
Abstract
Referrals to children’s palliative care services typically occur late in the illness trajectory, with many children who would benefit not referred at all. Previous studies report health care professionals’ (HCPs) assessment of various parent-related factors as barriers to referral. We conducted a cross-sectional survey of HCPs working in a paediatric tertiary care hospital in the United Kingdom, with an established paediatric palliative care team, to explore staff perceptions of barriers, knowledge and attitudes, with the aim of developing interventions to increase patient access to palliative care services. Survey respondents evidenced good knowledge of the principles of palliative care in closed questions, but their attitudes expressed in open-text questions and reported reasons to refer to a palliative care service demonstrated an association of palliative care with death and dying. We suggest that the association of palliative care with end of life may be a modifiable factor relevant to late and non-referral and deserving of further investigation and attention in education and training.
Introduction
Children with life-limiting or life-threatening conditions who are referred to palliative care services experience fewer symptoms and less suffering than those not referred (Heath et al., 2009; Wolfe et al., 2008). Guidelines issued by the Association for Children’s Palliative Care (ACT) and the American Institute of Medicine recommend that palliative care be initiated upon the diagnosis of a child’s life-limiting or life-threatening condition (ACT, 2009; Field et al., 2003; Mack and Wolfe, 2006). Such an approach implies an integration of services with paediatric palliative care offered in conjunction with disease-directed care (Bluebond-Langner et al., 2007; Liben et al., 2008).
However, only a minority of children who would benefit from palliative care services are referred (Craft and Killen, 2007; Midson and Carter, 2010), and few of those in a timely manner (Fowler et al., 2006). For example, a large UK-based paediatric tertiary care hospital with its own specialist palliative care unit reported that only 21% of children who died in the hospital were known to the palliative care team (Midson and Carter, 2010). In studying parental experiences of their child’s death in the hospital, the authors noted that some parents would have appreciated earlier preparation on the possibility that their child was going to die. Similarly, low rates of referral to hospice and palliative care services have been observed in the United States (Knapp and Thompson, 2012) and Canada (Johnston et al., 2007). As the rates of morbidity and the proportion of children living with chronic and/or irreversible conditions continue to rise (Fraser et al., 2012; Hoyert et al., 2001; Lenton et al., 2006), it is increasingly important to address this gap, as many families may be missing out on the benefits of paediatric palliative care services.
Several studies (Ahmed et al., 2004) have explored barriers to palliative care, but only a few have specifically focused on barriers to paediatric palliative care (Davies et al., 2008; Junger et al., 2010; Knapp and Thompson, 2012). Of those, the majority have been conducted in the United States where palliative care services for children are funded and organised in a manner that limits generalisation to other countries, particularly the United Kingdom where, in contrast to the United States, health care is predominantly publicly funded. In California, Davies et al. (2008) surveyed 198 nurses and doctors working in an academic health centre. The most commonly cited barriers were uncertainties in prognosis and discrepancies in treatment goals between staff and family members. Knapp and Thompson (2012) surveyed 303 paediatricians in Florida and California. The respondents were asked to rank each item on a list of potential barriers, on the extent to which this presented a barrier or not to palliative care in their experience and practice. Descriptive analysis of the results identified ‘family reluctance to accept hospice or palliative care’ and ‘a perception by families that hospice or palliative care indicates health care professionals are giving up’ as the most frequent barriers to palliative care referral. In contrast, in a study conducted in Germany with 293 general paediatricians, the respondents reported time constraints and lack of resources as barriers to the provision of paediatric palliative care (Junger et al., 2010). Communication with parents, emotional burden and uncertainty with the transition from curative to palliative care were specifically rated as not being a barrier to palliative care by a high proportion (around 70%) of respondents.
In this article, we report on the results of a survey developed to investigate knowledge and attitudes towards palliative care amongst health care professional (HCPs) working in a large paediatric tertiary care hospital in the United Kingdom. The survey was conducted in conjunction with a service development project aimed at informing the development of strategies and interventions to ensure improved and timely access for children and families to palliative care services in the tertiary centre (Craig and Bluebond-Langner, 2010). The purpose of the survey was to provide baseline data on tertiary care staff knowledge and attitudes towards palliative care, with attention to their role in the development and maintenance of barriers to paediatric palliative care services, and to inform future strategies and interventions including education and training. In addition to the survey, we conducted observations of ward rounds to explore how the structure of care and relationships amongst HCPs may impact on referral. These findings are reported elsewhere (Craig, 2011). To the best of our knowledge, this is the first study exploring barriers to paediatric palliative care referral conducted in the United Kingdom.
Methods
Survey design
A survey design methodology was selected as part of the overall project to capture the knowledge and attitudes of a broad spectrum of staff from across the hospital. The survey instrument was developed in consultation with experts in paediatric palliative care following a review of recent literature and consideration of items used in other studies (Davies et al., 2008; Jones and Carter, 2010; Kain et al., 2009; Knapp et al., 2009; St Laurent-Gagnon et al., 2008). Face and content validity of the developed instrument was pretested with a group of paediatric palliative care clinicians (five paediatricians, six senior nurses and one clinical psychologist). Cognitive interviewing (Presser et al., 2004) was carried out with paediatric HCPs from the target population (one paediatrician, one senior nurse and one clinical psychologist). As a result of this input, repetitive questions were removed and other questions were grouped and formatted to improve clarity for the reader. This process resulted in an instrument containing 14 multiple-choice and Likert scale questions (for each question respondents were presented with between 3 and 17 issues or statements to select or rate) and two open-ended questions. The questions covered (1) demographic background; (2) clinical and palliative care experiences; (3) knowledge of and attitudes to palliative care and palliative care services; and (4) confidence in skills related to palliative care provision and referral. Copies of the survey instrument are available on request from the corresponding author.
Survey distribution and study participants
The survey was distributed via email to all clinical staff (n = 923) in a large paediatric tertiary care centre in the United Kingdom, where there is a well-established paediatric palliative care service (McCulloch et al., 2008). The email contained a link to an online version of the survey on Survey Monkey®. Two reminders were sent out at one-week intervals. In addition, paper copies (n = 40) of the survey were distributed to two intensive care unit (ICU) wards of the hospital (paediatric ICU (PICU) and neonatal ICU (NICU)). Those staff who had not already completed an online survey were requested to complete the paper version and return it in an attached stamped addressed envelope. These ICU wards were given this additional opportunity to respond as the palliative care clinical team were planning an intervention where the information provided from the survey would be helpful in the design of the intervention. The overall project was approved as a service development project by the Central London Research ethics committee number 2, 06/01/2011, and as such did not require R&D or research ethics approval (National Patient Safety Agency, 2009). The survey was registered as a clinical audit (Clinical Audit registration 824) in compliance with clinical governance regulations within the host organisation. UK national guidance on ethics in health care research was followed (National Patient Safety Agency, 2009); survey responses were anonymous and respondents were fully informed of the aims of the study and their role in choosing to take part.
Analysis
Descriptive analyses of the responses to the survey were performed with the statistical package for social sciences (SPSS) 18.0. Responses to the open-ended questions were imported into the qualitative software package NVivo and coded using thematic analysis. Two researchers (KT and DRH) independently coded the data and then reached a consensus on emerging themes. The coded qualitative data were interrogated for how they related to barriers and facilitators to referral to palliative care services.
Results
Sample characteristics
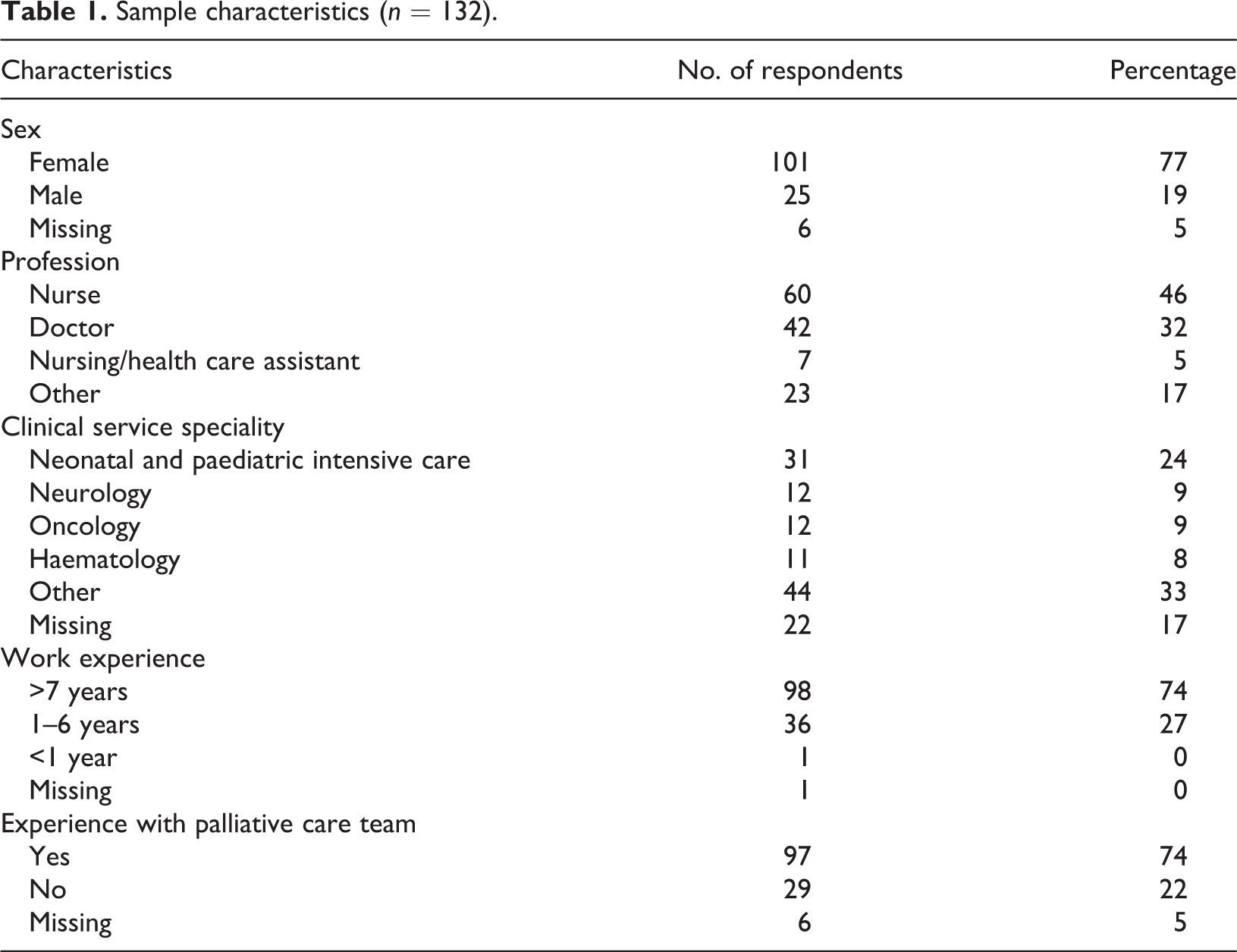
A total of 132 staff members completed the survey, with a 14% response rate (116 online and 16 on paper; Table 1). Survey respondents were primarily nurses and doctors. Other occupational groups included pharmacists, occupational therapists and psychologists. The respondents came from a variety of units within the hospital representing a diverse sample of specialities that look after children with a range of illnesses. The five largest groups of respondents came from ICUs (n = 31), neurology (n = 12), oncology (n = 12) and haematology (n = 11). Seventy four per cent of respondents had been working for seven years or over in their present profession. Seventy four per cent had experience with the hospital specialist palliative care team.
Sample characteristics (n = 132).
HCPs’ views on when to refer
In response to a closed question on when to refer, 48% of respondents reported that children and young people with life-threatening illness or life-limiting conditions should begin palliative care at diagnosis; 9% at ‘disease/stable’; 20% when the disease progresses or reoccurs; 19% when the condition deteriorates; and 4% at the time when the child or young person is at the end of his or her life or dying (Figure 1). No respondent felt that referral should begin after death. In addition, 63% disagreed with the statement ‘palliative care is primarily about providing care at the end of life’ (22% agreed and 15% neither agreed nor disagreed).
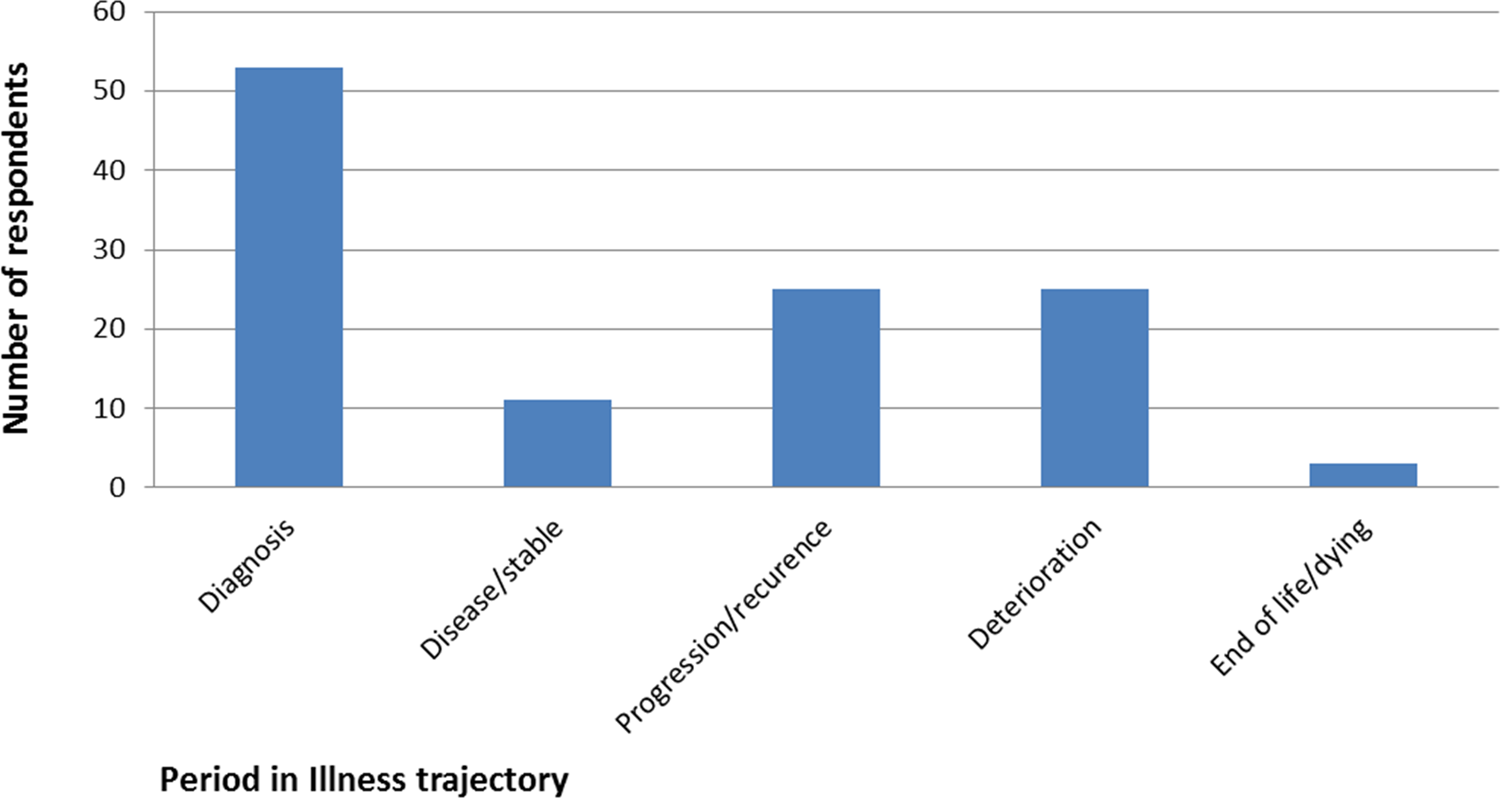
When should palliative care begin?
HCPs’ previous experiences and reasons for referral to palliative care
The majority of respondents (68%) reported making a referral to the hospital specialist palliative care team over the last year. Of those, 20% reported that they regularly referred, 35% that they occasionally referred, and 12% that they rarely referred. The most common reason given for previous referrals (Table 2) was to ‘discuss with the parents the option of the child/young person dying at home or in a hospice’ (49%). Symptom and pain management were also commonly cited as reasons for referral (42–44%). The least frequently mentioned reasons were those related to exploring spiritual issues with parents or young people (3–5%).
Reasons for referring to palliative care services.
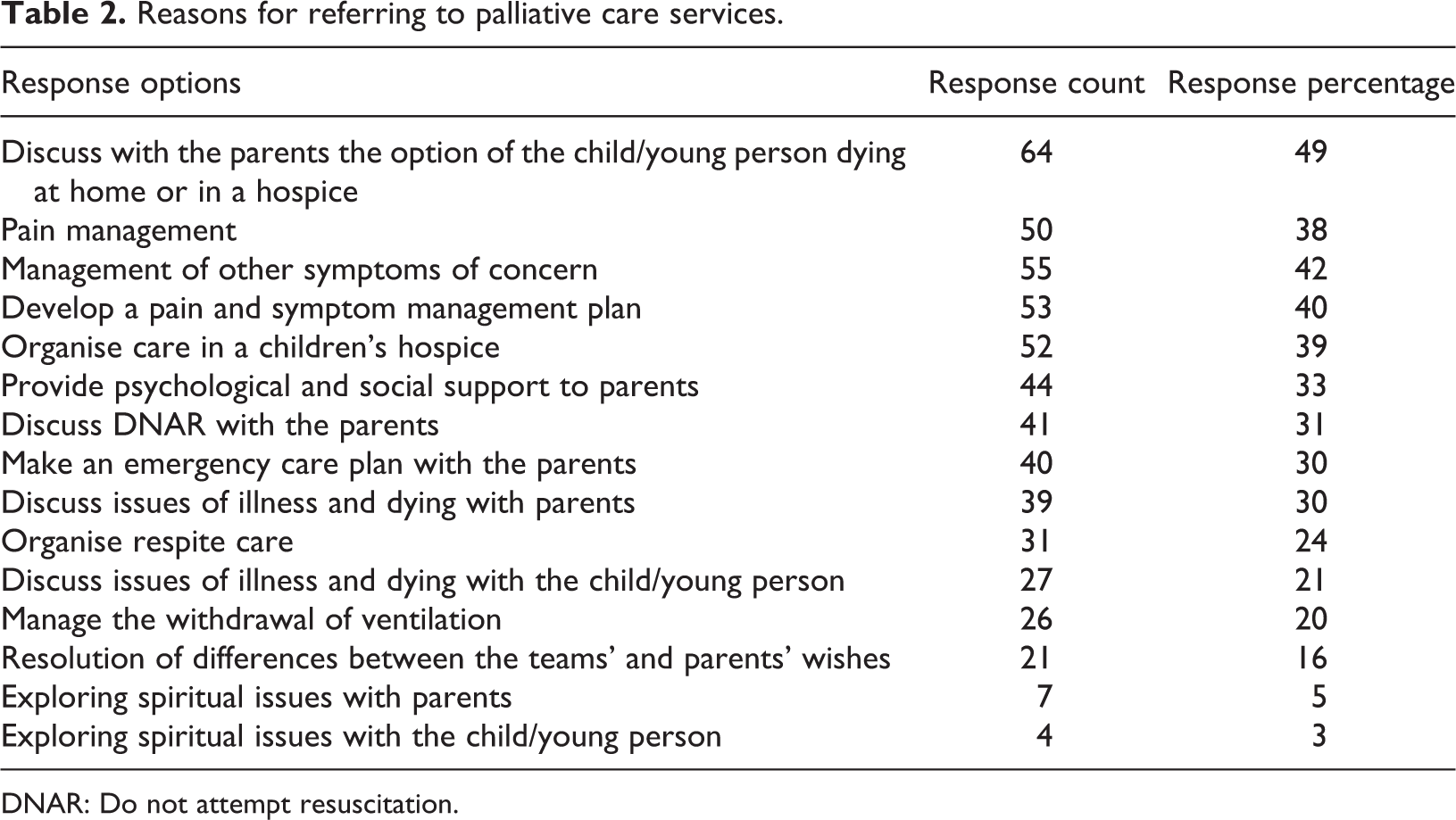
DNAR: Do not attempt resuscitation.
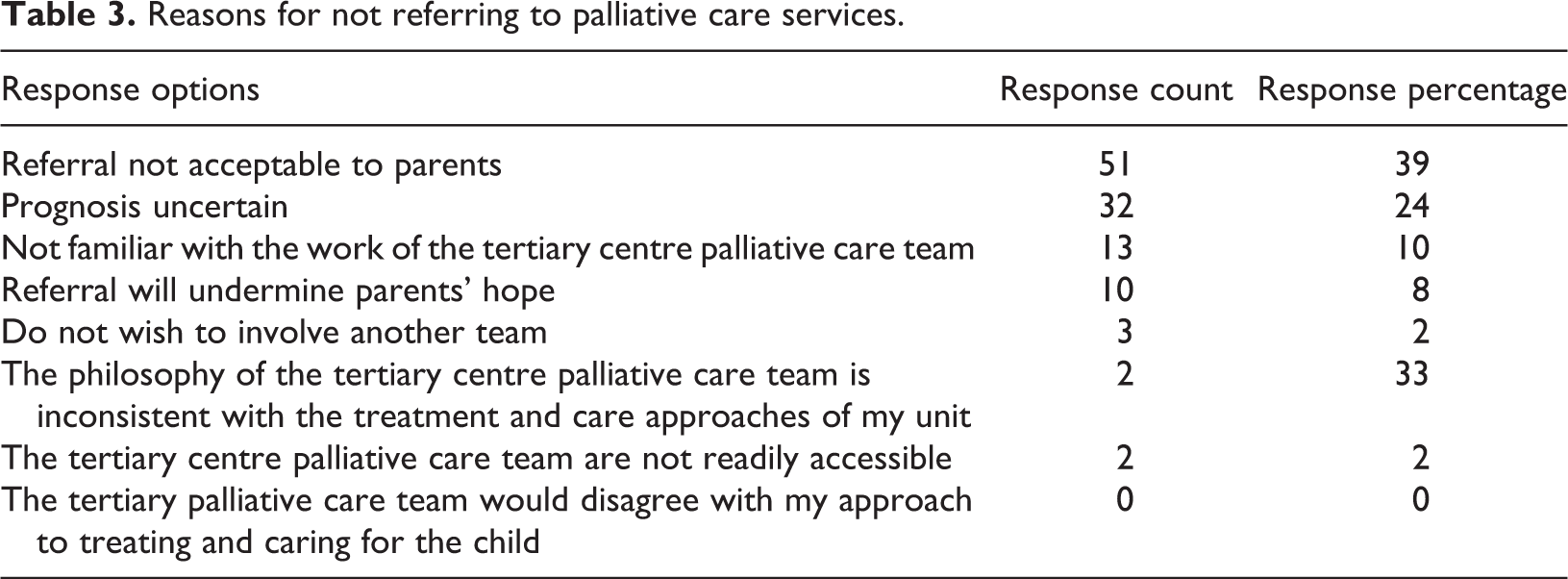
The most commonly cited reason for not referring to palliative care was that ‘referral would not be acceptable to the parents’ (39%; Table 3). Twenty four per cent cited ‘prognosis is uncertain’, 10% ‘not being familiar with the palliative care team’ and 8% ‘referral will undermine the parents’ hope’. Other reasons were cited by less than 3% of the respondents. Of note, respondents from NICU/PICU were more likely to cite ‘prognosis uncertain’ as a reason not to refer (40%, p < 0.05) than the rest of the sample.
Reasons for not referring to palliative care services.
HCPs’ attitudes to palliative care and palliative care services
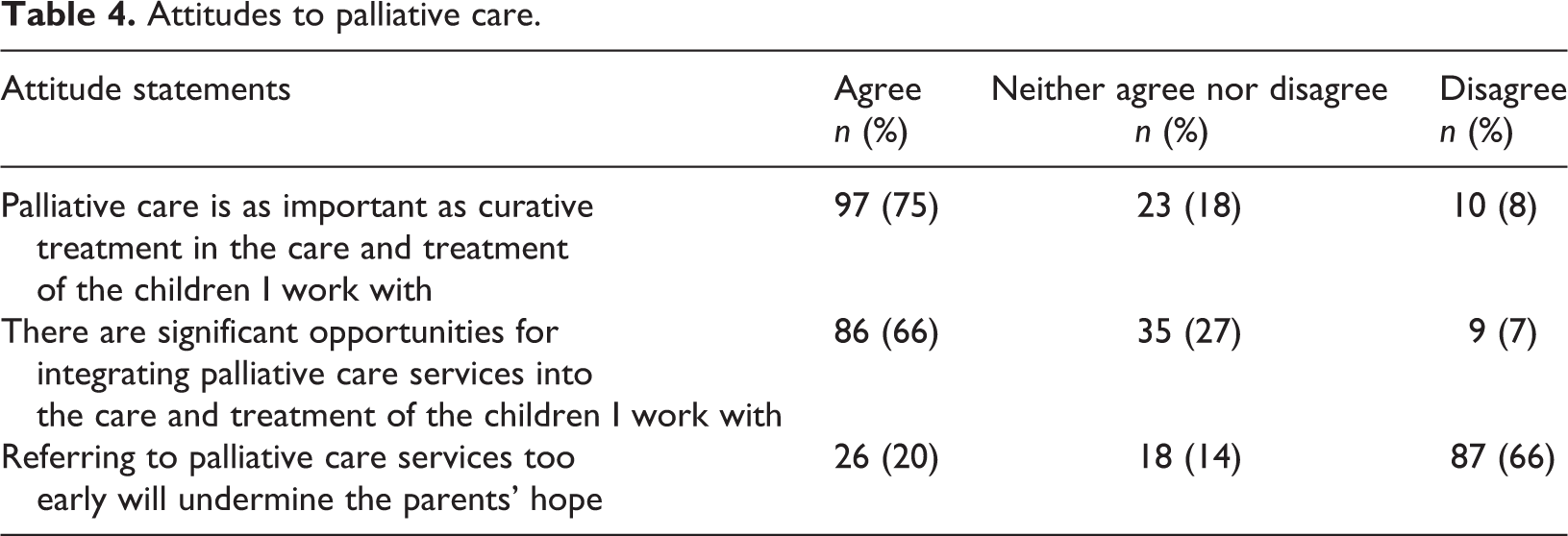
Closed questions on HCPs’ attitudes to palliative care revealed favourable attitudes towards the integration of palliative care (Table 4). Sixty six per cent of the respondents agreed that ‘there are significant opportunities for integrating palliative care services into the care and treatment of the children I work with’; 75% agreed with the statement ‘palliative care is as important as curative treatment in the care and treatment of the children I work with’. The majority (66%) of respondents disagreed with the statement ‘referring to palliative care services too early will undermine the parents’ hope’.
Attitudes to palliative care.
HCPs’ associations with palliative care
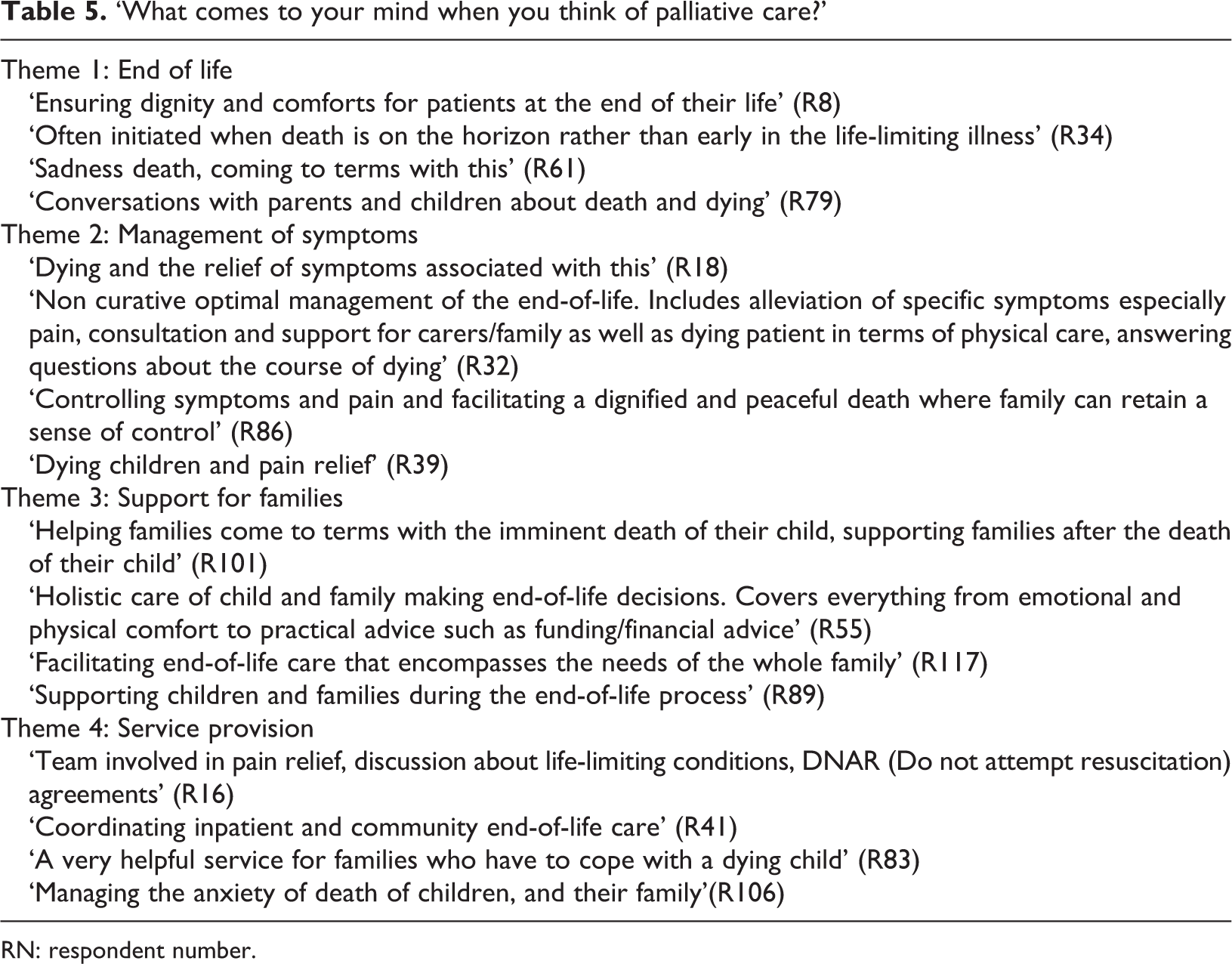
Responses to the open-ended question, ‘What comes to your mind when you think of palliative care?’ however, offered a different perspective. Here the HCP responses indicated a view of palliative care as a service for the end-of-life period. Of the 132 respondents, 120 answered this question. Analysis of responses identified four key themes: ‘end of life’, ‘management of symptoms’, ‘support for the family’ and ‘service provision’. Examples of respondents’ statements for each theme are shown in Table 5.
‘What comes to your mind when you think of palliative care?’
RN: respondent number.
Overall, half of all the respondents (n = 59) specifically cited ‘end of life’, death or dying in their response. Of the 120 responses to this question, 35 only comprised statements about ‘end of life’, death or dying and the issues they associated with this for children, parents and staff.
In addition, while the majority of respondents made statements related to the management of physical symptoms, with pain as the only symptom specifically identified (n = 89), many of these statements were made in the context of the end-of-life period or dying (n = 29).
Another theme that occurred frequently in responses was support for families (n = 54). This included practical, psychological and emotional support, alongside help with decision making about place of care, treatment and withdrawal of technological support. Some respondents framed supportive care in relation to enabling families to focus on quality of life and making the most of the time left. Twenty eight respondents on the theme of family support included end of life or death in their descriptions.
Finally, in service provision (n = 28), respondents articulated the range of ways in which palliative care could and should be provided by professionals including the tertiary-based palliative care service identified in the survey. Of these, eight respondents identified end-of-life care as the role of a palliative care service.
Discussion
The majority of survey respondents demonstrated knowledge of the principles of palliative care and awareness of services available, suggesting that neither misunderstanding of the principles nor lack of awareness of services should be barriers to timely and appropriate referral. Respondents most commonly reported that referral to palliative care services should begin at diagnosis. Additionally, when directly asked about the importance of paediatric palliative care, respondents reported a high level of appreciation for palliative care treatment, and the majority reported that there are significant opportunities for the integration of palliative and disease-directed care. Yet their reported referral practice indicated few referrals made late in the illness trajectory. The most commonly reported reason for having made previous referrals was to discuss with parents the option of the child or young person dying at home or in a hospice, suggesting that diagnosis of a life-limiting or life-threatening condition rarely provided a reason for referral to palliative care.
The discordance between knowledge, awareness and reported support for palliative care on the one hand and late referral to palliative care services on the other might be explained by the underlying understandings of palliative care as revealed in their responses to the open-text survey question: ‘What comes to your mind when you think of palliative care?’ The responses indicated that a high proportion of respondents associated palliative care with the end-of-life or dying period. Such views are consistent with those reported by HCPs and policy makers across England. An independent review of those involved in planning, commissioning, providing and using palliative care services for children in England found that most equated palliative care with end-of-life care (Craft and Killen, 2007).
The divergent results within our study emerged in relation to the type of question posed. Respondents evidenced good knowledge of the principles of palliative care in closed questions – such as it being more than just providing care at the end of life – but their attitudes expressed in open-text questions demonstrated that although survey participants recognised the potential of palliative care to contribute across the illness trajectory, the final period of a child’s illness was at the forefront of their thinking. As such, the barriers may not be one of lack of understanding of principles or awareness of services, but rather more deeply embedded attitudes that HCPs may not perceive as creating a barrier.
In short, HCPs (in a tertiary care hospital), in responding to what are essentially questions of fact, employ the view of paediatric palliative care which has been advocated by the World Health Organisation (WHO, 1998) – ‘active total care of the child’s body, mind and spirit […] It begins when illness is diagnosed, and continues regardless of whether or not a child receives treatment directed at the disease’ – but they have not fully translated this understanding of paediatric palliative care into their practice as evidenced in their reported referral practices. Thus, it is an as yet unchanged (perhaps unrecognised) association of palliative care with death that acts as a barrier to timely referral.
This is not to suggest, however, that the association of palliative care with end of life or dying is the only barrier to referral (Linton and Feudtner, 2008). The analysis of the observational data collected as part of the project of which this survey was a part indicates that other factors, including structure of care and relationship amongst services, also need to be considered amongst the salient factors in understanding barriers to referral (Craig, 2011).
Another potential factor is that some health care practitioners may feel competent to deliver palliative care without the support of the specialist palliative care team. While this means that children and young people may receive palliative care without referral to the palliative care team, there are additional benefits to joint working between disease-directed teams and palliative care services (Carter et al., 2004; Fraser et al., 2010; Midson and Carter, 2010; Pierucci et al., 2001) from which they will not be able to benefit.
Our study has some limitations. First, the sample was taken from one paediatric tertiary care centre, with a well-established paediatric palliative care team, limiting the generalisability of the findings to those without specialist palliative care teams. Second, the response rate was 14%, with no information on the non-responders who may have reported different knowledge and attitudes. HCPs particularly knowledgeable or supportive of palliative care are potentially more likely to have responded to this questionnaire. This response rate is, however, comparable with those from other paediatric palliative care studies employing similar research methods (Jones and Carter, 2010).
Despite these limitations, the study should not be overlooked. For one, this is to our knowledge the first reported survey on HCPs’ knowledge of and attitudes to this aspect of children’s palliative care in the United Kingdom and thereby begins to fill a noticeable lacuna. Second, and more significantly, the study identifies the relative role of knowledge and attitudes in the referral process, pointing to how underlying associations of palliative care with death and dying appear to act as a barrier to timely palliative care referral. This issue warrants further exploration in other tertiary paediatric settings nationally and internationally (Liben et al., 2008). Third, the findings reveal a disconnect between ideas and actions amongst a group of experienced and knowledgeable paediatric HCPs and, in so doing, point to the need to address both the disjuncture and the underlying attitudes in research, training and education. An awareness of this underlying barrier will enable those professionals developing palliative care education programs to target teaching for maximum patient impact. In addition, paediatric health care providers who may not be aware of how their own underlying attitudes to palliative care are impacting on children and young people’s access to palliative care services could find targeted education programs that allow exploration of a range of referral pathways for working alongside palliative care services instructive.
The environment in which this study was conducted differs from that of previous studies in four notable ways: (1) clinicians had access to a long established specialist paediatric palliative care team capable of supporting both inpatient and home care; (2) palliative care was fully funded and placed no financial burdens on patients; (3) a wide variety of non-hospital options for palliative care including free-standing paediatric hospices existed; (4) current policy as articulated by government health authorities and professional bodies recommends early involvement with palliative care (American Academy of Pediatrics (AAP), 2000, 2012; ACT, 2009; British Association of Perinatal Medicine (BAPM), 2010; Department of Health, 2008). Despite these opportunities, referral rates to palliative care remain disappointing.
Conclusion
Clinicians in both the United Kingdom and the United States identify several parent-related factors, such as a reluctance to entertain a referral, amongst the most significant barriers to a palliative care referral. This study raises the question of whether, in spite of changes in the conceptualisation of palliative care and demonstrations of its value when involved before end of life, clinicians continue to associate palliative care with death and dying. The further question which then arises is of whether this immediate association might affect either their perception of parental reluctance to accept referral or their inclination to diffuse such reluctance when they encounter it and as such lead to less than optimal time for referral. Further research is needed in two areas. One is into associations and attitudes towards palliative care, which may impede clinicians’ willingness to initiate earlier referral to palliative care – and to whether and how this can be best addressed by training and education. The second is into the accuracy of the perceived reluctance on the part of parents to accept referral, motivated by the suggestion here that such perceptions may be coloured by clinicians’ own associations. This work is all the more imperative, given the acknowledgement of an increasing prevalence of children with palliative care needs (Fraser et al., 2012).
Footnotes
Conflict of interest
The authors declared no conflicts of interest.