
Abstract
Teenage pregnancy rates in Uganda are among the highest in sub-Saharan Africa. Child marriage is often the result of unmarried teenage pregnancy and is recognised by Uganda's government as a form of sexual violence and an outcome of inequality. However, unmarried motherhood incurs stigma and shame within traditionally living rural communities. Using co-produced Open Space and ethnographic methods, we examined the psychosocial impact of unmarried motherhood on girls and their communities, and explored problem-solving with key local stakeholders. Findings indicate that girls experience extreme stress, social exclusion and rejection by their families, and experience bereavement from school expulsion and the loss of their career aspirations. Depressive symptoms and suicidal behaviour are reportedly not uncommon among this population group. Community and family efforts to promote marriage for these mothers to avoid social stigma increased the mothers’ feelings of depression, whereas mothers who became independent appeared to fare better psychologically. Community members and local stakeholders demonstrated a willingness to act locally to reduce the negative impacts of unmarried motherhood but lacked knowledge and support resources. Our findings indicate that mental health promotion for teenage mothers is likely to be better served through empowerment strategies rather than marriage and, in a context of poor mental health service access, there is a substantial role for community mobilisation and the promotion of self-help strategies to support teenage mothers. This study raises important points regarding different community understandings of depression and indicates collaboration between professionals and communities for a values-based approach.
Introduction
Uganda's teenage pregnancy rate is one of the highest in sub-Saharan Africa (Ochen et al., 2019). By 2018, one in four adolescent women (15–19 years) were already mothers or were pregnant with their first child. Teenage motherhood is higher in rural areas (27%) than in urban areas (19%) (Uganda Bureau of Statistics (UBOS) and ICF, 2017) resulting in high levels of teenage single motherhood and there have been increases during Covid lockdown periods in specific districts, including Mayuge and Kasese (UNFPA Uganda, 2021).
Teenage mothers in Uganda face moral barriers to remaining or returning to school after conception (Ministry of Education and Sports, 2020), and social and moral norms require the mother to marry the father (UNICEF, 2015). Marriage is therefore a common mitigation against the moral issue of unplanned teenage pregnancy. According to the Uganda Demographic Health Survey (UBOS and ICF, 2017), child marriage is still common in rural areas and among communities experiencing poverty and low education, and younger brides are more likely to experience domestic and sexual violence, be HIV positive and experience obstetric problems in childbirth.
Despite the legal age of consent being 18, an acceptance of child marriage persists and is reinforced by culturally embedded gendered social roles attached to parenthood and adult status within the community. Marriage is patrilocal and marriageable girls are valued because they carry the lineage of their husband's family, and so attract bride wealth into their parental family (UNICEF, 2015). It is expected that a girl's family are paid for the marriage, which also presents a motivation for child marriage in poor households (Nabugoomu et al., 2020).
The burden of child marriage is likely to fall unequally on girls, who face embedded gender and human rights inequality in education, economic power, land rights and justice, and lose further rights when married. For Datzberger and Le Matt (2018), social and political gender stereotypes are reinforced in Uganda by an education system that offers equality of access to girls, but is structured and practised in a way that undermines emancipation and the means to empowerment. Both curricula and teachers’ attitudes result in common experiences of sexual harassment, subordination and moral approbation for being female, and present what Kyoheirwe Muhanguzi (2011) describes as sexual double standards, whereby the girl is both to blame and victimised by sexual abuse, unwanted pregnancy and HIV infection.
Adolescent and maternal mental health
Maternal health and teenage pregnancy in low- and middle-income countries (LMICs) have been a particular focus for intervention (UNICEF, 2015; World Health Organization (WHO), 2020), including efforts to reduce young people's vulnerability to HIV and AIDS (Kalibala & Elson, 2010), and meet obstetric needs in adolescent pregnancy (WHO, 2020). However, there has been little examination of the psychosocial health issues associated with teenage pregnancy, especially among unmarried teenage mothers. Mental health in LMICs is included in the United Nations (UN) Strategic Development Goals (SDGs), and elimination of child and early marriage is a target in the SDG for gender equality and empowerment of women and girls (United Nations, 2020). However, the wider social environment in which young women live is seen as a key challenge in this population's mental health (The Academy of Medical Sciences, 2018). Globally, depression is one of the main health risks for adolescents, and suicide is the second leading cause of adolescent mortality (WHO, 2018), with depression and anxiety shown to be significant among pregnant women, particularly when associated with family stresses (Redinger et al., 2020). Identified factors associated with female adolescent depression in LMICs include low socio-economic status (SES), interpersonal and family-relating problems, problems with in-laws, domestic violence, lack of a partner or social support, unemployment and low levels of schooling (Fisher et al., 2012; Husain et al., 2006; Nakku et al., 2006). Nyundo et al. (2020) recently identified factors associated with depression among Ugandan adolescents, such as being female, bullying, loneliness and involvement in (unpaid) family work. Rural living was also significantly associated with depression in both Ugandan male and female adolescents.
Nyundo et al. (2020) suggest tension between school attendance and the need to earn a family household income presents an increased burden on rural-living adolescents. In addition, Miller et al. (2021) suggest that Uganda's recent rapid urbanisation marginalises more traditionally living rural communities and creates a greater socio-economic divide. They also suggest that although Uganda's endemic HIV may contribute to social marginalisation, it may also contribute biologically to rates of depression through chronic inflammation and reduced serotonin and tryptophan levels (Miller et al., 2021).
Ugandan mental health services
Uganda has one national psychiatric hospital, near Kampala, and five regional hospitals offering psychiatric services. There is no universal coverage for mental health but a network of community out-patient facilities provides follow-up care, albeit underfunded (Molodynski et al., 2017). The Programme for Improving Mental Health Care (PRIME) initiative is supporting the integration of mental health expertise into primary care (Nakku et al., 2019; PRIME, 2019). This is important for improving access because poor road infrastructure and bi-annual rainy seasons make travelling to hospitals difficult, although more problematic is the shortage and distribution of trained staff. There are reportedly fewer than 50 psychiatrists and currently 3 clinical psychologists working in the public sector, supported by 19 medical social workers, 135 psychiatric clinical officers and 1875 qualified psychiatric nurses (Kalani, 2021), most typically located in urban hubs. The private sector and non-governmental organisations (NGOs) provide substantially more allied mental health professionals (Kalani, 2021), but these are not universally available. The two regions of our study are in rural areas that require a day's travel on foot to access primary care, and a limited and unreliable call-out service for community mental health care.
Additional distractions in accessing mental health services stem from the use of traditional healing, often the first or only source of help-seeking, which can delay medical assessment, introduce exploitation (Molodynski et al., 2017) or counter medical advice (Zingela et al., 2019). Use of traditional healers in sub-Saharan Africa is common (Abbo, 2011; Patel, 2011; Zingela et al., 2019), particularly in Uganda for people with severe mental illness (Burns & Tomita, 2015). A study by Quinn and Knifton (2014) reveals a complex relationship between moral, religious and social reasons for using traditional healers, overlaid by some acceptance of western medical understanding of mental illness. Quinn and Knifton indicate some advantage from traditional beliefs in that a person who is ‘cursed’ with mental illness may be seen to be serving the community by carrying the curse for others. This can still result in social isolation, inequality and human rights abuses. Working with community leaders and traditional healers in the interests of shared decision-making and cultural sensitivity can be part of an effective community outreach for mental health (Ojagbemi & Gureje, 2021). However, efforts to overcome the perceived polarisation between western medicine and traditional values through co-creative processes for dialogue may still be undermined by a lack of trust of medical services among healers (Akol et al., 2018).
Non-psychotic mental illnesses such as depression tend not to be regarded in medical terms in many African cultures and can therefore be overlooked by communities, relatives and practitioners. Johnson et al. (2009) found diverse conceptualisations of depression according to social characteristics, indicating that less-educated community members were more likely to identify depression in physical or functional terms (i.e., loss of weight, being unable to work), with the more educated ascribing psychological terms to depression symptoms. This can also make it difficult to make a diagnosis in rural communities where only somatic symptoms are reported (Fischer et al., 2019). Sarker et al.'s (2018) exploration of the conceptualisation of perinatal depression suggested that understanding of the illness is embedded in social and physical explanations such as the status of being pregnant in the community, with the type of help-seeking dependent on the explanation of the affliction.
In response to concerns expressed by a Ugandan-based sexual health NGO (hereafter ‘The NGO’) about the mental health of unmarried teenage mothers, this study aimed to explore the particular mental health impact of unmarried pregnancy among young rural Ugandan girls.
Study setting and culture
Our aim was to establish community-based evidence with which to examine the psychosocial impact and community conceptualisations of unmarried teenage pregnancy, with a view to informing community action projects in tackling the mental health consequences for unmarried teenage mothers.
Uganda has a predominantly rural population, and this study was conducted in two contrasting rural districts. Mayuge in south-east Uganda is relatively socially stable but situated in the wider region of Busoga, which is currently experiencing high rates of teenage pregnancy, partly associated with Covid-related school closures (Marie Stopes, 2021). Kasese district on the border of the Democratic Republic of Congo (DRC) has experienced recent civil war and refugee immigration, floods and outbreaks of Ebola virus. General poverty in all rural areas, poor infrastructure and geographical distances constrain access to essential services such as reproductive or mental health services.
Uganda has free universal primary education (UPE), but families need to meet the costs of scholastic materials and meals, as well the costs of secondary education. Despite accessible education, Uganda has a school dropout rate of about 30% (Ministry of Education and Sports, 2017). Schooling is also less valued for girls and is governed by strict criteria inherited from Christian colonial standards, which result in gender inequality and pregnant students being expelled (Sekiwu et al., 2020). All districts follow a patrilineal system, whereby children belong to their husband's clan (Karimli et al., 2012), hence primary responsibility for the care of children resides with paternal kin. Polygamy is highly prevalent, and stepmothers in a household are not uncommon. However, the system is disintegrating: HIV and AIDS have resulted in high numbers of orphans and an increase in maternal relatives taking care of children, with associated poverty, child exploitation, reduced education and mental health problems (Karimli et al., 2012, 2019). Child marriage is a common expectation and a social norm in many districts, and becoming a parent is seen as an indicator of adulthood. Because brides can be a source of wealth to their families (UNICEF, 2015), pregnancy outside marriage may interfere with this value system. Despite early engagement in sex, there is limited access to family planning services for adolescents in rural communities owing to barriers of availability, cost and moralisation against contraceptive use outside marriage (Erone et al., 2020), hence adolescents are more vulnerable to unplanned parenthood.
Method
We deployed a qualitative, ethnographic approach to fieldwork and data collection, carefully crafted to suit the needs of and acceptability to the community under investigation. Two principal methods of data collection were used: community group meetings with teenage mothers and village members, and Open Space workshops (described below) with key stakeholders to generate visual artefacts such as participant-generated charts and posters. Simultaneous and retrospective written records (fieldnotes) were also made by the researchers for both methods and unplanned ad hoc encounters during fieldwork. Co-produced approaches to data collection, informed by the principles of ethnography, have proved useful in other areas of qualitative research with seldom-heard communities (Andrade & Angelova, 2020; Clayson et al., 2018; Cox et al., 2016) and this guided our decision to adopt them in this context.
Participants
Community meetings
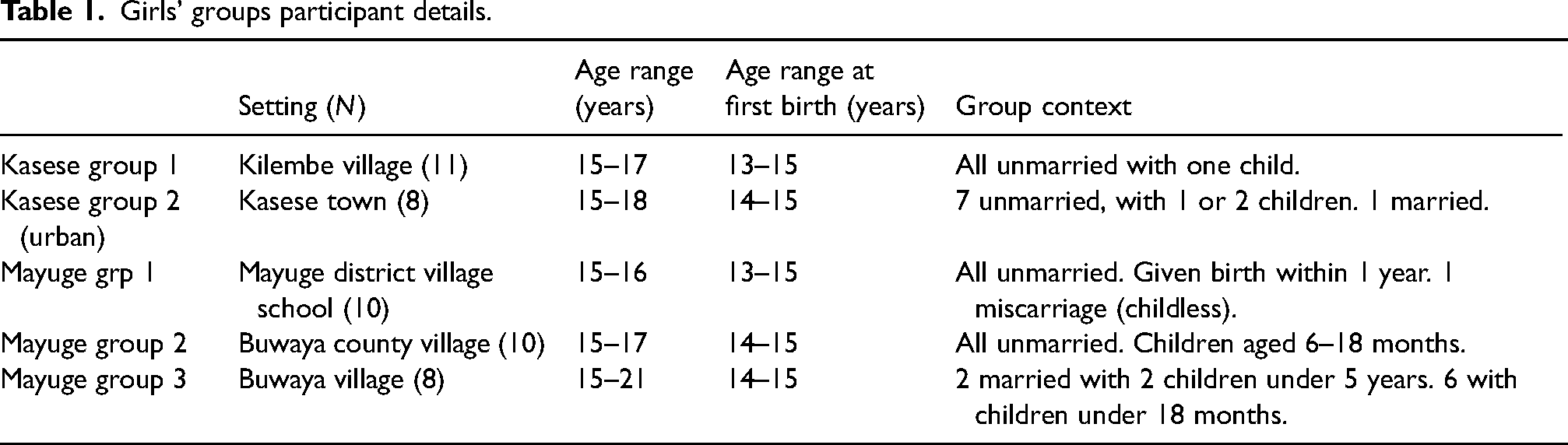
Five discussion groups, two in Kasese and three in Mayuge, were undertaken with girls and women who had conceived during adolescence and outside marriage, and were currently attending skills training with The NGO. The majority had conceived at or before the age of 15. Their age at time of participation ranged from 15 to 21 and approximately 80% remained unmarried (Table 1). One Kasese group had moved from their villages to town and are referred to here as the Kasese urban group. In addition, two open village meetings that included male and female elders, parents and whole families were held in Mayuge. To promote engagement, trust and rapport with local communities, The NGO provided interpreters conversant with the languages spoken (Lusoga, Lukonzo and Runyoro-Rutooro) and the cultural norms of the participants. Village meetings typically comprised 15–20 attendees, of whom mainly only the village elders contributed (approximately 5–10). Girls’ groups comprised between 8 and 11 members (Table 1).
Girls’ groups participant details.
Stakeholder workshops
A community stakeholder event was conducted in each of the districts using Open Space Technology (OST). Attendees (Kasese n = 12, Mayuge n = 13) included local councillors and politicians, mental health and social work practitioners, service managers, other health practitioners, NGO representatives, disability representatives and local radio news journalists. These meetings were conducted in English.
Data collection
Community meetings
Data collected from meetings with unmarried mother groups and village communities was generated largely from unstructured reflexive discussions focused on a priori themes (mental health, causes and impacts of pregnancy) and conducted in the local dialect, then translated into English. Data were collected in the form of fieldnotes written contemporaneously, and as reflections following the meetings.
Open space workshops
OST (Lightfoot et al., 2003; Owen, 2008) was used for the stakeholder workshops. This is a participatory, structured and time-limited consensus-forming methodology; a collaborative method of enquiry that ‘sits’ somewhere between a conventional qualitative focus group method (where a specific issue is brought to the participants for discussion) and a more activist, co-produced methodology (where participants have full control over the direction of conversation and the prioritisation of topics to consider and report upon). Unlike focus groups, where talk and dialogue form the principal mode of communication, our use of OST encompassed talk, text (as written contributions) and other media. In this case, stakeholders were recruited by The NGO on the basis of the topic being the issue of mental health and unmarried teenage motherhood, but were otherwise encouraged to explore themes that emerged from early discussion and community action options.
The first phase involved a general introduction, discussion and exploration of the topic as a whole group. For the second phase, participants formed subgroups to discuss and clarify ideas raised during the first phase and addressed key questions:
What are your concerns about mental distress in young women and girls who have unmarried pregnancy? What are the barriers to meeting mental health needs in the field? What would make it easier to increase efficiency in your work (in supporting unmarried teenage mothers) with colleagues/community?
Qualitative data outputs took the form of participant-generated visual artefacts (flipchart presentations, photographs) and fieldnotes taken during discussion, both of which were curated for qualitative analysis. Observations and fieldnotes were also made extant of group and community meetings, particularly during visits to rural communities and informal meetings with local informants.
Data capture and representation
Fieldnotes are intrinsic to the performance of ethnographically informed, community-based qualitative research (Spradley, 1979) and they contribute to this report by providing the reader with direct access to the researchers’ en-scene interpretations, Moreover, they provide an interpretative and analytical bridge to the broader corpus of collaborative research methods (Safronov et al., 2020) described herein.
Analysis
Thematic analysis was adopted for both emergent and a priori themes. To undertake the analysis, data from the Open Space stakeholder and village meetings were transcribed and analysed inductively: first, for emergent themes; and second, against the a priori themes (concerns, barriers, problem-solving). Fieldnotes from girls’ discussion groups were also analysed inductively for emerging and a priori themes (mental health, causes and impact of teenage pregnancy). Credibility was achieved via participation and community co-production during the Open Space and community discussion activities. Dependability and confirmability were enhanced through repeated close engagement with participants and the use of several group meetings across sites.
Ethics
Ethical approval was obtained from the Manchester Metropolitan University ethics committee. The adolescent girls gave their consent verbally rather than in writing owing to limited literacy. Parental consent for those under 16 was waived. In Uganda, mothers under 16 years of age are classified as ‘emancipated minors’ (UNCST, 2007) and deemed able to provide autonomous informed consent for their participation in research (Maly et al., 2017; Namusoke et al., 2021; UNCST, 2007). Our approach aligned with these national regulations. Anonymity and confidentiality were ensured in the girls’ group discussions by ensuring groups were ‘closed’ and included only members who were engaged by The NGO delivering skills training.
The ages of the girls and young women participating in discussions ranged from 15 to 21.
Consent from stakeholders and community elders was also given verbally at the time of discussion and consent was accepted by a willingness to participate after the reasons for the discussion were explained. As a collaborative African and European research team, we were committed to the primacy of individual informed consent to participate in research. Nonetheless, we remained mindful of both cross-cultural understandings of the concept of informed consent and, moreover, the troublesome legacy of the exploitation through research of economically vulnerable people and populations (St. Fleur & Schwartz, 2020). As such, community engagement not only formed a keystone for our methodology, but also played an essential role in providing the foundations of trust that underpinned our obtaining of individual, informed consent from participants.
The NGO supported the girls’ groups, village members and stakeholders, and remains as a contact and intermediary with the researchers. In addition, all stakeholders were given contact details for the principal researcher. No concerns were received from participants.
Results
Emergent themes from the girls’ groups and village meetings overlapped on the whole, with notable exceptions. All groups demonstrated that poverty, family disruption and a lack of sexual health education were factors in unmarried pregnancy, but the girls’ groups also emphasised the importance of school attendance to their futures and the need for school funds. Community explanations were more moralistic: apportioning blame on parental neglect or the girls themselves. Only the girls attributed blame to their babies’ fathers, and were the most acutely aware of, and impacted by, the gender differential inherent in the issue. The psychosocial health consequences of depression and social shame were recognised by all parties, but only the girls’ experiences factored social rejection and loss of aspirations. Professional stakeholder groups demonstrated an overall appreciation of the wider social and cultural issues, and expressed motivation for localised community-driven solutions.
Girls’ group and community discussions
Reasons given for unmarried pregnancy
Most of the girls stated that they had acquired a ‘boyfriend’ as financial support for continuing in school. They gave the reasons for needing this support as poverty at home, funds diverted for the education of siblings, de-valuing of their own (female) education, and a lack of parental support owing to separation or death, domestic violence or not being able to live at home. Many girls described being exploited by their boyfriend who promised to support them in exchange for sex. For all the girls, poverty at home and the inability to support themselves financially through school were apparent as underlying factors in their pregnancy.
Community elders blamed parents and guardians for a lack of supervision and support, but also identified a lack of sex education as reasons for pregnancy. As was noted by one male elder: Prostitution for school fees and other things – parents condone this behaviour – a way out of poverty. Parents neglect children – don’t teach morals and how to look out for themselves. Orphans have lazy guardians. (Male elder, Mayuge community group)
Consequences of unmarried pregnancy
All the girls reported being expelled from school once it was discovered they were pregnant. Many expressed anguish at being expelled and missing their education. Several had aspirations for professional careers (i.e., teaching, midwifery, police) but had their hopes reduced by not completing school. Most girls, we noted, wanted to return to school after the birth, but their families were not prepared to support them. In Uganda currently, maternity leave is mandatory after the third month of pregnancy, with return only permitted from one year after birth. This may change in recognition of the rates of teenage pregnancy following the pandemic and the barrier this ban represents to female education (Ministry of Education and Sports, 2020).
All the girls were linked with an NGO that provided vocational skills training to promote independence. For many, this appeared to be a very different form of self-sufficiency from that they had planned, and such economic activity is commonly seen as a last-resort alternative to income generation and less prestigious than education-based employment. The majority of girls reported being rejected by their parents or guardians when they became pregnant. Nearly all the girls attempted to live with the father's family, and some got married, but all reported this experience negatively. Many reported being bullied by mothers-in-law, abused and neglected by the baby's father, which resulted in their returning to their own family or living elsewhere. Explanations of rejection were given as the family's inability or unwillingness to support them with a baby, for reasons of expense burden or patriarchy.
Family structure and support
Most girls reported having poor support at home to attend school. These girls were living in single-parent families, with aunts, in polygamous families with stepmothers or were orphans. A disrupted family structure, such as the presence of a stepmother, or an absent or deceased father, was often an issue in their seeking support or ‘love’ elsewhere, which compounded their vulnerability to sexual exploitation. Also, this lack of a supportive family structure could lead to a lack of support following conception and birth of the baby.
Poverty
All the girls’ stories related back to family and individual poverty being at the root of the pregnancies and the consequences of becoming pregnant. They and the village elders described a lack of support from families owing to limited resources, an extra mouth to feed and then, as one male village elder described, the mother and baby become a burden on the family and the community: ‘In the first place, parents haven’t looked after your child, it [she] gets pregnant, then a burden of two’ (male elder, Mayuge community group).
Most of the girls reported becoming pregnant while seeking financial support for school or to meet basic needs outside the family, and then being exploited. They were also struggling to support themselves following the pregnancy, but those not in marriages were striving to become independent. One unmarried mother described a family poverty trap in being required to work for the family (in subsistence farming) and therefore not having her own means of income. Families and communities valued girls as workers in family subsistence farming activities, so although an unmarried pregnancy was seen as shameful, there was an advantage for some families from the child leaving school because they could then work for the family.
Gender inequality and patriarchy
Several girls claimed they were treated unfairly because they were girls. They were angry that the boys faced fewer problems after fathering a child, saying that boys do not get expelled from school, or they run away and do not face justice or their parental responsibilities. The legal age of consent in Uganda is 18 but, as both participants and The NGO staff reported, this is rarely upheld. We also noted that families often came to their own agreements rather than involve the police.
One girl implied that females are less valued than males because women are part of Adam's rib (a biblical allusion), therefore subservient. It was unclear whether she believed this or was explaining that is how others see girls: ‘Women are [considered] rib of man so only a small part’ (teenage mother, Kasese rural girls’ group).
Community and family views
Culturally, if not legally, it is acceptable for girls to marry early and become pregnant at a young age, but an unmarried pregnancy is unacceptable. We found, however, a clear difference in attitude between male and female elders. Older women at the village meetings were openly more sympathetic of the consequences for the girls: shame and stigma, and physical and mental risk due to the pregnancy. During a village meeting discussion, one mother of an unmarried teenage mother claimed: ‘It is not their wish to leave school and get pregnant. They are regretful. [They] beg for forgiveness – suffer disgrace and rejection – lack of care leads to medical neglect.’ This attracted sympathetic comments and agreement from many of the other women present. These women's sympathy may be based on their own past experiences as many may have become pregnant early and suffered chronic obstetric consequences such as an untreated fistula. Also, as one elderly female elder in the Mayuge group offered, to protests from male elders, ‘Put them on the pill’. Although this may seem a practical solution, the protest from male community members indicates that the moral imperative may be embedded in patriarchal values.
Mental illness and psychological distress
When discussing mental illness in others, many girls reported recognising this as a change in behaviour. Often, they described signs and symptoms to include isolation and social withdrawal, disruptive or disorganised behaviour such as throwing stones, collecting pans and one person was described who, ‘stopped wanting to greet’. This is a cultural norm for young people who are expected to greet the senior generation by kneeling at their feet. Repeatedly, ‘overthinking’ (translated term) was described as either a symptom or a cause of mental illness by all groups. ‘Overthinking’ is a common description globally, and particularly in sub-Saharan Africa, to describe psychological distress (Ashaba et al., 2019; Kaiser et al., 2015). Although the presentation of depression is often culturally determined (Kirmayer, 2001), the cultural understanding of distress being ‘overthinking’ may be lost in translation from both the original dialect and its conversion into English by an interpreter, or incorporated into common usage understood universally in Uganda. For instance, ‘overthinking’ in English is currently used for mental health promotion by the Ugandan Ministry of Health to refer to depression. The word used in Luganda – a sister dialect for Lusoga (of Mayuge) – is ‘Okwekyawa’, which can be directly translated as ‘hating yourself’. Our Basoga colleagues suggest ‘overthinking’ can be translated as ‘Enyiike’ or ‘Enaku empitirvu’, which is close to pain after suffering the loss of something, or grief.
Williams (2021) suggests that overthinking among post-war Northern Ugandans, within a constellation of dissociative symptoms, could be indicative of post-traumatic stress disorder, but the Baganda (Southern Ugandans) described ‘worrisome thoughts’ associated with depression for Okello and Ekblad (2006). They also identified ‘thinking too much’ or ‘too many thoughts’ as causative of depression and social withdrawal. In our study, ‘overthinking’ was used frequently in Kasese and Mayuge, by different interpreters translating different Ugandan dialects. The descriptions of preoccupation and disordered behaviour accompanying ‘overthinking’ among the girls certainly felt more like rumination associated with major depressive disorder than trauma. It is also interesting that ‘overthinking’ was seen by the girls as both a cause and a consequence of mental illness, especially if they are describing what western clinicians would see as negative cognitions that also increase negative affect (Nolen-Hoeksema et al., 2008).
Other causes of mental illness described by the community groups included traditional beliefs, substance use or association with physical illness, as one female elder was noted to describe: Mental illness is attributed to drug abuse, witchcraft, generational curse. Person considered ‘possessed’ so avoided. They may get sick, go to hospital, check blood pressure – too high or too low. Because of drugs or because of a disease [i.e. malaria] or overthinking. (Female elder, Mayuge community group)
In a study of perinatal depression among Ugandan women, symptom attribution was found by Sarker et al., (2018) to be dependent on the woman's social situation. Therefore, their symptoms could be attributed to interpersonal, economic or spiritual problems in their life. This social explanation of distress can determine help-seeking behaviour (Shah et al., 2017). Among our young mothers, their distress was attributed to their situation and, in explanation, they described emotions associated with social issues, and emotions rather than thoughts: ‘When you have anger you become hopeless – end of the world. [… ] Feel bad to stop school. Father died, brother promised to help. Didn’t. Frustrated’ (teenage mother, Mayuge girls’ group 3).
The emotions expressed were commonly associated with loss of aspirations, and also family rejection: ‘When your parents reject you, you feel bad and then you worry and overthinking how to do right. Doesn’t feel different (being married). Rejected at home and rejected in marriage’ (married mother, 20, Mayuge girls’ group 2).
The emotions were often expressed as physical sensations: ‘Feel pain in my head. When angry/disappointed, rejected, your body becomes weak and you can’t do things for yourself’ (teenage mother, Mayuge girls’ group 3).
The difference between the girls’ experience of distress, the community elders’ beliefs about the cause of mental illness, and the girls’ notions of mental illness in others is quite stark. The girls do not appear to associate their emotions with being mentally ill, attributing their emotions to loss, rejection and frustration/disempowerment. For them, the consequence of strong emotions is a loss of the ability to function well. Poor functioning and negative thoughts correspond with the DSM-5 definition of major depressive disorder, which includes low mood, feelings of sadness and loss of function as symptoms (American Psychiatric Association [APA], 2013). Also, DSM-5 lists feelings of worthlessness and inappropriate guilt; however, the girls do not appear to internalise their problems with any manifest sense of guilt or self-blame, because the concept of depression as an internally driven issue appears to be absent unless associated with physical ability ‘your body becomes weak’. Indeed, the girls’ emotions are generally directed outward as anger towards others, and a key driver for their distress appears to be loss: of prospects, family life, school life and belonging. Although they display some symptoms of depressive disorder as understood in western psychiatry, there is a marked sense of bereavement and grieving associated with their reports.
In contrast to the girls’ perceptions and attributions of their own mental states, community elders appear to recognise the risk of severe mental illness and attribute it to actions of the individual such as substance use, or external forces such as witchcraft. None of the community elders appear to appreciate the impact of loss and rejection on the girls’ mental states. This may of course be driven by a need to project blame away from the community itself. The girls also describe mental illness as behavioural and do not recognise this in themselves, although they may be conceptualising ‘mental illness’ as psychosis. This division between the girls’ intra-personal experience and the community elders’ extra-personal understanding reflects the findings by Sarker et al. (2018) in which symptoms are variously attributed to the social context of the individual and how their identity is understood. Although personal identity may matter, social identity may be seen as more relevant.
African cultures are sometimes characterised as being organised around social identity rather than the individual; however, the diversity specific to both particular persons and between groups of people in a specific health situation and social context – here unmarried pregnant girls in relation to the community elders – needs to be taken seriously. The representation of African health cultures as collective rather than organised around respect for personal identity is itself a western oversimplification of the complexities of community responsibility and shared decision-making to account for diversity in putting people first (Van Staden, 2011): ‘African health cultures are neither necessarily collective nor individualist but something different that incorporates both in a context-responsive way’ (Van Staden and Fulford, 2015: 32). Rather, the complexity of values pluralism and difference within African health cultures points to a background orientation of communal responsibility and social interconnectedness informed by mutual respect. Thus, for example, ‘Ubuntu’ is one of a number of words expressing a process of shared decision-making in sub-Saharan African languages (Metz, 2011; Ramose, 2003) in which all relevant values are voiced, both individual and communal. The collective dimension of African health cultures is better understood as a communicative practice appropriate to a given situation.
Open space stakeholder meetings
The OST meetings presented a different form of dialogue that contained more a reflection on the issue in contrast to a reflection within the issue of unmarried motherhood and mental ill health. Data from fieldnotes and artefacts following breakaway group discussions (flipchart presentations) were analysed for emergent themes.
Causes and concerns for girls and mental health
The professional stakeholders were able to take a wider perspective and tended to agree with both the girls and community elders when identifying socio-economic explanations for their concerns, the causes of distress and the limited solutions. The Kasese stakeholder group identified family disruption and abandonment for alienating and isolating the girls before and after conception, with domestic violence resulting in family breakdown and reducing pre-conception support, which often leaves the girl in the care of an aunt or stepmother. They also identified war as a key factor because these informants have professional experience of displaced families crossing the border from the DRC. The Mayuge stakeholders also identified family abandonment and lack of psychosocial support after conception and were concerned that families needed to be sensitised (educated) to the dangers of early marriage and the need to identify vulnerable girls and link them with support services. Unlike Kasese, the Mayuge region has experienced no wars or immigration of refugees, but is closer geographically to urban centres, with its population perhaps more habituated to western societal culture and health services, hence possessing higher expectations and awareness of wider societal support.
Barriers to meeting mental health needs
The professional stakeholders clearly held western notions of mental and psychosocial health, many being trained health professionals and social workers. They identified attitudes, beliefs and poor infrastructure as key barriers to meeting the mental health needs of teenage mothers. They explained that the large distances mental health and social workers need to travel to visit communities takes time, but in addition, the roads and unreliable transport, plus the cost of fuel, are inhibiting. Also, when workers are travelling, they are not in the office and poor mobile phone coverage means they are uncontactable.
Traditional beliefs and attitudes were also identified as key barriers by Mayuge and Kasese stakeholders. They reported that adherence to traditional beliefs limits people's access to medication because traditional healers will be consulted first, especially as this is often a cheaper option. The stakeholders made a distinction between traditional tribal beliefs (termed witchcraft) and predatory for-profit churches, but report that both are often conflated, and both can be obstructive to delivering medical care. A discussion with The NGO officer from Kasese, illustrates the conflict with traditional and for-profit churches: People feel God needs a sacrifice which is the mentally ill person. Religious beliefs [for-profit churches] encourage people to put their faith in the church and prayer instead of seeking medical help. One woman with psychosis was sent to pray all night and she would be cured. Mental illness attributed to witchcraft or hereditary, especially epilepsy. There is large gender inequality as mental illness seen differently in men and women. Men cursed by women through witchcraft – so women [are] blamed for male illness. (male Ugandan NGO worker, Kasese)
Problem-solving
Both groups of stakeholders identified a need to sensitise communities (educate and raise awareness) to mental illness and sexual health, including the girls’ families, to prevent rejection. However, they also noted that there is a lack of focus on mental health from NGOs, which instead focus on better funded communicable diseases such as HIV/AIDS, tuberculosis and malaria. Local councillors identified that the main support offered in rural areas for these girls tended to be maternal health care such as antenatal care, but stigma and travel distances prevented them from attending.
The stakeholder groups proposed ideas for tackling the issue, including sensitisation and improved access to help. Most ideas supported community engagement, partnerships and involving political members as well as practitioners and community leaders in problem-solving. Stakeholder discussion groups devised plans for community engagement using co-productive and participatory approaches to include all key community members. These included a multi-agency approach that would address planning and budget allocation, referral linkages and training in mental health. They also suggested establishing rehabilitation centres to improve access to service providers, along with outreach visits and the use of local radio talk shows to highlight the issues within communities. What was clear during the OST meetings was that many of these stakeholders had not previously met to exchange views collaboratively, and the notion of multi-agency planning meetings (‘camps’) appeared to be recognised as a feasible way to organise change.
Discussion
In the face of what can appear overwhelming adversity for unmarried teenage mothers in rural LMIC communities, accessible modifiable factors are likely to be a reduction in unwanted pregnancies and improvement in social and personal support following unmarried conception. The barriers to this appear to be cultural morals, engendered roles and poor access to supportive services. The economic and health burdens presented by high fertility in Uganda are responded to by researchers and policymakers in calling for sex education, access to contraception and adherence to and enforcement of existing laws relating to the age of consent (Chandra-Mouli et al., 2014; UNICEF, 2015; WHO, 2020; Yakubu & Salisu, 2018). We might add accessible and free secondary education to these interventions to reduce the sexual exploitation vulnerability of girls in poor communities.
Support to ensure girls remain in education is increasingly recognised as essential for developing Uganda's economic power and workforce. New policies focus on changing gender-biased attitudes towards pregnant teenage girls, and supporting their continuation and subsequent re-entry into school following the birth (Ministry of Education and Sports, 2020), driven by monitoring of schools’ performance on re-entry, but also promoting increased sex and reproductive health education, and tackling social and cultural barriers to education. However, vulnerable girls in rural and poor communities will continue to face material, resource and cultural barriers presented by poor infrastructure and long distances to travel, lack of funds for school or travel, access to reproductive education, religious objections to contraception, unenforced consent and rape laws, and cultural norms of child marriage and gender-biased attitudes to sex (Nabugoomu et al., 2020).
Psychosocial health
Depression is often reported as the most significant mental disorder in adolescents in LMICs, particularly in sub-Saharan Africa (Ismayilova et al., 2018; Kutcher et al., 2019; Osok et al., 2018). Redinger et al. (2020) identified a causative effect of family and partner stress on depression and anxiety during pregnancy and later family life. Our findings indicate that depressive symptoms, as understood in western psychiatry, are a possible consequence of becoming pregnant outside marriage. The girls in the discussion groups reported and demonstrated low mood, lack of motivation and strong emotions of anger and loss, linked to their changed social situation. These girls, in being accessible to our study, may of course have less troublesome depressive symptoms than others not engaged by The NGO, but anecdotal accounts of other teenage unmarried mothers within these communities describe apparent severe depression and suicidal behaviour. Although we did not conduct clinical assessments, and did not intend to use western conceptions of mental illness, many of the girls displayed or reported symptoms that would in the west suggest a need for assessment. We cannot rule out postnatal depression among this cohort; however, most had given birth more than 12 months prior to the discussions, and those with their children appeared well bonded. Some had experienced domestic violence and rape so we also cannot rule out post-traumatic stress disorder; however, the most common expressions of distress were of a loss of aspirations, suggesting grief reaction, and a sense of helplessness indicative of a lack of autonomy. It may be important to recognise the role of the social disruption that unmarried girls experience in supporting these girls’ mental health, because their distress may be associated more with experiencing the social rejection and loss of aspirations that accompany the pregnancy.
It was apparent that marriage was not a good experience for any of the married girls, nor was attempting to live with their in-laws. It is likely that parents pressure girls into marrying the baby's father, but any subsequent reduction in social stigma does not appear to reduce the mental stress the girls experience. The girls pursuing independent living expressed more hope than the married girls, indicating that an approach to addressing their psychosocial needs should emphasise personal empowerment rather than attempting to conform to traditional social acceptability within their communities. It was also clear that communities and families could recognise mental illness in others, but this rarely resulted in appropriate support. Normative moral values, poverty, limited professional resources and a lack of understanding appeared to present barriers to care.
Health responses
Culturally appropriate responses may require re-contextualisation of universal and abstract values in the context of lived experience (Bergqvist, 2020). The difference in understanding of the girls’ mental states in this study can be divided in three ways across the communities: experiential, lay and (western) professional. A re-contextualising of mental health and lived experience for effective interventions may need to include the capacity to understand alternative culturally sensitive terms (such as ‘overthinking’) for speaking of ‘depression’ and other mental issues. Healthcare workers will need to have the skills to identify situations where values are challenged, and analyse and make well-founded decisions in relating to others against the backdrop of social and moral norms within communal life (Bergqvist, 2020; Fulford & Van Staden, 2020; Sadler, 2005). This competence we term ‘mental health value literacy’ in understanding the existential dimension of how people have been affected by early teen pregnancy, both mentally and socially, includes understanding of lived experience and personal values in the particular context, but also accommodates community interpretation and understanding of individual members’ situations. This is more than a role for mental health education and westernising knowledge, but translational work incorporating locally meaningful concepts. For instance, it was clear from our findings that community efforts to mitigate against the stigma of unmarried motherhood are to normalise the girls’ status through marriage. However, this was experienced as traumatising and clearly more detrimental to the girls’ well-being. This illustrates a need to recognise how communities are challenged by westernising influences, changing expectations that are driving divisions between generations, and inviting more reflexive approaches in mental health interventions. den Hertog et al. (2021) suggest a merging of local and western psy interventions by considering how local responses can aid the cognitive and emotional symptoms by applying locally meaningful psychosocial interventions. In this case, an aim would be to reduce rejection, support validation of the girls’ experiences of grief, and empower girls practically and emotionally through returning to their families and to school, or supporting income generation and mutual aid and community support.
Evidence from this study suggests that mental health interventions post-conception would take the form of improving the understanding and recognition of mental illness from within the communities, and empowering community members to facilitate support for girls to mitigate against familial rejection. In an under-resourced and centralised mental health system, notions of recruitment and training of community members as agents of change have shown some success (Abramsky et al., 2014), and self-help is suggested by Petersen and Lund (2011), along with evidence of the impact of Friendship Benches (Chibanda et al., 2016) to reduce symptoms, stigma and engage self-help groups. Community-based training is also supported by Sibeko et al. (2018) through task-shifting to reduce the dependence on professional mental health services, whereas training community lay workers in brief psychotherapy can reduce women's depressive symptoms and improve their social networks (Strong Minds, 2015). Kigozi et al. (2015) similarly demonstrated the feasibility of training village-based Ugandan health workers in mental health, by engaging local stakeholders and providing a platform for sensitisation to mental health and reduction in stigma. In addition, the Open Space approach that facilitated community discussion and problem-solving in this study suggests a methodology for facilitating stakeholder mobilisation and community action in devising self-help strategies that are culturally and environmentally grounded.
Strengths and limitations of this research
Using OST facilitated a co-productive exploration of issues and a sharing of perspectives and ideas across a range of stakeholders. Although some concepts were pre-conceived (i.e. that unmarried motherhood is ‘a problem’), the tasks for the stakeholder groups were largely emergent from earlier stage discussions to identify how they understood the topic. Other discussions centred on how we might best improve the mental health of populations in a culturally appropriate way, and whether initiatives that target well-being and psychosocial understanding may be seen as more efficacious than current medical interventions. Relatedly, the research explored and exposed potential tensions between approaches, which generated bottom-up problem-solving and engagement of local agents.
Potential researcher bias
The field researchers were both white English professionals with psychology and mental health nursing backgrounds, trained and practised in western notions of psychiatry and a psychosocial understanding of health and well-being. There is often a tendency for mental health professionals to identify problems as medical deficits. In this instance, there was an effort to apply a more strengths/assets-based conceptualisation of the issues raised and to conceive issues holistically in accounting for social, cultural and geographical challenges, rather than using a narrow medical lens. Therefore, views on the girls’ mental state are impressionistic rather than clinical diagnoses. To help broaden the hermeneutic horizon in analysing the conceptual and cultural findings of the empirical research, our team included a philosophical psychiatry theorist specialising in cultural values, and a Ugandan medical anthropologist. This enabled the team to better interpret, critique and articulate the significance of African philosophy in understanding the mechanisms of co-production and shared decision-making in transcultural psychiatry and the prospects for a distinctly African values-based orientation in this domain.
As for the empirical research itself, it is also worth noting that the issue of mental health problems among unmarried mothers was first identified by Ugandan NGO sexual health education workers, and all group interviews and stakeholder consultations were assisted by The NGO and their experienced field officers. The field officers share the cultures of the communities investigated and also provided translation from regional dialects into English, and interpretation of cultural concepts or phrases and explanation of geographical factors.
Conclusion
Unmarried teenage mothers in rural Uganda may face the double stigma of mental distress and having a child outside marriage, but they are likely to have treatable mental health problems that would respond to psychosocial interventions delivered in their communities, by their communities, at the village and district level. Our research has revealed divisions in understanding the distress experienced by unmarried teenage mothers that may illustrate how normative cultural understanding is in flux: increasingly influenced by western notions of health, illness and well-being, and the changing aspirations for young people. This calls for more sensitive and nuanced interventions for health promotion and interventions generated and supported, as suggested by stakeholders, through local initiatives.
Current approaches may advocate community sensitisation to assist in reducing the effect of stigmatisation and social exclusion and enable girls to help themselves and each other, but there is an opportunity to mobilise self-help to create a low-resource, high-impact approach to community action that could be supported by community leadership for sustainability.
Footnotes
Acknowledgements
The authors would like to acknowledge Act4Africa Uganda staff for facilitating this study, providing translation and interpretation, and giving additional insight into to the lives of rural Ugandans and their world views.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Global Challenges Research Fund.