
Abstract
Low- and middle-income countries (LMICs) carry a significant proportion of the global burden of untreated mental health disorders. Peer-delivered programs offer LMICs with limited mental health professionals an opportunity to increase mental health service access. This study describes the process of adapting a lay-worker-delivered evidence-based youth mental health intervention to a peer-delivery model in Sierra Leone using participatory methods. We convened Youth Community Advisory Boards (YCABs) as partners to develop a peer-delivery model for an evidence-based intervention. In collaboration with YCABs, the Assessment, Decision, Administration, Production, Topical experts, Integration, Training, Testing (ADAPT-ITT) framework was applied to guide the adaptation. The ADAPT-ITT framework is an eight-step process to adapt evidence-based interventions. The ADAPT-ITT framework facilitated the adaptation of the Youth Readiness Intervention (YRI), an evidence-based mental health program intervention that has been delivered by adult lay-workers to the youth peer-delivery platform in Sierra Leone. The YCABs identified program modifications, including the incorporation of storytelling, refinement of metaphors, and alterations to make delivery more accessible to low-literacy youth with particular attention to gender. YCABs also provided recommendations on how to support youth facilitators in providing psychosocial support, emphasizing self-care and boundary setting to ensure high-quality intervention delivery and do-no-harm principles. Study findings suggest that the ADAPT-ITT framework can be feasibly applied to guide the intervention adaptation process in LMICs. The use of participatory methods generated modifications that reflected youth experiences, needs, and concerns as facilitators and participants. Next steps include refinement and pilot testing of the adapted intervention.
Keywords
Introduction
Mental health disorders are currently the leading cause of disability among youth and are projected to be the top contributor to global disability by 2030 (Gore et al., 2011; Mokdad et al., 2016; Vos et al., 2020). Low- and middle-income countries (LMICs) carry a large proportion of the global burden of untreated mental health disorders, with 75–86% of mental health disorders in LMICs left untreated (Demyttenaere et al., 2004; Vos et al., 2020). Youth in LMICs account for a disproportionate number of global mental health disorders, often due to exposure to risk factors associated with their social, environmental, and developmental conditions (Azzopardi et al., 2019; Betancourt, Thomson et al., 2020; Kessler et al., 2007; Kieling et al., 2011; Tol et al., 2011). These risk factors are further exacerbated by low service utilization, limited mental health services, poor healthcare infrastructure, and shortages in human resources (Fitts et al., 2020; Jacob et al., 2007; Wainberg et al., 2017). While evidence-based mental health interventions have reduced the treatment gap in high-resource settings, their implementation is limited in low-resource settings, often failing to reach youth (Patel et al., 2016; Patel, Araya et al., 2007; Patel, Flisher et al., 2007).
Innovative strategies are required to address the mental health treatment gap among youth in LMICs and increase access to evidence-based interventions. One promising approach to managing the limited mental health care workforce is peer-delivery models. A peer provider approach, which is the focus of this study, is defined as at least one individual with a history of mental health challenges whom has experienced improvements in their mental health offering services or support to other individuals with similar mental health difficulties (Davidson et al., 1999, 2006). A fundamental principle of peer-delivered mental health interventions that distinguishes them from traditional delivery models is shared lived experiences of mental health challenges and cultural alignment between program participants and peer providers (Davidson et al., 2006; Fuhr et al., 2014; King & Simmons, 2018; Repper & Carter, 2011). While a strength of this delivery type, shared experiences also introduce challenges with potential secondary trauma of providers and difficulties in balancing the provider–patient relationship. These challenges should be accounted for in program design.
Recent research, including a handful of studies from LMICs, demonstrates the acceptability and feasibility of implementing peer-delivered mental health interventions (Davidson et al., 2006; Fuhr et al., 2014; Ramchand et al., 2017). Several studies indicate that peer-delivered programs can improve intervention outcomes, including social support and daily functioning (Atif et al., 2017; Cook, Copeland et al., 2012; Cook, Steigman et al., 2012; Im et al., 2018; Tse et al., 2017). Studies also suggest that peer-delivered interventions can be implemented with high fidelity when provided with adequate training and ongoing supervision and support (Atif et al., 2017; Cook, Copeland et al., 2012; Cook, Steigman et al., 2012). The literature emphasizes the importance of shared lived experiences of mental health challenges and daily hardships for intervention success (Atif et al., 2016, 2017; Davidson et al., 2006; Repper & Carter, 2011; Simmons et al., 2020; Tse et al., 2017). Peers’ shared experiences are critical for establishing trust, respect, and cohesion between participants and peer workers, facilitating participants’ buy-in to and engagement with the intervention and enabling the development of supportive relationships (Atif et al., 2016, 2017; Delman & Klodnick, 2017; Im et al., 2018; King & Simmons, 2018; Simmons et al., 2020; Simpson et al., 2018; Tse et al., 2017; Vélez-Grau et al., 2019). The qualitative literature also suggests that peer workers who deliver mental health interventions often experience benefits in their own lives, including improvements in confidence, job skill development, and communication skills (Dennis, 2010; Simmons et al., 2020; Simpson et al., 2018; Tse et al., 2017).
Despite the growing evidence supporting peer-delivery models as acceptable and feasible implementation approaches, research is primarily concentrated in high-resource settings and with adult peer providers. Few studies have examined youth as delivery agents in LMICs or applied systematic methods to adapt existing evidence-based mental health interventions for peer delivery (Murray et al., 2013). This study aims to adapt an evidence-based youth mental health intervention systematically, the Youth Readiness Intervention (YRI), to a peer-delivery model in Sierra Leone. For this study, we are defining youth as someone 18–30 years old. Sierra Leone is one of the many LMICs with a growing youth population and it experiences difficulties delivering mental health services to this group (Fitts et al., 2020; Thuli et al., 2020). A peer-led model would leverage this large youth population and fill a need for mental health services among youth in Sierra Leone.
Methods
Study setting
The current study is linked to a larger implementation-effectiveness cluster randomized control trial in Sierra Leone, referred to as Youth Functioning and Organizational Success for West African Regional Development (Youth FORWARD; Trial Registration: NCT03542500). Youth FORWARD is a coordinated research initiative that focuses on scaling up evidence-based mental health interventions for youth in West Africa and expanding regional mental health research and implementation capacity (Betancourt, Hansen et al., 2020). The Youth FORWARD study implemented the YRI within the alternative delivery platform of a youth employment program in three rural districts of Sierra Leone: Kono, Koinadugu, and Kailahun. Youth FORWARD study participants gave oral informed consent before eligibility screening and enrollment.
Mental health intervention
The YRI was developed to address difficulties in mental health, emotion regulation, and daily functioning among youth affected by war and trauma (Betancourt et al., 2014). The intervention was created based on a large body of formative research on youth mental health in Sierra Leone and in coordination with community advisory groups (Betancourt, et al., 2014). The YRI is a 12-module short-term stability and skills-focused group intervention that integrates core components of cognitive-behavioral therapy, mindfulness, and group interpersonal therapy and is delivered by lay workers in community settings with quality, including fidelity to the intervention (Betancourt, et al., 2014). Due to the sensitive topics discussed throughout the intervention, male and female YRI groups are conducted separately with gender-matched facilitators. The intervention has demonstrated effectiveness in improving emotion regulation, daily functioning, and pro-social behaviors among Sierra Leonean youth aged 15–24 in school settings (Betancourt et al., 2014). In addition, the YRI has demonstrated clinical effectiveness in improving emotion regulation and post-traumatic stress symptoms among male Sierra Leonean youth aged 18–30 in a rural district (Desrosiers et al., 2021).
Intervention adaptation method
Researchers used a community-based participatory research approach. The Assessment, Decision, Administration, Production, Topical experts, Integration, Training, Testing (ADAPT-ITT) framework guided the YRI adaptation process (Wallerstein & Duran, 2011; Wingood & DiClemente, 2008). Community-based participatory research is an approach that prioritizes the equitable involvement of community members as partners in the research process (Israel et al., 2003; Wallerstein & Duran, 2011). This approach recognizes each partner's strengths and systematically incorporates community voices, participation, and decision-making into research efforts (Wallenstein & Duran, 2010, 2011). Developing a youth peer-led model that successfully leverages shared lived experiences requires a strong understanding of youth's challenges with mental health and daily hardships, as well as their cultural identity, skills, and strengths. The adapted intervention must also understand and account for the complex nature of youth identities, including sex, urban and rural, and education level, and accompanying cultural norms and expectations within Sierra Leone. Youth are best equipped to provide such a level of understanding. This adaptation process thereby demands an approach that engages youth as active partners. This is achieved through a participatory research approach that enables youth to be directly involved in developing the adapted intervention that is responsive and reflective of youth's needs and experiences while fitting with their cultural values and norms.
Following participatory research principles, two youth community advisory boards were established to shape the production of the adapted intervention. Youth members were invited to participate in the YCABs based on their eligibility for and involvement in the Youth FORWARD study, including 18–30 years old, experiencing elevated mental health difficulties, and completing all 12 YRI modules. YCAB participants were recruited from the Youth FORWARD implementation sites in the Kono district in coordination with district youth leaders. YCAB meetings were held monthly at a community youth center with separate sessions for male (n = 10) and female (n = 10) YCAB members. Each meeting was led by a Sierra Leonean YRI expert, a Research Fellow, and two youth YCAB members. Members rotated in the leadership role of meeting facilitator. All meetings were held in Krio, the most widely spoken language in Sierra Leone. A typical meeting included a discussion or role-play of an intervention module(s), completion of tasks related to intervention adaptations, and project updates. YCAB participation was voluntary, and members received a travel stipend and meal for every meeting attended. The YCABs held kick-off meetings in November 2019 and concluded in October 2020. Due to the Coronavirus pandemic, meetings were moved to a WhatsApp platform in June 2020. The shift to a virtual platform introduced additional challenges and resulted in communication disruptions due to connectivity issues and technological competency. The research team worked closely with community leaders and youth to overcome these challenges and to ensure that all members could actively participate in the virtual meetings, including providing phones, phone credit, and technical support. Six YCAB meetings were held in person, and six were held virtually.
Through shared decision-making, the YCABs determined intervention adaptations and centered the voice and experiences of youth in the adapted intervention (Latham et al., 2012). The goals of the YCABs were the following: (1) ensure intervention fit into a new delivery model by incorporating youth's knowledge and lived experiences with the intervention; (2) engage target implementers of the intervention (youth) in identifying potential implementation barriers and strategies; and (3) identify additional intervention implementation considerations needed to support youth in their role as YRI facilitators.
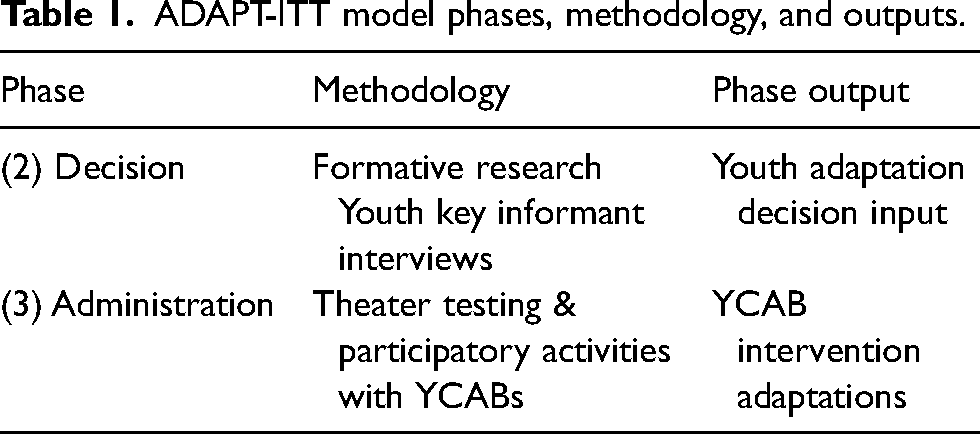
The ADAPT-ITT framework guided the intervention adaptation discussions and tasks. The ADAPT-ITT framework is an eight-step sequential process that informs adaptations to evidence-based interventions (Wingood & DiClemente, 2008). This systematic framework has been used to adapt various health interventions, including mental health interventions in low-resource settings (Audet et al., 2017; Magidson et al., 2015). A variety of methods informed the adaptation process, including discussions, role-playing, and visual tools. Table 1 illustrates the ADAPT-ITT phases, the methodology used during each phase of the adaptation process, and the output of each phase. The adaptation process focused on phases 2 and 3 of the framework, with an emphasis on four primary areas: (1) youth input on the acceptability of a peer-delivered YRI; (2) barriers to and facilitators of the implementation of a youth-delivered mental health intervention; (3) identification of modifications to intervention manual or content for youth facilitators; and (4) identification of the needs of youth mental health facilitators.
ADAPT-ITT model phases, methodology, and outputs.
Phase 1: Assessment
Formative research on mental health among youth in Sierra Leone provided a rich evidence base for the presence of mental health challenges among Sierra Leonean youth (Betancourt et al., 2010; Betancourt, McBain et al., 2014; Betancourt, Thomson et al., 2020; Thulin et al., 2022). For example, during eligibility screening in the Youth FORWARD study, 65% of youth screened positive for elevated emotion dysregulation and functional impairment (Staples & Mohlman, 2012; Üstün & WHO, 2010). In addition, youth also face various challenges in their environment, including lower education and literacy levels, unemployment, and financial hardships (Betancourt, Thomson et al., 2020; Thulin et al. 2022).
Phase 2: Decision
Intervention selection was guided by the previously discussed formative research on YRI acceptability, feasibility, and effectiveness. The decision to adapt the YRI to a peer-delivery model utilized quantitative findings from previous trials and qualitative results from the Youth FORWARD study. Eighty-eight key informant interviews (n = 44 female, 50%) from youth who received the intervention as part of the Youth FORWARD study were analyzed using thematic content analysis by two research team members. After completing the YRI and entrepreneurship program, youth were interviewed about their experiences, thoughts, and satisfaction with the intervention. Qualitative findings evaluated the youth's willingness and ability to share the YRI skills and components with their peers naturally. Further investigation into the natural diffusion of intervention skills and knowledge among peers of YRI participants is ongoing (Desrosiers, Kumar et al., 2020).
Phase 3: Administration
During the administration phase, YCAB members participated in and led several rounds of theater testing simulations of a peer-led YRI model. They role-played peer delivery of intervention modules to their same-aged peers (i.e., other YCAB members). Each meeting included an activity or discussion related to the original delivery method and adaptations needed for peer delivery. Youth shared their concerns and thoughts about the barriers and facilitators that may impact a peer-delivery model and potential implementation strategies to address the obstacles. Before theater testing simulations, YCAB facilitators were trained on the content of specific modules and the delivery approach by a YRI expert facilitator. Role-play activities simulated what youth facilitators could experience when delivering the YRI to their peers and what participants might experience when receiving the intervention delivered by their same-aged peers. Following each role-play activity, YCAB members discussed the facilitator's comfort with the delivery information, changes they wanted to make to the manual or delivery, the content they felt was missing, and support they felt was needed as youth facilitators. Members also engaged in discussions and activities around training, boundary setting, and other program implementation components.
YCAB discussions were recorded, and minutes from meetings were transcribed. Meeting minute transcripts were analyzed using thematic content analysis by two research members. The Framework for Reporting Adaptations and Modifications to Evidence-Based Interventions guided the analysis, which seeks to characterize the adaptation process and results to organize the YRI adaptations (Stirman et al., 2019; Stirman et al., 2013). This method includes the characterization of what is modified, the modification's level of delivery, and the reasons or goals for the change.
Results
Youth community advisory board participation
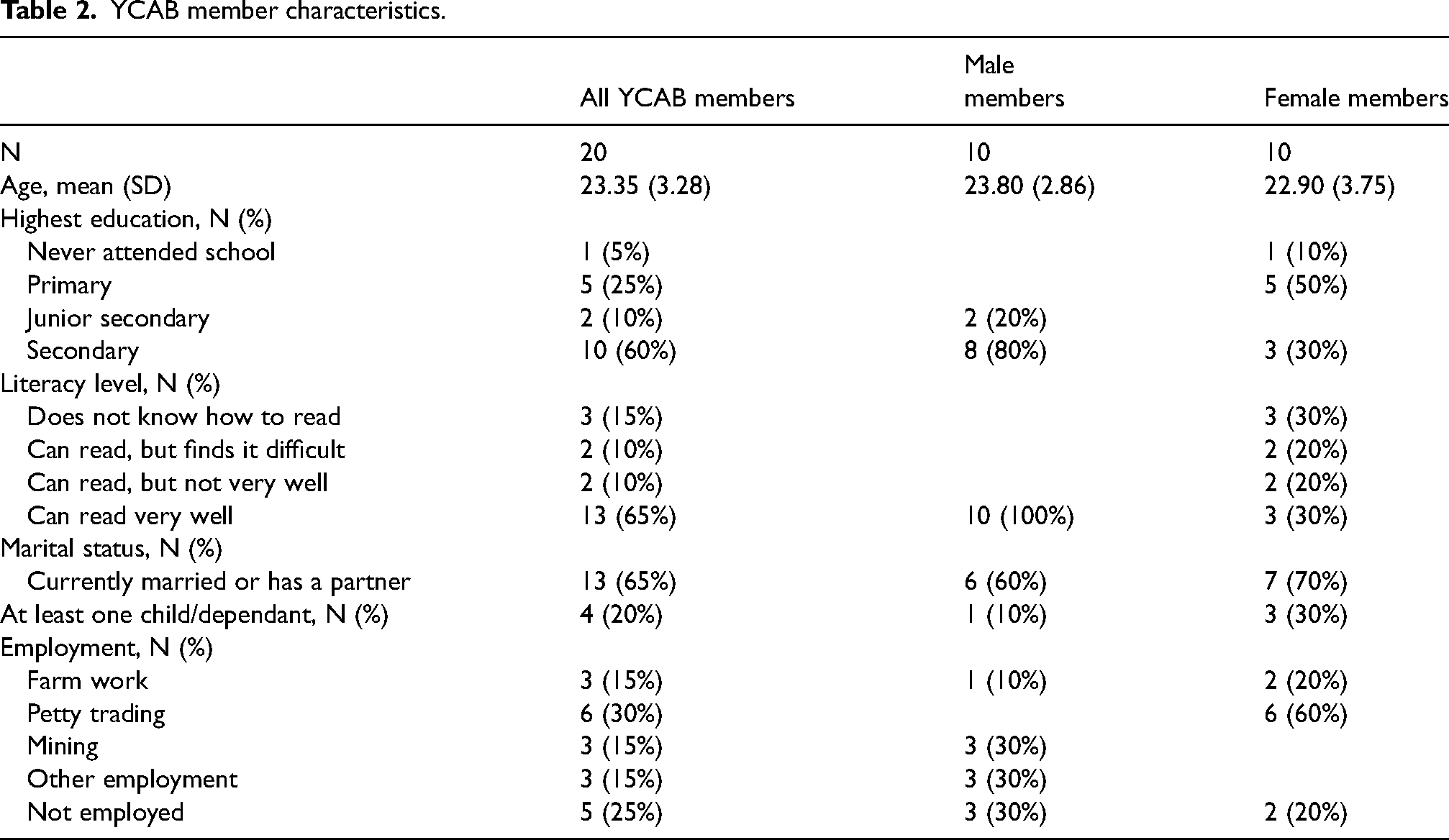
The YCABs included 20 former YRI participants, 10 male and 10 female. Males and females had separate meetings, reflecting the sex separation and sensitivity of the YRI. Members were between the ages of 18–30 and screened positive for elevated scores of emotion dysregulation and impairments as measured by the Difficulties in Emotion Regulation Scale and the WHO Disability Assessment Schedule, respectively (Staples & Mohlman, 2012; Üstün & WHO, 2010). Member characteristics are presented in Table 2. The average age for members was 23.35 years old, with the males (mean = 23.80) slightly older than the females (mean = 22.90). The males also had overall higher education and literacy levels, with 80% of males (n = 8) attending secondary school compared to 30% of females (n = 3). In addition, the youth engaged in a variety of employment opportunities, including petty trading (n = 3, 30% males; n = 0, 0% females), farm work (n = 0, 0% males; n = 6, 60% females), and mining (n = 3, 30% males; n = 0, 0% females). Attendance for meetings ranged from 100% to 50%, with similar attendance levels between male and female groups.
YCAB member characteristics.
Intervention adaptation results
Phase 2: Decision
The decision to adapt the YRI was made based on previous findings supporting the YRI's effectiveness in improving emotion regulation, interpersonal skills, and daily functioning among Sierra Leonean youth who face compounded adversity (Betancourt et al., 2014; Newnham et al., 2015), as well as qualitative analysis of youth key informant interviews. Qualitative analysis of key informant interviews from the Youth FORWARD study also demonstrated youth's willingness towards and need for a peer-delivered YRI. The YRI does not explicitly encourage sharing skills with peers, and sharing skills was not directly probed in the interviews. However, 67% (n = 59) of intervention participants mentioned spontaneous sharing of skills they learned with their peers, family members, and community leaders. Participants reported sharing specific skills with others who did not receive the YRI, taking on advisory roles in their community, and re-teaching other YRI participants to understand better YRI concepts communicated during YRI sessions. Participants shared skills learned most frequently with their families and community members and reported that they were often motivated by the benefits they personally felt to have gained from the intervention. For example, one participant stated, “My life has really [been] opened, least I am able to teach other people about things I have learnt. I use[d] to teach them so many things that will enable them to know how to live with our fellow human beings.”
Similarly, participants talked of becoming more oriented to the community around them and serving as peacemakers. For instance, some youth even played a role in helping other community members manage disagreements, such as: “like in my community I meet some people quarreling, I will first find out why are they quarrelling, I will talk to them not to make quarrel,” and encouraged them through difficult times: … if I even meet my friend wondering, I will ask why are you sitting like that; if there is something troubling that person, he/she could explain to me … I will advise that you have to take courage. If there is something troubling you, you should endure …
Additionally, some YRI participants talked of instances where the YRI groups would further explain and re-teach concepts to other YRI participants in and outside their group. One participant described this by talking about interactions with other intervention groups, “We will explain to them about the things we were taught like belly breathing and they will also explain to us about their own topic. So, we will do such interaction to share ideas amongst ourselves.” Over two-thirds of key informants discussed their willingness to share the YRI skills and knowledge with others, the importance of sharing the information, and their desire to act as peer advisors. This natural sharing provided a strong foundation for the proposed adaptation of the YRI to a peer-delivery model. For example, one participant said, “let them do some additional [training] so I will be able to gain more and to gain studies to teach my brothers and sisters who are not part of it so we all become peaceful youth in the country.” Subsequently, participants discussed how their community members reflected on the training, its impact on the participants, and the cultural fit, saying, “They have changed, after the training they have changed, people begin to talk so, saying as for now they have given a good training … God has made them learn something that will be with them till death.”
Phase 3: Administration
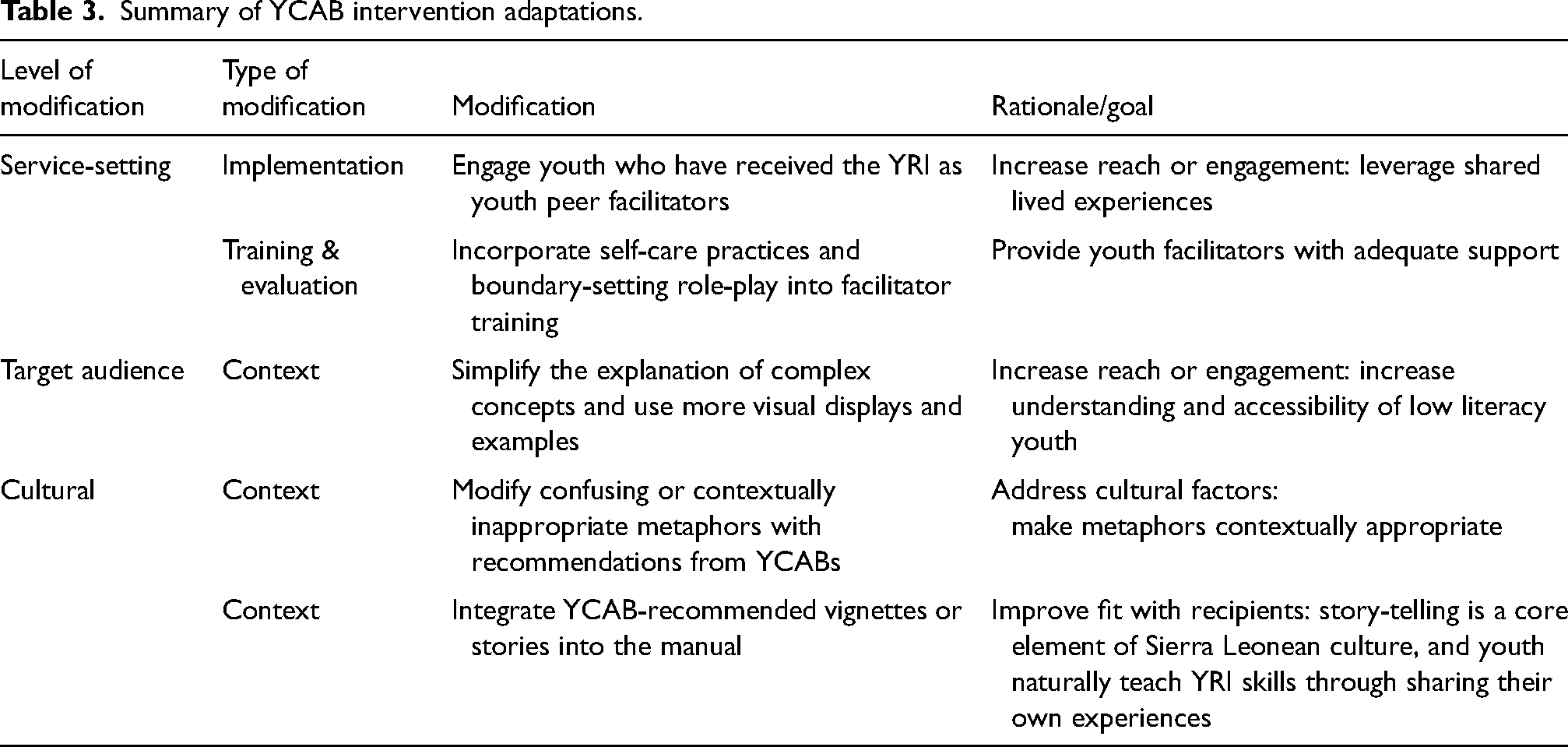
Analysis of the YCAB transcripts identified several program modifications and recommendations on best preparing youth facilitators to provide psychosocial support to their peers. YCAB modifications, presented in Table 3, are organized into three thematic areas characterized by the level of delivery for each modification: (1) service-setting modifications, (2) target audience modifications, and (3) cultural modifications.
(1) Service setting. The first modification that the YCABs agreed on was the change to engage youth who received the YRI as peer facilitators. Youth repeatedly emphasized the importance of their shared experiences in relating to what other youth experience in terms of culture, daily hardships, and mental health challenges. YCABs also believed that youth who received the YRI as participants fully understood the intervention itself, including its purpose and benefits.
Summary of YCAB intervention adaptations.
However, YCAB members also identified cultural challenges around their age and position in the community as potential barriers to establishing credibility as facilitators. For example, youth expressed concerns about not having standing, power, or credibility within their communities due to cultural perceptions associated with youth, including being inexperienced and lacking authority. YCAB members recommended several ways to address this barrier and establish their credibility, including having ID cards that designate them as YRI facilitators, receiving certificates of training, and holding mental health sensitization activities in collaboration with existing community mental health service providers and youth leadership groups. This modification aims to increase the reach and engagement of youth in the YRI by leveraging peer facilitators’ skills and experiences.
YRI experts, YRI developers, and YCABs also recognized that youth facilitators are not trained social workers or mental health providers and that youth would require additional training and supervision to deliver the intervention effectively. The YRI includes discussions around trauma, which can lead to adverse reactions in youth participants, including heightened emotions. Discussing sensitive topics and managing participant reactions could also negatively impact peer facilitators because many potential peer facilitators have histories of trauma and hardships. In light of these considerations, YCAB members discussed the need for stress management practices, boundary setting, and strategies to address heightened emotions and distress expressed by participants. The YRI expert provided several scenarios where boundaries between the facilitator and participants were needed. Example scenarios included YRI participants asking facilitators for financial or material support as well as YRI participants becoming reliant on facilitators for emotional support. YCAB members role-played how they would respond, discussing what boundaries need to be established and how they should be established. YCABs explored how to set these boundaries in a culturally appropriate manner. Self-care practices primarily centered around YRI facilitators working together and supporting each other to use YRI skills to manage their own stress. These strategies are consistent with Sierra Leonean communal culture. YCAB members emphasized that self-care and boundary-setting role-plays and preparation should be integral to YRI facilitator training. YCAB members also recommended ongoing support meetings with other YRI facilitators and supervisors to continuously reinforce skills from the YRI and encourage facilitators to be aware and take care of their mental health and wellbeing. This would also provide a space for youth facilitators to learn from each other how to manage stress. This modification offers youth facilitators adequate support to effectively deliver the YRI to youth while maintaining their mental wellbeing.
(2) Target audience. The second type of recommended YRI modification was related to the target audience. YCABs identified the need for content modifications to the YRI due to the literacy levels of youth participants in rural areas. YCAB members, including low-literacy youth, expressed difficulties understanding concepts presented in the YRI. During YRI delivery, concepts such as confidentiality and trauma required more complex explanations that were difficult for low-literacy youth to understand. YCAB members recommended modifications to content delivery to simplify complex concepts and use visual displays when possible. For example, when discussing goal setting, YCAB members recommended using a visual aid of a ladder drawing to illustrate the purpose of goal setting and taking steps towards achieving their goals. YCAB members believed these modifications would help low-literacy youth more easily understand and engage with the YRI material. (3) Cultural. The final type of recommended YRI modification was related to the cultural fit and context of the YRI. YCAB members identified intervention metaphors that did not fit the context or population of youth in rural areas. The YRI was previously implemented in an urban school setting and contained metaphors and appropriate examples for that population. Although the YRI was modified to fit a rural youth population, some metaphors needed to be more straightforward and relevant for youth in this setting. One example was using a metaphor of a car breaking down when discussing coping techniques. This metaphor was challenging for youth due to location and gender-related aspects. Cars, in general, are less common in many rural areas of Sierra Leone, meaning youth in these areas are not as familiar with how to manage a broken-down car compared to youth in urban areas. In addition, female Sierra Leonean youth participants were less likely to have experience handling a broken-down car than their male counterparts. Finally, due to the gendered nature of the YRI, with separate gender groups and same-sex facilitators, female participants had added challenges in their understanding of this metaphor. To address these challenges, YCAB members brainstormed substitute metaphors for rural youth and female participants. Recommendations included a metaphor of footwear breaking to discuss coping strategies.
Also, through YCAB discussions of YRI delivery, youth discussed the value of incorporating case studies or vignettes about the shared experiences of youth into the YRI manual. The incorporation of storytelling would leverage the shared experiences among facilitators and youth, potentially strengthening the development of rapport in the groups. When discussing how they naturally share YRI skills, YCAB members described sharing through telling their peers about their stories and experiences. Storytelling is also essential to Sierra Leonean culture, making it a culturally appropriate modification. To develop the vignettes, YCAB members first determined which areas of the YRI manual would benefit from a vignette and which skills would be explained through the story. YCAB members then brainstormed how they have utilized YRI skills or knowledge in their daily lives. Drawing on their personal experiences, YCAB members identified vignette scenarios that they felt captured the common challenges or concerns encountered by youth in everyday life. Each vignette presented a story of a fictional youth character experiencing a common challenge and illustrated the youth character utilizing the YRI skill learned in that session to address that challenge. When necessary, males and females developed distinct vignettes to be sure the story was culturally appropriate and relevant for each sex.
Discussion
This study describes and documents the process for adapting an evidence-based youth mental health intervention to a youth peer-delivered model. Through a collaborative approach that engaged youth as partners, the adaptation process followed the ADAPT-ITT systematic framework. The modifications developed from the YCABs will support the development of a peer-delivered YRI that is culturally and contextually appropriate and leverages youth peer facilitators’ shared lived experiences. Engaging youth as partners in the research and adaptation process enabled the meaningful incorporation of the youth voice into suggestions for YRI adaptation. The YCABs were instrumental in identifying critical elements of Sierra Leonean cultural identity, especially for youth, and developing intervention modifications that leveraged strengths and lived experiences or addressed potential barriers related to these cultural elements. The CBPR approach and the role played by the YCABs in the adaptation process are critical to developing a successful peer-led intervention.
Regarding the next steps, the outputs developed through the first three phases of the adaptation process will continue to move through the ADAPT-ITT phases to create a peer-delivered YRI. Each subsequent phase of the adaptation process will reference and build upon the adaptations, challenges, and strengths identified by the YCABs. The first draft of the adapted intervention will include modifications to the YRI facilitator manual, implementation considerations/strategies, and the needs of youth facilitators. Production (phase 4: production) of the first draft of the adapted YRI involved balancing youth-driven changes while maintaining fidelity to the YRI core components and underlying theory of change. Topical experts will review the modified intervention elements presented in this study to ensure that integrity to the YRI core components and theory of change are maintained through the adaptation process (phase 5: topical experts). Feedback from topical experts, including YRI creators, will then be integrated into a subsequent adaptation of the YRI manual (phase 6: integration).
Once the adaptations and refinements to the YRI manual are completed, topical experts will also provide feedback on adapting the training model to train youth peer facilitators, using lessons from the recent Youth FORWARD implementation study. Based on input from the YCABS, it will be essential to develop additional training materials related to the role of a facilitator, including a discussion of boundaries and roles, general principles of counseling, and self-care. We will then conduct youth/peer facilitator training on the adapted YRI using the adapted training materials and assess the competency and understanding of core YRI content and principles following the training (phase 7: training). The YRI training materials will be further refined based on the results of the competency assessment and peer facilitator qualitative interviews. Following the completion of training, the next step will be to conduct a pre-pilot of the adapted YRI delivered by peer facilitators with two YRI groups, one male and one female (phase 8: testing). The pre-pilot will use the adaptations and implementation lessons from the Youth FORWARD study to test the acceptability and feasibility of implementing a peer-delivered YRI and assess adaptation efficacy (Betancourt, Hansen et al., 2020). It will also explore any potential biases that are introduced in a peer-delivered YRI that may affect intervention effectiveness. Results from the pre-pilot will inform any further intervention refinements.
Although the YCABs identified many important areas to adapt and develop a peer-delivered YRI and improve the cultural fit of the YRI, several implementation considerations relevant to intervention delivery still needed to be explored. These considerations include who will provide supervision for YRI peer facilitators, compensation and employment structures, and the timing of YRI delivery. In addition, some areas raised by YCABs will need further exploration and attention from YRI developers and experts, including how YRI peer facilitators will manage risk-of-harm cases and the criteria to be selected as a YRI peer facilitator (e.g., age range, education level). Lessons from implementing the Youth FORWARD study, which utilized a collaborative team approach, including a seed team of YRI experts, to implement the YRI, can serve as a foundation for addressing many of these concerns (Betancourt, Hansen et al., 2020). The use of this approach enabled the training of new facilitators and developed a structure for a multi-agency system of employment structures. A pilot study of the peer-delivered YRI will leverage and build on this approach to address implementation challenges.
Limitations
Study findings should be considered in light of several limitations. YCAB members ranged in age from 18 to 30 and were recruited from rural regions of Sierra Leone, where the average educational level is low. Feedback from YCAB members on YRI adaptations may not generalize or be relevant to youth aged 18–30 in other regions of Sierra Leone, including those with higher educational attainment or those residing in urban areas. Recommendations to alter YRI content because it was difficult to understand might be better addressed by simplifying language or identifying more culturally relevant examples to explain concepts. Although the YRI has been evaluated with younger youth, ranging in age from 15 to 24, recommended YRI adaptations may also not generalize to younger populations of youth or those still in school. In addition, the lack of resolution around implementation factors limits this adaption process. Future research will explore the subsequent phases of the adaptation process, including addressing implementation challenges.
Conclusion
The current study successfully applied a CBPR approach and an intervention adaptation model with youth in a rural, underserved region of Sierra Leone. YCAB-recommended modifications reflected the experiences of youth with difficulties in emotion regulation and daily functioning and relayed their unique needs and perspectives. Findings support the importance of engaging the target population of an intervention in the adaptation process and incorporating their feedback to refine existing evidence-based practices to fit individual needs better. Given the potential for peer delivery to expand the reach and access of evidence-based mental health interventions, further research explores the impact of adapted peer-delivery models and implementation strategies that can best sustain the intervention with quality over time. In LMICs with severely constrained health systems, including Sierra Leone, peer-delivery models have the potential to strengthen health delivery systems and address human resource shortages, particularly if also bolstered by financial investment and policy support from government stakeholders to ensure ongoing supervision for quality and impact.
Footnotes
Acknowledgements
The authors would like to acknowledge the efforts of the whole research project team, the support of our partner agencies, and the generosity of the Sierra Leone youth community advisory boards and communities in the Kono district.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Minority Health and Health Disparities of the National Institutes of Health (grant number: U19-1U19MH095705-01).
Ethical Approval Statement
The Boston College Institutional Review Board, Sierra Leone Scientific Review Committee, and National Institute of Mental Health Data and Safety Monitoring Board approved the Youth FORWARD study: NCT03542500.