
Abstract
Chronic fatigue syndrome (CFS)/myalgic encephalomyelitis (ME) negatively impacts the quality of life for children with the condition. Although up to 2% of children have CFS/ME, the bulk of research investigates adults with CFS/ME. Using the PRISMA extension for a scoping review and the work of Arksey and O’Malley (2005), a scoping review was conducted of all relevant peer-reviewed research investigating nutrition, exercise, and psychosocial factors within a pediatric population diagnosed with CFS/ME. Key themes found were nutrition and dietary components, exercise therapy, psychosocial factors, and multifaceted treatment. Nutrition was explored on its own as a tool to decrease symptoms; however, there were very few studies found to examine nutritional deficiency or treatment with those under the age of 18. Graded exercise and resistance training improved fatigue severity and symptoms of depression in adolescents with CFS/ME. Research exploring psychosocial factors of CFS/ME presented attributes that could lead to being diagnosed as well as barriers to treatment. The multifaceted treatment undertaken typically consists of graded activities/exercise, cognitive behavioral therapy, nutritional advice, and family sessions. This has shown to increase school attendance and decrease the severity of the fatigue for adolescents. Minimal literature exploring CFS/ME within a prepubescent population presents the need for further research.
Introduction
Chronic fatigue syndrome (CFS)/myalgic encephalomyelitis (ME) is a serious and relatively common condition characterized by overwhelming fatigue and a decrease in physical and cognitive function (Mackenzie and Wray, 2013; Rowe et al., 2017). Pediatric CFS/ME has a prevalence of 0.4–2.4% (Chalder et al., 2003; Crawley et al., 2011; Crawley et al., 2012; Rimes et al., 2007) in population studies and .06–.1% (Haines et al., 2005; Nijhof et al., 2011) within a hospital setting. ME/CFS affects all ages, ethnicities, and socio-economic status (Rowe et al., 2017). For adults, it has been found that there is a higher prevalence in women (Nacul et al., 2011). Recognition of this disabling condition is increasing and incidence peaks at 10–19 years and 30–39 years (Bakken et al., 2014; Parslow et al., 2017a).
CFS/ME negatively impacts quality of life (QOL) for children (Collin et al., 2016; Mackenzie and Wray, 2013). Physical symptoms such as a sore throat, joint and muscle pain, nausea, heightened inactivity, and sleep dysfunction have been identified in children with CFS/ME (Collin et al., 2015). Other cognitive and psychosocial symptoms include cognitive dysfunction, social isolation, depression, and anxiety (Collin et al., 2015). It is a complex condition; the etiology is unknown, and currently, there is no known cure (Collin et al., 2015; Richards et al., 2006; Rowe et al., 2017).
Studies have shown that dietary, exercise, and psychosocial factors can reduce symptoms and improve QOL (Jenkins and Rayman, 2005; Lopez et al., 2011; Maes et al., 2006; Maric et al., 2014). Thus appropriate nutrition, exercise, and psychosocial management strategies may be beneficial in alleviating symptoms and improving QOL in children with CFS/ME. The objective of this article is to conduct a scoping review exploring current peer-reviewed research investigating these strategies to decrease symptoms of CFS/ME within a pediatric population (aged under 18 years). Therefore, the research question was: What has been shown in the literature investigating management of CFS/ME in a pediatric population within the key areas of nutrition, exercise, psychology and social factors?
Methods
Following PRISMA extension for scoping review guidelines (Tricco et al., 2018) and the work of Arksey and O’Malley (2005), a comprehensive electronic literature search of relevant peer-reviewed journal articles was conducted by the main researcher (SC). Subsequent hand searching of relevant articles and reports was conducted to identify additional literature. Inclusion criteria consisted of peer-reviewed research investigating clinically diagnosed individuals with CFS/ME who are under the age of 18; research exploring nutritional components, exercise and/or physical activity, and lifestyle and wellbeing for children with CFS/ME; and psychosocial factors that may influence the treatment and diagnosis of CFS/ME. Excluded literature investigated individuals with no medical diagnosis of CFS/ME; adults (over 18 years old) with CFS/ME; not peer-reviewed research or commentary/opinion pieces; and research prior to 1994 as this was the date of the published clinical definition of CFS/ME.
Databases used to search were CINAHL, Medline complete, Psychinfo, SportDiscus, PubMed and NICE evidence series. Multiple search terms were used to obtain findings. Such terms included child, adolescent, chronic fatigue syndrome, myalgic encephalomyelitis, CFS, ME, nutrition, trace elements (e.g., zinc, selenium, copper, aluminium, iron, magnesium), supplement, exercise, physical activity, lifestyle, wellbeing, family, treatment, therapy, environment, and psychology. Boolean operators and truncation of search terms were used to obtain a larger amount of the research results that were relevant. Following a comprehensive literature search by SC, the decisions of inclusion of literature were discussed with the second author (JM). As a result, 29 peer-reviewed research articles were used within this review (see Figure 1).
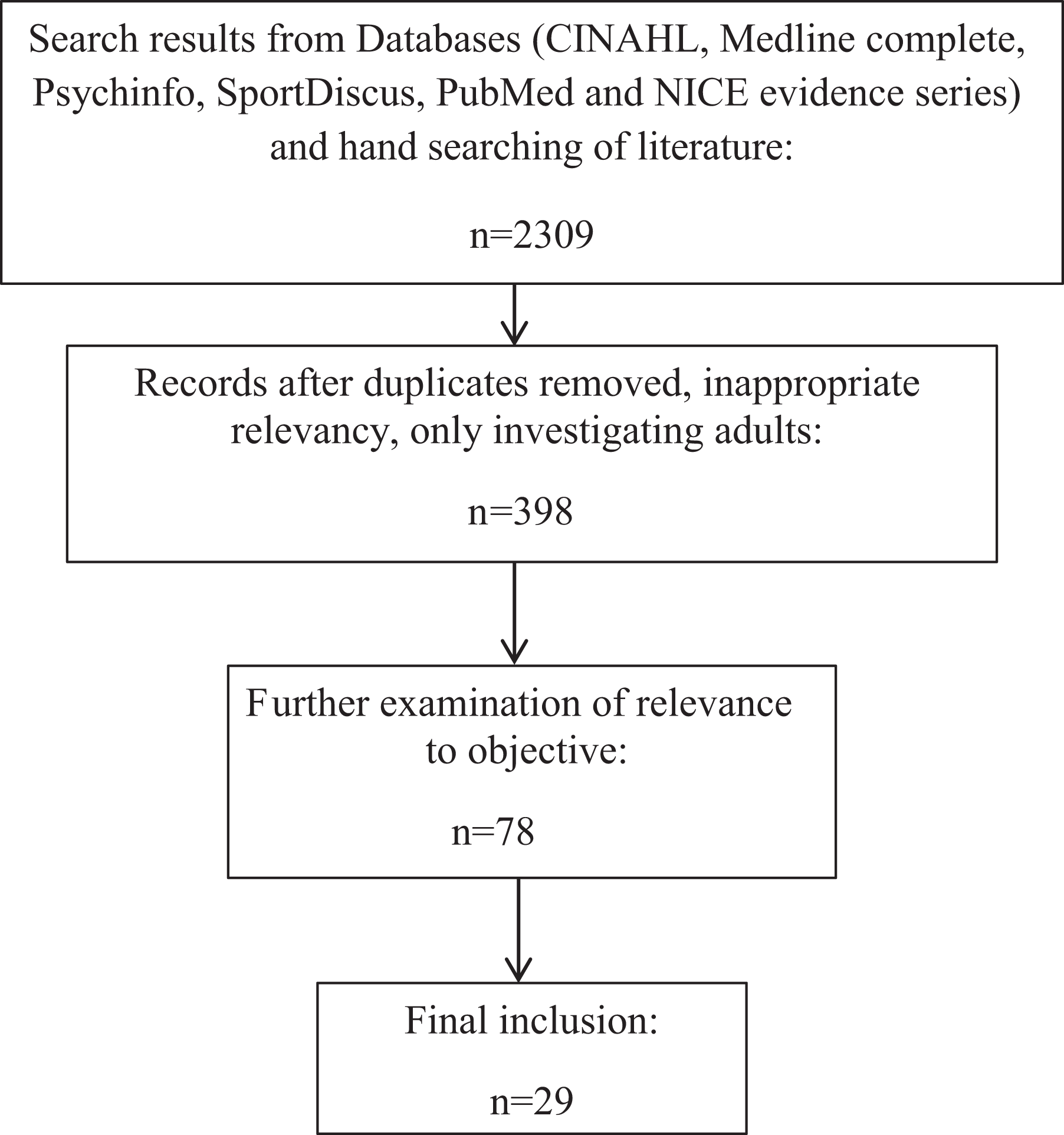
Search strategy and selection process.
Upon finalizing the search, SC developed a data charting form to collate the literature and extract the descriptive characteristics of the studies (e.g., authors, date, title, method, key findings). The finalized data chart was discussed with the co-author and approved (see Table 1). The data extracted for analysis consisted of the participants’ descriptions (e.g., age, male, female), main focus (e.g., nutrition, exercise, psychology therapy, etc.) and results. Once finalized, exploration of the relationships between studies (thematic analysis) was conducted and the strength of the summarized report was assessed (refining and organizing themes to provide an overall thematic summary). This was reviewed by JM and discussed with SC for the final article.
Summary of research included.

Note: CBT: cognitive behavioral therapy; CFS/ME: chronic fatigue syndrome/myalgic encephalomyelitis; RCT: randomized control trial; ALSPAC: Avon Longitudinal Study of Parents and Children; GET: graded exercise therapy; FITNET: Fatigue in Teenagers on the Internet; HRQOL: Health-related Quality of Life; QOL: quality of life.
Results
The initial literature search found 2309 records. Upon removing duplicates, studies only investigating adults, and those that were not relevant to this review, 398 papers remained. Further exclusions in relation to the focus and age of participants initially reduced the total to 78 articles, followed by further scrutiny of age of participants and focus of objective which resulted in 29 papers being included (see Figure 1).
Key themes emerging from the search were nutrition and dietary components, exercise therapy, psychosocial factors, and multifaceted treatment strategies. The research findings (see Table 1) within each key theme are discussed in the following.
Nutritional components and therapy
Few studies examined the influence of diet or dietary modifications on alleviating symptoms (Gibson and Gibson, 1999; Rowe et al., 2016). While included as an integral part of a multifaceted treatment, nutritional interventions were also explored separately as an independent factor which could decrease symptoms. Rowe et al. (2016) investigated the impact of cow’s milk intolerance in adolescents and young adults (10–23 years old) with CFS/ME as a contributor to gastrointestinal symptoms using mixed methods. Adolescents and young adults with CFS/ME had a higher rate of treatable milk intolerance (31%), compared to recent research presenting 6–7% milk intolerance within children of a healthy population (Boyce et al., 2010). Upon implementation of a six-month milk-free diet in the milk intolerant group, the participants’ Health-related Quality of Life no longer significantly differed to the CFS/ME participants who were milk tolerant.
Gibson and Gibson (1999)’s research of a nutritional intervention (wheat-free diet and nutritional supplements (e.g., Co-enzyme Q10, evening primrose oil, magnesium and fluoride) as part of a multifaceted treatment plan) showed a positive impact on improving symptoms after a six-month intervention period. This pilot study presented the first indication that such inclusions of nutritional components could potentially result in a positive impact on the reduction of symptoms for people with CFS/ME.
Harris et al. (2017) used qualitative methods to explore eating difficulties in adolescents (12–17 years old) with CFS/ME. This study found that the eating difficulties commonly experienced by adolescents with CFS/ME were mainly caused by abdominal symptoms, being too tired to eat, and changes in their ability to taste and smell. Psychological symptoms of low mood and anxiety exacerbated these difficulties. Participants expressed interest for interventions through medication and modifying diet, as well as interventions to include families in relation to education in caring for and living with an adolescent with CFS/ME. Furthermore, education and support for those experiencing eating difficulties were one method to ease this experience and thus also decrease the subsequent psychological co-morbidities.
Exercise therapy
Exercise to decrease symptoms of CFS/ME in children under 18 years of age has been explored through various means, for example, graded exercise therapy and progressive resistance training (Gordon and Knapman, 2010; Gordon and Lubitz, 2009). Although exercise has provided both positive and negative results as an effective treatment of CFS/ME in adults (Clark et al., 2017; Larun and Malterud, 2011; Loy et al., 2016; Yoshiuchi et al., 2007), research has shown that cardiovascular exercise and resistance training improve fatigue severity and symptoms of depression in adolescents with CFS/ME (Gordon and Knapman, 2010; Gordon and Lubitz, 2009). Gordon and Lubitz (2009) examined a graded exercise training program for adolescents (mean age: 16 ± 1.25 years) with CFS/ME as part of a four-week inpatient program. Results showed a decrease in fatigue, depression, and mental outlook as a result of the program. Additionally, positive physiological effects (e.g., upper body strength and function improvement) were shown. These results were similar to graded exercise training results reported in adult studies (Gordon and Lubitz, 2009).
Gordon and Knapman (2010) conducted a randomized control trial (RCT) examining the difference between aerobic graded exercise and progressive resistance training for adolescents (13–18 years old) diagnosed with CFS/ME. Compared to baseline measures, results showed no significant difference between the two intervention types in relation to physical capacity and QOL. However, fatigue severity and symptoms of depression improved for those in the aerobic graded exercise group.
Psychosocial factors
Psychosocial factors were also found to impact diagnosis and increase symptoms of CFS/ME (Lievesley et al., 2014; Parslow et al. 2017a; Rangel et al., 2000; Webb et al., 2011). Psychosocial factors are grounded in a psychological and social context. For example, the psychological impact upon the individual of the disbelief about the condition by healthcare professionals and the social impact of being treated as different and abnormal. Webb et al. (2011) found that living with the condition as a child can prevent access to appropriate treatment as the lack of knowledge of the condition (both carers and doctors) was one barrier to access. In addition, negative attitudes and beliefs concerning the condition in children have shown to reduce timely access to treatment and care for children with CFS/ME (Parslow et al., 2017a; Webb et al., 2011). Recent research on healthcare practitioners’ views of the complex nature of the condition and particular aspects of treating/diagnosing children with the condition show the impact having a child with CFS/ME has upon the family, the difficulty in treating symptoms where the child has difficulty in expressing the symptoms and a lack of support from schools in providing a nurturing return to education or environment where the child can work at his/her own pace (Parslow et al., 2017b).
Multiple studies have examined the topic of negative psychological experiences in childhood that could lead to a diagnosis of CFS/ME (Collin et al., 2015; Heim et al., 2006; Viner and Hotopf, 2004). Exploring childhood trauma in relation to an adult diagnosis of CFS/ME, it was shown that through a population study in the United States, childhood trauma was a risk factor for developing CFS/ME in adulthood (Crawley et al., 2013). Furthermore, Collin et al. (2015) explored the risk factor of maternal and childhood mental health in relation to a diagnosis of CFS/ME by 13 years of age. Through parent-completed questionnaires during the antenatal period and regular intervals after birth, this study found that maternal mood (e.g., anxiety, depression) could also be a potential risk factor for childhood diagnosis of CFS/ME (Rowe et al., 2017). However, this was not a clear and direct correlation as diagnosis of CFS/ME could also be a consequence of maternal anxiety and depression altering childhood behaviour, thus creating a risk of developing CFS/ME (Collin et al., 2015).
Rangel et al. (2000) showed no link between gender, age of onset of CFS/ME or symptoms during the worst of their episodes in children with severe CFS/ME and his/her parents over time. However, there was a positive association between low socio-economic status and poor recovery outcome (Rangel et al., 2000). One reason provided was the decreased access to care that could result from having a lower socio-economic status. Other links to poor recovery depended on the timing of the beginning of his/her symptoms (e.g., outside the autumn term) and if it was or was not preceded by a flu-type illness (Rangel et al., 2000).
Multifaceted treatment strategies
A key focus of the research involving children and adolescents with CFS/ME is the examination of interventions to decrease symptoms and improve overall QOL. The interventions reported were cognitive behavioral therapy (CBT), exercise therapy (e.g., graded exercise therapy), dietary amendments and education, and multifaceted therapy (typically included more than one of the above-mentioned intervention types) (Al-Haggar et al., 2006; Ashby et al., 2006; Crawley et al., 2013; Crawley et al., 2017; Gordon and Knapman, 2010; Gordon and Lubitz, 2009; Knight et al., 2013; Lim and Lubitz, 2002; Lloyd et al., 2012; Rimes et al., 2014; Viner et al., 2004; Wright et al., 2005). Key findings presented the positive impact that a multifaceted treatment strategy can have for children with CFS/ME (Al-Haggar et al., 2006; Crawley et al., 2013; Crawley et al., 2017; Gibson and Gibson, 1999; Rimes et al., 2014; Viner and Hotopf, 2004; Viner et al., 2004; Wright et al., 2005).
The multifaceted treatment typically consisted of graded activities and/or exercise programme, CBT, nutritional advice, and in some cases, family sessions (e.g., counselling, education). Research revealed that through comparing multifaceted treatment to supportive care alone, there was a reduction in the severity of the illness, improved school attendance, and higher Wellness scores (Viner et al., 2004). This treatment strategy has shown to increase school attendance and decrease the severity of fatigue for adolescents (Al-Haggar et al., 2006; Ashby et al., 2006; Gibson and Gibson, 1999; Rimes et al., 2014; Viner et al., 2004; Wright et al., 2005). Although there was a positive impact on symptom relief, only two studies were found that examined these treatment programs for those under the age of 10 (Viner et al., 2004; Wright et al., 2005).
CBT was one of the most commonly prescribed psychological therapies used to manage adolescents with CFS/ME (Al-Haggar et al., 2006; Lloyd et al., 2012; Rimes et al., 2014) and deemed the most successful because of its consistent positive impact on overall QOL, school attendance, mood, and symptoms of CFS/ME (Lloyd et al., 2012). CBT was often combined with another therapy tool, for example, the Lightning Process (LP) or biofeedback (Al-Haggar et al., 2006; Crawley et al., 2013; Crawley et al., 2017; Viner and Hotopf, 2004). Crawley et al. (2013, 2017) conducted an RCT of children and adolescents (aged 12–18 years) investigating standard medical care (SMC) which included CBT, compared to SMC plus the LP. Findings showed a decrease in symptoms (e.g., fatigue, physical function, anxiety) over time (6 and 12 months) in the LP plus SMC treatment. As seen in other intervention research, there was also an increase in school attendance by 12 months.
Family sessions were one other inclusion within multifaceted treatment interventions. Viner et al. (2004) showed that including the family sessions within multifaceted treatment (e.g., family sessions, graded-exercise) created a learning tool for the family as well as decreased negative psychosocial influences.
As the positive benefits of a cognitive-behavioral approach have been shown (Al-Haggar et al., 2006; Crawley et al., 2013; Crawley et al., 2017; Knight et al., 2013; Rimes et al., 2014), research has also discussed methods of adapting the treatment through the use of technology. In order to allow increased access to treatment compared to solely face-to-face therapy, telephone-based therapy was examined and shown to be successful in decreasing fatigue and improving school attendance after a six-month follow-up (Lloyd et al., 2012). To increase the uptake and outreach of these programs, the adaption of multifaceted treatment has also led to the development of an Internet-based therapy for adolescents with CFS/ME, which was shown to maintain a similar recovery rate when compared to usual care after a long-term follow-up (1.7– 3.8 years) (Nijhof et al., 2013). Through these multifaceted interventions, there are common threads of nutrition, exercise, and cognitive-behavioral aspects that are embedded in these approaches.
Discussion
This scoping review has shown the range of peer-reviewed literature exploring nutrition, exercise, and psychosocial factors in managing symptoms of CFS/ME, particularly in adolescents. However, there is a lack of research within these areas investigating younger children, specifically those under 12 years of age. The literature included in this review investigated those under 18 years of age, but this also included studies investigating both adolescents and adults. Only two studies were found to use a multifaceted treatment approach with those of a younger age; however, there were fewer numbers of those of a younger age compared to the adolescents that participated. This may be attributed to a lack of recognition of this condition in children as well as the impact of the social support network prior to and upon diagnosis (e.g., children not being believed or the inability to express their symptoms). There are only a few studies exploring CFS/ME within a prepubescent population and this highlights the need for more research within this age group. In this review, a range of instruments, some validated and non-validated, were used to evaluate outcome measures in the included studies. This highlights the lack of agreement of the best instrument to measure CFS/ME symptoms.
To improve CFS/ME treatment in a pediatric population, there are multiple avenues to further explore. There is insufficient evidence for the use of dietary modifications or the use of nutritional supplements to relieve CFS/ME symptoms in prepubescent children. For instance, there have been few studies, small sample sizes, mostly pilot studies, and the nutritional intervention has more commonly been part of a multifaceted intervention. Further research is warranted in children aged under 18 years through appropriately designed dietary modifications or controlled interventions. Studies with larger and younger populations should be conducted to determine if CFS/ME was the direct cause of dietary intolerance (e.g., the development of milk intolerance). Further research in larger and younger (e.g., prepubescent) samples would provide valuable information to determine if there is and/or should be a difference in nutritional treatment strategies for prepubescent children compared to adolescents. Subsequently, this new knowledge could support the development of new approaches to help reduce symptoms in children with CFS/ME.
In relation to exercise therapy, this review provided positive findings for the benefits of exercise for adolescents with CFS/ME in reducing physical and cognitive symptoms and subsequently improving QOL. There remains the need for further research in those diagnosed with CFS/ME at a younger age and subsequently, the impact of such exercise therapy on their symptoms and QOL. Lastly, the combination of possible psychosocial factors presents a need to conduct more exploratory research to support or disprove developing theories as well as add new possibilities to improve recovery and/or prevent the diagnosis of CFS/ME.
These findings reveal the need for further research to understand the effect that dietary modifications or nutritional interventions, exercise therapy, psychosocial factors and multifaceted treatment could have upon the symptoms of CFS/ME in a prepubescent child. As a result, this could lead to a better understanding of how management strategies within these key areas could inform practice to reduce symptoms and improve QOL of children with CFS/ME.
Footnotes
Acknowledgements
The authors are grateful to The Silk Trust for providing the support for this scoping review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Silk Trust.