interviewed twenty palliative care clinicians and reported that common sources of ‘burnout’ included increased workload as well as tensions between palliative care specialists and non-specialist staff. Mu et al. (2019) undertook a systematic review of published articles that focussed on the experiences of nurses, who were providing end-of-life care in paediatric intensive care settings; their work highlighted a particular emphasis on the emotional burden of caring and moral distress arising from the medical futility of care. This concept of the emotional work of nursing was also identified by Van Zyl and Noonan (2018) and Boyle and Bush (2018), who suggest that it can lead to burnout, stress and compassion fatigue.
Aponte-Soto et al. (2005) recognised emotional distress as a factor when working with terminally ill patients in hospice settings, highlighting that it contributed to difficulties in nursing staff retention. Within a children’s context, McClosky and Taggart (2010), in their study of children’s hospice nurses, community children’s nurses and children’s nurse specialists, identified a number of stressors which were considered to be of particular relevance to the context of children’s palliative care; these included the specific emotional demands of this type of nursing alongside the ethical conflicts that characterise it. Authors (including Aburn et al., 2018; Boyle and Bush, 2018; Morgan, 2009) have also identified negative emotional impacts experienced by nurses when caring for children with life-limiting and life-threatening illnesses.
There are a range factors that might enable nurses to stay within the speciality; for example, resilience is widely identified as being important in relation to how nurses may mitigate stress and distress (Jackson et al., 2018; Mu et al., 2019). Other studies have reported a positive relationship between staff support (including education) and retention (Francis and Bulman, 2019; McConnell and Porter, 2017; Taylor et al., 2019; Twigg and McCullough, 2014; Van Den Heede et al., 2013). Training programmes designed to enhance skills, knowledge and professional development within specialities are essential if nurses are to establish a career within a specific field and remain working within it. On this premise, this paper reports on a study that examined a specific training programme within children’s palliative care nursing and the factors associated with nurse retention in this sector.
The project
In April 2017, Children’s Hospices across London (CHaL) were awarded funding by the UK’s Burdett Trust for Nursing to implement pathways of development and training for nurses working in children’s palliative care environments. A CHaL employee acted as the overall project manager (PM). CHaL is a collaborative group of six hospices that support children and young people with life-limiting and life-threatening conditions and their families across all 33 London boroughs and parts of South East England. A 6-month programme was operationalised for senior nurses (who had a managerial role); this comprised of the Mary Seacole (MS) leadership course (https://www.leadershipacademy.nhs.uk/programmes/mary-seacole-programme/) and action learning sets (ALSs) that were facilitated by a day-to day training programme lead (PL), who was also a CHaL employee. The aim was for the nurses to develop their leadership and management skills alongside others working in similar environments; this provided a common understanding of challenges faced, as well as an opportunity to facilitate resolutions, with like-minded people. It was hoped that such a programme would be beneficial to those taking part and would also facilitate professional development for colleagues; therefore, positively impacting on nurse retention within children’s palliative care settings.
Aim
An independent research study was undertaken by the University of Hertfordshire to examine the programme; there was no affiliation with CHaL or any conflict of interest.
The aims of the research were: To report on the views of nurses undertaking the training programme. To examine factors which influence nurse retention associated with children’s palliative care.
Methodology
The research utilised an Appreciative Inquiry (AI) approach. AI enables good practice to be identified as well as allowing change to be introduced and successfully implemented (Shuayb et al., 2009). AI aims to engage key people in strategies that facilitate change, based on participants’ positive experiences (Breslow et al., 2015). Whilst AI was originally designed to support the development of organisations, it has been increasingly used within an education/training context (e.g., Curtis et al., 2017). Cooperrider (2012) states that AI is a method of managing change by drawing on positive experiences of a particular group of people or of an organisation, in this study, the experience of nurses working within the palliative care setting. AI works effectively with small groups of participants who are best placed to lead change (Bushe, 2011); in addition, transformational change emerges when there is a shift in the collective thinking and acting of a specific group, who have shared experiences and ideas (Hung, 2017). AI can also be beneficial at an individual level, as it works to elicit participant strengths (Grieten et al., 2017). This is not to say that challenges and difficulties are ignored; rather, these are acknowledged with an emphasis on learning from less favourable experiences and considering them from a positive perspective (McArthur-Blair and Cockell, 2018).
AI comprises of four stages (Figure 1). The methodology aimed to focus on the positives of working within children’s palliative care by capturing participants’ stories (Discovery and Dream) and highlighting areas for future planning and development (Design and Destiny). Appreciative Inquiry steps (from Cooperrider, 2012).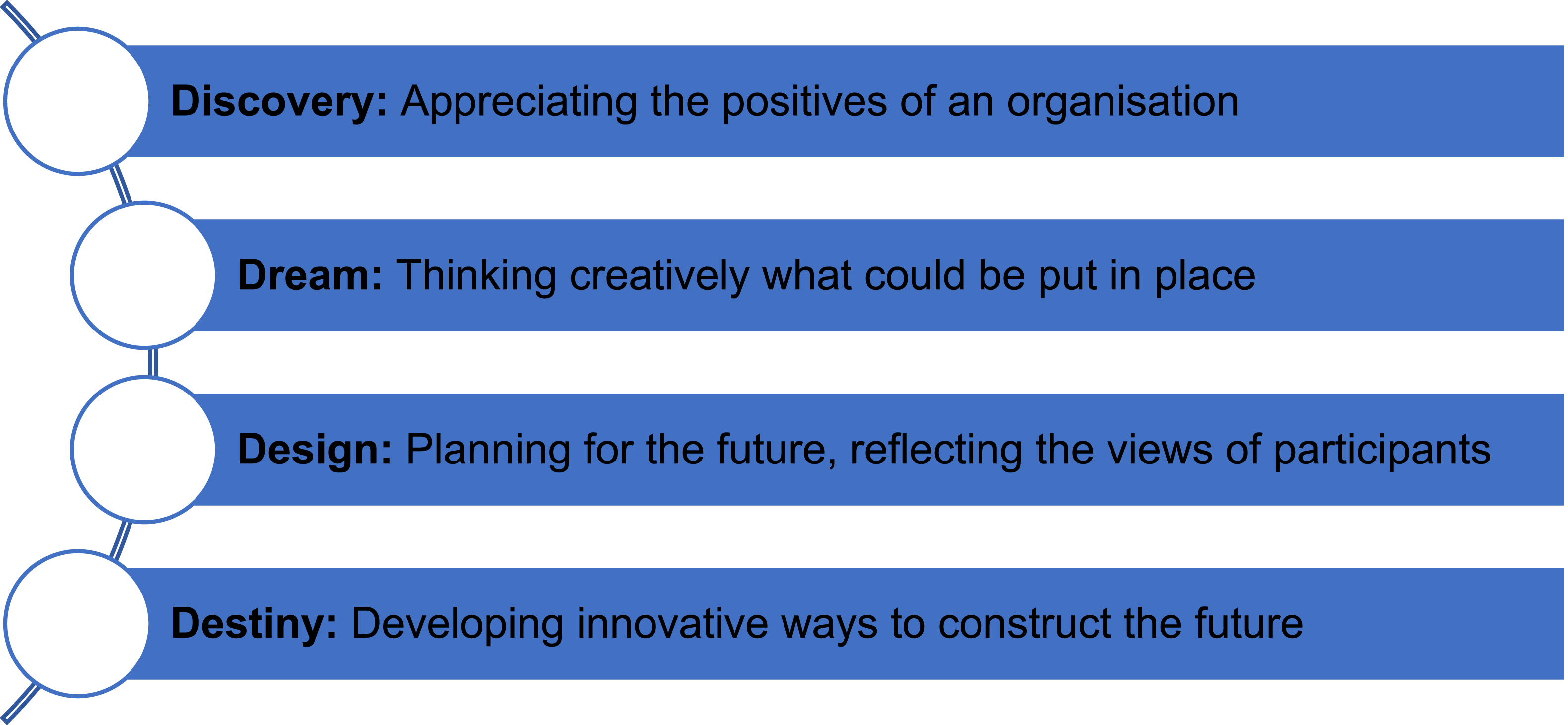
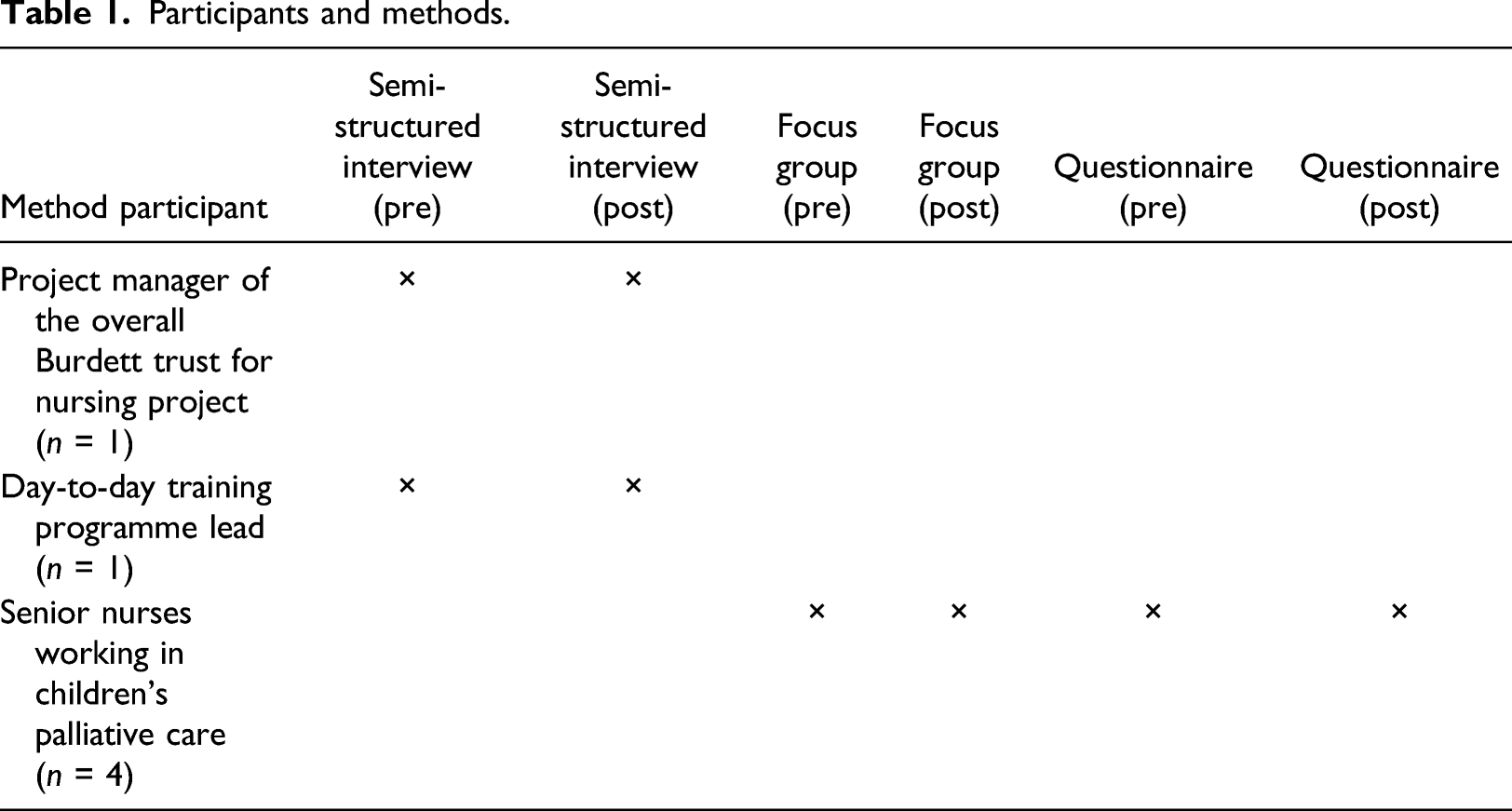
Participants and methods.
Recruitment
A purposive sampling approach was utilised as it facilitates the recruitment of people who possess relevant characteristics (Palinkas et al. 2015). The research team emailed both the PM and PL, attaching a participant information sheet and inviting them to take part in two face-to-face interviews. A similar approach was taken with the four senior nurses who were involved in the training programme; they were invited to participate in two focus groups and complete two questionnaires.
When sample sizes are small, maintenance of confidentiality in reporting study findings requires particular attention. To aid this, all participants were allocated a pseudonym, and care was taken when reporting the findings to avoid recognition.
Data collection and analysis
Open questions were used within the focus groups and interviews to explore good practice and peoples’ positive experiences (see Supplementary Material); a review of the literature facilitated the development of the questions and the meeting of the research aim.
Written consent was gained for each interview/focus group with implied consent being provided for the questionnaires. Interviews and focus groups were recorded and transcribed. All data collection took place between November 2018 and July 2019.
The pre-programme questionnaire (Q1) comprised of 16 questions and the post-programme questionnaire (Q2) 11 (demographic data were only collected in Q1). Both instruments included closed and open questions and Likert scale statements, the focus being the senior nurses’ expectations and perceptions of the programme at its beginning and on completion. The questionnaires were distributed to the participants by a CHaL employee and were completed in their own time.
The focus groups were undertaken by two members of the research team and the interviews by a third person. Interviews and focus groups were treated as a single data set. Transcripts were thematically analysed, drawing on the approach developed by Braun and Clarke (2006): Data familiarisation: Transcripts were reread and audio recordings listened to repeatedly. Initial coding: ‘Labels’ were assigned to each aspect of the transcript that was relevant to the research aim. Searching for themes: The codes were examined to identify key areas. Reviewing of themes: Re-examination of the themes helped to ensure that the final six were a true reflection of the data. Naming of themes: The central tenet was encapsulated. Writing-up of themes: This is presented in the findings section.
Stages 2, 3, 4 and 5 were initially undertaken independently by each of the three research team members who had conducted the data collection; each stage was then collaboratively reviewed. The fourth research member independently evaluated the process.
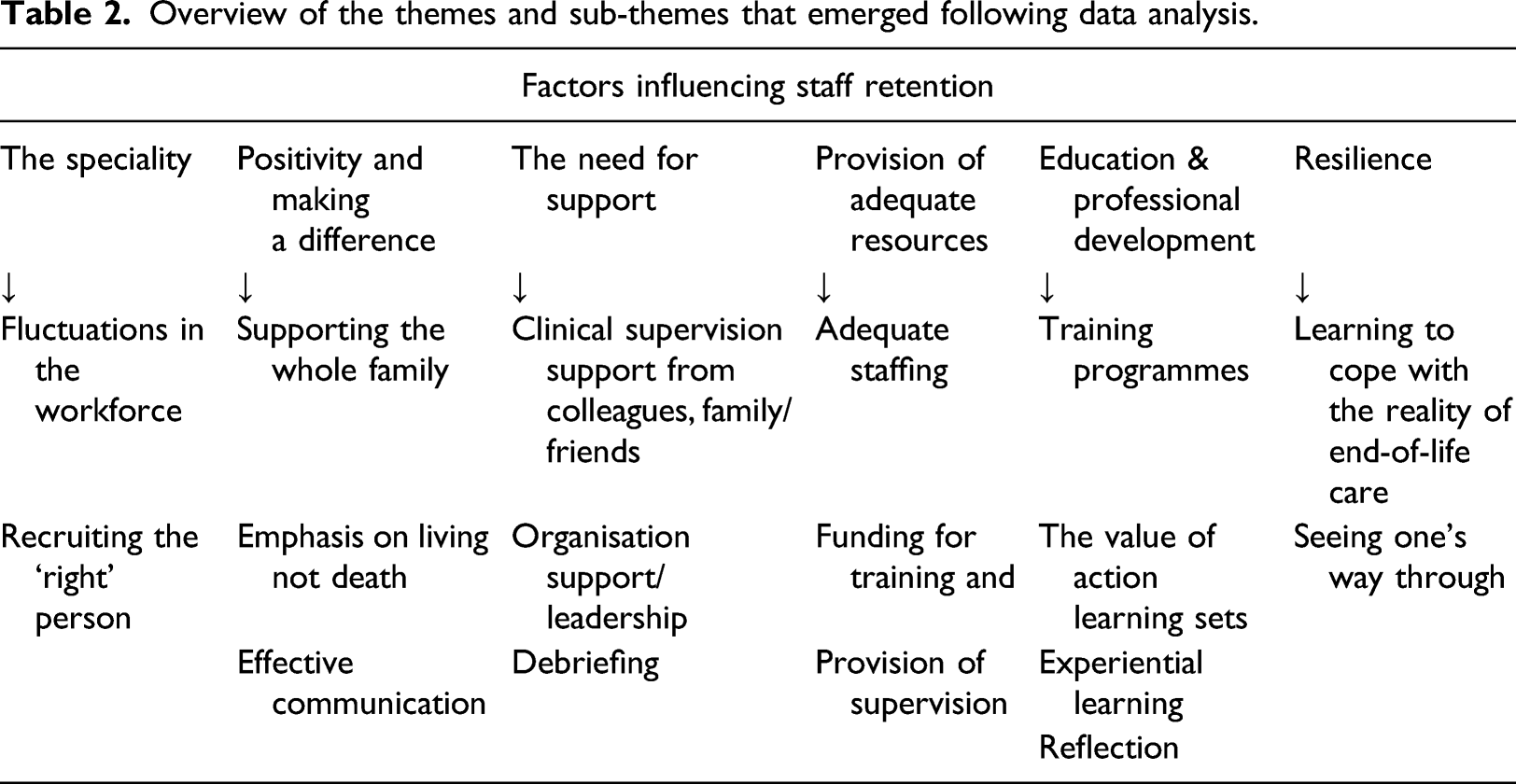
Overview of the themes and sub-themes that emerged following data analysis.
Findings: Interviews and focus groups
Interviews lasted for between 46 and 105 min; the focus groups were 58 and 66 min, respectively. Six themes emerged as a result of data analysis and are discussed below:
Speciality
Participants recognised the need to both recruit and retain the ‘right staff’ who were suited to the area of palliative care, who have: “passion for this type of work” (Beth).
It was highlighted that it was an area for some, but not others: “Palliative care isn’t for everybody, and you have to respect that as well” (Lottie).
Fluctuations in the workforce were also seen as an issue for all units but particularly the hospice sector: “Recruiting for the hospice is going to be difficult, speaking to my other colleagues in the hospice world, trying to find staff that want to work in hospices is really difficult” (Jasmine).
Positivity and making a difference
The senior nurses expressed positivity around being a palliative care nurse and were proud of their job, wanting to emphasise that: “it isn’t all about dying....it’s all about life”.
With the environment being: “….so supportive, and the child and the family are the centre of everything” (Lottie).
The positivity was due to being able to have an impact on the lives of children and families at a difficult time: “truly making a difference” (Liz).
The participants expressed great pride and passion about their roles with one describing herself as: “determinately passionate”. “It’s not just looking after the child. It’s the whole family, it’s the memory making, it’s the support after the child has died. It’s very nurturing as an organisation….I think that’s a massive one, being valued as a person” (Beth).
The PM (Jane) and PL (Liz) agreed that there was a philosophy about having time to care, coupled with a sense that staff are valued and seen as a great resource.
The second focus group highlighted the positive feelings towards the programme with one nurse saying the ALSs were: “fantastic” (Fay).
All commented how different they felt following completion of their programme; this was not just personal outcomes, but related to how their positivity had impacted on their team and that they were now able to give good care in a calm environment, supported by positive people and organisations.
Support
All the senior nurses commented on the support provided in their areas and how essential this was for staff. They also reflected on how this was received: “I think working in a hospice is different, it’s very supportive…you’re encouraged to have ideas and you can contribute to the service development, which is lovely’’ (Jasmine).
As well as emotional support, participants recognised the importance of clinical supervision and debrief strategies: “We have group supervision for staff, and we have individual….we have mental health awareness training and we do debriefs after every death.…to make sure the staff are looked after’’ (Jane).
In relation to the training programme, they commented on the overwhelming peer support that had come from the ALSs saying that they had all worked together in order to identify solutions; that was especially important when it can be:
“quite lonely at the top when you have no one to speak to’’ (Jasmine).
Overall, emotional/well-being support was not only very important, but it was recognised that this was done well, facilitating staff to stay working in the sector. There was recognition that working within palliative care does take its toll, emphasising the need for the training programme that they had undertaken.
Provision of adequate resources
The senior nurses highlighted that there was an inequality in provision between hospice and hospital setting: “because you’re working in a very well resourced, well-staffed area, I think nursing and caring staff can become complacent, and forget what it’s like out there in the real world” (Fay).
With this in mind, the PM and PL highlighted a need for joint and rotation posts between children's hospices and acute paediatric units to share knowledge. There was a need for competencies, to share resources, and to find ways to look after staff to retain them in the hospice/palliative care sector: “There are similarities between us but there are lots of differences and it shouldn’t be quite so different...there’s also expertise and knowledge to be shared across organisations” (Liz).
The PL also expressed her views on what was needed to recruit and retain staff: “What would make it attractive would be location, flexibility of shift patterns, support, leadership” (Liz).
Whilst pay scales were highlighted as being important (they can be lower in the hospice sector), one participant recognised the positive aspects of working in palliative care, commenting that it was worth it: “for my mental health and my own development” (Jasmine)
Tailored education and professional development
All of the senior nurses acknowledged that competency training played a huge part in their education provision within their palliative care service and the need to: “upskill and educate everybody as much as we can” (Fay).
There was a great deal of collaboration between the hospices and acute partners in accessing and fulfilling education needs. One nurse commented that: “a lot of it is in-house, or we reach out to other hospices…who have got some amazing in-house training’’ (Lottie).
Overall, participants were extremely positive about the ALSs and the programme: “I would recommend everybody does it” (Jasmine).
There was also an emphasis on professional development and its value in terms of staff retention: “For me, it was about a professional pathway...to further your career” (Beth).
Overall, comments about education included the need to have accredited programmes, enhancement of development opportunities for staff working in palliative care, including bespoke packages for nurses. Competency programmes should be tailored to individuals recognising again that the learning required is:
“not all about death and dying’’ (Jane).
Resilience
Resilience emerged as something that participants felt was important to possess; for example, one participant identified the need: “to be resilient in the face of not enough staff” (Jane).
Liz described how a member of the training programme had started to become more confident, vocal and was able to: “actually have a voice where she didn’t before”.
One comment referred to this being attributed to possible resilience as a factor to enable it: “I think it [the programme] also gives them that sense of self-worth… they probably come with the resilience” (Jane).
The programme was seen to have had a positive impact on the senior nurses’ leadership ability with their personal development being discussed within the second focus group.
Findings: Questionnaires
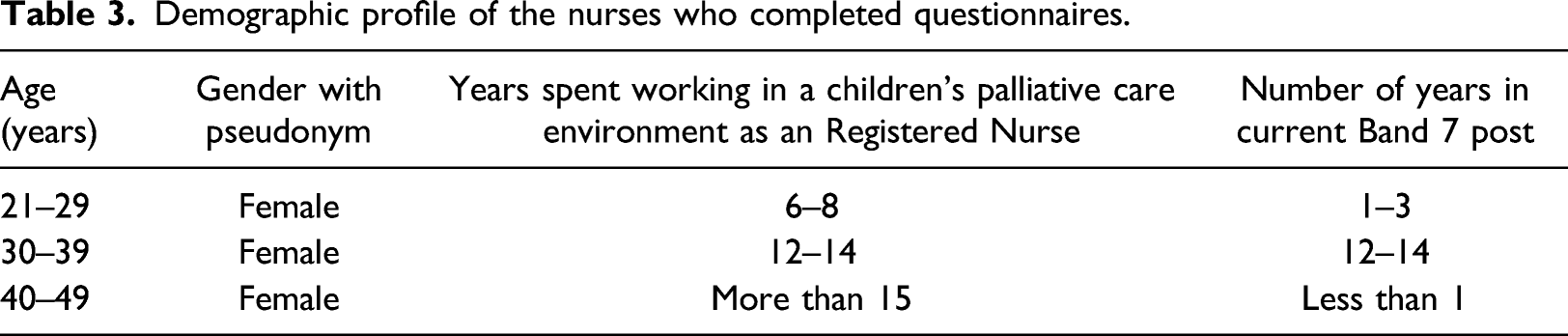
Demographic profile of the nurses who completed questionnaires.
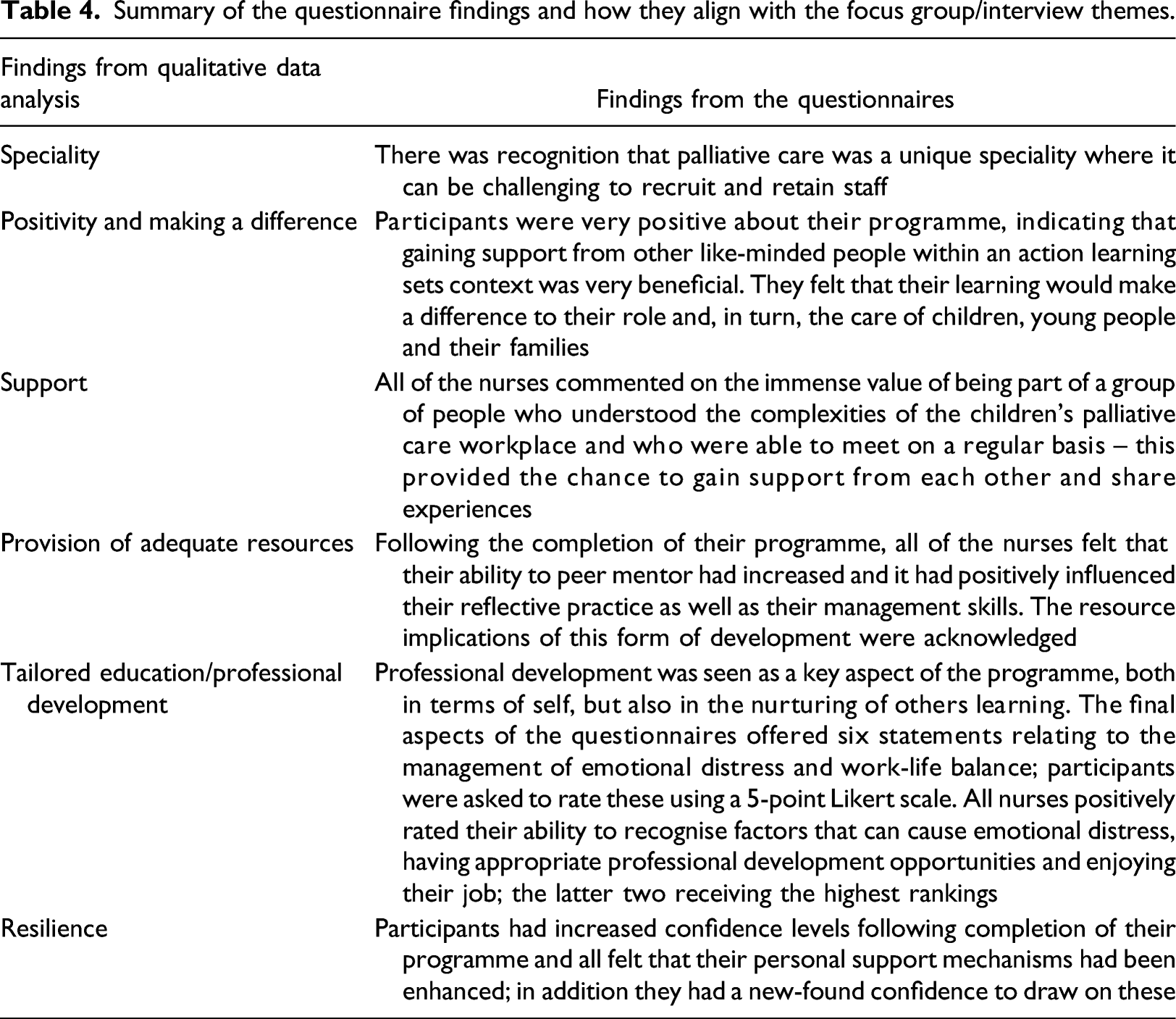
Summary of the questionnaire findings and how they align with the focus group/interview themes.
Discussion
This study utilised data collection methods that comprised of focus groups, individual semi-structured interviews as well as pre- and post-programme questionnaires. Each method offered a valuable insight and important perspective, incorporating the views of participants as well as the PM and PL. However, all data confirmed the value of the programme for individuals as well as the wider palliative care sector.
A range of factors were acknowledged in influencing nurses’ decisions to work and remain working in the children’s palliative care sector. Our research highlighted challenges associated with retaining staff in environments where patients are receiving end-of-life care, concurring with other previous literature. McConnell et al.’s (2016: 916) systematic review focussed on the provision of end-of-life care for children and concluded that:
“more difficulties arise in the hospital setting where the key focus is on short term or acute care.”
Participants in our study also identified this challenge of providing holistic palliative care in the acute hospital setting.
Whilst there are clearly difficulties associated with working with children who are receiving palliative care, one of the key findings from our research was the positivity and passion that staff articulated. Participants thought that those outside of the sector had a more negative view of palliative care –they felt that this meant that parents may be reluctant to consider a hospice option for their child as they may equate it with end of life. However, our respondents highlighted that palliative care focusses on life and living rather than death and dying; they talked about the available resources and alternative therapies as well as holistic care and having more time to spend with children and their families. In addition, they really valued the relationships between nurses, children and their families as well as feelings of reward and benefit from being able to offer a substantive amount of respite provision. Our findings resonate with a range of other literature that acknowledges positive factors that may influence how staff view working in this sector which may, in turn, contribute to staff retention. These align with the themes outlined in Table 2 and include: benefits of experiential learning (Rodríguez-Rey et al., 2019), clinical supervision (Francis and Bullman, 2019; McClosky and Taggart 2010), support of colleagues, family and friends (Cope et al. 2016; Kutluturkan et al., 2016; Slater et al., 2018; Sullivan et al., 2019) and sound organisational support (Jackson et al. 2018; Zander et al. 2013). In addition, participants in both this study, and other work, have reported the development of social and emotional competence (Edo Gual et al., 2015; Gillman et al., 2015) over a long period of time of working within the sector (Bursch et al., 2018; Koh et al., 2019). Opportunities for debriefing were also commonly welcomed (Harrington et al., 2019; McConnell et al., 2016; Pattison et al., 2019) including an embracing of reflection (Jestico and Finlay, 2017; Mirlashari et al., 2017) and effective communication within the care team (Gillman et al., 2015; Kutlurkan et al., 2016; Zysk, 2018).
This study concurs with what is already known about resilience, an attribute identified as potentially playing a part in nurses’ ability to remain working within this field. McAuthur-Blair and Cockell (2018) suggest that there are integral links between leadership, building resilience and AI; they also propose that a leadership journey is ongoing and ever evolving with a resilient leader demonstrating a willingness to deal with challenging situations, but coming through with greater strength and knowledge. Resilience is widely identified as an important factor in relation to how nurses deal with stress and distress (Grafton et al., 2010; Jackson et al., 2018; Mu et al., 2019; Powell et al., 2019). As articulated by participants in this study, resilience is an ability to persevere in dealing with challenges while also adapting, developing, learning and drawing on support mechanisms. Ablett and Jones (2007), who studied nurses working in adult hospice care, suggested that antecedent factors such as resilience and a sense of well-being may be influential in nurses’ decision-making both when entering and when continuing to work in the field of palliative care; whilst Edo Gual et al. (2015) found that emotional intelligence, resilience and self-esteem were important factors in relation to how the participants coped positively with death and dying.
A need for support, professional development and relevant resources emerged as a key finding from our study. Other previous programmes, such as that reported by Slater et al. (2018) have been introduced to address staff retention, well-being and stress related to team culture. Their programme included education, on-site counsellors, mindfulness sessions, debriefing, well-being resources, improved engagement, support and communication; staff reported a positive effect on awareness of self-care, addressing risks to resilience, seeking support from trusted colleagues, coping with critical incidents and the ability to interact positively with patients and families. Other education programmes (Breen, 2019; Edo Gual et al., 2015; Gillman et al., 2015; Klein et al., 2018; Kutlurkan et al., 2016; Slater et al., 2018; Sullivan et al., 2019) have highlighted similar rewards. The benefits of a specific programme were echoed in our study with staff highlighting the value to themselves, their palliative care team as well as children and their families. However, participants in our research also recognised the need to share their knowledge and experience with colleagues, with suggestions of both rotation and joint posts; this is something that warrants further exploration and forms the basis of a recommendation from this work. With this in mind, before turning to the implications for practice, the limitations of the study are acknowledged.
Limitations
It is recognised that our sample size was small and that the findings may not be representative of other similar participants elsewhere; in terms of the questionnaires, it is acknowledged that it is not possible to make statistical inferences or generalisations. The questionnaires relied on self-reporting and this can be associated with response bias (Polit and Beck, 2011); for example, there may have been a tendency for some of the nurses to present a favourable image of the programme. However, the questionnaires (which were completed privately in the nurses’ own time) mirrored the findings from the focus groups, thus adding strength to the data gathered.
In relation specifically to AI design, the positive approach to questioning may prevent participants from addressing crucial problem areas (Shuayb et al., 2009) with the potential for ignoring real issues that need addressing. This may also lead to an imbalance in exploration of views. However, as stated previously, challenges, if addressed in a shared and mutually beneficial way, can have positive outcomes in relation to learning and strengthening one’s ability to deal with them in the future (McAuthur-Blair and Cockell, 2018) – thus, exploring them within an AI approach is a seen as a strength rather than a problem.
Finally, to address potential bias associated with qualitative research with small groups of participants, a high degree of reflexivity on the part of the research team was employed to optimise the trustworthiness of findings.
Implications for practice
In line with AI (Cooperrider, 2012), it is clear that the positives of working within palliative care were valued by the participants in this study (‘Discovery’). Factors that both recruit and retain staff in this sector were recognised. In addition, participants articulated ideas to be put into place (‘Dream’) in respect of planning for the future and innovating (‘Design’ and ‘Destiny’). Strategies were identified to improve recruitment and retention including, as follows: highlighting the availability of flexible working, improved pay (that matches other nursing scales) and attention to the well-being of staff. In relation to staff recruitment, it was felt that those not working in the environment did not have a full appreciation of what it involved and there was a need to: “dispel the myths that are out there and give people a real insight into what it [palliative care] actually is’’ (Jasmine).
In terms of retention, it was important to continue peer support to further increase confidence and assertiveness, to be able to make changes, to learn and use new abilities such as coaching.
Joint posts between the acute and hospice sectors were identified as a strategy that could aid both recruitment and retention as they educate the acute sector about the benefits of hospice/palliative care: “it’s not about going there to die. It’s going there to live as best you can. If you could get these people to different environments, then you break down some of the ignorance around it” (Jane).
In addition, it was felt that joint posts had potential to save money, provide care continuity as well as enhance outcomes for children and families.
Finally, the programme itself made participants feel valued: “collaboration with the other professionals, time to reflect, the growth of our development. We don’t want it to end” (Fay).
It is therefore vital to have a commitment to continue training programmes that include peer support; a key feature for the PM, PL and senior nurses was allowing clinical leaders time to reflect, provide peer support and enthuse them to manage their teams more effectively.
Conclusion
This study sought the views of nurses who undertook a training programme (as well as the managers of it) and also explored factors that influence retention within a children’s palliative care context. An AI approach (Cooperrider, 2012) enabled the emergence of findings that identified positive attributes of working within this sector. This research revealed that staff are dedicated, motivated and passionate about their work; however, in order to retain staff in this demanding environment, they require the infrastructure to support their professional development and emotional well-being. Bespoke programmes, such as those offered in this study, offer a possible solution; whilst they are not without financial and resource implications, they have the potential to facilitate the retention of experienced nurses and impact positively on care for children and their families.
Supplemental Material
sj-pdf-1-chc-10.1177_1367493520971426 – Supplemental Material for Factors influencing nurse retention within children’s palliative care
Supplemental Material, sj-pdf-1-chc-10.1177_1367493520971426 for Factors influencing nurse retention within children’s palliative care by Lisa Whiting, Michele O’Grady, Mark Whiting and Julia Petty in Journal of Child Health Care
Footnotes
Acknowledgements
The authors would like to thank the Burdett Trust for Nursing for their funding as well as all of the participants who gave their time so freely and willingly.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by Burdett Trust for Nursing (Grant no. 10.13039/501100000386).
Ethical Approval
Ethical approval for the study was granted by the University of Hertfordshire Health, Science, Engineering and Technology Ethics Committee with Delegated Authority; protocol number: aHSK/SF/UH/03450.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.