
Abstract
It cannot be assumed that the experience of having an autistic child is the same across countries since demographic and systemic factors are as diverse as the manifestation of ASD symptomatology. This study explores the lived experiences of 20 Venezuelan parents after receiving an autism diagnosis for their child. Applied thematic analysis was used to analyze parental attitudes, challenges in identifying their child's delay, access to diagnostic services, beliefs towards autism, professional evaluations, family support, and perceptions toward health and educational services for autistic children. Venezuelan parents reported a generalized lack of autism awareness, an unsupportive school system, and judgment from their extended family. Despite the universal health coverage in the country, Venezuelan parents commented on the scarcity of services, as well as the lengthy and costly processes to receive an ASD diagnosis. The results support previous research findings showing that socioeconomic factors influence how parents experience the process of obtaining an autism diagnosis for their children. For most Venezuelan parents, it might imply a long journey in which limited resources and knowledge about autism will determine its route and length. For parents, cultural values and spiritual and religious beliefs will serve as both coping mechanisms and barriers to accessing services.
Autism Spectrum Disorder (ASD) is a lifelong neurodevelopmental condition characterized by difficulties in communication, social affect, and restricted and repetitive behaviors (American Psychiatric Association, 2013). Early identification and diagnosis might improve the likelihood of a referral for early intervention in autistic 1 children (Klin et al., 2015). For caregivers of autistic individuals, their children's difficulties in socioemotional development, some behaviors, and multiple health service needs can prove taxing (Corcoran et al., 2015; DePape & Lindsay, 2015; Ooi et al., 2016). In that respect, the literature on the lived experiences of caregivers of autistic children reports recurring themes such as stigma (Farrugia, 2009; Zuckerman, Sinche, Mejia, et al., 2014), social isolation (Myers, 2009; Safe et al., 2012; Schaaf & Zoghbi, 2011), cost of services (Altiere & von Kluge, 2009; Fletcher et al., 2012), and disrupted family dynamics (Bilgin & Kucuk, 2010; Bultas & Pohlman, 2014). These experiences become even more challenging among those residing in low- and middle-income countries (LMICs) due to rudimentary infrastructures, limited trained professionals, and low ASD awareness (Durkin et al., 2015). However, research from LMICs is limited since, with few exceptions, most studies exploring parents’ experiences have taken place in high-income countries (Desai et al., 2012).
ASD service provision and research are relatively new in Venezuela, given that autism was not widely recognized until 1978, when the first autistic individual was diagnosed (Negron, 2010). Prevalence research estimates that 1.7 in 1,000 Venezuelan children are diagnosed with ASD; this reflects minimum estimates of ASD in the country (Montiel-Nava & Pena, 2008). To obtain an ASD diagnosis, Venezuelan parents turn to medical professionals, which exemplifies the country's prevailing medical model of autism (Chown & Beardon, 2017). In this context, neurologists usually diagnose ASD by relying on their clinical skills without using standardized tests (Domínguez & Mahfoud, 2009). The Venezuelan constitution guarantees the right of all citizens to access free health care and adequate treatment, and most of the health provisions are offered via a network of public hospitals and clinics (Bonvecchio et al., 2011). Despite health service provision existing in the private sector, this is not accessible to many since only 11.7% of Venezuelans have private insurance (Comision Nacional contra el Uso Ilicito de Drogas, 2006).
Rates of identification and diagnosis, access and use of services, and the lived experiences of families with an autistic member vary across different races, ethnicities, and socioeconomic statuses (Divan et al., 2021). Additionally, cultural beliefs about autism affect parents’ recognition of symptoms and their treatment decisions (Wang et al., 2012; Zakirova-Engstrand et al., 2020), and influence their access to different educational and health care services (Cloete & Obaigwa, 2019; Daley, 2004; Desai et al., 2012; Dyches et al., 2004; Ooi et al., 2016). For example, Gómez (2022) stated that in Venezuela, people believe that autistic individuals would forever stay in a childlike and helpless state. The author also states that the public's perception of autistic individuals comes from movies and television, in which individuals with the diagnosis are typically seen as needing to be kept a secret, needing to recover from it, or even as loathsome.
Using a qualitative methodology, we aimed to explore the lived experiences of Venezuelan parents who had received an autism diagnosis for their child. This methodology facilitates the exploration of parental challenges, such as identification of their child's delays, diagnostic services accessibility, autism beliefs, professional evaluations, family support, and perceptions toward health and educational services for autistic children in Venezuela. A better understanding of cultural influences on parental attitudes would likely help professionals recognize the best ways to help parents access available services depending on their needs, resources, and beliefs and facilitate a more effective use of services.
Methods
Setting and participants
Maracaibo is the second-largest city in Venezuela, with an estimated 1,571,885 people constituting 5.43% of the Venezuelan population at the time of this study (Instituto Nacional de Estadistica, 2012). No national census has classified Venezuelans by ethnicity since 1926 because in Venezuela most inhabitants consider themselves to be mestizos. Ethnicity has a fluid definition in Venezuela wherein ethnic groups are not considered different but rather as variations along a single continuum (Davenport, 2020). At the time of this study, Venezuela was an upper-middle-income country (World Bank, 2015). However, because of a lack of more recent available data, it is now unclassified (World Bank, 2022).
We identified potential participants by using a non-probabilistic, purposive sampling approach and selected participants according to the following inclusion criteria: (a) being a parent of an autistic child, (b) having a professional diagnosis of ASD, (c) having a child between 5 and 10 years old, and (d) living with the child at the time of the study. Our sample size was consistent with standards for phenomenological research, requiring at least 12 interviews in homogeneous samples to reach saturation (Guest et al., 2012).
After the University of Zulia Institutional Review Board approved this study, we sent recruitment information to special education schools, institutions serving autistic children, and early intervention programs (both public and private). The research team contacted families interested in participating in the study by email or phone, and eligibility was determined based on the inclusion criteria and interviews were subsequently arranged. Participating parents provided informed consent, which included authorization to audiotape the interviews.
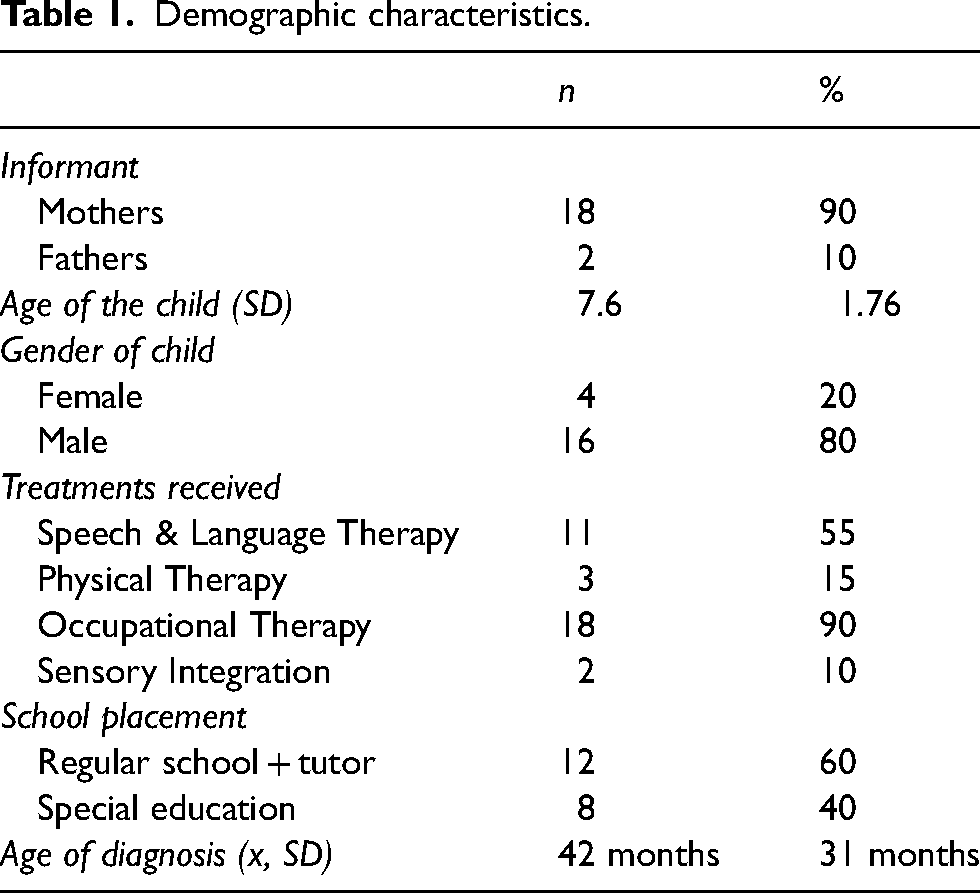
In total, 20 parents described their experiences of receiving a diagnosis of autism for their child. Mothers comprised 90% of the sample and fathers the remaining 10%, with a mean age of 32.4 years (SD = 6.24 years). Children's ages ranged from 5 to 10 years (x = 7.6 years, SD = 1.76), and they were predominantly male (80%), with a mean age of initial diagnosis at 42 months (SD = 31 months. See Table 1).
Demographic characteristics.
Procedure
Two trained bachelor-level research assistants conducted recruitment procedures, and one of them and the primary investigator (PI) conducted the interviews. Parents were given a choice to have the interviews at their homes or at the different agencies where their children were receiving services. All parents chose to have the interviews at the respective agencies. Interviews took place from January to October 2015, usually lasted 90 minutes, and if needed, had a follow-up session to clarify answers. The interviews followed a script developed for the study and were conducted in Spanish, audiotaped, and de-identified during the transcription process.
Measures
Sociodemographic questionnaire
Prior to the interviews, parents completed a demographic questionnaire that asked for information about their child's age, received services, and the school type their child attended at the time of the study.
Semi-structured interview
Guided by previous studies (Desai et al., 2012; Zuckerman, Sinche, Cobian, et al., 2014), we developed a set of possible questions for the semi-structured, open-ended, and in-depth interviews. We sent a preliminary set of questions to 10 professionals (four child psychologists, four special education specialists, and two child neurologists) and to two parents to validate the content and format. Findings from this expert validation procedure resulted in a new version of the interview, which we then piloted with two mothers of autistic children to test for understanding and length. There were no changes at this stage. We divided the final set of questions into five sections: (a) parents’ initial concerns about their child's development; (b) the experience of receiving an autism diagnosis; (c) interacting with service providers about ASD concerns; (d) communication with other members of the community about ASD; and (e) experiences within the family.
Data analysis
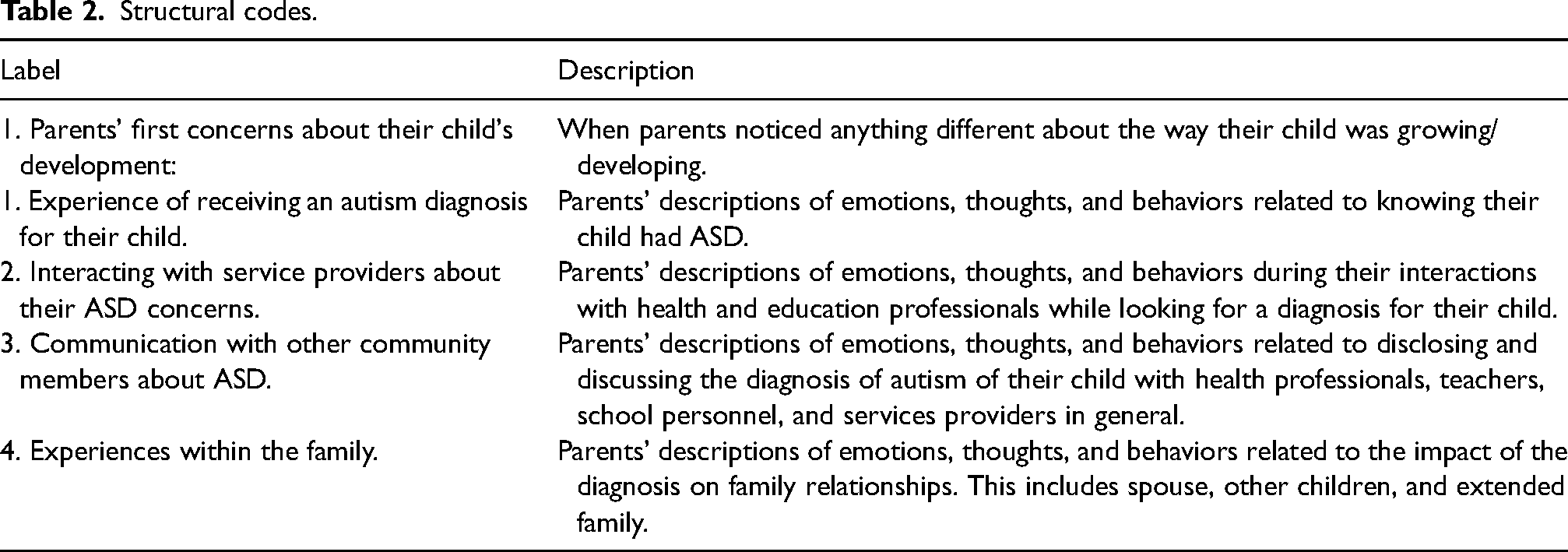
By using an applied thematic analysis methodology (Guest et al., 2012, 2020), we wanted to identify the pivotal shared lived experiences of the participants, and at the same time connect these experiences to the larger sociopolitical, economic, and cultural contexts of Venezuelan parents of autistic children. For the data analysis process, we developed a preliminary codebook using the interview categories as structural codes (Table 2) and integrated the original themes conceptualized for the interview's script and other themes that arose during the initial review of the interview transcripts. Three members of the team participated in the systematic review of the transcripts to assign structural codes. After coding was completed, the research team reviewed the coding framework and identified themes. As a part of data analysis, and to ensure trustworthiness and credibility, we examined the codes for consistency and redundancy via the constant iterative method. We collected interrater reliability data for 20% of the interview transcripts, with results suggesting strong reliability between raters (κ = 87; McDonald et al., 2019). After completing the analysis, the research team met to develop a summative grid of the emerging themes. We performed coding and theme development using ATLAS.ti software.
Structural codes.
Results
Our article describes Venezuelan parents’ lived experiences—including challenges, barriers, and facilitators—after receiving autism diagnoses for their children. A thematic map illustrates the key findings in Figure 1 with the six main themes derived from the data. Those themes reveal the different paths parents follow, from initial developmental concerns to obtaining a professional diagnosis of ASD and sharing the diagnosis with others.
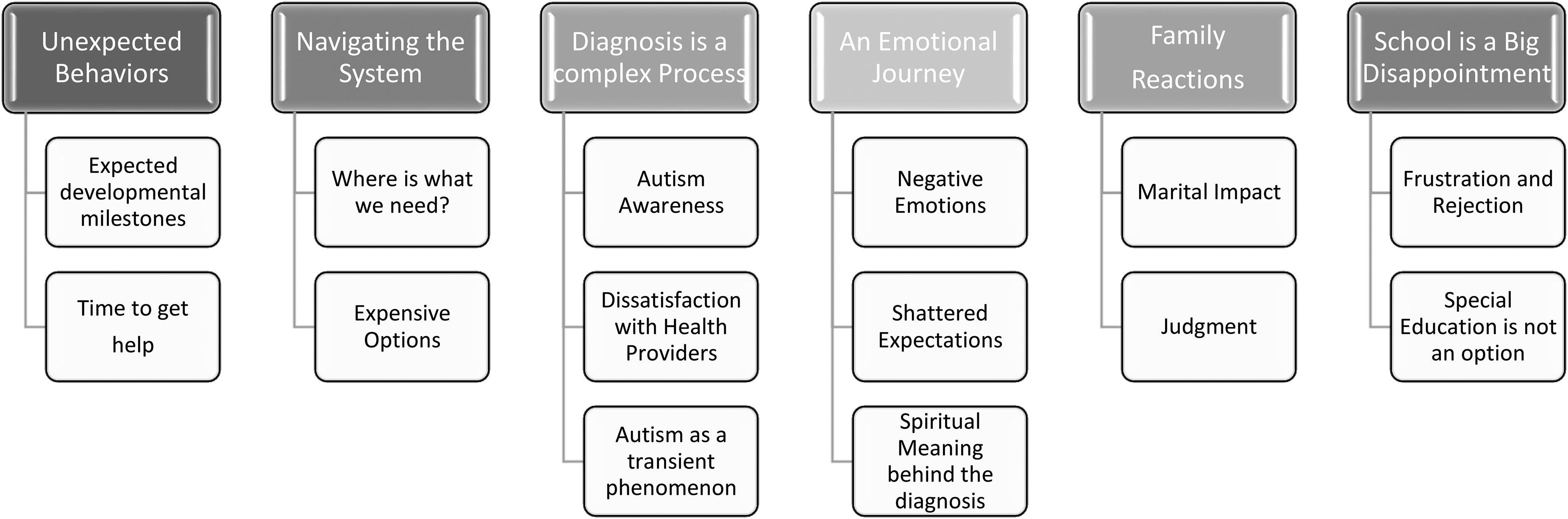
Themes map of parental lived experiences during the diagnostic process.
Theme 1: Unexpected behaviors
As parents started noticing the signs and symptoms of ASD in their child, they started looking for answers, and they described this seeking process in relation to two subthemes: expected developmental milestones and time to get help.
Expected developmental milestones
When we asked them to describe how they realized there was something different about their child, parents referred to autism-related symptoms such as language delay, inappropriate play, and not responding to their name: He was not talking … While my niece was already using sentences with two or more words, [child] only used three single words … he was mainly silent … His favorite game was touching the window curtains while running from one side of the room to another.
Even if parents were uninformed about the autism label, by the time they received the ASD diagnosis, they had already surmised their children's development was not appropriate. Moreover, because their child was exhibiting behaviors different from other children, they realized that it was much more than a delay.
Time to get help.
Because their children's development and behaviors deviated from neurotypical expectations, parents followed one of two different paths to move forward in searching for professional help. In some instances, parents were made aware of the need for a diagnostic assessment by teachers, school personnel, friends, or relatives. In others, they were the ones wanting to have the assessment and went to their child's pediatrician looking for answers and options: Her teacher recommended I take her for a psychological assessment. Later my mother called me and told me that she was worried, [child] was not talking … Then, I tried to register her for a new school, but the psychologist explained that her behavior was below what was expected for her age and that she might have autism. …
Theme 2: Navigating the system
Parents’ experiences while navigating the health system as part of the process of obtaining their children's diagnoses evolved around two subthemes: where to go for the diagnostic services and the cost of such services.
Where is what we need?
When parents realized they needed a diagnostic consultation, they were unaware of existing services. Additionally, they were confused about what type of service was rendered by each specialist and which professional to consult first (e.g., pediatrician, neurologist, psychologist, or therapist). Aside from parents’ limited knowledge about existing services, most of them also reported that health and educational professionals tended to ask them to have the child evaluated without specific descriptions of what the parents needed to request or expect, which added to their confusion and to delays. As participants recounted, delays were also affected by multiple assessments from different professionals who might not be working as a team or in the same institution: The teacher told me, “We need you to take [child] for a diagnostic evaluation.” … I took [child] to a child neurologist, and he requested an encephalogram, a letter from the teacher, and a psychological evaluation. …
Expensive options
Although there are government universal free services, the options are limited, and the waiting lists are very long. Considering this situation, some parents resort to private services to shorten the waiting period and obtain a more reliable diagnosis, which implies out-of-pocket expenses unless the parents have private insurance. However, the cost of private services is not affordable to regular Venezuelan citizens, so many utilize the public health care system, which entails logistical difficulties and long waiting periods: I was told that at the university hospital, there was a psychologist who could diagnose [child] … I had to go there—could not make the appointment by phone—and the waitlist was more than 6 months … I looked for other options, and the cost of an evaluation was more than my husband's salary.
Theme 3: Diagnosis as a complex process
The parents recounted the overall theme describing the process of receiving a diagnosis of autism along three main subthemes: awareness of ASD, dissatisfaction with health professionals, and autism as a transient phenomenon.
Autism awareness
Most parents voiced their feelings about lacking basic knowledge about the characteristics of autism at the time they received the diagnosis. Those who had heard the word autism before had a misconception of its meaning and had attributed different behaviors to the diagnosis: When the psychologist told me that my child had autism, I thought [child] had mental retardation [sic]. Before that day, I had never heard about autism. I never knew anybody with autism or heard about another person with autism.
Dissatisfaction with health professionals
As mentioned before, parents were aware that their children's development and behaviors were not within the expected patterns. However, when they expressed their concerns to their child's pediatrician or mental health professionals, they felt that the professionals disregarded their concerns and dismissed them without further examination or inquiries. As a result, in many instances, parents had to insist on getting a referral or navigate the system on their own to secure a referral with a specialist. Dissatisfaction was also linked to the short time professionals spent with their child and themselves before making and explaining the diagnosis: I felt the doctor was rushing the diagnosis. I was unsatisfied with the diagnosis, and I started looking for other doctors to tell me it was a mistake … If the first doctor had taken the time to explain to me in detail the diagnosis and how [child's] characteristics fit that, I would not have felt compelled to look for reassurance in others.
Autism as a transient phenomenon
Most parents thought their child was just delayed and would eventually catch up with some treatment, therapy, or medication. In sum, many reflected how they thought these symptoms were temporary and were a part of the child's expected development and assumed that the treatment would cure whatever their child had: I know he has this condition. However, I am taking him to all his therapies … I want him to be independent, to talk. I just want him to be happy, to have a job, a wife, and a family.
Theme 4: An emotional journey
In general, parents described this theme around three subthemes: a group of negative emotions to convey the depth of their experiences, a realization of their shattered expectations, and a search for spiritual meaning behind the diagnosis.
Negative emotions
As parents recounted their experiences after learning about their child's diagnosis of autism, they used various negative emotions to describe them. Most expressed disappointment, sadness, and grief as the main emotions related to their child's diagnosis, and at the same time they mentioned guilt. Specifically, they questioned themselves and thought of things they may have done to cause their child to be autistic or felt ashamed for having thought their child was lazy or spoiled: I felt defeated … Many ideas started racing in my mind, but I felt it was my fault, that I had failed my child by not making him talk, play, and behave appropriately … If I had worked harder, spent more time with him, or asked for help, my child would not be sick.
Shattered expectations
While talking about their emotional experiences, parents recalled feeling that their expectations of parenthood had been let down and that they were ill-equipped for the task ahead: I was disappointed with life. If you think that you want to be a mother, you would never think you would have to deal with sickness or disability. I had this beautiful child, but he has a condition—I did not know how to deal with it.
The spiritual meaning behind the diagnosis
As a part of the emotional journey of learning of their child's diagnosis, parents attempted to make sense of the diagnosis by attributing a spiritual meaning, specifically a Catholic meaning. While finding a spiritual and religious meaning, some parents explained their initial frustrations with the diagnosis and how they framed it as a God-sent message: It is a blessing and a lesson. God sent him to me so I could learn from him. I have all my hopes in God, and I know he will give me strength and wisdom to guide [child]. I know he [God] will help my boy.
Theme 5: Family reactions
The perceptions of others regarding ASD were also sources of frustration, and parents expressed the different impacts the diagnosis imposed on their families by choosing between two subthemes: marital impact and judgment and isolation.
Marital impact
For many parents, the experience of receiving the diagnosis of autism was lived as a joint task that brought them closer as a couple, and each partner found their spouse to be a source of support and strength. However, a few parents said they separated from their spouses after the diagnosis. After getting the diagnosis, my husband got very involved in the activities with our child. [Child's] autism brought our family together … Without my husband's support, I cannot see myself dealing with [child].
Judgment
When parents received their child's ASD diagnosis, they disclosed it to their extended families; in some instances, they were met with judgment, typically from their in-laws. The main content of such disapproving positions was related to denying the child's diagnosis or blaming the mother and her parenting practices for the child's difficulties: I did not want to tell my husband's family about the diagnosis, but he was adamant about letting them know. Then, to our surprise, his parents told him that [child] was OK, that he only needed discipline.
Theme 6: School is a big disappointment
All parents in our study perceived the school system as unsupportive and ill prepared to include children with developmental delays and develop individualized educational plans. They related their experiences through two main subthemes: frustration and rejection and having no available special education options.
Frustration and rejection
Parents expressed their frustration when dealing with the school system. The general experience was that the school would not assume the responsibility for teaching the autistic child and would transfer to the parents the task of finding a “good school” for their child, which could mean transferring to a private school with fewer children per classroom. For many parents, having their child enrolled at a school implied they had to pay out-of-pocket for an assistant teacher to attend classes with their child—an impossible expense for most families: You get tired of going to school after school and hearing, “This is not the school for your son; he will not be happy here.” … So, I learned to go from one rejection to another while figuring out how to help my child.
Special education is not an option
Venezuela's educational system lacks special education schools exclusively for autistic children. Special education schools are designed to educate children with all types of disabilities (Payà, 2020). However, parents in the study felt that sending their child to a special education school would present a setback since they do not offer services specifically for autism: But that was after visiting at least seven schools, all private because the public ones do not receive special children. You need to send them to special education schools with children that drool and do not talk. I did not want that for my boy.
Discussion
Although researchers have examined the experiences of parents of autistic children (DePape & Lindsay, 2015), studies in countries with little health infrastructure, few trained professionals, and a general lack of autism awareness are scarce (Bauer et al., 2022). We have tried to contribute to the literature by providing a sociocultural perspective showing the unique insights and experiences of parents from Venezuela, in a region with wide health disparity, barriers to accessing the few services available, and limited numbers of trained professionals (Da Paz et al., 2018; Smith-Young et al., 2020). Parents in Venezuela perceived the diagnostic process as a highly emotional, frustrating, and prolonged pilgrim's journey in which they had to proceed by trial and error, navigating uncharted territory and lacking health and educational systems, carrying a heavy burden of cultural expectations (i.e., parenting, discipline, marianismo).2 Ultimately, they felt abandoned when trying to obtain a diagnosis and treatment services.
The first stage of the journey began when parents first noticed unexpected behaviors that they described as atypical and that included preoccupations with language and speech delays, lack of response to their name, and other early clinical manifestations of autism. As in our 2017 study, the symptoms that triggered parents’ recognition were mainly related to the two dimensions of ASD: social affect and restricted behaviors and interests (Montiel-Nava et al., 2017). Scholars have suggested that in many Latino cultures, behavior problems in children are considered the result of poor parenting skills, and that parents might take longer to seek professional help (Chaidez et al., 2012; Magana et al., 2013). It is likely that if parents were noticing atypical behaviors, yet believed that they might be blamed for these, they might have taken longer to recognize or report them. In addition, Venezuelan families encounter daily challenges when fulfilling their basic needs (e.g., food, water, and personal safety), and thus, in that context, having a child that does not talk or is delayed may seem like a lesser problem, contributing to the delay in looking for services. Our participants thought their child's behavior was simply a delay and that the child would eventually catch up given proper treatment or medication. In this way, parents reflected on how they saw the delays as a transient phenomenon and expected that therapy would cure or fix the problem. By thinking that praying to God would help their child could overcome their problem, they also attached a religious meaning to a perceived temporary issue. These findings align with a growing body of research suggesting that underserved families have less access to information about mental health diagnoses (Zuckerman et al., 2015). Although we do not have information about the participating parents’ socioeconomic status, 90% of Venezuela's inhabitants live under the poverty level (Universidad Catolica Andres Bello, 2020). Such results highlight the importance of developing ASD awareness campaigns to educate parents living in underserved and low-resource areas. Campaigns could offer information about early ASD signs and which path to follow to get a professional diagnosis and referrals to early intervention services. To have an impact on Venezuelan parents, the information provided needs to address views about the cultural beliefs surrounding autism etiology (i.e., bad parenting, God's punishment), that could act as barriers to accessing services.
Similar to other studies, we found that parents complained about having to go to many appointments with various professionals, being placed on waiting lists in their attempts to obtain diagnoses for their children (Corcoran et al., 2015; Paula et al., 2020), and dealing with professionals who lacked the patience and understanding to work with autistic individuals (Phelps et al., 2009). A few studies on doctor–patient interactions in Venezuela have consistently shown that Venezuelan doctors’ communication with their patients about their condition is mediated by the perception that patients are unable to understand what they are being told (Cooper, 2015; Martinez, 2005). Furthermore, Venezuelan doctors think that economically disadvantaged people lack the rationality and understanding to deal with a clinical diagnosis (Martinez, 2005), and doctor–patient interactions can be understood as experiences of sociopolitical inclusion and exclusion (Cooper, 2015). Given this context, it is very likely that health care providers do not take the time to hear parents’ concerns and adequately explain to them their child's autism diagnosis. Equally important for health professionals is to listen to parents when they report concerns about their child's development. This awareness would mean validating parents’ references to unexpected behaviors, offering them relevant explanations of the meaning and possible etiologies of autism, and answering their questions, as opposed to assuming they would not understand. Consequently, children will receive earlier diagnoses and referrals, and parents will experience higher satisfaction with the diagnostic process.
Regarding the emotions experienced by parents when they learned about the diagnosis, parents in our sample reported denial, grief, guilt, and disappointment, which are similar as those reported in other studies (Corcoran et al., 2015; DePape & Lindsay, 2015; Desai et al., 2012). It is important to note that parents might doubt their parenting skills (Selkirk et al., 2009). Stigma also influences parents’ feelings of shame or guilt for having an autistic child (Mak & Cheung, 2008). However, Montenegro et al. (2022) found that compared to caregivers of autistic children from other Latin American countries, Venezuelan caregivers showed the lowest rate of perceived stigma. The authors considered that it might be possible that caregivers place concern on more pressing matters such as food and safety, pushing biases and negative stereotypes aside, and thus reducing the perception of stigma.
In Venezuela, as in most Latin American countries, perceptions of disability are heavily influenced by earlier Catholic teachings that disability was a consequence of sin (Gómez, 2022). From that perspective, some Latino parents with a disabled child consider said child as a gift from God, whereas others would believe the disability is a test from God or a punishment (Bailey et al., 1999; Skinner et al., 2001). Having this spiritual background, most of our participants understandably attached spiritual meaning to having an autistic child and used their spiritual beliefs to deal with negative emotions. On the other hand, fatalismo and faith could also be barriers to earlier diagnosis and intervention because parents might see their child's autism as a cross to bear or a punishment from God and thus something they need to accept (Gómez, 2022).
Societal roles and core cultural values could also affect how the child's extended family perceives the diagnosis. For our participants, most pressure to live up to traditional gender norms and criticism of parenting practices came from extended family members who blamed mothers for the child's difficulties. In Latin American cultures, mothers are viewed as the primary caregivers, whereas fathers are considered disciplinarians (Durand, 2011). Moreover, the value of marianismo promotes the idea that women must endure suffering with dignity by being nurturing and self-sacrificing (Abdullah & Brown, 2011). When endorsing marianismo, mothers are expected to do all the child rearing work, with limited involvement from fathers, which could contribute to family difficulties. Because of this cultural value, mothers could be blamed when a child exhibits unexpected behaviors, such as those displayed because of autism symptomatology.
A generalized experience for the participants was the lack of support from the school system. Even when teachers initiated the referral process for a diagnostic evaluation, they did not provide the child with accommodations or adaptations to help with their development. A shortage of special education settings might be responsible for this situation. In Venezuela, public education is free, including supplies, food, and transportation (Asamblea Nacional, 1999). However, public schools are overcrowded and lack resources. These limitations are even more prominent in special education facilities (United Nations Children's Fund, 2019). This critical situation leaves Venezuelan parents with the option of either registering their children in private schools or leaving them home with no educational services. Venezuelan parents must pay to register their child at a private school or send a tutor to attend school with the child. Because tutoring is a private service, an in-classroom tutor might only be an option to caregivers who can afford it. Consequently, most educational options for autistic children are private and expensive. Special education institutions are often perceived as “warehouse” institutions, without any individualized educational programs, interventions, or plans (León et al., 2008). The restriction in the number of options for educational placement leaves Venezuelan parents feeling lost and without governmental support to provide for their child's rights.
Although autism awareness, identification, and services in Venezuela have grown in the past decade, there is still inadequate access to health care and equal education. This inadequacy is a commonality among most LMICs (Durkin et al., 2015; Montiel-Nava & Pena, 2008; Montiel-Nava et al., 2017; Paula et al., 2020). Moreover, Venezuela has been afflicted with the worst inflation in the world (2,297%; World Bank, 2017), adding strain to the availability and accessibility of services for ASD. In this environment, the cost of a diagnostic evaluation becomes a powerful barrier to accessing care, as parents in our study reported. During the prolonged humanitarian crisis in Venezuela, the government systems coordinating services for the poor have collapsed, and children have been among those hit the hardest. The infrastructure of health and education systems has further deteriorated, and there has been an increase in the scarcity of trained professionals (Beyrer & Page, 2019). This sustained humanitarian crisis highlights the intersection of poverty, culture, social status, and disability—in this case, autism. Poverty is not a single factor but an array of physical and psychosocial stressors that affects many daily domains, such as educational achievement and health outcomes. Autistic children living in poverty have higher rates of poor health care outcomes (Durkin et al., 2015). The meaning of this relationship goes beyond the two variables in countries like Venezuela. We suggest in this study that being the parent of an autistic person in Venezuela would be a different experience depending on the parents’ income level, the type of health service they would have access to (public or private), and the speed at which they would receive the service. Income level might also determine the type of doctor–patient relationship they will have because Venezuelan doctors might perceive upper-class patients as possessing the rationality and understanding to deal with the diagnosis; whereas those with lower income could be underestimated (Cooper, 2015; Martinez, 2005). Wealthy Venezuelan families would have better and faster access to specialists who diagnose autism and better information about the condition than families living in poverty. This is an unfortunate finding since most of the population in Venezuela lives below the poverty level (Universidad Catolica Andres Bello, 2020).
We conducted our study in Maracaibo, Venezuela, and it has limits of generalizability because all participants were already receiving treatment, which does not represent the experiences of most parents in Venezuela—not even in Maracaibo. It excludes those parents whose children are not receiving treatment and those who have not yet obtained a diagnosis. However, our study's qualitative nature allows for the development of hypotheses and questions about the underlying meaning of autism for Venezuelan parents and the barriers to and facilitators of early diagnosis. For Venezuelan parents, developmental delays that are usually considered red flags for ASD might not be interpreted as problems, considering their other daily priorities (food, water, transportation, personal safety). The quantity and quality of information doctors share with parents about their child's diagnosis might be affected by the relationship with service providers if it is considered unsatisfactory and by doctors perceiving parents as being ill-equipped to understand the diagnosis. Having universal health coverage or public education does not warrant access to diagnostic services, and parents with no private insurance will wait longer for a diagnosis. Likewise, participants with no means to afford private school experience a lack of support from the school system, and special education is not a viable option for most Venezuelan parents. Cultural values such as fatalismo, marianismo, and even religious beliefs can also affect how the extended families perceive and conceptualize the diagnosis. In addition, Venezuelan parents consider faith and spirituality to be coping mechanisms that help them to find meaning in their children's ASD diagnoses.
Our study results have several clinical and practical implications. First, even when there is a generalized scarcity of services and a long-standing humanitarian crisis, parents are aware of some developmental delays in their children and want answers, which drives their search for a diagnosis. In addition, they require a diagnosis to receive any services. Second, these findings could inform evidence-based practices in Venezuela, which in turn will potentially improve the quality of care for autistic children and their parents. That means culturally sensitive and informed practices that consider parents’ perceptions of the patient–doctor relationship, spiritual beliefs, and cultural values affecting causal interpretations of the diagnosis. Third, sharing these findings with parents will help them share their experiences and understand that this is how most parents feel and act when they learn of their child's diagnosis of ASD. Fourth, as others have reported, participants in this study revealed that autism diagnoses are not accompanied by the supportive initiatives from health, education, or social service systems that parents expect. In Venezuela, a country with a communist government in which universal health and education are fundamental rights according to the constitution, parents rely on public institutions to fulfill those rights. However, as the parents in our study expressed, there are not enough facilities or professionals to serve all autistic children in the public system. Therefore, health and educational inequalities in Venezuela are evident for families with autistic children.
Conclusions
Our findings revealed that the mechanisms contributing to the Venezuelan parents’ lived experiences of obtaining a diagnosis of autism for their child were multi-dimensional. It might seem counterintuitive that in a country with a scarcity of services, ill-functioning institutions, most of its population living in extreme poverty, and cultural values emphasizing fatalismo and marianismo, a diagnosis of autism might be needed or sought after. Despite the extant health disparities and cultural values impacting the delays to diagnosis, Venezuelan parents recognize their children exhibited unexpected behaviors and want answers and a cure for the problem. That is their motivation to embark on this pilgrimage for a diagnosis. The negative emotions experienced during the process are like those described by parents in other geographical regions. However, the challenges of navigating the health care and educational systems, the spiritual connotation of the diagnosis, and the expectations for the doctor and patient interactions are embedded in a particular sociopolitical and cultural context that makes the experience unique for a Venezuelan parent. Obtaining a diagnosis of autism in Venezuela will depend on the parents’ income level. For most Venezuelans, it will imply a long journey in which limited resources and knowledge about autism will determine the route and length, and cultural values, as well as spiritual and religious beliefs, will serve as both coping mechanisms and barriers to accessing services. As mentioned in this article, there is little information about how Venezuelans conceptualize autism, highlighting the need for more research on this topic.
Our findings emphasize the need for programs that target underserved groups, children, and families living in LMICs. Programs focused on autism awareness should be adapted according to local socioeconomic implications of ASD symptoms and the understanding of developmental delays within cultural norms. Implementing such programs might require cultural sensitivity training for health and education professionals to facilitate earlier referral, timely diagnosis, and initiation of autism-specific interventions that can enhance child development.
Supplemental Material
sj-docx-1-tps-10.1177_13634615231211482 - Supplemental material for Pilgrimage for an autism diagnosis: A study of Venezuelan parents’ experiences
Supplemental material, sj-docx-1-tps-10.1177_13634615231211482 for Pilgrimage for an autism diagnosis: A study of Venezuelan parents’ experiences by Cecilia Montiel-Nava, Irina Vargas, Zoila Gonzalez-Avila, María Cecilia Montenegro, and Ana C. Ramírez in Transcultural Psychiatry
Footnotes
Author contribution
Cecilia Montiel-Nava: conceptualization, methodology, investigation, resources, Writing – review & editing, supervision, and project administration. Irina Vargas: conceptualization, investigation, and methodology. Zoila Gonzalez-Avila: methodology and investigation. María Cecilia Montenegro: Writing – review & editing. Ana C. Ramírez: Writing – review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.