
Abstract
Although the diagnosis of selective mutism (SM) is more prevalent among immigrant children, the link between the disorder and an immigration background has been elusive. Guided by ecocultural models of development, the current study aimed to construct a theory-based description of SM while considering individual, family, and contextual risk factors. Participants were 78 children with SM (38.4% with an immigration background), and 247 typically developed children (18.2% with an immigration background). Consistent with previous studies, our results suggest that anxiety was the most important predictor of SM symptoms, above and beyond immigration background. Immigration, especially if coupled with bilingual status and low family income, predicted increased levels of SM symptoms. Identifying multi-level predictors of SM may help researchers and clinicians to improve early identification and treatment of SM in culturally and linguistically diverse children.
Introduction
Selective mutism (SM) is a childhood psychiatric disorder, characterized by the child’s persistent failure to speak in specific social situations where speaking is expected, despite speaking in others (American Psychiatric Association (APA), 2013). SM is diagnosed in 6–8 per 1,000 children in the general population (Bergman et al., 2002) and has been associated with adverse emotional, social, and functional outcomes, such as anxiety, depression, social problems, and academic difficulties (Mulligan & Siphon-Blum, 2015). Previous studies have consistently showed that immigrant children are overrepresented among children with SM (Elizur & Perednik, 2003; Steinhausen & Juzi, 1996; Toppelberg et al., 2005). However, a direct examination of the link between an immigration background and the development of SM is still scarce. Guided by ecocultural models of development (Bronfenbrenner, 1979; Eriksson et al., 2018), the current study aimed to construct a theory-based description of SM while considering individual, family, and contextual risk factors.
Establishing an ecocultural perspective on SM
Developing a coherent, culturally relevant, theoretical model of SM entails a systematic examination of developmental, familial, and sociocultural risk and protective factors. The ecocultural perspective provides an appropriate conceptual framework to understand the complexity of SM because it situates a child’s mental health problems within a rich theoretical framework that relates higher-level cultural factors with child-related factors (Super & Harkness, 1986; Worthman, 2010).
According to the ecological model (Bronfenbrenner, 1979, 1995), contexts of development are organized into various levels. The first level is related to child-related factors (e.g., age, sex, temperament, cognitive skills). The next level, the microsystem, contains relations between the individual and the immediate environment surrounding him or her. Such factors include the home, school, and workplace. The last two levels, the exosystem and the macrosystem, consist of more distal factors that can influence a child’s development, such as neighborhood and cultural influences. The exosystem embraces significant institutions of society, such as the world of work, the mass media, and public agencies. The macrosystem consists of the ideological and behavioral patterns of a particular culture or subculture and integrates the microsystem, the mesosystem, and the exosystem.
Research conducted on children with SM revealed several factors that may influence child behavior, both directly and indirectly. At the individual level, SM has been attributed to high levels of anxiety, language deficits, limited social skills, and behavioral problems. The most popular explanation for SM suggests that the presented symptoms represent a high level of anxiety, and in particular social anxiety (Cornacchio et al., 2019; Gensthaler et al., 2016). A recent meta-analysis found that 80% of the children with SM were diagnosed with an additional anxiety disorder (69% social phobia) (Driessen et al., 2019). Nevertheless, the precise nature of the relationship between SM and social anxiety is still insufficiently clear.
One possible association between the two disorders is that SM represents a more severe manifestation of social phobia (APA, 2013). Another possible association between SM and social anxiety is that mute behavior may compensate for or regulate increased anxiety levels (Scott & Beidel, 2011). According to the ‘unsafe model of SM’ (Melfsen et al., 2021), the nervous system of individuals with SM appraises the environment as being ‘unsafe’ even when it is ‘safe.’ As a result, their physiological state does not support social engagement behaviors. High sensory-processing sensitivity to unsafety lowers the threshold when the nervous system triggers an activation of dissociation or the freeze mode.
The behavioral theory offers a different explanation of SM based on negatively reinforced learning (Leonard & Topol, 1993). From this perspective, symptoms of SM may arise primarily as a means of anxiety avoidance in social situations (Young et al., 2012). More specifically, mutism may reduce social anxiety, and thus may be negatively reinforced through avoiding opportunities for social exchanges (Bergman, 2013; Conn & Coyne, 2014).
Alternatively, SM has been associated with neurodevelopmental vulnerabilities that may impact communication, memory, and language skills (Cohan et al., 2006; Yeganeh et al., 2006). Although SM cannot be solely explained by a communication disorder (APA, 2013), previous studies suggested that between 20% and 50% of the children with SM experience language delays and deficits, including problems with receptive vocabulary, phonemic awareness, receptive grammar, and conversational rules (Katz-Bernstein, 2013; Manassis et al., 2007).
Another explanation attributes SM symptoms to social skills deficits (Cunningham et al., 2004, 2006; Muris & Ollendick, 2015). For example, Carbone et al. (2010) found that children with SM displayed significantly lower levels of social assertion and verbal social skills as compared to mixed anxiety and non-clinical control children. Finally, SM was linked to externalizing problems, including controlling, demanding, oppositional, and aggressive behaviors (Diliberto & Kearney, 2016). It is not clear, however, whether the high prevalence of externalizing symptoms in children with SM truly reflects comorbidity or should be considered as symptomatology occurring in children who are exposed to anxiety-provoking situations (Bubier & Drabick, 2009; Drabick et al., 2010).
At the microsystem level, the literature has identified several parental and school risk factors for SM. Traditionally, SM has been associated with family dysfunction, such as divorce, abuse, and trauma (Hayden, 1980). More recent research, however, does not seem to support such a view (e.g., Black & Uhde, 1995; Chavira et al., 2007). Numerous studies found an association between parental psychiatric morbidity, mainly depression and anxiety, and a child’s SM (Capozzi et al., 2017; Remschmidt et al., 2001). There is also evidence to suggest that parents of children with SM appear to be significantly more controlling and overprotective, probably to regulate high levels of parent and child anxiety (Edison et al., 2011).
Higher levels of parental distress have been found to be related to parental accommodation to SM, suggesting that parental overprotection may reduce a child’s distress in the short term, but reinforce anxiety over the long term (Thompson-Hollands et al., 2014). Accommodation strategies include facilitating children’s anxiety-related avoidance, modifying family routines, providing excessive reassurance, and adhering to rigid child-assigned rules related to anxiety-provoking stimuli. All of these strategies have the potential to maintain anxiety and facilitate further avoidance (Krysanski, 2003; Lebowitz et al., 2012).
School is an extremely important setting for children with SM, being the context in which the majority of children with the disorder exhibit mutism, and often where the impairment is most severe (Shriver et al., 2011). The school context often involves very high anxiety levels as a result of constant performance demands, most of which are related to verbal communication (Crundwell, 2006). Research suggests that children with SM are more likely to have lower academic performance (Nowakowski et al., 2009), especially in cognitive nonverbal measurements (Manassis et al., 2007). A recent study also found that teachers have difficulties establishing an affective and close relationship with children affected by SM, compared to their unaffected peers (Longobardi et al., 2019).
School may be particularly stressful for culturally and linguistically diverse children, due to racial or ethnic discrimination, lack of class support for children learning a second language, the high linguistic and cognitive demand resulting from sudden immersion in a second language, and conflicted parent–school relationships (Toppelberg et al., 2005). Teachers’ awareness of SM may be beneficial toward prevention of the disorder, or to ameliorate its effects (Martinez et al., 2015). Teachers may assist children with SM by providing enough opportunities to speak (e.g., avoiding closed yes/no questions, calling on children rather than waiting for them to volunteer, waiting a few seconds for responses, creating small-group discussions), as well as by refraining from reinforcing nonverbal responding. On the other hand, teachers who do not provide enough opportunities to respond, create excessive anxiety in class, or give up the expectation for speaking may increase the risk for the development and maintenance of SM (Busse & Downey, 2011).
Like most areas in developmental psychology research (Arnett, 2016), the effects of the ecosystem and the macrosystem on SM are rarely addressed. However, previous studies predicting a child’s behavior problems may provide several directions for examining SM in context. At the exosystemic level, low socioeconomic status (e.g., Zilanawala et al., 2015) and immigration history (Breslau et al., 2009) were identified as risk factors for a child’s behavioral problems. At the macrosystem level, parental acculturation difficulties (Calzada et al., 2009; Goforth et al., 2015), illegal status (Landale et al., 2015), and perceived discrimination (Cooke et al., 2014) were associated with increased likelihood of behavior problems.
SM in immigrant children
Increasing evidence suggests that immigrant and language/culture-diverse children are more likely to be diagnosed with SM than the general population (Cohan et al., 2008; Elizur & Perednik, 2003). For example, a community-based Israeli study that examined SM prevalence and correlates in immigrant and native children (Elizur & Perednik, 2003) found a prevalence rate four times higher in immigrant, bilingual children (2.2%) compared with native, monolingual children (0.47%). In another sample of children with SM, 28 of 100 diagnosed youngsters from Switzerland and Germany were immigrants (Steinhausen & Juzi, 1996).
Diagnosing SM in culturally and linguistically diverse children is a complex task because many children acquiring a second language may undergo a ‘silent period.’ While the DSM-based diagnosis of SM precludes diagnosing in immigrant children with limited language proficiency, it is not clear how much proficiency is required to fulfill this criterion. Most children learning a second language will not feel entirely comfortable in the second language in six or more months. Yet, this period greatly varies as a function of personality and temperament factors, particularly the level of anxiety in unfamiliar contexts (Tabors, 1997). Moreover, immigration itself is associated with social withdrawal and anxious or avoidant behaviors (Ash et al., 2014). Given that cultural adaptation and language acquisition take a long time, it is difficult to ascertain whether children’s silence reflects limited language proficiency or high levels of anxiety (Leacox et al., 2016). Support for the central role of anxiety in the development of SM in immigrant children may be found in a recent study by Starke (2018). This study found that the child’s ability to speak the mainstream language increased over time, regardless of his or her bilingual status, socio-economic status (SES), or receptive language skills. Anxiety, however, was significantly associated with the development of mute behavior.
To date, only two SM studies (Elizur & Perednik, 2003; Starke, 2018) examined culturally and linguistically diverse children separately from the dominant group. While these studies support the view that bilingualism and minority status might be associated with SM diagnosis, it remains unclear how migration history, ethnic identity, potential discrimination, second-language acquisition, and acculturation processes interact to produce and maintain SM in immigrant children (Toppelberg et al., 2005; Viana et al., 2009).
The current study
Although evidence suggests that immigrant and language/culture-minority children might be overrepresented among children with SM diagnosis, a direct examination of how migration or bilingual status is associated with SM is still scarce. Moreover, as most research in child development has overlooked the effects of culture and context (Arnett, 2016), little is known about the similarities and differences in the risk factors for SM in immigrant and non-immigrant children.
Guided by ecocultural models of development (Bronfenbrenner, 1979; Weisner, 2002), the current study aimed to construct a theory-based description of SM, addressing individual, family, and contextual levels of development. One compelling strategy to analyze data of ecological models is to assess paths of mediation. This model is based on the idea that factors can influence children’s behavior not only directly, but also through their influence on other variables that are directly related to children’s mental health. Evidence suggests that several risk factors may act as mediators between an immigration background and children’s development, including parenting practices (Glick et al., 2012), social support (Atzaba-Poria & Pike, 2005), and marital relationships (Gonzales et al., 2000). Another method to analyze the data of ecological models is to test for moderation effects. While only a few studies have examined moderation effects in the link between immigration background and children’s mental health, studies in various cultural settings have suggested that aspects of the environment, such as SES, cultural values, ethnic identity, and acculturation, may moderate the effects of risk factors on mental health outcomes (Bauer et al., 2020; Reiss et al., 2019).
The present study focuses on SM in Israeli immigrant and non-immigrant children. Israel is a multi-cultural country which actively supports the absorption of immigrants. Clear cultural and ethnic differences in everyday practices and in the utilization of health care (Kerub et al., 2021) make the Israeli context an interesting case for exploring the effects of immigration, bilingualism, and socio-cultural factors (and their interactions) on the development of SM. Since Israel's establishment as a State, about 3.3 million immigrants immigrated to Israel, 44.3% of whom immigrated from 1990 onwards. Immigrants from the former Soviet Union comprise the largest group of immigrants (forming 20% of the Jewish population), followed by immigrants from Eastern Europe (Romania and Poland) and North Africa (Morocco, Algeria, and Tunisia) (Central Bureau of Statistics, 2021). Group differences in social capital, educational level, acculturation, and segregation may be relevant to the development and persistence of SM. For example, immigrants from the former Soviet Union emphasize the importance of higher education as a means of social mobility (Prashizky & Remennick, 2015; Rapoport & Lomsky-Feder, 2002), surpassing immigrants from other origins and on many levels merging with the Ashkenazi middle class (Lerner et al., 2007). At the same time, they are considered to be a more segregated group in terms of language and culture (Al-Haj, 2004; Remennick, 2004).
Based on the previous studies, the current study was directed by three hypotheses: (1) immigration background and bilingual status would increase the likelihood of SM diagnosis, (2) parental risk factors (parenting style and parental accommodation to SM symptoms) would mediate the association between an immigration background and the child’s level of SM symptoms, and (3) contextual risk factors, such as bilingual status and family income, would moderate the association between an immigration background and the child’s level of SM symptoms. Figures 1 and 2 present the study's theoretical mediation and moderation models, respectively.
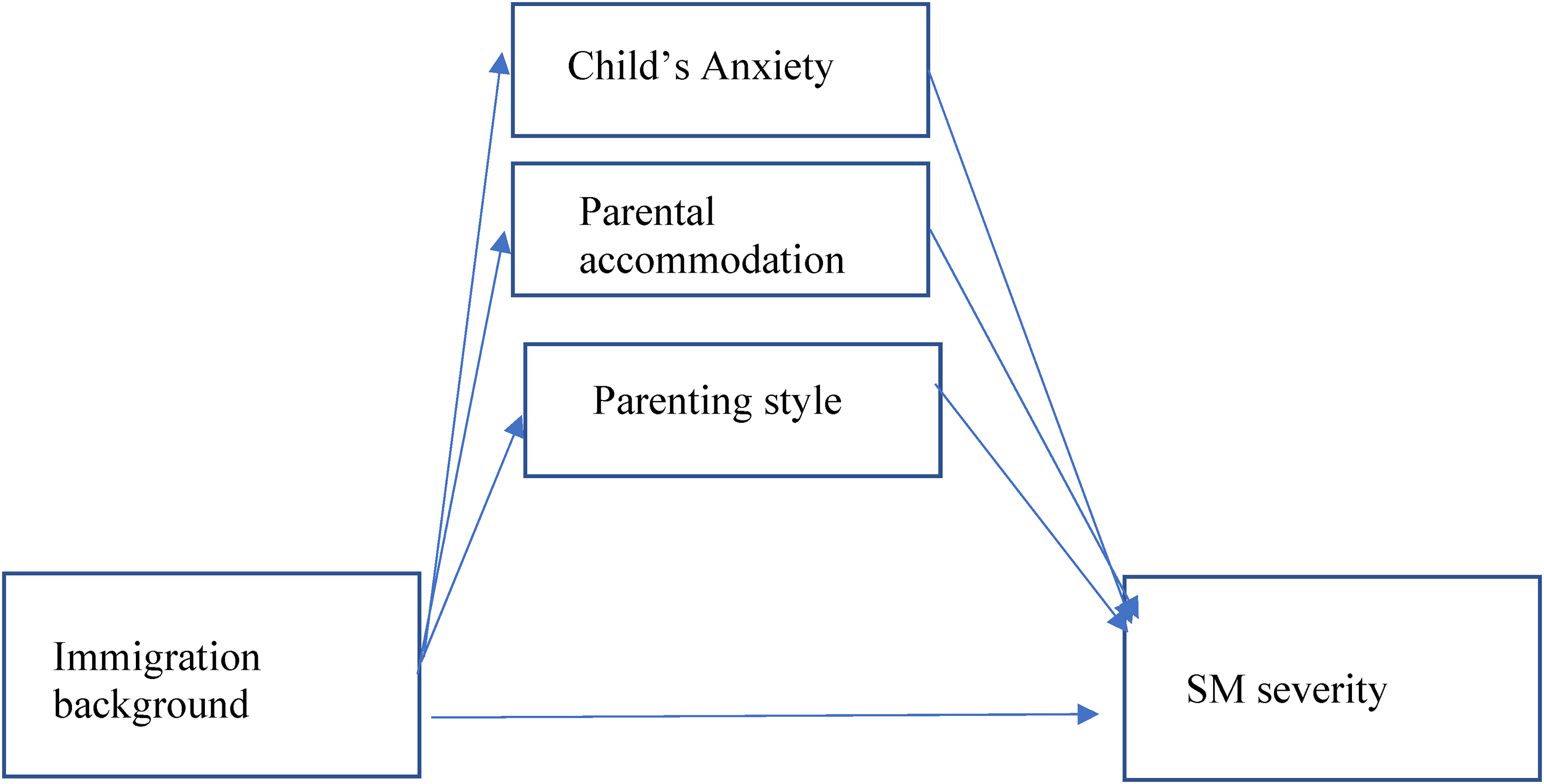
The study hypothesized mediation model.
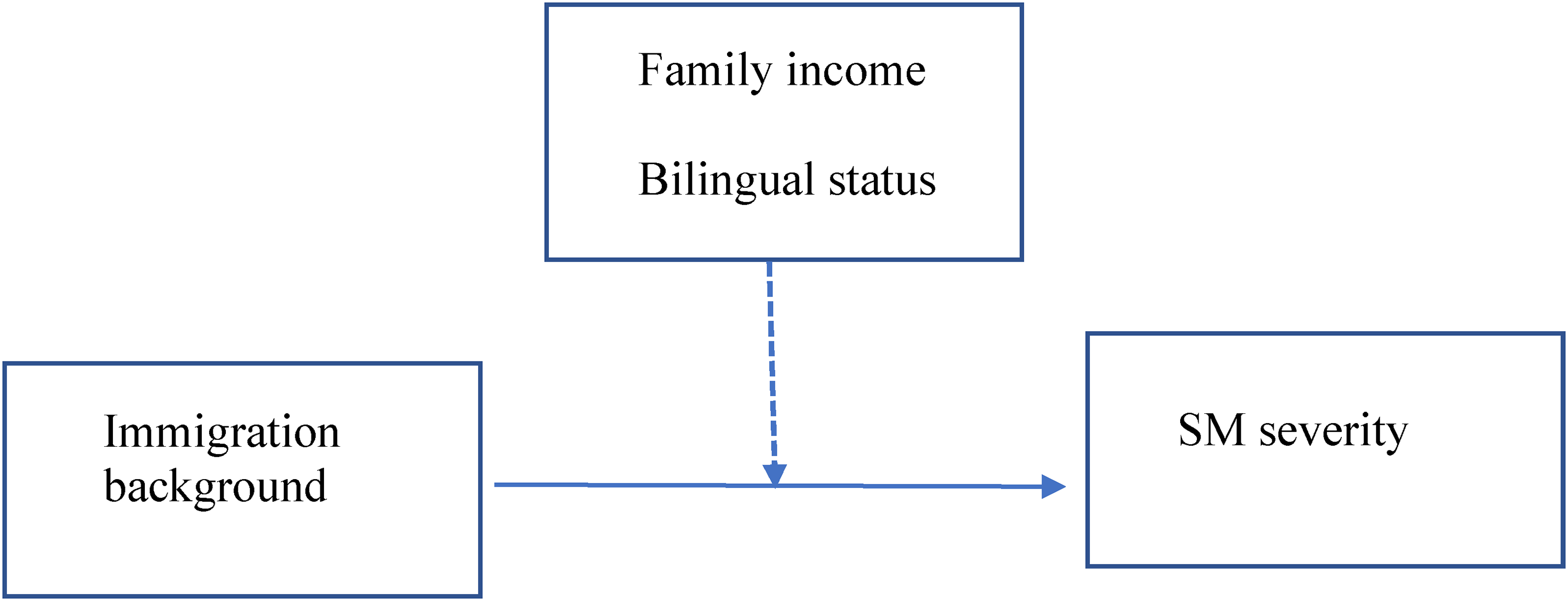
The study hypothesized moderation model.
Method
Participants and procedure
Participants were 325 Israeli children and their parents. Children’s ages ranged between 3 and 8.5 years (mean = 5.21, SD = 1.04, 54.5% females). Of the total sample, 78 children were diagnosed with SM (38.4% with an immigration background, n = 30), and 247 were typically developed children (18.2% with an immigration background, n = 45). All parents reported being heterosexual and most of them (93.5%) reported being married. About a third of the parents (34.2% of the fathers and 34.5% of the mothers) were first-generation immigrants, primarily from the former Soviet Union (9.8% of the fathers and 11.6% of the mothers). Children were mostly native-born (97%). Fathers’ and mothers’ mean levels of education were 15.96 years (S.D = 3.08) and 17.12 years (S.D = 6.78), respectively.
Participants in the SM group were clinic-referred children recruited from an out-patient psychiatric clinic at the Schneider Children’s Medical Center of Israel. The clinic specializes in the diagnosis and treatment of SM and serves a heterogeneous population in terms of ethnicity, SES, and religiosity. Families were approached during their first visit to the clinic. Participation was voluntary and independent of the child’s treatment. All participants in the SM group met the criteria for SM, according to DSM-5 (APA, 2013), as assessed by a certified clinical psychologist. Exclusion criteria for the SM group included diagnoses of psychosis, autistic spectrum disorders, or mental disability, and pharmaceutical treatment for anxiety that started within 2–6 weeks before participation in the study. Participants in the control group were approached through e-mails, social media, and online groups.
The inclusion criterion for participation in the control group was an absence of academic or behavioral problems based on parents’ reports. All families had lived in Israel for at least five years before the study. In both study groups, the parent who was identified as the primary caregiver completed online questionnaires (using Qualtrics software), assessing the child’s and parent's variables. All participants agreed to participate in the study, and both of their parents provided written informed consent to the study, approved by the institutional ethics committee.
Measures
All measures were reliable and validated scales and were available in Hebrew as well as in the parent's dominant language (e.g., Russian, English, Arabic).
Background variables included the child’s age, sex, school, medication, place of birth, number of siblings, parents’ education, family income, and number of spoken languages.
Children with an immigration background were defined as children with at least one first-generation immigrant parent.
Diagnostic status. The Anxiety Disorders Interview Schedule for DSM-IV, Parent Version (ADIS-P; Silverman & Albano, 1996), was used in the SM group to assess and confirm diagnostic status, including anxiety, mood, and externalizing behavior disorders. The ADIS-P has good test-retest reliability (k = 0.65–0.88) (Silverman et al., 2001), good interrater reliability (k = .90) (Lyneham et al., 2007), and good convergent validity (Wood et al., 2002). The ADIS-P has also demonstrated sensitivity to treatment effects in studies of adolescents with anxiety disorders (Kendall et al., 1997; Walkup et al., 2008). A clinical severity rating of 4 on a 0–8 scale is indicative of a clinically significant disorder and was required for an SM diagnosis.
The severity of SM symptoms was assessed by the 17-item Selective Mutism Questionnaire (SMQ; Bergman et al., 2008). The SMQ assesses the degree of a child’s speech inhibition in various situations. The SMQ includes 17 statements describing typical situations in which children are expected to speak (e.g., “When called on by his/her teacher, my child would answer”), spanning three domains: “at school” (five items), “with family” (five items), and “in social situations” (seven items). Three overall interference and distress questions supplement the situational statements (e.g., “Overall, how much did not talking interfere with daily living for your child?”). Parents are asked to rate the frequency of each item, using a four-point scale. The Cronbach's α in the current study was .85 in the SM group, and .88 in the control group.
Social anxiety was assessed with the Social Anxiety Scale for Children-Revised (SASC-P; Parent version). This is an 18-item questionnaire for social anxiety that has demonstrated reliability and validity (Bergman et al., 2013; La Greca & Stone, 1993). In this study, the SASC was completed by parents. Each item can be answered using a five-point Likert-type scale. The scale is composed of three subscales: Fear of Negative Evaluation (eight items), Social Avoidance and Distress-New Situations (six items), and General Social Avoidance and Distress (four items). Higher scores reflect greater anxiety. Sample items include “My child feels shy around kids he/she doesn’t know” and “My child is quiet when he/she is with a group of kids.” In the current study, the internal consistency of the SASC-P was Cronbach's α = .86 in the SM group and α = .87 in the control group.
The Family Accommodation Scale–Anxiety (FASA; Lebowitz et al., 2013) includes nine items that query the frequency of participation in child symptoms (five items) and modification of schedules and routines (four items). Items are rated from 0 (never) to 4 (daily). FASA has good internal consistency (α = .9), as well as convergent and divergent validity (Lebowitz et al., 2013). Sample items include “Have you modified your family routine because of your child’s symptoms?” and “Has your child become distressed when you have not provided assistance? To what degree?” In the current study, the internal consistency of the FASA was α = .84 in the SM group, and α = .80 in the control group.
The Parental Authority Questionnaire (PAQ; Buri, 1991) was used to assess parents’ authority style. It consists of a 30-item self-report questionnaire assessing levels of parents’ authoritativeness, authority, and permissiveness. Each item is rated on a five-point scale. The PAQ has good psychometric properties (Buri, 1991). Sample items include “I often tell my children exactly what I want them to do and how I expect them to do it” (authoritarian parenting), “I take my children’s opinions into consideration when making family decisions, but I don’t decide on something simply because my children want it” (authoritative parenting), and “I do what children in the family want when making family decisions” (permissive parenting). In the current study, the permissive scale had Cronbach's α = .66 in the SM group and α = .70 in the control group, the authoritarian scale had Cronbach's α = .83 in the SM group and α = .79 in the control group, and the authoritative scale had Cronbach's α = .77 in the SM group and α = .79 in the control group.
Data analysis
Preliminary analysis was performed to detect univariate and multivariate outliers and nonnormal distributions. No outlier was detected. The listwise deletion strategy was used in case of missing values (Kang, 2013). The roles of immigration background and bilingual status as risk factors for SM diagnosis were examined by logistic regression while controlling for a child’s age, sex, parental education level, and family income. Next, we examined the role of bilingual status in predicting SM diagnosis in immigrant children using logistic regression, with the child’s age, sex, parental education level, and family income as control variables. Next, a Pearson correlation matrix was used to identify associations between the main study variables.
To test the mediational model of the child’s anxiety, parental accommodation, and parenting style as parallel mediators of the relationship between immigration background and the level of SM symptoms, we used Model 4 in PROCESS (Hayes, 2013). PROCESS estimates indirect effects using bootstrap confidence intervals. In these analyses, mediation is significant if the 95% bias-corrected and accelerated confidence intervals (lower limit, LL), the upper limit (UL) for the indirect effect, do not include 0. Finally, to test the moderating roles of family income and bilingual status in the association between immigration background and the level of SM symptoms, we used Model 2 in PROCESS (Hayes & Matthes, 2009). The sample size provided adequate power to detect a medium effect size in multiple regressions, using a two-tailed test, with 8+ predictors, α = .05, and power = .80 (Cohen, 1992).
Results
Immigration and bilingual status as risk factors for SM diagnosis
Results of the logistic regression in predicting the presence of SM while controlling for the child’s age, sex, parental education level, and family income are presented in Table 1.
Logistic regression predicting SM diagnosis (n = 233).
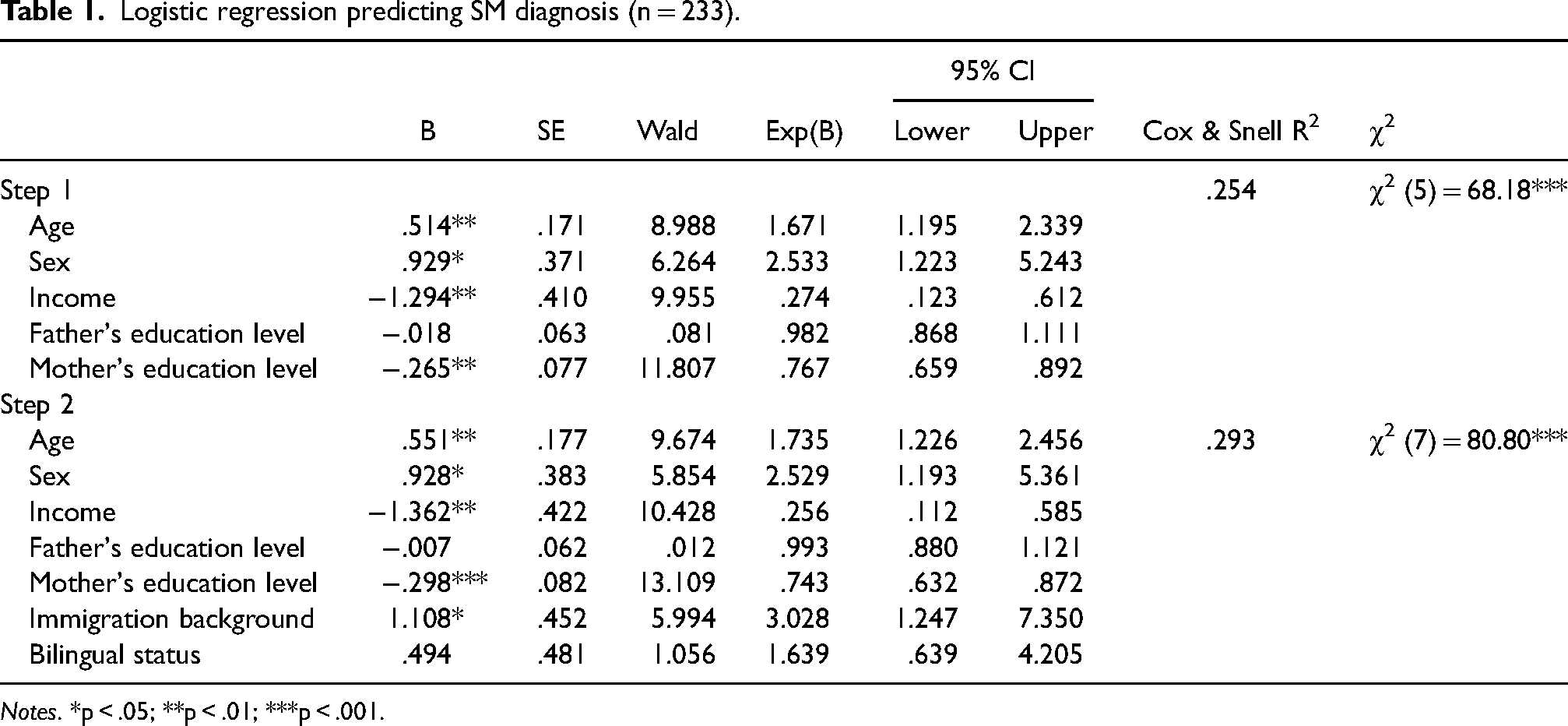
Notes. *p < .05; **p < .01; ***p < .001.
As seen in the table, older age, female sex, lower family income, and lower mother's education level increased the risk for SM diagnosis. Immigration background increased the risk for SM diagnosis even after controlling for the demographic variables. Children with an immigration background had a 3.028 higher odds ratio of SM diagnosis (95% confidence interval 1.247–7.350) than children without such a background. Table 2 presents the results of the logistic regression predicting the presence of SM in immigrant children only. Results showed that in immigrant children, older age and having a bilingual status were identified as risk factors for SM diagnosis. Among children with an immigration background, those having a bilingual status had a 10.375 odds ratio of SM diagnosis than monolingual children (95% confidence interval 2.457–43.819).
Logistic regression predicting SM diagnosis in immigrant children (N = 64).
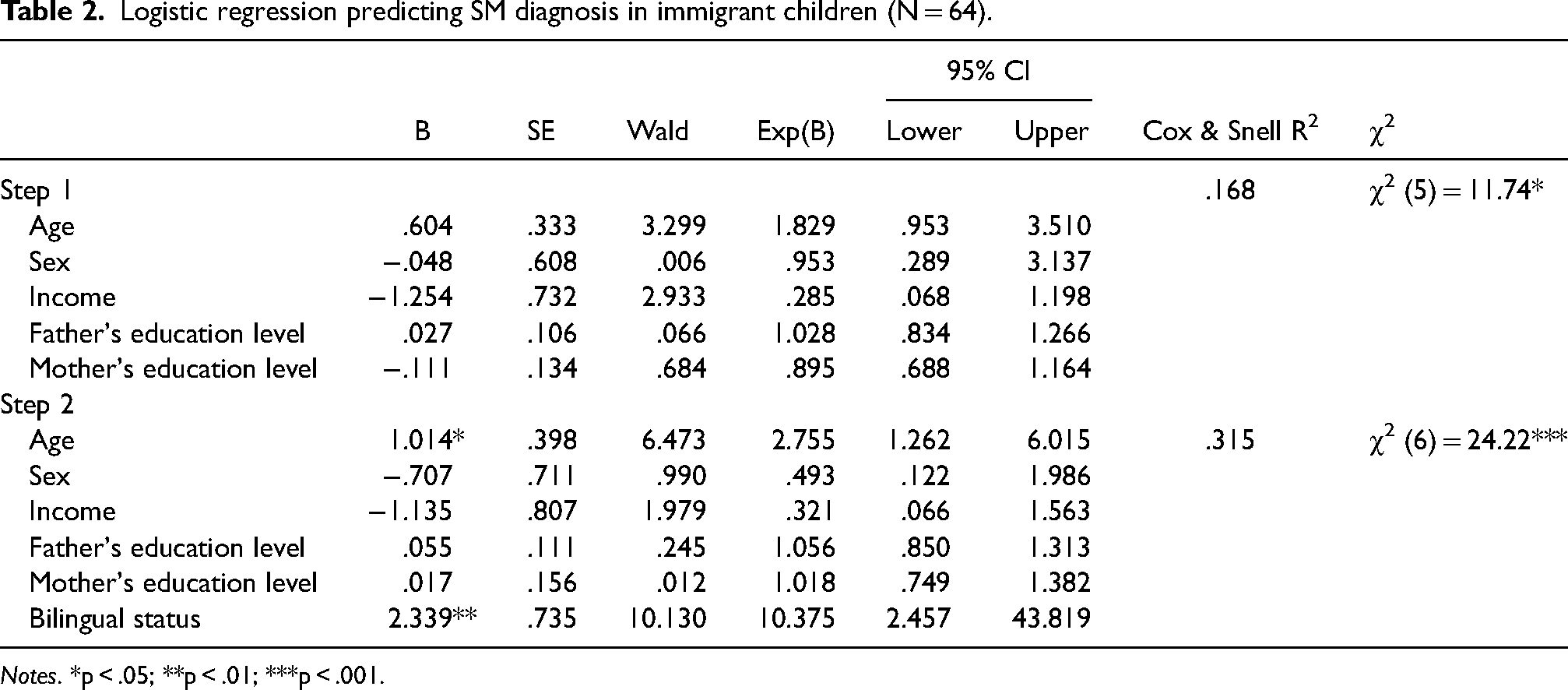
Notes. *p < .05; **p < .01; ***p < .001.
Testing the mediating roles of child and family variables in the relationship between immigration background and the level of SM symptoms
Pearson correlation coefficients are presented in Table 3. As can be obtained from the table, the level of SM symptoms was positively correlated with the child’s age (r = .336, p < .01), immigrant background (r = .139, p < .05), anxiety level (r = .668, p < .01), parental accommodation level (r = .518, p < .01), and with more permissive parenting practices (r = .136, p < .05). SM symptoms were negatively correlated with family income (r = −.270, p < .01) and with authoritative parenting practices (r = −.292, p < .01). However, bilingual status was not associated with the level of SM symptoms.
Correlation matrix between study variables.
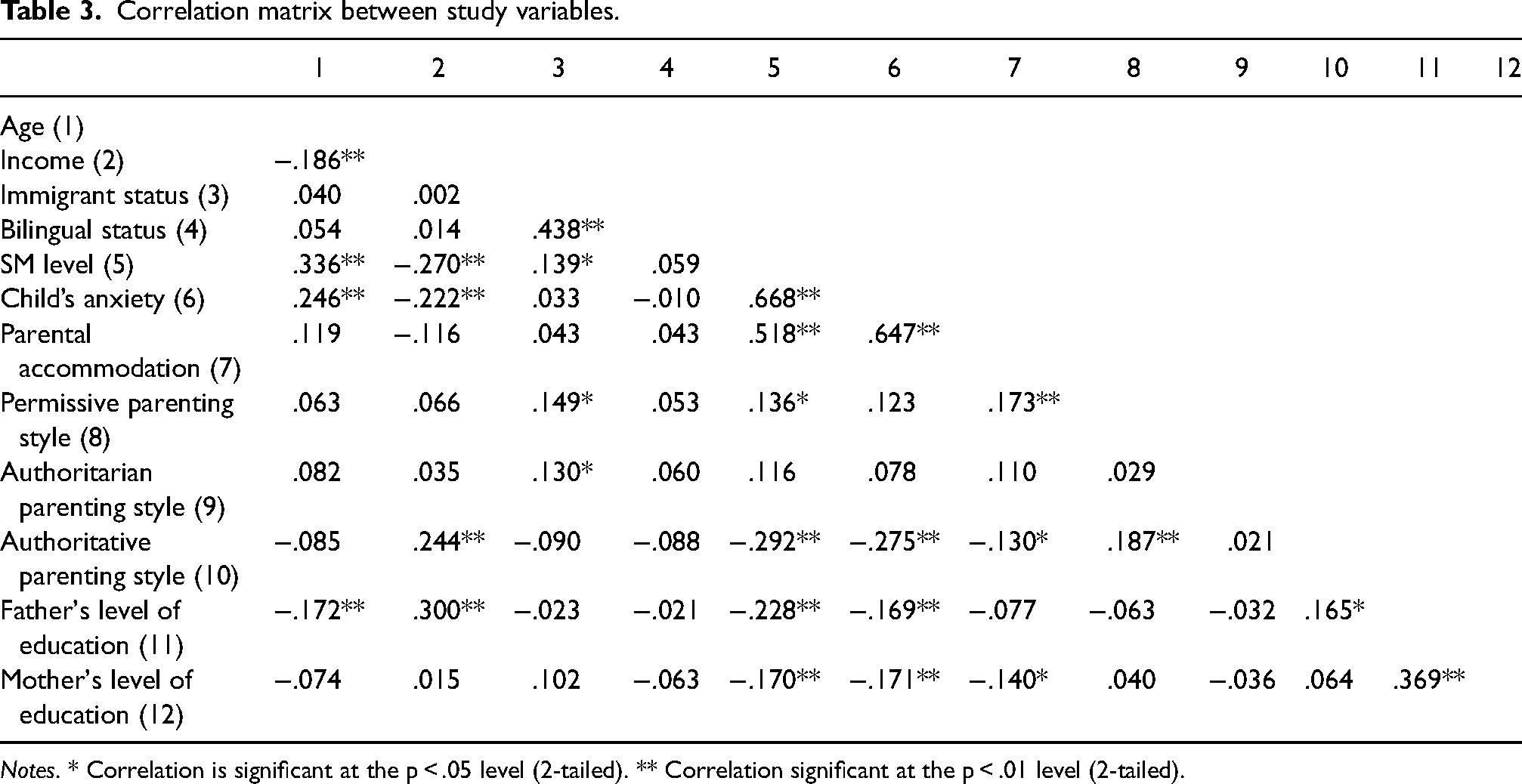
Notes. * Correlation is significant at the p < .05 level (2-tailed). ** Correlation significant at the p < .01 level (2-tailed).
Next, we examined the mediating role of child and parental risk factors in the relationship between immigration background and the level of SM symptoms, using Process macro (Hayes, 2013). We created a parallel multiple mediation model (Hayes, 2013) using a child’s anxiety, parenting styles (permissive and authoritative), and parental accommodation as mediators. Sex, age, parental level of education, and family income were controlled throughout these analyses. Table 4 presents direct and indirect effects between immigration background and SM. Results showed that the model was significant, F (10,193) = 26.33, p < 0.001, accounting for 57.7% of the variance in SM symptoms. Having an immigration background, older age, lower family income, and increased levels of child’s anxiety and parental accommodation predicted higher levels of SM symptoms. The indirect effects of the child’s anxiety, parenting styles (permissive and authoritative), and parental accommodation were statistically insignificant.
Parallel mediation analysis to identify direct and indirect effects between immigration background and the level of SM symptoms (N = 204).
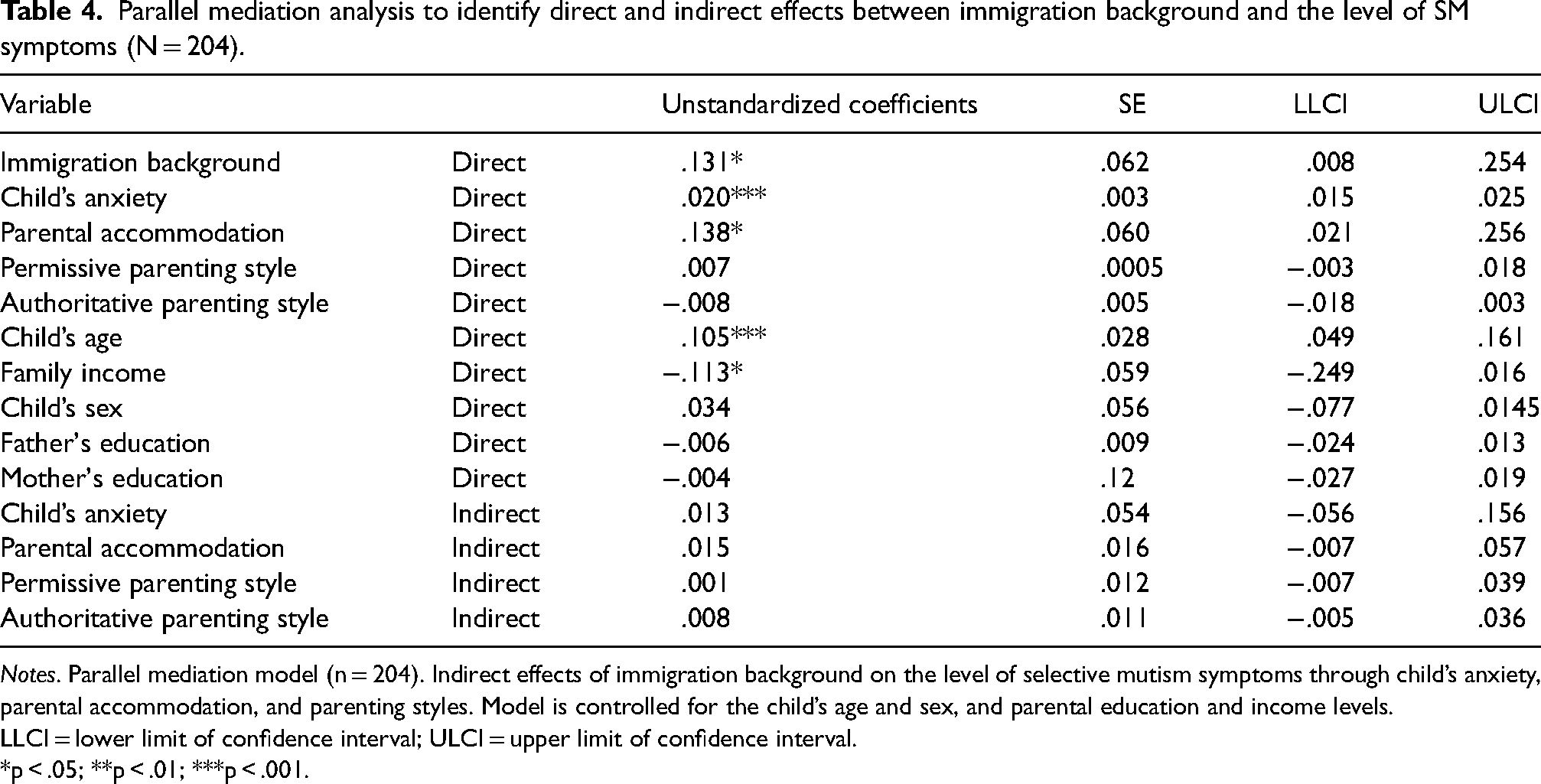
Notes. Parallel mediation model (n = 204). Indirect effects of immigration background on the level of selective mutism symptoms through child’s anxiety, parental accommodation, and parenting styles. Model is controlled for the child’s age and sex, and parental education and income levels.
LLCI = lower limit of confidence interval; ULCI = upper limit of confidence interval.
*p < .05; **p < .01; ***p < .001.
Testing the moderating effects of bilingual status and family income in the relationship between immigration background and the level of SM symptoms
Results showed that the model was significant, F (9,219) = 9.43, p < .001, accounting for 27.9% of the variance in SM. Income, bilingual status, and the child’s age had main effects on SM (B = −.018, SE = 0.08, p < .05; B = −.38, SE = 0.14, p = 0.007, and B = 0.15, SE = 0.03, p < .001, respectively). The product term of the interaction between immigration background and bilingual status was significant (B = .56, SE = 0.19, p = .004), indicating that bilingual status moderated the link between immigration background and SM. This product term explained 2.7% of the variance in the dependent variable (level of SM symptoms). The product term of interaction between immigration background and family income was insignificant (B = −.12, SE = 0.11, p = .499). This product term explained 1.5% of the variance in the dependent variable (level of SM symptoms). However, the three-way interaction between immigration background, bilingual status, and family income was significant (p < .001). This product term explained 3.1% of the variance in the dependent variable (level of SM symptoms). Post-hoc probing of the three-way interaction (immigration, bilingual status, and income) revealed that for all income levels, bilingual status, but not monolingual status, interacted with immigration background to increase the level of SM symptoms (low income: B = .68, SE = 0.18, p < .001; medium income; B = .62, SE = 0.16, p < .001; high income; B = .56, SE = 0.19, p = .003). Figure 3 displays the interaction plot for the association between immigration background and SM symptoms under the condition of low (−1 SD), medium (0 SD), and high (+1 SD) levels of family income. As seen in the figure, bilingualism increased the level of SM only in immigrant families. The relationship between bilingualism and immigration became weaker with the increase in family income.
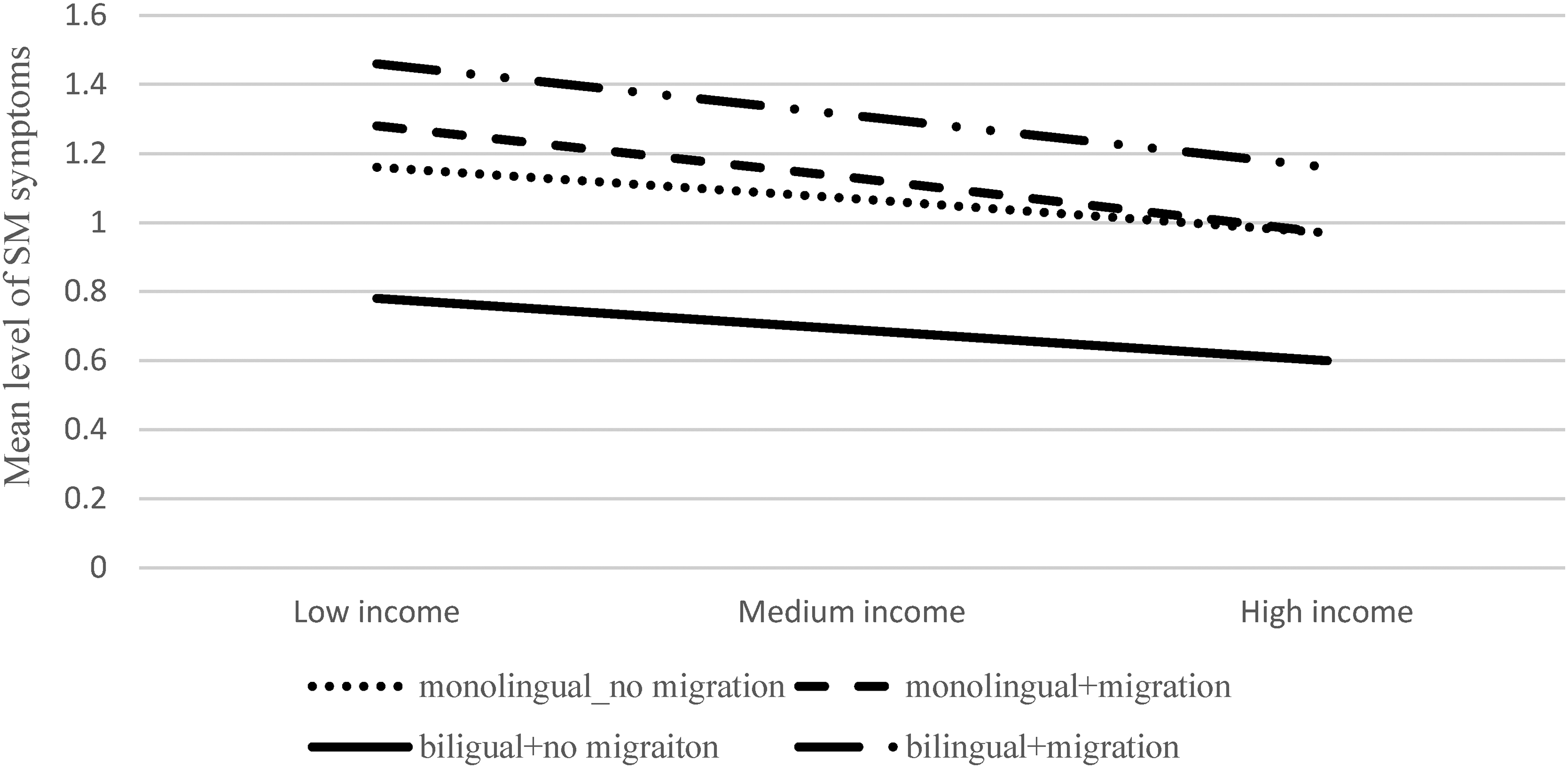
The three-way interaction effect of immigration background, bilingual status, and family income on the level of SM symptoms. Low income = −1 SD, medium income = 0 SD, high income = +1 SD.
Discussion
Previous studies have pointed to a surprisingly high prevalence of SM in immigrant children (Elizur & Perednik, 2003; Steinhausen & Juzi, 1996). However, a systematic examination of the link between immigration status and the development and persistence of SM is still scarce. The current study aimed to construct a theory-based description of SM in immigrant children while considering individual, family, and contextual risk factors.
In line with previous studies (Elizur & Perednik, 2003; Toppelberg et al., 2005), our results support the view that children with an immigrant background are overrepresented among children with SM. Although the vast majority of the children in the current sample were native-born, and all families had lived enough time in the host country to acquire a minimal level of language proficiency, having a first-generation immigrant parent was associated with an increased risk for SM diagnosis. This finding was consistent even after controlling for the effects of the child’s age, sex, parental education level, and family income.
To provide more insight into the link between immigration background and SM, we examined the mediating roles of child and family variables in this relationship. We found that after controlling for the child’s age, sex, parental education level, and family income, the child’s anxiety level and parental accommodation had positive direct effects on the level of SM symptoms. However, the child’s anxiety, parenting styles (permissive and authoritative), and parental accommodation did not mediate the relationship between immigration background and SM. These findings provide further support for the association between SM and social anxiety (Driessen et al., 2019, for meta-analysis). The only study that examined the role of anxiety in the development of SM in bilingual children revealed that anxiety would be the largest factor influencing the development of SM in both monolingual and bilingual children (Starke, 2018). Consistent with this view, our results suggest that anxiety was the most important predictor of SM symptoms, above and beyond immigration background. Further, our results pointed to a moderating effect of bilingual status and its interaction with family income on the level of SM symptoms. Specifically, we found that bilingualism increased the level of SM symptoms, only in children of immigrant families. In fact, native-born children who spoke more than one language were less likely to suffer from SM than native-born children who spoke only one language. Consistent with other studies focusing on general language development (Byers-Heinlein & Lew-Williams, 2013) or SM specifically (Starke, 2018), our findings indicated that bilingualism per se cannot explain the supposedly higher vulnerability to SM of immigrant children. Possibly, the children’s proficiency in multiple languages on its own does not inhibit their speech in social situations, but rather other culturally related values and norms that may limit opportunities to respond and practice the mainstream language (Baker, 2007; Chumak-Horbatsch, 2008).
Previous studies of early bilingualism, which attempt to explain and predict the nature of young children’s dual language behaviors, have emphasized the importance of considering parental language attitudes (De Houwer, 1999; King, 2000). These attitudes directly affect their linguistic practice and their interactional strategies, including how they choose to respond to children’s conversation contributions. Immigrant parents wishing to integrate into the new society may encourage children’s proficiency in the dominant language, sometimes at the expense of maintaining the heritage language (Kolancali & Melhuish, 2023). Other parents, on the other hand, may be focused on securing cultural identity by emphasizing the heritage culture (Farruggio, 2010; Guardado, 2002). Some parents, therefore, may delay children’s exposure to the new culture or restrict their access to the dominant language (Chumak-Horbatsch, 2006). Notably, the causal relationship between language attitudes and SM is bidirectional, so that children’s anxiety and mute behavior negatively influence parents’ perceived integration into the mainstream culture (Starke, 2018). Thus, it is necessary for future studies to consider parental language attitudes as a possible underlying mechanism of the link between immigration background and SM symptoms.
Examining the three-way interaction effect (immigration background * bilingual status * income) on SM showed that the relationship between bilingualism and immigration became weaker with the increase in family income. In other words, the exacerbating effect of bilingualism on SM in immigrant children was attenuated by higher income. It is possible that the cumulative effects of poverty, limited parental ability to mediate language and culture, and parental migration stress place young immigrant children at risk for SM diagnosis (Shany et al., 2010). In contrast, bilingualism in native-born children may represent sufficient financial resources to support the acquisition of a second language.
While our findings are consistent with previous studies documenting the high risk for SM in immigrant children, the literature has warned against overdiagnosis of the disorder in this population.
Learning a second language takes the average immigrant child a long time. Therefore, it is often unclear whether the child with SM symptoms has achieved the right level of linguistic knowledge or familiarity to qualify for such a diagnosis. The risk for SM overdiagnosis is particularly increased in young children (3- to 8-year-olds), who present longer silent periods (Tabors, 1997). Moreover, personality and temperament factors influence the duration and the magnitude of the silent period. Behavioral inhibition, for example, may characterize several SM features that link SM and social phobia (Dummit et al., 1997; Steinhausen & Juzi, 1996). Thus, shy, anxious, or inhibited children expected to function in a second, unfamiliar language may be more prone to reacting with mutism. Toppelberg et al. (2005) emphasized that in contrast to typically developed children who usually present with mutism in one language, in one or two settings, and for only a few months, children with SM present with mutism in both languages, in several unfamiliar settings, and for significant periods.
Limitations
The findings should be considered in relation to several limitations. The first limitation, which is common to most studies of SM, is the high overlap between immigration and bilingual status. Such confounding is difficult to avoid in countries where bilingualism is associated with immigrants and their descendants (Bialystok et al., 2016; Paap & Greenberg, 2013), or where bi- and monolingual participants are recruited from different parts of the same country (Antón et al., 2014). In such cases, both groups might differ not only in language but also in other important variables such as social structure, SES, and education (Cox et al., 2016). Distinguishing bilingualism from immigrant backgrounds allowed us to separately examine their role in SM. However, since the number of bilingual children in the non-immigrant group was limited (n = 18), it was impossible to draw firm conclusions about the different effects of these two variables or their interaction. One strategy of addressing the confound between immigration and bilingual status is to investigate SM in countries in which knowledge of different languages is not necessarily connected to immigrant status (Bak & Alladi, 2016; Woumans et al., 2015).
The second limitation is related to the reliability and validity of SM diagnosis, which was based on clinical assessment and supported by parental reports. While the reliability and validity of the ADIS-P (Silverman & Albano, 1996) are well established in clinical settings (Bergman et al., 2013; Cohan et al., 2008), no interrater reliability of SM diagnosis was examined in our study. Given the complexity of diagnosing SM in immigrant children, further validation of the diagnosis by an independent clinician may contribute to accurate diagnosis and treatment. Also, we have no information about the age of onset of SM symptoms. Considering the age of onset is important not only as a control variable but also for the purpose of differential diagnosis (Mulligan et al., 2015). Several researchers have suggested that SM is a developmental subtype of social anxiety disorder, with earlier onset than other symptoms of the disorder (Bergman et al., 2002). Thus, early identification of SM may help professionals to intervene earlier with the treatment of social anxiety disorder symptoms (Black & Uhde, 1995; Ford et al., 1998).
Third, the current study did not examine the different faces of bilingualism that might have different effects of SM, including the age of second-language acquisition, the level of exposure to a second language, and the levels of proficiency in both languages (Marini et al., 2019; Paradis et al., 2011). Fourth, the exclusive reliance on parents’ self-report measures may cause problems of shared method variance, such that the associations obtained between the child’s anxiety, SM, parental accommodation, and parenting practices may become artificially inflated. Future research should include more objective assessments to measure some of the constructs or to include multi-informant measurement (e.g., clinician observation, school report, etc.). It is worth noting that although the three socio-cultural risk factors addressed in this study (i.e., immigration background, bilingual status, and family income) and their interactions explained a relatively small proportion of the variance in SM symptoms, their clinical value in assessing and treating SM in culturally and linguistically diverse children may still be significant. Expanding our understanding of SM to larger circles in children’s lives, including social, cultural, and political influences, may shed important light on how children’s and parents’ psychological, physiological, and psychiatric risk factors for SM vary in different socio-cultural contexts.
Finally, the current study included primarily immigrants from the former Soviet Union and did not distinguish immigrants from different origins and ethnicities. Therefore, future studies should consider how various levels of acculturation, stigma, and discrimination are related to parental accommodation and children’s anxiety. Given that SM is a childhood disorder, it is also essential to consider the cultural practices of classroom talk. Previous studies in different sociocultural contexts pointed to large heterogeneity in the extent to which classroom talk is allowed or encouraged (Inagaki et al., 1998; Xu & Clarke, 2019). In Western classrooms which tend to perceive speech as conducive to learning (Lyle, 2008), children’s silence may often be perceived as problematic (Nakane, 2007). However, Eastern educators perceive silence as a sign of attentiveness, sincerity, and trustfulness (Kim & Markus, 2002). Therefore, Eastern classrooms are much more dominated by students’ listening (Lee & Sriraman, 2013; Xu & Clarke, 2013). This cultural variance in how silence and talk are accepted and reinforced may play a crucial role in the identification or treatment of SM symptoms, as well as in parental accommodation practices (Alrabiah, 2017; Slobodin, 2023).
Conclusion
As Dowdy et al. (2011) noted, young children learning a second language are one of the fastest-growing segments of the global population. Consistent with previous studies, our results suggest that anxiety was the most important predictor of SM symptoms, above and beyond immigration background. Immigration, especially if coupled with bilingual status and low family income, predicted increased levels of SM symptoms. These results may encourage an early investment of public resources in facilitating mainstream language acquisition in immigrant children and their families. Schools can often provide an ideal setting to access these families because they are often one of the earlier institutions to be introduced in the new country (Slobodin & de Jong, 2015). Identification of the individual, family, school, and sociocultural mechanisms underlying mental health problems would help guide the development of personalized treatment strategies that might produce superior treatment outcomes (Compton et al., 2014).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.