
Abstract
Language is an important aspect of communication and language status is known to impact healthcare accessibility, its perceived suitability, and outcomes. However, its influence on treatment engagement and/or disengagement is unknown. Our study therefore sought to investigate the impact of language on service disengagement in an early intervention psychosis program in Montreal, Quebec (a province with French as the official language). We aimed to compare service disengagement between a linguistic minority group (i.e., English) vis-à-vis those whose preferred language was French and to explore the role of language in service engagement. Using a mixed methods sequential design, we tested preferred language and several sociodemographic characteristics associated with service disengagement in a time-to-event analysis with Cox proportional hazards regression models (N = 338). We then conducted two focus groups with English (seven patients) and French speakers (five patients) to further explore differences between the two linguistic groups. Overall, 24% (n = 82) disengaged from the service before the two-year mark. Those whose preferred language was English were more likely to disengage (n = 47, 31.5%) than those whose preferred language was French (n = 35, 18.5%; χ2 = 9.11, p < .01). This remained significant in the multivariate regression. In focus groups, participants identified language as one aspect of a complex communication process between patients and clinicians and highlighted the importance of culture in the clinical encounter. Language status of patients plays an important role in their engagement with early psychosis services. Our findings underscore the value of establishing communication and cultural understanding in creating clinical/therapeutic alliance.
Introduction
Communication is the foundation of the clinician–patient relationship and in mental healthcare, effective communication can improve therapeutic alliance (Street et al., 2009), medication adherence (Thompson & McCabe, 2012), and treatment engagement (Dixon et al., 2016). Communication has been previously defined as the transmission of information through symbols (Berelson, 1964; Theodorson, 1969) and is a complex phenomenon with multiple components (Berlo, 1960). Language is one component of communication, and an important consideration when designing health services to improve the poorer health outcomes experienced by linguistic minority groups (Bauer & Alegria, 2010; de Moissac & Bowen, 2019; Landry, 2014).
In Canada, there are two official languages, English and French (Statistics Canada, 2017a). Canada's history of Indigenous settlement and subsequent colonization by and conflict between the British and French has had lasting effects on the geographic distribution, legal status and protection, and politics of the two languages (Landry, 2014). French is the sole official language of Quebec; New Brunswick is officially bilingual. In all other provinces and territories, English is the predominant language with federal services being offered in both languages. In parts of the country, speakers of English or French constitute recognized minorities (e.g., Francophones outside Quebec and Anglophones within Quebec). These “official language minorities” represent about 5.3% of the Canadian population (Statistics Canada, 2017a).
In Canada, universal healthcare is federally mandated but provincially organized and administered. No federal legislation exists for the provision of language access services for minority groups, though some provinces have elaborated policies for that purpose (Bowen, 2001) as others have established laws on active offer of services in the official minority language (Forgues et al., 2017; The Francophone Community Enhancement and Support Act, 2022). Consequently, linguistic minorities’ access to services in their preferred language varies substantially by region.
Francophones, a linguistic minority in Canada as a whole, constitute 80% of the population of Quebec (Statistics Canada, 2017a). Given the precariousness of French in North America, the provincial government of Quebec has implemented policies to protect its use and prevent its assimilation into Anglo-Canadian or American culture. For example, the 1977 Charter of the French Language, also known as Bill 101, promotes the ascendency of French in Quebec society: while designating French as Quebec‘s sole official language, the bill authorizes certain healthcare institutions, whose catchment areas contain sufficiently large Anglophone populations, to offer services in English. Yet, Quebec Anglophones have been reported to have lower access to and satisfaction with health services than Francophones (Landry, 2014; Zhao et al., 2021).
Accessibility of and engagement in treatment are particularly important in serious mental illnesses like psychotic disorders. Specialized early intervention services for psychosis aim to alleviate the suffering associated with these illnesses by identifying needs early, making services more accessible and engaging, and providing high-quality treatment, usually for two years (Iyer et al., 2015). Although such programs emphasize patient-centred communication and invest in keeping patients engaged in treatment, disengagement nonetheless remains a challenge (Lal & Malla, 2015). A number of sub-groups have been identified as being at high-risk for disengaging, including immigrants (Ouellet-Plamondon et al., 2015), those who misuse substances (Doyle et al., 2014), and individuals of low socioeconomic status (Doyle et al., 2014). To some degree, issues around engaging immigrant and ethnocultural minority patients in early psychosis programs have been explored (Maraj et al., 2018; Ouellet-Plamondon et al., 2015). However, the role of language in the provision of equitable care for psychosis has not been addressed. For example, it is not known whether individuals from official linguistic minority groups are more likely to disengage, despite language status being known to impact healthcare accessibility, its perceived suitability and outcomes.
We therefore examined service disengagement among those whose preferred official language was English vis-à-vis those whose preferred language was French in an early intervention program for psychosis in Montreal, Quebec. Because this program is based in a designated bilingual institution and offers all its services in both official languages, we expected that service disengagement rates would be similar between French and English speakers and that language would not be perceived as a significant barrier to care by either linguistic group.
Methods
Using a mixed methods sequential explanatory design (Ivankova et al., 2006), we studied the association between language and service disengagement in early psychosis. The quantitative analysis was conducted first and used to inform the qualitative data collection that followed, resulting in equal emphasis on both phases of the study. The quantitative analysis utilized a multivariate regression to investigate the relationship between preferred language and service disengagement. An inductive qualitative approach with focus groups was used to compare the linguistic and cultural differences in the perceived barriers to service engagement experienced by English- and French-speaking patients. Building on the quantitative findings, the qualitative protocol was then designed to gather information on the impact of language on the experience in care and grounded in the results of the quantitative phase (Ivankova et al., 2006).
Context
This study was conducted in a single early intervention for psychosis program in Montreal, the largest city in a province (Quebec) whose sole official language is French. Of Montreal's 4 million citizens (Statistics Canada, 2017d), 11% reported English as their only mother tongue, while 63% reported French as their only mother tongue. For their preferred official language to converse in, 73.5% of Montrealers endorsed French, 18.9% endorsed English, 6% endorsed both and 1.5% endorsed neither (Statistics Canada, 2017d).
The clinical team (approximately 30 individuals) in the early intervention program has always included a mix of individuals whose mother tongues include English, French, and other; many of whom are first- and second-generation immigrants; and who are either White or visible minority. In Canada, the term “visible minority” refers to “persons, other than Aboriginal peoples, who are non-Caucasian in race or non-white in colour” (Statistics Canada, 2011). Services are provided in either English or French by predominantly bilingual psychiatrists, case managers, and other clinicians. The few staff members who are more comfortable in English or French are assigned patients of the corresponding language preference. Throughout, patients have the right to request services in the official language of their choice.
The publicly-funded program is the only one for first-episode psychosis in its catchment area, which includes approximately 350,000 people (Iyer et al., 2015). Individuals are admitted if they have a diagnosis of non-affective or affective psychosis, not secondary to an organic brain disorder (e.g., epilepsy); are 14 to 35 years old; have a minimum IQ of 70; and have had no more than one month of antipsychotic pharmacotherapy. The program offers a two-year follow-up including case management, pharmacotherapy, and other psychosocial interventions (Iyer et al., 2015). This report uses data that was collected as part of a larger naturalistic cohort study approved by the Research Ethics Board at the Douglas Mental Health University Institute.
Phase one: Quantitative data collection
The first-episode program is a clinical-research program in which all patients are systematically asked to participate in research. Those who consent are included in the program‘s research database, from which the quantitative data was acquired. The quantitative study sample included all patients who had been admitted at least 24 months before August 2018, provided informed consent to participate in research, and had complete data for the variables of interest. Language was assessed as the official language in which patients preferred receiving services. We focused on preferred official language as our focus was on service engagement and services in our program are provided in English and French. Patients who identified themselves as preferring a third language (n = 7) or as completely bilingual (n = 4) were excluded from the quantitative analysis.
In line with previous analyses, a patient was considered to have disengaged from the service at the end of three consecutive months of no clinical contact (Anderson et al., 2013; Maraj et al., 2019; Maraj et al., 2018). Time to disengagement was calculated as the time from entry into the program until the first of the three consecutive months of no contact. Participants who moved or were transferred while in treatment were not considered to have disengaged and were censored (censoring occurs when the time-to-event is not known for a participant because the event of interest did not occur, the participant was lost to follow-up, or the participant withdrew from the study; Kleinbaum & Klein, 2005) at the time of move or transfer. Those who completed 24 months of treatment were censored at that time.
We assessed sociodemographic and clinical variables known to be associated with service disengagement in early psychosis (Conus et al., 2010; Doyle et al., 2014). These included age; sex; visible minority status; immigration status (non-immigrant or immigrant, including first- and second-generation) (Statistics Canada, 2011); duration of untreated psychosis (DUP; log-transformed); Social Deprivation Index and Material Deprivation Index (Pampalon et al., 2011) of patients’ neighbourhoods used as proxy measures of their socioeconomic status; family involvement in treatment (defined as presence or absence of contact with the treatment team) (Daneault et al., 2019; Maraj et al., 2019); and diagnosis of substance use disorder at baseline based on the Structured Clinical Interview for DSM-IV (First et al., 2002) (yes or no). Modal medication adherence within the first year was assessed. Antipsychotic medication adherence was assessed at baseline, months 3, 6, 9, and 12 based on self-report and family reports. Medication adherence was determined for each month and modal medication adherence was calculated over the first year of treatment. Patients were considered adherent if they had been adherent for >75% of the time (Dama et al., 2019; Daneault et al., 2019). DUP was defined as the time in weeks between the onset of the first psychotic episode (based on positive psychotic symptoms) and the commencement of adequate treatment, that is, taking antipsychotic medication for one month. It was calculated using the Circumstances of Onset and Relapse Schedule (CORS; Payne et al., 2006).
The Social Deprivation Index is drawn from Canadian census data and combines three census indicators: the proportion of the population aged 15 and over living alone; the proportion of the population aged 15 and over who are separated, divorced or widowed; and the proportion of single-parent families. The Material Deprivation Index combines three Canadian census indicators: the proportion of the population 15 years and over without a high school diploma (or equivalent); the employment to population ratio for those 15 years and over; and the average income of the population aged 15 years and over. Both indices are based on individuals’ postal codes and are reported as continuous variables based on centiles, with higher scores denoting greater deprivation (Pampalon et al., 2011).
Phase two: Qualitative data collection
The qualitative phase was added to more deeply explore and “explain” the results from our first phase (Ivankova et al., 2006). The focus group method was chosen because it allows patients to collectively construct responses by addressing each other‘s comments; supporting or disagreeing with one another; and sharing perceptions and experiences (Wilkinson, 1998). For the qualitative study sample, purposeful sampling was used. This technique is widely used in qualitative research to identify information-rich cases for the most effective use of limited resources. Clinicians briefly introduced the study to potential focus group participants. If they accepted to be contacted for further information, a trained research assistant contacted potential participants to further explain the study and invite them to the focus group. Before the focus group, the consent form was presented and consent obtained. Participants for each group were recruited based on their preferred language for receiving services to allow for homogeneity in language within each group (English or French). The English focus group was held in December 2017, and the French group in February 2018 in the early intervention program‘s conference rooms. Each focus group lasted approximately 2 hours.
Focus groups were conducted by trained qualitative researchers fluent in English or French, and digitally recorded and transcribed. Following the recommendations of Krueger and Casey (2009), focus groups included opening, introductory, key, and ending questions. The focus group guide included questions about interactions with the healthcare system, experience with the first-episode program, communication generally, and specific questions about language. It also asked for participant opinions about the connection between language and service engagement. Results from the quantitative analysis were shared during the groups. Groups were facilitated in a way that allowed openness to themes or topics that participants brought up themselves. Co-facilitators debriefed with each other after each group.
Data analysis
For the quantitative design, descriptive statistics are presented as proportions for count data and means with standard deviations for continuous data. Group differences between English and French speakers were determined using independent samples t-tests and Pearson's chi-squared tests for continuous and dichotomous variables, respectively.
Kaplan-Meier time-to-event analysis was conducted using the log-rank test to compare the probability of disengaging from services between English- and French-preferring patients. Multivariate Cox proportional hazards regression analysis, including preferred language, age, gender, education, substance use disorder, DUP, Social Deprivation Index, Material Deprivation Index, and family contact was used to identify factors associated with disengagement. Two post-hoc time-to-event analyses were conducted, the first replacing preferred language with immigrant status and the second replacing preferred language with mother tongue. Results are presented as hazard ratios (HRs) with 95% confidence intervals (CIs). All analyses were performed using SPSS version 24.
For the qualitative design, thematic analysis (Braun & Clarke, 2006) was used to identify, analyse, and report patterns within the data. Inductive and deductive procedures were used to develop themes relevant to our research question (Braun & Clarke, 2006). Analysis was conducted by three team members (two were fluent in both in French and English to allow coding in the original language; three team members were used to provide two coders for each focus group), who iteratively coded data and listed emerging themes about the role of language, perceptions about services, barriers to service engagement, and service engagement and language. Focus group transcripts were analyzed in their original language. The codebook was generated from a mix of English and French focus group content. The French quotes were translated by a fluently bilingual research assistant only for the purpose of this paper and are italicized for ease of identification. Themes from English-speaking and French-speaking patients were compared to determine similarities and differences.
Following individual analysis of the quantitative and qualitative data, all results were reviewed to conduct the mixed methods analysis. The results from both phases were integrated during the interpretation of all data (Ivankova et al., 2006). Convergence and divergence of the quantitative and qualitative data were examined for the primary research question.
Results
Quantitative results
Sociodemographic characteristics
Out of a total of 516 patients, 338 were included in the analysis and 178 were excluded due to missing data. Those excluded were older and more likely to be immigrants (see Table S1 in Supplemental Material). Of the 338 patients included in the quantitative analysis, 189 (55.9%) preferred receiving services in French, and 149 (44.1%) in English (Table 1). Of note, the language breakdown for participants was relatively proportional to that of the catchment-area population (the general distribution of the surrounding population is 57% French and 34% English; Statistics Canada, 2017b, 2017c, 2017f, 2017g). Language preferences were similar between White and visible minority participants, χ2(1, N = 338) = 2.92, p > .05.
Demographic data for participants included in quantitative analysis.
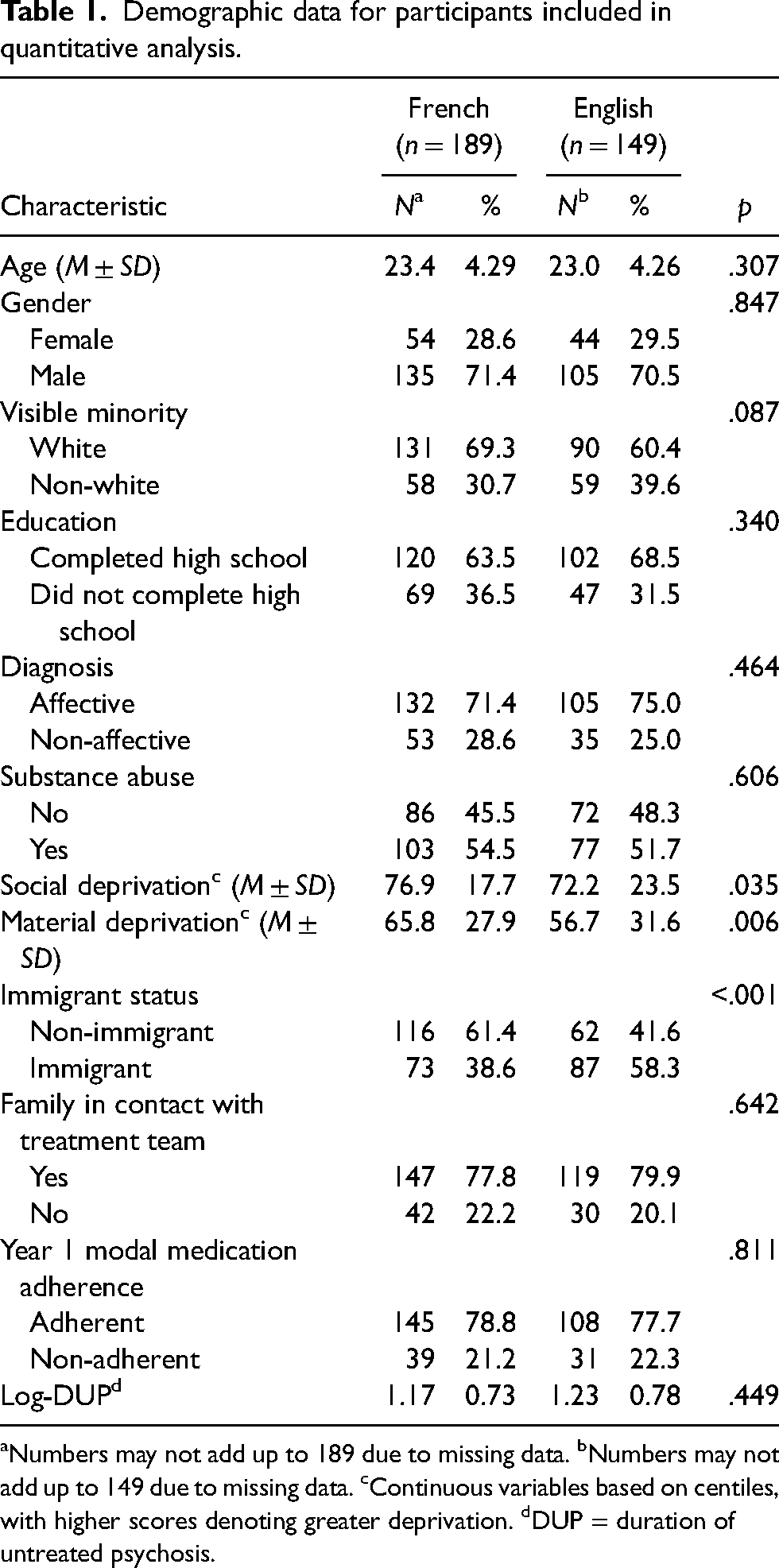
Numbers may not add up to 189 due to missing data. bNumbers may not add up to 149 due to missing data. cContinuous variables based on centiles, with higher scores denoting greater deprivation. dDUP = duration of untreated psychosis.
Among French speakers, 24.9% (n = 47) were first-generation immigrants; 13.8% (n = 26), second-generation immigrants; and 61.4% (n = 116), non-immigrants. Of the English speakers, 24.8% (n = 37) were first-generation immigrants; 33.6% (n = 50), second-generation immigrants; and 41.6% (n = 62), non-immigrants. Immigrants were more likely to prefer English than non-immigrants, 58.3% vs. 38.6%, χ2(1, N = 338) = 13.06, p < .001.
Deprivation indices were high in both linguistic groups, but French speakers demonstrated greater material and social deprivation. Material deprivation index scores for French speakers (M = 65.8, SD = 27.9) was significantly higher (i.e., greater deprivation) than English speakers (M = 56.7, SD = 31.6); t(336) = 2.78, p < .01. The Social Deprivation Index for French speakers (M = 76.9, SD = 17.7) was also higher than for English speakers (M = 72.2, SD = 23.5); t(336) = 2.12, p < .04. There were no differences between French and English speakers in age, gender, substance abuse, family contact, medication non-adherence or DUP (Table 1).
Service disengagement
A total of 82 (24.3%) patients disengaged. Those whose preferred language was English were more likely to disengage from services (n =47, 31.5%) than those whose preferred language was French (n = 35, 18.5%); χ2 = 9.11, p < .01 (Figure 1). Time-to-disengagement was 14.1 months (SD = 5.4) for French speakers and 10.5 months (SD = 5.8) for English speakers, t(80) = 2.84, p < .01.
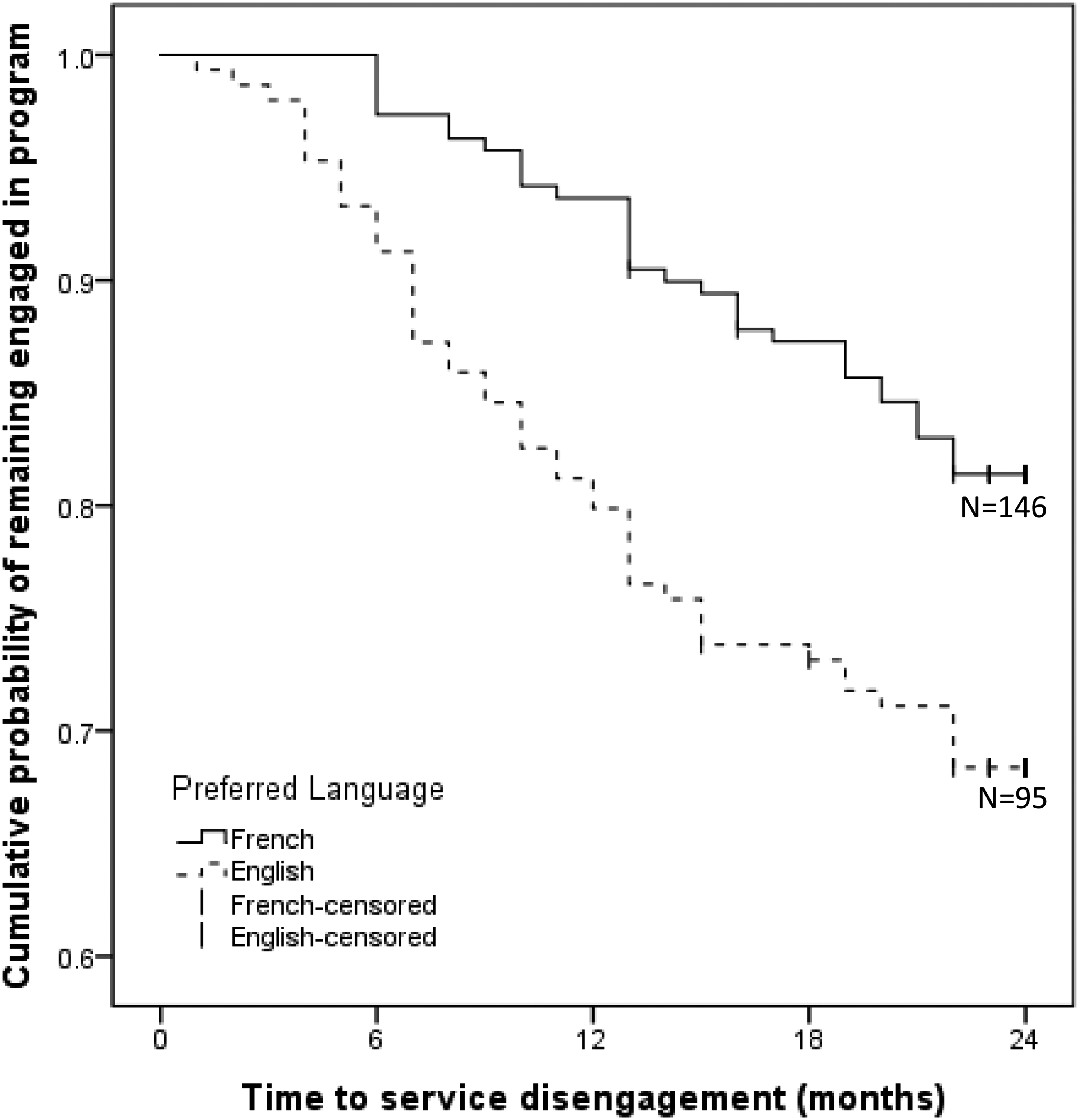
Time-to-disengagement curves for English and French speakers. French-censored: Data censored for French-speaking patients; English-censored: Data censored for English-speaking patients.
In the multivariate Cox proportional hazards regression that included known predictors of service disengagement, only preferring services in English, HR = 2.07, 95% CI [1.31, 3.28], and family involvement, HR = 1.97, 95% CI [1.20, 3.21], were associated with service disengagement (Table 2).
Cox proportional hazards regression analysis.
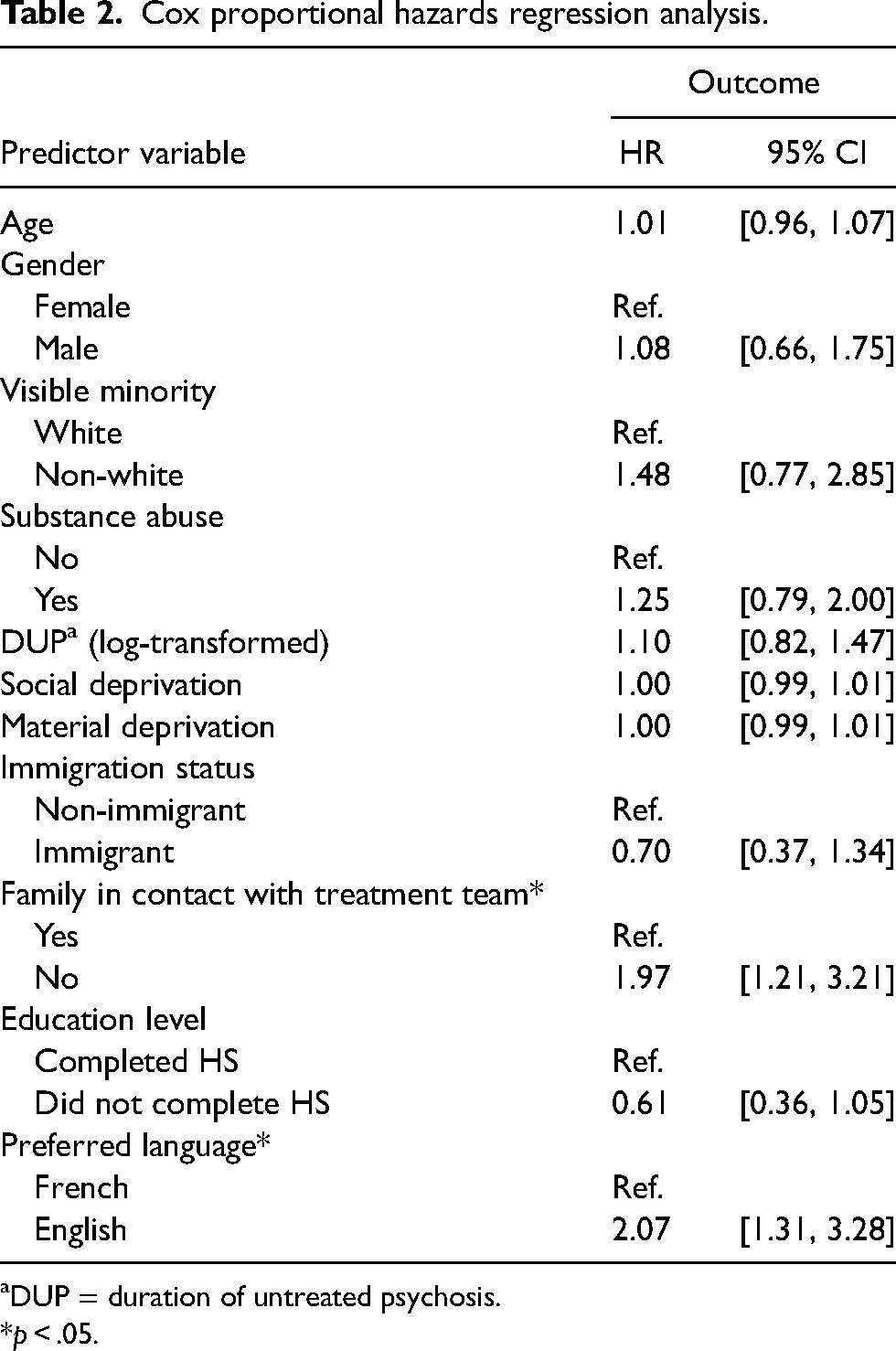
DUP = duration of untreated psychosis.
*p < .05.
A post-hoc time-to-disengagement analysis was done replacing preferred language with immigrant status (n = 338); in this analysis, there was no difference in disengagement between non-immigrants (n = 178, 24.7% disengaged) and immigrants (n = 160, 23.8% disengaged); χ2 = 0.12, p > .05 (see Figure S1 and Table S2 in Supplemental Material). Similarly, post-hoc time-to-disengagement analysis was conducted using mother tongue divided into three groups (English, French, and Other); the disengagement findings remained the same with English speakers more likely to disengage than French speakers or those whose mother tongue was neither English nor French (n = 325); χ2 = 7.79, p < .05 (see Figure S2 and Table S3 in Supplemental Material).
Qualitative results
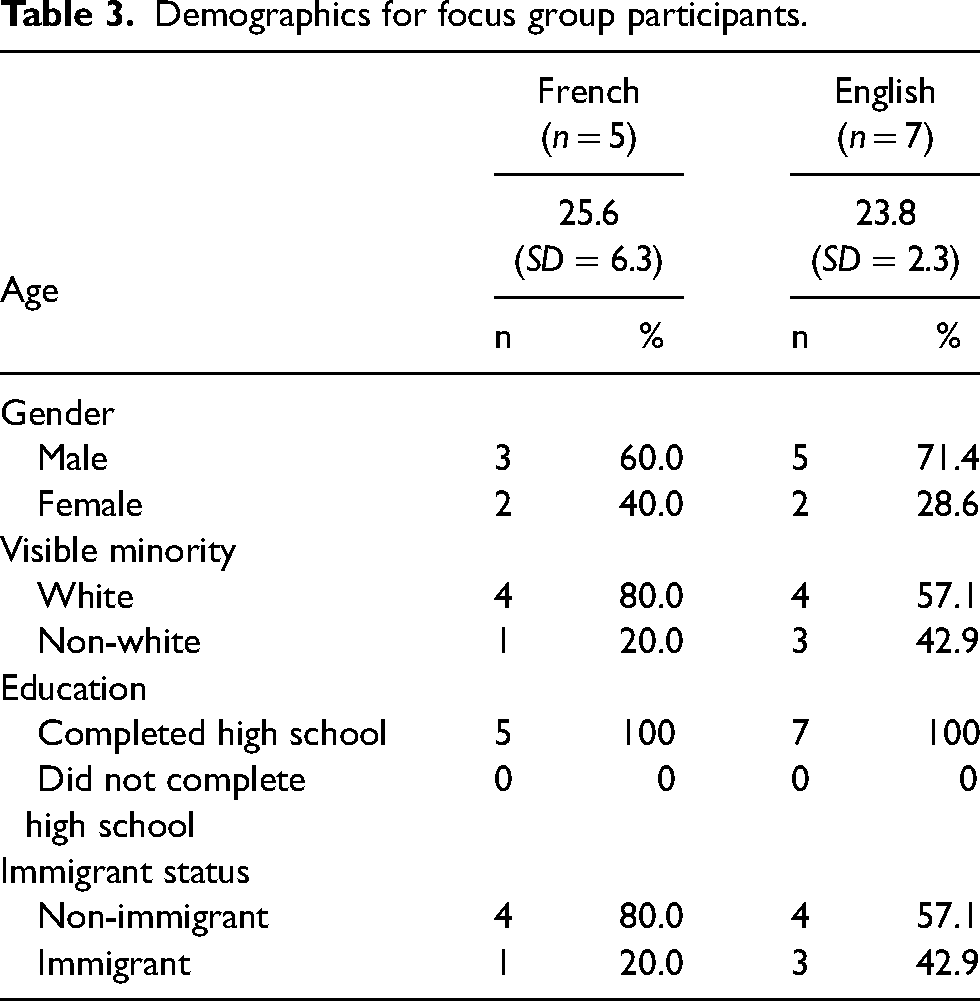
We conducted one English-speaker focus group (five males, two females) and one French-speaker focus group (three males, two females) (see Table 3 for participant characteristics).
Demographics for focus group participants.
Focus group results were similar between the two groups, each provided an overarching picture of the importance of communication as an essential mediator of the clinician–patient relationship (Figure 2). Experiences within the healthcare system prior to engaging with the program impacted the way participants initially approached communication with program clinicians. Regarding communication at the program, two themes were identified: (a) technical communication/syntax, referring to the structure and form of language; and (b) semantic communication/meaning-making, referring to the underlying information communicated. Each theme builds on sub-themes (including French and English) depicted in Figure 2 and described below. Furthermore, communication within the therapeutic relationship impacted the way the clinical encounter was experienced, which then resulted in a feeling of being supported or not, and at times, linked to a wish to continue engaging with care or not (Figure 1). We also describe differences in topics that emerged between the two groups.
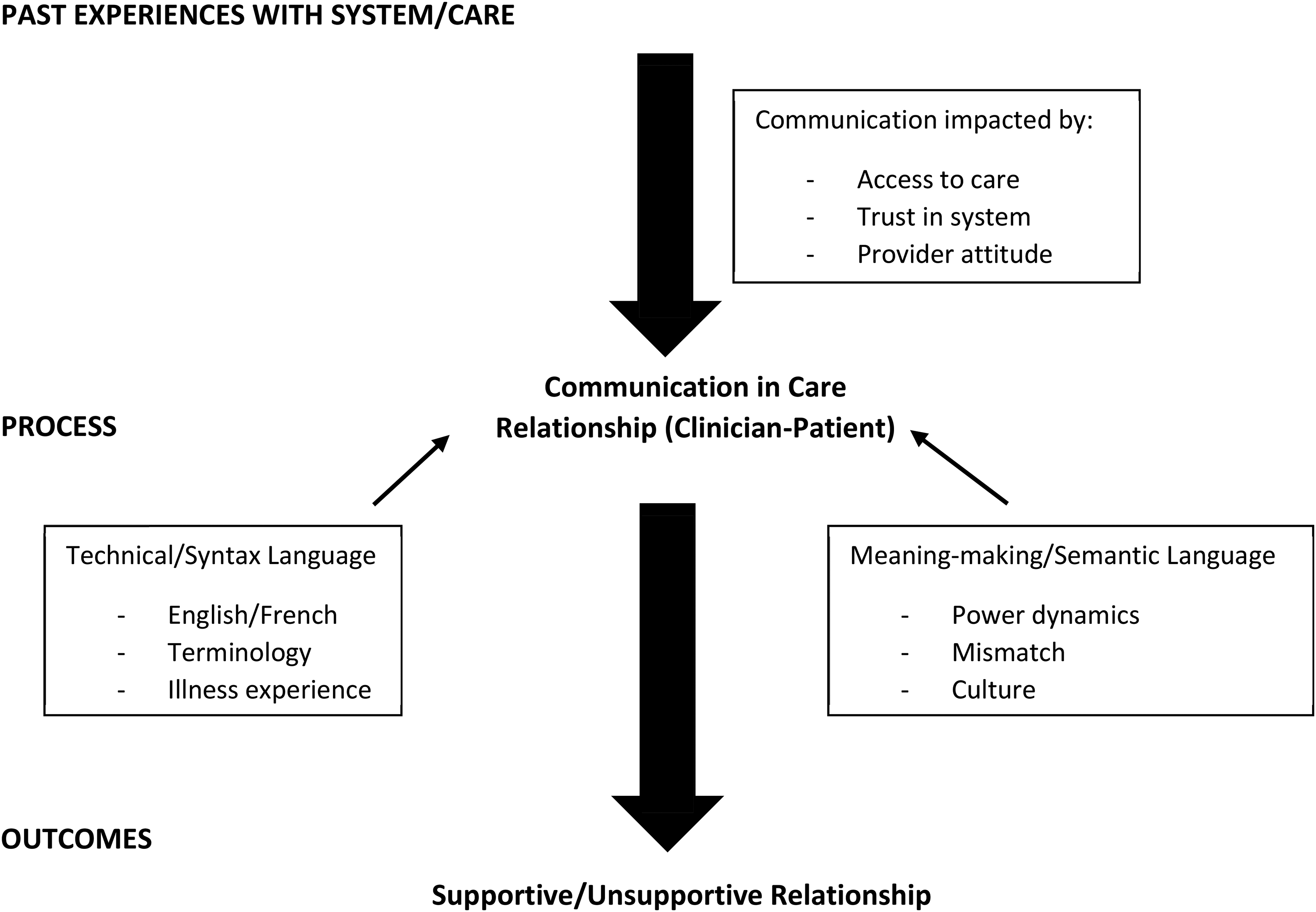
Factors related to communication in clinician–patient relationship.
Entering the therapeutic relationship.
Participants in both groups described having past experiences with the healthcare system that impacted the attitudes with which they approached care at the early intervention program, including the initial communication with their clinicians. These past experiences encapsulated a variety of system attributes, including access to care, development of trust in the system, clinician attitude and judgement: … like judgement of maybe how I appear and stuff like that. Say I’m a bit disheveled, some things like that, I feel like that might affect the care that I get. (Male, E3)
Sometimes it can be long in the hospital, I say that to someone and he turns his back and can start laughing at me. (Male, F3)
Communication and clinical interaction: Technical/syntax and semantic communication/meaning-making
Most focus group participants described the importance of communication in clinical interactions. In both groups, participants discussed the complexity of communication, identifying its multiple dimensions: a technical component comprising terms/words, syntax and structures; and a semantic/social component generated by the meanings that terms/words embodied: In my opinion, they [the program team] do speak the same language, as in like English, so topically it's the same. But underneath, no, I don't think they speak the same language as us. Like first of all, I know their background is very different…. So like the content like of every thought is different. So, they can't relate to us on a – I understand it's part of the job – not on genuine, genuine, genuine level… (Male, E2)
Multiple participants spontaneously and explicitly identified the two aspects of communication at different times throughout the focus groups, as evident in the following exchanges: Moderator: “[Participant's name], do you think your clinician speaks the same language as you?”
Participant: “Technically or metaphorically?” (Male, E5)
Moderator: “Do you feel that clinicians, the clinical team, speaks the same language as you?”
Participant: … “but is that a metaphor or is it literal?” (Male, F1)
Within each of these aspects of communication, multiple sub-aspects were identified. Technical communication incorporated issues related to the form, structure, and delivery of language. Three subthemes emerged from the focus groups as important to communication in the clinical encounter:
The use of French/English language: “I noticed that when talking to my psychiatrist, syntax was important. And depending on if you’re French or English… sometimes it's upside down…. And depending also if you think in French and then you’re talking in English, [you] might make those syntax mistake.” (Male, E2) The use of specific terminology (or diction) and differences in word choice between clinician and patient based on factors such as age, social status, and familiarity with medical terminology: “And to expand on language, a thing that I noticed and this isn't necessarily a matter of like French and English but like using the language that the patient or client uses to describe themselves and describe their experiences is super important for me. That was a thing that was a barrier for a while. Having psychs and stuff that wouldn't be using my vocabulary when I’m talking about my psychosis because I would describe it in like certain words.” (Female, E1) The impact of illness symptoms on communication. Participants described disturbances in their thoughts and ability to share their thinking in a clear and concise manner due to the symptoms they were experiencing: “For me, it's pretty hard to explain what I feel because of the voices and it's not everyone who will understand that the first time either” (Male, F3) The importance of culture (e.g., origin, beliefs, value systems) was highlighted as an important feature of the way individuals communicate: “Sometimes immigrants, they come here, they have a different mindset because they don't have the same culture, not the same religion, not the same way of talking to people. That affects the language and… you can spark emotions or receive emotions. So the emotional patterns are not necessarily the same and I think that plays a role in respect. Like let's say in my country, you could say something to someone, he won't get offended. But here, if you say the same thing, totally offensive.” (Male, E2) “I seriously think that even if you come from an immigrant family … maybe establishing a relationship with professionals will be more complex.” (Male, F1) The power dynamics between service provider and client. Participants shared experiences of feeling dismissed and disempowered during clinical encounters as a result of providers’ behaviours and attitudes experienced routinely during patient–clinician interaction: “And if a client… watches the psychiatrist starting to scribble down on his piece of paper, the client might freak out because he's like, ‘Okay, what's happening? I’m talking about something totally normal, I’m trying to communicate it.’” (Male, E2) “I’m a little helpless in this because I’m not the psychiatrist.” (Male, F1) The relational mismatch between client and service provider was highlighted. For example, a participant commented on having to adjust his communication to cover a generational gap: “So I find that that doctors are more of an old-school genre or era. So you got to talk to them a little bit how to say, in their way, you have to force yourself to adapt to that I find in order to get the best results or overly compensate to make them understand where you’re coming from in this day and age.” (Male, E4)
Discussions of semantic communication/meaning-making also incorporated social issues, such as those of identity and relationships. Again, three sub-themes emerged related to the clinical encounter:
Outcomes related to communication within the therapeutic relationship.
In daily relational interactions with their treatment teams, patients could feel supported or unsupported, valued or alienated, close or distant, depending on how communication with service providers unfolded: I think one thing that was a nice touch at one point was I have a bit of a technical-like mathematical background. And they tried to explain… in mathematical ways. Like when I was having these sorts of delusions-type problems, like delusions of persecution, delusions of reference, well, the probability that these things are really true is low. (Male, E1)
I haven't seen her [the psychiatrist] in a bit, and she’ll go through this list of questions. And it’ll be this like monotonous tone of like asking me really intense, deep personal questions that I just kind of need to disconnect from in order to answer them. And it's like a really dreary thing to be going into and knowing it's going to happen. (Female, E1)
I think the communication is really excellent. They offer us many options, like email or phone, directly. I like the fact that they offer us the ability to communicate at all times. (Male, F1)
You’ll arrive, you’ll start talking a little bit about your problems and they’ll quickly redirect you to your medication. Sometimes, it leaves you a little … since we were talking about communication, this could be a communication problem. It's that our communication intentions are not always the same. That can be room for improvement in terms of intervention. (Male, F1)
The nature of communication seemed to make patients desire or fear/avoid contact with their service providers. In choosing to engage or disengage, patients may weigh pros and cons, among which communication is likely an important one.
Language and treatment engagement.
In the focus groups, the role that patients’ preferred language played in their engagement in treatment did not emerge spontaneously. We stimulated discussion on it by presenting the results of the quantitative analysis to the participants. Participants were surprised to learn that the quantitative analysis demonstrated that English speakers were more likely to disengage: And there's actually I think, I hear a lot more English spoken at [program name] than I do French amongst people who work there. So I’m just wondering – so to me, I’m a bit surprised. (Male, E1)
Some agreed that language was important: I mean it's made me and [case manager name] have like a lot stronger of a connection because that's like our mother tongue for both of us. (Female, E1)
I seriously think that even if you come from an immigrant family, for example, or that you are an Anglophone, yes, maybe establishing a relationship with professionals will be more complex, but I do not think it will necessarily advance the quality and speed of your care. (Male, F1)
A few participants offered possible explanations for the quantitative findings: I think a lot of immigrants prefer to learn English as like a second language. So, I think that they might think in another language while they speak in English. So, the amount of reception that you get isn't the same because there's like more filters, it's like twice the filter…. So, to get through to them, to give a message, it's a bit harder. (Male, E2)
Maybe because they have fewer interventions because they are English-speaking or maybe there is less communicate with them because of their language. It can be a little discouraging. (Male, F1)
Some, particularly bilingual participants, reported having a different experience, feeling that speaking English or French was not important: I’m bilingual. So, there was not a language barrier and I believe, most of my clinicians here are bilingual as well. (Male, E1)
Yeah, I feel like everyone on the team that I interacted with, they spoke English and I feel like there was good communication. (Male, E3)
I do not think that speaking French will get things done faster. Everyone should be understood in their language. At some point you have to know yes or no in French to tell them what you need. (Male, F1)
Others acknowledged that language was important but went on to suggest that other aspects of communication were more relevant: And to expand on language, a thing that I noticed, and this isn't necessarily a matter of like French and English, but like using the language that the patient or client uses to describe themselves and describe their experiences is super important for me. That was a thing that was a barrier for a while. (Female, E1)
…when it comes down to the relationship between engagement and language is like if you sense that the overall tone of the language is one of trying to help you and being collaborative and so on, then I think engagement is likely to correlate positively. (Male, E1)
It depends on the person and not the language, I think. If he wants to, he’ll want to, he’ll find the time. Language, in my opinion, has nothing to do with it. (Male, F3)
Group differences.
While participants from both focus groups commented on the above topics, some topics were discussed at greater length in the English group and a number of topics emerged only in the French focus group. Issues related to culture and relational mismatch were touched on in both groups but discussed more in the English focus group compared to the French focus group (see examples above).
In the English group, some noted personal experiences related to issues with language: My psychiatrist… she was Francophone. So, we spoke English anyway but it [was] difficult at first just to talk to her because she didn't always understand what I was saying. I didn't always understand what she was saying because she had a hard time finding the right word. I’m just saying it's easier when you‘re speaking in your mother tongue in the way that comes most easily to you without having to pick your words too much. (Female, E1)
The biggest problem I think most memorably was always trying to make jokes and [my psychiatrist] didn't understand what I was saying. That's not really a big issue, I know… just now that I have a different person who's Anglophone, I find I have a funner, better, easier time just talking to him about what's going on in my life because he can immediately grasp what I’m trying to say. (Female, E1)
Mixed methods analysis
Comparison of the quantitative and qualitative findings revealed both convergence and divergence relating to the role of language in service disengagement. The quantitative analysis demonstrated a significant association between preferred language and service disengagement, with English speakers being more likely to drop out; the qualitative data demonstrated that language was considered significant in a variety of ways. Some shared personal experiences that aligned with this and others shared possible explanations. Divergence from the quantitative findings was evident in some participants discussing having not experienced language per se as an important factor in receiving care but seeing language as part of a larger and more complex communication process: In my opinion, they do speak the same language as in like English, so topically it's the same. But underneath, no, I don't think they speak the same language as us. (Male, E2)
Notably, immigrant status was identified as important by participants in the qualitative phase and informed the post-hoc analysis. However, it was not associated with service disengagement in either the initial or post-hoc time-to-disengagement analyses.
Discussion
To our knowledge, this is the first study to use a mixed methods approach to study service engagement for linguistic minorities in first-episode psychosis. Given concerns about the provision of equitable healthcare for linguistic minority groups (Landry, 2014), we investigated the role of language in service disengagement. Overall disengagement rates were relatively low; yet, in an institution required to provide services in English and French in a city that has a large Anglophone population, we found that English speakers were twice as likely to disengage before the two-year mark from early psychosis care compared to their French-speaking counterparts. This initial finding was further explored through qualitative methods that shed light on the importance of communication in care and identified language as one component of a complex communications process.
Technical and semantic communication
Turning to the qualitative data, we see that communication in care is an important topic for patients. When we ask about language, they spontaneously identified two aspects of language: the “technical” and the “metaphorical”. Their responses align with theory that identifies both technical (or syntax) and semantic communication (August et al., 2011). Participants identified that the technical aspect of communication impeded communication in the clinical encounter if they felt their clinician did not fluently understand their preferred language (English or French), as well as if their clinicians used terminology they could not understand or if their illness symptoms impacted their ability to communicate their thoughts. Importantly, less concern was demonstrated towards these technical aspects, while more time was spent discussing the difficulties encountered with semantic communication.
Beyond the difficulties posed by the technical aspects of communication, participants strongly felt that issues of power dynamics and relational mismatch impacted communication between clinicians and patients. The existence of a power hierarchy between patient and clinician contributed to patients feeling judged, disempowered, and excluded in their clinical encounters. A disconnect between the realities, including age and life experience, of clinicians and patients was identified as an obstacle to optimal communication. Participants felt that the use of medical jargon, note-taking and the emphasis on medication impacted how messages were conveyed and received, and the ability to feel connected in the therapeutic relationship. They expressed a desire for clinicians to connect to patients’ interests, understand their perspectives and be more open to patient-generated solutions. Overall, the quality of patient–clinician relationships impacted the flow and openness of communication, which, in turn, further affected the relationships.
Culture and communication
Focus group participants identified various aspects of culture and identity, including country of origin, age, and sexual orientation, that impacted on communication. For the purpose of this article, culture was defined as “systems of knowledge and practice that give our lives identity, meaning, and purpose” (Kirmayer et al., 2014, p. 1).
The diversity of English speakers in Montreal (Donovan, 2019) stems from multiple waves of immigration, starting with the British in the 18th century and then Irish, Black Canadians, and multiple European groups (Jewish from Eastern Europe; Italians; Greeks) (Linteau, 2015). More recently, Montreal has welcomed immigrants from English- and French-speaking nations around the world, has seen a rise in immigrants from Asian countries (Donovan, 2019), and a growing population of Indigenous peoples (Statistics Canada, 2017d).
Quebec employs its own immigration policies, criteria and conditions, distinct from the rest of Canada (Labelle, 2015). Overall, immigrants make up less than 14% of the Quebec population, and 86% of Quebec's immigrants live in Montreal. In Montreal, 23% of the population are immigrants (Statistics Canada, 2017e). Quebec has a policy of interculturalism that accepts and encourages interaction between diverse cultural groups, while insisting on maintaining the primacy of the French language and culture (Brosseau & Dewing, 2018). This stance has been reflected in government legislation, objectives, and communications (Brosseau & Dewing, 2018). The integration of immigrants, inequality, and discrimination were identified as areas of concern in the 2000s and the Ministry of Immigration and Cultural Communities was created in 2005 with the aim of improving intercultural relations (Brosseau & Dewing, 2018). Despite these efforts, respect for diversity remains an issue in the province. Recently, Quebec has passed Bill 96 (2022) and Bill 21 (2019). Bill 96 is legislation that outlines the increased requirements for the use of French for public services and businesses operating in Quebec or those transacting with Quebec clients and customers. Bill 21 is legislation that prohibits the wearing of religious symbols by public workers in positions of authority and mandates that individuals must have their face uncovered when giving or receiving specific public services. While each has clearly defined aims (i.e., to promote the use of the French language and to promote religious neutrality, respectively), both have been criticized for discrimination against marginalized populations (e.g., linguistic and religious minorities; Kinsinger, 2019).
Also notable is that the equality of women and men is endorsed as a fundamental value of Quebec society in government policies. In fact, in 1975, Quebec adopted the Charter of Human Rights and Freedoms, which officially prohibited any form of discrimination based on gender (Commission des droits de la personne et des droits de la jeunesse Québec, 2022). Within the English-speaking group in our study, there is significant heterogeneity in multiple aspects of identity including race, ethnicity, migration experience, religion, and social class. Thus, while English-speaking participants have a common preferred official language, they differ in other aspects of cultural identity.
Most service users in the program seem to fall into two groups—White non-immigrants (so the service user or their parents did not immigrate to Canada) and visible minority immigrants (the service user or at least one parent immigrated to Canada). Quantitatively, consistent with our previous findings (Maraj et al., 2018), immigrant status did not significantly impact service disengagement rates. Nonetheless, ways of communicating and engaging with institutions, including healthcare, may indeed differ between immigrants and non-immigrants. Also, our sample included 18% of individuals whose mother tongue was neither English nor French. Although they were all able to communicate in one of the two official languages in which services were provided, it may have been “harder” for them to discuss psychological experiences and emotions in a language that is not one's mother tongue.
Overall, as our qualitative more than our quantitative findings suggest, intersectionality of identity (Crenshaw, 1989) may be important in fully understanding the way people engage with mental health services. Perspectives on mental illness, accessing healthcare, and the relationships with clinicians vary greatly across cultures (Gopalkrishnan, 2018). Understanding these cultural differences and nuance is imperative, as culture impacts on communication (Carbaugh, 2007; Hall, 2006), and language is just one facet of culture.
Of note, focus group participants identified past experiences with healthcare as important in approaching their present experience. These past experiences may also be enmeshed with their cultural identities. While communication in the clinician–patient relationship is important in developing a supportive relationship, there are indeed a variety of other factors that may play into an individual's decision to come to an appointment or not. Some of these reasons may be embedded in culture—such as stigma (Franz et al., 2010) and explanatory models (Maraj et al., 2017).
Strengths and limitations
Taken together, we have demonstrated that there is a discrepancy in service utilization between English and French speakers in a bilingual early intervention for psychosis program in Montreal, Canada. Caution must be applied to interpretation of these results. The complexity of communication, language, and disengagement make a simplistic interpretation misleading and inappropriate. Importantly, the program of study is a bilingual service, with the vast majority of clinicians being bilingual and language-matching applied in the few cases where the clinician is only comfortable in one of the official languages. Additionally, all programming is provided according to established standards of care by individuals with the necessary training and is offered in both languages. Given these longstanding features of the program, this leads us to believe that the present findings are not likely due to language mismatch.
Furthermore, it is unlikely that the availability or quality of service differs between the linguistic groups; it is reasonable to believe that language, while an important construct, is also an indicator of more complex differences related to the heterogenous cultural groups that have been reduced to “English speakers” in the present study.
This study has been carried out in a single early intervention for psychosis service. However, one can surmise that the experience of availing healthcare may also be impacted by linguistic minority status elsewhere, including for English-minority groups across Quebec, Francophone communities in other provinces, and linguistic minority groups in other countries. Thus, considerations of preferred language for receiving services are important in delivering equitable access to mental healthcare everywhere.
Our study had several limitations. Due to the number and demographics of patients excluded due to missing data, there is potential for selection bias and possible limitations in representativeness. Future work should attempt to discern the robustness of these findings through additional data gathering to minimize missingness, particularly data missing not at random, and advanced statistical techniques. We used patients’ preferred language as services are only offered in English and French. Even if clients received care in their preferred language, it may not have been their mother tongue. Themes around verbal communication emerged in this study, however, an analysis of non-verbal communication between clinicians and patients would be important to more fully understand the role of communication in therapeutic engagement.
Our relatively small sample size precluded the investigation of interactions between demographic variables, and our assessment of culture in the present study is limited to the use of the variables of language, immigrant status, and visible minority status, which does not allow for the unpacking of intersectional identities and culture. Each of these groups is highly heterogenous and future work would benefit from larger sample sizes allowing for more specific characterization of groups in quantitative analyses and more fine-grained insights in qualitative analyses. Such work has the potential to illuminate how diversity, immigrant status, speaking English in a French-majority province, and other intersecting identities may interact to influence experiences of care and engagement. Our focus group participants were also heterogeneous in regard to service utilization, language ability, and cultural identity, thereby limiting the conclusions that can be drawn from qualitative data regarding the role of culture. Importantly, we recognize that language issues come draped in a variety of political nuances related to identity and inclusion in Quebec; this politicization of language may impact patient engagement in their communities and in their treatment in complex ways that patients (and clinicians) may not be aware of. This politicization of language, including public dialogue with hostile and discriminatory undertones, in day-to-day life in Quebec, and the lack of awareness or deep understanding of the multitude of influences at play, make it unlikely that this complexity would be articulated in a focus group.
Furthermore, in line with previous research, disengagement was defined as three consecutive months of no clinical contact. This is one of several operational definitions of disengagement, reflecting the complexity of this construct. While there is evidence of poorer outcomes for those who disengage from treatment, we also recognize the possibility that not returning to care could be related to improved functioning, sustained recovery or simply finding oneself no longer needing the service.
Our focus groups also included patients who remained sufficiently engaged in services and, as such, may not have been representative of the perspectives of those who had disengaged from treatment. Those remaining in care may have had different experiences in care as compared to those who disengaged. They may not face the same challenges, or they may have resources that enable them to remain engaged despite these challenges. Moreover, previous work (Cowan et al., 2020) from our program that included individuals who were engaged in and who had disengaged from services demonstrated that dis/engagement was a dynamic process and may sometimes reflect positive progress such as engaging with life goals. We were limited in our ability to investigate what contributed to disengagement given that our focus group participants had not disengaged from the program. We also acknowledge that engagement (often categorized as “engaged” or “disengaged”) may in fact represent various positionalities with respect to services and recovery.
Future directions
Future research should examine whether linguistic minority groups in other geographic contexts have poorer rates of engagement in early psychosis care; and how language, communication, and culture interact to affect engagement in and the outcomes of mental healthcare. Future research may seek to better understand the impact of clinician identities (including age, gender, visible minority) on communication and therapeutic alliance. Overall, patients also consistently identify sub-optimal communication as a problem—making it important to develop and evaluate strategies to enhance clinician–patient communication.
Conclusion
This study identifies the need to improve communication between patients and clinicians in early intervention programs for psychosis and to consider the role of culture in our clinical encounters. Communication between patients and clinicians can be enhanced not only by ensuring that they are matched by language (English or French in our case) but also by organizing communication around goals of fostering shared understanding, trust, mutual regard and alliance, which, ultimately, will lead to better engagement. Services should also consider the use of translators and cultural brokers when necessary.
Overall, the language status of patients plays an important role in their engagement with early psychosis services. The complex interaction of patients’ preferred language with other aspects related to cultural identity and social status, such as country of origin, age, power dynamics and knowledge of technical terminology, impacted communication during clinical encounters, and ultimately, on engagement with services. Our findings thus underscore the value of establishing communication and cultural understanding in creating clinical and therapeutic alliance.
Supplemental Material
sj-docx-1-tps-10.1177_13634615231167067 - Supplemental material for Engaging with care in an early intervention for psychosis program: The role of language, communication, and culture
Supplemental material, sj-docx-1-tps-10.1177_13634615231167067 for Engaging with care in an early intervention for psychosis program: The role of language, communication, and culture by Anika Maraj, Manuela Ferrari, Kathleen MacDonald, Matthew Peters, Ridha Joober, Jai L. Shah, and Srividya N. Iyer in Transcultural Psychiatry
Footnotes
Acknowledgements
We would like to thank Matthew Peters, Kevin MacDonald, and Nicole Pawliuk for their contributions to the successful completion of this project.
Author note
Jai L. Shah and Srividya N. Iyer are senior authors with equal contributions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a combination of grants from the Institute of Health and Social Policy, Language and Health Student Program (Maraj); National Institute of Mental Health (MH093303), Canadian Institutes of Health Research (CIHR), CIHR New Investigator Award (Iyer), Fonds de Recherche du Québec – Santé (FRQS) Clinician-Scientist Award (Shah, Iyer) and the joint doctoral training award from FRQS and the Unité Soutien- Stratégie de recherche axée sur le patient Québec (MacDonald).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.