
Abstract
Due to cultural and systemic factors, Chinese-Canadians tend to use mental health services less or when mental health problems are more severe. Services need to be more culturally responsive in their treatment of mental illness. Around important life events, when there may be heightened vulnerability to mental illness, this is especially important. In this study, postpartum cultural practices were examined among recent immigrant, longer-term immigrant, and Canadian-born Chinese women. We conducted a longitudinal cohort study of 493 women in Toronto, Ontario, with livebirths in 2011–2014. Participants completed a demographic survey and Postpartum Rituals Questionnaire. Most women (82.2%) practiced at least one postpartum ritual. Younger age (OR 0.93; 95% CI 0.87–0.99) and greater participation in the heritage culture (OR 1.28; 95% CI 1.02–1.61) were associated with ritual practice. From among five types of postpartum rituals identified (i.e., avoidance of homeostatic disturbances, dietary practices, wind avoidance, organized support, and cold avoidance), dietary practices were most commonly undertaken and cold avoidance was least commonly undertaken. There were differences in postpartum ritual patterns by immigration status, with immigrant women being more likely to undertake a greater number of rituals, to attribute these rituals to Chinese culture, and to ascribe health benefits to these rituals and being less likely to feel forced into performing these rituals. Our findings underscore the importance of clinicians becoming more aware of Chinese postpartum rituals to provide women with culturally competent and patient-centered care.
Keywords
Introduction
Chinese-Canadians account for 5% of the population in Canada and are one of the fastest growing minority groups, with an estimated population of 1.77 million (Statistics Canada, 2017). Due to a myriad of cultural and systemic factors, Chinese-Canadians tend to use mental health services less or when mental health problems are more severe (Chiu et al., 2016; Fung & Wong, 2007). Mental health services need to be more culturally responsive in their treatment of mental illness, including improved efforts to understand, maintain, and promote mental health in a multicultural context. Around important life events when there may be heightened vulnerability to mental illness, this is especially important. Postpartum mental illness affects one in five women and has a significant negative impact on maternal and child health (Howard et al., 2014). Understanding cultural beliefs regarding the postpartum period may have important implications for preventing and treating postpartum depression and anxiety in Chinese-Canadian women (Dennis et al., 2007; Fung & Dennis, 2010; Grigoriadis et al., 2009).
As with many major life transitions, the perinatal period is steeped with rich cultural practices (Andermann & Fung, 2015). Postpartum practices, important in Chinese culture, include periods of rest; organized support in the undertaking of infant care, household chores, and meal preparation; dietary recommendations related to avoidance of cold or raw foods; and other practices (Dennis et al., 2007; Grigoriadis et al., 2009). There have been postulations that such practices may be protective against postpartum depression (Stern & Kruckman, 1983). There are multiple reasons for this. First, there are cultural beliefs that postpartum rituals confer both immediate and long-term health benefits, and failure to be able to perform such rituals may lead to distress (Stern & Kruckman, 1983). Second, our previous review found evidence that social support is one of the active ingredients in rituals associated with a reduction in risk for postpartum mental illness (Grigoriadis et al., 2009).
This review, which included 12 studies, found that participation in the Chinese ritual of “doing one month” was less important than the fact that women had considerable support during that time period (Grigoriadis et al., 2009). However, the protective value of the social aspect of postpartum rituals depended on numerous contextual factors. For example, if the support was less useful because of conflict with a family member, such as the mother-in-law, the ritual was less protective. Supports also had a negative effect on postpartum mental health if they were accompanied by pressure not to report symptoms or to accept one's emotions, without complaint, as a necessary part of becoming a mother. Since this review, several studies have described the impact of postpartum rituals on maternal mental health, generally demonstrating a protective effect (Chen et al., 2012; Demirel et al., 2018), with studies confirming that this protective effect depends on the type of postpartum ritual and other contextual factors (Ho et al., 2015).
Whether cultural rituals are maintained among immigrants depends on many factors. Acculturation describes the changes in beliefs, attitudes, and practices that occur when individuals from different cultures have frequent and regular interactions with one another, such as after immigration. Acculturation can be conceptualized as a bi-dimensional process, as individuals can identify with the new culture and retain their traditional culture to varying degrees, resulting in integration, assimilation, separation, or marginalization. This in part depends on the individual's acculturative strategy, available resources, and societal forces or policies (Fung, 2012). First-generation immigrants, including immigrant mothers, often face acculturative stress (D’Anna-Hernandez et al., 2015). For second-generation immigrants, there may be cultural conflicts regarding traditions, which could lead to even worse mental health than first-generation immigrants (Takeuchi et al., 2007; Vang et al., 2015). Adoption of new customs may involve giving up some of those of the culture of origin, resulting in conflict with family and exclusion because of differing values. Time since immigration may play a role in determining the level of acculturative stress. Therefore, as there may be a subjective component to the effect of postpartum rituals on postpartum mental health, it is important to examine differences between women who practice these rituals and those who do not, as well as the volition and rationale behind these practices, all of which may have differential effects on their mental health.
The objectives of the current study were: (1) to estimate the prevalence of postpartum ritual practices by Toronto-based Chinese immigrant and Canadian-born women early in the postpartum period; (2) to identify background characteristics associated with practicing postpartum rituals among Chinese immigrant and Canadian-born women; and (3) among those who practice these rituals, to describe uptake and motivation for practicing and differences by immigrant status.
Methods
Data for the current study were derived from a longitudinal observational study that followed 571 Chinese-Canadian women from four weeks postpartum to one year postpartum (Dennis et al., 2017). Self-identified Chinese immigrant or Canadian-born Chinese women were recruited within the first four weeks after a livebirth from Toronto, Ontario, the largest city in Canada (population: ∼3 million), via referrals and self-referrals from public health visitors, community organizations, study flyers, and ethnic newspapers, and provided informed consent to participate in the study. The exclusion criteria were: having an infant who was not discharged home at the time of recruitment, having active suicidal thoughts, and currently using antidepressants or antipsychotics. Only women who responded to the 12-week postpartum follow-up telephone survey, which included the postpartum rituals questionnaire, were included in the current analysis. Ethics approval for the study was obtained from the University's Research Ethics Board.
Measures
Background Characteristics. The background characteristics investigated as being predictive of postpartum rituals were selected a priori and included age (in years), parity, education level (postsecondary or less), employment status in the year prior to giving birth (employed or not employed, the latter including keeping house and obtaining education), home country (mainland China, Hong Kong, and other), immigration status, and acculturation. Immigration status was categorized into three groups: recent immigrants (i.e., migrated to Canada within five years from study date), longer-term immigrants (i.e., migrated to Canada more than five years from study date), and Canadian-born women (i.e., born in Canada or migrated at age five or younger, before formal schooling began). Using the Vancouver Index of Acculturation (VIA), participants were asked to rate the extent to which they participated in heritage culture (heritage subscale) and mainstream culture (mainstream subscale) (Ryder et al., 2000). The VIA is a 20-item measure of acculturation; the heritage and mainstream subscales each have 10 items, for which means are calculated. The subscales had Cronbach's alphas of 0.82 and 0.88, respectively, at follow-up.
Postpartum Rituals. The primary outcome was the practice of postpartum rituals. A Postpartum Rituals Questionnaire was designed by the lead author based on a systematic review of the literature (Dennis et al., 2007). The questionnaire had three sections. The first section contained descriptive questions about whether the respondent had participated in any “customs, rituals or other types of activities” based on her “Chinese culture or family traditions” in the first month after having her baby (yes/no), and if so, whether she wanted to or was forced to. In the second section, those who replied affirmatively were asked to respond to a 41-item scale about specific rituals or practices drawing from four general areas: (1) organized support for the mother (e.g., “did you have a family member come and stay with you to help you?”), (2) periods of rest and restricted activities (e.g., “did you remain at home?”), (2) prescribed food to be eaten or prohibited (e.g., “did you avoid raw foods?”), and (4) hygiene and physical warmth practices (e.g., “did you take hot showers?”). For each question, the respondent was asked to categorize the ritual or practice according to uptake and motivation using five response options: “yes, because of Chinese culture,” “yes, because of Chinese culture, but I would have preferred not to,” “yes, but not because of Chinese culture,” “no, didn’t need or want to,” or “no, but I would have liked to because of Chinese culture.” The third section contained questions relating to the women's overall description of the postpartum rituals, including length (e.g., “how long did you practice these activities?”) and anticipated benefits (e.g., “did you practice these activities because of their health benefits or because of tradition or both?”).
Statistical analyses
We calculated the proportion of respondents who practiced any postpartum ritual overall. Likelihood of practicing postpartum rituals according to background characteristics was calculated using Chi square tests for univariable analysis and logistic regression multivariable analyses showing adjusted associations for each baseline characteristic, controlling for other baseline characteristics.
Descriptive questions from the Postpartum Rituals Questionnaire were summarized using frequencies and percentages or means and standard deviations, as appropriate. Univariable comparisons across immigrant groups (recent immigrants, longer-term immigrants, and Canadian-born women) were made using Chi square tests and t-tests. Data from the 41-item scale were then analyzed using principal component analysis (PCA) to determine the structure of the scale. As the response options were categorical, Nonlinear Principal Component Analysis (NLPCA) was employed using CATPCA in SPSS. NLPCA uses a process referred to as “optimal scaling” to find the best possible quantifications for the categorical variables so that the greatest amount of variance is accounted for. The number of principal components was selected using parallel analysis and the nonparametric bootstrap to assess the significance of the loadings (Linting & van der Kooij, 2012). The component loadings were rotated using the Varimax rotation to increase interpretability. After the scale structure was determined, the scale data were summarized using medians, interquartile ranges or frequencies, and percentages and compared across immigrant groups using the Kruskal-Wallis test, with planned contrasts comparing new and longer-term immigrant groups. Statistical significance was established using the cut-off of < .05. All analyses were undertaken using SPSS version 24.
Results
Of the 571 women who responded to the four-week survey, 494 completed the 12-week survey. All except one woman completed the Postpartum Rituals Questionnaire, resulting in a final sample of 493 recent immigrant (40%), longer-term immigrant (42%), and Canadian-born (18%) Chinese women. Women were mostly from Mainland China (71%), were primiparous (69%), had post-secondary education (92%), and worked before giving birth (66%).
Prevalence and predictors of postpartum rituals practice
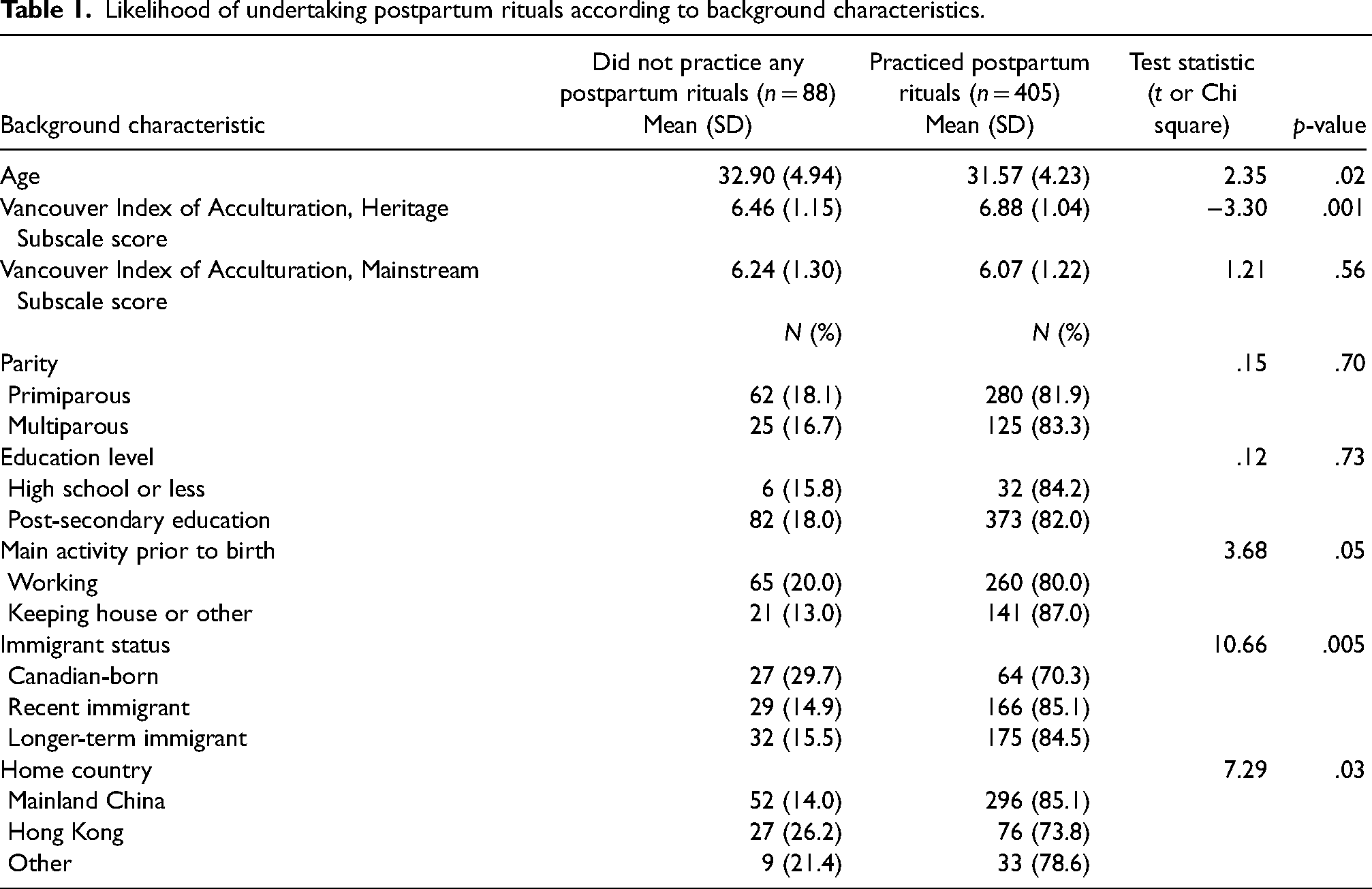
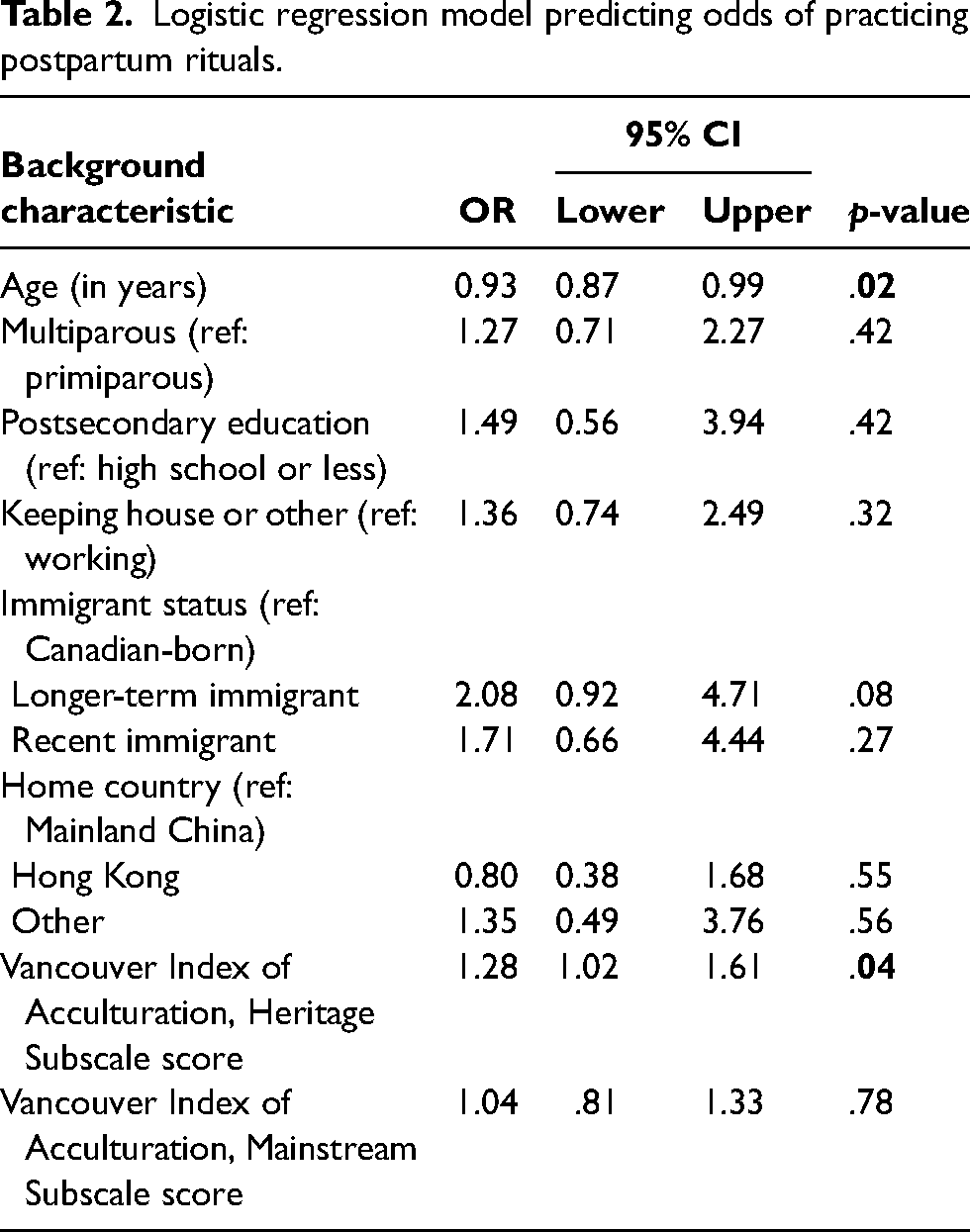
In total, 405 women undertook at least one postpartum ritual in the first month after childbirth, a prevalence of 82.2% (95% CI 78.5–85.3%). Table 1 presents a summary of the background characteristics associated with women practicing postpartum rituals. Younger age, a higher heritage score on the VIA, “keeping house” (vs. working) prior to birth, being an immigrant (vs. Canadian-born), and coming from mainland China (vs. Hong Kong or elsewhere) were associated with higher odds of postpartum ritual practice in univariable analyses. When all variables were considered together (Table 2), age (OR 0.93; 95% CI 0.87–0.99) and heritage score (OR 1.28; 95% CI 1.02–1.61) remained statistically significantly associated with postpartum ritual practice.
Likelihood of undertaking postpartum rituals according to background characteristics.
Logistic regression model predicting odds of practicing postpartum rituals.
Analysis of the postpartum rituals
The distributions of Postpartum Ritual Scale items were inspected, as response categories with very low frequencies can result in model instability (Markus, 1994). Two response options suggesting ambivalence, “yes, because of Chinese culture, but I would have preferred not to” and “no, but I would have liked to because of Chinese culture,” were seldom used and were combined with the corresponding categories indicating if the ritual was performed, resulting in three categorical responses: ritual practiced because of Chinese culture; ritual practiced but not because of culture; and ritual not practiced. Five low-frequency items that were not common Chinese rituals were dropped. Two further low-frequency items were removed to reduce redundancy, i.e., “take hot showers” vs. “avoid hot showers” and “take hot tub baths” vs. “avoid hot tub baths,” in which case the former items in each pair were removed.
NLPCA was undertaken on the remaining 34 items. A model with six dimensions was initially selected based on parallel analysis. However, even after rotation, the sixth component was not interpretable. The three items in this component, “apply heat to your abdomen,” “participate in religious ceremonies,” and “have a friend come and stay with you,” were not related to one another and offered little explanatory value (Variance Accounted For [VAF] .37–.44). We removed these items and re-ran the analysis. Parallel analysis on the reduced scale selected five factors, which provided best separation of the components while aligning well with our theoretical model. One item was subsequently removed (“have meals brought to you in bed”) because it offered minimal contribution to the overall VAF (< .30) (Linting & van der Kooij, 2012).
The rotated loadings and total VAFs for the final 30-item scale are presented in Table 3. Components were rest and activity restrictions for avoidance of homeostatic disturbances (Component 1), specific dietary practices (Component 2), wind avoidance (Component 3), organized support (Component 4), and proscriptions of hygienic practices for cold avoidance (Component 5). Cronbach's alphas based on the rotated solution were .91, .85, .88, .78, and .73, respectively. Cross-loadings were noted with a few items. The item “avoid wind (including hair dryers)” is potentially ambiguous, as it included both avoidance of indoor homeostatic disturbance (i.e., artificial air currents from a hair dryer against wet hair, Component 1) and elemental wind (Component 3). We assigned this item to Component 3, but future iterations of the scale may separate this item into two parts or remove the hair-drying component. The item “eat only certain types of food” fit best with Component 2, although it loaded onto both Components 2 and 5.
Rotated component loadings for four-dimension solution of the Postpartum Rituals Questionnaire.
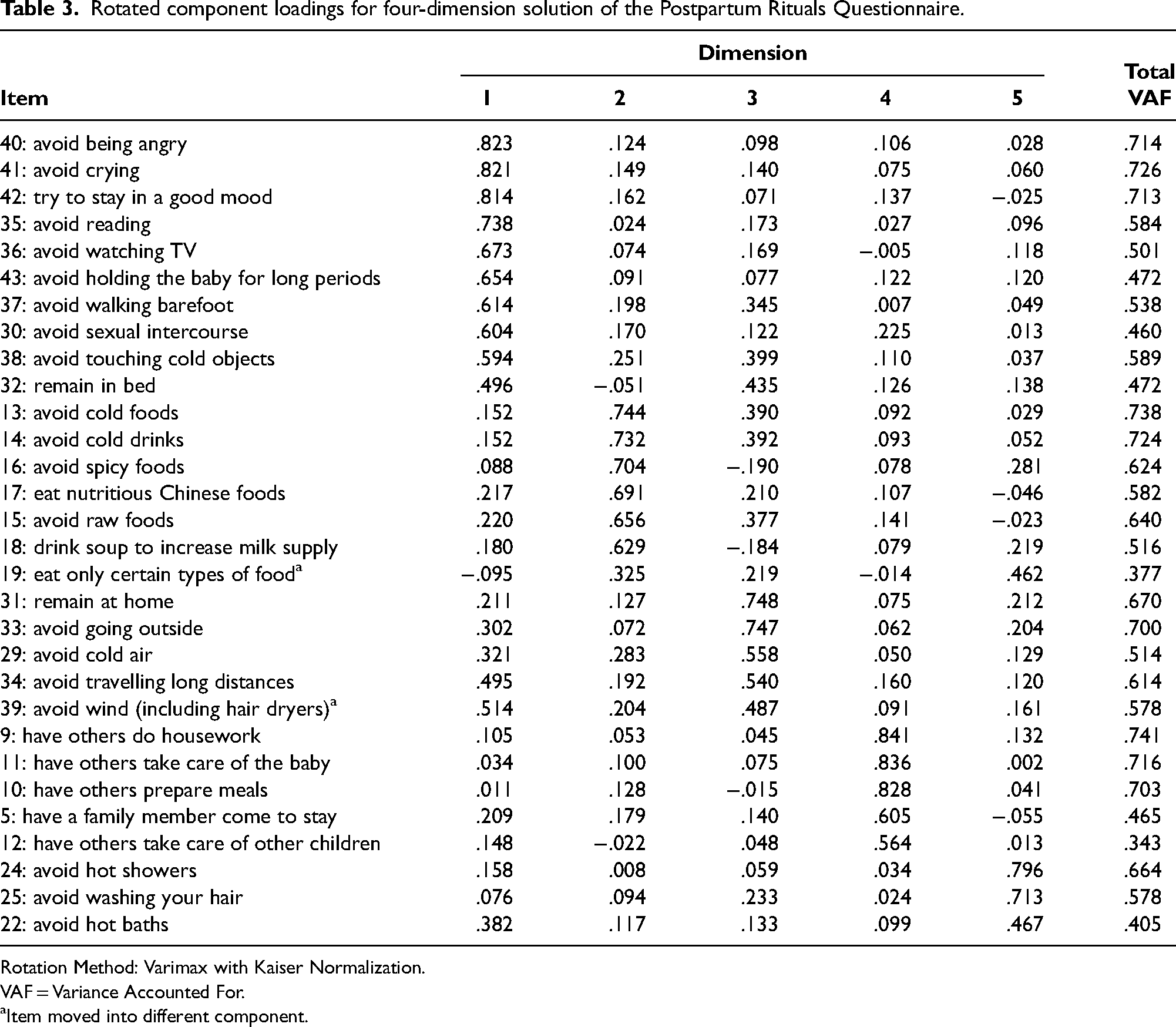
Rotation Method: Varimax with Kaiser Normalization.
VAF = Variance Accounted For.
Item moved into different component.
As shown in Table 4, the women undertook a median of 14 rituals because of Chinese culture and five rituals not ascribed to Chinese culture. About half of the women (46.7%) practiced the majority of rituals listed and attributed them to Chinese culture. Only 12.1% of women never attributed any of the rituals to Chinese culture. The rituals most highly undertaken because of Chinese culture were dietary practices. Almost three out of four (71.9%) women practiced the majority of dietary rituals and attributed them to Chinese culture. In contrast, only 26.4% of women said they practiced the majority of organized support rituals and attributed them to Chinese culture. The largest proportion of rituals not undertaken related to cold avoidance; a median of two out of three rituals were not adhered to.
Summary of scores of the postpartum rituals questionnaire.
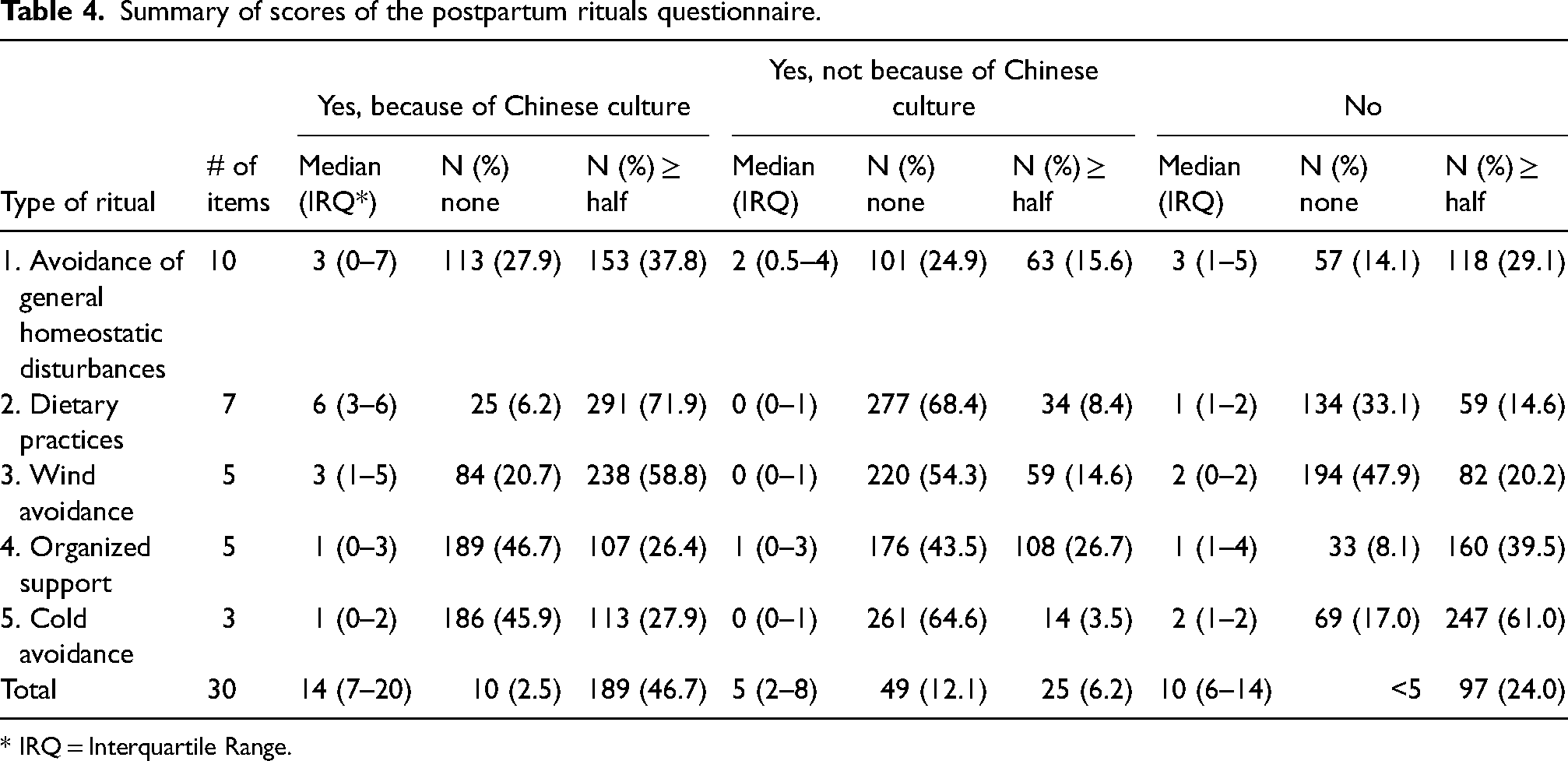
* IRQ = Interquartile Range.
As shown in Table 5, more rituals were undertaken due to Chinese culture by recent and longer-term immigrants than their Canadian-born peers in all subscales (all p < .001), except organized support (p = .76). By contrast, Canadian-born women undertook significantly more organized support (p < .001) and wind-avoidance rituals (p = .006) not because of Chinese culture than immigrants. No differences were found between recent and longer-term immigrants, with the exception of avoidance of homeostatic disturbances, for which more rituals were undertaken due to Chinese culture, and fewer not undertaken, by recent immigrants (both p < .001). The largest proportion of rituals undertaken due to Chinese culture by Canadian-born women came from dietary practices (four out of seven) and the smallest from avoidance of homeostatic disturbances and cold avoidance (both 0 out of 3).
Median number of postpartum rituals practiced by reason and subscale compared by immigrant status (inter-quartile range in parentheses).
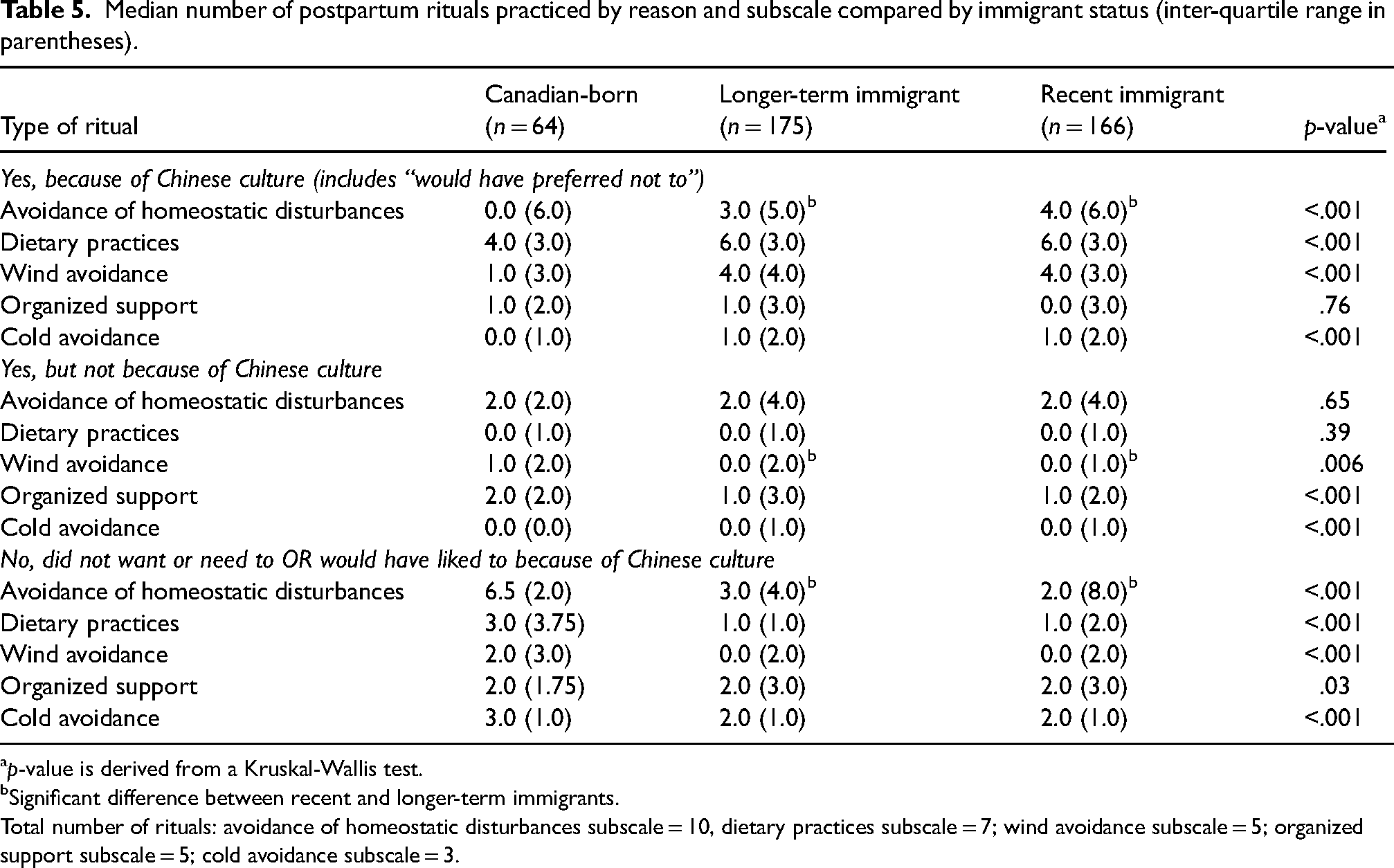
p-value is derived from a Kruskal-Wallis test.
Significant difference between recent and longer-term immigrants.
Total number of rituals: avoidance of homeostatic disturbances subscale = 10, dietary practices subscale = 7; wind avoidance subscale = 5; organized support subscale = 5; cold avoidance subscale = 3.
Chinese Canadian women's perception of postpartum rituals
Among women undertaking postpartum rituals, most practiced for 30 days (75.6%) and did so because of both tradition and the belief that these activities would benefit their health (69.1%). Most believed that practices would benefit their current (81.9%) and future (83.4%) health, and just over two-thirds thought that they would benefit their baby's health (64.2%). Under a third of women indicated that they were forced or expected to undertake rituals (29.3%). There was no difference in the length of time that rituals were practiced by recent immigrants (mean [M] = 29.9 days, standard deviation [SD] = 8.3), longer-term immigrants (M = 30.6 days, SD = 10.2), and Canadian-born women (M = 27.3 days, SD = 16.0; p = .13). However, Canadian-born women more frequently identified tradition as the only reason for undertaking rituals (31.3%) compared to immigrants (4.0% [longer-term] and 7.8% [recent]; p < .001). A higher percentage of Canadian-born women indicated that they were expected or forced into practicing (64.5%) than recent (17.5%) or longer-term (27.6%) immigrants (p < .001). Additionally, they less frequently thought that the practice would improve their current (67.2%) or future (62.5%) health compared to recent (current: 84.8% and future: 86.1%) and longer-term (current: 84.6% and future: 88.4%) immigrants (p = .004 and < .001, respectively). No differences were found by immigrant status with respect to perceived benefit for the baby's health (59.4% [Canadian-born] vs. 66.5% [recent] vs. 63.8% [longer-term]; p = .60).
Discussion
To our knowledge, this is one of the first studies to examine the practice of postpartum rituals in a large, diverse sample of Chinese-Canadians in the greater Toronto area. Of note, we found that the majority of women (82.2%) practiced at least some form of postpartum ritual, of whom 97.5% practiced at least one ritual attributable to the Chinese culture, with a median of 14 rituals practiced because of Chinese culture. Further, a majority (around 80%) believed that these activities would benefit their current and future health. Due to trends in immigration in Canada, there has been a recent wave of immigrants from mainland China, following the immigrant wave from Hong Kong in the 1980s (Bélanger & Malenfant, 2005). Chinese-Canadian women represent a clinically important proportion of the postpartum population. Our findings therefore underscore the importance of frontline clinicians becoming more aware of Chinese postpartum rituals to provide women with culturally competent and patient-centered care. Some prohibitions, such as cold and wind avoidance, may have important implications in conventional healthcare practices, from the delivery suite to recommendations during early postpartum visits.
While immigrant status was not significant, identification with heritage culture was statistically significant. This suggests that a direct measure of heritage culture may be a better predictor of rituals and that immigrant status may not be as sensitive. We found that recent and longer-term immigrants had a significantly higher median number of rituals than Canadian-born women. While the distinction between recent and longer-term immigrants was not drastic, it was statistically significant for avoidance of homeostatic disturbances, which consisted of 10 items. Dietary practices may not be different between recent and longer-term immigrants because they were both high – a median of six out of seven rituals. Overall, our findings suggest that the practice of postpartum rituals does not rapidly decline within the same generation and still persists to a significant degree even in the next generation, though lessened. Clinicians should therefore attend to the practices of both recently migrated and Canadian-born women.
The principal components analysis of the Postpartum Rituals Questionnaire aided in highlighting important functional clusters that are consistent with a cultural understanding of postpartum rituals. In particular, it highlights two distinguishable kinds of avoidance, cold and wind avoidance, that separated out in the analysis. The two appeared related but are different. Wind can lower the temperature causing coldness, but wind itself is believed to be a cause for ailments, in the sense that wind can damage the body in the same way that elemental wind can damage trees (Dashtdar et al., 2016). Another important distinction was between cold avoidance and dietary practices. Some foods may be selected or avoided due to general dietary concern, such as the selection of foods thought to aid breastfeeding and recovery of strength, while others may be guided by the content of “hot” versus “cold” foods (Poh et al., 2005), which is not referring to the temperature of the food but classification according to Chinese traditional medicinal beliefs. The Postpartum Rituals Questionnaire may be used by clinicians to understand the use of cultural practices in the postpartum period and to tailor their care accordingly.
A cultural understanding of the purpose of these rituals may also help us understand women's perceptions and their reasons for uptake. Among the different types of postpartum rituals, dietary rituals were the most commonly practiced and specifically attributed to Chinese culture. Even among Canadian-born women, this subscale had the highest proportion of rituals undertaken due to Chinese culture, even though the total number of rituals undertaken was lower than among immigrant women. Other studies have found that traditional dietary practices are maintained because of the belief that women need nutrient-rich food to promote their health and ability to breastfeed. For example, some foods that are prescribed in traditional culture, such as pig's liver, are high in iron and vitamin A, which are integral to postpartum health (Yeh et al., 2014). Diet also plays an important role in Chinese culture as a symbol of caring for family members and as a means of maintaining health, according to Traditional Chinese Medicine beliefs. For immigrants, not having cultural foods may cause acculturative distress, since having access to traditional foods is a means of connecting with one's culture and health beliefs. Collectively, these factors may reinforce the importance of diet in the postpartum period.
Other rituals were not perceived to be a result of Chinese culture or were less commonly practiced in our study. For example, rituals surrounding organized support, when practiced, were not necessarily perceived to be due to Chinese culture. Some women may simply see these practices as addressing practical needs. According to traditional beliefs, even hot showers and baths may risk exposure to the element of cold during the postpartum period (Dashtdar et al., 2016). However, cold avoidance through not showering or bathing was not often adhered to in our sample. Modern hygienic considerations may trump traditional beliefs in this case (Yeh et al., 2014), and there is evidence from other studies of women moving away from this particular cultural taboo (Hsieh et al., 2017). This finding is an example of how some traditional postpartum rituals may evolve and change with the incorporation of new knowledge and practices and in the context of available modern facilities.
The above findings indicate that the meaning of and adherence to cultural rituals change with time, context, and acculturation. However, in our study, explicitly stated psychological ambivalence around specific ritual items was seldom endorsed. Less than one-third of the women endorsed that they were forced or expected to uphold the rituals. More research is needed to tease out ideas of force versus expectation, or, specifically, the differences between those who felt socially compelled versus those who upheld rituals for the sake of cultural expectations, rather than belief, and yet did so freely. Functionally, for Canadian-born women, who may hold less firm underlying cultural beliefs around rituals, the practice may remain just as important, if they themselves are indeed willing and feel empowered to do so. On the other hand, rituals that put women in a position where their views are challenged or oppressed, even if culturally sanctioned, may bring about distress and worse outcomes. This was noted in a recent study in China, where postpartum women living with their in-laws, who presumably may have specific expectations related to postpartum rituals, were found to have a higher risk of postpartum depression than those living only with their husbands (Wang et al., 2017).
Limitations
There are various limitations that need to be kept in mind when interpreting this study. Women included in the sample were highly educated and may not be representative of the broader Chinese-Canadian population. Further, as the study was conducted in Chinese-Canadian women in Toronto specifically, caution is recommended in generalizing the results to other Canadian women or other Chinese women living elsewhere. The major subscales of the Postpartum Rituals Questionnaire identified, while useful in research and clinical practice, need to be replicated in future studies. The postpartum ritual data came from one time point only. Longitudinal data may help to further explore whether perceptions change with time across the postpartum period and whether they predict other health and mental health outcomes. As the study relied on quantitative rather than qualitative methods, some of the nuances may also not be fully captured. In this regard, it is fortunate that the literature in this area tends to have more qualitative papers describing the rituals than quantitative (Poh et al., 2005). Nevertheless, a mixed methods approach within a Chinese-Canadian cohort may further elucidate and triangulate the more nuanced ambivalences and their relationship with outcome, which may still be relevant for clinicians dealing with individual patients.
Conclusion
Our study is one of the first large-scale studies to examine postpartum practices among Chinese-Canadian women in Toronto. Most immigrant and Canadian-born Chinese women were found to practice various postpartum rituals, with the former having a higher degree of cultural belief in the rituals’ health benefits. Dietary rituals were more often adhered to with particular cultural significance, while organized support was just as likely due to cultural and non-cultural motivations, perhaps reflecting practical need. It would appear that cold avoidance, in terms of not taking hot showers, was often not adhered to, reflective of modernization. Further studies are needed to examine the correlation of these practices with health outcomes, as well as the potential moderating effect of the degree of cultural identification and beliefs and whether the rituals are performed willingly or not. In the meantime, this study reinforces the importance of culturally competent maternal care, even among second-generation Canadian-born immigrants. It is helpful for clinicians to be aware of the major types of postpartum rituals and explore with their patients their own particular meaning ascribed to them. The Postpartum Rituals Questionnaire may aid in such assessments. Addressing any distress associated with cultural practices may be one possible intervention in care that can help improve perinatal mental health outcomes among immigrant women.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an operating grant from the Canadian Institutes of Health Research (Grant # IGO-79958 and MOP-102673). The funding source had no role in the study design, data collection, data analysis or interpretation, writing of the report, or decision to submit the article for publication. The authors have no conflicts of interest to declare.