
Abstract
Heavy drinking and smoking have been found to be among the leading causes of morbidity and mortality within Indigenous youth in North America. The focus of this study was to examine the relative roles of cultural identity, parent–child communication about the harms of substance use (SU), and perception about peers’ opinions on heavy drinking and cigarette smoking among Indigenous youth. Strong Indigenous cultural identity, parent–child communication about SU, and affiliation with peers who do not use and/or who disapprove of substance use were all expected to reduce risk for heavy drinking and smoking. Substance use beliefs were hypothesized to mediate these effects. Youth (N = 117; Mage = 14.07; grades 6–11) from two Indigenous communities in Quebec completed self-reports. Consistent with the hypotheses, strong cultural identity predicted increased negative beliefs about substance use, which predicted reduced drinking and smoking. Similarly, affiliating with peers who did not use alcohol predicted decreased positive beliefs about alcohol use, which predicted reduced drinking. Affiliating with peers who did not smoke cigarettes predicted reduced cigarette smoking. Parental influences were not supported in this model. Intervention strategies may benefit from targeting cultural identity, peer groups, and substance use beliefs among Indigenous youth.
In this contribution to the special issue in celebration of the life of Michael Chandler and his formative work on the study of the identity, culture, resilience, and well-being of Indigenous Peoples, we attempt to extend his specific focus on the protective influence of cultural identity against deleterious, self-harming behaviors among Indigenous youth (e.g., Chandler & Lalonde, 1998, 2008; Chandler et al., 2003). Whereas Chandler and Lalonde emphasized the link between community engagement in reclaiming their culture and diminished rates of suicide among both Indigenous youth (Chandler & Lalonde, 1998) and adults (Chandler & Lalonde, 2008), we explore the link between individual adolescents’ self-reports of association with their Indigenous culture, as well as of parental and peer influence, on substance use. In contrast to Chandler and Lalonde's use of government records that included data from virtually all of the Indigenous communities from across British Columbia, we used self-report data from youth from two communities in Quebec. Despite these differences between the studies, this study is largely inspired by Chandler and colleagues’ far-reaching conceptualizations of cultural identity and implications for understanding and promoting well-being among Indigenous persons.
The focus of this study was the disproportionate risk and burdens related to substance use among Indigenous youth (Farahmand et al., 2020; Smallwood et al., 2021; Urbanoski, 2017). Heavy drinking and smoking have been found to be among the leading causes of adolescent morbidity and mortality within Indigenous communities in North America (Walls et al., 2013). In Canada, Indigenous youth are more likely to report drinking alcohol in the past year and to become a regular cigarette smoker as compared to their non-Indigenous peers (Sikorski et al., 2019). According to Indigenous youth’s self-reports from the First Nations Regional Health Survey (2018), 25% of Indigenous youth in Quebec drank alcohol, with over 50% of these youth binge drinking at least monthly. Approximately 20% of Indigenous youth smoked, of whom 10% smoked on a daily basis.
In contrast to the deleterious impact of early alcohol and cigarettes on the physical and mental health of Indigenous youth, identification with ancestral cultures has been associated with positive educational, social, and emotional well-being outcomes across places and contexts (Berry et al., 2020; Blacklock et al., 2020; Burack et al., 2017; Flanagan et al., 2011; Whitesell et al., 2014). Following from Chandler and Lalonde's work (1998, 2008; Chandler et al., 2003), Indigenous culture is seen as protective in maintaining and improving health, as well as reducing risk factors for physical and mental health problems. For example, youth’s strong ties to Indigenous culture, which discourages substance use and promotes approaches for wholistic wellness, reverence toward elders and parents, and general well-being of community members (i.e., peers), may lead to less positive beliefs about substance use. Furthermore, the protective factors of culture, such as practicing traditional activities and having a positive ethnic identity (Burack et al., 2014; Kirmayer et al., 2016; Venner et al., 2021), are particularly salient among youth, as adolescence and early adulthood are developmental periods characterized by uncertainty about identity and belongingness that has been associated with engagement in risky behaviors, such as substance use.
The social environment
In addition to cultural identity, other factors that have been hypothesized to exert an influence on substance use among Indigenous youth include peer influence and parental communication (Cheadle & Whitbeck, 2011; Ritland et al., 2020). During adolescence, youth tend to spend a significant amount of time with their peers, highlighting the potential protective role of the peer group to communicate values and expectations that are inconsistent with substance use (Cheadle & Whitbeck, 2011). Similarly, parents may exert a protective influence by communicating the harms of risky behaviors to their children (Schwinn & Schinke, 2014). In support of this notion, Moon et al. (2014) found that parental monitoring was negatively associated with marijuana use among Indigenous adolescents in the United States, while affiliating with peers who engaged in substance use increased marijuana use.
The current study
The focus of this study was the role of cultural identity in the context of other developmental influences, such as the role of parental communication about the harms of substance use and peers’ influence on substance use. It explores the unique protective effects of cultural identity, parent–child communication, and peers on alcohol and cigarette smoking among youth in two Indigenous communities in Quebec. We hypothesized that self-reports of strong Indigenous cultural identity, parent–child communication about the harms of substance use, and perceptions that peers do not use or condone substance use would be associated with reduced risk for drinking to intoxication and cigarette smoking. We also hypothesized that youth's beliefs about the negative and positive effects of alcohol and cigarette use will mediate these pathways.
Method
The study was conducted as part of ongoing multi-year collaborations between the researchers and the two participating schools and their respective communities. Through collaboration, the larger research program has been focused on the role of cultural identity and relationships for academic success, social adaptation, and emotional well-being. The leadership of both communities approved the battery of measures that were administered to the participants of the study. The study was approved by the Research Ethics Board Office at McGill University and the University Human Research Ethics Committee at Concordia University.
Participants
Nearly all of the students (N = 157) in grades 6 to 11 from two Indigenous communities in northern Quebec were recruited to participate in the larger program of research from which data was used for this study. Participation was premised on active or passive parental consent and participant assent. The parents were provided the option to inform the schools if they did not want their child to participate. Additionally, the students were also told that even if they agreed to participate, they could withdraw from the study at any time. The final group whose data was used for this study included 117 students (52% male; Mage = 14.07 years, SDage = 1.87) who completed all of the relevant measures. The completion rate was relatively low due to some participants’ absences from school and/or students deciding to discontinue during the study. Independent sample t-tests revealed no significant differences for sex, age, or grade between those students who were eligible and did not complete the measures (N = 40) versus those students who were included in the analyses (N = 117). The distribution of the participants across school years was 15% in grade 6; 15% in grade 7; 21% in grade 8; 18% in grade 9; 26% in grade 10; and 5% in grade 11.
Multigroup ethnic identity measure (MEIM)
The cultural identity scale (14 items) of the larger 23-item MEIM (Phinney, 1992) was used. This questionnaire was developed to assess the level of ethnic identity. While the measure is not specific to Indigenous communities or cultures, it utilizes language that is thought to be common across cultural groups (e.g., I have a clear sense of my ethnic background and what it means for me). As the term ‘ethnic identity’ was not frequently used in the community, an explanation was provided to all of the participants, who were encouraged to replace the term with identification with Indigenous culture. All of the participants were encouraged to ask questions if an item was unclear. In the younger grades, the teachers and their assistants often provided an explanation and examples in their native language. The participants indicated (1 = strongly disagree to 4 = strongly agree) how much they agreed with each statement. A mean score was derived. The internal consistency was calculated (α = .81).
Early adolescent substance use measure (EASUM)
Perceptions of parent communication about the harms of drinking and smoking were measured with 17 items from the original 19-item EASUM (Kodl & Mermelstien, 2004). The two other items were dropped because they were unrelated to alcohol or cigarette use. The participants indicated (1 = never to 4 = many times) how often their parents talked about the harms of alcohol (eight items) and cigarette (nine items) use. Two mean scores were derived reflecting communication about drinking and smoking. The internal consistencies were calculated for both the drinking (α = .88) and smoking (α = .89) subscales.
Peer perception of substance use (PPSU)
Perceptions of peer use and approval of alcohol and cigarettes were measured with an adapted 10-item version of the PPSU (Johnston et al., 2003; see Trucco et al., 2011). The participants indicated (1 = none to 6 = all) how many of their friends’ drank alcohol and smoked cigarettes. They also indicated (1 = strongly disapprove to 5 = strongly approve) what they thought their close friends would think if they drank alcohol and smoked cigarettes. Four mean scores were derived, indicating perception of peer drinking (three items) and smoking (two items) and perception of peer approval of drinking (three items) and smoking (two items). Internal consistencies for all four peer perception subscales ranged from α = .88 to α = .92.
Alcohol expectancies
Beliefs about the effects of drinking were assessed using an adapted 20-item alcohol expectancies questionnaire (Leigh & Stacy, 2004). The participants indicated (1 = very unlikely to 4 = very likely) how likely it was that they would experience a series of positive and negative outcomes if they drank alcohol. Separate mean scores were derived for positive (10 items) and negative (10 items) beliefs about alcohol use. Internal consistencies were calculated for positive (α = .89) and negative (α = .80) beliefs.
Smoking expectancies scale for adolescents
Beliefs about the effects of smoking were assessed using an adapted 27-item smoking expectancies questionnaire (Hine et al., 2007). The original questionnaire was adapted to only include items (27 out of 43 items) that demonstrated loadings of greater than .50 and no cross-loadings above .30 in a pattern matrix from a confirmatory factor analysis (CFA). The participants indicated (1 = completely unlikely to 10 = completely likely) how likely a series of positive and negative outcomes would occur if they smoked cigarettes. Separate mean scores were derived to reflect positive (13 items) and negative (14 items) beliefs about cigarette use. Internal consistencies were calculated for positive (α = .83) and negative (α = .91) beliefs.
Self-report delinquency scale
Two items from the self-report delinquency scale (Elliott et al., 1989) were used to measure frequency (1 = never to 6 = 40 + times) of alcohol and cigarette use in the past year. Due to the lack of variability in responses, these variables were coded dichotomously (0 = none in the past year, 1 = at least once in the past year).
Data analytic overview
Internal consistency reliability was evaluated by the Cronbach's α coefficient. The value of the Cronbach's α coefficient can vary between 0 and 1, with values between .70 and .95 deemed acceptable. Higher values represent higher internal consistency or higher congruence between the items (Cho, 2016). The analysis of the reliability of the self-report questionnaires, as measured by the internal consistency of items and dimensions, revealed that overall scale reliability was acceptable, as demonstrated by Cronbach's α statistic values which ranged from .80 to .92. Path modeling was used to test the proposed model from cultural, parental, and peer variables (predictors) to substance use (outcomes) via alcohol and cigarette beliefs (mediators). Two path models were run to test effects on the dichotomously coded outcomes of drinking to intoxication and cigarette use. In both models, grade was added as a covariate. Model fit is excellent if the CFI is > .95, if the RMSEA is < .06, and if the model χ2 is not significant (Hu & Bentler, 1999). Bias-corrected bootstrapping with 95% CIs was used to test the presence and magnitude hypothesized indirect effects. If a hypothesized model provided inadequate fit, theory, empirical evidence, and modification indices (MIs) informed the adjusted model. Additional paths were freed incrementally. Improvement in the model fit was assessed using the χ2 difference test and Cheung and Rensvold's (2002) recommendation of ΔCFI ≥ 0.01.
Results
Data screening
All of the continuous predictors and mediators were normally distributed (Skew <3.0 and Kurtosis <10; Kline, 2009).
Descriptive statistics and bivariate correlations
The descriptive statistics and bivariate correlations are presented in Table 1. Perception of peer use of alcohol and cigarettes and of their approval of this (but not identification with Indigenous culture or parent communication) were positive correlates of drinking to intoxication and cigarette use.
Descriptive statistics and bivariate correlations of alcohol and cigarette use.
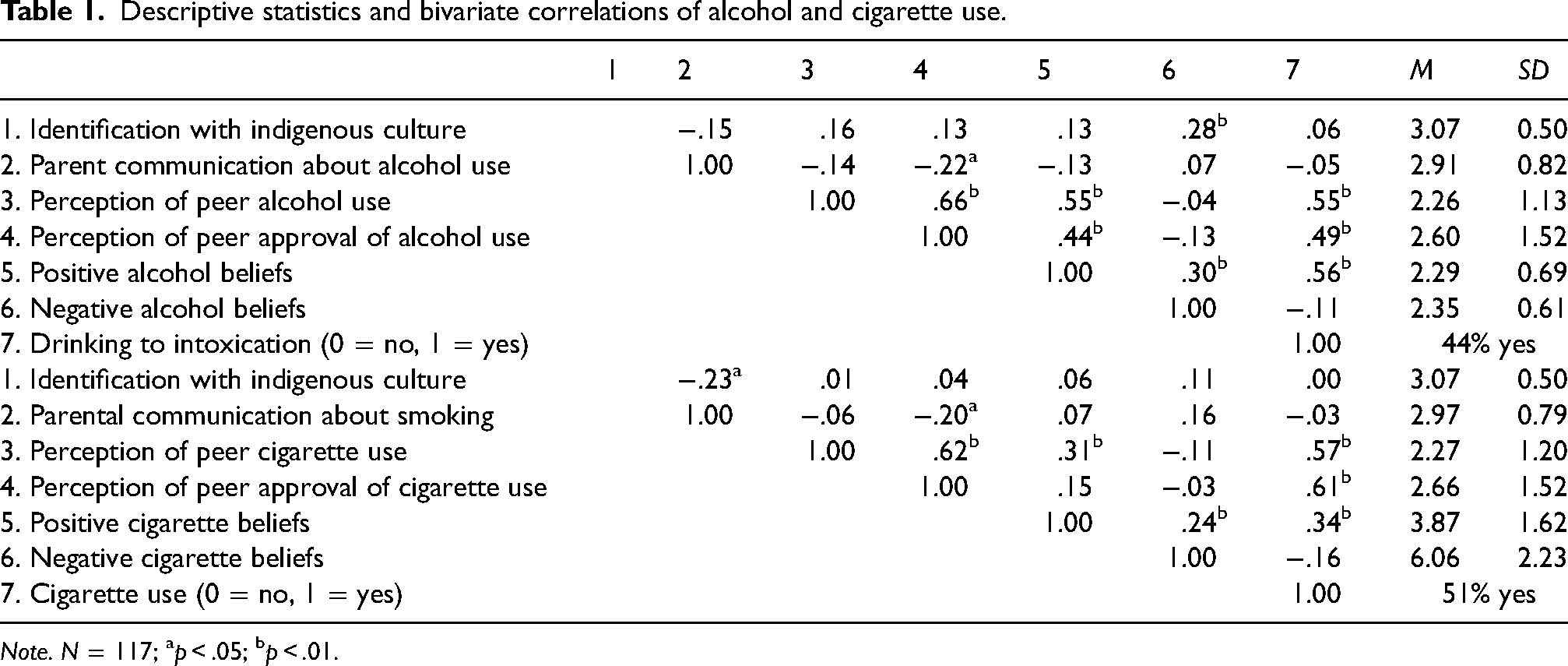
Note. N = 117; ap < .05; bp < .01.
Hypothesis testing
Model 1: Drinking to intoxication
The hypothesized model fit the data well for drinking to intoxication (χ2(4) = 4.772, p = .311, CFI = .9962, RMSEA = .05, 90%CI[0.000, 0.150]) (see Figure 1). As expected, controlling for grade, identification with Indigenous culture was positively associated with negative alcohol beliefs, and perception of peer alcohol use was positively associated with positive alcohol beliefs. Perception of peer alcohol use also had a direct positive effect on drinking to intoxication. As expected, positive alcohol beliefs were positively associated with drinking to intoxication, whereas negative alcohol beliefs were negatively associated with drinking to intoxication.
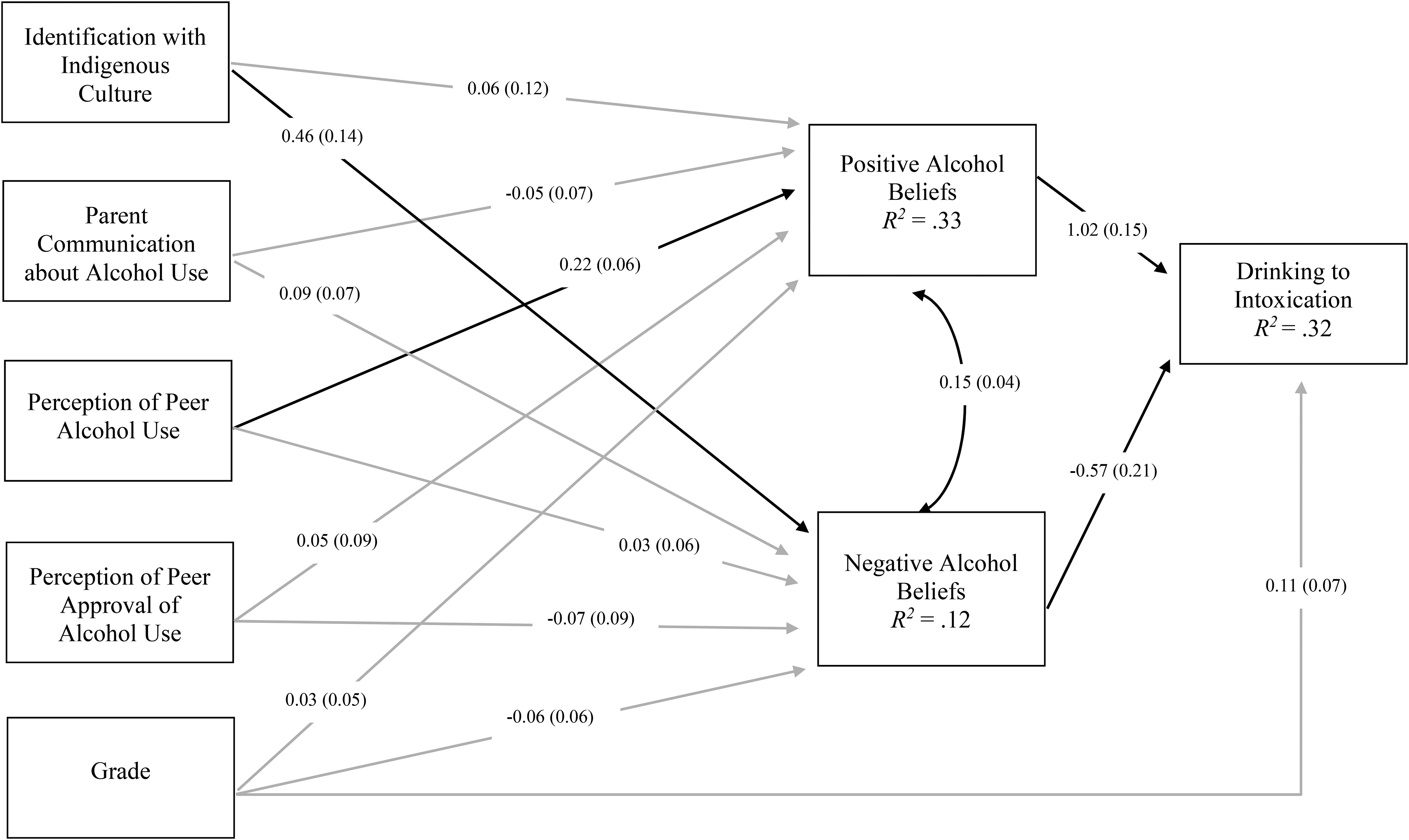
Unstandardized path estimates with standard errors (in brackets). Bold lines are paths that were statistically significant and gray lines are paths that were non-significant. Covariances among predictors are not displayed for clarity of presentation. Grade was added as a covariate in this model.
The effect of identification with Indigenous culture on drinking to intoxication was mediated by negative alcohol beliefs (B = −0.129, 95%CI[−0.332, −0.038]). Strong Indigenous cultural identification was associated with elevated negative alcohol beliefs, which in turn were associated with a decreased probability of past-year drinking to intoxication. Also, the indirect effect of perception of peer alcohol use on drinking to intoxication was mediated by positive alcohol beliefs (b = 0.221, 95%CI[0.076, 0.348]). The perception that peers are not drinking or are drinking at low levels was associated with decreased positive alcohol beliefs, which were associated with a low probability of past-year drinking to intoxication.
Model 2: Cigarette use
The hypothesized model provided inadequate fit to the data for cigarette use (χ2(4) = 8.621, p = .071, CFI = .904, RMSEA = .099, 90%CI[0.000, 0.190]). Based on MIs, a direct effect from perception of peer approval of cigarette use to cigarette use was added. This led to significant improvements (Δχ² = 6.364, p < .05, ΔCFI = 0.096), and the fit of the final model was excellent (χ²(3) = 2.257, p = .520, CFI = 1.00, RMSEA = .00, 90%CI[0.000, 0.139]) and was retained (see Figure 2). As expected, Indigenous cultural identification was positively associated with negative cigarette beliefs. Also consistent with hypotheses, perception of peer cigarette use was positively associated with positive cigarette beliefs. Perception of peer cigarette use also had a direct positive effect on one's own cigarette use. Positive cigarette beliefs were not associated with cigarette use, but negative cigarette beliefs were negatively associated with cigarette use. The effect of Indigenous cultural identification on cigarette use was mediated by negative cigarette beliefs (B = −0.154, 95%CI[−0.430, −0.022]). Strong Indigenous cultural identification was associated with elevated negative cigarette beliefs, which in turn were associated with a low probability of past-year cigarette use.
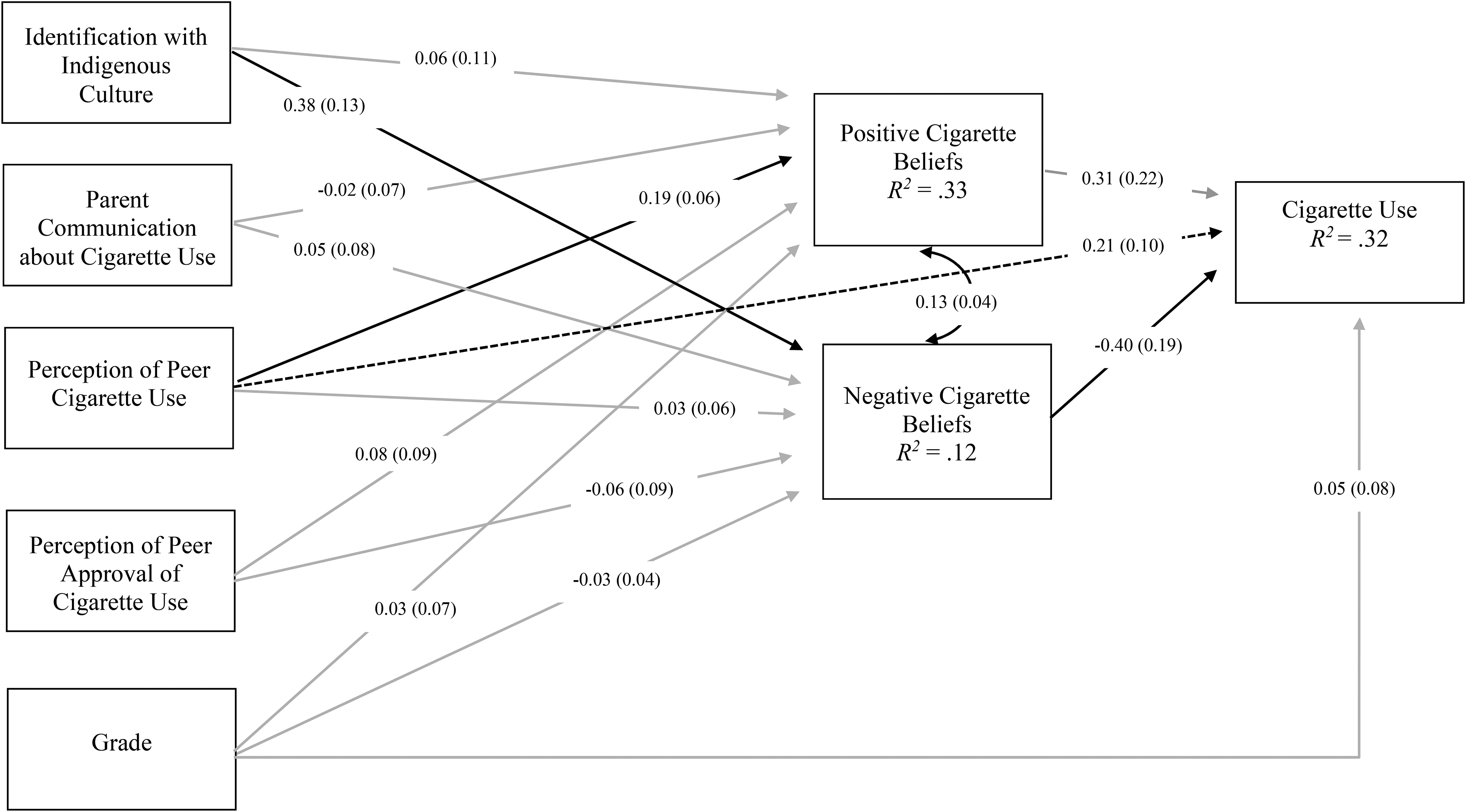
Unstandardized path estimates with standard errors (in brackets). Bold lines are paths that were statistically significant and gray lines are paths that were non-significant. Dashed lines indicate the path added based on theory and MIs. Covariances among predictors are not displayed for clarity of presentation. Grade was added as a covariate in this model.
Discussion
Consistent with one of our main hypotheses and Chandler's emphasis on the restorative impact of cultural identity, the Indigenous youth who identified strongly with their Indigenous culture were less likely to have drunk to intoxication and smoked in the past year. This low-risk pathway was explained by more negative beliefs about drinking and smoking among the participants. In partial support of hypotheses, the perception that peers never or rarely use alcohol was associated with decreased drinking to intoxication during the past year. This low-risk pathway was explained by decreased positive beliefs about drinking among participants. The perception that peers never or rarely smoke cigarettes was directly associated with decreased cigarette smoking during the past year. Contrary to the hypotheses, we did not find protective effects of parent communication or low peer approval.
These findings inform about the protective role of cultural identity on substance use among Indigenous youth. While no link was found between cultural identification and alcohol and cigarette use at the bivariate level, this pattern is in line with some evidence of weak or null associations between identification with Indigenous culture and substance use (Bates et al., 1997; Petoskey et al., 1998; Whitesell et al., 2014). However, as we examined the role of culture in the context of other developmental influences, such as the role of parents and peers, on drinking alcohol and smoking cigarettes, we observed that identification with Indigenous culture was uniquely associated with substance use resistance among Indigenous youth. Those youth who reported strong ties to their culture tended to endorse strong negative beliefs about substance use, and this further reduced the likelihood that they would either drink heavily or smoke cigarettes. This is consistent with Currie et al.'s (2011) finding that strong identification with ancestral culture was associated with reduced drinking among a sample of Indigenous university students in Alberta. Currie et al. suggested that cultural ceremonies, such as purification ceremonies, allowed youth to cope with stress and to connect with peers in ways other than substance use. These findings are also in line with the Truth and Reconciliation Commission’s (2015) recommendations that Indigenous people are not only made aware of the history of colonization and assimilation, but that they are supported in healing and re-establishing their collective cultural identities. Reconnecting to one's cultural identity and engaging in culturally based practices is essential in promoting wellness for Indigenous people (Fiedeldey-Van Dijk et al., 2016). Helping Indigenous youth build a strong sense of cultural identity may better equip them to conquer the burden associated with the historical trauma faced by their people by turning back to traditional ways of life and re-establishing their cultural identity (Kirmayer et al., 2016).
The unexpected finding that parent communication about substance use risks was not a unique predictor of reduced drinking and smoking suggests some methodological concerns regarding research with Indigenous youth. For example, the questionnaire used to assess parent communication may not capture the communication style of Indigenous parents (e.g., storytelling). Alternatively, shared parenting is common in many Indigenous communities (Neckoway et al., 2007), as parents, grandparents, aunts, and uncles often reside in the same house and may exert an influence over adolescent substance use behaviors. Although parent communication about the risks of substance use was not associated with reduced drinking and smoking, the bivariate correlations suggest that parent communication was associated with reduced affiliation with peers who approve of substance use. This association between parents and peers may indicate that the protective role of parents is indirect through impact on peer selection. This may be essential to well-being, as the link between youth’s perceptions of their peers’ substance use and their own substance use may be most influenced by the friend group to which they belong, rather than the larger peer group (e.g., same-aged peers).
Our findings support the protective role of affiliating with peers who do not engage in substance use, as the youth who held the perception that their peers were drinking, smoking, or both were more at risk for substance use. This finding is consistent with longitudinal evidence of increased risk for developing an alcohol use disorder among North American Indigenous youth who affiliate with peers who engage in substance use as they progressed throughout adolescence (Armenta et al., 2016). This link between the youth’s perceptions of their peers’ substance use and their own substance use may be explained by their overestimation of substance use among their peers (Henry et al., 2011). Conversely, youth who held the perception that their peers do not, or rarely, drink endorsed fewer positive beliefs about alcohol use, and in turn were less likely to drink themselves. Concordantly, perceptions that their peers do not or rarely smoke cigarettes directly decreased the risk of engaging in cigarette smoking. The direct effect of perceived peer smoking on own cigarette use is consistent with evidence that youth reports of friends’ smoking behavior remain one of the most consistent and strongest predictors of smoking (Yu et al., 2005; Yu & Whitbeck, 2016). Youth who affiliate with a group of friends who do not or rarely smoke may not feel pressure to begin smoking, and may be less exposed to cigarette offerings.
Peer disapproval or low approval was not a significant predictor of refraining from drinking to intoxication and smoking cigarettes. However, bivariate correlations supported positive associations between peer disapproval or low approval, less positive substance use beliefs, and less drinking to intoxication and smoking cigarettes. Yet, pitted against peer substance use (or abstinence), the role of peer disapproval of substance use may be less influential on drinking and smoking. This pathway is consistent with primary socialization theory in which modeling is considered one of the key determinants of learning social behaviors (Borsari & Carey, 2001). Accordingly, youth who affiliate with a peer group that does not engage in substance use may be less likely to use these substances, especially in a reckless manner.
Limitations and future directions
This study has some limitations. One, only youth who attended school were recruited. While the vast majority of the youth in these two communities attend school, the relevance to those who do not regularly attend or are not enrolled in school should be examined. Two, the findings are from youth from two communities in Quebec whose data were combined for statistical purposes, although the communities differ with regard to many factors including history, language, and cultural practices, which were not taken into account. Three, defining and measuring cultural identity is multifaceted and complex. The youth’s own perceptions of what it means to identify with their culture and assessment of the various facets of cultural identity were limited. The use of multiple measures specific to Indigenous cultures and qualitative interviews may be useful in better understanding the meaning that youth attribute to Indigenous cultures and identities. Four, as we only examined youth’s reports of direct communication with their parents, we have no information relevant to the youth’s relationships with their grandparents and other family members who may play an integral role in child-rearing. Given the bivariate correlation between parent communication about substance use and peer approval of substance use, a next step could also further explore the influence of parents and/or other important caregivers on peer selection. Five, we utilized a cross-sectional design that does not allow us to disentangle the temporal relation between substance use and youth perceptions of cultural identity, family communication about substance use, or peer use and beliefs about substance use.
Summary
The findings from this study suggest that Indigenous youth who identify with their culture are at decreased risk for drinking and smoking because they endorse negative substance use beliefs. Further, Indigenous youth who affiliated with peers who do not (or rarely) use alcohol have a decreased risk for drinking because they have fewer positive alcohol use beliefs. Indigenous youth who affiliated with peers who do not (or rarely) smoke cigarettes have a decreased risk for smoking. The next step would be to extend this model to other licit (e.g., cannabis use) and other illicit drug use (e.g., methamphetamine). Nonetheless, the evidence suggests that identifying with one's Indigenous culture and connecting with a peer group that does not engage in substance use can act as a buffer against drinking alcohol and smoking cigarettes among Indigenous youth. These findings are yet further evidence in support of Michael Chandler and colleagues’ foundational lessons about the power of strong community and identification with ancestral culture in facilitating the well-being of Indigenous youth.
Footnotes
Acknowledgements
Thank you to the participating students, families, and educators in the schools in which we conducted the study, and to the communities for their collaboration on this project. Thank you to the members of the McGill Youth Study Team and the Young Adult and Alcohol Research Lab who collected and entered the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Network for Aboriginal Mental Health Research, Canada Research Chairs, Canadian Institutes of Health Research.