
Abstract
This prospective study examined the psychosocial adaptation of a community sample of newly resettled Syrian refugees in Canada (N = 235). Specifically, depressive symptoms, perceived stress, and perceived control were collected in Arabic at baseline and 1-year follow-up. Two theory-informed, cross-lagged panel models demonstrated that higher baseline depressive symptoms predicted lower perceived self-efficacy and lower perceived control at 1-year follow-up. Similarly, baseline depressive symptoms were concurrently correlated with higher perceived helplessness, lower perceived self-efficacy, and lower perceived control. Secondary regression analyses further demonstrated that baseline depressive symptoms predicted lower perceived social support and higher anxiety symptoms, though neither were assessed at baseline. Empirical results identify a potentially broad, precipitating, and persistent effect of depressive symptoms on Syrian refugees’ psychosocial resources and adaptation post-migration, which is consistent with both the transactional model of stress and coping and the self-efficacy theory of depression, respectively. Clinically, the study results highlight the importance of early screening for depressive symptoms among refugee newcomers within a culturally and trauma-informed, integrated health setting. Furthermore, this study underscores the value and need for theoretically guided longitudinal studies to advance future research on refugee mental health and psychosocial adaptation.
The United Nations Higher Commissioner for Refugees (UNHCR, 2022) recently reported that in 2020 there were an estimated 82.4 million displaced persons globally, of whom 26.4 million were refugees. Among refugees, depressive disorders have been found to be highly prevalent and severe, particularly among those who are affected by wars and conflicts (Blackmore et al., 2020; Peconga & Thøgersen, 2020). Evidence consistently identifies risk for both acute and chronic stress among displaced persons due to premigration trauma and ongoing post-migration stressors (e.g., barriers) after resettlement in host countries (Porter & Haslam, 2005; Turrini et al., 2017). Even though refugees have been found to be highly resilient (Boucher & Kuo, 2020; Yaylaci, 2018), there is growing concern over refugee distress and trauma as the number of displaced persons and asylum seekers grows worldwide because of widespread conflicts including those in Syria, Afghanistan, and Ukraine. For instance, at the individual level, multiple barriers have been identified that hinder refugees’ access to mental health services, including communication/language difficulties, lack of trust, confidentiality concerns, shame, and limited mental health literacy (Hynie et al., 2023).
Despite these psychological and logistic challenges faced by many refugees, the UNHCR's (2019a) recent sustainable development goals call for refugee-receiving countries to take a step further by seeking means to include refugees in the social and economic development of the resettled nation. As follows, empirical knowledge about the adaptation trajectory of resettled refugees in their host society over time is sorely needed in the existing refugee mental health literature (Borho et al., 2020; M’zah et al., 2019). Against this backdrop, the purpose of this study was to expand the current, emerging research on Syrian refugees by exploring and testing depression and its temporal effects on stress, perceived control, social support, and anxiety longitudinally in a sample of recently resettled Syrian refugees in Canada. The evidence generated from this prospective research will shed critical light on our currently, limited knowledge about the lingering effects of psychological conditions, such as depression, on the long-term mental health and adaptation of displaced refugees. In turn, such knowledge can be translated to better inform services and support provided by the host country for refugees at and beyond the initial point of resettlement.
Syrian refugee mental health and adaptation
The mass displacement of Syrian refugees from their home country, due to the protracted Syrian conflict that started in 2011 has resulted in an estimated 6.7 million displaced Syrian refugees around the world (Hassan et al., 2015; UNHCR, 2019b). Incidentally, depressive, anxiety, and post-traumatic stress disorders (PTSD) have been identified as the most prevalent psychiatric conditions experienced by displaced Syrian refugees in Lebanon (Naal et al., 2021), Germany (Borho et al., 2020), and the USA (Javanbakht et al., 2019). Specifically, a recent review of research on resettled Syrian refugees across 10 countries reported average prevalence rates of 40.9% for depressive disorders, 26.6% for anxiety disorders, and 43% for PTSD (Peconga & Thøgersen, 2020). However, scholars have observed a number of persistent conceptual and methodological gaps in the extant mental health literature concerning refugees and asylum seekers (Yaylaci, 2018). These include the need for research that: (a) extends beyond the heavy focus on trauma or PTSD, to study other prevalent psychiatric and psychological conditions, such as depressive and anxiety symptoms in refugee communities (Barkil-Oteo et al., 2018; Turrini et al., 2017); (b) identifies biopsychosocial factors that may impact refugee mental health and psychosocial adaptation (Porter & Haslam, 2005; Wells et al., 2016; Yaylaci, 2018; and (c) tracks or examines changes in refugees’ mental health and adaptation longitudinally (Borho et al., 2020; Euteneuer & Schäfer, 2018; M’zah et al., 2019). On this last point, the current authors could identify only two published studies that investigated mental distresses and disorders among Syrian refugees with a longitudinal design (Ahmad et al., 2021; Borho et al., 2020). Specifically, no published study to date has employed a longitudinal design to investigate change in the severity and the precipitation impacts of depressive disorders on theoretically driven psychosocial factors related to stress, control, and social support in resettled Syrian refugees. Accordingly, the current study intends to address this critical gap.
Theoretical perspectives on perceived stress and perceived control in refugee mental health
The transactional model of stress and coping by Lazarus and Folkman (1984) posits that distress, including depressive disorders, may be a consequence of complex person–environment interactions involving an individual’s life stressor(s), appraisal/perception of the stressor, resources to respond, and coping capacity (Lazarus & Folkman, 1984, 1987). Accordingly, this theoretical framework implicates the pivotal roles of an individual's stress appraisal and resource/control in shaping their psychological outcome, functioning, and coping response. In a seminal review, Kessler (1997) further identified robust evidence pointing to the association between cumulative stress and depressive symptoms based on both experimental and clinical studies. Kessler (1997) observed and postulated that the strength of the perceived stress–depression link is attenuated by multiple psychosocial factors, including personality dispositions, appraisal processes, intellectual/cognitive resources, coping, social competence, social support, among others. In support, numerous studies suggest that, among individuals affected by a depressive disorder, perceived stress may impact subsequent coping resources (e.g., social support), distress experiences (e.g., anxiety), and psychological well-being (e.g., self-esteem), in both clinical and non-clinical samples (Bovier et al., 2004; Li et al., 2016; Moradi & Risco, 2006).
Depression and perceived stress
In Kessler's (1997) seminal review, he further hypothesized a reciprocal relationship between depression and the stress-coping process, in which the individual’s depression severity can, in turn, impact and shape their subsequent stress responses and adaptation. This interactive relationship between depression and stress was further expounded by the self-efficacy theory of depression (Maddux & Meier, 1995), which evolved from Bandura's original social cognitive theory of depression (Bandura, 1992). The self-efficacy theory predicts that depression (as a mood state) can hinder individuals’ self-efficacy by undermining their cognitive and behavioral effectiveness and goal attainment. Moreover, the theory dictates that depression is often associated with either an individual’s low self-efficacy (one does not have the ability to perform the behavior/action required to achieve a goal) or low outcome expectancy (one's behavior will not affect the ultimate outcome; Stanley & Maddux, 1986). As Maddux and colleagues noted, the elements of these cognitive expectancies predispose individuals to their sense of helplessness, controllability, and behavior–consequence contingency, all of which can feed into and/or be maintained by depression symptoms (Maddux & Meier, 1995; Stanley & Maddux, 1986). Despite the foregoing evidence, empirical research on the depression → stress appraisal → coping pathway/process, with depression acting as an antecedent and precipitating variable in the stress-coping and adaptation processes, remains scanty and profoundly understudied in both the extant depression literature and the refugee trauma and mental health literature (LeMaster et al., 2018).
Depression and perceived control
The construct of perceived control, which is characterized by an individual’s appraisal of personal resources, mastery, and agency in a time of stress, has also been shown to mediate the stress–depression relationship in previous research (Bovier et al., 2004; Ghorbani et al., 2008). As with perceived stress, the self-efficacy theory of depression stipulates the critical role of controllability or lack thereof (i.e., helplessness) in predicting and/or perpetuating depression (Maddux & Meier, 1995). In two separate studies, Moradi and colleagues examined the mediating effects of perceived control between discrimination-based stressors and mental health in samples of Arabic Americans (Moradi & Hasan, 2004) and Latinx Americans (Moradi & Risco, 2006), respectively. The results of path analyses from both studies consistently revealed that perceived control partially mediated the effect of discrimination on psychological distress for both cultural groups. In addition, Bovier et al. (2004) found stress and personal control, measured by internal resources (perceived mastery and self-esteem), to be the strongest correlates of mental health indicators among university students in Switzerland. In the same sample, social support was also shown to be a positive intervening variable, which diminished the contribution of perceived stress and strengthened the contribution of personal control. Importantly, the current research sought to specifically examine the association between Syrian refugees’ perceived control and depression. The findings will enhance our current strength-based understanding of refugees by assessing the role of personal agency and control in their resettlement and adaptation process (Hassan et al., 2015; Kuo et al., 2020a).
The current study
Informed conceptually by the transactional model of stress and coping (Lazarus & Folkman, 1984), the self-efficacy theory of depression (Maddux & Meier, 1995), and empirically by relevant research on the depression–stress–resilience of culturally diverse populations (Ghorbani et al., 2008; Moradi & Risco, 2006) and resettled refugees (LeMaster et al., 2018) reviewed above, the current research intends to leverage a longitudinal design to explore and examine depression and its temporal effects on the perception of stress (helplessness and self-efficacy), perception of control, social support, and anxiety among Syrian refugees in Canada. As such, this prospective study proposed to explore the following two principal research questions. Specifically, “To what extent do Syrian refugees’ baseline depressive symptoms correlate with (a) baseline perceived stress (i.e., helplessness and low self-esteem) or (b) control”, and “To what extent do Syrian refugees’ baseline depressive symptoms predict (a) perceived stress or (b) control at one-year follow-up?” (Figures 1 and 2). Furthermore, secondary analyses were conducted to examine whether Syrian refugees’ baseline depressive symptom severity would also predict anxiety symptoms or the perceived availability of social support at 1-year follow-up.
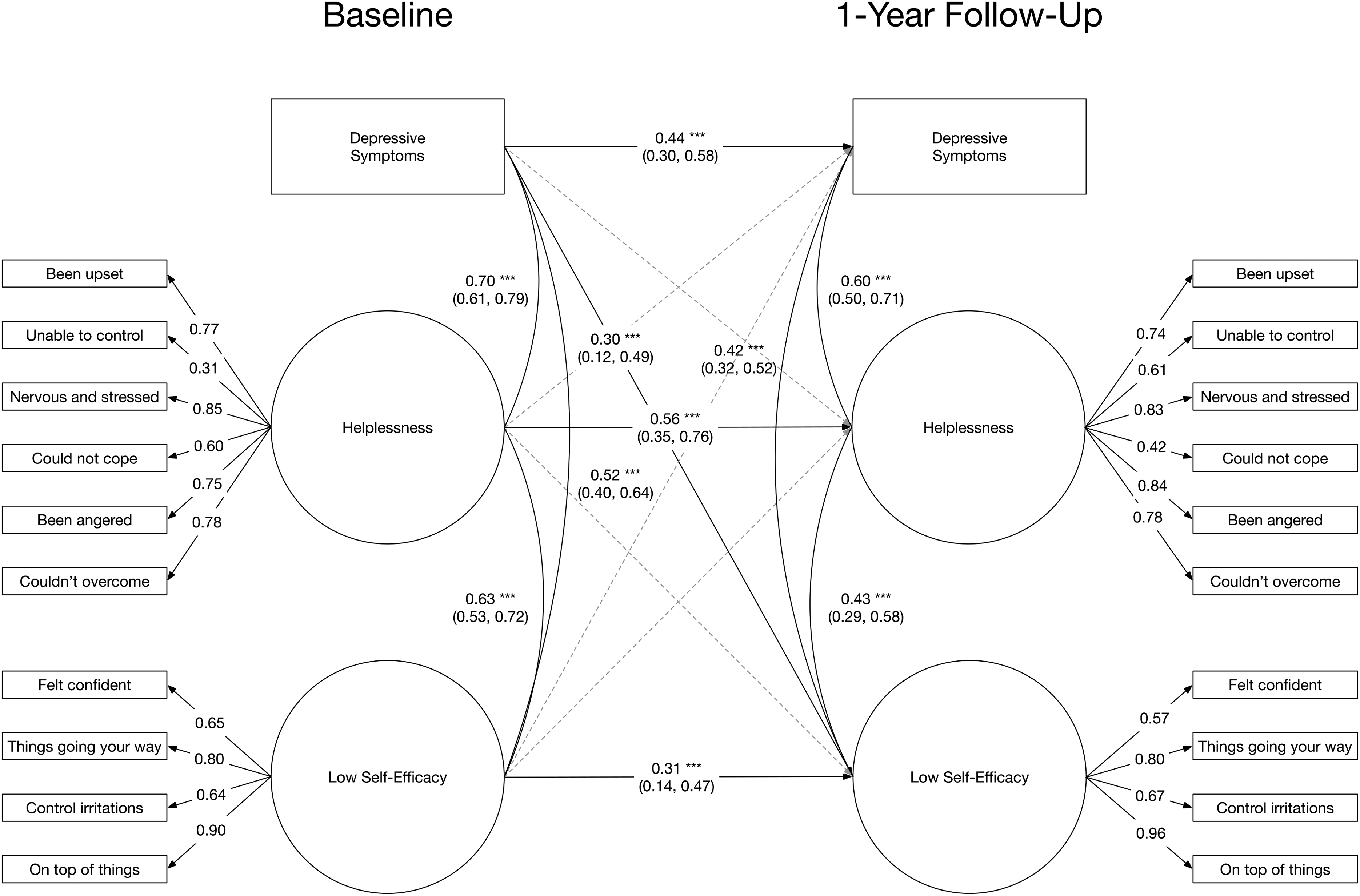
Prospective association of perceived helplessness and self-efficacy with depressive symptom severity from baseline to 1-year follow-up assessment. Estimates reflect standardized regression or correlation estimates. *p < .05, **p < .01, ***p < .001.
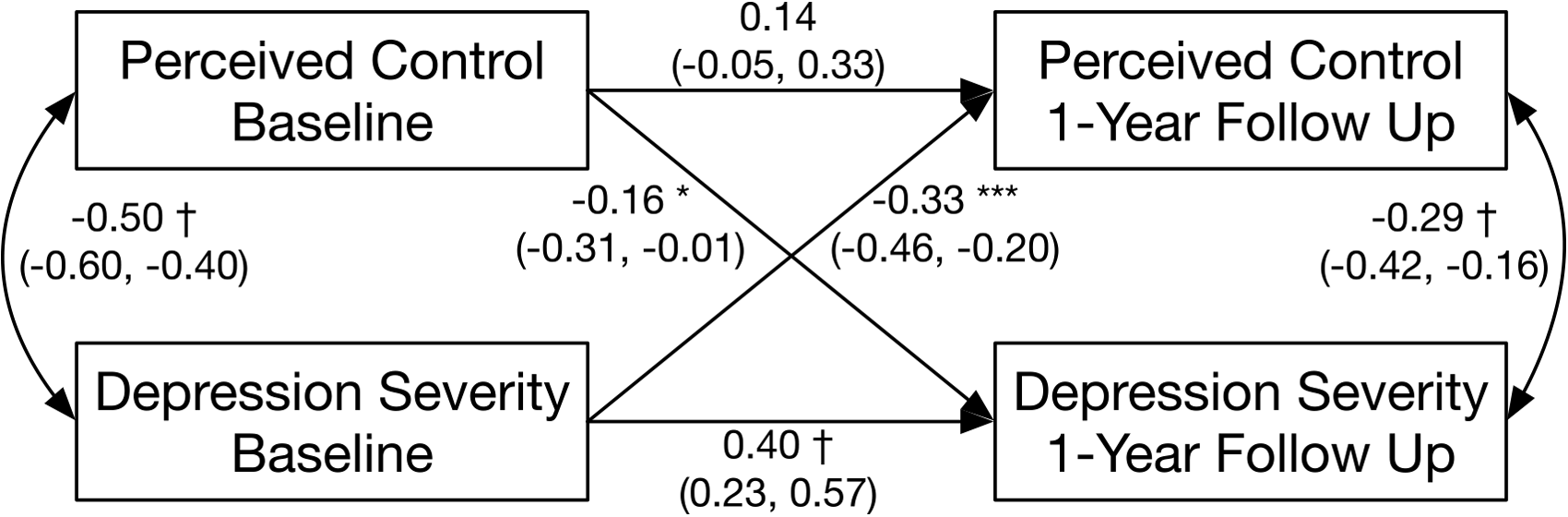
Prospective association of perceived control and depressive symptom severity from baseline to 1-year follow-up assessment. Estimates reflect standardized regression or correlation estimates. * p < .05, **p < .01, ***p < .001, †p < .0001. Model is adjusted for participant age, gender, and marital status.
Method
Participants/sample characteristics
The sample was part of the Canadian Government's 2016 initiative “#WelcomeRefugee,” implemented to resettle 40,081 Syrian refugees between November 2015 and January 2017 across 350 communities in Canada (Government of Canada, 2019). The city of Windsor, Ontario, where this study was undertaken, represents one of the originally designated hubs for hosting newly arrived Syrian refugees in Ontario. Between 4 November 2015 and 31 December 2016, the City of Windsor (2019) reported having resettled an estimated 1,389 Syrian newcomers. Participants in this study were recruited from this population.
The current Syrian refugee sample in Windsor was recruited within a larger, national, grant-funded, multiyear parent study designed to track and examine the post-migration integration and long-term health conditions in Syrian refugees resettled across six major cities in Canada (Hanley et al., 2018). The current study is distinguished from the parent project by its exclusive focus on selected psychosocial variables and the corresponding data collected from Syrian refugees in the Windsor during wave 1 (year 1 data in 2017) and wave 2 (year 2 data in 2018) of this longitudinal project. In total, 235 Syrian refugees (male = 49.4%; female = 50.6%) with a mean age of 36.6 (SD = 11.85) took part in this study in Windsor. Most participants reported having children (77.9%), having been in Canada for an average of 12.76 months (SD = 5.41), and having been displaced for an average of 39.22 months (SD = 21.1). In addition, 89.9% were reported to be Arab and 8.9% Kurdish; 71.1% were married; 52.3% attained elementary education, 21.3% high school education, and 20.4% university/college/trade certificate. This sample information was reported in a previously published study by Kuo et al. (2020b), which examined the social determinants/predictors of mental health and physical health outcomes based solely on the baseline data of the same Syrian refugee sample.
Procedures
This study received ethics clearance from both the Review Ethics Board of the University of Windsor, where this study took place, and from the Office of Research Ethics of York University, where the overall project was centrally administered. Multiple community-focused recruitment strategies were employed to reach prospective Syrian participants. First, participant recruitment was supported and facilitated by a local refugee–immigrant settlement agency, the Multicultural Council of Windsor-Essex, which had direct contact with Syrian refugees being resettled in Windsor. In addition, public announcements and advertisements of the study were posted in community agencies, at Syrian community events, and on Facebook. Lastly, snowball sampling was employed (Hanley et al., 2018). A maximum cap of up to six participants per household was implemented in collecting the data, to help maximize the sample size while ensuring that the sample reflects Syrian participants with diverse family and background characteristics (Ahmad et al., 2021). Arabic–English-speaking research assistants were recruited from the six cities involved in the parent project. As a group, the research assistants received a full-day’s training on administering the study questionnaire and managing the data collection process. In the Windsor site, eligible Syrian participants were interviewed in their homes in Arabic by one of the two trained bilingual research assistants. Such a home-based survey data collection was adopted to ensure convenience for the refugee participants who took part in the current study, because most of them did not have transportation. Using online surveys via iPad, each research assistant walked individual Syrian participants, item-by-item, through completing the study measures. Baseline interviews were conducted from April to August 2017; follow-up interviews were conducted by the same research assistant 1 year later during the same period in 2018. An honorarium of $40 Canadian was offered to each participant to thank them for their time and effort.
Measures
Systematic steps were undertaken to ensure the cultural and linguistic appropriateness of all the measures used in this study. First, in selecting each scale, measures with validated Arabic versions were given priority. Second, for other measures and questions that originated in English, an English–Arabic back-translation procedure was conducted by two bilingual Syrian Canadians to confirm accuracy. Third, a pilot study was conducted with 24 Syrian refugees to ensure the linguistic appropriateness of the entire survey. The study's demographic items included participants’ date of birth, educational level, marital status, gender, and English proficiency level. Additional questions adopted from the General Social Survey (Statistics Canada, 2010) and the Social Integration Inventory (Hynie, 2014) were used to gather information pertaining to refugee participants’ post-migration, contextual factors. Among the measures involved in the current study, the Patient Health Questionnaire-9 (PHQ-9), the Perceived Stress Scale (PSS), and the Perceived Control Scale (PCS) have existing Arabic-translated versions, and hence they were adopted in the study.
The Patient Health Questionnarie-9
The PHQ-9 is a nine-item, multipurpose scale designed to screen, diagnose, monitor, and assess frequency of depressive symptoms rated from 0 (not at all) to 4 (nearly every day; Kroenke et al., 2001). The measure was developed based on the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) diagnostic criteria for a major depressive episode; it asks participants to report symptoms experienced over the past 2 weeks. A score >20 marks the potential presence of a major depressive episode. The PHQ-9 has been effectively used and shown robust psychometric properties in previous samples of Syrian refugees in Lebanon (Naal et al., 2021) and Germany (Borho et al., 2020). In the current study, the PHQ-9 showed strong internal consistency at baseline (polychoric α = 0.91, polychoric ωhierarchical = 0.87) and follow-up assessment (polychoric α = 0.92, polychoric ωhierarchical = 0.88).
Perceived Stress Scale
The PSS assesses respondents’ perceptions of their stress over the past month and the items are rated from 1 (never) to 5 (very often). The original version of the scale (Cohen et al., 1983) has 14 items, but the Arabic version of the PSS adopted in this study has 10 items (Almadi et al., 2012). Consistent with previous psychometric evaluations of the PSS (Barbosa-Leiker et al., 2013; Leung et al., 2010; Roberti et al., 2006; Taylor, 2015), confirmatory factor analytic models indicated that one latent factor may be insufficient to capture the latent structure of constructs assessed by the PSS items at both baseline [χ2(35) = 238.69, p < .0001, root mean square error of approximation (RMSEA) = 0.16, 95% confidence intervals (95% CI; 0.14, 0.18), comparative fit index (CFI) = 0.88] and follow-up assessment [χ2(35) = 353.06, p < .0001, RMSEA = 0.20, 95% CI (0.18, 0.22), CFI = 0.81]. Instead, two latent factors indicative of helplessness and low self-efficacy to manage perceived stress evidenced adequate fit to the data at both baseline [χ2(34) = 94.05, p < .0001, RMSEA = 0.09, 95% CI (0.07, 0.11), CFI = 0.96] and follow-up assessment [χ2 (34) = 50.52, p = .034, RMSEA = 0.05, 95% CI (0.01, 0.07), CFI = 0.99]. Furthermore, in line with previous research (Taylor, 2015), the current data are most consistent with a model in which the two factors are correlated at both baseline [r = 0.63, 95% CI (0.53, 0.73), p < .001] and follow-up assessment [r = 0.47, 95% CI (0.35, 0.60), p < .001].
Perceived Control Scale
The PCS measures individuals’ sense of agency and control over several domains (e.g., at home, life situations, self-improvement, health, etc.) on nine items rated from 1 (strongly disagree) to 5 (strongly agree) (Bobak et al., 2000). Two items pertaining to heart attack and cancer risk were excluded from this project as being of less relevance for Syrian participants. The scale was developed with cross-cultural samples involving seven eastern European countries and has been strongly associated with respondents’ self-rated health (Bobak et al., 2000). Ahmad et al. (2021) report acceptable psychometric properties for use (α = 0.63) with Syrian refugees in Canada. In this study, the PCS showed similar, adequate internal consistency at baseline (polychoric α = 0.65, polychoric ωhierarchical = 0.61) and at 1-year follow-up assessment (polychoric α = 0.63, polychoric ωhierarchical = 0.67).
Multidimensional Scale of Perceived Social Support
The 12-item Multidimensional Scale of Perceived Social Support (MSPSS; Zimet et al., 1988) was designed to assess respondents’ perception of interpersonal support and resources from family, friends, and significant others. Specifically, participants rate statements that reflect the availability and quality of support from each source from 1 (very strongly disagree) to 7 (very strongly agree). A previous study with Syrian refugees in Turkey demonstrated reliability of the MSPSS (Yildirim et al., 2020). In the current research, the MSPSS showed strong internal consistency at follow-up assessment (polychoric α = 0.92, polychoric ωhierarchical = 0.91).
Generalized Anxiety Disorder
The Generalized Anxiety Disorder 2 (GAD-2) is a brief measure of anxiety derived from the original GAD-7 (Spitzer et al., 2006). The two included items tap into the core symptoms of many anxiety disorders and ask respondents to rate the frequency of their anxiety symptoms occurring within the past 2 weeks from 0 (not at all) to 4 (nearly every day). A score above three indicates a possible anxiety disorder. Several studies with Syrian refugees in Germany demonstrated good utility of the GAD-2 and GAD-7 (Borho et al., 2020; Georgiadou et al., 2018). The GAD-2 showed strong internal consistency at follow-up assessment (polychoric α = 0.90, polychoric ωhierarchical = 0.86) in the current study.
Data analytic plan
We fit cross-lagged panel models within a structural equation modeling framework to examine the prospective association of dimensional depressive symptom severity at baseline assessment with perceived stress, namely perceived helplessness and low perceived self-efficacy, and perceived control at 1-year follow-up assessment (Figures 1 and 2). The cross-lagged panel models employed were considered ideal to adjust for autoregressive change in perceived stress (helplessness and self-efficacy) and control over 1 year while simultaneously examining the alternative direction hypothesis, namely that baseline perceived stress or control might prospectively predict altered depressive symptom severity at follow-up. Items from the PSS were treated as ordinal. Therefore, the model of perceived stress was estimated using weighted least squares estimation adjusted for mean and variance. The model of perceived control was estimated using full information maximum likelihood (FIML) estimation. Both models used a sandwich estimator of parameter standard errors to adjust for non-independence due to the nesting of some participants within families (Muthén & Satorra, 1995). In 68 (69.39%) families, one or two people were drawn from each family; therefore, there was an insufficient density of participants within each cluster (family) to estimate each model as multilevel (Wu & Kwok, 2012). Although participant anxiety symptoms and social support were not in the baseline assessment battery, secondary analyses used multivariate regression to examine whether baseline depressive symptom severity predicted dimensional anxiety symptom severity or social support at 1-year follow-up assessment. Specifically, regression analyses used Huber–White robust standard errors to adjust for nonindependence due to nesting of participants within families via the estimator package in R (Blair et al., 2022).
Participant age, gender, and demographic correlates of data missing at follow-up were included as covariates in regression and structural equation models. However, the number of categories assessed for participants’ marital status precluded estimating model fit when including marital status as a covariate in the model of perceived stress. Instead, both structural equation models were estimated without covariates to assess model fit and estimate model parameters (Figures 1 and 2), then repeated with covariates included to evaluate whether parameter estimates were affected by the inclusion of age, gender, and any empirical correlates of data missing at follow-up assessment. Structural equation models with covariates used FIML estimation to benefit from the robustness of FIML estimation to data missing at random conditional on covariates included in the model (Little et al., 2014). Data management and multivariate regression were conducted in the open source R statistical framework version 4.1.2 (R Core Team, 2020) using the estimator and psych packages (Revelle, 2015). Structural equation models were estimated using Mplus version 8.8 (Muthén & Muthén, 1998).
Results
Descriptive statistics and missing data
Descriptive statistics indicate, on average, mild depressive symptoms at both baseline and 1-year follow-up assessments consistent with psychological distress in this sample (see Table 1 for descriptive statistics). Overall, at baseline assessment, 57 participants reported depressive symptoms in the mild range, 7 reported depressive symptoms in the moderate range and 1 reported depressive symptoms in the severe range. At 1-year follow-up assessment, 57 participants reported depressive symptoms in the mild range, 6 reported depressive symptoms in the moderate range and 5 reported depressive symptoms in the severe range (Kroenke et al., 2001; Kroenke & Spitzer, 2002). By contrast, the assessment of anxiety symptoms at 1-year follow-up is, on average, below the putative thresholds to identify possible cases for further clinical assessment (Kroenke et al., 2007). Kroenke and colleagues evaluated two putative thresholds for the GAD-2; at follow-up assessment, 110 participants reported anxiety symptoms that exceed the lower severity threshold, whereas 30 reported anxiety symptoms that exceed both severity thresholds.
Descriptive statistics.
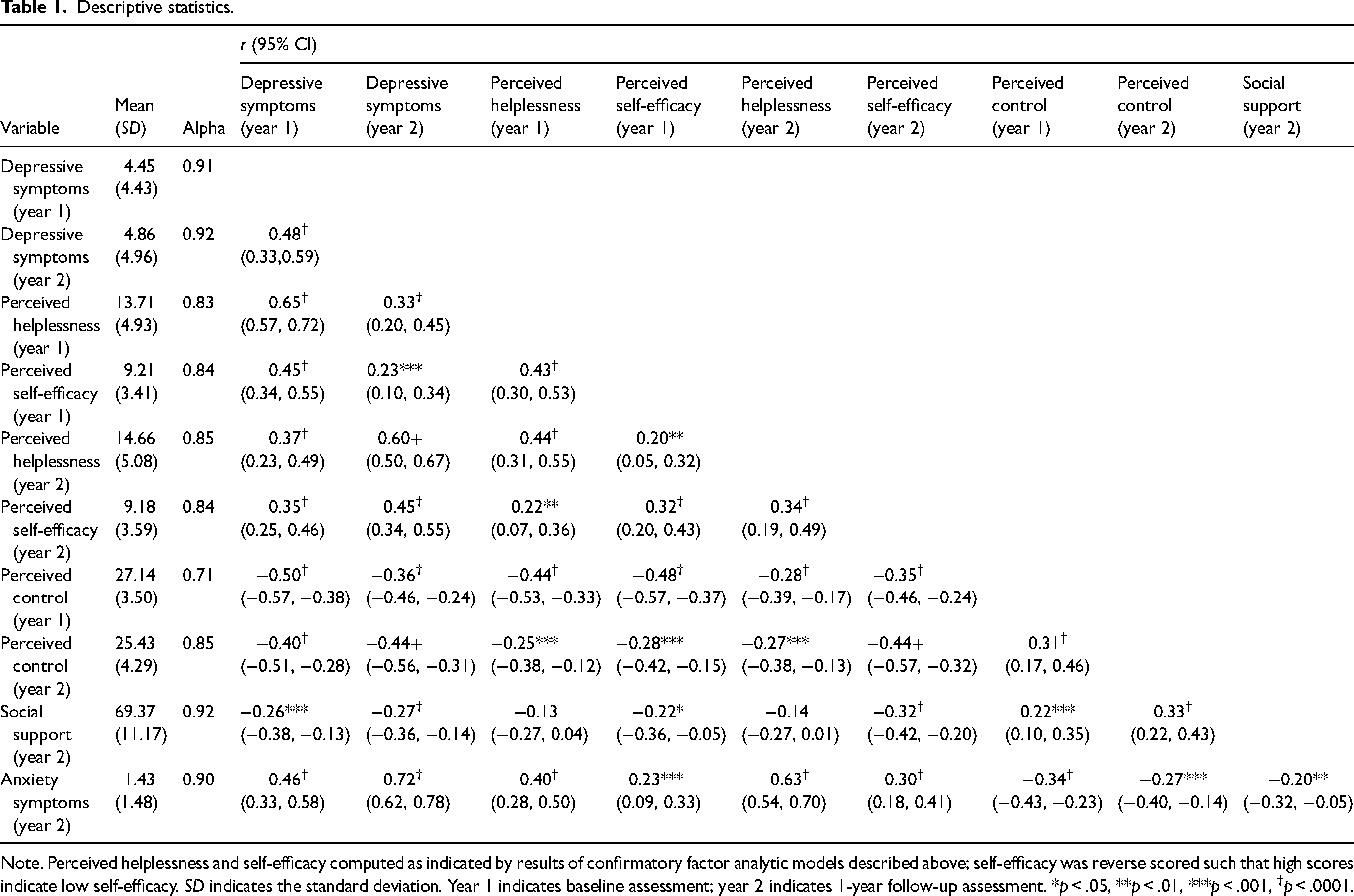
Note. Perceived helplessness and self-efficacy computed as indicated by results of confirmatory factor analytic models described above; self-efficacy was reverse scored such that high scores indicate low self-efficacy. SD indicates the standard deviation. Year 1 indicates baseline assessment; year 2 indicates 1-year follow-up assessment. *p < .05, **p < .01, ***p < .001, †p < .0001.
Preliminary analyses examined possible associations of focal and demographic variables with whether or not data were missing at the 1-year follow-up assessment. Overall, 15 (6.38%) participants did not provide data at the follow-up assessment. Attrition at follow-up was associated with participant marital status, χ2(4) = 14.15, p = .007. However, this was only evident because attrition was particularly common (50%) among the few participants (N = 4) who reported being divorced at baseline assessment. Attrition at follow-up assessment was unrelated to participant age, gender, ethnicity, language, sexual orientation, education, religion, or baseline report of depressive symptoms, perceived helplessness, self-efficacy, or control (p values > .12). As described above, participant age, gender, and marital status were evaluated as potential covariates in subsequent analyses.
Associations of depressive symptoms with perceived helplessness, self-efficacy, and control
As an overview, the current study sought to examine contemporaneous and prospective associations among depressive symptoms, perceived helplessness, perceived self-efficacy, and perceived control among Syrian refugees over the first year of resettlement in Canada. The cross-lagged panel model of depressive symptoms with perceived helplessness and self-efficacy at baseline and 1-year follow-up assessment fit the data well [χ2(196) = 269.52, p = .0004, RMSEA = 0.040, 95% CI (0.027, 0.051), CFI = 0.975]. Depressive symptoms were concurrently correlated with higher helplessness and lower self-efficacy at both assessments (Figure 1). Principally, baseline depressive symptoms prospectively predicted low self-efficacy at follow-up, whereas neither helplessness nor self-efficacy at baseline prospectively predicted depressive symptoms at follow-up. Similarly, the model of depressive symptoms with perceived control fit the data well as a fully saturated path model (Figure 2). Depressive symptoms were concurrently correlated negatively with perceived control at both assessments. Consistent with results pertaining to self-efficacy, baseline depressive symptoms predicted low perceived control at follow-up. However, high baseline perceived control may also prospectively predict low depressive symptoms at follow-up despite a robust autoregressive correlation for depressive symptoms from one year to the next. Results for both models remained following adjustment for participant age, gender, and marital status, as described in the data analytic plan above. There was limited evidence that participant age, gender, or marital status were associated with perceived control (p > .18), helplessness or self-efficacy (p > .08) at follow-up assessment.
Association of depressive symptoms with anxiety symptoms and perceived social support
Although consideration of participant burden precluded the assessment of perceived social support and anxiety symptoms during the baseline assessment, both were assessed at follow-up. Even after adjustment for participant age, gender, marital status, perceived helplessness, perceived self-efficacy, and perceived control, baseline depressive symptoms are associated with lower perceived social support at 1-year follow-up assessment (Table 2). Similarly, baseline depressive symptoms are associated with higher anxiety symptoms at 1-year follow-up assessment.
Regression model of social support and anxiety at 1-year follow-up assessment on depressive symptoms at year 1 – b (95% CI).
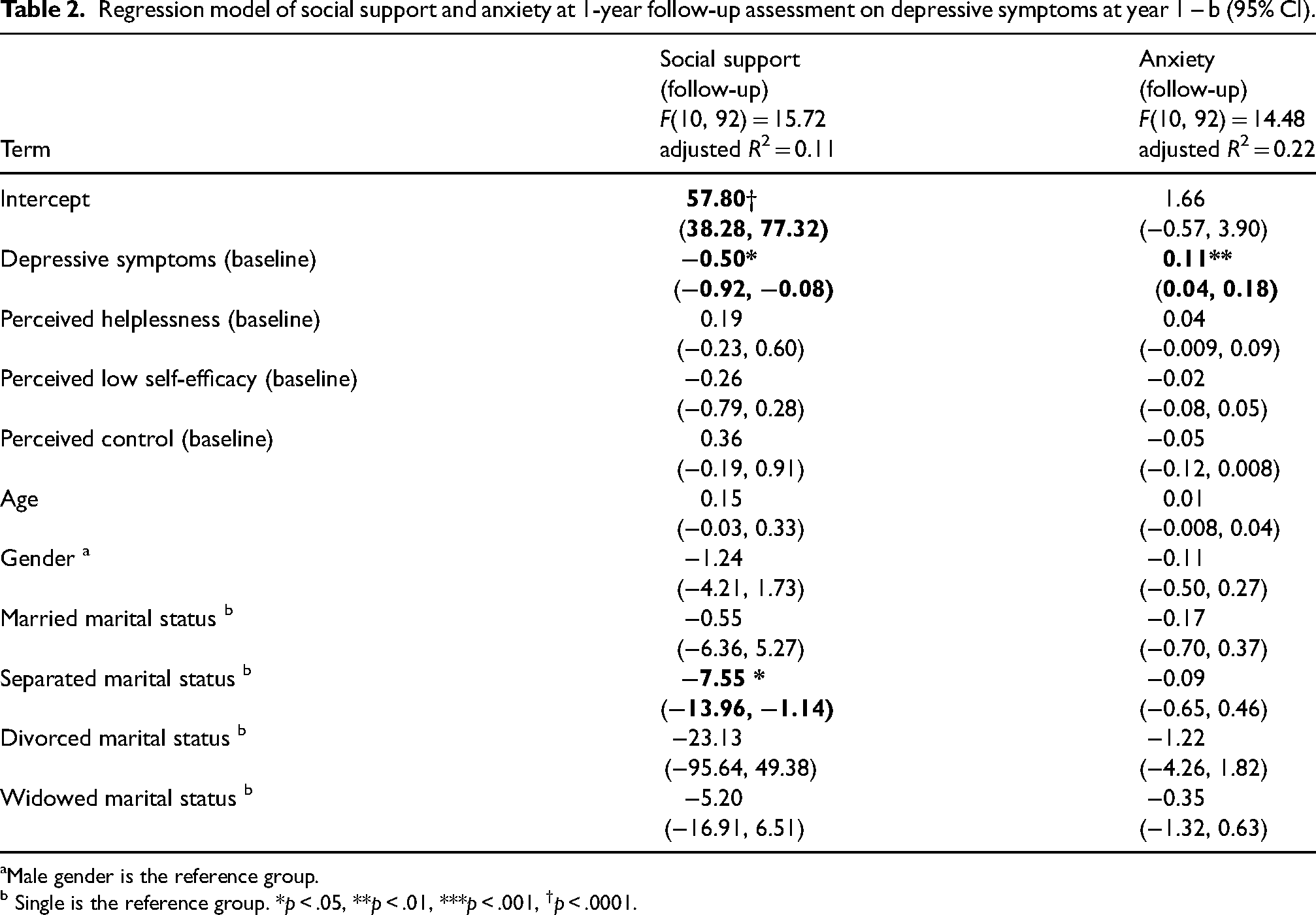
Male gender is the reference group. b Single is the reference group. *p < .05, **p < .01, ***p < .001, †p < .0001.
Discussion
Amid a rapidly growing international literature about displaced Syrian refugees (Barkil-Oteo et al., 2018; Peconga & Thøgersen, 2020), the current research represents a rare longitudinal examination of temporal changes in Syrian refugees’ mental health and psychosocial adaptation post-resettlement in host societies. Specifically, the current research leveraged a prospective design to assess and examine depression and its temporal effects on the perception of stress (helplessness and self-efficacy), perception of control, social support, and anxiety in a community sample of recently resettled Syrian refugees in Canada. Crucially, this study demonstrates that elevated baseline depressive symptom not only correlate with broad, impaired psychosocial well-being (e.g., lower perceived control, elevated helplessness) at the initial point, but also implicate the pervasive effects of baseline depressive symptoms on refugees’ psychosocial adaptation a year later in the resettlement process at follow-up. These results are highly consistent with evidence from LeMaster et al.'s (2018) longitudinal cohort study of newly arrived Iraqi refugees (N = 298) in the United States, which implicated baseline depressive symptom severity in refugees’ depressive symptoms and poorer acculturation outcome (e.g., lower social support) over 2 years. The current study extends the research by LeMaster and colleagues to underscore the profound and prolonged precipitating effects depressive symptoms may bear on displaced populations even after being resettled in a new host country with relative safety. The importance of depressive disorders for refugee mental health is supported by large-scale epidemiological reviews of refugee mental health based mostly on cross-sectional research (Blackmore et al., 2020; Kirmayer et al., 2011). However, the longitudinal design of the current study provides a critical innovation in demonstrating the contribution of initial depressive symptoms to refugee psychosocial adaptation over time.
Clinically, the wide-ranging and long-term effects of depression on Syrian refugees’ adaptation documented here draw attention to the exigency of early, depression-targeted screening, assessment, and treatment for Syrian refugees specifically (Hassan et al., 2015; Peconga & Thøgersen, 2020; Wells et al., 2016) and refugee populations in general (Magwood et al., 2022). The current findings suggest that early detection of depressive disorders and timely intervention and support for Syrian refugees struggling with depressive disorders may disrupt the adverse psychosocial sequelae of depression and other traumatic/stressful experiences. Some experts in refugee health observed a critical time window following trauma exposure, for which inventions would be most effective to provide relief and healing for refugee survivors (LeMaster et al., 2018). For instance, in a study of refugee survivors of torture resettled in the United States, Song et al. (2015) found that a provision of early culturally responsive and trauma-informed mental health services to refugees not only helps offset the negative effects of “a chain of psychosocial loss that threatens well-being” (Song et al., 2015, p. 558) for refugees, but also enables refugees to preserve the much-needed resources to cope with many post-migration stressors.
Conceptually, longitudinal, cross-lagged panel models used in this research provide support for existing theories on stress-coping and depression, namely the transactional model of stress and coping (Lazarus & Folkman, 1984, 1987) and the self-efficacy theory of depression (Maddux & Meier, 1995). The current study demonstrates that Syrian refugees’ baseline depression severity predicted greater perceptions of stress, specifically lower appraisal of self-efficacy, control, and social support availability 1 year into resettlement. Results pertaining to self-efficacy and control adjusted for concurrent associations at baseline. Therefore, even though depression is often treated as a psychological “outcome” (e.g., of trauma or life stress) in refugee populations (Euteneuer & Schäfer, 2018; Li et al., 2016; Naal et al., 2021), this study critically demonstrates that refugees’ depressive symptoms can effectively act as an antecedent risk factor to impede post-migration psychosocial adaptation.
Implications
This study has several potential implications for future research and to help bolster clinical services and interventions for the Syrian refugee population in Canada and worldwide. The study demonstrates the potential value of longitudinal assessment, which informs the development and progression of refugees’ adaptation. Therefore, this study meets the call of many experts in advocating for prospective, longitudinal research on the mental health and adaptation of refugee populations globally (Blackmore et al., 2020; LeMaster et al., 2018; Li et al., 2016) and Syrian refugee populations specifically (Borho et al., 2020; Peconga & Thøgersen, 2020).
Regarding the provision of clinical services, the study's findings underscore the urgency for early detection and screening of depressive symptoms for newly arrived Syrian refugees in their host country of resettlement. Previous recommendations that promote widespread assessment of depressive symptoms in routine medical and psychosocial care have been controversial (Canadian Task Force on Preventive Health Care et al., 2013; Siu & U.S. Preventive Services Task Force, 2016; Solutions for Public Health, 2020; U.S. Preventive Services Task Force, 2009), including calls for evidence-based confirmations on the potential clinical utility of routine depressive symptom severity assessment (Thombs et al., 2012; Thombs & Ziegelstein, 2014). Notwithstanding the argument that mild symptoms may not develop into a more severe presentation, ample psychosocial evidence identifies current or future impairment associated with mild depressive symptoms (Rucci et al., 2003). The current results further highlight the importance of assessing depressive symptoms early in Syrian refugees’ resettlement because depressive symptoms may index one's propensity for adaptation broadly and persist across multiple psychosocial indices, such as perceived stress, control, social support, and other aspects of mental health (e.g., anxiety symptoms). Kirmayer and colleagues further note that the Canadian recommendations, which recommend screening for depressive symptoms in high-risk populations (e.g., those with a history of trauma exposure), should be heeded in the detection and assessment of depressive symptoms among refugee and immigrant newcomers (Kirmayer et al., 2011), inclusive of recently resettled Syrian refugees.
The current study also demonstrates the suitability of a brief tool (the PHQ-9) to assess depressive symptoms among Syrian refugees resettled in North America. However, large-scale reviews caution against routine psychiatric and psychological screening or assessment of refugees without an appropriate trauma-informed context (to reduce the risk of triggering trauma; Hodes & Vostanis, 2019; Kirmayer et al., 2011) or follow-up support (Magwood et al., 2020; Pottie et al., 2011). Within the requisite integrated and interdisciplinary healthcare system, experts recommend a stepped-care model to address refugee mental health (Pottie et al., 2011; Song et al., 2015). In addition, recommendations consistently emphasize the importance of the presence of a well-trained language interpreter or cultural broker throughout the assessment and intervention process to ensure the cultural and linguistic responsiveness of services (Kuo et al., 2020a; Boucher & Kuo, 2020; Kirmayer et al., 2011).
In addition, considering the wide-ranging impacts of depressive symptoms on Syrian refugees documented here, clinicians may consider measures to promote effective coping and greater resilience among resettled Syrian refugees (Kuo et al., 2020a). Hassan et al. (2015) suggest that mental health and psychosocial support for Syrian refugees require a shift from “vulnerability-based frameworks” to “resilience and recovery-based approaches” that emphasize a strength-based perspective to enhance refugees’ agency, existing resources, and active participation in treatment. Consistent with personalized intervention approach, integration of specific culturally adapted intervention modules (e.g., behavioral activation) may also be particularly beneficial to the resettlement and success of refugees who report elevated depressive symptoms early in their resettlement process.
Finally, the critical importance of psychological and mental health support for refugees notwithstanding, increasing research has evidenced the fundamental role “social determinants” play in affecting refugees’ post-migration health and well-being Hynie (2018), including Syrian refugees in Canada (Kuo et al., 2020b). Hynie (2018) observed that social determinants of health for post-migration refugees and asylum seekers encompass income, employment, housing, language skills and access to interpretation, and social isolation. As follows, effective services and support for resettled refugees should include advocacy work to address refugees’ immediate logistic and subsistence needs, such as seeking housing, transportation, language interpretation, language training, education, employment, and more (Kuo et al., 2020a, 2020b). That is, a more holistic approach based on social, physical, mental health and community-based support and interventions is warranted to support resettled refugee individuals and communities.
Limitations
The results of this study should be considered in light of several limitations. First, there is statistical evidence of a strong autoregressive path for depressive symptoms over the 1-year follow-up period. Although consistent with previous longitudinal research (Cacioppo et al., 2010), this may leave less interindividual variance to be explained by other model parameters, such as baseline perceived self-efficacy. We note moderate to strong correlations of perceived hopelessness, self-efficacy, and control with depressive symptoms at both baseline and follow-up assessment. In addition, perceived control at baseline was associated with later depressive symptom severity. Also, the strong autoregressive path for depressive symptoms may indicate the relatively static nature of depressive symptoms as assessed by the PHQ-9. Second, it cannot be ruled out that the relatively low reported prevalence of depressive and anxiety symptoms reported in the current sample of Syrian refugees might be the consequence of some uncontrolled extraneous factors. However, this study identified similar prevalence rates for depressive and anxiety disorders as research on Syrian refugees in Germany (Borho et al., 2020; Georgiadou et al., 2018). Similarly, average reported social support at assessment 1-year follow-up was comparable with or slightly below other community adult samples (Clara et al., 2003) and higher than social support reported by participants in psychiatric samples (Eker & Arkar, 1995). Perceived helplessness and self-efficacy are comparable with that reported in an undergraduate university student sample by Roberti et al. (2006), but slightly higher than that reported in a sample of outpatient smoking cessation patients in China (Leung et al., 2010). Further research is needed to understand potential causes of variable prevalence rates for psychopathology in international research, which may be attributable to multiple factors such as differential self-selection into voluntary research; stigma in relation to disclosing psychiatric or psychological disorders to interviewers; or to the buffering effects of contextual factors associated with supportive resources in some high-income countries (Georgiadou et al., 2018; Hodes & Vostanis, 2019).
Conclusions
This model-testing prospective study points to the intricate, temporal relationships between baseline depression and subsequent impacts on Syrian refugees’ broad psychosocial responses, including their sense of helplessness, self-efficacy, control, social support, and anxiety. The study's results underscore the need, the value, and the merit of implementing prospective refugee trauma, mental health, and adaptation research informed by culturally and conceptually supported theoretical frameworks. The empirical insights and practical recommendations derived from this study should be considered carefully, but with an eye on their broader, potential implications for other rapidly emerging refugee populations internationally, including but not limited to refugees from Ukraine, Afghanistan, Myanmar (Rohingya Muslins), Venezuela, and South Sudan (UNHCR, 2022). It is hoped that this prospective research of resettled Syrian refugees may serve as a catalyst or example for future refugee mental health research to emulate, verify, or build on.
Footnotes
Acknowledgements
The parent project of this study was supported by a project grant from the Canadian Institute of Health Research (CIHR; 2016–2021) to Dr Michaela Hynie at York University, as the principal investigator, and the first author, Ben C. H. Kuo, as a co-applicant. The project title is “Refugee Integration and Long-Term Health Outcomes in Canada” (the SyRIN.lth project).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Canadian Institute of Health Research (grant number Operating Grant: Application #367393).