
Abstract
Mental health service use by individuals of South Asian origin living outside of South Asia is influenced by cultural factors such as endorsing psycho-social-spiritual over biological explanations, somatisation, and stigma. The aim of this review is to synthesise the evidence about (a) explanatory models of common mental disorders (CMDs) among people of South Asian origin residing in high-income countries, and (b) their help-seeking for CMDs, including formal and informal care. The systematic review protocol was registered a priori on Prospero (registration number CRD42021287583). We ran extensive searches on explanatory models and help-seeking of people of South Asian origin across five databases (MEDLINE, Embase, Cumulated Index to Nursing and Allied Health (CINAHL), PsycINFO, and Global Health). We extracted the data and conducted a narrative synthesis. We included 33 reports and 29 studies (9,030 participants). The participants in the included studies viewed CMDs through a psychosocial rather than a biological lens (e.g., resulting from family issues vs. neurotransmitters). Causal attributions included life stressors and attitudinal and religious/spiritual factors. Commonly used help-seeking strategies included private coping (i.e., crying or praying), speaking to friends and family, and visiting their General Practitioner. We can conclude that cultural factors play an important role in how South Asian individuals experience and understand CMDs. To cope, they use pluralistic help-seeking strategies. Implications for clinical practice and policy include increasing research on the explanatory models of CMDs, involving family in services, and developing community-based interventions for individuals who do not engage with formal care.
Background
Common mental disorders (CMDs), which include depression and anxiety disorders, are leading causes of disease burden, with a global prevalence estimate of 29% for adults within their lifetime (Steel et al., 2014). The prevalence of depression ranges from 5% to 44% for first-generation immigrant groups versus 8% to 12% for the general population, and for anxiety it ranges from 4% to 40% in first-generation immigrant groups compared to 5% in the general population (Close et al., 2016). While prevalence estimates of CMDs among South Asian individuals vary (Bhavsar et al., 2021), there is consensus that people of South Asian origin who reside outside of South Asia experience similar or higher rates of CMDs than the native population. For example, in the UK, South Asians have lower levels of psychosis but higher levels of deliberate self-harm and psychological distress than the majority White population (Bhavsar et al., 2021) and in Canada the prevalence of depressive symptoms among South Asians (21%) was double that of the national average (10%) (Lai & Surood, 2013).
However, immigrants are less likely than the general population to access mental health care for reasons such as language, stigma, cultural perception, experiences (i.e., presentation of symptoms), and a limited understanding of a new healthcare system (Lu et al., 2020; Pollard & Howard, 2021). Even if mental health services are accessed, there is a significant delay when compared to the native population (Bhui et al., 2003; Fernando, 2014; Tribe & Marshall, 2020). South Asian immigrants (individuals originating from India, Pakistan, Sri Lanka, or Bangladesh) underuse mental health services in comparison to their White counterparts and other ethnic minority groups (Bowl, 2007; Hussain & Cochrane, 2016; Prajapati & Liebling, 2022). For example, Pakistani and Bangladeshi women in England are less likely to access mental health services than White women (Pakistani OR = 0.23, Bangladeshi OR = 0.25) (Kapadia et al., 2018), and Asian groups in the UK are 38% less likely to have received treatment for a CMD than White groups in the UK (Ahmad et al., 2021).
Meeting the needs of immigrant groups is important considering that the global movement of people, driven by interconnecting social, political, environmental, and economic factors, has increased, particularly from low-income country to high-income country (HIC) settings (Bhugra, 2004; United Nations Department of Economic and Social Affairs, 2020). Particularly, South Asians represent a rapidly growing ethnic group in HICs such as the United States, UK, Canada, and Australia (Prajabati & Liebling, 2022). Besides the challenges of the migration process itself (particularly in cases of forced migration), post-migration acculturative stress, socio-economic-political conditions, familial factors, age of migration, and country of birth (e.g., discrimination, position in society) in the host country may cumulatively contribute to CMDs in immigrants and their subsequent generations (Bhugra, 2004; Crowley, 2022; Karasz, 2005; Lubin & Khandai, 2017).
In addition to systemic barriers, one explanation for poor service use is the explanatory models of illness—defined as “the way people perceive, interpret and respond to [illness]” (Dinos et al., 2017, p. 106). Explanatory models influence whether someone seeks or receives formal or informal help, when they receive help, who they receive help from, and how effective the help is (Kleinman et al., 2006). If a healthcare provider's explanatory model differs from their patient's, providers may face difficulties empathising with their patient, as well as understanding their symbolic language, explanations of illness, and their perspective on the role/responsibility of the healthcare provider (Bhui et al., 2013; Delara, 2016; Gopalkrishnan, 2018). This can lead to misdiagnosis, delayed diagnosis, or referrals to inappropriate services for immigrant and ethnic minority groups who may refer to maintain their cultural and religious perceptions of health (Bowl, 2007; Helman, 1994).
Discounting an individual's explanatory model in a clinical setting contributes to poorer treatment outcomes, particularly for immigrant and ethnic minority groups (Bhui & Bhugra, 2003). Conversely, exploring explanatory models can centre the role of culture in mental health experience and management, allow for a tailored response to an individual's generational status and life context, involve a patient's family in decision-making, reduce stigma, diversify treatment options / sources of help, and ultimately lead to greater and more appropriate use of mental health services (Dinos et al., 2017).
South Asian individuals living in HIC settings often do not perceive available mental health services or mental health prevention initiatives to be culturally appropriate (Bhui & Bhugra, 2002; Bowl, 2007; Islam et al., 2014). In Canada, South Asian individuals with a major depressive disorder had the highest percentage of unmet mental health care need (48%) and perceptions of barriers to mental health service use (33%) compared to eight other ethnic minority groups (Gadalla, 2010; Islam et al., 2014).
This may be partly explained by the overuse of the biomedical model in Western settings, which fails to account for psychological, social, and cultural factors, and emphasises individualism, biological explanations, and pharmacological treatment for mental health conditions (Deacon, 2013). These characteristics are in direct contrast with many South Asian individuals’ explanatory models regarding the cause and appropriate treatment of CMDs, somatic expression of symptoms, and collectivism. These are all directly related to refusal of mental health service use (Antoniades et al., 2017; Beiser et al., 2003; Karasz, 2005; Rastogi et al., 2014).
South Asian individuals in HIC settings understand CMDs through religious (e.g., supernatural forces or God's will), social (e.g., difficult life events), or moral (e.g., weakness) lenses rather than as an illness requiring biomedical intervention (Antoniades et al., 2017; Gilbert et al., 2006; Jacob et al., 1998; Karasz et al., 2013; Rastogi et al., 2014). These explanations link with stigma, which may cause South Asian individuals to believe that seeking formal help could lead to humiliation in their community if their CMD is perceived to result from a character flaw (Karasz et al., 2019). South Asian individuals may therefore prefer to seek help for mental health problems from informal support (such as relying on oneself, family, or faith healers) rather than Western healthcare services (Bradby et al., 2007; Hussain & Cochrane, 2010).
South Asian individuals often express their mental distress as somatic symptoms (Anand & Cochrane, 2005; Gunasinghe et al., 2019; Hussain & Cochrane, 2016; Karasz, 2005). Along with language barriers, this can cause miscommunication between service users and care providers (who largely possess a biomedical view on health and disease such as the body–mind dichotomy) (Bhui et al., 2013).
Individual–collectivist discord is an important cultural factor that plays a role in determining help-seeking (Soorkia et al., 2011). Collectivism is an important aspect of South Asian identity; South Asian individuals often prioritise family over the individual (Masood et al., 2009; Tummala-Narra, 2013). Collectivist values, for both South Asian parents and their children, can inhibit the sharing of mental health concerns if the affected individual does not want to place burden on their family members or is conscious of embarrassing their family in the wider community. If individuals do seek professional help, the care offered could be incompetent if a host country's Western model of medicine does not, for example, consider parent–child relations in immigrant families, where views on family obligation differ from the mainstream culture's ideology (Bismar, 2018).
It is well established in the literature that culture influences how individuals understand, experience, and manage mental health conditions. However, there is yet to be a review on the specific cultural factors that influence mental health in the South Asian diaspora, which can inhibit the delivery of, and access to, culturally informed care for this population. To grow the evidence base, this systematic review aims to synthesise the evidence about: (1) explanatory models of CMDs among people of South Asian origin residing in HICs; and (2) their help-seeking attitudes, intentions, and behaviours towards informal and formal mental health support for CMDs.
Method
Design
Systematic review of observational studies. The systematic review protocol was registered a priori on Prospero (registration number CRD42021287583).
Eligibility criteria
We included peer-reviewed research articles describing observational studies, published in English. We did not have any restrictions on year of publication. We included studies that described the explanatory models of and help-seeking for CMDs by South Asians (from India, Pakistan, Sri Lanka, or Bangladesh) living in HICs as categorised by the World Bank. CMDs were defined as depression and anxiety disorders such as post-traumatic stress disorder, panic disorder, generalised anxiety disorder, obsessive-compulsive disorder, and phobias (Kendrick & Pilling, 2012). Explanatory models were defined as “prior knowledge on the causation, perception, experiences, and traditional belief held by the patients, their caregiver, and the population in general” (Lilhare et al., 2020, p. 327). Help-seeking was defined as “attempts to maximise wellness or to ameliorate, mitigate, or eliminate distress” (Arnault, 2009, p. 2) through informal (personal networks such as friends and family) and formal (including professionals such as General Practitioners (GPs), nurses, psychiatrists, and non-health professionals such as teachers, spiritual and religious leaders, and community workers) support, and self-help (Kim & Lee, 2021).
Search
We searched electronic databases (MEDLINE, Embase, Cumulated Index to Nursing and Allied Health (CINAHL), PsycINFO, and Global Health) on 6 December 2021, using search terms under the following concepts: South Asian (e.g., Indian, Bengali), CMDs (e.g., depression, anxiety), and explanatory models (e.g., beliefs, attitudes, culture). We updated the search across all databases on 1 February 2023, to find articles published in 2022–2023 to identify recent extant literature. The detailed search strategy is described in the Supplementary Materials. To identify other relevant articles, the bibliographies of the included studies were hand-searched by the primary author (RJ).
Procedures
After automatic and manual de-duplication in EndNote, the search results were imported into the Rayyan software. Two reviewers (RJ and KB) independently screened the titles and abstracts, and a third reviewer (AN) resolved any conflicts. Two reviewers (RJ and KA) independently did the full-text screening and conflicts were discussed until an agreement was reached. When the search was updated, one reviewer completed the title/abstract screening (RJ) and two reviewers completed the full-text screening (RJ and AN). A data extraction form was designed to extract the data needed to meet the study objectives and covered domains such sample demographics, mental health condition under study, and findings pertaining to explanatory models and help-seeking. The data was first extracted 9 March 2022.
Quality assessment
Qualitative studies were assessed using the Critical Appraisal Skills Programme (CASP) (CASP, n.d.) which covers the appropriateness of research design and data collection tools, consideration of ethics and the researcher/participant relationship, the rigour of the data analysis, and the overall value of the research. For mixed methods studies, we used the 2018 Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018) which includes the effectiveness of the sampling strategy and sample, the risk of no-response bias, the appropriateness of the measurements and statistical analysis for quantitative studies, the usefulness of using mixed methods, and the interpretations of the results of the quantitative and qualitative components for mixed methods studies.
Data synthesis
We conducted a narrative synthesis, which provides a qualitative summary of the findings. Informed by the Economic and Social Research Council's Methods Programme guidance (Popay et al., 2006), we followed the following steps: (1) We conducted preliminary data synthesis using thematic analysis, in which the main, recurrent and/or most important (based on the review question) themes and/or concepts across multiple studies were identified; (2) We examined how the results converged and diverged for participant subgroups (i.e., immigrant generation status, sex, country of origin); and (3) We used the evidence grading systems described above to assess the robustness of the synthesis. We used a flow diagram following the PRISMA guidelines to report the selection process and all results (Page et al., 2021).
Ethics approval
Ethics approval was not required for this study because it did not involve human participants.
Results
After removing duplicate articles, we screened 7,445 titles and abstracts, of which 145 records were eligible for full-text screening. A total of 32 articles met our eligibility criteria and were included in the review (Figure 1). When we updated the search in 2023, we screened 619 articles and found seven articles to be eligible for full-text screening. One study was found to be eligible in this round of screening. Finally, we included a total of 33 articles of 29 individual studies (N = 9,030 participants) (Table 1).
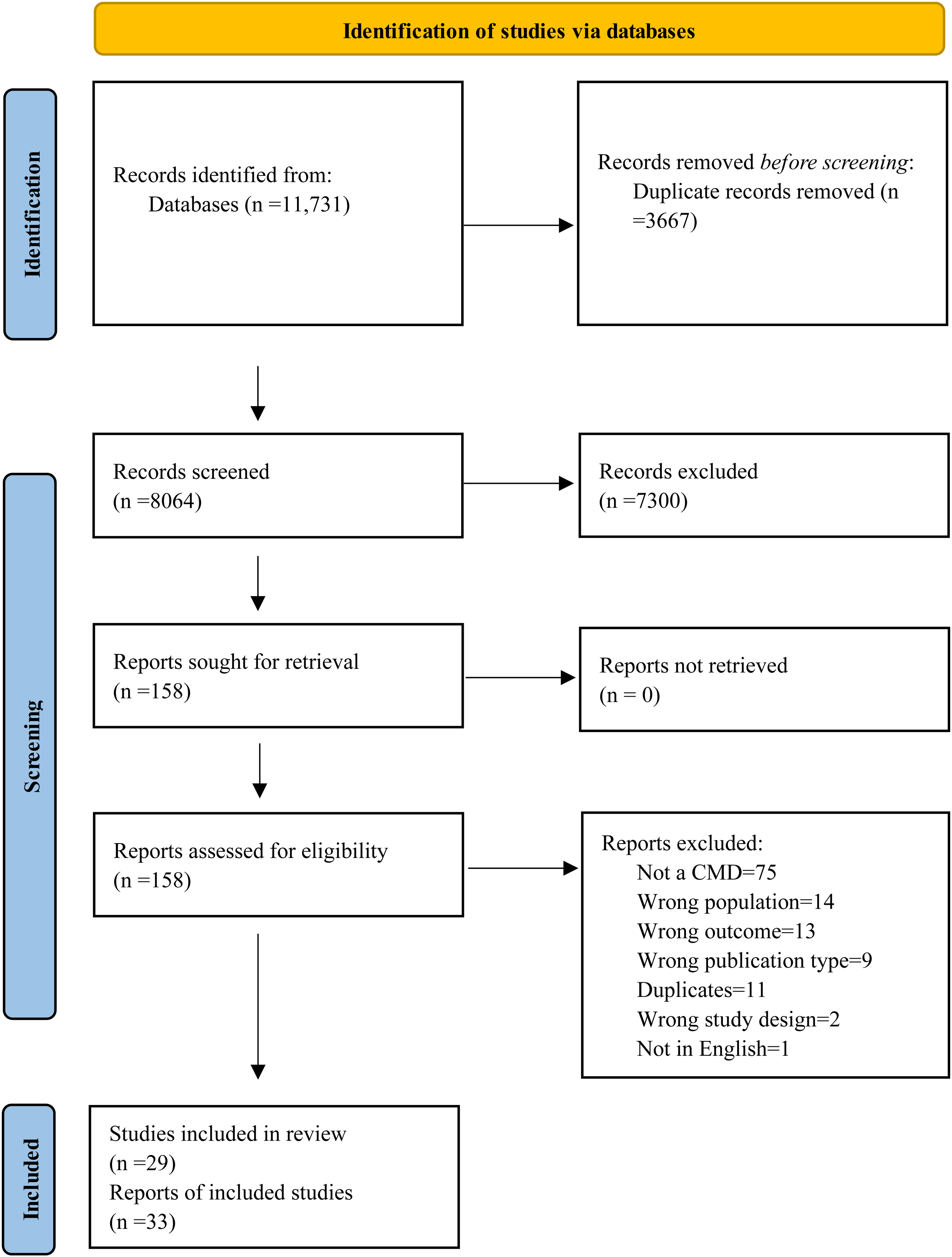
Prisma diagram of identification of included studies in 2022 and 2023.
Summary of included studies (n = 29).

Note. The presented data is only for the relevant South Asian population. However, in one case, the age range is presented for the entire sample because the study did not disaggregate the data (**). Also, in some cases the mean age was calculated by the authors of this review (*).
In Table 1, we present the findings of the included studies in two categories (explanatory models and help-seeking), the definitions of which can be found in the eligibility criteria section of the Methods.
Characteristics of included reports
Most of the reports were qualitative (n = 15), focusing exclusively on depressive disorders (n = 21), and explored a combination of explanatory models and help-seeking (n = 27). The studies were primarily based in the UK (n = 20). Other countries included Australia (n = 3), Canada (n = 2), Norway (n = 1), the United States (n = 2), and Greece (n = 1). The participants in the included reports were recruited online (n = 3), from the community (including educational institutes) (n = 16), healthcare settings (n = 11), or a combination of community and healthcare settings (n = 3). The ages of the participants ranged from 16 to 90. The year of publication of the included reports ranged from 1994 to 2022.
Quality of included reports
The detailed quality assessment is summarised in the Supplementary Materials. The quality of the qualitative articles was generally high. The primary concern for seven out of 15 of the qualitative articles was inadequate consideration of the researcher–participant relationship. Another issue with some of the qualitative studies was insufficient detail on the data analysis process. For mixed methods articles, the authors justified why this study design was used, and both the qualitative and quantitative components were explained in detail. The quantitative articles were assessed to be of good quality. However, many samples were sourced from primary care services, and therefore over-represented individuals who engage with mainstream healthcare, with consequent implications for findings on help-seeking.
Key themes: Explanatory models
Understandings of CMDs
Descriptions of mental health: Descriptions of mental health varied among the South Asian participants in the included studies. A 2011 UK-based study found that South Asian participants did not identify with diagnostic words based on Western understandings of CMDs. One Tamil participant drew on their experience working at a GP practice, saying, “Lots of people who come to us do not have a clue of what they are going through … there's still lack of knowledge and awareness among this community.” Another participant mentioned that there is no direct translation for “anxiety” in Urdu (Loewenthal et al., 2012). The participants in this study were more familiar with general mental health concepts and this topic sparked discussion on the term “pagol” (mad or crazy in Hindi). Conversely, in Mallin and Popay's study with 31 individuals of Pakistani origin (19 first-generation immigrants to the UK, 12 UK-born) recruited from a GP practice, it was found that participants were willing to use diagnostic terms such as depression (Mallinson & Popay, 2007). Those Pakistani-origin participants who did not use diagnostic terms such as depression or anxiety instead used descriptions such as “worried and on edge,” “really down and weak,” and “very low” (Mallinson & Popay, 2007, p. 864). In the 2017 Antoniades et al. study, it was found that Sri Lankan participants with depression used terms echoing “a sense of entrapment” (i.e., hopelessness), while the Anglo-Australian participants used terms to convey a “force weighing or dragging them down” (Antoniades et al., 2017, p. 5).
Psychosocial definitions: South Asian participants generally define depression in psychosocial (i.e., life circumstances) rather than biological (i.e., genetic factors or neurotransmitters) terms. For example, Commander et al. (2004) and Bhui et al.'s (2006) studies respectively found that 67% and 86.1% saw their CMD as a psychosocial issue. In McClelland et al.'s study, the British White participants were more likely to endorse biological explanations of depression, while the British Bangladeshi participants were more likely to endorse non-biological explanations such as a boring life (McClelland et al., 2014).
Perceived causes of CMDs
Situational and moral factors: Many South Asian participants in the included studies saw the cause of their CMD as arising from situational factors, rather than biological factors (Roberts et al., 2015; Taylor et al., 2013). They mentioned family conflict, grief/bereavement, missing their family in their country of origin, and generation gaps with their children as possible causes. One participant in Gask et al.'s (2011) study said that their child was disrespectful to their elders and this “comes in form of depression for parents” (p. 53). In a study with South Asian parents of children with obsessive compulsive disorder, participants cited children's friends and parenting/family issues as the most likely causes (Fernández de la Cruz et al., 2016). This was also mirrored in Birtel and Mitchell’s (2023) study where South Asian participants were found to “endorse greater supernatural but also moral beliefs [such as character flaws] about the causes of depression than White British” (p. 11).
Spiritual/religious factors: Participants gave spiritual/religious explanations for CMDs (Hanley, 2007), though less frequently than anticipated. In some studies, participants saw their distress because of “Jinn,” a supernatural being in Islam, or “evil whisperings” (Lavendera et al., 2006; Loewenthal et al., 2012; Wittkowski et al., 2012). In Hanley's (2007) study of South Asian mothers with post-natal depression, religious causes were often cited. However, in a qualitative study with South Asian women with depression in Toronto, no spiritual explanations were given (Ekanayake et al., 2012) and in a study of Sri Lankan Australians with depression, only one spiritual explanation was given (Antoniades et al., 2018).
Experiences of CMDs
Symptoms: Common symptoms expressed were crying, tiredness, hopelessness, aches and pains, isolation (Bhui et al., 2001; Kumari, 2004), “thinking too much,” having “too many emotions” (Rafique, 2010; Wittkowski et al., 2012), trouble concentrating, memory loss, mental tension, and pressure/pain in the head (Lawrence et al., 2006a, 2006b; Rafique, 2010). In Bhui et al.'s (2002) study, it was found that Punjabi individuals with CMD were more likely to report poor concentration and memory than English individuals. Punjabi individuals were also more likely to express their CMD as somatic symptoms than English individuals.
Consequences of CMDs: CMDs were conceptualised as stigmatised issues with social consequences. A 25-year-old male Indian-Australian participant reported, “It's a social statement that, ‘Oh he has depression, I don’t want to get close to him.’ And it's almost like people think it's contagious” (Brijnath & Antoniades, 2018, p. 8). The same study showed that South Asian Australians were more likely to focus on the social impact of their depression, in contrast to Anglo-Australians who were more concerned with the work impact (Brijnath & Antoniades, 2018). Additionally, a mixed methods study in California found that fear of gossip in the South Asian community was directly related to anxiety (Roberts et al., 2015).
Generational differences in explanatory models of CMDs
Cultural differences in the understanding and experience of CMDs between parents and their children or older and younger generations emerged as a common theme on CMD cause, experience, and help-seeking.
In some studies, participants noted that their CMD stemmed from cultural differences (e.g., thoughts on marriage, rules, Westernisation) between themselves and their parents and/or other family members (Ekanayake et al., 2012). In Roberts et al.'s (2015, p. 11) study with Punjabi individuals in California, one participant said “… as an adolescent it's depressing … you’re growing up in this first-generation culture where it's like your parents don’t understand where you’re coming from … there can be times that it can be, you know, really depressing.” Additionally, Farver et al.'s (2002) study found that adolescents were more likely to be assimilated to their country of residence than their parents and that families with larger acculturation gaps had higher anxiety scores.
Beyond cultural differences being a root of CMD development, disparities in the understanding of, and attitudes towards, CMDs between parents and their children and/or older and younger generations were also apparent. In McClelland et al.'s (2014) study, the older British Bangladeshi participants were more likely to demonstrate negative perceptions of depression younger British Bangladeshis and British Whites. The older British Bangladeshi participants also had more stigmatising beliefs about depression like it resulting from personal failures and leading to consequences for the family's respect (McClelland et al., 2014). Similarly, Furnham and Malik (1994) found that the young South Asian sample in their study held beliefs on depression that were consistent with their British counterparts. Conversely, for example, an older-generation South Asian participant stated that “the depression that exists in Indian-Australians, it really is nothing, it's just the style of living” (Gilbert et al., 2019, p. 297). This result was mirrored in Antoniades et al.'s (2018) study. A 22-year-old participant stated: “my parents were like ‘there is no such thing as depression … no one is depressed in Sri Lanka” (p. 6).
Key themes: Help-seeking
Informal care
Many self-management techniques for depression and anxiety were reported, such as distraction (“keeping busy”), getting married, crying, exercise, altering your perspective to a more positive one, and “sitting and thinking” (Brijnath & Antoniades, 2018; Gask et al., 2011; Kumari, 2004; Markova et al., 2020a, 2020b; Rüdell et al., 2008). In Norway, Markova et al. (2020a, 2020b) found that Pakistani immigrants preferred disengagement coping strategies (such as avoidance, distraction, and finding a partner) in comparison to other immigrant groups and Norwegian students (Markova et al., 2020a, 2020b). While some participants reported wanting to keep their mental health issues private, others described talking to family and friends as a source of support. A mixed methods study with Bangladeshi individuals in the UK found that 68.4% used social help-seeking (i.e., speaking with your family) (Rüdell et al., 2008). Additionally, spiritual coping strategies such as praying or visiting a faith healer were frequently cited in studies examining help-seeking (Taylor et al., 2013). Finally, one study highlighted how participants sought support from “compatriots” online, who in this case were people with lived experiences or those who had a deep understanding of mental health issues (Antoniades et al., 2018).
Formal care
South Asian participants’ views on attending primary care to receive treatment for depression and/or anxiety were mixed. Some reported not wanting to see a GP for fear of judgement, issues of confidentiality, miscommunication, only going to the GP for physical health problems, and lack of access (Gask et al., 2011). For example, Wittkowski et al.'s (2012) study with 10 South Asian mothers with postnatal depression highlighted that they did not feel comfortable going to a male GP, especially since they thought they would be judged for the number of children they had. In Kumari's (2004) qualitative survey, only 2/88 participants (who were all in counselling) said they would see a doctor for mental health problems. Similarly, a participant in another study mentioned that depression is a problem of the mind and as such “doctors’ medicine cannot work” (Lavender et al., 2006, p. 655) Conversely, participants in another study stated that “the doctor should decide what is best for the patient as he knows better” (Gask et al., 2011, p. 52). Another participant believed that medication could positively impact the mind (Lavendera et al., 2006). In Rüdell et al.'s (2008) study, Bangladeshi participants were more likely than their White British and Black Caribbean peers to visit a GP, receive medication, and find it helpful.
A Canadian survey found that South Asians underutilised mental health care services; 51.4% of South Asians with suicidal ideation reported seeking help for their mental health concerns in the past year (Chiu et al., 2018). In another study, it was found that most South Asian participants had contacted a family doctor but only 55% had discussed their mental health concerns (Commander et al., 2004). In Mallinson and Popay's (2007) quantitative study, White women and Pakistani individuals with depression were found to visit GPs a similar number of times for symptoms of depression of anxiety, “GP consultation rates were higher in depressed people of Pakistani origin because they consulted more often for bodily symptoms” (p. 862).
Finally, perspectives on strategies to address cultural issues in primary care were highlighted. A study based in a community health centre for South Asian women found that participants wanted to attend healthcare services with professionals of their own cultural background (Kumari, 2004). The presence of interpreters at GP services was not found to be useful to some because of mistranslation issues and preferring to speak to their doctor directly and confidentially (Loewenthal et al., 2012). Some participants in Lavendera et al.’s (2006) study recommended the use of mullahs (Islamic religious leaders) alongside GPs: “Without mullah, doctor cannot do anything.”
Generational differences in help-seeking
Furnham and Malik’s (1994) study found that younger-generation participants preferred speaking to friends for support, while the older generation preferred to speak with family. One explanation some participants cited was that their family members lacked understanding of mental health and would therefore be unable to help: “they just have absolutely no understanding of it … if I said to my mum, all she is going to do is pray” (Antoniades et al., 2018, p. 8). Other participants mentioned that they would not seek help from mental health professionals without permission from their parents (Antoniades et al., 2018): “I would get permission from my parents first and then I would go there” (p. 6). Antoniades et al.'s study also illustrated the role that family plays in promoting help-seeking behaviour. The Anglo-Australian participants were more likely to be encouraged by their friends, while for Sri Lankan Australians family members were more important (Antoniades et al., 2018).
Discussion
To our knowledge, this is the first systematic review that aimed to synthesise the evidence on explanatory models of CMDs and help-seeking among South Asians living in HICs. The following sections highlight our key findings.
Explanatory models
The South Asian participants in the included studies primarily described CMDs in non-diagnostic terms such as “feeling low,” although some participants were comfortable using labels such as “depression” or “anxiety.” These descriptions were echoed in Awan et al.'s (2022) systematic review; South Asian participants with long-term conditions were more likely to use words such as “tension,” “stress,” or “anger” to explain their emotional distress than medical terms. This use of non-diagnostic terminology is likely related to how South Asian individuals often frame CMDs as psychosocial (resulting from factors such as family conflict or personality traits) or religious issues rather than biological. It may therefore be necessary to invest in the development of culturally adapted psychosocial interventions for this population in addition to pharmacological interventions. For example, psychosocial group interventions (“structured cognitive, behavioural and social interventions intended to improve mental health implemented among a group of people who meet together on multiple occasions” (Mathias et al., 2023, p. 2)) run in South Asia were shown to improve mental health outcomes at intrapersonal, interpersonal, and community levels because they increased participants’ awareness of mental health tools and resources, provided trusting relationships, and increased their feelings of social support and inclusion (Mathias et al., 2023).
Stigma also influences the explanatory models of CMDs for this population. The included studies showed that many South Asian participants were concerned about the social consequences of their CMD, such as being labelled as “weak” or “crazy” in their family or wider community. Based on the definitions of Corrigan and Rao (2012), two types of stigma are particularly important for the South Asian diaspora in HICs; public stigma (“the prejudice and discrimination directed at a group by the larger population”) and self-stigma (“when people internalize these public attitudes and suffer numerous negative consequences as a result”) (Corrigan & Rao, 2012). Addressing all forms of stigma in South Asian communities is crucial to increase help-seeking and improve mental health outcomes. In Naeem et al.'s (2020) “call to action,” the authors bring attention to how stigma acts as a barrier to accessing support for South Asian Canadians. When discussing strategies to address stigma, they point to Fung et al.'s (2022) study with 495 Asian men in Toronto (including South Asian men). Stigma-reducing interventions such as acceptance and commitment therapy (ACT), contact-based empowerment education, or both, and psychoeducation were found to be effective due to mediating factors such as empowerment and, for ACT, “psychological flexibility.”
Family dynamics
Family dynamics played an important role in how South Asian individuals perceived the cause, impact, and experience of their CMD, which in turn influenced their preferred coping strategies. For some participants, family acted as a protective factor and their primary support, while for others family acted as a cause for CMD and a barrier to help-seeking. These mixed results are echoed in Anand and Cochrane’s (2005) review of British South Asians’ mental health status, where they found that for this group “family is both a source of strength and a source of stress.”
Family issues, a psychosocial factor, were cited as a cause for the onset of depression or anxiety in multiple studies (Antoniades et al., 2017; Ekanayake et al., 2012; Rafique, 2010; Wittkowski et al., 2012) . Our results highlighted that one of the most significant issues described was conflict arising from cultural differences within families, especially between first-generation parents and their second-generation children or grandchildren. Similarly, in a recent study, it was found that grandmothers with granddaughters who considered themselves “Hindu” or “Indian” over British, had better psychological adjustment scores (Guglani et al., 2000). Second-generation children, meanwhile, have the pressure of balancing their family culture and their host country's culture, which can lead to heightened levels of stress and anxiety (Shariff, 2009). These findings also appear to be true from the perspective of healthcare providers. Rastogi et al. (2014) and Islam et al. (2022) interviewed clinicians and mental health workers with experience of working with people of South Asian origin in the United States and Canada respectively and both groups of study participants perceived cultural differences (in ideas about mental health, academics, dating, and clothing, for example) to be a cause for the onset of CMDs and a barrier to mental healthcare (Islam et al., 2022; Rastogi et al., 2014). Also, while this review was specific to HICs, attributing a CMD to life circumstances has also been seen in low-income settings. For example, a study of primary care attenders with a CMD in India found that the most common explanation for their illness was psychosocial factors such as marital strife and concerns about family members with alcoholism (Patel et al., 1998).
We also found that many participants were primarily concerned with the impact their CMD would have on their family, which is unsurprising given that it is well established that South Asians endorse a collectivist orientation where the family is prioritised over the individual. In some cases, it emerged that CMDs were not discussed with family in order to protect them from pain, worry, or humiliation (Brijnath & Antoniades, 2018). This finding was echoed in Rafique’s (2010) study, where participants did not want to concern their family with their worries, and in Loewenthal et al.'s (2012) study where an older Tamil participant stated that they turned to religion as a coping strategy to remain “strong” for their family.
Conversely, other participants stated that support from family was essential to combating depression and that they would rather share their mental health issues with family than with a professional (Hanley, 2007; Lawrence et al., 2006a, 2006b). This finding is supported by the theory that perceived support from a spouse or family can reduce depressive symptoms (Singla et al., 2021). Further, family played an important role in accessing primary care services, which ranged from wanting a husband to be present when seeing a male doctor (Wittkowski et al., 2012) to requiring their child to be present to translate from their spoken language to English (Loewenthal et al., 2012). These results were also mirrored in Prajabati and Liebling's (2022) systematic review of South Asians and mental health service use in the UK, which found that “family was viewed as the main source of support.”
Coping strategies
Individual coping strategies such as crying, praying, exercise, isolation, or thinking were a prominent finding in this review. One proposed reason is that the familial factors often translate to private coping strategies as they avoid issues of shame, stigma, and familial burden (Cinnirella & Loewenthal, 1999). This may be especially true for girls and women. For example, in Loewenthal et al.'s (2012) study, in addition to stigma, the female participants expressed that they wanted to remain strong (and therefore not seek help) given the patriarchal nature of the community (Loewenthal et al., 2012). This finding is mirrored in a 2021 study with British-born South Asian girls, which found that the “desire to avoid disrupting cultural norms can close down opportunities to seek help” (Sangar & Howe, 2021, p. 19). Additionally, a study in Scotland found that shame resulting from stigmatised views on mental health problems decreased social and professional help-seeking in Indian, Pakistani, and Chinese communities in Scotland (Knifton, 2012).
Besides family considerations, there are other plausible explanations for why self-reliance and individual coping strategies (such as using “inner strength”) were found to be popular in the included studies. We found that South Asian individuals attributed depression/anxiety to attitudinal factors (Lawrence et al., 2006a, 2006b). This was also seen in a study that found that South Asian students were more likely to link character deficit to mental illness than their White counterparts (Mokkarala et al., 2016). Considering that “cultural causal beliefs about mental distress [are] significant predictors of attitudes for seeking help” (Sheikh & Furnham, 2000, p. 326), we can posit that viewing CMDs as a consequence of personal problems is correlated to the use of individual help-seeking strategies.
Implications for clinicians and service delivery
To better integrate culture into mental health service delivery in high-income settings, the following should be considered. First, it is important for healthcare professionals to acknowledge, and therefore make time for, exploring their South Asian patients’ cultural context in order to deliver person-centred care (Keynejad, 2011). Efforts in clinical settings have escalated in recent years through the implementation of tools such as the Cultural Formulation Interview, which is a guide to help clinicians elicit information on their patients’ social and cultural context. However, there are some limitations. In a recent review of its trial, Jarvis et al. (2020) highlighted that some clinicians without social sciences backgrounds struggled to understand a question intending to determine “clinically relevant aspects of the patient's cultural identity” (p. 41). Second, healthcare professionals and decision-makers must be aware of the significant role that families and differing immigrant generation status play in the development and treatment of, and recovery from, CMDs. In the Kingdom of Saudia Arabia, for example, pharmacological intervention (i.e., prescribing medication) was the most common form of support offered to patients for mental health issues (71%), compared to family therapy (8%) (Algahtani et al., 2017; Rathod et al., 2017). A study with South Asian families in the United States has suggested that care providers allow for differences in values between parents and their children when addressing mental health concerns (Sharma et al., 2020). Culturally adapted family therapy could use the tool of “cultural brokering” in which issues between first-generation South Asian parents and their second-generation children are reframed as a difference in cultural values, rather than a problem stemming from an individual (Segal, 2018; Shariff, 2009). Third, strengthening and diversifying the healthcare workforce may make care more accessible to some South Asian individuals, which can include involving traditional or faith healers in primary care or working with key community members to deliver educational workshops (Keynejad, 2011; Shah et al., 2023). Fourth, community-based interventions, outside of the traditional healthcare system, need to be considered to increase access to care for South Asians with CMD. Digital technology could offer an important avenue to deliver said interventions: “these platforms can be designed with features that are culturally tailored and available in multiple languages” (Shah et al., 2023, p. 382). Finally, future research should focus on South Asian sub-groups (i.e., by country of origin) and immigration generation to develop prevention strategies and service delivery (Prajabati & Liebling, 2022).
Limitations
This review had some limitations. First, we only included English publications. However, considering that most research from HICs is published in English journals, it is unlikely that we have missed publications that are published in non-English languages. Second, some articles in the search did not define South Asian in their study context and were excluded. Therefore, some articles may have met this review's inclusion criteria but were excluded due to lack of detailed definitions. Third, most of the studies were based in the UK, which potentially limits the generalisability of these findings, considering that a host country's political-social-cultural environment can impact an individual's explanatory models. Fourth, inter-rater reliability was not calculated between the reviewers for the data selection process, which could impact the reliability of the review. Fifth, considering that this is an exploratory systematic review, we did not weight the findings of the included reports based on the quality assessment.
Importantly, the selected articles included varying sub-groups within the group of “South Asian,” which meant that sub-group analysis by country of origin was not possible. This limitation is important given the economic, political, cultural, and social differences that exist within this group (Prajapati & Liebling, 2022). Additionally, many articles were not clear about the immigration generation of the South Asian participants, which is important considering that the characteristics associated with ethnicity, passed through generations, could shift through processes such as migration (Durà-Vilà & Hodes, 2012; Rutter & Tienda, 2005). Nevertheless, it was possible to make some conclusions on how the views of parents and their children converge and/or differ regarding CMD understanding, experience, and help-seeking.
Conclusion
Academics, policy makers, and clinicians must work with South Asian communities in their local context to achieve “vertical equity” where healthcare services are tailored to meet the needs and expectations of diverse groups, as opposed to “horizontal equity” where identical services exist for everyone (Tribe & Marshall, 2020). In the past, even when efforts have been made to address issues of diversity and achieve equity in the healthcare systems of HICs, there are “numerous examples of stereotyping of specific cultural groups leading to interventions that are often inadequate or inappropriate” (Gopalkrishnan, 2018, p. 3). An important step in achieving vertical equity is to continuously develop the evidence base on how culture influences explanatory models of, and help-seeking for, CMDs (Deacon, 2013). Exploring the cultural influences on the explanatory models of, and help-seeking for, mental healthcare among South Asian individuals, which this review aimed to do, can provide valuable knowledge to mental health service providers who work in diverse contexts.
Supplemental Material
sj-docx-1-tps-10.1177_13634615241296302 - Supplemental material for Explanatory models of common mental disorders among South Asians in high-income countries: A systematic review
Supplemental material, sj-docx-1-tps-10.1177_13634615241296302 for Explanatory models of common mental disorders among South Asians in high-income countries: A systematic review by Ruchika Jain, Ritsuko Kakuma, Daisy R. Singla, Kirsty Andresen, Khawater Bahkali, and Abhijit Nadkarni in Transcultural Psychiatry
Footnotes
Acknowledgements
Thank you to the librarians at the London School of Hygiene and Tropical Medicine for their support.
Author contribution
Ruchika Jain contributed to all parts of the review as the lead author. Abhijit Nadkarni was the mentor author and provided guidance to Ruchika on all parts of the review as well as the design of the review and contributed to writing and editing the draft paper. Ritsuko Kakuma and Daisy Singla helped with the design of the review and contributed to writing and editing of the draft paper. Kirsty Andresen and Khawater Bahkali contributed to the screening process and reviewed the final paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.