
Abstract
Research about the relation between migration and mental health as well as factors influencing the mental health of migrants has been growing because challenges of migration can constitute a significant mental health burden. However, its divergent findings seem to reflect group-specific differences, e.g., regarding country of origin and receiving country. Almost no empirical studies about individual migrant groups in different receiving countries have been undertaken so far. The present population-based study explores symptoms of depression, anxiety, and somatization as well as quality of life in an Austrian and a German sample of ex-Soviet Jewish migrants. We mainly investigate the relationship of religiosity and perceived xenophobic and anti-Semitic discrimination to the psychological condition of the migrants. Standardized self-report scales, specifically the Beck-Depression-Inventory-II (BDI), State-Trait-Anxiety-Inventory (STAI), Brief Symptom Inventory (BSI), and WHO Quality of Life Questionnaire (WHOQOL-BREF), were used to measure mental health. Ex-Soviet Jewish migrants in Austria showed significantly more symptoms of depression than those in Germany. Regression analyses support a protective effect of religiosity on mental health in the sample in Germany and an adverse effect of perceived discrimination in the sample in Austria. The present study reveals a less favorable situation for ex-Soviet Jewish migrants in Austria, in terms of income, residence status, and xenophobic attitudes in the local population, compared to the group in Germany. Furthermore, our data suggest that the receiving country matters for the mental health of this migrant group. However, further research is needed to support these conclusions.
Introduction
Migrating from one country to another can be a difficult process which often involves multiple challenges such as learning a new language, finding new work, losing the acquired social network and having to build a new one, as well as coping with an unaccustomed and culturally distant environment. Therefore, migration can constitute a mental health burden (Morawa & Erim, 2015).
Migration and mental health
In recent years, there has been a growing research interest in the relation between migration and mental health. The findings on the question of whether migration leads to impaired mental health, the so-called Migration-Morbidity-Hypothesis (Mirsky, 2008), are controversial. Many studies conclude that immigrants have elevated rates of mental distress and psychiatric morbidity compared to the host populations, although the prevalence rates vary among studies (Bermejo et al., 2010; Beutel et al., 2016; Lindert et al., 2009). Others, however, indicate that there is no generalized mental health risk for migrants (Carta et al., 2005; Glaesmer et al., 2009) or even report lower prevalence of mental disorders in migrants (Alegria et al., 2008; Dhadda & Greene, 2017; Salas-Wright et al., 2014). These divergent findings reflect group-specific differences, e.g., regarding country of origin and receiving country (Stompe et al., 2009).
Ex-Soviet Jews and emigration
Ex-Soviet Jews typically have Russian as their mother tongue, a high level of education (with up to 75% holding a university degree), assimilation into the mainstream Soviet/Russian culture, a history of oppression and discrimination under communism, and little knowledge and observance of Judaism as a religion (Jurcik et al., 2013; Remennick, 2007). Due to Soviet anti-religious propaganda and forced secularity, (ex-)Soviet Jews were detached from their religion and traditional culture and “became an ethnic minority rather than a religious denomination” 1 (Remennick, 2007, p. 21). Collective memory of the Holocaust and present-day expressions of anti-Semitism built instead the basis of their Jewish identity. In addition, they might have a strong connection to the Soviet/Russian culture and, after immigration, to the host society's culture, leading to a tri-cultural identity (Birman et al., 2010).
The emigration of (ex-)Soviet Jews started in the 1970s, reached its peak after the fall of the Soviet Union (USSR), and continues until now. Of the 2.2 million Jews living in the USSR in 1970, 1.9 million had emigrated by 2009 (Tolts, 2016). The Soviet Jews lived mostly in the Russian, Ukrainian, and Central Asian republics. Some Russian or Ukrainian Jews did not emigrate, while almost all Central Asian and Caucasus Jews left the former Soviet Union (FSU) (Remennick, 2007). The main destinations were Israel, the United States, and, starting from 1990, Germany, which invited ex-Soviet Jews to settle as refugees. Most ex-Soviet Jewish immigrants live in these countries today (Jurcik et al., 2013). Until 1990, the most common reasons for emigration were religious oppression, institutional discrimination, as well as the ensuing lack of educational and professional opportunities (Flaherty et al., 1988). Later, emigration became mostly economically motivated (Jurcik et al., 2013).
The estimated number of ex-Soviet Jewish migrants is approximately 230,000 in Germany and 20,000 in Austria, but there are no official records of religious affiliation or ethnic origin of immigrants in these countries (Tolts, 2016). In Germany, this migrant group consists mostly of non-observant Russian and Ukrainian Jews settled all over the country, with 40,000 living in Berlin. In Austria, the migrant population is concentrated in Vienna and consists of both traditional Central Asian and Caucasus Jews and mostly non-observant Russian and Ukrainian Jews.
Mental health and post-migration factors among ex-Soviet Jewish migrants
Important factors influencing the mental health of migrants are religiosity (Bonelli & Koenig, 2013), experienced discrimination (Bernstein et al., 2011), income (González-Castro & Ubillos, 2011), and acculturation attitude (Berry et al., 1987), but also other socio-economic, cultural, and migration-specific variables.
Although the migration of many ex-Soviet Jews was mostly economically motivated, they often faced difficulties such as non-recognition of professional qualifications and lack of adequate employment in the host countries (Jurcik et al., 2013). In Germany, in contrast to Austria, ex-Soviet Jewish migrants receive considerable financial and Jewish community support. In the receiving countries, the social network of (ex-)Soviet Jewish immigrants consists mostly of compatriots and they often form residential ethnic enclaves (Remennick, 2007). After immigration, migrants tend to develop a stronger Jewish cultural and religious identity than before (Glöckner, 2010).
There are few studies on the mental health of ex-Soviet Jewish immigrants. Their results support the Migration-Morbidity-Hypothesis (Mirsky, 2008), showing that Jewish immigrants from the FSU appear to be particularly vulnerable to depression and anxiety (Aroian & Norris, 2003; Mirsky et al., 2008; Tselmin et al., 2007). Ullmann et al. (2013), for example, report a higher rate of depression, anxiety, and psychosomatic symptoms in this migrant group as compared to natives in Germany. In our previous study, we also found significant differences in depression and anxiety between the migrant group and the local population in Austria (Trilesnik et al., 2018). Moreover, this migrant group tends to present somatic symptoms as an expression of psychological ones (Hundley & Lambie, 2007).
Religiosity, xenophobia, and anti-Semitism can be considered important post-migration factors in this context. Religiosity is a multifaceted construct that describes the level of involvement with a religion, which is commonly defined as a set of common “beliefs, practices and rituals related to the sacred” (Koenig et al., 2012, p. 37). The intrinsic aspects of religiosity (e.g., faith in God, set of beliefs, private prayer) provide explanations for life's meaning, including human suffering, and could therefore influence mental health. The extrinsic aspects (e.g., frequent religious service attendance, membership in religious organizations) could affect mental health by establishing a feeling of belonging and social support (Boehnlein, 2006).
Accordingly, some studies suggest a protective effect of religiosity on mental health. Notably, two thirds of the studies reviewed by Koenig (2009) found less depression and half found less anxiety among the more religious compared to the non-religious. However, most studies were conducted with Christians (Krumrei et al., 2013) and only a few have addressed other religious groups. For example, Jarvis et al. (2005) found no evidence for a protective effect of religiosity on mental health among Jews and Buddhists. Rosmarin et al. (2018) concluded, however, that religiosity has a buffering effect against mental distress and psychiatric morbidity across all Jewish religious groups. In a sample of ex-Soviet immigrants in Israel, being secular was associated with distress (Ponizovsky et al., 2009). A negative correlation between religiosity and depression but no link between religiosity and anxiety was also found in ex-Soviet Jews in Austria (Trilesnik et al., 2018) and elderly ex-Soviet Jews in Germany (Nesterko et al., 2014).
Ex-Soviet Jewish migrants potentially face double discrimination, due to xenophobia and anti-Semitism. Following the main relevant German research project, we define xenophobia as a negative or devaluing attitude towards people and cultures considered different from one's own, usually referring to foreigners or immigrants (Zick et al., 2011). Motives for xenophobia could be socioeconomic envy, perceived competition for jobs and housing etc., supposed exploitation of the social welfare system, as well as fears of foreign infiltration as a threat to one's cultural identity. Additionally, a devaluation of “others” maintains or increases one's own self-esteem, according to Social Identity Theory (Tajfel & Turner, 1986).
Zick et al. (2011, p. 40) define anti-Semitism as “social prejudice directed against Jews simply because they are Jewish.” McLean (2020) identifies ethnocentrism and xenophobia as driving forces of anti-Semitism. There is a distinction between “classic anti-Semitism” which depicts Jews as evil people, and newer forms of “secondary anti-Semitism” (e.g., portraying Jews as trying to take advantage of their historical status as Holocaust victims), and “Israel-related anti-Semitism” (e.g., equating Israel's treatment of Palestinians to Nazi crimes; Heyder et al., 2005). Since generally “classic anti-Semitism” is socially not acceptable, the newer “harmless” forms are more common and should therefore be assessed to measure anti-Semitic attitudes in a society. In her review, Loewenthal (2012) concludes that anti-Semitism is the main risk factor for mental health among Jews in the United Kingdom and other countries. Among Jews in Germany, anti-Semitic experiences have been linked positively with depression and anxiety (Ullmann et al., 2013). Nesterko et al. (2014) show a similar link in ex-Soviet Jewish migrants in Germany for general, not specifically anti-Semitic, discrimination.
Objectives and hypotheses
Within migration research, the group of ex-Soviet Jewish immigrants outside Israel is understudied. Given the assumption that immigrant groups differ in their mental health burden, more epidemiological research in this migrant group would be beneficial. This study is designed to examine the relationship of religiosity, perceived anti-Semitism, and xenophobia to mental health in ex-Soviet Jewish migrants in Germany and Austria. Specifically, it explores symptoms of depression, anxiety, and somatization as well as quality of life as parameters of mental health.
As hypotheses, we expected less depression and somatization and higher quality of life in more religious participants and no association between religiosity and anxiety, following the two studies of the same population stated above (Nesterko et al., 2014; Trilesnik et al., 2018). Additionally, we expected poorer mental health in participants who experience more anti-Semitism and xenophobia in their daily lives.
Methods
Study design
This study is part of a larger research project investigating the mental health of ex-Soviet Jewish migrants in three host countries. We introduced a unique migration research study design by combining a standard procedure of studying a migrant group in comparison to native controls inside a given host country with a rare procedure of studying one migrant group in different host countries (Figure 1).
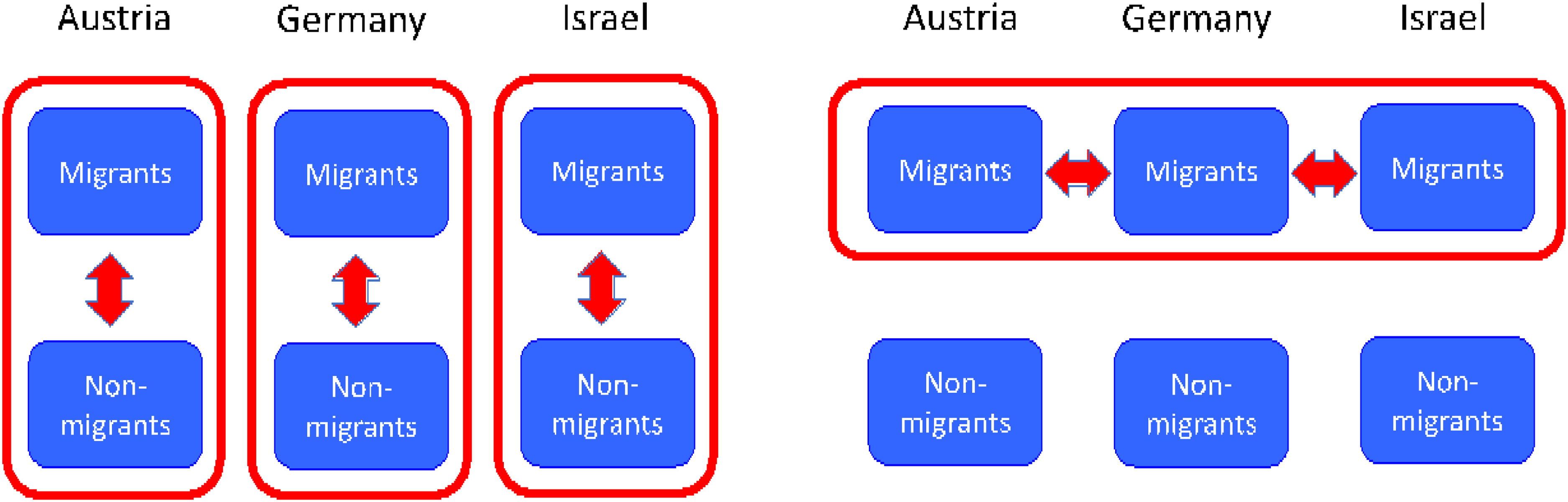
Study design: Cross-national comparison of a migrant group to local population.
Procedure/sample
A non-clinical sample of ex-Soviet Jewish migrants and native controls was compiled in Austria, Germany, and Israel for the overall research project. The data collection was conducted from 2014 to 2016 in Vienna, Berlin, and Tel Aviv as major cities of these countries.
The migrant sample is defined as first-generation migrants born in the (former) SU, with at least one Jewish grandparent 2 and living in the major city of the respective host country. In Austria and Germany, we considered as controls third-generation natives without a migration background, according to the definition of Schenk et al. (2006). In Israel, the vast majority of the population has such a migration background, therefore we used first- and second-generation natives as the control groups.
Each country sample consists of approximately 100 migrants and 100 natives, adding up to 600 participants altogether. The purposive sampling method was applied, as random sampling could not be implemented due to non-availability of data on religious and ethnic affiliation of migrants in population registries. The control and migrant groups were matched by age and sex. All study participants were recruited by the first author at religious and cultural events, in food and crafts shops, as well as on the street. The refusal rate (percentage of approached eligible persons to be enrolled in the study who refused to participate) was about 20% in all subsamples, the response rate (percentage of people who agreed to participate that filled out the questionnaires) was between 70 and 85% depending on the subsample. All participants were reminded to fill out the questionnaire one week after agreeing to participate; for 60%, multiple reminders over the period of one month were needed. The participants gave their written consent for an anonymized data analysis. The study was approved by the Ethics Committee of Hannover Medical School, Germany.
The present study refers to an extract of the overall data, namely the two subsamples from Austria and Germany. The Israeli subsample was not included in this study, as perceived anti-Semitism is not meaningful in a country where Jews constitute the majority population. The overall sample will be used for follow-up publications.
Measures
In this study, standardized and well-established self-report measures were used which have been administered in previous research and showed good psychometric properties. The questionnaire was provided in Russian and German. Scales without original or pre-existing validated translations were translated into the respective languages and verified through back-translation by native speakers. The questionnaire was tested in a test run on migrants and non-migrants to assess the cross-cultural equivalence and the psychometric properties of the scales’ adaptations.
Mental health
In addition to depression and anxiety, we also measured somatization as a specific manifestation of psychological distress in migrant groups (Gutkovich et al., 1999) and quality of life as indicators of mental condition, using the Beck Depressions-Inventory-II (BDI), the State-Trait-Anxiety-Inventory (STAI), the Brief Symptom Inventory (BSI), and the World Health Organization Quality of Life Questionnaire (WHOQOL-BREF) respectively.
BDI-II assesses the presence and severity of depressive symptoms over a period of the past two weeks. The 21 items are each worded as four multiple choice statements and are coded from 0 to 3 (total scores: 0–63). Total BDI scores over 13 indicate elevated levels of depression. In studies, BDI demonstrates a high test-retest-reliability (Pearson's r = .93), internal consistency (Cronbach's α = .91), and validity (correlation to BSI depression subscale: Pearson's r = .80; Hautzinger et al., 2006).
STAI measures the degree of anxiety at present (state subscale) and generally (trait subscale). In this study, the state subscale of STAI was omitted as we are not interested in situational effects. The trait subscale consists of 20 items rated from 1 (“almost never”) to 4 (“almost always”), with total scores between 20 and 80. Total STAI scores above 44 suggest pathological anxiety (Chanin, 2002). The test-retest-reliability coefficient has been reported as .86 and the correlation to other anxiety scales as between .73 and .85 (Laux et al., 1981).
BSI is a short version of the self-rating Symptom Checklist (SCL-90-R) which assesses psychological and somatic impairment. Only its depression, anxiety, and somatization subscales were used in this study. The symptomatic burden is estimated on a five-point Likert-scale (0 = “not at all” to 4 = “extremely”). The internal consistency for the depression and anxiety subscales is relatively high (Cronbach's α = .72 - .89 and α = .62 - .86), as is the test-retest-reliability (Pearson's r = .84 - .92 and r = .79 - .88) (Franke, 2000).
WHOQOL-BREF is a short version of the cross-culturally applicable WHO quality of life scale with 26 items and a response scale from 1 to 5 (WHO, n.d.). Psychometric properties were tested internationally and have been shown as high (Skevington et al., 2004).
Religiosity
In the migrant sample, religiosity was measured with the adapted version of the Cultural and Religious American Jewish Identity Scale (C&R-AJIS) by Friedlander et al. (2010) which is the best validated and broad measurement available for assessing Jewish identity. Its cross-cultural equivalence was validated in the test run. The scale consists of 33 items using a 5-point response scale. The 18 religious identification items focus on adherence to religious laws, principles, and rituals of Judaism (e.g., “I observe the Sabbath”). The cultural identification items reflect secular Jewish values, attitudes, behavioral lifestyle, and cultural traditions (e.g., “I enjoy Jewish literature”). The scale shows high internal consistency (Cronbach's α = .93), test-retest-reliability (Pearson's r = .93), as well as high convergent validity (r between .65 and .80).
Perceived discrimination
Perceived xenophobia and anti-Semitism were assessed with an adapted scale from Finch et al. (2000). To the original three-item scale capturing perception of discrimination in everyday life (e.g., “How often do people treat you unfairly because you are a foreigner?”), three additional items were added to measure anti-Semitism (e.g., “How often do people treat you unfairly because you are Jewish?”). The items are rated on a four-point scale from 1 (“never”) to 4 (“always”). Internal consistency of α = .76 is reported in the source.
Other factors
In the native control group, xenophobic and anti-Semitic attitudes were assessed. For xenophobia, a scale with 10 items (e.g., “foreigners exploit the social welfare system”) by Manzoni (2007) was used. Anti-Semitism was measured using a 10-item scale (e.g., “Jews have too much influence in the country in question”) from Zick et al. (2011). Both scales are rated from 1 (“strongly disagree”) to 4 (“strongly agree”).
The socio-demographic and migration-specific data about age, sex, marital status, income, level of education, reason for emigration, duration of residence, legal status, migration to multiple countries, use of mental health services, religious affiliation, Jewish ethnic group, and social network were collected.
Data analysis
The collected data were analyzed using IBM SPSS Statistics 24. Preliminary analyses were performed to confirm scale reliability and the comparability across subsamples. The comparability of the two migrant groups was assessed with analyses of variance (ANOVA) for continuous variables and with chi-square-analysis (χ2) for discrete variables. Descriptive analyses were followed by linear regression analyses to test the hypotheses.
The data from the religiosity measurement were used as a continuous variable in the regression analysis. Additionally, for descriptive analysis of the sample, it was transformed into a categorical variable by splitting the scale evenly into low, moderate, and high values. 3
Results
Our preliminary analysis confirmed the scale reliabilities. All measures showed a high internal consistency, varying between .75 and .97.
The migrants in the Austrian and German samples are comparable in terms of age, sex, and marital status (see Table 1). Regarding other socio-economic items like income (48% in Austria and 36% in Germany earn less than 1,000 Euros per month; χ2(2) = 6.687, p < .05) or education (51% in Austria and 85% in Germany hold university degrees; χ2(2) = 28.744, p < .001), the data showed significant between-group differences. Notably, both samples include recent as well as long-time migrants, with a mean duration of residence of 15 years for Austria (M = 15.3, SD = 12.3) and 18 years for Germany (M = 17.7, SD = 7.8). Migration in both samples occurred mostly for economic or educational reasons or for family reunification (82.5% and 84.3%). In both samples, the social network consists mainly of people from the same group or other foreigners.
Sociodemographic and migrant-specific characteristics (one-way ANOVA / χ2-tests).
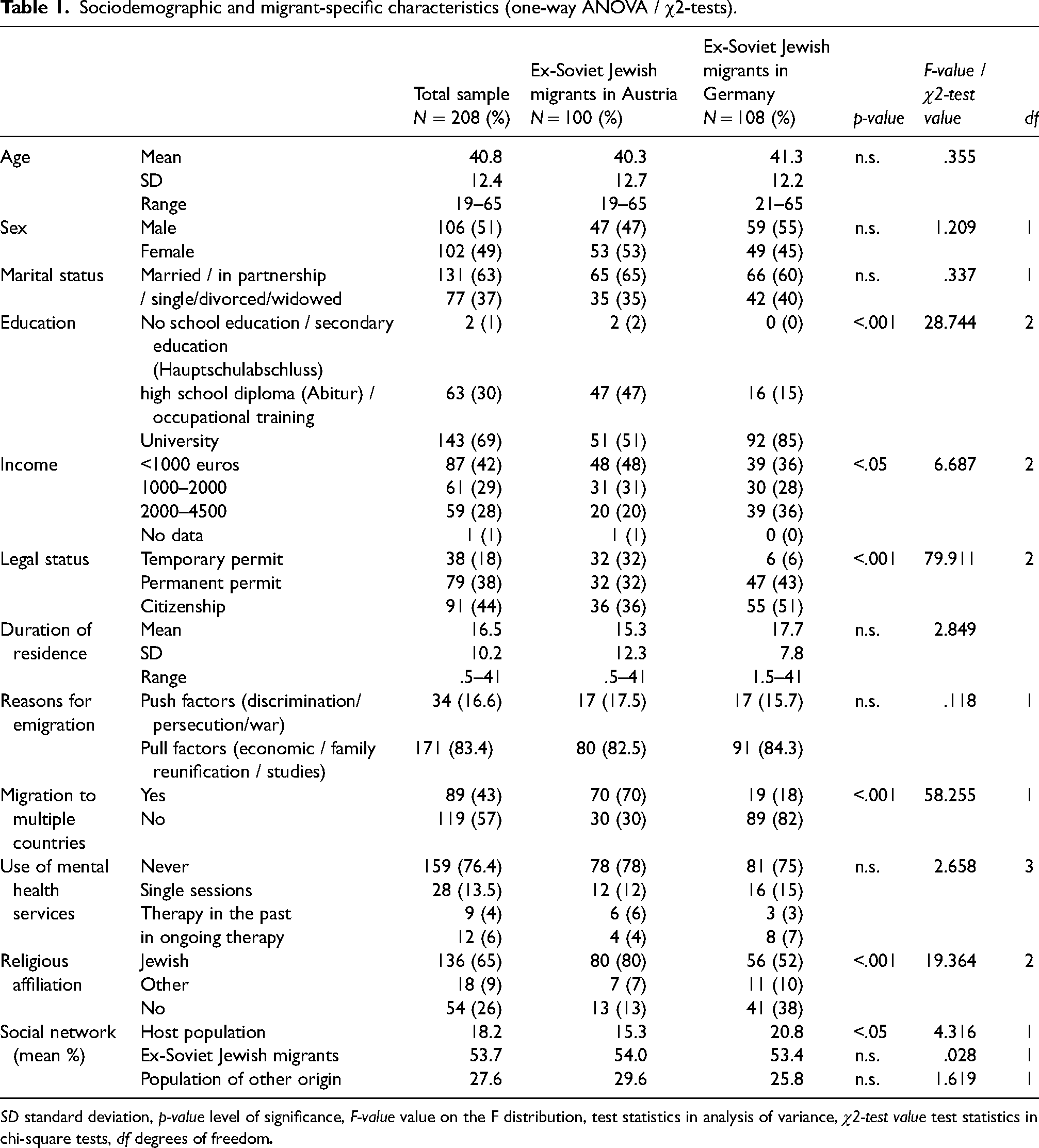
SD standard deviation, p-value level of significance, F-value value on the F distribution, test statistics in analysis of variance, χ2-test value test statistics in chi-square tests, df degrees of freedom
Ex-Soviet Jewish migrants in Austria display significantly higher levels of depressive symptoms than the migrant group in Germany (see Table 2). However, the use of mental health care services does not vary between the samples (χ2(3) = 2.659, ns), with only 10% in past or ongoing therapy.
Mental health parameters in ex-Soviet Jewish migrants in Austria and Germany (One-way MANOVA).
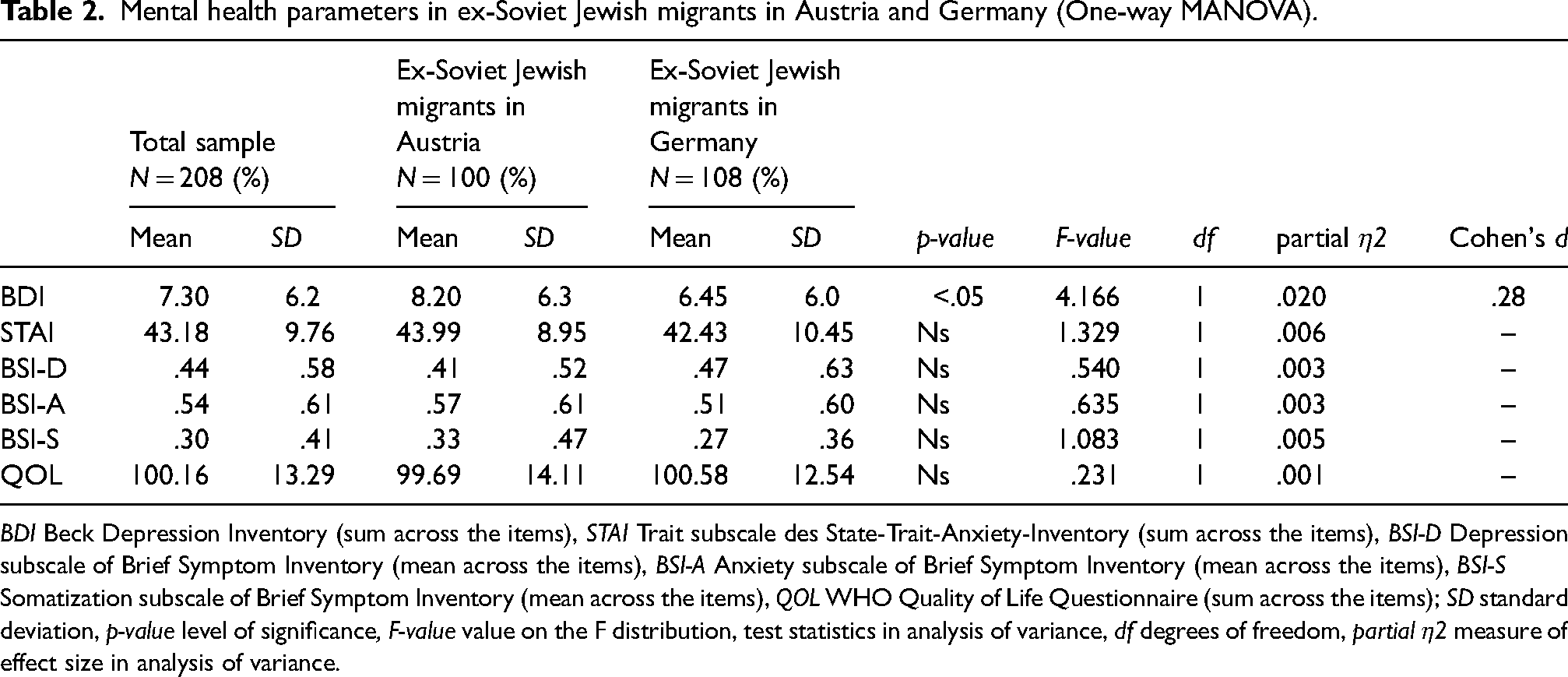
BDI Beck Depression Inventory (sum across the items), STAI Trait subscale des State-Trait-Anxiety-Inventory (sum across the items), BSI-D Depression subscale of Brief Symptom Inventory (mean across the items), BSI-A Anxiety subscale of Brief Symptom Inventory (mean across the items), BSI-S Somatization subscale of Brief Symptom Inventory (mean across the items), QOL WHO Quality of Life Questionnaire (sum across the items); SD standard deviation, p-value level of significance, F-value value on the F distribution, test statistics in analysis of variance, df degrees of freedom, partial η2 measure of effect size in analysis of variance.
The samples differ significantly in religiosity. Only one third of the Austrian but 60% of the German migrant sample can be categorized as slightly or not religious (χ2(2) = 14.410, p = .001), whereas 34% of the Austrian and 21% of the German subsample can be considered highly religious and observant. The remainder was classified as moderately religious. These findings are also reflected in the share of participants who self-identified as being of Jewish religion, 80% in the Austrian as opposed to 52% in the German sample (see Table 1).
The rates of perceived anti-Semitic as well as xenophobic discrimination in the migrant samples were comparable in both countries. Regarding anti-Semitism, 41% versus 37% of participants never, 42% versus 46.3% seldom, 12% versus 16.7% sometimes, and 5% and 0% often felt discriminated against as Jews in Austria and Germany respectively (χ2(3) = 6.610, ns). Participants more often experienced xenophobic discrimination: 20% versus 19.4% never, 45% versus 42.6% seldom, 30% versus 34.3% sometimes, and 5% versus 3.7% often felt discriminated against as foreigners in Austria and Germany respectively (χ2(3) = .571, ns). However, regarding xenophobic and anti-Semitic attitudes of the host population, rates assessed in our control groups are higher in Austria than in Germany (14% vs. 8% and 8% vs. 5% respectively).
To answer the research questions whether religiosity and perceived anti-Semitism and xenophobia influence mental health, a stepwise linear regression analysis was performed in the combined sample (Tab. A in Appendix). Income, education, legal status, and duration of residence were accounted for, as each of them varies a lot between or within the subsamples and constitutes potential impact factors on mental health. Additionally, we added the host country as a predictor to the model. Jewish religious identification appeared to be a significant predictor for depression (BDI, t = − 2.532, p < .01) and anxiety (STAI, t = − 2.714, p < .01), whereas Jewish cultural identification appeared to be a predictor for depression (BSI-D, t = -3.853, p < .001) and quality of life (QOL, t = 4.581, p < .001). Notably, these two religiosity variables as well as the two discrimination variables are by their nature highly correlated, which leads to multicollinearity. 4 This effect was found in all four regression models above. Perceived xenophobia was shown to have links to depression (BSI-D, t = 3.428, p < .001) and somatization (BSI-S, t = 2.000, p < .05). Due to multicollinearity, only perceived anti-Semitism was linked to quality of life (QOL, t = − 3.690, p < .001). Income played an important role for all mental health parameters, while duration of residence and legal status did not have a statistically significant effect on any mental health parameters.
However, in the country-wise analysis, significant differences appeared between the subsamples (Table 3). The link between Jewish religious identification and mental health was not found in the Austrian sample, while in the German sample this link was significant for BDI (t=-2.579, p < .05, R2=.059), STAI (t =-2.624, p < .01, R2 = .063) and QOL (t = 2.763, p < .001, R2 = .043). On the other hand, the Austrian sample did show a significant link between Jewish cultural identification and BSI-D (t =-2.907, p < .01, R2 = .178). Perceived xenophobia, on the contrary, is a significant predictor for mental health in the Austrian sample: BDI (t = 2.015, p < .05, R2 = .040), STAI (t = 2.558, p < .05, R2= .063), BSI-D (t = 3.260, p < .01, R2 = .106), BSI-A (t = 2.310, p < .05, R2 = .052), BSI-S (t = 2.205, p < .05, R2 = .047), QOL (t = −3.888, p < .001, R2 = .134). However, in the German sample, perceived anti-Semitism was a less strong predictor, namely only for quality of life [QOL (t = −2.055, p < .05, R2 = .027)], while perceived xenophobia was not a significant predictor at all.
Factors explaining mental health in ex-Soviet Jews, country-wise analysis (stepwise multiple linear regression).
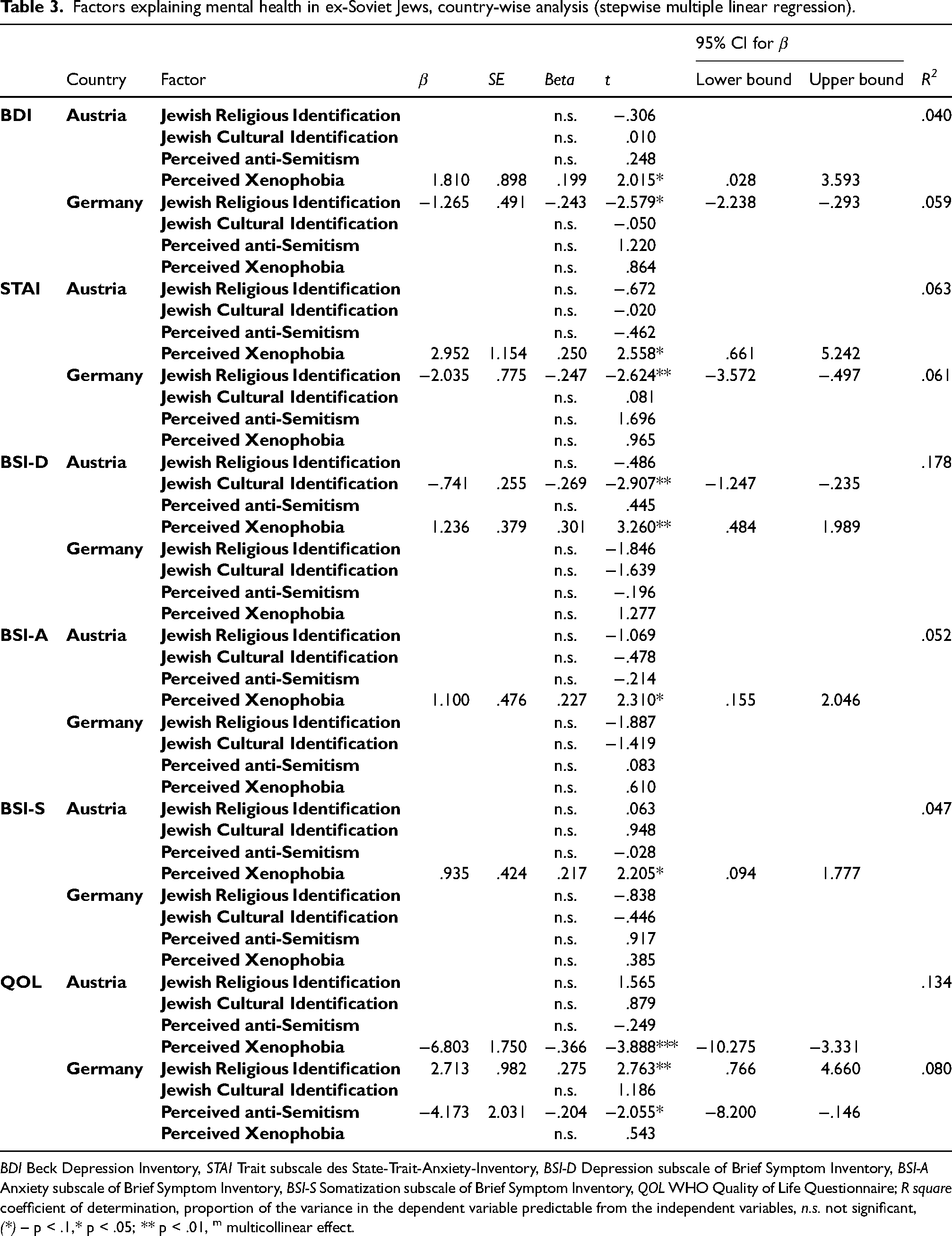
BDI Beck Depression Inventory, STAI Trait subscale des State-Trait-Anxiety-Inventory, BSI-D Depression subscale of Brief Symptom Inventory, BSI-A Anxiety subscale of Brief Symptom Inventory, BSI-S Somatization subscale of Brief Symptom Inventory, QOL WHO Quality of Life Questionnaire; R square coefficient of determination, proportion of the variance in the dependent variable predictable from the independent variables, n.s. not significant, (*) – p < .1,* p < .05; ** p < .01, m multicollinear effect.
According to our model, a very religious (mean value over all religiosity items = 5) ex-Soviet Jew in Germany shows an expected lower level of depression (by nearly 5 points on BDI scale) and anxiety (8 points on STAI scale), as well as higher quality of life (11 points on QOL scale) than his or her non-religious counterpart (mean value over all religiosity items = 1) who has the same level of income and other control variables.
On the other hand, an ex-Soviet Jew in Austria who experiences no xenophobic discrimination (mean value over all perceived discrimination items = 1 (never)) can be expected to show reduced levels of depression (by more than 3 points on BDI, 2.5 points on BSI), anxiety (6 points on STAI, 2 points on BSI), and somatization (2 points on BSI) as well as higher quality of life (13.5 points on QOL) as compared to one who experiences such discrimination often (mean value over all perceived discrimination items = 3 (often)), again controlling for the other variables in our model (Table 3).
Discussion
In the present study, we examined the link of religiosity, perceived anti-Semitism, and xenophobia to mental health among ex-Soviet Jewish immigrants in Austria and Germany. In the combined sample, we found that religious and cultural identity were linked to lower depression and anxiety and increased quality of life. Nevertheless, the findings differed between the Austrian and German subsamples.
Supporting our hypotheses, religious and cultural involvement was associated with substantially lower depression and higher quality of life in the German subsample. Additionally, religiosity was linked negatively to anxiety in this subsample, which is a common finding for Christians but has also been described for some Muslim or Jewish samples (Goldberg & O’Brien, 2005; Koenig et al., 2001; Vasegh & Mohammadi, 2007).
However, our Austrian subsample showed no relation between religiosity and mental health. This finding is not in line with our previous study with this migrant group in Austria, where an effect of religiosity on depression was reported (Trilesnik et al., 2018). These inconsistent findings could be explained by the fact that religiosity is a multifaceted construct and therefore its various aspects as measured by different instruments in both studies could be divergently related to mental health (Hackney & Sanders, 2003). For example, the effect of religiosity on depression found in the previous study could be reflected in the link between Jewish cultural identity and symptoms of depression found in the current study.
The lack of a positive relation between religiosity and mental health in the present study's Austrian subsample is also not in line with other studies on Jewish populations in different countries (e.g., Loewenthal, 2012). A possible explanation for these cross-country differences could be that the relationship between religiosity and mental health varies between different populations. For instance, Braam et al. (2010) highlight differences in the effects of religious coping on depressive symptoms between various migrant groups. Similarly, host country conditions may influence the effect of religiosity on mental health. For example, more prevalent anti-Semitic attitudes might diminish the protective effect of religiosity.
This study also provided interesting results regarding the other factors. Perceived anti-Semitism explained some variance in the mental health of the combined sample but only in terms of quality of life. Perceived xenophobia also predicted quality of life, symptoms of depression (as measured by BSI) and somatization.
A country-wise analysis provided further insight. In the Austrian subsample, depression, anxiety, somatization and quality of life were predicted by perceived xenophobia but not by anti-Semitism, whereas in the German subsample only quality of life was predicted only by perceived anti-Semitism. One possible explanation for this difference could be that xenophobia and anti-Semitism are experienced differently in the two countries. Ex-Soviet Jews in Germany and Austria may feel differently about their respective host society as a whole and their place in it as Jews in a way that goes beyond our measurement of perceived daily discrimination. Two factors that could influence these perceptions are the association with the Holocaust and the remembrance culture, both of which are strongly present in Germany but not in Austria. However, a qualitative approach is required to clarify this question.
Another possible explanation could be that the greater religiosity in the Austrian sample buffers against anti-Semitic but not against xenophobic experiences. Such a mediation was, however, not supported by our data. There could be other mediating or moderating factors not taken into account in our study, pointing to the need for further research. 5
Even though the levels of perceived xenophobia and anti-Semitism did not differ significantly between the German and Austrian migrant subsamples, we did find higher rates of xenophobic and anti-Semitic attitudes in our control group in Austria as compared to Germany. This tendency is also reported in the literature, e.g., Zick et al. (2019) state that 18.8% of the German survey respondents can be categorized as xenophobic, 5.8% as “classically anti-Semitic,” and 24.2% as “Israel-related anti-Semitic.” According to surveys in Austria, the rate of anti-Semitic attitudes in that country is higher than in Germany. For example, 34% of Austrians exhibit the “Israel-related anti-Semitic” attitudes (Zeglovits et al., 2018). Another survey reports Austria as having among the highest rates of anti-Semitism in European comparison (Gottschlich, 2012). Austria underwent a less thorough denazification than Germany, which might explain these high rates of anti-Semitic attitudes.
Moreover, we found that ex-Soviet Jews in Austria display more symptoms of depression than those in Germany. This might be explained by differences between the samples regarding income and legal status or between the countries regarding social welfare options, migration and integration policies, 6 xenophobic attitudes, and ethnic density. Additionally, in line with previous research, the ex-Soviet Jews in both countries show poorer mental health values in our study than the respective control groups. Both findings will be investigated further in a follow-up publication.
There are several limitations to our study. Regarding the sample, first, refusal to participate or non-completion of the questionnaire could be correlated with factors in the model which would have led to sample bias. Second, the great variation in duration of residence could be seen as a limitation, however it reflects the extended migration period in the population under study. Regarding the model, other non-included factors, such as acculturation attitudes, ethnic identity, social inclusion etc., could be relevant for explaining the mental health of migrants. Some of these will also be explored in follow-up publications. Regarding methodology, the chosen cross-sectional as opposed to longitudinal study design cannot establish cause-and-effect relations and delivers only limited conclusions about how factors changing over time impact mental health. Moreover, there are also constraints on the level of insight that purely quantitative research can offer on the complex topic of migration. Mixed-method studies are a promising approach since they could provide a better understanding of how migrants perceive the post-migration process and which factors help or impede coping with it.
Conclusion
In this population-based study with a unique migration research study design, we assessed the mental health in the understudied migrant group of ex-Soviet Jews in different host countries together with the respective control groups. Our findings indicate that religiosity has a protective effect on mental health in ex-Soviet Jewish migrants in Germany and perceived discrimination has an adverse effect on mental health in this group in Austria. Furthermore, our data suggest that the receiving country matters for the mental health of this migrant group, with less favorable conditions found for ex-Soviet Jews in Austria.
Our findings on the positive link between religiosity and mental health could have implications for clinical practice. Specifically, in the therapy context with individuals from this migrant group it would seem beneficial first to include an exploration of religious involvement and potential identity diffusion, social support system, and a feeling of belonging, and second to work on the development of an integrated identity, fostering the social support systems, and enabling better integration in the host society and ethnic group.
Footnotes
Acknowledgements
We gratefully thank Andreas Pähler for the editing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by a PhD scholarship from Ernst Ludwig Ehrlich Studienwerk, Germany.
CORRECTION (December 2022):
Since the original online publication, this article has been updated, please refer to correction notice for it.