
Abstract
The COVID-19 pandemic exacerbated the challenging working conditions of healthcare workers (HCWs) in many regions. A considerable proportion of HCWs in Germany are migrants facing additional migration-related stressors. The aim of this cross-sectional web-based survey was to examine depressive and generalized anxiety symptoms among migrant and native HCWs in Germany during the pandemic. We compared 780 migrant (first- and second-generation) HCWs from different backgrounds with 6,407 native HCWs. Multiple linear regression analyses were used to examine associations between occupational and COVID-19 related variables, controlling for sociodemographics. Migrant HCWs from low-/middle-income countries more frequently had clinically relevant depressive symptoms (PHQ-2 ≥ 3) than did those from high-income countries (29.9% vs. 16.7%, p = .002, ϕ = .156) (all other ϕs/Cramer's Vs ≤ .036). There were no clinically relevant differences in anxiety levels (GAD-2 ≥ 3) between native vs. migrant HCWs, native vs. the individual migrant HCW groups, or between the sexes (all ϕs/Cramer's Vs ≤ .036). After controlling for key sociodemographic characteristics, native HCWs did not differ from the individual migrant HCW groups on depression and anxiety severity (depression: all βs ≤ |.030|, anxiety: all βs ≤ |.014|). A high percentage of HCWs reported distress, with migrants from low-/middle-income countries reporting highest burden. The results indicate the need to establish prevention programmes for HCWs, with special consideration to vulnerable populations including certain migrant groups.
Introduction
In recent decades, there has been a shortage of skilled workers in the German healthcare system. The changing demography of German society—with low birth rates and an aging population (Kovacheva & Grewe, 2015; Oltmer, 2016)—suggests that this shortage will worsen in the future (Braeseke & Bonin, 2016; Kovacheva & Grewe, 2015). This condition has prompted government institutions in Germany to actively recruit healthcare workers (HCWs) from abroad (Kovacheva & Grewe, 2015) and to enter into cooperation agreements with countries within Europe (such as Greece, Spain, Bulgaria, Romania, and the Baltic states; Braeseke & Bonin, 2016; Gkolfinopoulos, 2016) as well as worldwide (Braeseke & Bonin, 2016). Further, refugee movement to Europe from 2014 to 2016 (Grote, 2018) and in 2022 (Spiegel, 2022) was recorded as a reason for migration to Germany. Due to increased migration to Europe in recent years, more and more foreign-born physicians, nurses, and other HCWs have settled in Germany (Garcia-Perez et al., 2007; Larsen et al., 2005). Within the last 26 years, an upward trend in the number of foreign-born physicians working in Germany was observed, rising from 10,651 in 1995 to 57,200 in 2021 (Statista, 2022). According to the definition of the German census, individuals born in another country than Germany and who do not obtain German citizenship by birth are regarded as first-generation migrants. These can be distinguished from second-generation migrants who were born in Germany and obtain German citizenship by birth, while this is not the case for at least one of their parents (Destatis, 2020).
Due to the above-mentioned shortage of HCWs, it is essential to retain them in their profession. For this reason, it is of great importance to investigate possible reasons for absenteeism, attrition, as well as potential underlying psychological complaints of HCWs. The working conditions of HCWs are considered to be particularly stressful, for example due to a lack of personnel (Adriaenssens et al., 2015; Schilgen et al., 2019). This problem was exacerbated by the COVID-19 pandemic, resulting in altered work tasks (Alderwick et al., 2020; Williams et al., 2020) which caused increased workload and longer working hours (Weilenmann et al., 2021), highlighting low staffing coverage. Increased workload in combination with lacking staff may pose a risk to mental health. A number of studies have already addressed the psychological disadvantages HCWs were exposed to during the COVID-19 pandemic, revealing prevalence rates of 12 to 50% for depression and 13 to 44% for generalized anxiety symptoms (Li et al., 2021; Pappa et al., 2020; Shaukat et al., 2020; Shechter et al., 2020; Weilenmann et al., 2021).
Compared to native Germans, migrant workers in general are confronted with additional post-migration difficulties at work such as language barriers (Heponiemi et al., 2018) or discrimination and prejudices (Schilgen et al., 2020), which makes them a particularly vulnerable population group. Migrant workers are known to suffer more frequently from mental health problems (Arici et al., 2019; Brydsten et al., 2019; Campbell et al., 2018; Claassen & Broding, 2019) and are often employed under worse working conditions than the native population (Arici et al., 2019; Brydsten et al., 2019). Because of these disadvantages in the workforce, it is of great importance to pay special attention to migrants in the examination of mental health in the workforce.
Migrant healthcare workers in Germany originate from many different regions, representing countries with diverse cultural and socioeconomic backgrounds. The World Bank has developped a country classification system based on the Gross National Income per capita of each country. According to this ranking, countries all over the world can be divided into low- (US$1,085 or less), lower middle- (US$2,086–4,255), upper middle- (US$4,256–13,205), and high-income countries (US$13,206 or more) (World Bank, 2022b).
A similar socioeconomic status of the country of origin to the host country could be beneficial for acculturation. In such cases, the educational level, living standard, mentality, and possibly culture of the country of origin might align with those of the host country, leading to fewer adaptations needed in the acculturation process. This, in turn, could help prevent the manifestation of mental disorders among migrants from these societies (Lindstrom et al., 2001; Morawa & Erim, 2014b; Nestmann & Niepel, 1993). Furthermore, pre-migratory stressors of first-generation migrants such as traumatic experiences of persecution, war, or violence are likely to have an impact on the salience of mental problems (Chen et al., 2020), especially among migrants from low-income countries such as Afghanistan, Ethiopia, and the Syrian Arab Republic (World Bank, 2022a). Indeed, migrants from these countries are more likely to be refugees than those from higher-income countries (Statista, 2021). Consequently, HCWs from low-income countries may be more psychologically distressed than HCWs from high-income countries. Therefore, when investigating the mental health of first-generation migrant HCWs, their country of birth should be taken into account. This consideration should thus encompass the socioeconomic status of their home country.
However, first- and second-generation migrant HCWs might suffer from mental health issues to varying degrees. As already described, first-generation migrants directly experience pre- and post-migratory stressors that second-generation migrants do not experience to the same extent or at all. In addition, second-generation migrants have grown up in the host culture and are therefore very familiar with it, which may account for lower acculturation efforts. For these reasons, it could be assumed that second-generation migrant HCWs might be less mentally burdened than those of the first-migration generation (Hirschman, 1996).
When considering the mental health of HCWs during the COVID-19 pandemic, women in general appear to be particularly at risk in terms of anxiety (Huang et al., 2020; Lai et al., 2020), depression, distress (Lai et al., 2020), and posttraumatic stress (Huang et al., 2020). This also applies to female migrants, regardless of occupation (Bogic et al., 2015; Morawa & Erim, 2014a). Therefore, females and males should be considered separately.
In a multi-centered study, we surveyed HCWs in Germany and analyzed their mental health.
The research questions of this study included:
Do migrant and native HCWs differ in the frequency of clinically relevant depressive and anxiety symptoms? We divided migrant category as follows: second-generation migrants, first-generation migrants, first-generation migrants from low-/middle-income countries, and first-generation migrants from high-income countries. Do sex-specific differences exist in the frequency of clinically relevant depression and anxiety symptoms? Do migrant and native HCWs differ in terms of the severity of depression and generalized anxiety symptoms after controlling for important sociodemographic, occupational, and COVID-19-related variables?
Methods
Setting and population
We conducted an online survey between April 20 and July 5, 2020 as the first measurement of the prospective VOICE study, which is part of the egePan Unimed project supported by the German Federal Ministry of Education and Research (BMBF). The project supports development, testing, and implementation of regionally adaptive care structures and processes for evidence-based pandemic management coordinated by the University Medical Center. The psychosomatics departments of the university hospitals of Erlangen, Bonn, Ulm, Cologne, and Dresden in Germany shared the survey link via online platforms or mailing lists to their staff. Hospitals and various professional associations and professional online platforms promoted participation in the survey. The German survey, hosted on Unipark (www.unipark.com) and SoSci Survey (www.soscisurvey.de), consisted of 77 items and took approximately 15 min to complete. The study was approved by the Ethics Committee of the Medical Faculty of the Friedrich-Alexander University Erlangen-Nürnberg (FAU) (reference number: 133_20 B), Bonn (reference number: 125/20), Cologne (reference number: 20-1199), Dresden, and Ulm (no reference numbers because the approval was based on the other Ethics Committees) and registered on ClinicalTrials (DRKS-ID: DRKS00021268). A plot of infected, deceased, and recovered COVID-19 cases in Germany over time displaying the context of the survey can be found in a study already published (Morawa et al., 2021). Inclusion criteria were a minimum age of 18 years, working in the healthcare sector, working in Germany, and sufficient German-language competency.
A total of 8,061 HCWs participated in this online survey. Twenty subjects were excluded due to missing information on their sex and 27 subjects were excluded due to missing information on their country of origin (born in Germany or not). Furthermore, 827 participants were excluded because they had more than 20% missing responses in key mental health measures (see Section 2.2. below for a description of measures). This resulted in 7,187 subjects. However, 23 participants in this population reported being born outside Germany and thus counted as first-generation migrant HCWs but did not provide information on their country of birth.
Frequencies of the most common countries of birth of first-generation migrant HCWs among the occupational groups.
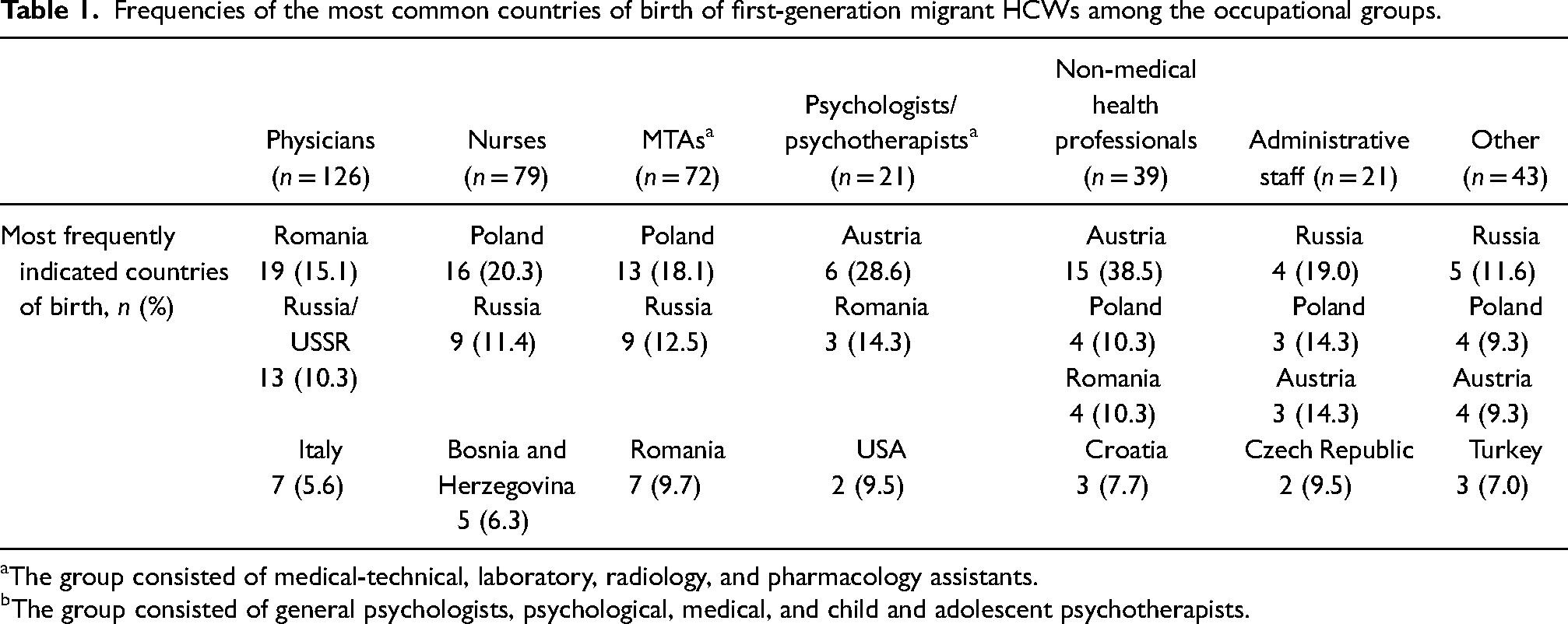
The group consisted of medical-technical, laboratory, radiology, and pharmacology assistants.
The group consisted of general psychologists, psychological, medical, and child and adolescent psychotherapists.
Measures
Sociodemographic, occupational, and COVID-19 related variables
The online questionnaire contained the following items on sociodemographic data: sex, age group (18–30, 31–40, 41–50, 51–60, >60), living situation (living alone or not), having children (yes or no), possess German citizenship by birth and of both parents (yes or no), and country of birth. Occupational information collected included profession, work setting, working in patient care (yes or no), years of professional experience in patient care, and working full or part time. The following COVID-19-related variables were assessed: having been infected with SARS-CoV-2, having direct contact at work with SARS-CoV-2 infected patients proved by a test, having direct contact with contaminated material at work, belonging to an at-risk group due to age or chronic illness, degree of occupancy of the wards, displacement of the department due to the pandemic, and presently working from home (partly, exclusively, or not).
Depression and anxiety symptoms
Depression and anxiety symptoms were assessed using the ultra-brief form (PHQ-4 (Kroenke et al., 2009)) of the German version (PHQ-D (Löwe et al., 2002)) of the Patient Health Questionnaire (PHQ (Spitzer et al., 1999)), consisting of four items. This questionnaire version can be divided into two modules: the depression module (PHQ-2) and the generalized anxiety module (GAD-2) (Kroenke et al., 2009). The sum scores of the PHQ-2 and GAD-2 range from 0 to 6. A cut-off value of ≥3 has been suggested to identify probable cases of clinically relevant levels of depressive and anxiety symptoms (Kroenke et al., 2003; Plummer et al., 2016). In the present sample, the validated German version achieved a Cronbach's alpha score of α = .75 for the PHQ-2 and α = .78 for the GAD-2.
Other measures
In addition, the survey also included information on work–family conflict, working conditions during the COVID-19 pandemic, COVID-19-related problems, effort and reward imbalance at work, post-traumatic symptoms, social support, optimism, religiosity, moral distress, quality of life, and vaccination readiness. The results of these questionnaires have already been published in more than 10 articles (e.g., Morawa et al., 2021; Schug et al., 2021a, 2021b) or will be reported in future publications.
Statistical analysis
Data analyses were performed using SPSS V.28. Descriptive statistics (absolute and relative frequencies) were computed to describe the sociodemographic, occupational, and COVID-19-related characteristics of the total sample and the subgroups. Group differences were tested with χ²-tests for categorial variables with Bonferroni-adjusted post-hoc analysis (Z-tests). The effect sizes ϕ and Cramer's V are also reported (|.1| ≤ Cramer's V/ϕ < |.3| = small, |.3| ≤ Cramer's V/ϕ < |.5| = moderate, Cramer's V/ϕ ≥ |.5| = large effect size (Lenhard & Lenhard, 2016)).
Respondents who stated that they and both their parents obtained German citizenship by birth were categorized as native German HCWs; otherwise they were classified as first-generation migrant HCWs (if country of birth was not Germany) or as second-generation migrant HCWs (if born in Germany) (Destatis, 2020). Subsequently, first-generation migrant HCWs were categorized in terms of their declared countries of origin according to the country classification by the World Bank (World Bank, 2022a). Because the present sample did not include enough migrant HCWs from countries of low (such as Afghanistan, Ethiopia, and the Syrian Arab Republic), lower-middle (such as Morocco, Philippines, and Ukraine), and upper-middle income (such as Romania, the Russian Federation, and Turkey), we combined these categories into one category titled “migrant HCWs from low-/middle-income countries” and contrasted them with the category called “migrant HCWs from high-income countries” (such as Austria, the United Kingdom, and the United States) (World Bank, 2022a). Migrant HCWs group differences in terms of clinically relevant depression and generalized anxiety symptoms were calculated using χ²-tests using three analyses in each case. First, native HCWs were compared with the whole group of migrant HCWs (first and second generation together), followed by calculations in which native, first-generation migrant, and second-generation migrant HCWs were compared. Ultimately, native HCWs, first-generation migrant HCWs from low-/middle income countries, and first-generation migrant HCWs from high-income countries were compared. This served the purpose of being able to capture particularly vulnerable populations within the group of migrant HCWs depending on their countries of origin and migration history. Furthermore, overall sex differences in terms of clinically relevant depression and generalized anxiety symptoms were examined using χ²-tests. Non-binary respondents (0.2%, n = 16) were excluded from all sex comparisons due to low case numbers. Because of the small group sizes and the resulting lack of power, no analyses were conducted on sex differences within the individual migrant groups.
Multiple linear regression analyses were performed to examine whether second-generation migrant HCWs, first-generation migrant HCWs from low-/middle income countries, and first-generation migrant HCWs from high-income countries differed from native HCWs in terms of the severity of depression and generalized anxiety after adjusting for key sociodemographic, occupational, and COVID-19-related characteristics. Taking into account the standardized β-value, only significant and clinically relevant predictors are reported (β ≥ .1) (Cohen, 1988).
Alpha error level of p < .05 (two-tailed) was used for testing significance except for the case of alpha error correction according to Bonferroni.
Results
Response rates
Due to a heterogeneous recruitment strategy, no response rate could be calculated for the total population. Response rates can only be reported for physicians, nurses, and medical-technical assistants (MTAs) of four university hospitals. The highest response rate was among MTAs (24.5%), followed by physicians (10.0%) and nurses (8.9%) (Morawa et al., 2021).
Sociodemographic and occupational data
Absolute and relative frequencies on key demographics can be found in Supplementary File 1. The group of native German HCWs comprised 89.1% (n = 6,407) of all respondents; 10.9% (n = 780) were categorized as migrant HCWs. The subgroup of first-generation migrant HCWs consisted of 5.6% (n = 401) of the total sample and 5.3% (n = 379) belonged to the group of second-generation migrant HCWs. Accordingly, the first-generation migrant HCWs represented 51.4% of the migrant sample, and second-generation migrant HCWs 48.6%. More than one third (39.2%; n = 157) of first-generation migrant HCWs descended from low- or middle-income countries, more than a half (55.1%; n = 221) from high-income countries, and 5.7% (n = 23) did not specify their country of birth. The most frequently mentioned low-/middle-income birth countries of first-generation migrant HCWs were the Russian Federation (10.5%, n = 42), Romania (9.7%, n = 39), Turkey (4.0%, n = 16), Kazakhstan (3.5%, n = 14), and Iran (2.0%, n = 8). The most frequently mentioned high-income countries of birth of first-generation migrant HCWs were Poland (11.5%, n = 46), Austria (9.0%, n = 36), Italy (2.7%, n = 11), Greece (2.5%, n = 10), and France (2.0%, n = 8).
Over three quarters (76.3%) of the subjects were female and more than half of the total sample were between 41 and 60 years of age (51.9%). The majority of subjects did not live alone (78.2%) and more than half of the respondents (56.1%) reported having children.
Physicians were the most often represented profession (25.3%), followed by MTAs (22.5%) and nurses (17.4%). The distribution of the countries of origin of first-generation migrant HCWs across occupational groups can be found in Table 1.
Almost two thirds (63.5%) performed their work in a hospital setting. Nearly two thirds of the subjects reported professional experience in patient care of more than six years (63.9%) (Supplementary File 1).
COVID-19-related variables
Absolute and relative frequencies on COVID-19-related variables can be found in Table 2.
COVID-19-related characteristics of the study sample.
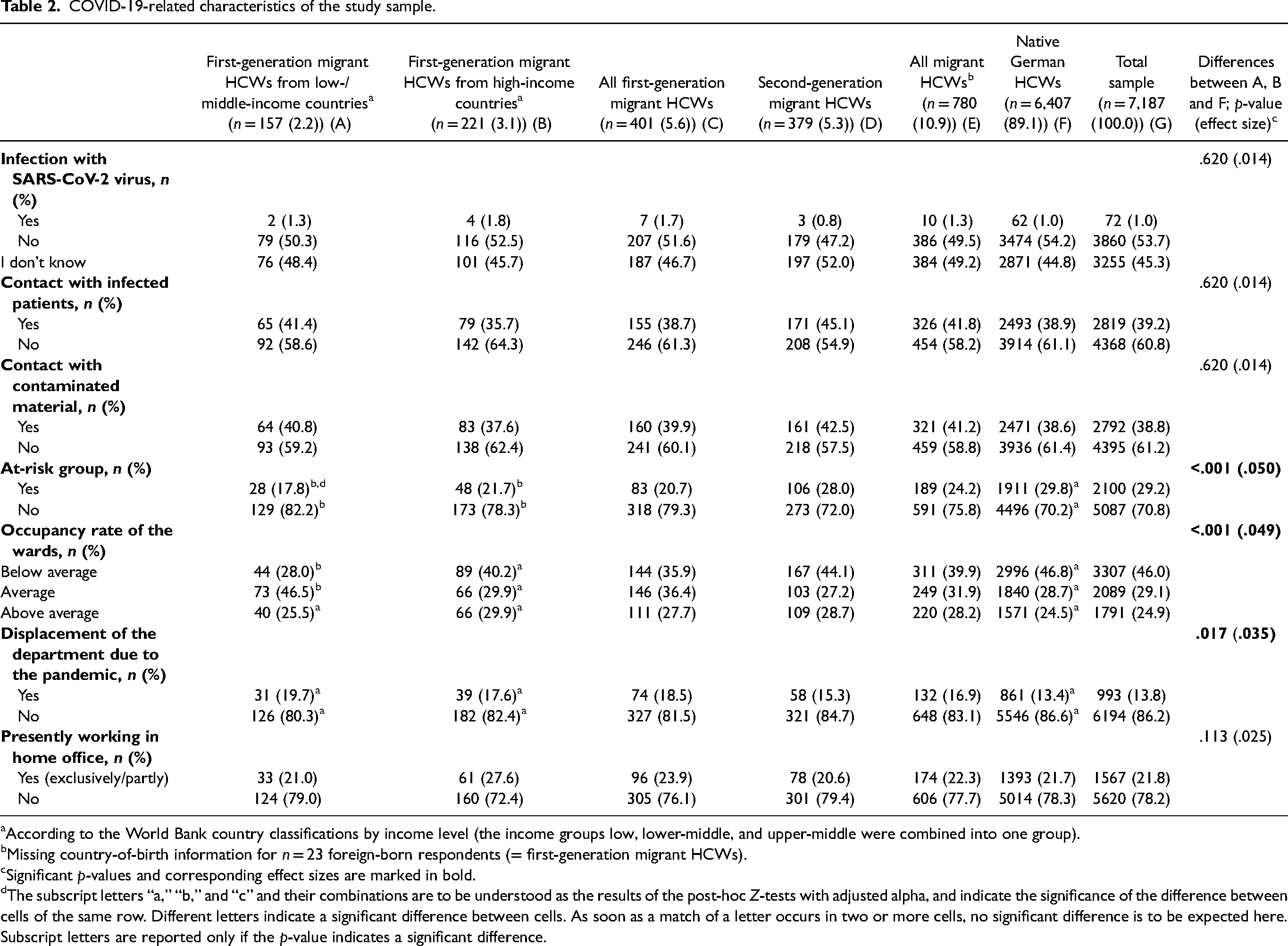
According to the World Bank country classifications by income level (the income groups low, lower-middle, and upper-middle were combined into one group).
Missing country-of-birth information for n = 23 foreign-born respondents (= first-generation migrant HCWs).
Significant p-values and corresponding effect sizes are marked in bold.
The subscript letters “a,” “b,” and “c” and their combinations are to be understood as the results of the post-hoc Z-tests with adjusted alpha, and indicate the significance of the difference between cells of the same row. Different letters indicate a significant difference between cells. As soon as a match of a letter occurs in two or more cells, no significant difference is to be expected here. Subscript letters are reported only if the p-value indicates a significant difference.
Only 1.0% of subjects reported having been previously infected with SARS-CoV-2, although nearly 40% reported having direct contact with infected patients (39.2%) or contaminated material at work (38.8%). Almost 30% (29.2%) of all respondents identified as belonging to the at-risk group due to age or chronic illness. Almost one quarter (24.9%) of the total sample perceived the occupancy rate of the wards as slightly or strongly above average.
Clinically relevant depressive symptoms
The overall frequency of clinically relevant levels of depressive symptoms was 20.6% (n = 1,477) of the total sample. Native HCWs (20.4%, n = 1,304) and the group of all migrant HCWs (22.2%, n = 173) did not differ in the frequency of their clinically relevant depressive symptomatology (χ²(1) = 1.421, p = .233, ϕ = .014). The comparison between native HCWs, first-generation migrant HCWs (22.7%, n = 91), and second-generation migrant HCWs (21.6%, n = 82) also proved not to be significant (χ²(2) = 1.555, p = .460, Cramer's V = .015). However, native HCWs, first-generation migrant HCWs from low-/middle-income countries (29.9%, n = 47), and first-generation migrant HCWs from high-income countries (16.7%, n = 37) were significantly different from each other (χ²(2) = 10.587, p = .005, Cramer's V = .040). Post-hoc tests revealed that HCWs originating from low-/middle income countries differed significantly and meaningfully in the frequency of clinically relevant depressive symptoms from those from high-income countries (χ²(1) = 9.245, p = .002, ϕ = .156). All other post-hoc comparisons did not show any significant and meaningful effects (all other ps ≥ .003, all other ϕs ≤ .036) (Figure 1).
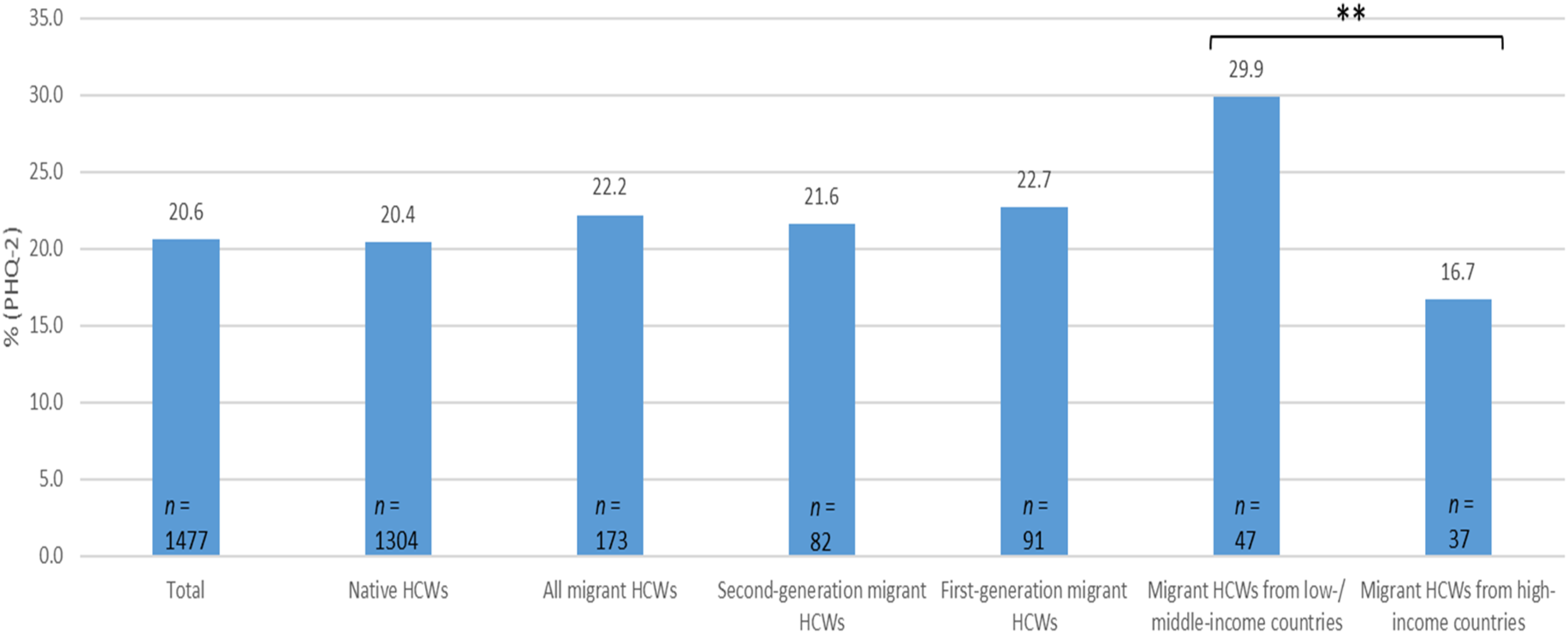
Frequencies of clinically relevant depressive symptoms (PHQ-2 ≥ 3) of HCWs of the total sample, native HCWs, second-generation migrant HCWs, all first-generation migrant HCWs, migrant HCWs from low-/middle income countries and migrant HCWs from high-income countries. **p < .01 (the corresponding effect size ϕ = .156).
Male (20.1%, n = 339) and female HCWs (20.6%, n = 1,132) did not differ significantly in terms of the frequency of their clinically relevant depressive symptoms (χ²(1) = .251, p = .617, ϕ = .006).
Clinically relevant generalized anxiety symptoms
Clinically relevant anxiety symptoms were found in 20.5% (n = 1,472) of the total sample. The group of all migrant HCWs (24.0%, n = 187) suffered significantly more frequently from generalized anxiety symptoms than native HCWs (20.1%, n = 1,285) (χ²(1) = 6.555, p = .010, ϕ = .030). However, this effect is considered negligible. Native HCWs, first-generation migrant HCWs (24.2%, n = 97), and second-generation migrant HCWs (23.7%, n = 90) differed significantly (χ²(2) = 6.578, p = .037, Cramer's V = .030), which, however, could not be demonstrated in post-hoc tests (all ps ≥ .046, all ϕs ≤ .024). Native HCWs, first-generation migrant HCWs from low-/middle-income countries (25.5%, n = 40), and first-generation migrant HCWs from high-income countries (24.0%, n = 53) did not show any significant differences (χ²(2) = 4.687, p = .096, Cramer's V = .026) (Figure 2).
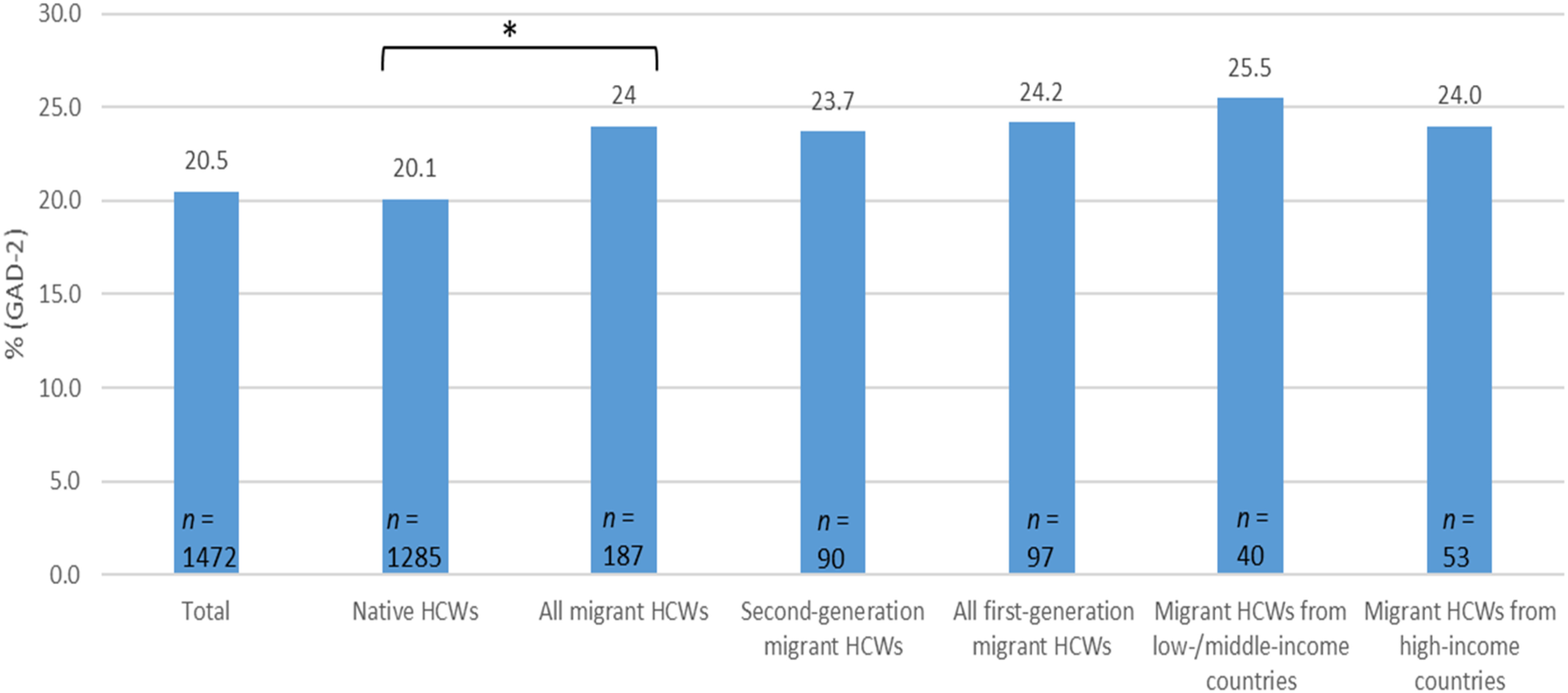
Frequencies of clinically relevant generalized anxiety symptoms (GAD-2 ≥ 3) of HCWs of the total sample, native HCWs, second-generation migrant HCWs, all first-generatin migrant HCWs, migrant HCWs from low-/middle income countries and migrant HCWs from high-income countries. *p < .05 (the corresponding effect size ϕ = .030).
Women (21.3%, n = 1,167) were significantly more likely to suffer from clinically relevant anxiety symptoms than men (17.8%, n = 301) (χ²(1) = 9.448, p = .002, ϕ = .036). However, this effect is considered negligible.
Regression analyses
In order to examine differences between native HCWs and the individual migrant HCW groups regarding the severity of depression and anxiety symptoms when controlled for important sociodemographic, occupational, and COVID-19-related characteristics, multiple linear regression analyses were performed for the entire sample (Model 1: depressive symptoms, adjusted R² = 3.7%, Model 2: generalized anxiety symptoms, adjusted R² = 3.1%) (Supplementary File 2). Both Model 1 and Model 2 showed that neither HCWs of the second migration generation nor the individual first-generation migrant groups (HCWs from low-/middle income countries and from high-income countries) differed from native HCWs in the severity of either depression or generalized anxiety symptoms after controlling for important key factors. No significant and meaningful protective or risk factors could be found for depression. Being in the at-risk group due to a pre-existing ilness was considered a significant as well as meaningful risk factor for anxiety (p < .001, β = .119). For a more detailed examination of risk and protective factors, see already published works of the VOICE survey (Morawa et al., 2021; Schmuck et al., 2021; Schug et al., 2021b).
Discussion
The aim of the present study was to determine whether migrant and native HCWs differ in the frequency of clinically relevant depressive and anxiety symptoms with consideration of the socioeconomic status of the country of origin and migration history. In addition, sex-specific differences among these variables of interest were assessed. Further, we examined whether individual migrant HCW groups differed from native HCWs after adjusting for important key factors. No differences were found between migrant and native HCWs in either anxiety or depression symptoms, even after controlling for important key variables. However, first-generation migrant HCWs from low/middle-income countries showed significantly higher depression levels than those from high-income countries. Sex differences could not be found.
Mental health among HCWs during the COVID-19 pandemic
Various studies that examined the mental health of hospital staff during the COVID-19 pandemic showed widely varying findings (clinically relevant depressive symptoms: 12 to 50%, clinically relevant anxiety: 13 to 44% (Li et al., 2021; Pappa et al., 2020; Shaukat et al., 2020; Shechter et al., 2020; Weilenmann et al., 2021). Ultimately, it appears that the present sample yielded relatively low to average levels of psychological distress (depressive symptoms: 20.6%, anxiety: 20.5%) during the pandemic compared to similar samples of HCWs.
Group differences between migrant and native HCWs
Previous studies showed that migrant workers suffer from poorer mental health than their native equivalent (Arici et al., 2019; Claassen & Broding, 2019). However, the present study could not support this finding among HCWs in Germany, neither for depression nor for anxiety symptoms, even after controlling for important sociodemographic, occupational, and COVID-19-related variables. This might be attributed to the fact that the participants who were examined included HCWs with a strong willingness to participate in the study alongside their regular work responsibilities. Our study may thus have mainly selected those HCWs who were already well integrated and acculturated, and thus experienced less distress than those who did not participate. The migrant HCWs examined in this study might thus not reflect all migrant HCWs in terms of their psychological distress.
However, first-generation migrant HCWs from low-/middle-income countries did show higher prevalence rates of clinically relevant depression than first-generation migrant HCWs from high-income countries. This group also showed the highest rates of anxiety symptoms. One possible explanation for a higher mental health burden on migrant HCWs from low-/middle-income countries could be linked to the associated stressors of forced migration due to persecution, war, or violence. These may have accounted for more harmful and traumatic pre-migratory experiences (Chen et al., 2020) than migrants from high-income countries have experienced. In addition, the asylum process has been shown to have a potential negative impact on mental health (Laban et al., 2004). Furthermore, migrants from high-income countries originate from societies that are more similar to Germany in terms of social, economic, medical, cultural, as well as political structures than migrants from low-/middle-income countries. Thus, migrants from high-income countries might be more familiar with processes in a country like Germany and therefore experience less acculturation stress and associated mental burden (Lindstrom et al., 2001; Morawa & Erim, 2014b). This is confirmed by studies comparing the mental health of general migrants with that of refugees. Refugees seem to be particularly at risk with regard to their mental health (Lindert et al., 2008).
Sex differences
While within the group of HCWs, some studies showed that women are more mentally distressed than men (Bohlken et al., 2020; Shaukat et al., 2020; Spoorthy et al., 2020), this pattern was not evident in the present sample. In regression analyses, sex was also not found to be a meaningful predictor. It is argued that female HCWs often suffer mental health disadvantages because they are disproportionately more likely to work as lower-ranking staff (e.g., nurses, MTAs) (Regenold & Vindrola-Padros, 2021) and thus experience lower socioeconomic status than higher-ranking staff (e.g., physicians) (Morawa et al., 2021), which may negatively impact mental health (Everson et al., 2002; Volkers et al., 2007). The present sample showed that men held 50% and women 42% of higher-ranking occupations (physicians, psychologists/psychotherapists, non-medical health professionals/pedagogues). This relatively balanced ratio of higher-ranking occupations could be responsible for similar levels of depression and generalized anxiety symptoms.
Generalizability to international conditions
Shortages of HCWs are not unique to Germany. This trend represents a global phenomenon (WHO, 2022). Countries such as the United States (Eckenwiler, 2009), Canada (Canadian Nurses Association, 2022b), the United Kingdom (NHS Digital, 2022; The King's Fund, 2018), New Zealand (Ministry of Health, 2006), and Norway (OECD/European Observatory on Health Systemas and Policies, 2021) suffer from similar shortages and have also been pursuing a strategy of recruiting trained HCWs from abroad for years (Canadian Nurses Association, 2022a; The King's Fund, 2018). Accordingly, the work-related burdens encountered by native as well as migrant HCWs in Germany may also be comparable to other Western countries, highlighting the international relevance of support for and investigation of the mental health of HCWs, especially with special consideration of migrant HCWs.
Strengths and limitations
The present study is part of a large survey on the mental health of HCWs during the first wave of the COVID-19 pandemic in Europe. To the best of our knowledge, this is the first study to examine the mental health of HCWs in Germany during a global health crisis, with special consideration given to migrant HCWs and their countries of origin. On the one hand, a similar sex and age category distribution (Statistisches Bundesamt, 2021) (Supplementary File 1), as well as the distribution of foreign-born HCWs (Bundesagentur für Arbeit, 2021; Bundesärztekammer, 2021) between the current sample and censuses of the general healthcare workforce, suggests a fairly high degree of representativeness in terms of sociodemographic characteristics of the sample. On the other hand, the rate of first-generation migrant HCWs surveyed in this study is not entirely representative of HCWs in Germany. Across Germany, the proportion of foreign-born nurses is 9% (Bundesagentur für Arbeit, 2021), while it was only 6.3% in the present study. Furthermore, more than 10% of physicians in Germany are foreign born (Ärztestellen, 2022), against 6.9% in the present sample. Although a migrant rate of almost 11% itself can be considered relatively high considering the difficulties in recruiting this particular population (Dingoyan et al., 2012), the lower migrant rate in the present occupational groups compared to the working HCW population in Germany suggests that selection bias may have occurred. Thus, migrant HCWs who participated in our study may have primarily been well-adjusted to German society and professional life, accounting for a low mental health burden. Additionally, the cross-sectional design precludes the drawing of causal conclusions regarding the measured variables. Such conclusions may be possible in further studies, as additional survey time points have already been collected in a longitudinal design. Furthermore, it must be noted that all the data collected were assessed using self-report instruments. Self-report measures should always be approached with caution due to their susceptibility to bias, stemming from factors such as social desirability or specific response tendencies of the participants (Furnham, 1982). This holds true even when the survey is conducted anonymously online. Finally, we did not control for pre-existing mental illness, nor did we recruit a control group from the general population. Another limitation is the relatively large difference in the size of the compared groups. This might have led to insufficient statistical power to detect subtle yet significant effects.
Conclusion
Although the frequencies of clinically relevant depressive and anxiety symptoms did not differ from HCWs previously studied, we found a high percentage of HCWs who report psychosocial distress. Moreover, our findings indicate that certain sub-groups of migrant HCWs, notably those originating from low-/middle-income countries, which constitute a substantial and significant segment within the healthcare professions (Garcia-Perez et al., 2007; Larsen et al., 2005; Schilgen et al., 2020), experience greater impact compared to other sub-groups (migrant HCWs from high-income countries). Due to the limitations of the study, our results should be treated with caution. The results highlight a need for action to protect the mental health of migrant HCWs in Germany and thus preserve their ability to work and prevent further worker shortages in healthcare. Future studies should include control groups and take a more in-depth look at the psychosocial distress of different migrant groups to identify the factors contributing to the heightened psychological burdens experienced by certain migrants and to provide targeted interventions for vulnerable HCWs with a migration background.
Practical implications for the healthcare system derived from this study point to the need to establish regular mental health screening and prevention programmes for HCWs, which may help deliver early and rapid support services. Here, the specific needs of HCWs with a migration background should be given special attention.
Supplemental Material
sj-docx-1-tps-10.1177_13634615241253153 - Supplemental material for The mental health of first- and second-generation migrant vs. native healthcare workers during the COVID-19 pandemic: The VOICE survey of 7,187 employees in the German healthcare sector
Supplemental material, sj-docx-1-tps-10.1177_13634615241253153 for The mental health of first- and second-generation migrant vs. native healthcare workers during the COVID-19 pandemic: The VOICE survey of 7,187 employees in the German healthcare sector by Regina Herold, Eva Morawa, Caterina Schug, Franziska Geiser, Petra Beschoner, Lucia Jerg-Bretzke, Christian Albus, Kerstin Weidner, Nina Hiebel, Andrea Borho and Yesim Erim in Transcultural Psychiatry
Supplemental Material
sj-docx-2-tps-10.1177_13634615241253153 - Supplemental material for The mental health of first- and second-generation migrant vs. native healthcare workers during the COVID-19 pandemic: The VOICE survey of 7,187 employees in the German healthcare sector
Supplemental material, sj-docx-2-tps-10.1177_13634615241253153 for The mental health of first- and second-generation migrant vs. native healthcare workers during the COVID-19 pandemic: The VOICE survey of 7,187 employees in the German healthcare sector by Regina Herold, Eva Morawa, Caterina Schug, Franziska Geiser, Petra Beschoner, Lucia Jerg-Bretzke, Christian Albus, Kerstin Weidner, Nina Hiebel, Andrea Borho and Yesim Erim in Transcultural Psychiatry
Footnotes
Acknowledgements
We thank Dr. Werner Adler for statistical support, and Frederik Wuchenauer for assistance in data visualization. We acknowledge financial support by Deutsche Forschungsgemeinschaft and Friedrich-Alexander University Erlangen-Nürnberg with the funding programme “Open Access Publication Funding.”
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data management and evaluation were performed in the collaborative research project egePan Unimed, which is financially supported by the German Federal Ministry of Education and Research (BMBF) as part of the Network University Medicine (NUM) (funding code: 01KX2021). The project is led by Prof. Dr. Michael Albrecht, Prof. Dr. Jürgen Graf, Prof. Dr. Jochen Schmitt, and Dr. Michael von Wagner. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Data analysis and manuscript preparation were financially supported as part of the project “friaa” (“Frühe Intervention am Arbeitsplatz”) by the BMBF (reference number: 01GX1902C).
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.