
Abstract
Migrants and ethnic minorities are at risk of being under- and overdiagnosed with personality disorders (PDs). A culturally informed approach to the classification of PDs guides clinicians in incorporating migration processes and cultural factors, to arrive at a reliable and valid assessment of personality pathology. In this article, we provide a tentative framework to highlight specific interactions between personality disorders, migration processes, and cultural factors. It is argued that migration processes can merely resemble personality pathology, activate certain (latent) vulnerabilities, and aggravate pre-existing personality pathology. We propose that these migration processes can include manifestations of grief about the loss of pre-migratory psychosocial and economic resources, and the struggle to attain psychosocial and economic resources in the host culture. Moreover, several cultural dimensions are outlined that can either resemble or mask personality pathology. The term “culturally masked personality disorder” is coined, to delineate clinical cases in which cultural factors are overused or misused to rationalize behavioral patterns that are consistently inflexible, distressing, or harmful to the individual and/or significant others, lead to significant impairment, and exceed the relevant cultural norms. Additionally, the role of historical trauma is addressed in the context of potential overdiagnosis of personality disorders in Indigenous persons, and the implications of misdiagnosis in migrants, ethnic minorities, and Indigenous populations are elaborated. Finally, clinical implications are discussed, outlining various diagnostic steps, including an assessment of temperament/character, developmental history, systemic/family dynamics, migration processes, cultural dimensions, and possible historical trauma.
Introduction
Clinicians today are faced with the task of assessing personality disorders (PDs) in an increasingly globalized and culturally diverse patient population. A lack of contextualization of patterns of thinking, feeling, and behaving may lead to misdiagnosis of PDs, particularly among migrants and ethnic minorities. A culturally informed approach to the classification of PDs guides clinicians in incorporating migration processes and cultural factors, to arrive at a reliable and valid assessment of personality pathology.
As Ryder et al. (2015) argue, an approach that places the person in a sociocultural context can guide clinicians to assess PDs in a more contextually grounded way, rather than locating the patient’s problems entirely within the individual. A contextual perspective on PDs should include an assessment of temperament/character, developmental history, systemic/family dynamics, migration processes, cultural dimensions, and possible historical trauma.
The current article provides a tentative framework to highlight specific interactions between PDs, migration processes, and cultural factors. We offer suggestions on how migration processes could resemble several PD traits, how certain (latent) vulnerabilities could be manifested in a post-migratory context, and how pre-existing personality pathology could be aggravated. Additionally, we offer suggestions on how several cultural dimensions could resemble or mask personality pathology. Finally, the role of historical trauma is addressed in the context of potential overdiagnosis of PDs in Indigenous persons, and the implications of misdiagnosis in migrants, ethnic minorities, and Indigenous populations are discussed. We emphasize that the following paragraphs primarily offer hypotheses that can generate future research in the field of PDs, migration, and culture.
Culturally informed perspectives on PDs
In a critique of the conceptualization of PDs, Fabrega (1994) argues that many of the characteristics of PDs constitute deviations in behavior that are conceptualized purely in terms of contemporary Anglo-American norms. He states that culture has been discouraged from challenging the scientific foundation and content of psychiatric categories, including the domain of PDs (Fabrega, 2001). Similarly, Mulder (2012) argues that the conceptualization of PDs as medical entities was largely a Western phenomenon, and that PDs are “based on a concept of the self and on values that have evolved in Western societies” (p. 260). His main objection is how PDs are “objectified as impersonal phenomena separate from social and cultural values” and portrayed as “pan-cultural and universal” (Mulder, 2012, p. 262). Millon et al. (2004), for example, conclude that all DSM-IV PDs have evolutionary underpinnings, and are therefore cross-culturally valid.
Looking at empirical studies on personality traits across cultures, different studies using the Five Factor Model of personality do support the concept of cross-cultural validity of the corresponding personality traits, although there are cultural mean differences in trait scores (Allik, 2005; McCrae et al., 2005; Rolland, 2002). As Piedmont et al. (2009) describe, these five personality domains are thought to be “genetically based, empirically robust and universal aspects of personality that offer a useful framework for understanding [PDs]” (p. 1245). Kendler et al. (2011) argue that “the etiological factors underlying normal and abnormal personality are either identical or highly correlated, and that the high phenotypic correlation and joint factor structure observed between [normal and abnormal personality] should result from common genetic and environmental factors” (p. 350). For example, there is a strong positive phenotypic association between borderline PD traits and neuroticism, and negative associations with conscientiousness and agreeableness (Samuel & Widiger, 2008). In this context, Widiger (2011) points out how premorbid personality traits can provide a vulnerability (or a resilience) to stress, which explains why some collapse under life stresses (such as migration), while others remain unscathed by severely traumatic circumstances. Thus, normal and abnormal personality are strongly related at the etiologic level, and abnormal personality seems to represent extremes on continua in common with normal personality (Markon et al., 2005). This can explain the findings that most PDs are found in various non-Western cultures, albeit with varying prevalence rates (Leung & Leung, 2009; Loranger et al., 1994; Moriya et al., 1993; Tang & Huang, 1995; Yang et al., 2000). The study by Loranger et al., for example, concluded that PDs can be classified with reasonably good reliability in 11 different countries in North America, Europe, Africa, and Asia, using a semi-structured clinical interview.
Nonetheless, Lin (1997) rejects the reliability criterion as a basis for the universal application of PDs, by referring to Kleinman’s category fallacy: “The reification of one culture’s diagnostic categories and their projection onto patients in another culture, where those categories lack coherence and their validity has not been established” (Kleinman, 1988, pp. 14–15). The previously cited study by Leung and Leung (2009), for example, addresses this issue to some extent by also assessing the construct validity of borderline PD in a Chinese population.
Kleinman’s caution is underscored by several findings, suggesting that diagnostic biases may inflate rates of several PDs among migrants and ethnic minorities. For instance, Salas-Wright et al. (2014) found that second-generation immigrants are significantly more likely to meet criteria for borderline PD than native-born Americans. Schizoid PD was diagnosed more often in African-Americans and Caribbean Blacks compared to European Americans (Gibbs et al., 2013). Wu and colleagues (2013) found that mixed-race patients were more likely to have a PD diagnosis. Additionally, borderline PD was diagnosed more often in Hispanics than in Caucasians and African-Americans (Chavira et al., 2003), possibly due to ‘acculturative stress’ or ‘diagnostic bias’ (p.488)
Contrary to these findings, other researchers have found no significant ethnic differences in DSM-IV cluster A, B and C PDs (Lenzenweger et al., 2007), or have found some evidence of ethnic variations but caution that methodological characteristics can account for some of the variation (McGilloway et al., 2010). Interestingly, in the latter (systematic review) study, it was concluded that British Black patients were less likely than their White counterparts to receive a diagnosis of PD, when assessed using clinicians’ case notes only, suggesting that PDs may also be underdiagnosed in routine clinical practice (McGilloway et al., 2010). In addition to potential diagnostic biases, underdiagnosis could also result from differences in help-seeking behavior per ethnic group and structural barriers to services (Clement et al., 2015).
Misdiagnosis of PDs among migrants and ethnic minorities can come at great costs. First, overdiagnosis of PDs can lead to psychiatric stigma (Haslam, 2011), and result in various psychological essentialist views: it can distract clinicians from institutional discrimination, structural inequalities, and systemic oppression, which can produce racialized, gendered, and class-related “symptoms” in clinical settings (Metzl & Hansen, 2018). Second, underdiagnosis of PDs may lead to ineffective management strategies, treatment delay, and, given the economic burden of PDs (Soeteman et al., 2008), higher direct and indirect medical costs.
The focus in this article is on the PD criteria of the DSM-5, which is a widely used psychiatric classification system and the basis for extensive research on PDs. There is an increased recognition in the DSM-5 of the role of culture in diagnostic assessment, as outlined in the Cultural Formulation chapter. Additionally, the DSM-5 specifies brief “culture-related diagnostic issues” for most PDs. To counter misdiagnosis, the DSM-5 specifically states that “[PDs] should not be confused with problems associated with acculturation following immigration or with the expression of habits, customs, or religious and political values professed by the individual’s culture of origin” (APA, 2013, p. 648). The purpose of this article is to provide an in-depth overview of such cultural factors, particularly in the context of migratory and acculturative stress, which clinicians may incorporate more systematically in their diagnostic assessment.
We will discuss the role of migration processes and cultural dimensions in the assessment of PDs first separately to emphasize the importance of both factors. The section on Clinical Implications will, eventually, outline a number of diagnostic steps, highlighting an integrative perspective on the significance of culture and migration for PD assessment.
Assessing PDs in migrants
In the following section, we offer hypotheses on how migration processes can overlap with PD traits, leading to potential overdiagnosis, and how migration processes can lead to manifestation of certain (latent) vulnerabilities, and aggravation of pre-existing personality pathology. In this context we also elaborate on how the assessment of PDs in migrants is complicated by the fact that migration processes can manifest in a delayed manner or co-occur with the possible development of PD traits.
Overdiagnosis of PDs in migrants
A migrant is defined here as a person who moves voluntarily from one place to another to find better living conditions (i.e., immigrant, expatriate), or a person who leaves their country involuntarily to escape war, persecution, or natural disaster (i.e., refugee, exile). In this process, migrants are at greater risk of developing post-traumatic stress disorder (PTSD), depression (Fazel et al., 2005; Steel et al., 2009), and schizophrenia (Cantor-Graae & Selten, 2005).
During the postmigration acculturation phase, migrants (and their offspring) can display several modes of thinking, feeling, and behaving that can resemble various maladaptive personality traits. This can occur in the process of attaining psychosocial goals (i.e., developing a new (hybrid) cultural identity, forming close relationships, building a social network; Bhugra, 2004) and economic goals (i.e., acquiring social status, financial means and material resources, opportunities for work and education; Bhugra, 2004). For example, a strong emphasis on status and high achievement standards could be typified as bordering on narcissistic or compulsive, while this behavior can be adaptive in positioning oneself in the host society (Torres & Wicks-Asbun, 2014). Similarly, migrants can show modes of thinking, feeling, and behaving that resemble various maladaptive personality traits in the process of grieving about the loss of pre-migratory psychosocial resources (loss of cultural identity, loss of emotional attachments, loss of social support systems) and economic resources (loss of a position or business, loss of a social hierarchical position, loss of financial and material resources, loss of status symbols; Bhugra, 2004; Bhugra & Jones, 2001). For example, migrants grieving about the loss of these economic resources could boast about their pre-migratory social status and living standard, which could be misinterpreted as displays of self-aggrandizement.
In this sense, migration employs specific survival strategies that could resemble pathological behavioral traits, but are in essence adaptive, functional, and/or temporary in nature. In this context, clinicians should be able to distinguish pathological defenses from adaptive coping (Comas-Diaz & Minrath, 1985).
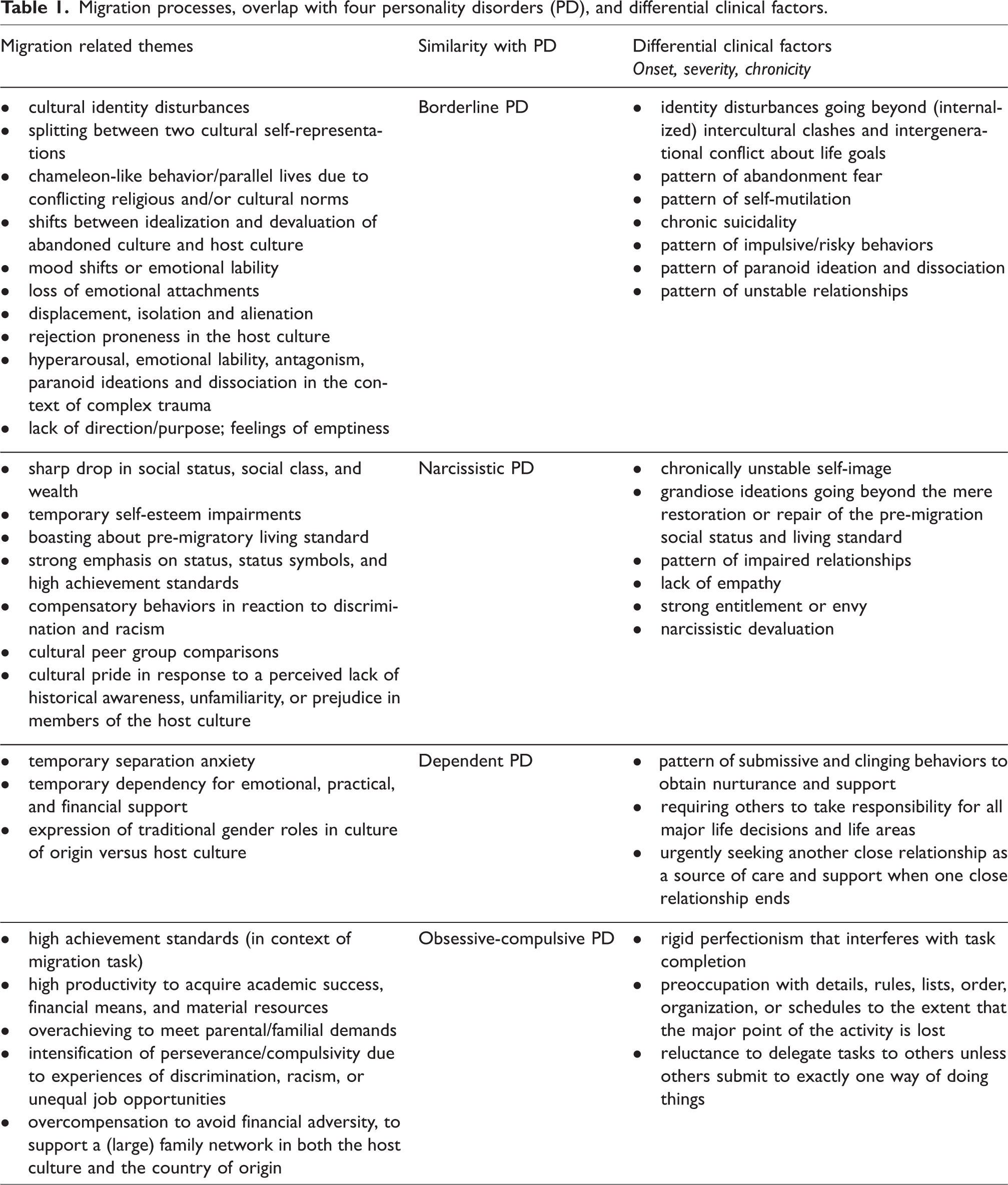
We propose that migrants are at risk of being overdiagnosed with (at least) one of four PDs, including the borderline, narcissistic, dependent, and obsessive-compulsive PD. These four PDs in particular touch upon specific migration-related themes such as identity, attachment, abandonment, status-seeking, pride, initiating and sustaining new relationships, (in)dependency, and high achievement standards.
Borderline PD
The borderline PD criterion of identity disturbance can be confused with cultural identity disturbances and fragmented identities that the migrant acquires. The migrant can display splitting between two contrasting or mutually exclusive self-representations from different cultures, display complex hybrids of various cultural identities, or display shifts between idealization and devaluation of the abandoned culture versus the host culture (Akhtar, 1999; Benet-Martínez & Haritatos, 2005).
Also, conflicting religious and cultural norms can lead to chameleon-like behavior in the form of parallel lives with different sets of beliefs, values, goals, and behaviors. Internalized clashes between cultural values from the host culture versus the culture of origin, and intergenerational conflict (driven by strong familial enmeshment) about life goals can lead to chronic indecision, rapidly switching between life goals, or reporting a lifelong experience that most important life choices were not one’s own. In addition, the sense of displacement, isolation, and alienation following migration, including the sense of not being rooted anywhere or connected to significant others, combined with the migrant’s loss of close relationships and emotional attachments, could lead to symptoms resembling the borderline criteria of identity diffusion and abandonment fear. The migrant’s limited social network and rejection proneness (i.e., ‘acculturative stress’ (Berry, 2006) in the host culture can intensify such abandonment fears. A related concept is ‘cultural bereavement’ (Eisenbruch, 1991): “the experience of the uprooted person or group resulting from loss of social structures, cultural values, and self-identity” (pp. 673–674). The rapid shifts of intense rage, sadness, and anxiety, resulting from ruminating about various losses and the uncertain future, could resemble the criterion of affective instability. Ronningstam et al. (2018) note that “Suicidal ideations and behavior can in this context be caused primarily by subjective or social and interpersonal experiences related to acculturation” (p. 7).
Refugees, with a history of persecution, imprisonment, and torture, can display hyperarousal, emotional lability, antagonism, paranoid ideation, and dissociation as part of complex trauma (Liddell et al., 2019), which could resemble the borderline criterion of transient, stress-related paranoid ideations, or severe dissociative symptoms. Chronic experiences of boredom or worthlessness, stemming from the migrant’s experience of lacking purpose or direction, could resemble the criterion of feelings of chronic emptiness.
In the differential diagnostics of the borderline PD the following factors need to be considered and assessed: identity disturbances going beyond (internalized) intercultural clashes and intergenerational conflict about life goals, the presence of chronic suicidality, a pattern of impulsive/risky behaviors, a pattern of self-mutilation, recurring paranoid ideations and dissociation, and a pattern of unstable relationships.
Narcissistic PD
A sharp drop in social status, social class, and wealth following migration could deliver blows to the self-image, triggering various strong affective responses like anger, shame, sadness, and jealousy, possibly also long after the loss has occurred. These losses include the loss of jobs, loss of status and prestige, loss of occupational networks, the devaluation or rejection of degrees or diplomas in the host culture, and the loss of financial and material resources (Ronningstam et al., 2018). In this context Akhtar (2011) states: “If the vocational shift is sharply downward, the resulting psychic turmoil can be great indeed” (p. 39). The grief associated with these losses can be masked by the patient boasting about his or her previous positions and possessions, or by displaying intense anger and resentment about their post-migratory living standard, which could be misinterpreted as displays of self-aggrandizement. In addition, a strong emphasis on status, status symbols, and high achievement standards can be misinterpreted as a search for narcissistic supply in the context of grandiose ideations. In this context, Alarcón and Foulks (1995) note: “Desires of recognition, coupled with feelings of envy toward people perceived as more successful, are often transient responses to individuals from certain social and cultural groups who feel estranged from the mainstream” (p. 9).
Akhtar (2011) notes several restrictions on an immigrant’s work-related success, including racial, ethnic, and religious prejudice. Such experiences of discrimination and racism in social, educational, and occupational spheres could lead to overcompensatory behaviors, which could be mistaken for antagonistic traits such as hostility or grandiosity. In addition, ethnic minorities can elaborately boast about their cultural heritage, particularly when they experience unfamiliarity, prejudice, or a lack of historical awareness in the host culture, which could present itself as self-glorification and superiority. Finally, continual comparisons with the cultural peer group can lead to feelings of jealousy or inadequacy. As Akhtar describes, “differences in the velocity or extent of acculturation are not well tolerated,” and can lead to “hidden rivalries” (p. 87).
In the differential diagnostics of the narcissistic PD the following factors need to be considered and assessed: a chronically unstable self-image, grandiose ideations going beyond the mere restoration or repair of the pre-migration social status and living standard, a lack of empathy in intimate relationships, strong entitlement or envy, narcissistic devaluation, and a pattern of impaired relationships.
Dependent PD
Migrants who enter a novel environment with new societal structures and limited knowledge about day-to-day life, and who lack support of family members or friends, can display temporary separation anxiety, and a temporary clinginess or dependency on others for emotional, practical, and financial support. They can also temporarily display hesitation in initiating new tasks or taking up responsibility due to lack of confidence. The level of self-sufficiency of the migrant in the host culture is dependent upon several factors including language proficiency, social support systems, and socio-economic factors (Chung et al., 2008). Clinicians need to be careful in solely attributing dependency behaviors during the liminal phase of migration to the realm of personality. Furthermore, different expressions of (traditional) gender roles in the culture of origin versus the host culture could lead to overdiagnosis of this PD in migrants from patriarchal and collectivist societies, where for example women are on average socio-economically more dependent on their male counterparts. Similarly, Chen et al. (2009) argue that the DSM-IV conceptualization of the dependent PD is based on American individualistic cultural norms which could pathologize East-Asian Confucian beliefs. Chen et al. (2009) state: “acting submissively and dependently may be a good coping strategy and a sign of emotional regulation, rather than a direct display of an individual’s personality” (p. 798). The DSM-5, however, does caution that “an emphasis on passivity, politeness, and deferential treatment is characteristic of some societies and may be misinterpreted as traits of dependent personality disorder” (p. 677).
In the differential diagnostics of the dependent PD the following factors need to be considered and assessed: a pattern of submissive and clinging behaviors to obtain nurturance and support, requiring others to take responsibility for all important life decisions and life areas, and urgently seeking another relationship as a source of care and support when a close relationship ends.
Obsessive-compulsive PD
Migrants can display high achievement standards and high productivity to acquire academic success, status, financial means, and material resources in the host society. An internal or external drive (i.e., parental expectations) to excel and “to make it” in the host culture can resemble strong compulsivity or perfectionism. Experiences of discrimination, racism, or inequality can intensify perseverance and compulsivity in order to obtain positions, achieve academic success, or build a business. An emphasis on status, status symbols, and financial affluence can also reflect the migrant’s underlying fear of losing control, or a strong need to be self-reliant, and avoid exposures to previous financial adversity. In addition, when the migrant is the sole provider for a (large) family, and/or faces (financial) expectations from family members in the country of origin, he or she can be excessively devoted to work and productivity to the exclusion of leisure activities and friendships. As Akhtar (2011) notes: “to give money, one needs to acquire money and this, in part, fuels the immigrant’s ambition and “work addiction” (p. 50).
In the differential diagnostics of the obsessive-compulsive PD the following factors need to be considered and assessed: rigid perfectionism that interferes with task completion, preoccupation with details, rules, lists, order, organization, or schedules to the extent that the major point of the activity is lost, and the reluctance to delegate tasks to others, unless others submit to exactly one way of doing things.
Underdiagnosis of PDs in migrants
Alongside these important precautions to prevent potential overdiagnosis of PDs in migrants, migration could also in fact activate (latent) vulnerabilities or aggravate pre-existing personality pathology. In this context, Ziegenbein et al. (2008) argue: Migration can [also] be understood as a risk factor and potential inductor for [PD]. Migration as a cultural, social, and geographical phenomenon can also, due to the process-inherent vulnerability, directly function as a pathogenic (and naturally pathoplastic) factor for [PD]. (p. 44)
In a similar vein, Paris and Lis (2013) note: Patients who have not suffered from BPD in their country of origin can develop this condition once they immigrate to the West. One possible explanation is that when one grows up in a more traditional society, behavior is more closely monitored, and emotional stability is promoted by having provided social roles, associated with the support of extended families and a tightly knit community. (p. 146)
It is noted here that migration can particularly serve as a risk factor and potential inductor in migrants with a history of early life stressors, and a subsequent development of early maladaptive schemas (Young et al., 2003). For example, a patient with a history of parental neglect or abandonment could function at a subclinical level in an environment that offers a sufficient degree of continuity between generations, social cohesion, and (cultural) identity (Paris, 1996). In the case of sudden or involuntary migration, the few protective layers that partially suppress impulsivity, emotional instability, and identity diffusion are removed (Ronningstam et al., 2018). The resulting clinical symptoms not only entail the hallmarks of a borderline PD, but in a cyclical process also sustain the inability to achieve various migration goals. The lack of familial support and social cohesion can trigger and feed pre-existing borderline cognitive schemas like abandonment, mistrust, and emotional deprivation, while these same schemas hamper the attainment of a hybrid (cultural) identity, intimate relationships, and a social network. This can lead to a scenario in which personality pathology has not yet manifested in adolescence / early adulthood but exists at a subclinical level. This is in line with dimensional approaches to PD classification that assess the degree to which a patient meets diagnostic criteria instead of a presence-absence judgement (Ofrat et al., 2018). As Ofrat and colleagues argue, a dimensional approach can improve diagnostic subtlety in patients who present with subclinical features of PDs that may still be impairing.
In the case of the patient predisposed to narcissistic personality pathology, early parental overemphasis of the child’s specialness or harsh criticisms of failures and shortcomings, leading to the development of cognitive schemas such as defectiveness, grandiosity, and approval-seeking, could complicate the mourning process associated with the loss of social status, social class, and wealth following migration. In other words, the losses associated with involuntary migration could deliver blows to an already fragile sense of self, making it much harder to recuperate. In addition, a sense of entitlement and grandiosity can lead to the unwillingness to put in the effort needed to reposition oneself in the host society, resulting in the unwillingness to accept a job perceived as below one’s level, or the expectation that one’s talents should be noticed without putting in the required work, which could complicate the attainment of economic goals.
In the case of the patient predisposed to obsessive-compulsive personality pathology, the process of acquiring academic success, status, financial means, and material resources can aggravate pre-existing strong perfectionism and high achievement standards. In the case of the patient predisposed to dependent personality pathology, the loss of emotional, practical, and financial support could lead him or her to latch on even more to significant others, reinforcing previous dependency behaviors.
Mapping the longitudinal nature of PD traits in migrants
Although the DSM-5 criteria for PDs require that patterns of pathological inner experience and behavior are stable and of long duration, and its onset can be traced back at least to adolescence or early adulthood, clinicians are faced with several scenarios that could complicate the assessment of PDs in migrants and their offspring.
First, migration can take place after adolescence / early adulthood, allowing the clinician to assess pre-migration and post-migration functioning in various life areas, and thus map the longitudinal nature of PD traits. Second, migration can logically also occur before adolescence / early adulthood, leading to a scenario in which migration processes potentially manifest in a delayed manner, for example when young migrants are faced with developing a hybrid cultural identity from very different cultural norms and values. Disturbances in forming a hybrid identity, shifts between idealization and devaluation of the culture of origin and host culture, and feelings of displacement and alienation may all manifest at an older age, years after the actual migration took place. Third, migration can occur during adolescence / early adulthood, leading to the co-occurrence of migration processes and possible development of PDs traits in the same timeframe, obfuscating which behaviors are a result of migration stressors / acculturation problems, personality pathology, or both.
To assist the clinician in disentangling migration processes from PD traits, we provide an overview of migration processes, as outlined in this paragraph, as differential factors.
Table 1 shows per PD which migration processes could resemble PD traits and could thus lead to overdiagnosis of personality pathology, and which differential clinical factors need to be assessed.
Migration processes, overlap with four personality disorders (PD), and differential clinical factors.
A case example is presented to illustrate the potential overlap between DSM-5 PD criteria and the before-mentioned migration processes.
Case example 1
Farshid is a 35-year-old Iranian male political refugee. He fled from Iran to the Netherlands five years ago, due to fears of persecution. In Iran he worked as an underground dissident journalist, reporting human rights violations. He has been unemployed now for several years and is hesitant to accept any job “under his level.” He aims to write new articles and send them to several renowned international newspapers. He frequently elaborates on his previous status, high-profile connections, and importance of his journalism work. He complains about the lack of political awareness of his Iranian peer group and views himself as more intelligent and cultivated than those dealing with the “superficialities of everyday life.” He also elaborates on how people are misinformed on Iranian culture. He is frequently caught up in discussions about Persian history and states that, if foreign powers had not intervened in Iran, it would have been a superior and prosperous nation.
From the perspective of DSM-5 narcissistic PD criteria, one could argue that, in one life domain (occupational domain), Farshid 1) has an exaggerated sense of self-importance, 2) expects to be recognized as superior, 3) is preoccupied with fantasies about success and brilliance, and 4) behaves in an arrogant or haughty manner. The clinician needs to assess the age of onset of these behavioral patterns, whether Farshid meets these criteria in several life domains, and to what extent there is significant distress or impairment. The clinician also needs to assess whether he meets other narcissistic PD criteria in various life domains, including a pattern of impaired relationships, a lack of empathy, strong entitlement or envy, and narcissistic devaluation.
From the perspective of the migration themes provided in Table 1, Farshid is undergoing the following migration processes: 1) a sharp drop in his social status, social class, and wealth, 2) temporary self-esteem impairments, 3) boasting about his pre-migratory living standard, 4) a strong emphasis on status, status symbols, and high achievement standards, and 5) cultural pride in response to a perceived lack of historical awareness, unfamiliarity, or prejudice among members of the host culture.
The question is whether Farshid’s behavioral patterns merely consist of the aforementioned grief about the loss of psychosocial and economic resources, and the struggle to attain new psychosocial and economic resources, or whether his (involuntary) migration activated latent narcissistic traits or aggravated pre-existing narcissistic traits. For a full overview of the diagnostic steps that need to be taken, we refer to the Clinical Implications section.
Overdiagnosis and underdiagnosis of PDs in ethnic minorities
The same complications in the assessment of PDs in migrants can also be found in the assessment of PDs in ethnic minorities, although these two areas often overlap. To minimize the risks of overdiagnosis in ethnic minorities, the following cultural dimensions need to be taken into account: 1) collectivism–individualism, 2) interdependent self-concept – independent self-concept, 3) traditional gender roles – non-traditional gender roles, 4) emotional expressiveness – emotional inhibition, and 5) supernatural–material. Although this list of cultural dimensions is not exhaustive, behaviors stemming from these dimensions are regarded as most likely either to merely resemble or to mask underlying personality pathology.
Collectivism–individualism
Brewer and Chen (2007) have outlined three levels within the collectivism–individualism dimension, divided by locus of identity, locus of agency (beliefs), and locus of obligation (values). Two out of three levels are discussed here. One level is the individual level, in which the locus of identity involves individual uniqueness, a core essence, and consistency. The locus of agency involves the belief in individual agency and responsibility as the basis for achievement. The locus of obligation involves self-interest as primary, pursuing personal preferences, self-actualization, freedom, and independence. Another level is the collectives level, in which the locus of identity involves social identification and where the group defines the self. The locus of agency in the collectives level involves achievements based on collective interdependence, and the locus of obligation involves obligation to group welfare and conformity to group norms.
There is a striking overlap between these concepts of locus of identity and locus of agency/obligation, and the Alternative DSM-5 Model for Personality Disorders conceptualization of personality pathology as involving significant impairments in the areas of identity and self-direction. One could argue that this alternative model favors Brewer and Chen’s definition of the individual level (a core essence, consistency in the self, independence, and self-actualization), and could put those who identify with Brewer and Chen’s definition of the collectives level at risk of being labeled as excessively dependent on others for identity definition, with compromised boundary delineation, a weak sense of autonomy or agency, experiencing a lack of identity, and over-identification with others.
Interdependent self-concept – independent self-concept
Although the interdependent self-concept – independent self-concept dimension has theoretical overlap with the collectivism–individualism dimension, in this article it is described solely in the context of intimate relationships. Markus and Kitayama (1991) argue that depending on the cultural context, individuals can have strikingly different construals of the self, of others, and of the interdependence between self and others. They delineate an independent versus interdependent view of the self. The independent self is defined as “construing oneself as an individual whose behavior is organized and made meaningful primarily by reference to one’s own internal repertoire of thoughts, feelings, and action, rather than by reference to the thoughts, feelings, and actions of others” (Markus and Kitayama, 1991, p. 226). The interdependent self is defined as: seeing oneself as part of an encompassing social relationship and recognizing that one’s behavior is determined, contingent on, and to a large extent organized by what the actor perceives to be the thoughts, feelings, and actions of others in the relationship. (Markus and Kitayama, 1991, p. 227)
Markus and Kitayama’s description closely resembles Aron et al.’s (1991) self-expansion model which posits that people with whom we have close relationships progressively come to be included within the self, and are thus even treated as self due to weakened boundaries, and a confusion between the self and significant others. There is a risk that in the context of intimate relationships this culturally determined dimension could be confused with or translated into psychodynamic constructs such as strong enmeshment, symbiotic relationships, identity diffusion, merging, idealization, or co-dependency.
Misuse or overuse of the collectivism–individualism and interdependent–dependent self-concept constructs
At the same time, a patient’s match with Brewer and Chen’s collectives level does not exclude the presence of a dependent PD, and a match with Markus and Kitayama’s interdependent self-concept does not rule out the possibility of a narcissistic, borderline, or dependent PD. These cultural dimensions should be weighed and taken into consideration, but not misused by the clinician, patient, or significant others to rationalize behavioral patterns that are consistently inflexible, distressing, or harmful to the individual and/or significant others, lead to significant impairment, and exceed the relevant cultural norms. Pathological personality traits in ethnic minorities can therefore also be misclassified as “stereotypical” for the patient’s socio-cultural background, while the chronicity or severity of pathological behavior is downsized or overlooked.
This phenomenon is labeled here as a “culturally masked PD”: the behavioral patterns match certain aspects of what is culturally accepted or dictated, but still exceed the relevant cultural norms, cause significant distress to the patient and/or others, and lead to impairment in different life areas. In this context, Castillo (1997) notes: “when a person’s dependent behavior greatly exceeds his or her own cultural norms, thus causing clinically significant distress, a diagnosis of dependent PD should be made” (p. 108). Similarly, Mulder (2012) states: “extreme independence or interdependence might be risk factors for personality pathology regardless of the society individuals find themselves within” (p. 266).
Additionally, Tang and Huang (2006) warn that “the blind application of cultural yardsticks runs the risk of subjective interpretation of PDs in the name of culture” (p. 145). They emphasize that individuals from the same culture disagree about whether or not certain behaviors are acceptable within their own culture, “which is frequently encountered in a society undergoing rapid changes when successive generations adopt different behavioral codes in adapting to societal changes” (p. 145). Consequently, due to well-intentioned cultural caution in classifying PDs in ethnic minorities, the dangers of underdiagnosis could be as great as those of overdiagnosis.
Traditional gender roles – nontraditional gender roles
Research on the relationship between gender roles and PDs has revealed sex differences in prevalence rates (Braamhorst et al., 2015). Women are more often diagnosed with borderline, dependent, and histrionic PDs, while men are more often diagnosed with narcissistic, compulsive, and antisocial PDs (Anderson et al., 2001). This can reflect true sex differences or reflect a sex bias in diagnosing PDs.
Different cultures can dictate different ways of adhering to (hyper)masculine or (hyper)feminine gender roles, and these can match or conflict with gender roles in the host culture. The therapist’s notion of what an adaptive gender role entails can impact how the male or female ethnic minority is viewed. A male patient’s hypermasculine traits such as aggression, dominance, and grandiosity could be reinforced in the culture of origin, while being denounced in the host culture. The same applies to the female patient who is rewarded for displaying hyperfeminine traits such as humility, seductiveness, and self-sacrifice, but is labeled as histrionic and unassertive in the host culture. Awareness of the possible contrasts between gender roles in the culture of origin versus the host culture could minimize the risks of over-diagnosis of PDs.
It is furthermore noted that a culture that advocates high male dominance or male privilege, sexism, and misogyny points to a macro-level socio-cultural condition that is beyond the realm of psychiatry. For example, a male patient who displays emotional, physical, and sexual abuse of women, reinforced by misogynistic cultural values, could unequivocally meet the criteria of a DSM-5 PD, but the point here is that not all harmful behavior necessarily originates from mental disfunction.
Emotional expressiveness – emotional inhibition
Norms for emotional expressiveness versus emotional inhibition vary widely across cultures. In the context of the histrionic PD, for example, Ziegenbein et al. (2008) argue that “hyper-emotionality, seductiveness, tendency to dramatize in interhuman relations are to a certain degree culturally determined personality traits” (p. 43), causing patients from the Mediterranean and from Latin America to be overdiagnosed with this PD. Similarly, Ziegenbein et al. warn that flamboyance and an exaggerated evaluation of one’s importance, supposedly more common in men from Southern European or Latin American cultures, can be misinterpreted as narcissistic PD. Also, behaviors such as passivity, obedience, and dependence, desired behaviors in Asian societies, can be misinterpreted as part of an avoidant or dependent PD. Ziegenbein et al. (2008) conclude that the same error applies to “confounding religious conservatism or adjustment to rigid social rules with compulsive [PD]” (p. 43).
Supernatural–material
Cultures differ in the extent to which they adhere to supernatural beliefs. Paniagua and Yamada (2013) describe the following warning in diagnosing ethnic minorities with a schizotypal PD: Cognitive and perceptual distortions may be associated with religious beliefs and rituals, which may appear to be schizotypal to clinicians uninformed with these cultural variations. Examples of these distortions include voodoo ceremonies, speaking in tongues, belief in life beyond death, mind reading, evil eye, and magical beliefs associated with health and illness. (p. 35)
Similarly, Castillo (1997) warns that “[the schizotypal PD] is most appropriately used in modern societies where superstitiousness and magical thinking are not consistent with the prevailing cultural schemas” (p. 101). However, it is of course possible that cognitive and perceptual disregulation, unusual beliefs and experiences, suspiciousness, and withdrawal can lead to considerable personal distress and impairment in functioning, and exceed the norms tied to religious beliefs and rituals.
A case example illustrates the potential overlap between DSM-5 PD criteria and several of the before-mentioned cultural dimensions.
Case example 2
Diego is a 35-year-old Argentinian male patient, who moved to the Netherlands in early adulthood. He reports obsessive thoughts after his girlfriend ended their relationship. He is determined to restore the relationship and wants advice on how to proceed. According to his girlfriend, he was too demanding and controlling, and she needed space. Patient describes that most of his previous relationships have been like rollercoasters, and that his previous partners increasingly felt suffocated. He expected them to text or call him several times a day, otherwise he felt like the connection was lost. He also wants women to comply with his wishes and ideally to “submit.” He displays desperate attempts to restore the contact, and sends them elaborate love letters and gifts. He does not view his own behavior as problematic, and says it is a reflection of his Latino warmth, passion, and masculinity. He argues that in Latin-American romantic love relationships, it is normal that two lovers eventually “merge.”
From the perspective of DSM-5 borderline PD criteria, one could argue that, in one life domain (personal relationships), Diego seems to meet the criteria of 1) a pervasive pattern of instability of personal relationships, and 2) a frantic effort to avoid real or imagined abandonment. From the perspective of DSM-5 narcissistic PD traits, in one life domain (personal relationships), Diego 1) requires excessive admiration, 2) has a sense of entitlement, and 3) lacks empathy. The clinician needs to assess the age of onset of these behavioral patterns, whether Diego meets these criteria in several life domains, and to what extent there is significant distress or impairment. The clinician also needs to assess whether he meets other criteria of the borderline and narcissistic PDs.
From the perspective of cultural dimensions, the following dimensions need to be weighed and taken into account. Diego seems to conform to an interdependent self-concept (wanting to blur the boundaries between himself and the other). Diego emphasizes that this is how ideal love is viewed in Latin-American culture. He adheres to traditional gender roles (hypermasculine, strong need for admiration, sexually seductive, dominant, and grandiose), and he says his emotional expressiveness matches Latin-American culture (hyper-emotional, seductive, and dramatic). For an overview of the diagnostic steps that need to be taken, refer to the Clinical Implications section.
Historical trauma and PDs
In the assessment of PDs, particularly (but not exclusively) in Indigenous persons, the inclusion of historical trauma could allow for a broader contextualization of cognitive, emotional, and behavioral patterns. As Balaratnasingam and Janca (2017) point out, “when large numbers of people experience similar problems, the diagnosis of PD may be less meaningful than re-conceptualizing this as the trickle-down effects of assimilatory policies and forcible deculturation” (p. 34). Although the links between psychological trauma and PDs are well established, the links between historical trauma and PDs are relatively unknown.
Gone (2013) describes how historical trauma is conceptually distinguished from PTSD: [Historical trauma] is described as a collective phenomenon shared by members of an identifiable group who have experienced deliberate conquest, colonization, or genocide, whereas PTSD remains a disorder of the individual. For example, the members of any given Native community may have together grappled with particular expressions of colonial subjugation, including military conquest, epidemic disease, forced relocation, reservation captivity, religious suppression, resource theft, environmental degradation, government dependency, and coercive assimilation. Thus, [historical trauma] is described as incorporating both the psychological and social sequelae of historical oppression whereas PTSD (…) is largely confined to the psychology (…) of the individual. (p. 687)
Balaratnasingam and Janca (2017) argue that assessing PDs in Indigenous persons is “complicated by historical trauma from colonization, disruption of kinship networks, and ongoing effects of poverty and social marginalization” (p. 31). They argue that Indigenous Australian communities are based on the needs of the extended kinship network, which may lead to overdiagnosis of dependent and avoidant PDs. Also, in the context of colonization and oppression, antisocial or narcissistic behaviors can be understood as adaptive survival mechanisms; distrust of authority and resistance to control may also lead to misdiagnosis of paranoid or schizotypal PD. Similarly, Fromene et al. (2014) compared the nine borderline personality symptoms with alternative interpretations based on historical and social contexts reported by Indigenous Australians formally diagnosed with a borderline PD. For example, the criterion of “frantic efforts to avoid real or imagined abandonment” can be viewed as stemming from removal from birth families, violence, and neglect in the aftermath of colonization. Similarly, the criterion of identity disturbance in Indigenous persons can be viewed in the context of “racism, walking in two worlds, [and] removal from culture” (Fromene et al., 2014, p. 570).
Conclusion
Given increasingly globalized and culturally diverse patient populations, it is vital that clinicians take a contextual perspective on PDs, including an assessment of temperament/character, developmental history, systemic/family dynamics, migration processes, cultural dimensions, and possible historical trauma. Overdiagnosis of PDs in migrants and ethnic minorities (including Indigenous persons) can lead to psychiatric stigma and can distract the clinician from institutional discrimination, structural inequalities, and systemic oppression, while underdiagnosis of PDs may lead to ineffective management strategies, treatment delay, and higher direct and indirect medical costs.
We argue that migration processes could be treated as differential factors, to assist the clinician in disentangling migration processes from PD traits. Migration processes can merely resemble personality pathology, activate (latent) vulnerabilities, or aggravate pre-existing personality pathology. These migration processes include manifestations of grief about the loss of pre-migratory psychosocial and economic resources, and the struggle to regain these in the host culture. Moreover, several cultural dimensions can both resemble or mask personality pathology. These include the dimensions of collectivism–individualism, interdependent self-concept – independent self-concept, traditional gender roles – non-traditional gender roles, emotional expressiveness – emotional inhibition, and supernatural–material. We coined the term “culturally masked PD” to delineate clinical cases in which cultural factors are overused or misused to rationalize behavioral patterns that are consistently inflexible, distressing, or harmful to the individual and/or significant others, lead to significant impairment, and exceed the relevant cultural norms. Furthermore, in the assessment of PDs, particularly (but not exclusively) in Indigenous persons, the inclusion of historical trauma could allow for a broader contextualization of cognitive, emotional, and behavioral patterns, which can be shared by a group who has experienced conquest, colonization, or genocide.
Clinical implications
Although it is beyond the scope of this article to provide an overview of diagnostic instruments, we propose that a semi-structured clinical interview to classify PDs, such as the SCID-5-PD, should include the following diagnostic steps to contextualize personality disorder assessments:
A thorough biographical clinical interview needs to be conducted, including an assessment of early childhood stressors, with specification of the nature, age of onset, severity, and chronicity of these stressors. The earlier and the more severe and chronic the childhood stressor, the greater the potential negative impact (Anda et al., 2006). A mapping of early maladaptive schemas and modes elucidates to what extent these early life stressors have led to maladaptive patterns of thinking, feeling, and behaving (Young et al., 2003). Dimensional approaches to PD classification can furthermore improve diagnostic subtlety in patients who present with subclinical features of PDs that may still be impairing. It is noted that early childhood stressors do not automatically or necessarily lead to the later development of personality pathology, and that the absence of early life stressors does not rule out the development of personality pathology. As Gilmore and Meersand (2014) argue, developmental progression is inherently nonlinear, unpredictable, and complex. Patterns of behavior need to be assessed within the dynamics of family systems, and their own norms, hierarchies, and subsystems. These family systems operate within a larger socio-cultural system, consisting of social, economic, religious, and political elements (Ng, 2003). In this context, protective factors, on the level of the individual, family system, and social support system, also need to be taken into account. The pre-migratory functioning of the patient in the culture of origin and post-migratory functioning in the host culture need to be assessed, on personal, relational, social, and occupational life domains. With regard to migrants who migrated before adolescence / early adulthood, migration processes can manifest in a delayed manner, whereas in migrants who migrated during adolescence / early adulthood, relevant migration processes need to be disentangled from possible PD traits (see Table 1). An assessment of the loss of psychosocial and economic resources needs to be made, in addition to an assessment of what the patient aims to attain on a psychosocial and economic level. Several above-mentioned cultural dimensions need to be weighed, via additional interviews with the patient about his or her dynamic, fluid, and hybrid cultural experiences. Additional interviews with significant others and cultural brokers are necessary to broaden the scope of information. The inclusion of historical trauma could allow for a broader contextualization of cognitive, emotional, and behavioral patterns, to prevent these patterns from being simplified, attributed to a single patient, or stripped from their historical context. Clinicians should critically assess their own stance regarding the five cultural dimensions, and be aware of how attention biases, confirmation biases, and cultural biases could affect the processing of diagnostic data.
Figure 1 depicts the diagnostic considerations that need to be taken into account during the assessment of PDs in migrants and ethnic minorities.
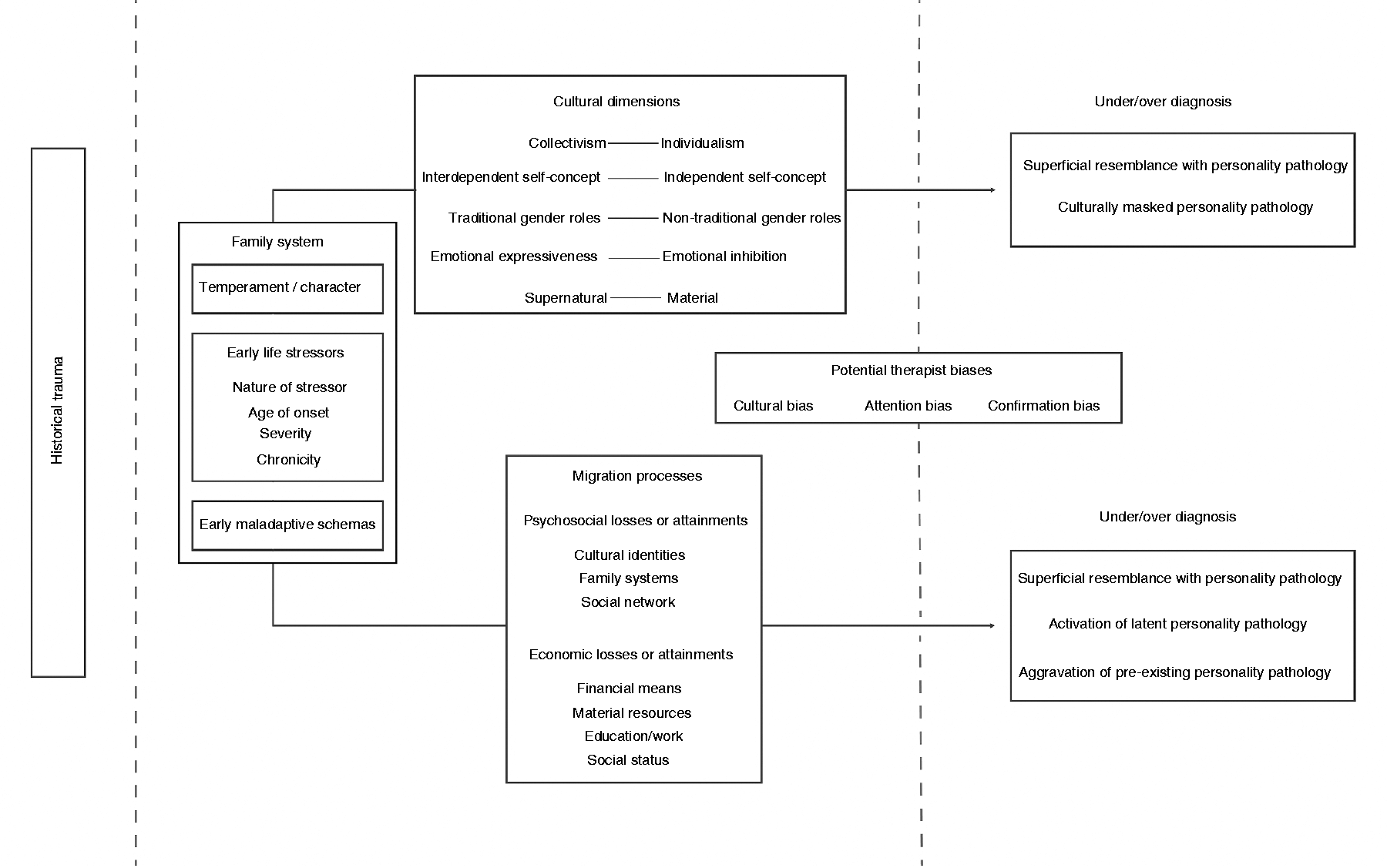
The diagnostic process in the assessment of PDs in migrants and ethnic minorities.
The migration processes and cultural dimensions outlined in this article are not exhaustive, and offer a framework that can be built upon. Future research can map additional migration processes and cultural schemas that overlap with DSM-5 PD criteria. An empirical evaluation of migration- and culture-related approaches to PD assessment can strengthen the biopsychosocial model. In clinical training, a convergence between fields such as medical anthropology and psychiatry, with a specific focus on contemporary migration waves, systemic discrimination, racism, and historical trauma, could broaden the scope of clinical information.
Supplemental Material
sj-pdf-1-tps-10.1177_13634615211036408 - Supplemental material for The role of migration processes and cultural factors in the classification of personality disorders
Supplemental material, sj-pdf-1-tps-10.1177_13634615211036408 for The role of migration processes and cultural factors in the classification of personality disorders by Ardalan Najjarkakhaki and Samrad Ghane in Transcultural Psychiatry
Supplemental Material
sj-pdf-2-tps-10.1177_13634615211036408 - Supplemental material for The role of migration processes and cultural factors in the classification of personality disorders
Supplemental material, sj-pdf-2-tps-10.1177_13634615211036408 for The role of migration processes and cultural factors in the classification of personality disorders by Ardalan Najjarkakhaki and Samrad Ghane in Transcultural Psychiatry
Footnotes
Acknowledgements
The authors thank prof. Dr. J. T. V. M. de Jong for his feedback and support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.