
Abstract
Despite the success of psychoeducational interventions at improving willingness to seek professional help for mental illness, limited research explores the effect of culturally tailored psychoeducational interventions on African American (AA) college students. The objective of this study was to determine if exposure to a culturally relevant psychoeducational intervention impacted AA young adult attitudes, subjective norms, perceived behavioral control, depression stigma, disclosure and willingness to seek help for depression. We conducted a one-group pre- and post-test intervention study of AA college students (N = 75). The 2.5-h intervention featured presentations, large-group discussions, videos, and active learning exercises and was guided by applying a cultural adaptation framework to an existing psychoeducational intervention. The self-administered surveys were created using the Theory of Planned Behavior as a guide. Data were analyzed using paired t-tests. A total of 70 participants completed both pre- and post-test surveys. Overall, willingness, attitude, and disclosure significantly increased after the intervention (p < .001). Additionally, depression stigma significantly decreased after the intervention, indicating fewer stigmatizing beliefs about depression (p < .001). Willingness to seek help for depression among AA college students can be improved through culturally relevant and interactive psychoeducational interventions. These interventions can also improve negative attitudes and perceived behavioral control toward seeking help and decrease stigmatizing beliefs. More research is needed to explore the longitudinal impact of culturally relevant psychoeducational interventions and how they may affect actual help-seeking behavior among AA college students.
Introduction
African Americans (AAs) are only 50% as likely to receive treatment as Whites for depression with similar severity (Williams et al., 2007). This disparity exists across professional mental health services and medication use (Williams et al., 2007). Antidepressants are first-line medication therapy for treating moderate and severe depression and are one of the most commonly used therapeutic drug classes in the United States (DiPiro et al., 2017; National Center for Health Statistics, 2016). Despite a 65% increase in antidepressant use in the last decade, AAs are less likely to initiate antidepressant therapy (Bengtson et al., 2016; Brody & Gu, 2020; Pratt et al., 2017). AA young adults represent a subset at-risk population less likely to receive professional mental health services (e.g., psychosocial interventions or medication therapy), when compared to AA adults and their White young adult counterparts (Substance Abuse and Mental Health Services Administration, 2015). Among those with mental illness, 81% of AA young adults report receiving no professional mental health services compared to 70% of AA adults and 66% of White young adults (Substance Abuse and Mental Health Services Administration, 2015). The objective of this study was to determine if exposure to a pharmacist-led culturally relevant psychoeducational intervention impacts AA college students’ attitude, subjective norm, perceived behavioral control, stigma, disclosure, and willingness to seek help for depression. In this study, we define seeking help for depression as seeking professional help for treatment which might include medication therapy or psychosocial interventions like therapy.
Barriers to seeking treatment for depression that are common across race and ethnicity include cost of services, lack of awareness, and having health insurance that does not cover mental health services (Center for Behavioral Health Statistics and Quality, 2021). Further, young adults and college students face unique barriers to seeking treatment for depression, which include believing that stress is normal in school, a lack of perceived need for help, concerns about confidentiality, and lack of time (Czyz et al., 2013; Eisenberg et al., 2007, 2012). Although factors such as lack of awareness or perceived need may be barriers to help-seeking across all races and for all college students, cultural factors that are unique to AAs and AA young adults like religiosity or spirituality; cultural mistrust; negative attitudes toward treatment; stigma and disclosure; and the influence of family and friends have also been identified (Alvidrez et al., 2008, 2009; Carpenter-Song et al., 2010; Cruz et al., 2008; Matthews et al., 2006; Roberts et al., 2008; Schnittker, 2003; Thompson et al., 2004; Ward et al., 2013). Further, there is evidence that negative attitudes toward treatment; stigma and disclosure; and the influence of family and friends are particularly relevant barriers to help-seeking among AA young adults (Barksdale & Molock, 2009; Duncan & Johnson, 2007; Masuda et al., 2009).
Among those living with and without mental illness, there is evidence that AAs report strong negative attitudes toward psychotropic medications (Alvidrez et al., 2009; Matthews et al., 2006; Schnittker, 2003). AAs report concerns regarding medication safety, side effects, and fear of addiction to or dependence on medications (Alvidrez et al., 2009; Matthews et al., 2006). Some AAs view medications as a temporary fix that masks problems and feel that medications are prescribed to them as a means to get them “out of the way,” leading to feelings of being unheard and ignored by health care professionals (Carpenter-Song et al., 2010; Matthews et al., 2006). Additionally, AA patients report feeling experimented on with regards to medications, especially when medications or dosages are changed (Carpenter-Song et al., 2010). These negative attitudes toward medications are rooted in both personal and historical experiences of racism in health care (Matthews et al., 2006; Mishra et al., 2009). Though younger AAs may have limited experience with prominent examples of racism in health care, such as the Tuskegee experiment and the unethical use of Mrs. Henrietta Lacks’ cells, there is evidence that their health beliefs mirror older generations, who may be more familiar with historical events of racism in health care (Hamilton et al., 2006). Negative attitudes toward medications in AAs have been linked to actual treatment-seeking behaviors, where more medication concerns among AA patients (e.g., “I’ll become addicted to the medication”) were associated with a decrease in treatment engagement (i.e., psychotherapy visits) (Alvidrez et al., 2010).
Stigma and disclosing of a mental illness are two related concepts that have been identified in the literature regarding AAs and mental illness. While some AAs simply identify public stigma (i.e., attitudes and beliefs of the general public about people living with mental illness) as a barrier to help-seeking (Alvidrez et al., 2008; Cruz et al., 2008; Roberts et al., 2008; Thompson et al., 2004), others describe the label that one receives once they seek treatment (Alvidrez et al., 2008). AAs who have sought help for mental illness describe having to bear the diagnosis as a lifelong label (Matthews et al., 2006; Mishra et al., 2009). Some study participants link the disadvantage of being Black and having a lifelong label to racism. These participants report beliefs that help-seeking among Whites is different because seeking treatment while being a member of this group does not affect employment or reduce future opportunities (Matthews et al., 2006). The influence of race on stigma has led researchers to coin the term “double stigma” (Gary, 2005). Double stigma describes situations where AAs face prejudice and discrimination due to minority-group membership and also to being a person living with a mental illness. In addition to being labeled, participants also describe a particular stigma surrounding disclosure of a mental illness. Participants express concerns that disclosure of a mental illness leads to shame, embarrassment, and rejection (Cruz et al., 2008; Matthews et al., 2006), which can also serve as additional barriers to seeking treatment (Cruz et al., 2008; Thompson et al., 2004).
Studies also show the importance of family and friends with regards to AA help-seeking behaviors. Informal support and help-seeking from family or friends are common among AAs. A national representative study reported that among AAs meeting diagnostic criteria for a mental illness, the majority of participants relied on their social networks, with 64% reporting using some sort of informal support (e.g., help from family, friends, or other acquaintances) (Woodward et al., 2008). For AAs, families seem to be an especially important source of support. The literature provides evidence that some AAs believe that problems related to mental illness are to be handled within the family (Alvidrez et al., 2008; Mishra et al., 2009). This belief is also tied to the belief that family issues should not be shared with outsiders and that disclosure of mental illness is unheard of and can bring dishonor, embarrassment, and shame to families (Alvidrez et al., 2008; Carpenter-Song et al., 2010; Hamilton et al., 2006; Matthews et al., 2006; Mishra et al., 2009; Thompson et al., 2004).
Given low levels of help-seeking across all races and ethnicities and even lower levels among AAs, psychoeducational interventions have emerged as a tool to prevent major depressive disorder (Cuijpers et al., 2009), increase mental illness knowledge, decrease stigma, and improve intentions and behaviors related to seeking help (Hadlaczky et al., 2014; Hart et al., 2016; Kitchener & Jorm, 2002). Despite the success of psychoeducational interventions and the identification of cultural variables that are unique to AAs, limited research has addressed the influence of culturally linked barriers and interventions, and even less has focused specifically on AA young adults (Alvidrez et al., 2005, 2009; Primm et al., 2002). Primm et al. evaluated the effectiveness of a psychoeducational video, Black and Blue: Depression in the African-American Community, among AA adults who screened positive for depression at health fairs and in other community settings (Primm et al., 2002). This sample included AA college students as well, although they represented a small proportion (Primm et al., 2002). Although the intervention improved depression knowledge, it was ineffective at decreasing stigma, which significantly increased after the intervention. Another psychoeducational intervention, Mental Health First Aid (MHFA), is a U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) National Evidence-Based Program. Though, MHFA has been successfully developed in various ethnic and cultural groups (e.g., Chinese, rural communities), with measured success in improving knowledge and decreasing stigma (Armstrong et al., 2011; Hart et al., 2016; Jorm et al., 2004; Kanowski et al., 2009; Lam et al., 2010; Minas et al., 2009), no culturally adapted MHFA course exists for AAs.
Considering the disparities that exist in help-seeking among AAs, the unique cultural factors that impact help-seeking, and the success of psychoeducational interventions, there is a need to evaluate the utility of a culturally adapted psychoeducational intervention. In light of the influence of culturally linked attitudes, stigma, and the family among AAs, the Theory of Planned Behavior (TPB) was selected as a model for study outcomes. The TPB posits that behavior is predicted by the intention or willingness to perform the specific behavior. According to the TPB, willingness is then predicted by a person's attitude, subjective norm (i.e., important others who might approve or disapprove of the behavior), and perceived behavioral control (i.e., facilitators and barriers to performing the behavior) related to the behavior in question. Utilizing the TPB and MHFA as guiding frameworks, the objective of this study was to determine if exposure to a pharmacist-led culturally relevant psychoeducational intervention impacts AA college students’ attitude, subjective norm, perceived behavioral control, stigma, disclosure, and willingness to seek help for depression.
Methods
Sample, setting, and intervention
This study was a prospective, pre- and post-test one-group intervention study and has been previously described (Bamgbade et al., 2020). Participants were AA undergraduate students enrolled at a southwestern U.S. university. Inclusion criteria were age between 18 and 25 years old, self-identifying as Black or AA, and no current or previous diagnosis or treatment for a mental health condition. Participants were recruited in partnership with a historically Black fraternity chapter at the university. Study recruitment flyers and emails invited participants to “an interactive information session and discussion about depression [with] the purpose of understanding how African American students’ willingness to seek help for depression can change.” Participants received a US$50 gift certificate for their participation.
The 2.5-h intervention featured presentations, large-group discussions, videos, and active learning exercises and was developed using MHFA and Barrera and Castro's cultural adaptation framework as guiding models (Barrera & Castro, 2006; Kitchener & Jorm, 2002). MHFA, a SAMHSA evidence-based program, is a psychoeducational intervention developed to provide community members with skills to assist someone who may have a mental health problem or crisis (Kitchener & Jorm, 2002). Cultural adaptation of the intervention included changes to discussion topics, activities that allowed for group discussion, videos, and utilizing an AA facilitator, psychologist, and consumer educator. The intervention began with a discussion contrasting health behaviors for a physical illness and a mental illness and a presentation on depression prevalence, signs and symptoms, and treatments. Active learning exercises were also used throughout the intervention to engage participants and emphasize important messages related to the intervention. For example, during one exercise, the pharmacist read a statement (e.g., most people with depression need to be hospitalized) and participants were asked to hold up a fact or fiction sign. When disagreement occurred, participants were asked to discuss the statement with their neighbor, and this was followed up by a large-group discussion. An AA psychologist from the university mental health center moderated a discussion on cultural factors related to seeking help for depression and gave an overview of psychotherapy. Lastly, an AA college student consumer educator from the National Alliance on Mental Illness, who did not attend the participants’ institution, shared his lived experience with major depressive disorder and schizophrenia.
Pre- and post-test surveys
Paper pre- and post-test surveys were administered to participants immediately before and after the intervention. Details regarding development of the survey have been previously described (Bamgbade et al., 2020). In short, surveys were informed by knowledge gained through focus groups of AA young adults and developed using the TPB as a model for survey outcomes. To maintain anonymity and facilitate matching pre- and post-tests, participants were asked to create a unique code from an algorithm. Surveys were pre-tested with five AA pharmacy students who were not included in the study. Minimal wording changes were made. A list of survey questions is provided in Supplemental Table 1.
Theory of Planned Behavior variables
Items related to TPB variables (i.e., willingness, attitude, subjective norm, and perceived behavioral control) were developed in accordance with the TPB and were measured on a bipolar 7-point semantic differential scale ranging from −3 (extremely unlikely) to + 3 (extremely likely). Willingness to seek help was measured using three items with higher scores indicating increased willingness to seek help. Attitude, subjective norm, and perceived behavioral control were assessed using belief-based evaluation or indirect measures (Ajzen, 2002; Montano & Kasprzyk, 2015).
Attitude was comprised of questions about behavioral beliefs (e.g., “If you screened positively for depression, how likely do you think the following outcomes would be if you sought professional help?: Being labeled a depressed person”) and the associated outcome evaluation of that belief (e.g., “Even though you may not agree with the outcomes listed, how good or bad do you feel each of the following outcomes would be if you screened positively for depression and sought professional help?: Being labeled a depressed person”), as per the TPB (Ajzen, 2002; Montano & Kasprzyk, 2015). The measured behavioral belief (b) score and the associated measured outcome evaluation (e) score were multiplied. These values were then summed across all items to create the attitude (A) scale total,
Other variables
Depression stigma was measured using the 9-item personal stigma subscale of the Depression Stigma Scale, which has demonstrated reliability (Griffiths et al., 2004, 2006, 2008). Items were measured on a 5-point Likert scale, with higher scores representing greater levels of depression stigma. Disclosure was measured using five items developed for this study. Items were measured on a bipolar 7-point semantic differential scale ranging from −3 (very unlikely) to + 3 (very likely). The authors added this measure based on findings from focus groups of AA college students who before discussing whether important others would approve or disapprove of their seeking help (i.e., subjective norm), first discussed whether they would share a positive depression screening with their important others. For consistency with TPB variables and with previous literature, disclosure and depression stigma are also presented as scale totals, where higher scores represent a more favorable disposition to disclosure and greater levels of depression stigma, respectively. Lastly, demographic (i.e., age, sex, race/ethnicity, school classification, and major area of study) and personal (i.e., personal experience with mental illness) characteristics were collected.
Data analysis
Descriptive statistics were conducted for all study variables. Paired t-tests were used to analyze changes in willingness, attitude, perceived behavioral control, and depression stigma from pre- to post-test. Effect sizes were calculated using Cohen's d and a Bonferroni correction for multiple t-tests was applied to all p-values, resulting in a corrected p-value for statistical significance of p ≤ .001. Cronbach's alpha was used to assess scale reliability of the depression stigma scale, with alpha coefficients greater than 0.6 considered acceptable and reliable (Shaver et al., 1991). Scale reliability for depression stigma, measured using Cronbach's alpha, was 0.74 at pre-test and 0.73 at post-test. Reliability was not evaluated for measures of TPB variables because there is no assumption of internal consistency. A person may have mixed beliefs regarding a particular behavior. While this is a practical outcome, such a situation would seriously decrease the internal consistency, suggesting a problem with the measures when this is not the case. Theoretically, measures are viewed as an aggregate representation of a latent construct and therefore do not necessitate reliability assessments (Ajzen, 2006). This study was approved by the University of Texas at Austin Institutional Review Board (protocol number: 2016-10-0111). Data were analyzed using SAS (Version 9.4).
Results
Of the 103 students who signed up to participate in the study, 75 participants (72.8%) completed the survey pre-test, and 70 of these (93.3%) completed the post-test survey. Results presented here are only from those who completed both the pre- and post-test surveys. Participant demographic and personal characteristics are detailed in Table 1. Participants were on average 19.7 ± 1.6 years, primarily female (62.9%), and nearly 89 percent of students identified as AA of Black American or AA of African origin. All participants self-identified as Black or AA, including participants who also identified as “other” (e.g., mixed race, Japanese/Asian). School classifications were about equally represented for each classification and participants’ majors were primarily in the natural and health sciences (45.7%) and the professional and applied sciences (41.4%). Lastly, with regards to personal characteristics, 38.6 percent of participants reported having a family member or close friend who was diagnosed with a mental illness which included anxiety, bipolar disorder, depression, and schizophrenia.
Demographic and personal characteristics of participants (n = 70).
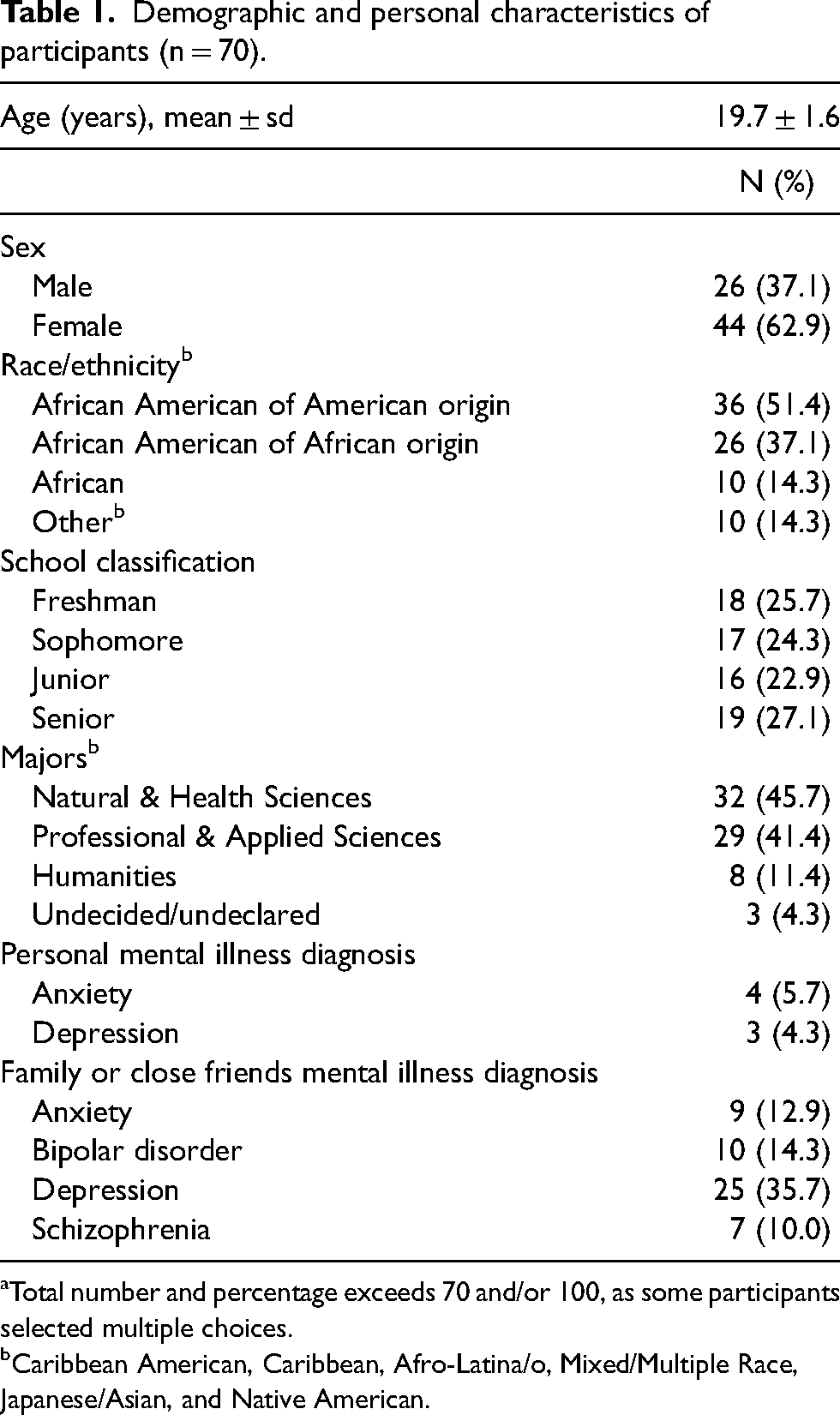
Total number and percentage exceeds 70 and/or 100, as some participants selected multiple choices.
Caribbean American, Caribbean, Afro-Latina/o, Mixed/Multiple Race, Japanese/Asian, and Native American.
Overall, willingness, attitude, and disclosure significantly increased after the intervention (p < .001). Additionally, depression stigma significantly decreased after the intervention, indicating fewer stigmatizing beliefs about depression (p < .001). Results are presented as scale totals or sums, as described in the Methods section.
Following the intervention at post-test, 13 participants screened positively for depression. These students were asked to complete a separate survey and did not answer items related to willingness to seek help and instead answered questions related to actual help-seeking behavior. Results for willingness presented here represent students who screened negatively for depression to allow for appropriate pre-test and post-test comparison (Table 2). At pre-test, participants had a very weak positive willingness to seek professional help (mean = 1.7 ± 4.4). At post-test, participants reported a moderate positive willingness to seek professional help following the intervention (mean = 4.0 ± 4.0). Overall, willingness significantly improved from pre- to post-test (p ≤ 0.05), with a moderate effect size (Cohen's d = 0.55).
Comparison of mean pre-test and post-test scores for willingness to seek professional help (n = 56).
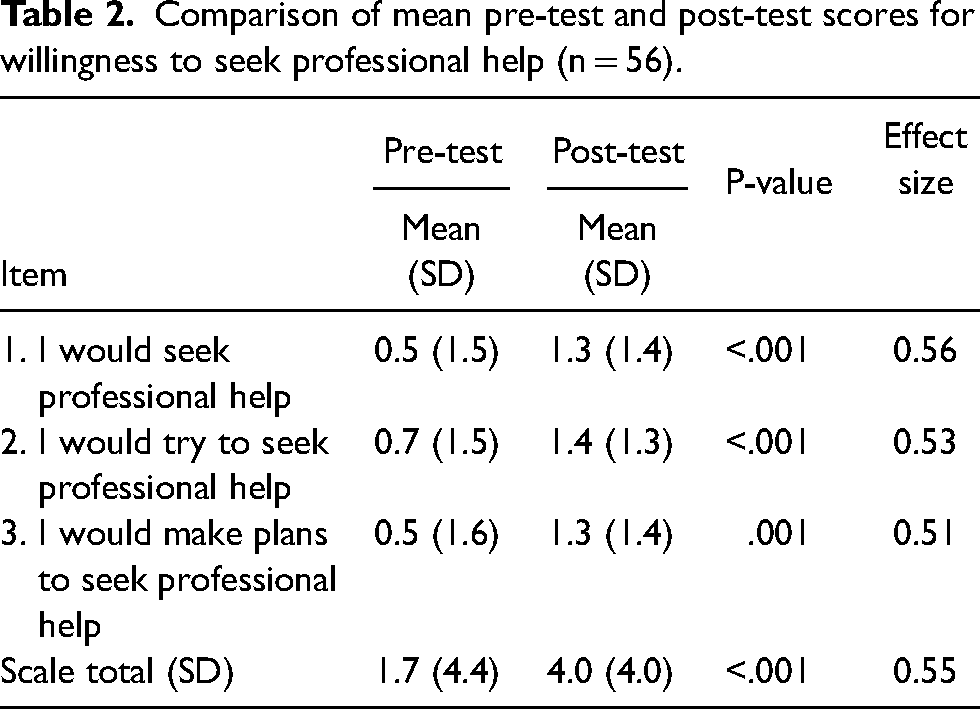
Table 3 displays the results for the TPB variables attitude, subjective norm, and perceived behavioral control. Attitude significantly increased in favorability from pre- to post-test (p < .001), with a moderate effect size (Cohen's d = 0.76). At pre-test, the attitude scale total was 24.6 ± 23.1, reflecting a very weak positive attitude toward seeking professional help for depression. Following the intervention, the overall attitude scale total increased to 43.4 ± 26.1, reflecting a moderately weak positive attitude toward seeking professional help for depression. At both pre- and post-test, the top driver of attitude was the item “talk to someone in a safe space without judgment” (pre: 4.5 ± 4.0; post: 5.9 ± 3.3). The other top drivers of attitude both at pre- and post-test were: talk with someone who is knowledgeable about and understands depression (pre: 4.4 ± 3.9; post: 5.4 ± 4.0); prevent things from getting worse (pre: 4.1 ± 3.0; post: 5.7 ± 3.3); and be able to unload or release (pre: 4.1 ± 3.4; post: 5.3 ± 3.3). The largest changes from pre- to post-test were regarding the items “be a burden to others” (pre: −0.5 ± 3.7; post: 1.7 ± 3.7) and “become dependent on or addicted to medication” (pre: 1.9 ± 5.3; post: 4.0 ± 4.7). Lastly, at both pre- and post-test, there was a divide in attitude scores. For items 1 through 7, scores ranged from 1.9 ± 5.3 to 4.5 ± 4.0 at pre-test and 2.8 ± 3.6 to 5.9 ± 3.3 at post-test. These items were distinct from items 8 through 14, with scores ranging from −0.1 ± 4.1 to 1.0 ± 4.4 at pre-test and 0.4 ± 3.8 to 2.4 ± 4.0 to at post-test.
Comparison of mean pre-test and post-test scores of attitude, subjective norm, and perceived behavioral control (n = 70).
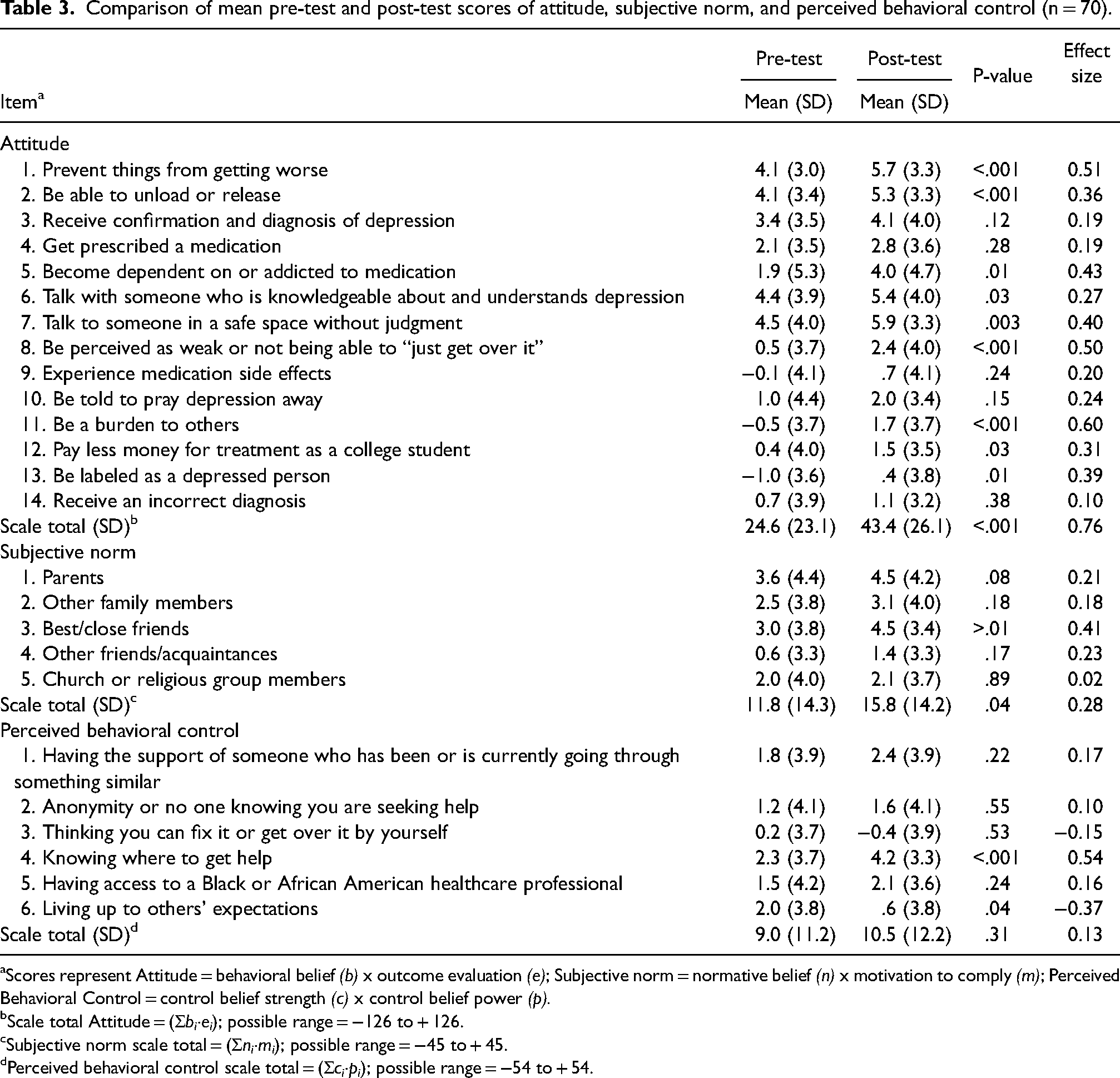
Scores represent Attitude = behavioral belief (b) x outcome evaluation (e); Subjective norm = normative belief (n) x motivation to comply (m); Perceived Behavioral Control = control belief strength (c) x control belief power (p).
Scale total Attitude = (Σbi·ei); possible range = −126 to + 126.
Subjective norm scale total = (Σni·mi); possible range = −45 to + 45.
Perceived behavioral control scale total = (Σci·pi); possible range = −54 to + 54.
The subjective norm scale total of 11.8 ± 14.3 reflected a very weak positive social influence on participants’ seeking professional help for depression. After the intervention, though improved, the subjective norm did not significantly change, with an overall subjective norm score of 15.8 ± 14.2, representing a weak positive social influence. At pre-test, parents had the highest influence on participants’ professional help-seeking (mean = 3.6 ± 4.4), followed by best or close friends (mean = 3.0 ± 3.8). However, at post-test, the influence of parents and best or close friends was the same (mean = 4.5 ± 4.2 and 4.5 ± 3.4, respectively).
The perceived behavioral belief score at pre-test was 9.0 ± 11.2, reflecting a very weak positive perceived control over seeking professional help for depression. At post-test, though improved, participants’ perceived behavioral control did not significantly change, with a perceived behavioral belief scale total of 10.5 ± 12.2, reflecting a very weak positive perceived control. At both pre- and post-test, the top driver of perceived behavioral control was the item “knowing where to get help” (pre: 2.3 ± 3.7; post: 4.2 ± 3.3). At pre-test, the second top driver of perceived behavioral control was “living up to others’ expectations” (mean = 2.0 ± 3.8). However, at post-test, this item changed to the lowest driver of perceived behavioral control (mean = 0.6 ± 3.8).
At pre-test, participants reported an overall disclosure of 0.3 ± 6.8, representing a very weak positive disclosure (Table 4). Following the intervention, participants reported a moderate positive disposition toward disclosure at 3.5 ± 6.4, a significant increase from pre to post (p ≤ 0.001), with a small effect size (Cohen's d = 0.48). At both pre- and post-test, the highest item scores were associated with disclosure to parents (pre: 1.2 ± 2.2; post: 1.5 ± 1.9) and best/close friends (pre: 1.2 ± 1.9; post: 1.7 ± 1.3). Additionally, the largest changes from pre- to post-test were related to disclosure to other friends/acquaintances (pre: −1.1 ± 1.8; post: −0.4 ± 1.7) and church/religious group members (pre: −0.8 ± 2.1; post: 0.1 ± 2.0).
Comparison of mean pre-test and post-test scores for disclosure (n = 70).
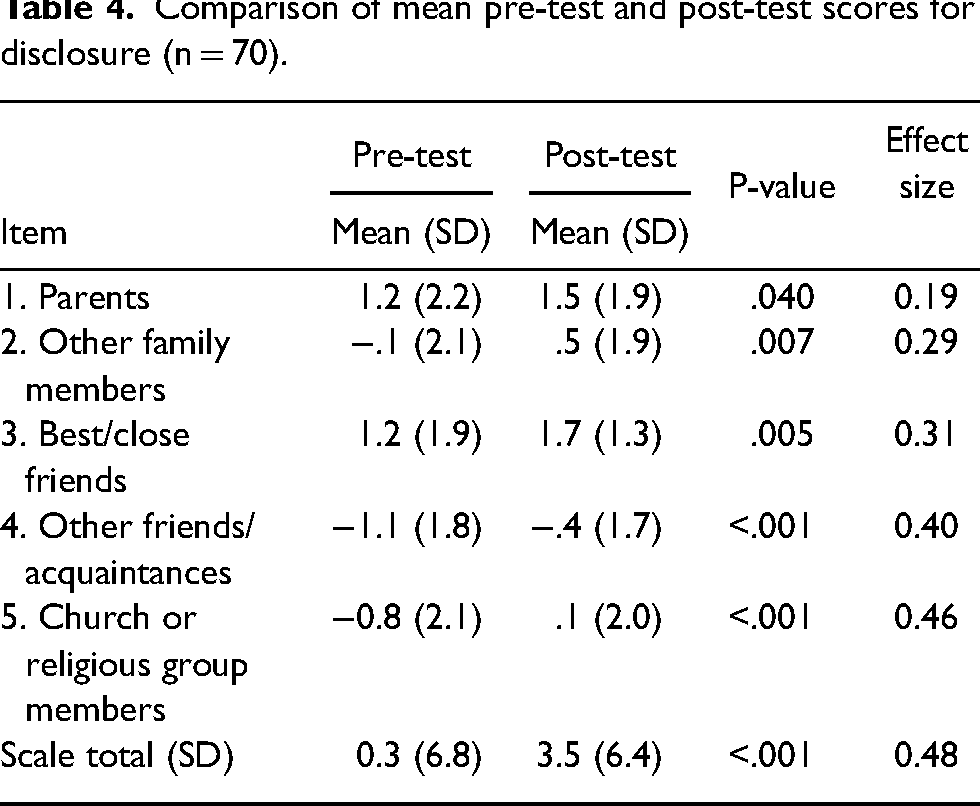
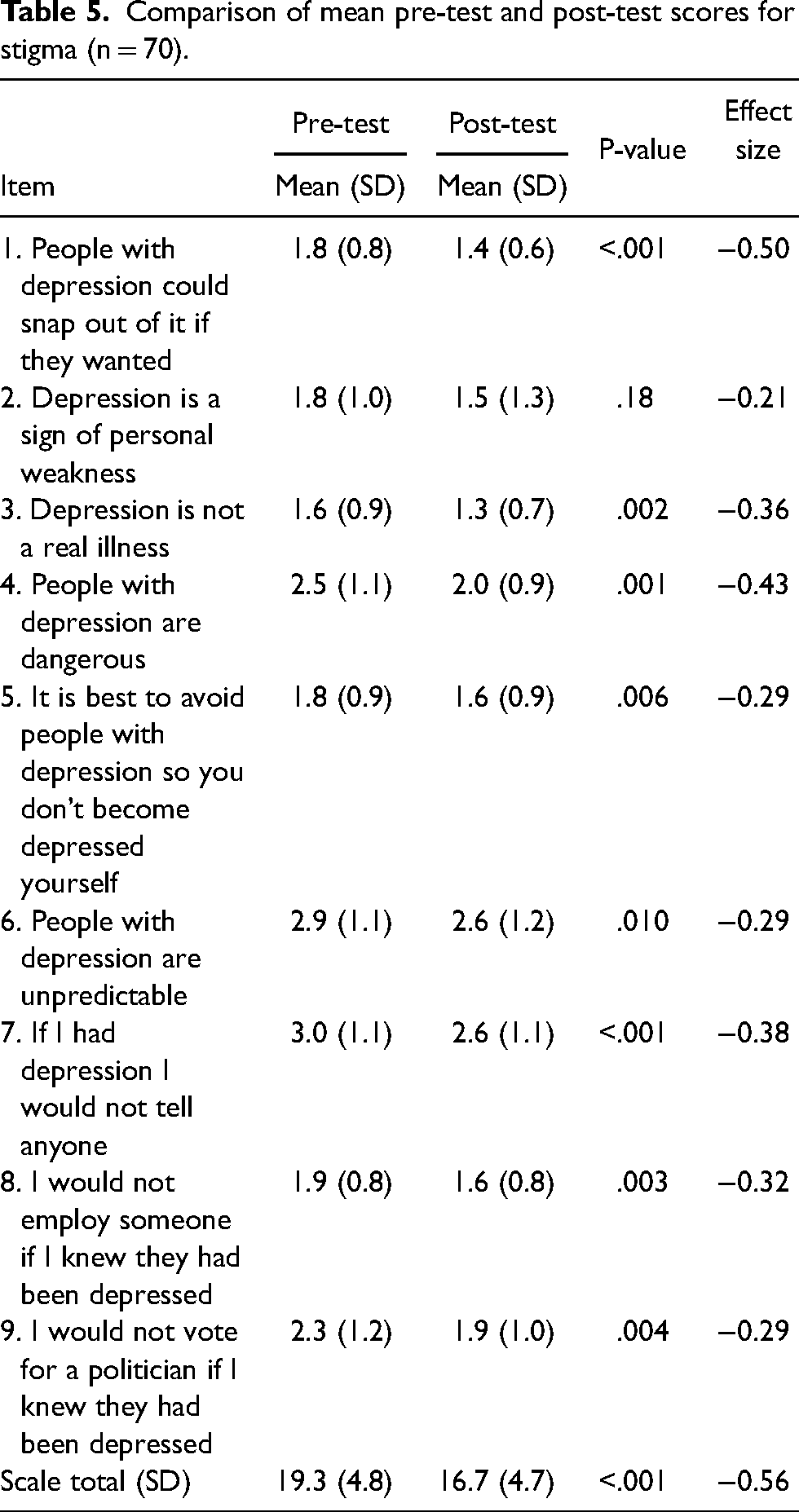
Table 5 displays results related to depression stigma items at pre- and post-test. At pre-test, the depression stigma scale total was 19.3 ± 4.8, on a 5-point Likert scale from 1 (strongly agree) to 5 (strongly disagree). Following the intervention, participants’ depression stigma significantly decreased to 16.7 ± 4.7 (p < .01), with a medium effect size (Cohen's d = −0.56). The largest changes from pre- to post-test were related to participant depression stigma regarding being able to snap out of depression (pre: 1.8 ± 0.8; post:1.4 ± 0.6); the dangerousness of people with depression (pre: 2.5 ± 1.1; post: 2.0 ± 0.9); not telling anyone if they had depression (pre: 3.0 ± 1.1; post:2.6 ± 1.1); and voting for a politician living with depression (pre: 2.3 ± 1.2; post: 1.9 ± 1.0).
Comparison of mean pre-test and post-test scores for stigma (n = 70).
Discussion
This study provides preliminary evidence that a culturally relevant, theory-based, interactive psychoeducational intervention can improve participants’ willingness to seek professional help, decrease their depression stigma, and positively change their attitude and disclosure regarding seeking professional help immediately following intervention. This study adds to the growing literature regarding the positive impact of psychoeducational interventions and further extends the literature by demonstrating the potential utility for culturally relevant interventions targeted toward AA young adults.
Our findings that willingness to seek professional help, depression stigma, and attitude significantly changed and that these changes represented a medium effect size by conventional definitions is consistent with previous research of psychoeducational intervention in college students which similarly found significant changes in stigma and attitude toward seeking professional help that represented medium effect sizes (Conceição et al., 2022; Sharp et al., 2006; Taylor-Rodgers & Batterham, 2014). Further, these studies provide evidence that these immediate effects persist for up to four or five months post-intervention, and that these changes represent medium effect sizes (Conceição et al., 2022; Sharp et al., 2006; Taylor-Rodgers & Batterham, 2014). It is possible that the effect of this culturally tailored intervention similarly persisted five months after it was administered. More research is needed to further explore this.
At pre-test, participants had a weak positive willingness to seek professional help for depression. Following the intervention at immediate post-test, participants’ willingness significantly increased to a moderate positive willingness. This finding is similar to findings in another study of students who completed an MHFA course. Immediately after the intervention, participants reported increased willingness to seek help (e.g., professional, non-professional, or self-help) and were significantly less likely to report a non-help-seeking action (e.g., do nothing or push people away) (Hart et al., 2016). Intention, in the present study measured as willingness, has been shown to be a valid and significant predictor of behavior (Armitage & Conner, 2001; Azen & Madden, 1986; Godin & Kok, 1996). Therefore, AA college students’ help-seeking may be increased by targeting their willingness to seek professional help and subsequently may lead to help-seeking behavior. Given differences in willingness observed between the literature and the present study, there is still an opportunity to improve AA college student willingness, thereby potentially improving help-seeking behavior.
Participants’ attitude significantly increased post-intervention with a medium effect size, though at post-test attitude was still relatively weak and positive. More favorable attitude following a psychoeducational intervention in the present study is consistent with the literature (Hadlaczky et al., 2014; Jorm et al., 2004; Kitchener & Jorm, 2002; Lam et al., 2010; Primm et al., 2002). The largest contributors to attitude at pre- and post-test were talking to someone in a safe space without judgment; talking to someone who is knowledgeable about and understands depression; and being able to unload or release. This finding is unique to the literature and provides insight into AA young adults and help-seeking. When seeking help for depression, students may want to “unload” their issues in a safe space with someone who is familiar with depression. While the literature surrounding AA help-seeking has often focused on other concepts such as stigma and religiosity, future interventions may consider emphasizing concepts of “unloading,” safe spaces, and knowledgeable providers when discussing help-seeking among AA young adults. The largest change from pre to post was regarding the item being a burden to others (pre-test: −0.5 ± 3.7; post-test: 1.7 ± 3.7). Participants described their desire to not be a burden in terms of not wanting to worry their parents or others with their problems. During the intervention, these concerns were directly challenged by the consumer educator. In discussing his lived experience, the consumer educator talked about his fears in sharing his diagnosis with his family and friends and shared how revealing his diagnosis was met with support and understanding. Hearing this experience from the consumer educator may have been instrumental in changing participants’ views, especially considering that participants identified the consumer educator as one of the most impactful components of the intervention in intervention evaluations. The second largest attitudinal change from pre to post was the item become dependent on or addicted to medication (pre-test: 1.9 ± 5.3; post-test: 4.0 ± 4.7), though it was not statistically significant after Bonferroni correction. The literature provides evidence that AAs have strong negative views toward psychotropic medications (Alvidrez et al., 2009; Matthews et al., 2006). This change from pre to post may be because a significant amount of time was spent on this issue during the intervention due to participant discussion. During the fact or fiction activity, one statement presented was, “Fact or Fiction: Antidepressants are addictive.” Students were surprised to learn that the statement was fiction. Their surprise generated a robust discussion about addiction and medications, which was led by the primary researcher, who is a licensed pharmacist. Primm et al. had similar findings in their study which involved a psychoeducational video intervention. The percentage of participants who disagreed or strongly disagreed with the item “Antidepressant medicines are usually addictive” increased and was one of the largest changes among the attitudinal beliefs evaluated in the study (Primm et al., 2002). When engaging with AA young adults, clinicians might consider spending time discussing medications and addiction science to address any potential misinformation regarding mental health therapy. Lastly, for both pre- and post-test attitude, there was a considerable drop in scores. For items 1 through 7, scores ranged from 1.9 ± 5.3 to 4.5 ± 4.0 at pre-test and 2.8 ± 3.6 to 5.9 ± 3.3 at post-test. These items were distinct from items 8 through 14, with scores ranging from −0.1 ± 4.1 to 1.0 ± 4.4 at pre-test and 0.4 ± 3.8 to 2.4 ± 4.0 to at post-test. This divide seems to separate items that are generally personal (i.e., prevent things from getting worse; talk to someone in a safe space without judgment) from items that relate to other people and stigma (i.e., be a burden to others, be told to pray depression away). This suggests that attitudes toward professional help-seeking may be driven more by personally based attitudes and less by other people and stigma. Researchers should consider emphasizing positive, personally related attitudinal beliefs when designing interventions for AA college students and focus less on efforts to manage public stigma.
Though improved, participants’ subjective norm did not significantly change from pre- to post-test after Bonferroni correction. Before and after the intervention, the biggest driver of subjective norm was parents. The literature provides evidence of the important role that family plays in AA mental health help-seeking (Alvidrez et al., 2008; Carpenter-Song et al., 2010; Masuda et al., 2012; Matthews et al., 2006; Mishra et al., 2009; Thompson et al., 2004). Furthermore, there is evidence that as people mature from adolescence to young adulthood, normative influences shift away from peers and shift toward parents and trusted adults (Biddle et al., 1980). Interventions specifically targeted toward students who have screened positively for depression might consider incorporating parents directly into their efforts and clinical encounters as a joint intervention. In contrast to subjective norm, disclosure significantly improved from a very weak positive disposition toward disclosure to a moderate positive disposition toward disclosure. At pre- and post-test, the highest item scores were associated with disclosure to parents and best/close friends. Before the intervention, participants were willing to disclose to their best/close friends though they were less influenced by their best/close friends (subjective norm). This distinction supports our previous focus group findings where when discussing normative beliefs, focus group participants would first discuss whether they would disclose screening results with important others. It also highlights the need to distinguish between normative beliefs and disclosure in young adults. Assessing only normative beliefs in young adults may provide an incomplete picture with regards to depression help-seeking. Though participants’ normative beliefs were driven by their parents, they felt more comfortable disclosing to their friends. More research is needed to further explore the relationship between disclosure, subjective norm, and help-seeking for depression in young AA college students.
At pre-test, participants reported a very weak positive perceived behavioral control over seeking professional help for depression. Immediately following the intervention, though improved, participants’ perceived behavioral control did not significantly change. Although perceived behavioral control did not change significantly from pre- to post-test, the item “knowing where to get help” was a large driver of perceived behavioral control at pre- and post-test, with a medium effect size. Before the intervention, participants reported somewhat having control over knowing where to get help, and following the intervention participants reported having the most control over knowing where to get help. At freshman orientation, students are told that there are professional mental health services available to them on campus and are told the building where these services are located. During the intervention, students met and engaged with a licensed AA psychologist from the university health center who specifically served as the liaison to Black and AA students within the counseling and mental health center. Also, students received printed information on specific opportunities to receive professional help (e.g., date, time, and location for a black voices support group, women of color discussion group, and office hours of diversity coordinators). It is possible that personifying professional help through interacting with the AA diversity liaison psychologist and receiving more specific information about available services led to students’ perceiving more control of knowing where to get help. College and universities may consider providing students, especially those at risk for not seeking help like AA students, with specific information about available resources. Colleges and universities might even consider having counselors and diversity counselors meet with students at events like freshman orientation or through course guest lectures to help personify professional help. Further, colleges and universities should consider making these encounters interactive by featuring activities like the Q&A session used in the present study.
At pre-test, participants reported low depression stigma. The Depression Stigma Scale (DSS), used to measure stigma in the present study, has primarily been used in studies conducted outside of the United States. Studies of adults in Europe (multi-country), Australia, Japan, and Germany suggest that participants in the present study may have lower stigma toward depression than other groups (Coppens et al., 2013; Dietrich et al., 2014; Griffiths et al., 2006). At pre-test, the stigma sum score of the present study was 19.3 ± 4.8. This was lower than the sum scores of 23.4 ± 6.9 and 24.0 reported in two European studies of community-dwelling adults (Coppens et al., 2013; Dietrich et al., 2014). Though depression stigma scores are objectively lower compared to previous studies, it is unclear whether these differences are significant. Lower depression stigma in the present study may be related to participants’ majors and areas of study, as 87.1 percent of participants were natural and health sciences or professional and applied sciences majors. Additionally, some participants were members of the University of Texas Black Health Professions Organization. Participants’ majors and organizational involvement suggest that these students may have plans to become health care professionals themselves, which may explain their lower depression stigma. Despite low stigma scores at pre-test, at post-test participants’ stigma significantly decreased. Although statistically significant, the small change from pre to post (decreased by 0.2 points with a small effect size) may not be practically significant. Small changes from pre to post may have been due to a possible ceiling effect, as participants’ depression stigma scores were low at pre-test.
As nearly two-thirds of our sample self-identified as female, it is important to consider the potential role of sex and intersectionality in our study. Across race, the prevalence of depression among women is higher than in men from puberty into adulthood (Substance Abuse and Mental Health Services Administration, 2022). Further, there is evidence that women report more familiarity with depression (Furnham et al., 2014; Holzinger et al., 2012). These differences are also consistent among AA women when compared to AA men (Henderson et al., 2005; Williams et al., 2007). Future research might consider exploring the effect of sex differences among AA young adults as they relate to the impact of culturally tailored psychoeducational interventions and willingness to seek help for depression.
Results of this study should be interpreted in light of several limitations. First, our study did not have a control group, in which an untailored intervention would have been used for comparison to the culturally tailored intervention. This limits our results as there is no direct evidence regarding the benefit of a culturally adapted intervention. More research is needed to understand the utility of a culturally tailored intervention when compared to an untailored intervention. Further, the data are cross-sectional and represent very short-term and immediate effects following an intervention. Therefore, results presented do not represent the long-term effects of the intervention. The study sample consisted of undergraduate students at a predominately White institution. Results may not be generalizable to AA young adults at historically Black colleges and universities or to AA young adults who are not in higher education and may have additional issues such as access to mental health care. Exclusion criteria for this project, as stated on recruitment materials, required participants to have never been diagnosed or received treatment for a mental health condition. Despite this, seven participants reported having received a diagnosis for anxiety or depression. However, there were no significant differences between those with and without a personal mental health diagnosis across key variables including willingness to seek help, attitude, subjective norm, perceived behavioral control, disclosure, and stigma. Additionally, given the nature of the study, it is unclear what role social desirability may have played with regards to the results. In addition to social desirability associated with the topic of depression, social desirability bias may have also been present because participants completed the post-test survey immediately following the intervention when the researchers and presenters were present. Some social desirability bias may have been mitigated in the present study by the use of an algorithm, that participants created, rendering the surveys anonymous.
Conclusion
To our knowledge, this is the first study to use the TPB to investigate AA college students’ willingness to seek professional help for depression. A culturally relevant, theory-based, interactive psychoeducational intervention improved willingness to seek professional help for depression among AA young adults. The intervention also improved participants’ attitude toward professional help-seeking, improved their disclosure regarding professional help-seeking and decreased their depression stigma. Findings from this study suggest that depression help-seeking among young AAs is a complex behavior that may be influenced by other factors not yet identified in the literature, like disclosure. The findings from this study are preliminary. Future studies might consider including a comparison or control group to provide direct evidence of the value of this culturally adapted intervention. Those interested in improving help-seeking in this vulnerable population might consider: incorporating concepts of unloading issues, safe spaces, and knowledgeable providers; emphasizing the non-addictive role of medications; including parents or adult guardians; and personifying professional help through engaging interactions with mental health professionals. In order to address and potentially reduce disparities in mental health treatment, more research is needed to further understand how these issues and willingness to seek help relate to actual help-seeking behavior among young AAs with mental illness.
Supplemental Material
sj-docx-1-tps-10.1177_13634615241253167 - Supplemental material for Impact of a psychoeducational intervention on willingness to seek help for depression among African American young adults
Supplemental material, sj-docx-1-tps-10.1177_13634615241253167 for Impact of a psychoeducational intervention on willingness to seek help for depression among African American young adults by Benita A. Bamgbade, Jamie C. Barner, Carolyn M. Brown, Kentya H. Ford, William B. Lawson and Kimberly Burdine in Transcultural Psychiatry
Footnotes
Acknowledgements
The authors would like to thank the Eta Theta Chapter of Omega Psi Phi Fraternity, Inc., the Epsilon Iota Chapter of Alpha Phi Alpha Fraternity, Inc., Chib Amuneke-Nze, Dr. Angelica Morris, Fiona Imarhia, Yi Liang, Sabina Nduaguba, Kemi Ibrahim, Serene Zhang, Sanket Shah, Chisom Chima-Kanu, and Dr. Tolani Ogunsanya for all of their efforts in making this project a reality.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Hogg Foundation for Mental Health through the Harry E. and Bernice M. Moore Fellowship for Doctoral Research and by grant K01HL155236 from the National Heart, Lung, and Blood Institute.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.