
Abstract
Little is understood about the dynamic circumstances within which the initiation of technology dependence takes place in children. The aim of this scoping review was to identify the influences on the initiation of technology dependence and the issues that require further exploration and consideration. Scientific literature that directly or indirectly discussed the initiation of technology dependence in children was identified. A three-stage screening process of title and abstract scrutiny, full-text scanning and in-depth full-text reading resulted in 63 relevant articles from 1133 initially reviewed. These were then subjected to descriptive and thematic analysis. Articles ranged from the 1970s to the present, reflecting the evolution of ethical debates around the approaches to clinical practice and changes in cultural and societal attitudes. Three themes emerged: how technology alters the meaning of futile care, dissonance in the perspectives of decision makers and increasing support for joint decision-making. Only articles in English and predominantly from the clinician’s rather than the patient’s perspective were included. Societal and cultural factors as well as the structural, financial and cultural environment influence the initiation of technology dependence in children. However, to what extent these overt and implicit influences guide decision-makers in this field remains largely unknown.
Introduction
Little is known about the dynamic circumstances within which the initiation of technology dependence takes place in children, despite the fact that technology dependence is becoming an increasingly common treatment option. Between 1960 and 2011, the mortality rate of children younger than 5 years in 21 countries in Europe, North America, Australasia and Asia decreased from 29 per 1000 to 4.2 per 1000 live births; this was largely attributed to the development of modern paediatric intensive care units (PICUs) (Lozano et al., 2011). The thousands of infant lives saved represent the positive outcome of innovations and advances in maternity care, in early diagnosis and in paediatric intensive care medicine. However, survival measures of seriously ill children fail to describe the gravity of some of the unintended physical, social, psychological and ethical consequences of the technological advances that sustain life, all of which may well influence decisions about whether to initiate or not initiate technology dependence.
Aim
In order to begin to understand the influences on current decision-making around the initiation of technology dependence in a child, we conducted a scoping review to establish what influences on initiation of technology dependence have already been described or discussed in the literature and how these have changed in their significance as technology and society develop. This scoping review asks the following questions: How have decisions around the initiation of technology dependence been approached in the past? And what are the current issues that require further exploration and consideration?
Methods
Identifying the relevant studies
The review took place between April and September 2019. A three-strand search of the scientific literature surrounding technology dependence in children was conducted with the aid of a specialist librarian. Seven key databases were identified to ensure a wide coverage of the literature. (EBSCO)Medline (1946-), CINAHL (1981-), PsycINFO (1990-), (Ovid) Embase (1966-), WHOLiS, Web of Science (1864-) and ASSIA (1970-). Firstly, the databases were scanned to identify appropriate index terms. A secondary keyword search string was then developed. This was populated using lists of synonyms and with input of keywords suggested by the research team, based on key concepts – technology dependence and physical disability, chronic illness and complex care needs. A combination of index terms and keyword search strings was used to create a systematic search. Additional citation and bibliographic searches were conducted on all included studies to identify additional relevant studies for inclusion. All results were exported into EndNote for deduplication and then into Covidence for screening.
The review was intended to provide an understanding of the conceptual, social and clinical environments in which current decision-making takes place, by tracing the history of how life-sustaining technology has been adopted and accepted for use with children as recorded in the scientific literature. Our inclusion and exclusion criteria were, therefore, as broad as possible in terms of subject, but specific in that included articles must describe issues around the initiation of technology dependence for children. In order to establish a level of quality, each article must be peer-reviewed or part of national government report or guidelines.
Study selection
We retrieved 1133 articles and identified a further 78 from hand searching references. After an initial screening of titles and abstracts, 757 articles were discarded. The remaining 454 articles were subject to more detailed analysis to ascertain if medical technology was discussed in the context of children’s care. A brief reading of the introduction and discussion sections of the articles was conducted by two researchers, and the text was searched to determine if any relevant passages were included that would describe decisions around technology dependence for children, even if this was not the main focus of the article. We excluded articles that discussed the long-term management of children with technology dependence if they did not include the initiation of technology. This lengthy process resulted in a further 391 articles being rejected leaving us with 63 articles eligible for the review (Figure 1). Inclusion and exclusion of relevant articles in the scoping review.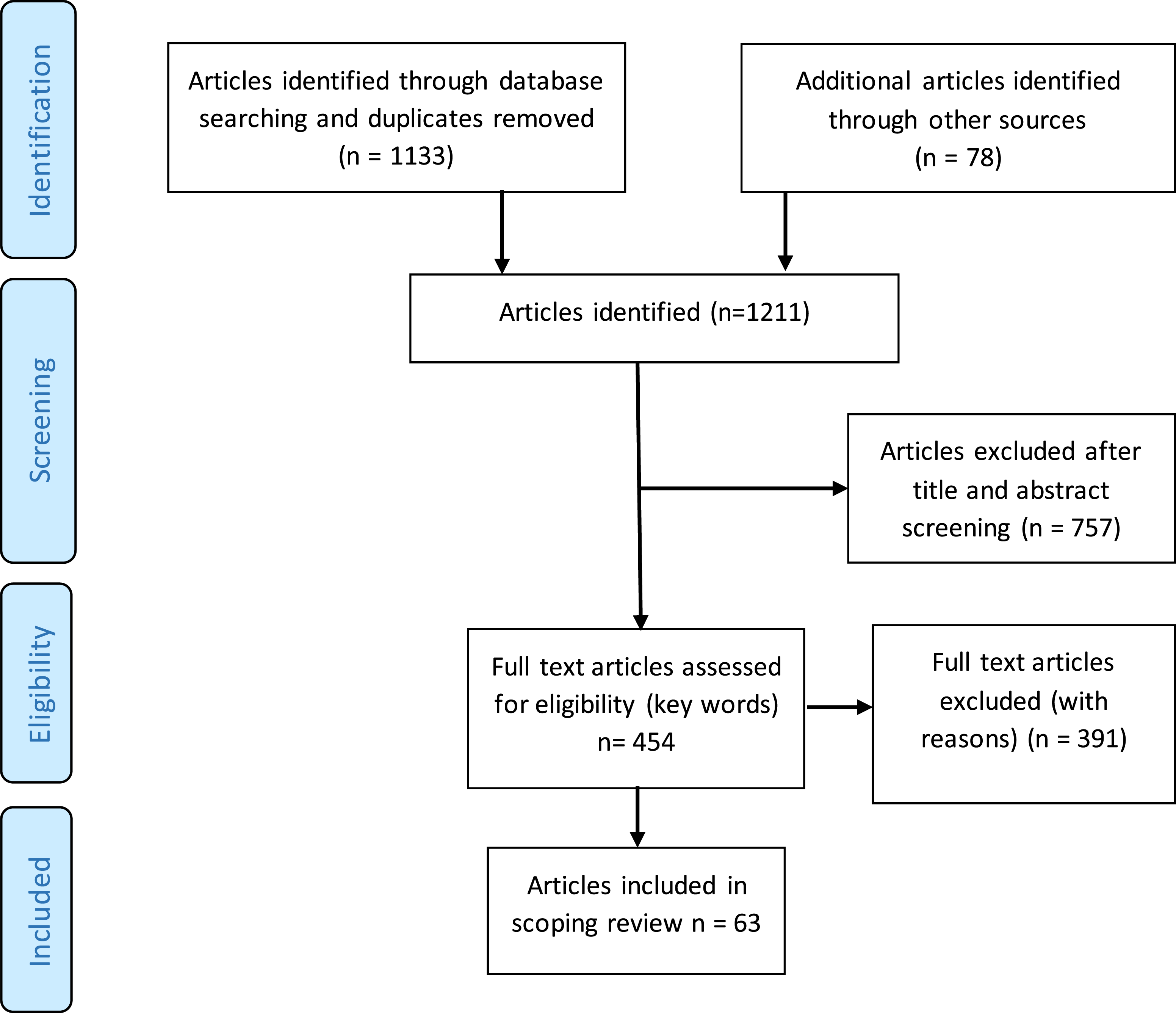
Charting the data
Relevant literature was examined for discussions about how the initiation of technology was approached in each article. In addition, we noted the environment in which these decisions were made; the population groups involved, for example newborns, paediatric patients, or children and adults in intensive care units. Two researchers independently extracted data from the first 6 studies to determine that the approach to data extraction was consistent.
Analysing the data
A descriptive summary of the literature allowed us to place it within a context, and a thematic analysis of the literature identified important or recurring themes. The themes were then analysed to identify any chronological changes in care delivery presented in the literature, including issues such as care priorities, differing approaches to decision-making and any shift in the type of conclusions reached at different times. This also included examination of the importance given to various factors in the decision-making process over time.
Findings
Descriptive summary
The articles ranged in date from the 1970s until the present day, reflecting the development of life-sustaining technology and the growth in paediatric intensive care for children over these decades (Epstein and Brill, 2005; Kelly et al., 2014). The majority of the later articles took the form of reviews, results of qualitative research, or large-scale surveys of physicians or other health professionals. Earlier articles tended to be in the form of bioethical discussion essays or narrative reviews, particularly on the subject of the ethics of using life-sustaining technology and making decisions about children’s futures. Most of the articles’ subjects were children in intensive care units, although some dealt with overall concepts of ethical issues and covered all ages of patients, with reference to children’s needs within the discussion. The initiation or non-initiation of life-sustaining technology was often described in the context of ‘end of life’ narratives. Most articles focussed on neonates in need of technology for survival and the ethical debates that arise from this. The vast majority of the articles originated from and were pertinent to care delivery in the United States, though there were also many from European countries. Few articles were found from Asia (see supplementary material).
Thematic analysis
We identified a subtle but profound change in the approaches to decision-making around life-sustaining technology in intensive care that fell broadly within 3 themes. These were: technology altering the meaning of futile care, dissonance in perspectives of decision-making and the emergence of collaborative decision-making as a solution to the ethical dilemma.
Technology altering the meaning of futile care
The literature shows the emergence of futile care as a concept resulting from the use of medical technology that could sustain a child’s life, but which did not improve the child’s underlying condition. It also refers to technology that could support a child’s life temporarily but ultimately not change the inevitable outcome of death (Brunkhorst et al., 2014; Duff, 1979; Jordan et al., 2018; Morata, 2018; Rivers, 1996; Sundean and McGrath, 2013).
Ethical and legal concerns
The literature of the 1970s onwards begins to explore ethical and legal concerns, particularly as the technology is seen as in danger of outpacing legal clarifications and the ethical norms that previously informed actions (Crane, 1973; Culliton, 1975; Frader, 1979; Hauerwas, 1975; Howard et al., 1977). Emerging as a means of navigating these ethical challenges is a recognition of the value of parent or family contribution to the decision-making process (Crane, 1973; Culliton, 1975; Frader, 1979; Hauerwas, 1975, Howard et al., 1977). Later literature shows physicians attempting to make ethically challenging decisions and changing the way they practice to recognise the input of the child’s family and the consequences for the child. We see the concept of futile care as a result of political struggles about who should make the decision and the amount of information that should be passed on from the medical team to the family of the child (Asch et al., 1995; Cuttini et al., 1997). Ethical concerns emerge that continuing to provide futile care is a violation of good medical practice, even if it is requested by the family (Riviera et al., 2001). The literature from the end of the 20th century more frequently discusses the notion of ‘futile care’ as an eventuality rather than a potential occurrence (Asch et al., 1995; Cuttini et al., 1997) and suggests that technology should be withdrawn once it becomes clear that it is no longer beneficial (Cram and Wheeler, 1995).
Technology and the concept of futile care
Alongside these arguments is a change in the power of the technology itself to influence decisions. Initially, concerns are expressed in the literature that not only has medical technology created the possibility of making a decision about whether a child lives or dies (Crane, 1973; Hauerwas, 1975; Howard et al., 1977; Culliton, 1975; Frader, 1979) but that its presence might become a powerful factor itself, in terms of ‘the technology is there and should be used’ (Howard et al., 1977; Duff, 1979; Frader, 1979). Later literature continues to discuss how technology increasingly makes possible the need for a decision, for example in the lowering of the age of potential viability of newborns (Nguyen and Ho, 2013; Verloove-Vanhorick, 2006). Societal expectations emerge surrounding technology’s ability to preserve life, and there is increased reluctance to deny treatment if the technology exists (Kohrman, 1994; Riviera et al., 2001). This narrative is set against a social discourse of increasing distrust in physicians’ judgements (Carter and Miller-Smith, 2016; Leask, 2005; Riviera et al., 2001), unrealistic expectations of the technology’s potential (Batavia, 2002; Cogliano, 1999; Fontugne, 2014; Leask, 2005) and disputes between the decision makers (Carter and Miller-Smith, 2016; Cuttini et al., 2000; Linney et al., 2019; Riviera et al., 2001; Tripp and McGregor, 2006). Eventually, the term ‘futile care’ becomes burdened with negative connotations (Bosslet et al., 2016; Luce and White, 2009; Walters, 2016).
Fluidity of ‘futile care’ as a term
Futility of care is fluid term, dependent on the complex needs of the child as well as on the interpretations of the (adult) decision makers surrounding the child. Solutions proposed in the literature include relying on the assistance of a hospital ethics committee to navigate these dilemmas (Carter and Miller-Smith, 2016), preventing disputes by developing and respecting advance care planning for children who are old enough to consider such a concept (Horridge, 2015; Lotz et al., 2015) and redefining what futility means in terms of the potential of life-sustaining technology and the future outcomes of the technology-dependent children (Batavia, 2002; Bosslet et al., 2016; Morata, 2018). Renaming futile care as ‘potentially inappropriate care’ allows for the complexities in interpretation of the term to be acknowledged (Bosslet et al., 2016) and notes the difficulty in providing a robust prognosis of very seriously ill or very young children (Batavia 2002; Brunkhorst et al., 2014; Morata, 2018; Sundean and McGrath, 2013).
Dissonance in perspectives on decision-making
Evident in the literature is the increasing dissonance in perspectives amongst those who make decisions about whether a child should become dependent on technology to sustain life, and the profound, and changing, moral conundrums that emerge from this phenomenon.
Need for multiple decision makers
The advent of life-sustaining medical technology identified the need for more than one decision maker (Crane, 1973; Campbell and Duff, 1979; Frader, 1979; Hauerwas, 1975). The recognition that parents should be involved in decisions relating to their children, and later that children should be involved if they are old enough and cognisant enough, stimulates a consideration of the fundamental role of the physician and the role of the parent (Crane, 1973; Hauerwas, 1975; Van der Heide et al., 1998). The traditional roles of physician as clinical caretaker and parent as nurturer for the child are soon found to be inadequate in the presence of life-sustaining technology (Hauerwas, 1975). Wider influences such as future health outcomes, quality of life and family burden force the individuals out of their traditional roles (Campbell and Duff, 1979; Culliton, 1975; Frader, 1979; Rivers, 1996). The combination of more decision makers and the uncertainties of the roles of each decision maker in the light of fundamental decisions about life and death is expressed in the increasing narrative of difficulty in decision-making (Campbell and Duff, 1979; Frader, 1979). As time goes on, technology becomes more available in intensive care units (Bogetz et al., 2015; Epstein and Brill, 2005; Kelly et al., 2014; Paulides et al., 2011) and parents increasingly feel confident in expressing their rights to be involved or determine their child’s treatment (Brinchmann et al., 2002; McHaffie et al., 2001; Samanta and Samanta, 2006; Shooter and Watson, 2000). This occurs by questioning decisions (Samanta and Samanta, 2006; Shooter and Watson, 2000) or discussing options for treatment with the medical team (Brinchmann et al., 2002; McHaffie et al., 2001; Van der Heide et al., 1998) and eventually becoming more and more skilled in caring for their children who have complex care needs (Rennick et al., 2019).
Child-centred solutions
A means of resolving this impasse is articulated in the more recent literature by placing the child at the centre of the decision. The physician becomes the ‘advocate’ for the child (Cuttini et al., 1997; McHaffie et al., 2001) and decisions are made with ‘the best interests of the child’ (Larcher, 2013; Larcher et al., 2015). There are attempts to recognise and discuss the challenges of proxy decision-making for a child and paternalism (Horridge, 2015; Larcher, 2013) or attempting to lessen uncertainty where possible (Horridge, 2015; Lotz et al., 2015; Samanta and Samanta, 2006).
Avoiding disputes
Physicians have used different means to avoid disputes. This includes making unilateral decisions (Campbell and Duff, 1979; Culliton, 1975; Frader, 1979), imparting only some information in order to nudge parents into a particular decision path (Cuttini et al., 1997; Matthews, 1986; Nguyen and Ho, 2013; Shitaya et al., 2018), or not taking parental wishes into account (Milton, 2010; Nguyen and Ho, 2013; Russell and Simon, 2014; Van der Heide et al., 1998). While some parents were satisfied with this approach (Brinchmann et al., 2002; McHaffie et al., 2001), others reported that they were unable to comprehend the meaning or gravity of what they were told (Russell and Simon, 2014) or they interpreted decisions differently to the physicians (Tripp and McGregor, 2006). Most decisions are recorded as being made by physicians (Asch et al., 1995; Cuttini et al., 2000), but increasing percentages of parents interviewed believe it should be, and is, their decision to make (Cuttini et al., 2000; McHaffie et al., 2001).
Moral challenges contributing to dissonance
The ethics of initiating, withholding or withdrawing life-sustaining technology in children are a recurring debate. The literature describes how the moral norms that have guided the medical profession for centuries seem inadequate to inform physicians and parents in making decisions about using technology to sustain the life of a child (Duff and Campbell, 1976; Hauerwas, 1975; Horridge, 2015; O’Brien et al., 2010). Technology has instigated a tension between the traditional focus of caring and the opportunity to preserve life at all costs. A ‘disease-focussed’ perspective prioritises treating or stabilising the condition that leads to the need for technology dependence but risks ignoring the patient (Duff and Campbell, 1976; Hauerwas, 1975) and a ‘person-focussed’ perspective prioritises the needs of the patient and takes into account the quality of life as well as the underlying clinical condition (Duff and Campbell, 1976; Rivers, 1996). In some countries, however, this may contravene legal imperatives to sustain life whenever possible (Bülbül et al., 2015; Campbell and Duff, 1979; Duff and Campbell, 1976; Frader, 1979). Greater weight seems to be attributed to the person-centred model and the guiding influence of the personal values of all the participants in the decision-making process (Brunkhorst et al., 2014; Cuttini et al., 2000; Larcher, 2013; Larcher et al., 2015; Lotz et al., 2015, 2016; Nguyen and Ho, 2013; Sundean and McGrath, 2013). However, there is initial reluctance to admit to these influences (Hauerwas, 1975; Sørlie et al., 2000, 2001). Since the millennium, articles show the emergence of moral distress in health professionals who must act to carry out decisions they do not agree with (Carter and Miller-Smith, 2016; Mekechuk, 2006; Sørlie et al., 2000, 2001). There is also a strong belief in their duty to save the parents any subsequent feelings of regret or guilt (Brunkhorst et al., 2014; Horridge, 2015; Nguyen and Ho, 2013).
Emergence of ‘joint’ decision-making: A solution to ethical dilemmas?
The final theme identified in the literature can be regarded as a consequence of the first two themes and a proposed solution to the ethical and moral dilemmas that exist. Formally sharing decisions has become a standard practice (General Medical Council, 2010; Larcher et al., 2015; Simon et al., 2012) and a partnership between the clinician and the patient or patient’s representatives rather than a hierarchical relationship is often presented as the ideal. However, there remains no clear best option on how to operationalise this when a decision must be made (Larcher, 2013; Milton, 2010; Schneider et al., 2019; Russell and Simon, 2014; Simon et al., 2012; Tripp and McGregor, 2006). The most recent literature expresses the challenges in achieving a mutually satisfactory decision around the initiation or cessation of life-sustaining technology in a child. There is a growing recognition of the impossibility of providing adequate and comprehensive guidance for practice (McHaffie et al., 2001; Sundean and McGrath, 2013; Tripp and McGregor, 2006; Wilkinson, 2011). Much of the scientific literature around technology dependence in children focusses on the facilitators or barriers to achieving genuine involvement or consensus in decisions around life-sustaining treatment (Shooter and Watson, 2000; Tripp and McGregor, 2006). Effective communication and compassionate leadership are increasingly seen as essential skills of physicians (Edwards et al., 2017; Leask, 2005; Linney et al., 2019; McHaffie et al., 2001; Nguyen and Ho, 2013; Sundean and McGrath, 2013; Tripp and McGregor, 2006). The nature of the interaction shifts from the physician informing parents of a decision, to helping them understand why a particular treatment option has been chosen or rejected (Tripp and McGregor, 2006), to focussing on imparting advice to guide parents through a decision process in which they are the ones who make the final decision (Leask, 2005).
Discussion
This scoping review explores the changes of perspective relating to decision-making around the initiation or non-initiation of technology dependence, with particular reference to the unique situation of the child in the intensive care context. It is not a comprehensive history of decision-making. The identified themes of the influence of technology on futile care, dissonance between the decision makers’ perspectives and the aim of collaborative decision-making are interwoven, and the timeline of arguments is not strictly linear. The attitudes and discussions repeat and appear in different forms throughout the decades.
Concept of futile care
A myriad of influencing issues contribute to the emergence of futile care as a concern. Essentially, the literature expresses the struggle to manage the unintended consequences of being given a choice about preventing or postponing death (Banjar, 2017). The initial unease about who should make such a decision is so enormous that it stimulates many discussions about moral dilemmas and questions who should (or has the right to?) make decisions. The difficulty in satisfactorily navigating the moral dilemmas leaves room for dispute and doubt.
As with all the themes, the debate about futility is closely related to a wider context. The intrusion of medical technology into the very personal space of life versus death has allowed the wider society to become more interested in the making of very private decisions (Banjar, 2017). Arguably, this is where long-held tradition meets a new world, and what is needed is a new bioethical code to understand it. The ‘worship’ of technology, in that families pin hopes on miraculous recoveries, future innovation and hope is, as Fontugne (2014) stated, a reflection of wider societal values. Before the 1980s, parents were generally hesitant to sanction the use of life-sustaining technology to save the life of their child; but after that decade, parents were more likely to insist that ‘everything possible be done’ to extend life (O’Brien et al., 2010). There exists a hope, or even an expectation that technology can conquer death; and if it does not succeed, this is a failure of medicine or the consequence of a conspiracy designed to save money or time (O’Brien et al., 2010). When this attitude is placed against the physician’s attempts at medical pragmatism with assertions that the technology will be ineffective, or cause increased discomfort for the child, an apparently unresolvable situation emerges.
From this, we can identify one of the key elements of the literature, that of the difficulty in imparting complex, distressing and in-depth medical information to lay participants in decision-making. This is challenging at any time, but in times of extreme emotional stress is particularly difficult. Societal changes have occurred in the past 50 years alongside the emergence of paediatric intensive care. These include greater respect of the rights of patients and their parents to make decisions about their own health, greater patient education about their health, access to research knowledge and the increasing acceptability of questioning clinical decisions. This implies a recognition of the humanity and fallibility of the medical profession and in this respect can be regarded as beneficial, but this does not make the issues easier to understand and unpick.
Different perspectives as influences on decision-making
A key feature is an increasing narrative of dispute. The nuances of a decision about technology initiation are not binary, a child may live, but with considerable disability, and making the decision to allow a child to die is very challenging. Such choices are well beyond the remit of the clinician alone and involve personal values and principles, which can be different for each involved party. The relationship of parents and physicians both as advocates of the vulnerable child means that strong emotions are involved. Investigating who is the decision maker takes into account the societal shifts in how parents are regarded, the rights of the patient and new perspectives of the qualities of a physician as fallible as well as responsible. The changing parameters of technology, limits of viability and the ability to continue life-sustaining technology at home (Reeves et al., 2006) (although this is not the focus of this article) add to dissonance. The morality and the bioethics of the use of technology to sustain life are an enormous topic in itself. Related to the influences on the initiation or not of technology are the arguments not only of who makes the decision but also the reasons and consequences of the decision. For example Culliton’s (1975) concern that the body might be saved, but not the mind, is echoed throughout amid concerns of futility, no chance of improvement, pain and intrusiveness, and also to issues debating quality of life, the role of childhood and technology and attitudes to death.
Moving towards collaborative decision-making
There is a sense in the literature that the move to collaborative decision-making is a response to the myriad of ethical, clinical and moral challenges that can be posed by the existence and use of the technology. The initial recognition that these decisions are too grave to be undertaken by the clinician alone moves towards an exploration about the degree to which the participants should collaborate and what roles they should take in the collaboration. Alongside this is the wider context of increased recognition of the rights of the patients, including children, to have control over decisions on their treatment and their health. What is also evident in this context is the changing role of physicians from paternalistic, authoritative figures to that of a more inclusive leadership role. An aspect of this is the focus on the need for physicians to communicate effectively with the patient and family, in times of extreme stress, to help them make an informed decision. The success of this aim is variable, and even perhaps unattainable, as evidenced in the disparities between what physicians believe to be the situation and what parents believe to be true (Cuttini et al., 2000).
Achieving a truly authentic and collaborative decision is articulated as a worthy aim, especially in the existing guidelines and frameworks (General Medical Council, 2010; Larcher et al., 2015), but seems to be suspected as ultimately impossible to achieve in much of the literature. The narrative of dispute is present in terms of preventing, managing or resolving differences of opinion by the parties involved. A consequence of this impasse is seen in the concerns about the prolongation of invasive and futile treatment in children and the resulting moral distress experienced by carers. These unsatisfactory outcomes are also ironic, in that the focus of the arguments shifts from ‘the best interest of the child’ to the interests and challenges faced by the adult decision makers, and the child is lost in the muddle.
All of the themes identified are closely interwoven in the complexity of the issue. To some extent they are arbitrary, but they allow us to understand more clearly all the factors that are expressed as arising out of the emergence of life-sustaining technology for children and its increasing use in modern medical care of very sick infants and children. The recognition of patient rights and the changing functions and duties of the physicians are common to all of the themes, in what can be seen as a change in balance of power, but to what extent this is a true change is unclear when just investigating the literature. Another factor is the technology development itself and society’s attitude towards it. This can be seen in the different attitudes towards technology and its use in different countries, for example the finding that children at the end of life are more likely to be dependent on artificial ventilation in the United States than they are in the Netherlands at the time of death (Verhagen et al., 2010). The literature we identified suggests that technology is to be more readily used, and more difficult to withhold or withdraw in the United States than in parts of Europe, perhaps due to increased social expectations of the progress of technology and unrealistic views of its abilities. Joint decision-making is thus a worthy aim, but is it being used as a ‘magic bullet’ to share the responsibility of such enormous decisions?
Limitations
There are a number of limitations to this review. The issues that influence decisions about life-sustaining technologies are profound and complex. Reflecting the complexity of the issue is the vast number of articles we initially retrieved in our search. Screening articles for inclusion is necessarily subjective, and in this review, we undertook two stages of screening in order to identify the most informative articles. We have attempted to be transparent in order to compensate for any bias that emerges. The number of articles retrieved through hand searching was more than we anticipated. This was a challenging topic to search, even with the assistance of a specialist librarian. Many of the nuanced attitudes towards the initiation of technology were contained within broader texts that focus on other aspects of intensive care medicine, ethics or technology dependence, and we could find little agreed terminology to identify these. In addition, we only searched literature in English for this review, which may have also introduced a bias. The issue of equity of access to care was beyond the scope of this review. The literature we identified reflects the societies where life-sustaining technology is becoming increasingly ubiquitous in PICU. Most of the articles we identified originated in the United States. It is entirely possible that a wider linguistic and cultural base would reveal different influences on technology dependence in children.
Most of the literature we identified is from the point of view of the physician, rather than the child who is the person who is the subject of the technology dependence. This is largely due to the fact that the debates presented in the literature on the decision-making are predominantly centred on the adults who act as agents for the child.
Finally, we have identified how the influences are reflected in the scientific literature, and this might not reflect the current lived experiences of physicians in PICU. There is not only a time lag between the research and publication, but it might be that only the more thought-provoking cases or cases where dispute has occurred are explored and published.
Implications for practice
This review is a first step in highlighting an important and yet often under-researched or even hidden aspect of care delivery. What influences a clinician in the liminal space before initiating (or not initiating) technology dependence in a child? A scoping review identifies the known issues around the topic to emerge, allowing pertinent empirical research to be conducted. In addition, understanding the historical bases behind current conventions of care delivery allows greater understanding of why and how decisions are made today, and the grounding of future research conclusions in practice. A greater understanding of the process of technology initiation may well improve communication and successful joint decision-making at this profoundly challenging point of care delivery.
Conclusion
This scoping review examined the presentation of decisions around the initiation of technology dependence in the literature and identified the current issues that require further exploration and consideration. The use of life-sustaining technology is a concept of care that remains poorly researched and poorly understood and is often associated with long-term sequelae for the child and family.
The findings highlighted the importance of the societal influences and of cultural assumptions on the value and initiation of technology dependence. The health system, financing arrangements and funding of technology, is potentially an important influencer, as is the culture of the individual hospital or unit. The socio-political landscape within which technology dependence is initiated is worth further exploration.
Overarching frameworks or guidelines are difficult to create because of the uniqueness of each case. The need for technology dependence for survival itself suggests a complex combination of health issues that will be different for each child. It is imperative that the individual values of the child, family and health professionals are taken into account into any decision alongside the clinical and technological possibilities. With this in mind, there is great value in developing a clear understanding of what influences the initiation of technology dependence to sustain a child’s life.
Supplemental Material
sj-docx-1-chc-10.1177_1367493520961884 – Supplemental material for Approaches to the initiation of life-sustaining technology in children: A scoping review of changes over time
Supplemental material, sj-docx-1-chc-10.1177_1367493520961884 for Approaches to the initiation of life-sustaining technology in children: A scoping review of changes over time by Denise Alexander, Jessica Eustace-Cook and Maria Brenner in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the H2020 European Research Council (grant No. 803051/15591).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.