
Abstract
Indonesia is a country of immense socio-cultural and economic diversity in Southeast Asia. Over the past century, Indonesia epitomized a colonial and post-colonial scientific laboratory for developing early interventions in international health, transcultural psychiatry, and Global Mental Health (GMH). Psychological and psychiatric anthropology have greatly benefited from research on the interplay between culture, mental health, and illness in Indonesia. Given the impact research on severe mental illnesses (SMI) in Indonesia has had on the development of GMH and adjacent disciplines, this review aims first, to provide a systematic review of the scope of SMI research in Indonesia. Second, it aims to identify potential gaps in the literature, cross-country collaborative networks, and traveling concepts of mental health and illness. Third, it points to entanglements between cultural concepts and illness experiences. We focused our search on the PubMed database and discovered 110 relevant records to review. We found a heterogenous body of literature that shows the complexities of being confronted with or living with SMI in Indonesia. We also identified a reliance on high-resource settings for mostly quantitative research. Some limitations appear to be, accounting for cultural hyperdiversity, limiting population samples, and relatively few geographical areas covered in the studies. Inspired by recent commentaries in Global Health research, we suggest more solidarity with low-resource settings and more horizontal approaches in international mental health and illness research. Ultimately, we highlight the need for GMH research and researchers working in contexts of hyperdiversity to ask more culturally sensitive questions.
Introduction
Despite the increasing focus on Global Mental Health (GMH) methods in low- and middle-income countries and ongoing efforts to decolonize the field, the power dynamics embedded in the expansion of GMH favor knowledge centers in resource-rich settings (Moitra et al., 2023). Consequently, GMH remains a movement dominated by knowledge frameworks and understandings of mental health and illness established in the Global North (Bracken et al., 2016; Rose, 2019). This power disparity perpetuates inadequate analytical choices and interpretations of scientific findings that are disconnected from the cultural contexts in which they originate (Moitra et al., 2023). In response to this knowledge gap, the current scoping review aims to map the interests and expertise concerning severe psychiatric disorders from Indonesia, historically an important site in the advancement of international health, transcultural psychiatry, and GMH.
Indonesia, the largest archipelago in the world, is a country of immense socio-cultural and economic diversity in Southeast Asia. The population of around 270 million people is distributed on around 2000 islands that are inhabited, out of more than 7000 that comprise the archipelago. Indonesia is the fourth most populous country in the world. It is also home to more than 1000 ethnic groups speaking more than 700 regional languages, with most people speaking the national language Bahasa Indonesia. There are six state-sanctioned religions: Islam, Hinduism, Buddhism, Protestantism, Catholicism, and Confucianism; and around 4% of the population belongs to other forms of religious practices, officially clustered under the term “beliefs” [kepercayaan].
Over the past 100 years, Indonesia has been representative of a colonial and post-colonial scientific laboratory (Rabinow, 1989; Pandolfi, 2008) for developing early interventions in international health. It was one of the first countries to adopt and implement international health programs, like the eradication of malaria and smallpox, and internationally established agendas for birth-control and family planning targeting Asia and Africa (Packard, 2016). In the late 1970s, studies conducted by Alfred Sommer in the Aceh province on vitamin A deficiency revolutionized the fight against measles and diarrheal diseases (Packard, 2016, p. 320). Indonesia was, furthermore, instrumental in the development of early empirical and transcultural psychiatry, starting with Emil Kraepelin's early work on schizophrenia (initially dementia-praecox) in Java (Pols, 2006). Cross-cultural comparative research of some—notably few—early international psychiatrists and psychologists in solidarity with their Indonesian colleagues have delivered some of the most scathing arguments against the racist attitudes of the Dutch colonial government in Indonesia (Pols, 2018).
More recently, in the context of international mental health interventions and cross-country collaborations, the aftermath of the tsunami of 2004 that severely affected the Aceh province has provided a template to initiate international mental health programs aimed to go beyond the initial emergency event (Eaton et al., 2014, p. 308). The tsunami not only reshaped subjectivities and forced people into new configurations of envisioning the future and remaking of life-worlds (Samuels, 2019) but also brought to an end the nearly two-decades-old conflict between the Indonesian army and the Free Aceh Movement, with the International Organization of Migration involving anthropologists to provide consultation for mental health strategies in previous high-conflict areas (Good et al., 2015).
The devastation that followed in Aceh brought to the fore the complex intertwinement of psychological distress with the cultural experience of a natural disaster. Jones et al. (2007) found that many of the afflicted from the Acehnese communities developed somatic complaints associated with grief and loss. Such instances motivated Indonesian and international organizations to implement context-sensitive intervention strategies, like community education activities about severe psychiatric disorders, or the construction of “quiet houses” used for mourning. They also encouraged the use of local healing methods through music and dance. These not only provided an opportunity to serve the victims of the tsunami but also parts of the populations that previously had no access to psychological and psychiatric treatments.
However, the more than 400 NGOs and other international disaster response units deployed to Aceh departed soon after the emergency response phase. The delivered psychosocial support was uncoordinated, unregulated, and unaccountable, prompting the development of the IASC Guidelines on Mental Health and Psychosocial Support in Emergency Settings (Tol et al., 2014, p. 395). Although national and international collaborations have helped rebuild and strengthen the psychiatric infrastructure, access varied greatly across the province, with the interest waning especially in sub-districts that considered other health interventions a priority (Marthoenis, Yessi, et al., 2016). Furthermore, some members of the population developed symptoms of distress only years after the event, despite people's lives returning to some degree of normality. Past experiences of the tsunami were culturally reimagined and relived in the form of dreams and appearances of ghosts and navigated through local idioms around acceptance of destiny, patience, and surrender to the will of God (Samuels, 2019).
In addition, psychological and psychiatric anthropology have greatly benefited from research on the interplay between culture, mental health, and illness in Indonesia. Gregory Bateson and Margaret Mead (1942), both contributors to the “culture and personality” school, have (erroneously) argued that Balinese childrearing practices and local cultural values lead to “schizoid” personalities. Linda Connor (1982, p. 787) has situated “sacred experiences” associated with voice-hearing and trance-like states, outside of forms of psychosis and thus contributed to later definitions of cultural-bound syndromes, an argument that was later discarded by systematic research on voice-hearing experiences (Luhrmann, 2017). The apparent better illness outcome of people suffering from a severe mental illness (SMI), that was already signaled by Kraepelin during his research in Java, has drawn the attention of international scholars studying the impact of culture on the illness experience and progress of people diagnosed with an SMI in Java and Bali (Good & Subandi, 2003; Lemelson & Tucker, 2017).
Definitions and notes on writing
One of the key concepts we are interested in is that of culture, and how culture can be accounted for in research on SMIs. We understand culture to be […] not a place or a people, not a fixed and coherent set of values, beliefs or behaviors, but an orientation to being-in-the-world that is dynamically created and re-created in the process of social interaction and historical context. Culture has more to do with human processes of attention, perception, and meaning that shape personal and the public sphere in a taken-for-granted manner: What do we pay attention to and how? What matters, and what does not? [emphasis added] (Jenkins, 2015, p. 9)
In other words, when we tried to identify the works of culture and how they are accounted for in the scientific literature on severe mental illnesses in Indonesia, we looked for reflections on institutionalized exchanges of information with the potential to influence people's perceptions, meaning making practices, and behaviors (see also Sperber, 1985).
To define Indonesia as a place of hyperdiversity, we rely on the definition provided by Hannah (2011), who looks at the cultural environment of hyperdiversity as a social setting that is highly diverse (in terms of race and ethnicity as well as social class, immigration status, and religion), dynamic (unstable or undergoing change), and multidimensional (individuals may choose to identify with broad racial and ethnic categories or narrower categories such as country of origin, neighborhood, or sexual orientation). [emphasis added] (p. 41)
In their collective volume on diversity in the United States, titled Shattering Culture: American Medicine Responds to Cultural Diversity, M.-J. D, Good, Willen, et al. (2011) appear to focus mostly on diverse contexts involving people with a migration background in the U.S. We would like to expand on their definition and suggest that hyperdiversity is also possible in places of high linguistic diversity and internal migration, elicited by economic displacement, as is the case for Indonesia.
The authors of this review can confirm that, in Bali and Java, for example, it is not unusual for research participants to switch naturally during interviews between Bahasa Indonesia and Javanese or Balinese, respectively. Even within apparent homogenous linguistic contexts, the differences in usage between groups are significant. For instance, the Javanese spoken in Yogyakarta differs from that spoken in East Java or the northern coast. Similarly in Bali, the spoken Balinese varies across the island. Therefore, we suggest that Indonesia fulfills all the necessary markers to be qualified as a cultural context of hyperdiversity. We believe it is important to understand Indonesia as a hyperdiverse cultural environment for two reasons. First, it taps into major political discussions around health system provision in Indonesia, which needs to account for the complexities of a highly diverse economic and cultural context (Agustina et al., 2019). Second, it invites scholars from the Global North, such as Hannah (2011), to think about hyperdiversity in conditions where immigration, although it exists, is not the main factor contributing to cultural diversity.
Objectives
Given the impact research on SMIs in Indonesia has had on the development of Global Mental Health (GMH) and adjacent disciplines, following Munn et al.’s (2018) recommendations for conducting a scoping review, the aim of this review is threefold. First, we intend to provide a systematic review of the scope of SMI research in Indonesia. Second, aligned with the goals of the larger research project the authors collaborate on, we aim to identify potential gaps in the literature, traveling concepts and related ethnocentric biases of researching mental health and illness, and trace the extent and quality of national and international collaborative networks operating in the field of mental health and illness. The aim of our collaborative project is to understand how global psychiatric information flows influence local perceptions and understandings of mental illness and how these affect the corresponding emotional and moral milieus of people diagnosed with an SMI in Bali and Java. Finally, we try to identify entanglements between cultural concepts and illness experiences in these studies. Consequently, this scoping review contributes to existing psychiatric knowledge on mental health and illness in Southeast Asia, more particularly in Indonesia, and hopes to inform future pathways for cross-cultural interdisciplinary collaborations.
Method
Search strategy
Consistent with similar reviews (e.g., Read & Doku, 2012 or Rajkumar, 2020), our search strategy focused only on the PubMed database and follows the reporting guidelines of the PRISMA extension for scoping reviews (Tricco et al., 2018). Because of the heterogeneity of selected articles, we did not conduct a quality appraisal of the evidence (Jordans et al., 2014), which would be beyond the scope of a review such as this (Bragge et al., 2011).
Our search strategy is informed by the search parameters used by Gamieldien et al. (2021) to explore the concept of recovery of people living with SMIs in low- and middle-income countries. We adapted our search according to our research interest and looked for the following terms in the PubMed database on the 23rd of March 2022: (severe mental illness) OR (bipolar) OR (delusional disorder) OR (major depressive disorder) OR (major depressive disorders) OR (schizophrenia) OR (manic) OR (manic-depressive) OR (paranoid disorder) OR (paranoid disorders) OR (psychoses) OR (psychosis) OR (psychotic disorder) OR (psychotic disorders) OR (schizoaffective disorder) OR (schizoaffective disorders) OR (Schizophreniform) OR (serious mental disorder) OR (serious mental disorders) AND (Indonesia). We did not impose any date restrictions in our search. However, based on our eligibility criteria, we only reviewed articles published after the year 2000.
Eligibility criteria
The search identified 376 articles. We selected relevant articles in two phases. In the first phase, two authors (SD and FC) individually screened the title and abstract of each article and cross-checked their results. In this first phase, if the abstract did not mention sampled country of evidence, but the topic was considered relevant for the review, we checked the text in full. We reached reviewer consensus after discussing the differences and included articles if the main topic covered was related to SMIs and used research participants from Indonesia. Ultimately, we identified 121 relevant articles for full-text review.
During the second phase, we read the full text of the 121 articles considered relevant for our review. After the full text review we excluded an additional 11 articles. The remaining articles focused on chronic depression (n = 20), bipolar disorder (n = 6), and schizophrenia and/or psychosis (n = 89), with 5 articles addressing more than one SMI. Figure 1 presents the PRISMA-ScR flowchart on article selection.
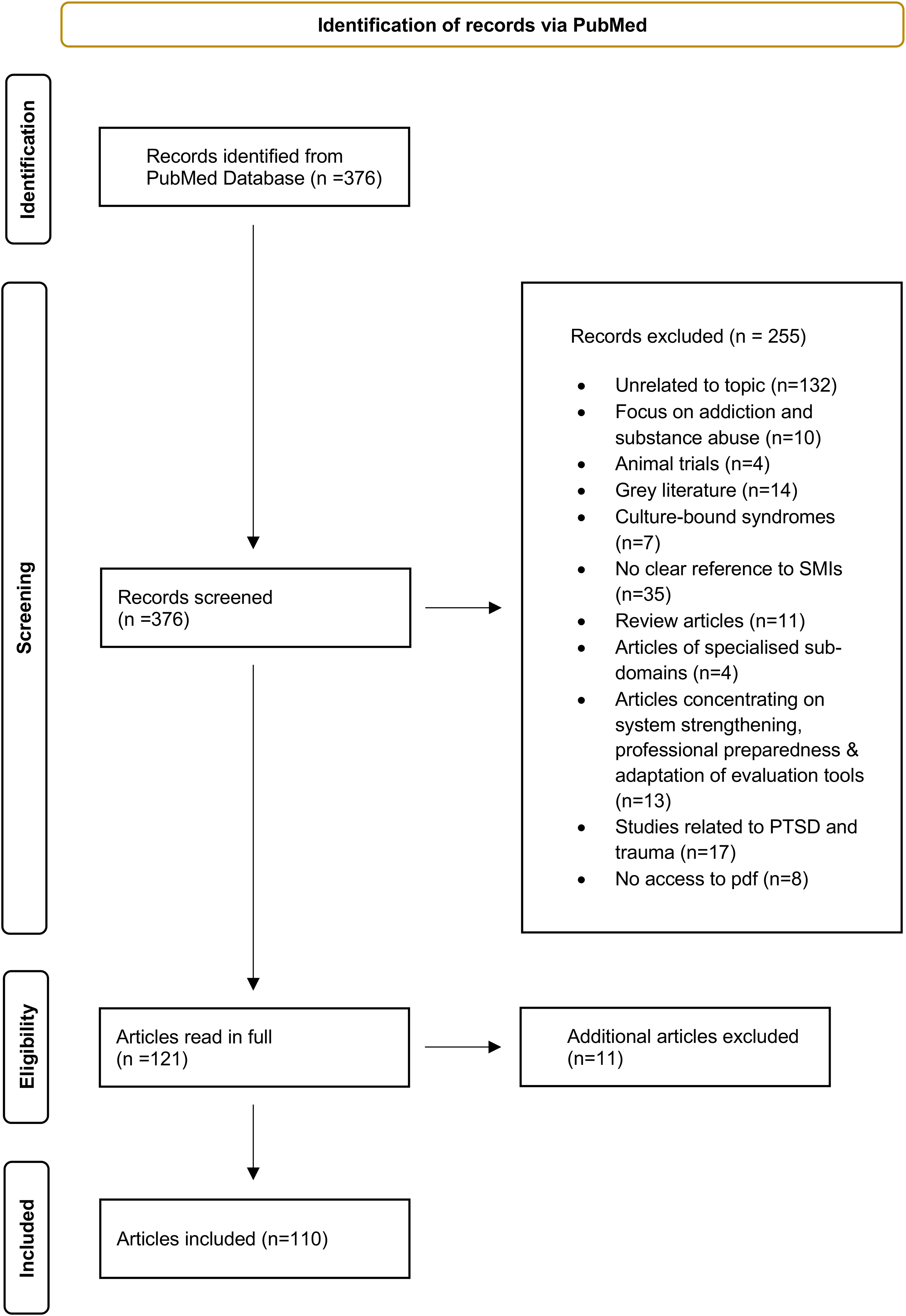
PRISMA-ScR flowchart for identifying and selecting relevant studies.
Data analysis
We charted the data from articles using MS Excel (Arksey & O’Malley, 2005). The resulting table guided our analysis and provided an initial overview of selected articles. All authors had the option to check, confirm, and suggest amendments to the table. The following characteristics informed our charting table: (a) Authors; (b) Authors’ affiliation country; (c) Year of publication; (d) SMI type; (e) Study design (f) Sample location in Indonesia; (g) Compared regions in cross-country studies; (h) Topic of interest (covered by research question).
The themes discussed in this scoping review were established inductively (Glaser & Strauss, 1967), based on thematic analysis (Braun & Clarke, 2006). We recognize our analysis was analyst-driven, in that we tried to find themes that are relevant to the larger project this review is part of. However, we also tried to remain faithful to recurring themes in the selected studies (Boeije, 2002). We defined a theme as the summaries of compared segments that “captured something important about the data in relation to the research question and represented some level of patterned response or meaning within the data set” (Braun & Clarke, 2006, p. 82).
We uploaded the PDFs in MaxQda (version 22.2.1) and analyzed the content in two stages. First, we independently coded relevant segments from selected articles based on the objectives of this review. We considered each identified paragraph to be the unit for analysis. Once we reached consistency between coders, we organized the codes into a matrix and compared the content to identify the themes discussed in this review: Indonesian particularism in cross-country comparison; factors associated with a negative impact on illness outcomes and behaviors; factors associated with a positive impact on illness outcomes and behaviors; and relevant cultural dimensions for understanding the illness experience, health-seeking, and illness behaviors of people diagnosed with an SMI.
Findings
A summary of the selected articles is presented in Online Supplemental Table 1, which is available as an online supplement. Here we first give an overview of the literature and then present the findings of our thematic analysis.
Overview of articles
The articles focused on bipolar disorder, depression, and schizophrenia/psychosis and base their findings on data drawn from Indonesia alone or in comparison to other countries. Several articles focused on more than one SMI and are mentioned at several points in our overview.
Research design
The least covered SMI in the identified literature is bipolar disorder (n = 6), followed by depression (n = 20), with a clear preference for schizophrenia and psychosis-related research (n = 89). However, we only accessed articles published after the year 2000, with more than 50% of the studies (n = 64) published between 2019 and 2022. Most studies follow a quantitative logic of inquiry (n = 82), leaning in favor of survey-based research (n = 57). Two studies combined survey data with reviews of medical records (Purba et al., 2021) and with genetic testing (Utami et al., 2019). Moreover, we found heightened interest in research based on genetic testing (n = 10). These articles were followed by experimental studies, such as randomized control trials (n = 8), evaluations of medication efficacy and effects (n = 5), or reviews of medical records (n = 3). Additionally, one epidemiological study measured the vulnerability of schizophrenia patients to the Toxoplasma gondii parasite (Muflikhah et al., 2018).
In comparison, we identified relatively few qualitative studies (n = 22), accounting for around 19% of the included articles for review. Most of these studies (n = 12) used a research design based on interviews (n = 10) and focus group discussions (n = 2). These articles were followed by case studies (n = 7) and ethnographic studies or research informed by observations in natural settings (n = 3). Additional articles engage with qualitative research in combination with quantitative methods (n = 6), varying in terms of breadth of the methods combined. For instance, two studies (Good et al., 2019; Subandi et al., 2021) combined ethnographic and observational methods with surveys and interviews. Along with experimental interventions, one article used focus group discussions (Fitryasari et al., 2021) and one interviews (Suryani et al., 2011) to evaluate the outcome of the experiment. Finally, two mixed-method studies combined surveys with interviews (Kurihara et al., 2006b) and focus group discussions (Rai et al., 2021).
International collaborative networks
A significant number of SMI articles resulted from established international cross-country collaborations (n = 59), with 20 articles written in the context of the Research on Asian Prescription Pattern (REAP) project. The REAP project focused on comparative patterns of medication intake and related attitudes and behaviors in Asian countries, including Indonesia. In particular, bipolar disorder (BD) and depression studies tended to be designed by international collaborative networks. For example, four out of six papers addressing bipolar disorder emerged from cross-country collaborations. These articles are suggestive of South–South patterns of cooperation, meaning between institutions of countries politically situated in the Southern Hemisphere. Three are part of REAP (Lin et al., 2022; Rajaratnam et al., 2016, 2017). The fourth study had contributions from authors more substantially from the Global North (Bauer et al., 2021). Notwithstanding overall few articles focusing on BD, none of these collaboration-based articles had a lead author from Indonesia.
Similarly, the largest share of depression-related research (14/20) was published as part of international collaborations, with most studies involving researchers based in Indonesia (n = 13), but only one article having a lead author from Indonesia (Arjadi et al., 2018). The REAP study contributed to South–South cooperation (n = 7). The other seven articles also seem to have emerged through the interest of authors in the Global South, with four articles not having any author from the Global North (Kurihara, Kato, Sakamoto, et al., 2000; Manit et al., 2017; Purborini et al., 2021; Srisurapanont et al., 2018). Two articles had a lead author from Indonesia or India in collaboration with other researchers from the Global South and also from the Netherlands and Austria (Arjadi et al., 2018; Wadasadawala et al., 2021). Aside from case studies, the only qualitative article on depression we identified came from a Canadian–Indonesian partnership (Brintnell et al., 2013).
International collaborations were particularly visible in schizophrenia and psychosis research; 44 out of 89 articles have emerged from international collaborations. REAP studies were again prominent, contributing 12 studies to the existing literature. Furthermore, compared to BD and depression research, there were more qualitative studies (n = 14) based on international collaborations. There were a few lead authors affiliated with Indonesian institutions (n = 16) and they were especially visible in qualitative research (n = 8).
Just three articles out of 59 written collaboratively did not include any author with an Indonesian affiliation. However, only 16 studies had lead authors from Indonesia.
Research sampling
A significant number of SMI studies (n = 34) emerged as part of comparative projects between different geographic regions, with most investigations comparing countries from South Asia, East Asia, and Southeast Asia (n = 26). The largest share of these studies appeared in the context of REAP (n = 20). However, apart from geographic proximity and shared diagnostic labels, we found that there was little explanation of the choice of samples or whether socio-economic and cultural differences allowed for meaningful comparison.
Similarly, cross-national studies included wide variations in geographic proximity, again, providing very little explanation for choice of countries or regions to compare (Jaya & Lincoln, 2016; Jaya et al., 2017, 2018, 2022; Lam et al., 2019; Lee et al., 2021; Wüsten & Lincoln, 2017). One notable exception is the study by Bauer et al. (2021) that used purposive sampling to compare mean winter and summer insolation to determine potential correlation with suicide attempts in patients diagnosed with bipolar disorder. Nevertheless, only a few comparative cross-country studies accounted for cultural variability in their research or mentioned it in their findings.
Despite Indonesia being a country marked by immense socio-economic and cultural variation or “hyperdiversity,” non-comparative research carried out in Indonesia presents few efforts to examine this variability. We found only a minority of studies considered potential cultural differences.
Furthermore, in studies focusing on participants exclusively from Indonesia and that mention the geographical location of participants, only 10 out of 34 Indonesian provinces appeared in the research: North Sumatra (n = 16), Jakarta (n = 12), West Java (n = 11), Yogyakarta (n = 9), East Java (n = 8), Central Java (n = 8), Bali (n = 6), Aceh (n = 4), South Sumatra (n = 1), and Lampung (n = 1). In addition, two studies mentioned Sumatra, Java, Kalimantan, or Sulawesi without reference to specific provinces (Arjadi et al., 2018; Purborini et al., 2021).
To the extent the articles mentioned sample location, in cross-national comparative studies, the same few regions appear to have drawn scientific interest. One of the preferred locations was Bali (n = 3). Two other articles based their findings on participants from West Nusa Tenggara (Bauer et al., 2021), or East Java, North Sumatra, Riau, West Java, North Sulawesi, Central Java, Jakarta, South Sumatra, Yogyakarta, and Lampung (Wadasadawala et al., 2021).
Thematic interest
Most studies focused on the experiences and behaviors of hospitalized patients and outpatients. These studies investigated medication intake, prescription patterns, and the effect and efficacy of medical treatment, with a considerable influence from the REAP project (n = 20). Several articles investigated the incidence and prevalence of SMIs, nationally or cross-nationally, and the associated outcomes (n = 12). Next, some studies focused on insight (perception and understanding of the disease) and related implications for illness-behaviors and health-seeking behaviors of patients and outpatients (n = 15). Several studies addressed cultural variations in symptomatology, diagnosis, and experiences (n = 9). Finally, two additional topics that recur in the existing literature concern the impact of the environment, both social and natural, on illness-behavior and the experience of people with an SMI (n = 8). Several articles considered the potential and possibilities of non-pharmaceutical interventions (n = 5).
In looking at the social environment of people suffering from SMI, the literature often investigated opportunities for strengthening the response of the environment and the non-clinical care landscape (n = 7). Some studies evaluated the impact of providing care on therapy management groups (kin, clinical personnel, other support structures) related to the quality of life and mental health (n = 8). Other studies looked at the responses of the social environment and care networks toward people suffering from an SMI (n = 6). Major themes in these articles include: pasung (the forceful seclusion or restraint of people with an SMI) (n = 2); level of Expressed Emotion in the environment of outpatients (n = 3); and a comparison of the attitudes of the general population toward people with an SMI in Tokyo and Bali (Kurihara, Kato, Sakamoto, et al., 2000). Several studies explored the knowledge and perception of SMI within therapy management groups and their potential impact on health-seeking behaviors (n = 5).
Finally, at the biological level, most studies we identified cover genetic factors influencing or pre-disposing people to an SMI (n = 10), or measured the physical consequences of suffering from an SMI and/or associated medication intake (n = 5).
Thematic analysis
Based on the wider project the authors are engaged in on global psychiatric knowledge flows and their impact on illness experiences, and reflecting common themes in the literature, we considered the following themes most relevant for determining the scope of research focusing on SMIs in Indonesia.
Indonesian particularism in cross-country comparisons; Factors associated with a negative impact on illness outcomes and behaviors; Factors associated with a positive impact on illness outcomes and behaviors; Relevant cultural dimensions for understanding the illness experience, health-seeking, and illness behaviors of people diagnosed with an SMI.
Indonesian particularism in cross-country comparison
In several cross-country studies, samples from Indonesia appear to do better than their counterparts in other countries on various mental health measures. For instance, participants from Indonesia perceived more family support and greater satisfaction regarding their family relationships (Wüsten & Lincoln, 2017). In a study comparing Indonesia with Japan, researchers observed a lower prevalence of intense Expressed Emotion in Bali that could explain longer tenure in the community compared with Tokyo (Kurihara, Kato, Reverger, & Yagi, 2000). The general public in Indonesia showed more positive attitudes toward people with a history of psychiatric treatment than participants from Japan (Kurihara, Kato, Sakamoto, et al., 2000), while psychiatric patients had a shorter cumulative length of stay in psychiatric hospitals in Indonesia (Kurihara, Kato, Tsukahara, et al., 2000).
Similarly, in another cross-country study, nurses from Indonesia diagnosed with depression following the COVID-19 outbreak showed milder symptoms when compared to a similar sample from Bangladesh (Wadasadawala et al., 2021). Finally, Rajaratnam et al. (2016) found that antidepressant prescription in Indonesia was the lowest compared to the other 10 countries surveyed for antidepressant dosing in Asia.
In contrast, there were few studies reporting negative research findings particularizing Indonesia in cross-country studies. In fact, we only identified negative comparisons concerning higher levels of diagnosed depression (Lee et al., 2021), and more antidepressants being prescribed for children and adolescents (Chee et al., 2016), as well as for people diagnosed with bipolar disorder (Lin et al., 2022).
Despite these differences, we found few explanations for the choice of populations to compare and of potential cultural variability. Back translation was usually assumed to account for language variation. The justification for research participants was commonly based on geographical location (“Asia”), economic status (high income compared to low income), and shared diagnostic label, with several authors acknowledging they did not address ethnic diversity as a potential limit of their study (Y. C. Park et al., 2019; Xu et al., 2020; Yang et al., 2018).
Some studies did reflect on cultural variability as part of their analysis, for example, discussing their findings in relation to local kinship structures and values of care (e.g., independent vs. interdependent values) (S. C. Park, Jang, et al., 2020; Wang et al., 2017; Wüsten & Lincoln, 2017). Several authors (Bauer et al., 2021; Kurihara, Kato, Tsukahara, et al., 2000) explained their findings in terms of culturally specific non-biomedical factors, such as religious and spiritual explanatory models. Finally, some studies used specific indicators to account for variance in socio-cultural background, such as the multidimensional index developed by Lampert and Kroll (2009) based on census categories from Indonesia (Jaya & Lincoln, 2016; Jaya et al., 2017). In another study, Chee et al. (2015) reflect on cultural diversity by tracing commonly identified core symptoms based on categories from the ICD-10 and DSM-IV.
Factors associated with a negative impact on illness outcomes and behaviors
The determinants described as having a negative influence on the experiences associated with a SMI commonly mirror the conditions reported in the literature focusing on the Global North. Structural barriers, including limited access to mental health services and few available psychiatrists, poverty, or reduced literacy about SMIs, were often referred to as the main impediments to acquiring or continuing psychiatric treatment across the archipelago (Browne, 2001; Christiani et al., 2015). Other factors include poor clinical condition and comorbidities at the onset of psychosis or as the illness progresses (Kurihara et al., 2005; Rai et al., 2020), symptom severity (Pribadi et al., 2020; Sari et al., 2021), and the period between the onset of psychotic symptoms and the start of treatment (referred to as duration of untreated psychosis or DUP) (Marchira et al., 2016; Marthoenis, Aichberger, & Schouler-Ocak, 2016).
Additionally, negative attitudes toward people suffering from an SMI, stigma, and perceived discrimination were common themes emerging from the literature (Fitryasari et al., 2018; Maramis, Sofyan Almahdy, et al., 2021). Several of these studies associate internalized shame of affected individuals and caretakers with reduced willingness to seek psychiatric help and social isolation (Purborini et al., 2021; Yosep et al., 2021), with not an uncommon outcome being the practice of pasung, the restraining or shackling of individuals to confined rooms or sheds (Minas & Diatri, 2008; Suryani et al., 2011).
However, some particularities related to Indonesian social organization and structure stand out in the literature. Several authors reference an inability to conform to local cultural norms and expectations as a factor impeding (re)integrating into communities. In particular, studies from Java and Bali suggest that one of the most common violations a person suffering from an SMI engages in is disturbing the community's peace (Good et al., 2019; Suryani et al., 2013). Disapproving attitudes can also be a consequence of not fulfilling expected gender roles, such as men's inability to pursue income-producing jobs or, in the case of women, not fulfilling household-related duties and getting married (Christiani et al., 2015; Pribadi et al., 2020; Rai et al., 2020).
Religion is also reported to negatively impact people's response to a person diagnosed with an SMI, leading to self-stigmatizing behaviors of affected individuals and their families. Irrespective of location, such instances were usually described as following from the communities’ view of SMI as a consequence of sinful behavior (Subandi, 2015) or spiritual possession (Budiono et al., 2021). In both Muslim and Hindu contexts, studies suggest that an inability to participate in religious interrelatedness as part of established rites puts a heavy burden on families that may be excluded from the religious community (Brintnell et al., 2013; Suryani et al., 2013).
Studies across Indonesia found a high level of economic and emotional burden experienced by family members caring for a person diagnosed with an SMI (Janah & Hargiana, 2021; Lestari et al., 2021). Women appear to be most affected, as they are frequently in charge of care, especially mothers of affected individuals (Fitryasari et al., 2018; Handi et al., 2019). Negative attitudes toward affected families take an additional toll, with most studies reporting blaming behaviors within the immediate community (Bachtiar et al., 2020; Widiyawati et al., 2020). Studies often reported reduced literacy regarding SMIs impacting the ability of families to cope with their situation (Hugo, 2007; Laila et al., 2018).
Factors associated with a positive impact on illness outcomes and behaviors
The literature reflects an interest in positive factors impacting people diagnosed with an SMI or their affected communities. Interventions examined for their effectiveness and efficiency consistently report positive findings. These interventions cover a wide range of approaches, from purely biomedical medication and treatment-related trials (Wiguna et al., 2014) to therapeutic interventions combined with religious practices such as prayer (Putri & Effendy, 2019) and meditation (Suryani et al., 2011). In addition, a focus on psychoeducation stands out in the literature as part of treatment strategies (Erawati et al., 2014; Mubin et al., 2020) and as a recommendation for policymakers and practitioners (Laila et al., 2019; Siregar et al., 2022).
The literature also draws the attention of policymakers and practitioners to socio-cultural determinants with a positive impact on either the recovery process or on the experiences of affected individuals, their immediate caretakers, and surrounding communities. Studies report positive attitudes toward people diagnosed with an SMI in their immediate social environment, both at the level of community (Kurihara et al., 2011) and in the context of family caretakers (Ferliana et al., 2020). Several studies emphasize cultural scripts that may enable more rapid reintegration into the community, with variations depending on sample location. These scripts relate to the normalization of voice-hearing in everyday life (Suryani et al., 2013), drawing strength and making meaning through prayer, meditation, and one's religious identity (Rai et al., 2022), as well as acquiring social support in communities under the precept of a harmonious living together (Subandi, 2015). Associated practices include appeasing supernatural entities presumed to induce a negative disease progression (Kurihara et al., 2006a), and accepting that a higher power decides one's fate and health (Widiyawati et al., 2020). Finally, several authors associate a supportive immediate social network that facilitates community involvement and employment with more positive experience for people diagnosed with an SMI and their families (Browne, 2001; Maramis, Sofyan Almahdy, et al., 2021).
Cultural matters
Through qualitative studies, we have access to a rich vocabulary of culturally specific ways of addressing SMIs. Within this vocabulary, three themes stand out. First, authors studying SMIs in Java, Bali, and Aceh suggest that a particular focus on emotion languages is necessary to understand the experiences of affected individuals and caretakers. These studies commonly draw attention to patients’ excessive emotionality at the time of the onset of psychosis. High emotionality shapes negative perception by others in communities where maintaining a calm and contented demeanor is regarded as having high moral value (Browne, 2001; Subandi et al., 2021). Several studies find that the most common culturally sanctioned behavior is disturbing the peace of the immediate social environment (Good et al., 2019; Hugo, 2007), with re-integration into the community being facilitated by a tempered emotional attitude (Subandi, 2011).
Second, and related, the ability to exert control over one's emotions, behavior, and social environment appears to be an accepted marker of recovery. Changes perceived positively by either caretakers or communities include the ability to take control over one's thoughts (Suryani et al., 2013), one's actions in the immediate social environment (Browne, 2001), and even over one's living space (Subandi, 2015).
Finally, and probably most importantly, illness experiences do not occur in a vacuum. Apart from biomedical notions, spiritual and religious ideas about health and illness drive health and help-seeking behaviors throughout the archipelago (Budiono et al., 2021; Marchira et al., 2016). As a consequence, not attending to or following expected religious practices represent cultural transgressions that can negatively impact self-perception and encourage stigmatizing attitudes. Such instances become more significant if the unmet expectations are related to practices associated with one of the state-sanctioned religions (Brintnell et al., 2013; Suryani et al., 2013). To cover the need for spiritual relief, Indonesia provides a therapeutic landscape marked by medical pluralism, shaped by different practices and healers (e.g., various dukun in Muslim contexts and balian in Bali) (Marchira et al., 2016; Suryani et al., 2011).
As we have noted, Indonesia is a context of hyperdiversity, and generalizations should be made with caution. Even within apparently homogenous ethnic communities, such as “the Javanese” or “the Balinese,” the differences between groups can be striking (Barth, 1993; Geertz, 1976). Some studies reference diversity when describing the context of their research (Christiani et al., 2015; Irmansyah et al., 2008). Nevertheless, we found several articles that suggested their sample was homogeneous, without clarifying if such homogeneity was documented or just assumed (Amir et al., 2019, p. 2581; Kurihara et al., 2006a, p. 1795).
Similar to cross-country studies, we found few instances where cultural diversity was addressed, with several studies admitting they fell short of doing so in the interpretation of their data (Laila et al., 2018; Pardosi et al., 2019). The degree by which hyperdiversity was accounted for depended mainly on the methods used for data collection. Some studies included a diverse sample of the population, grouped by ethnic self-identification (Marthoenis, Aichberger, & Schouler-Ocak, 2016; Rai et al., 2020) or adjusted questionnaires and interview guides to be sensitive to local idioms of distress (Browne, 2001; Kurihara et al., 2006a). Other studies collaborated with local experts (such as psychiatrists and non-biomedical healers) to consult in the interpretation of their data (Hugo, 2007). Brintnell et al. (2013) looked for commonalities and consistencies within a relatively diverse sample. In contrast, framing the research question in a culturally sensitive way from the onset of the study led to interesting findings in the context of Javanese research participants (Good et al., 2019; Marchira et al., 2019).
Discussion
Compared to the large number of articles published on SMIs in resource-rich settings, the literature from Indonesia is small. We found a preponderance of survey-based quantitative studies, with more than half of the studies emerging from international collaborations, mainly led by institutions and authors from high-income countries. There was more work on schizophrenia and psychosis-related research than on chronic depression and bipolar disorder. With regard to sample diversity, the same provinces were often covered in the literature, leaving a large part of the archipelago uncharted. Most research focused on individual perceptions and behaviors of people diagnosed with an SMI, leaving a gap in the literature about the experiences of caretakers and surrounding social environments. This point is relevant, considering the potential impact of the immediate social environment on the illness progression and outcome of people diagnosed with an SMI (Myers, 2010). We echo a point raised by Kirkbride et al. (2010): that socio-environmental factors in schizophrenia are more easily modifiable and preventable than genetic factors. Therefore, we argue that research on social environments should draw more attention, especially in contexts with limited biomedical resources.
Still, our thematic analysis shows that, even if limited in scope, the domains covered by available studies indicate the complex social realities people diagnosed with an SMI, their caretakers, and their social environments face. In the early 2000s, several programmatic articles determined the priorities of the Global Mental Health (GMH) movement, calling for the necessity to close the treatment and knowledge gap between high-resource and low-resource settings (Patel et al., 2008; Saraceno et al., 2007). Proponents of GMH continue their call for increasing knowledge production from low-resource contexts such as Indonesia (Collins et al., 2014; Jablensky, 2013; Saxena & Belkin, 2017). Psychiatric knowledge appears to be increasingly emerging from Indonesia, but the impact on global knowledge production mechanisms remains uncertain.
With few exceptions, there does not seem to be a significant challenge to the biomedical canon established in countries from the Global North. Some studies have questioned the applicability of existing diagnostic labels and biomedical approaches in some populations from Indonesia (Suryani et al., 2013). Nevertheless, especially in cross-country studies, authors compare samples based on diagnostic labels of the ICD or DSM. A focus on diagnostic labels alone ignores findings on the ambiguities inherent and neglected in the development of respective categories (Kirmayer & Ban, 2013) and the ways that disease categories are clustered together in current nosology (Hyman, 2010).
We realize that, for the moment, the available diagnostic manuals are the best tools for creating comparable groups, and hence their importance for advancing psychiatric research. For instance, the high prescription rate for depression for children and adolescents compared to other countries in the region should be of immediate interest to policymakers in Indonesia (Chee et al., 2016). However, future comparative studies could consider further contextualizing their data by including additional behavioral or cultural markers. We identified a few cross-country studies that have successfully done so (e.g., Good et al., 2019; Laila et al., 2018; Marchira et al., 2019; Marthoenis, Aichberger, & Schouler-Ocak, 2016). These authors either reflected on local values of care and kinship or consider local cultural explanations in their interpretation. Whenever warranted by the research question, reflecting on what cultural diversity means for findings should become the norm in cross-country studies.
A similar point can be made regarding what psychiatrists usually refer to as “insight” or knowledge about the disease. The findings reported are contradictory. Several studies identified a good grasp of biomedical knowledge and positive attitudes toward SMIs in communities, whereas others found the opposite. These conflicting findings could be attributed to Indonesian socioeconomic and cultural diversity or a “halo effect” (Yang et al., 2010), with participants responding what they believe to be the correct or expected answer. What is more interesting is the repeated call of these authors for psychoeducation, which leads us to conclude that insight or awareness is commonly measured based on biomedical categories. We suggest that, in contexts of limited access to biomedical treatment facilities, existing definitions could be expanded to measure insight as a socio-cultural process (Saravanan et al., 2004) that includes culturally construed versions of experience that fit with people's social worlds (Tranulis et al., 2008).
In the same vein, authors repeatedly call for psychoeducation to fight against stigma. The results of the studies are, again, contradictory in the sense that several studies report positive attitudes toward people with an SMI and their families, while the majority emphasize stigma as a significant problem for recovery. The focus on psychoeducation to resist stigma is concerning for two reasons. There is evidence, in the context of marginalized communities in Java, that even highly educated professionals with the best intentions can reproduce stigma through nuanced individual emotional expression (Stodulka, 2017). This raises the question of the efficacy of educational programs to decrease stigma. Second, the sole focus on psychoeducation obstructs alternative interventions that could have a positive outcome. For instance, a systematic review and meta-analysis of 62 randomized control trials found that contact interventions yielded similar results to educational interventions in reducing stigma toward people with severe mental illness (Morgan et al., 2018).
Furthermore, we observed that many articles recruited samples in psychiatric hospitals or in cooperation with local clinics and community health centers (puskesmas]. In fact, several authors highlighted the focus on clinical adherent outpatients as a significant limitation of their studies (Marthoenis, Aichberger, & Schouler-Ocak, 2016; Purba et al., 2021). On top of the structural barriers, like affording access to hospitals and clinics, several authors mention a low public awareness about accessing psychiatric care when struggling with an SMI (Hardi, 2021; Pols, 2006). Low public awareness and reduced access to biomedical treatment facilities should not only raise a question about the accuracy of the picture that can be inferred from the available literature but also highlights the need to expand scientific interest beyond the urban centers spearheading available studies.
The large number of collaborative studies is also indicative of the dependency of Indonesian authors on support from high-income countries. This dependency points to the need to promote more research led by institutions from Indonesia. At the same time, we believe that the established collaborative networks are a strength for transcultural investigations of mental health and illness and should be nurtured. The COVID-19 pandemic brought to light the need for more solidarity in the global community and more horizontal approaches in global health interventions and research (El Bcheraoui et al., 2020). Such calls appear in a context where the norm in pandemic response was countries working in isolation and not as part of a coordinated effort of the global community (Skegg et al., 2021).
More solidarity and a horizontal approach in GMH could advance collaborations and interventions. The already established transnational networks, many of which emerged from South–South collaborations, could offer a foundation for improving psychiatric care and research in Indonesia. However, greater attention to the categories being compared is warranted. Equivocal ideals of “Asian-ness” are apparent in some articles, for instance, in some of the REAP studies that base their comparisons on geographical regions that vary significantly in their access to psychiatric treatments or in comparing heterogeneous units such as Tokyo with Bali (e.g., Kurihara, Kato, Reverger, & Yagi, 2000). Such comparisons do not always provide a coherent framework for interpreting results.
Arguments for developing and implementing culturally sensitive psychiatric diagnostic systems and interventions in diverse settings have a long-standing tradition in medical, psychological, and psychiatric anthropology (Good, Hannah, & Willen, 2011). Despite the recognition of the importance of attention to culture in research, the literature reviewed suggests that this has had less uptake. In places of cultural hyperdiversity, such as Indonesia, conducting culturally sensitive research should be a primary concern. Only a few studies have accounted for cultural diversity in the interpretation of their findings. There is a need for studies that capture the meanings people attributed to SMIs that may affect their responses, perceptions, and attitudes (Jenkins, 2015). This requires adjusting research tools to elicit local categories and explanatory models, collaborating with local experts, and including samples of the population representative of diverse ethnic groups.
GMH research with diverse populations can better address diversity by ensuring collaboration between different disciplines, such as anthropologists and historians. Inspired by Good et al. (2019), we believe that cultural accountability should begin with the research question. In their study of psychosis in Java, they emphasized the relevant dimensions that need to be accounted for in culturally sensitive research: Anthropologists have long argued for a broader “cultural phenomenology”, one that asks questions about the “behavioral environment of the self” in local cultures, about shaping of experience and mental illness by local cultural worlds, about important differences across cultures in symptoms, about not merely the “primary deviance”, but also social responses to early symptoms of illness and the development of what sociologists called “secondary deviance”—illness experience and behavior as shaped over time by social, cultural, and institutional responses. (Good et al., 2019, p. 513) (references omitted)
Limitations
This review has several limitations. Due to the restrictive definition of SMIs and the constraints of a small team, we only included English-language articles from a single database and did not include several studies that could have broadened our analysis and interpretation. Some of the studies we excluded present phenomenologically groundbreaking work on the illness experience of people with symptoms that resemble SMIs but which they refer to with local terms, sometimes considered examples of culture-bound syndromes (Burton-Bradley, 1968; Connor, 1982; Geertz, 1968; Lemelson & Suryani, 2006). However, we believe that the 110 articles for our analysis paint a relatively accurate portrait of the scope of recent SMI-related research in Indonesia.
Conclusion
In this review, we aimed to capture the scope of SMI-related research in Indonesia. Our search identified a heterogenous body of literature that examines the complexities of living with SMI. There was a reliance on researchers from high-resource settings and on conducting mostly quantitative research. However, we also suggest this reflects already established collaborative networks that represent a strength for GMH and that should be expanded and nurtured.
The wide array of topics and domains discussed in the literature should encourage emerging scholars interested in SMIs in Indonesia and Southeast Asia to refine their research questions. We were surprised to find little deviation from entrenched notions and norms of health and illness based on work from the Global North. The rich body of anthropological literature on health and illness has emphasized the entanglement between socio-cultural environments, local values and understandings, and illness and health-seeking behaviors (Bhasin, 2007). Biomedical systems also tend to take different shapes in different cultural contexts (Gaines & Davis-Floyd, 2004). We therefore expected that studies would have captured more details of the culturally complex environment of Indonesia. Future studies need to consider a more culturally sensitive approach for collecting and interpreting the data. Echoing similar calls from other evaluations of global health research (El Bcheraoui et al., 2020), we end this article with a plea for more solidarity with low-resource settings and more horizontal approaches in international mental health and illness research, and highlight the need for GMH research and researchers working in contexts of hyperdiversity to ask more refined and culturally informed questions.
Supplemental Material
sj-docx-1-tps-10.1177_13634615251342638 - Supplemental material for Research on severe mental illness in Indonesia: A scoping review
Supplemental material, sj-docx-1-tps-10.1177_13634615251342638 for Research on severe mental illness in Indonesia: A scoping review by Florin Cristea, Putu Aryani, Saskia Duchow, Pujo Semedi, and Thomas Stodulka in Transcultural Psychiatry
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication is part of a project funded by the German Research Foundation (DFG grant number: 460656552).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.