
Abstract
Brua is an Afro-Caribbean religion and healing tradition predominantly practised on the ABC islands of the former Netherlands Antilles. It is grounded in oral tradition and shrouded in strict social taboos. Existing literature suggests that the majority of people on and from the islands are familiar with Brua and that it plays a substantial role in shaping their illness conception and idioms of distress. A lack of knowledge of Brua may therefore lead biomedically trained health professionals to misdiagnose these patients. This article discusses how religious beliefs related to Brua influence the illness concepts and idioms of distress of psychiatric patients originating from the ABC Islands, based on semi-structured interviews with former islanders receiving treatment at a psychiatric institute in the Netherlands. We found that of the 29 interviewees, 93.1% knew what Brua involved, 72.4% believed in it, 48.2% had first-hand experience with Brua practices, and 34.5% attributed their mental illness to Brua with greater or lesser certainty. However, only one patient had previously discussed her belief in Brua with her psychiatrist and only when asked to do so. The role of psychoactive substances in the context of Brua practices was negligible. Thus, the present study indicates that the majority of psychiatric patients from the ABC islands are familiar with Brua, but feel reluctant to discuss their concerns in this area with mental health professionals. Recommendations for clinical practice and further research are provided, including the need for a culture-sensitive approach and integrative care.
Keywords
Introduction
Brua is a local religious and healing tradition practised in Aruba, Bonaire, and Curaçao, also known as the ABC islands of the former Netherlands Antilles. Like other Afro-Caribbean religions, Brua is a syncretism of African religions, Christianity, and the religious beliefs of the Arawak Indians, the Indigenous inhabitants of the islands. As an old oral tradition, written information on its content and practices is limited. The modest existing body of literature on Brua, previously summarized by our group (Blom et al., 2015), and especially the testimonies of patients described therein, led us to conclude that it might play a more prominent role in the illness conception of psychiatric patients stemming from the islands than recognized by health practitioners in the Netherlands.
Moreover, we found indications that botanical hallucinogens and other pharmacological agents—as used in the context of Brua practices—may influence the clinical presentation of these patients. Substances containing neurotropic alkaloids, for example, may evoke visual distortions (i.e., metamorphopsias) and visual, compound, and kinesthetic hallucinations, the latter being characterized by the illusory sensation of moving or flying. According to Rutten (2003), who prepared a compendium of botanical substances traditionally used on the islands, the effects of neurotropic alkaloids may well have inspired, or at least amplified, the stories about levitation and magical flights to Africa (i.e., transvection) told to this day on the islands. In toxic dosages, the same substances are held responsible for causing states of cholinergic delirium.
Based on the findings presented in the literature, as well as our own experiences in clinical practice, we concluded that a lack of knowledge of Brua among biomedically trained health professionals may give rise to communication problems and hence to both the over-treatment and undertreatment of psychiatric disorders. The interpretation of culture-specific idioms as indicative of pathology may be equally likely to occur as the failure to recognize pathological phenomena when expressed in such idioms. Since empirical studies on Brua and its influence on illness conception and idioms of distress are confined to a handful of case reports (e.g., Hoffer, 2009; Jessurun & Raes, 2005; Mensinga, 1994; Minkenberg & Blom, 2015), the present study explored the belief in Brua and its relationship with mental illness in people with roots in the ABC islands. The study was carried out in the Netherlands where many of these patients reside.
Historical and demographic context
As the name suggests, the former Netherlands Antilles and the Netherlands have a common history that dates back to the 1630s when these Caribbean islands were occupied by the Dutch West India Company and subsequently turned into a Dutch colony (Martis, 2018). The islands—most notably Curaçao—soon became notorious as an important port of the transatlantic slave trade (Wallerstein, 1974). Starting with the abolition of slavery in 1863, the islands travelled a long road to their current autonomy (Oostindie, 1998), culminating in the eventual dissolution of the Netherlands Antilles in 2010, with Aruba and Curaçao now having the status of separate countries within the Kingdom of the Netherlands, and Bonaire now being a special municipality.
According to Statistics Netherlands (the Netherlands’ national statistical office), by the end of 2017 a total number of 153,469 first- and second-generation migrants from the former Netherlands Antilles resided in the Netherlands (Centraal Bureau voor de Statistiek, 2017). Although this is only 0.89% of the Dutch population (totalling 17.25 million), it is almost half of the islands’ current inhabitants. Since healthcare facilities on the ABC islands are comparable to non-academic facilities in Western countries and overall very accessible, biomedical thinking is commonplace to people from all ethnic groups and socio-economic strata of the islands’ populations. And yet, prevalent illness conceptions often also deviate markedly from the biomedical model. If we are to give patients on and from the islands proper care, it is essential for health professionals to be aware of their idioms of distress and concepts of disease.
The differences in illness conceptions are at least partly due to the patients’ diverse religious backgrounds. During the colonial era, most of the islands’ inhabitants were converted to Christianity and even today 80% are Roman Catholic (Centraal Bureau voor de Statistiek, 2013). Nonetheless, having been forced to leave their African countries of origin and had been put’ to work as slaves on the islands, had succeeded in preserving many of their religious beliefs and traditions. From the those who had been forced 17th century onwards, the fusion of these African religious elements with Christianity and the beliefs and practices of the Arawaks eventually developed into Brua, the principal non-official religion of the islands (Allen, 2007). At first it was practised exclusively by slaves but later also by other population groups. Prohibited by the Roman Catholic Church from the outset and often publicly frowned upon as “inferior” and “evil,” Brua has remained an underground religion up to the present day, with practices taking place in locations well hidden from the public eye but still attended by individuals from all social, ethnic, and economic strata. Brua is seldom openly discussed, especially in the presence of outsiders, including Western, biomedically trained health professionals (Streefkerk, 1977). Based on the literature and our own clinical experience, we know that many patients from the ABC islands are reluctant to speak about Brua or may simply deny that they have ever heard of it, making it difficult for health professionals to explore the extent of their beliefs and their influence on their conceptions of health and disease.
What is Brua?
Brua is a monotheistic religion chiefly practised in the southern part of the former Netherlands Antilles. Although it is often compared with other Afro-Caribbean religions such as Vodou, Santería, and Obeah (the latter being practised in the northern part of the former Netherlands Antilles), it has its own set of religious beliefs, magical practices, and healing traditions, which may, however, vary considerably among different subgroups and individuals (Blom et al., 2015). At its centre is the belief in the Christian God (called papa Dios in Papiamento, the islanders’ vernacular language), but prayers may also be directed at Catholic saints, whom many Brua adherents equate with African gods and spirits. Individuals may even address the almasola, the ‘servant of the devil’ or ‘the devil himself’ who allegedly resides in the ocean surrounding the islands, from whence he can strike out at anyone. Many adherents of Brua consequently do not only believe in biological and psychological causes of disease but also in spiritual causes, claiming that saints, spirits, and, notably, the almasola are important promoters of health and/or disease (Allen, 1989; Hoffer, 2012). Although most see biomedically trained professionals for their health issues, (former) islanders may prefer Brua practices for the treatment of health problems they consider either too simple or too complex for biomedicine (Blom et al., 2015). The same holds for ‘mysterious’ cases, where they suspect magic or sorcery to be implicated. Here, individuals may resort to countermeasures involving the use of amulets, herbs, cigars, poisons, and numerous other practices and rituals. When such measures are taken pre-emptively, they are referred to as furá or ‘armouring’ (Brenneker, 1966). Brua experts, referred to as hasidó di brua (‘brua practitioner’), kurioso, or kurado (‘traditional healer’), are specialized in the use of furá but also in natural as well as supernatural remedies to treat somatic and psychiatric diseases. A subgroup specializes in sorcery for destructive purposes such as eliminating a person suspected of doing harm.
Since stories about Brua and its alleged destructive effects are rife among people from the ABC islands, many of them may fear that they have fallen victim to supernatural powers whenever they become ill. This suspicion may accordingly also shape their idioms of distress (Jessurun & Raes, 2005). To explore this assumption empirically and in conformity with the tradition of clinical ethnography, our study presents qualitative and quantitative data on the influence of religious beliefs in Brua on the subjective experience of mental illness among psychiatric patients originating from the ABC islands who are receiving treatment in the Netherlands. We will use these insights to formulate recommendations for clinical practice and further research.
Methods
For the purpose of the present study, we conducted semi-structured interviews with patients recruited at Parnassia Psychiatric Institute, located in The Hague. The study was carried out from August 2017 to July 2018. Inclusion criteria were i) age ≥18 years; ii) having been born (or having at least one parent born) on Aruba, Bonaire, or Curaçao; and iii) being diagnosed with one or more mental disorders as classified in the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; APA, 2013). Potential candidates were identified via Parnassia’s electronic patient records, after which their treating physician was contacted to inquire whether they deemed the patients suitable and sufficiently mentally stable to take part in the survey.
All participants were interviewed by a junior physician under the supervision of a clinical psychiatrist. The interviews lasted 30–75 minutes and were conducted at the hospital, at the hospital’s outpatient clinic, or in the patient’s home—whichever was deemed most convenient to the participant. One patient was interviewed via telephone because she did not want to run the risk of being recognized by the researcher if she met her in person. The semi-structured interview was designed specifically by our group for this study (Appendix A). To maximize its cultural validity, we addressed the most salient—and often highly specific—themes that we had catalogued in our review of the literature (Blom et al., 2015). Apart from a section on demographics and other baseline characteristics, the questionnaire therefore comprised 18 questions inquiring into knowledge of Brua, belief in Brua, experience with Brua, personal ideas about relations between Brua and disease, personal experience with traditional and biomedical therapeutic interventions, protection against Brua, fear of Brua, and the influence of knowledge about Brua on the therapeutic relationship. Notes made during the interviews were analysed using thematic content analysis (TCA; Braun & Clarke, 2006). Some of the responses were converted to categorical data and analysed using SPSS version 23.0 to calculate prevalence rates.
The research protocol was submitted for approval to the Medical Ethics Committee of Leiden University Medical Centre, who judged that the study required no formal approval or written informed consent, as obtaining oral consent was judged to be satisfactory by the Committee (registration no. P18.062). Accordingly, eligible patients were provided with both oral and written information, after which oral consent was obtained from all participants prior to their participation.
Results
Demographics
On 1 April 2018, Parnassia Psychiatric Institute had a total of 77,775 registered patients, of whom 1,229 (1.6%) originated from the former Netherlands Antilles. During the time of our study, we received feedback on the suitability and mental stability of 101 patients (8.2%). Of these, 37 were judged unsuitable to take part in the survey, due to either mental instability or an expected adverse reaction to being interviewed on this topic, while eight were no longer registered as patients. Additionally, 11 patients could not be reached, and 14 others did not wish to participate. Two patients were excluded during the interview: one because he was deemed mentally unstable and the other because of undue distress. We were thus able to include 29 patients (2.4%; see the flowchart in Figure 1), of whom 14 were female (48%). The participants’ mean age was 50 years, with a range of 22–75 years, and 72.4% were born on Curaçao. All but one participant were first-generation migrants to the Netherlands. Two participants came to the Netherlands as toddlers, the remaining ones as young adults. The most frequent diagnosis was schizophrenia spectrum disorder (58.6%), followed by unipolar or bipolar mood disorder (27.6%), post-traumatic stress disorder (6.9%), and attention-deficit/hyperactivity disorder (6.9%). In addition, almost half of the patients were diagnosed with a comorbid psychiatric or substance-use disorder, with a range of 1–3 per patient (Table 1). The TCA yielded six central themes, which will be discussed below.
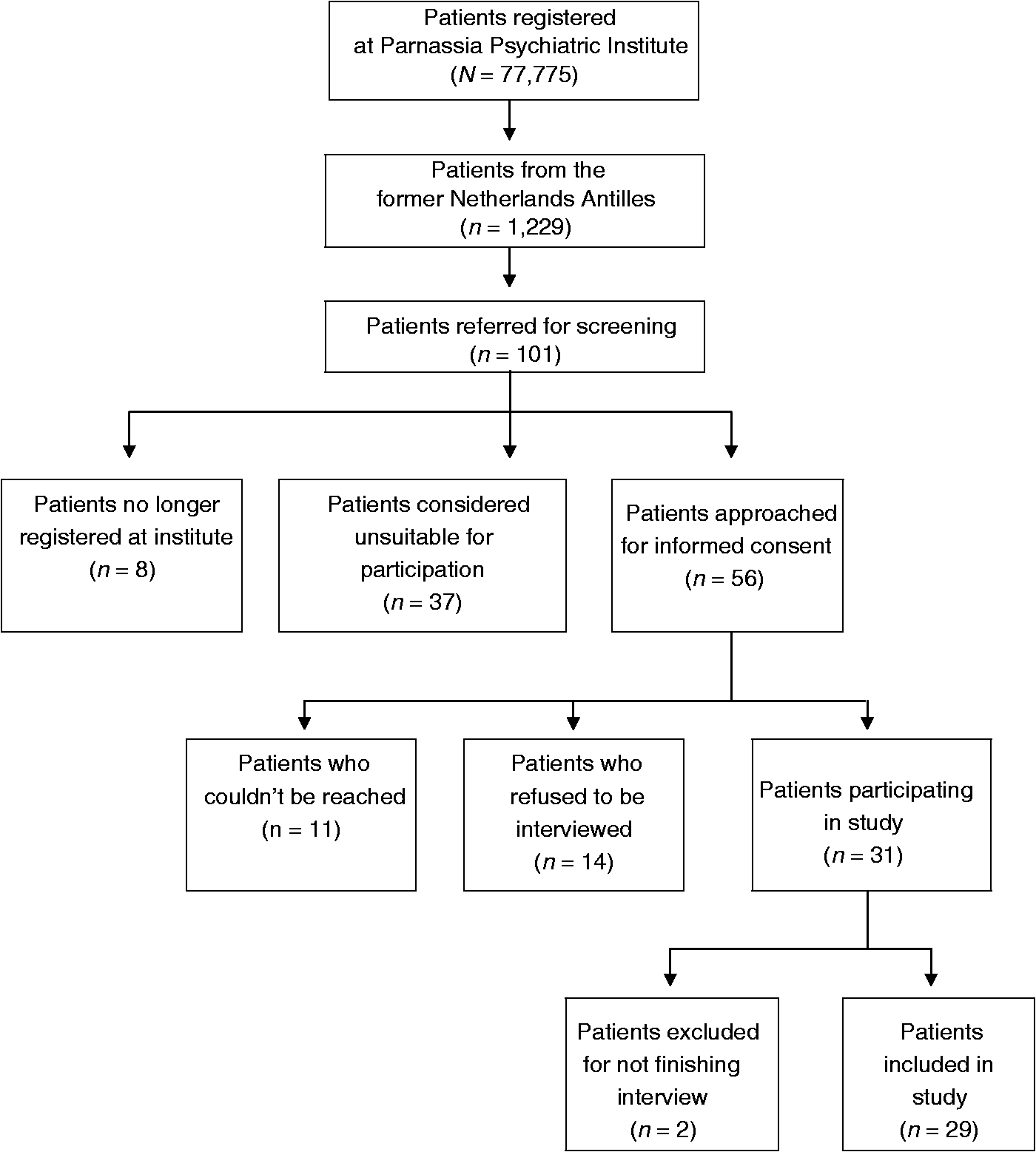
Flowchart of participant recruitment.
Demographic and clinical characteristics of study participants (N = 29).
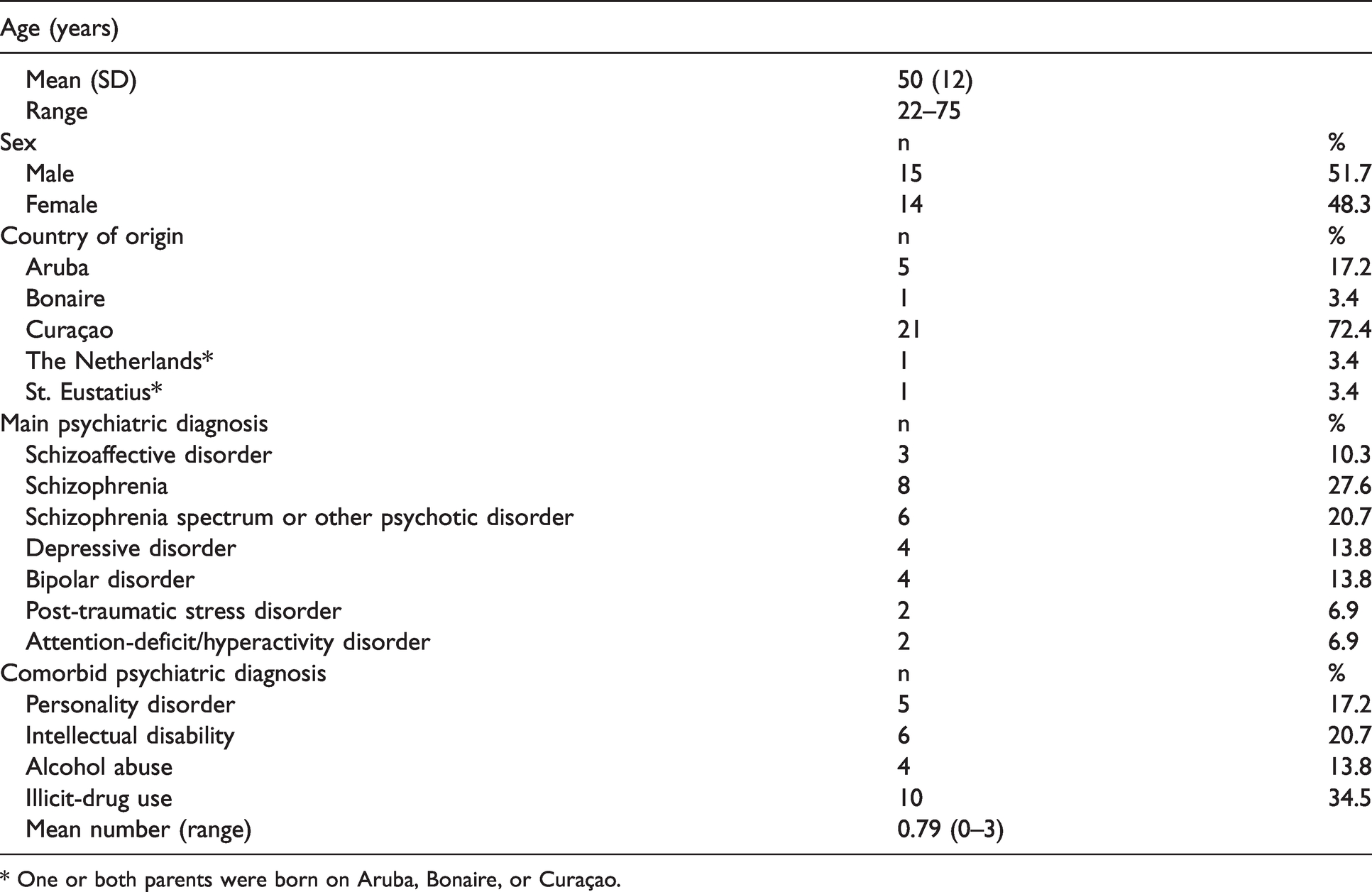
* One or both parents were born on Aruba, Bonaire, or Curaçao.
Religiosity
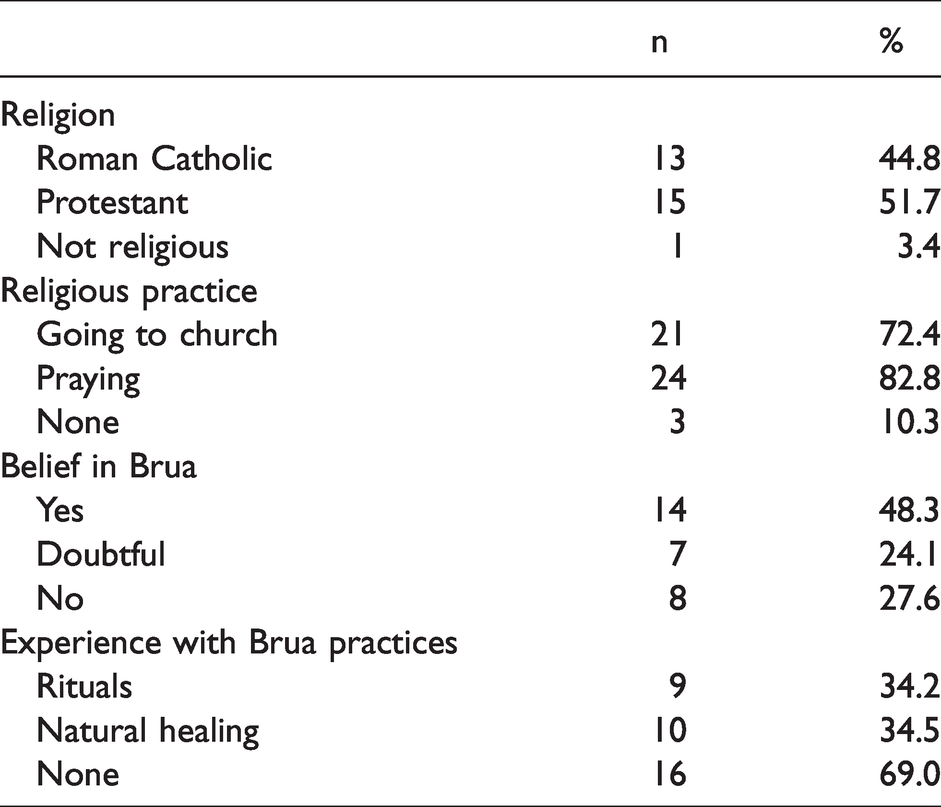
All participants had been raised Christian, while 89.7% considered their Christian faith of ongoing significance in their daily lives (Table 2), with 82.8% saying daily prayers, 72.4% going to church on a regular basis, and 86.2% acknowledging that God played an important role in their health. Explanations of this role varied from a general “God provides me with strength and inner peace,” to more specific convictions such as “Nothing happens without God’s will, and even doctors can only cure with His permission.” Home visits and visits to patients’ quarters on the ward showed evidence of their ongoing commitment to Christianity, with rooms often being decorated with religious imagery and a Bible lying within easy reach. Some patients would even assess their own mental state by asking themselves whether they were able to go to church or not. All but two participants (93.1%) confirmed that they knew about Brua and 72.4% that they believed in it, often expressed in a matter-of-fact tone of voice. As one of the participants said, “It’s just there, everybody knows it’s there.” Despite many participants regarding Brua as a local form of Vodou, many also linked it to Christianity, saying “It exists, because the Bible says so.” Another participant explained that in order for good to exist, there should also be something like Brua, because “good and evil go hand in hand, creating a balance.” The latter statement also reflects what some participants considered to be true of Brua: that it is mainly a vehicle for doing evil. As one of them offered, “Brua is a collection of occult practices of people who are playing with darkness,” and another, “It is the wish to make ugly things happen to others.” Participants who did not believe in Brua gave different clarifications, saying, “You don’t want to be associated with Brua,” and, “If you start believing in Brua, you will go crazy.” Others conceived of Brua as “a culture-bound superstition,” calling it “total nonsense,” while adding that it “may still have value for the sake of culture.”
Religious characteristics (N = 29).
Experience with Brua practices
Although the subject of Brua and its practices is notoriously taboo among individuals from the ABC islands, 65.5% of the interviewees were willing to share stories about it, nine of them recounting personal experiences, three sharing stories they had heard from family members/close acquaintances, and seven recounting other peoples’ experiences, which were told without disclosing their sources. The practices described ranged from fortune-telling with a deck of cards or cigarette ashes to cleansing rituals and other procedures often involving the use of candles or incense, and sometimes use of chicken feathers or blood. In some cases, the assumption that Brua had been at play seemed to rest on rather vague, intuitive notions, with one participant divulging that her ex-partner had had “hairs in the walls of his home,” without, however, being able to explain how she had found out or how this indicated Brua was at play in her life. Still, she had felt forced to flee from Curaçao and had not dared to return for over 15 years. What may have played a role in her reluctance to return is that she was pregnant with the man’s daughter, who she wished to keep safe. Another participant recounted that, having sought the help of a kurioso to learn about the future, he had been instructed to hold up a chicken egg in front of the sun to allow the kurioso to talk with it, who then proceeded to break the egg, telling the participant that the future would reveal itself within seven days (although the participant could not tell us how that had worked out). Yet another participant related how he had once safely passed through the border control of two international airports with certain unnamed substances in his possession after engaging in a preparatory Brua ritual that had involved a thorough body cleansing, dressing up in a brand new set of designer clothes, and the induction of a trance state, all intended for protection and good fortune. It was the participant’s conviction that this had prevented him from being caught smuggling said substances.
Throughout the interviews, a recurring theme was the act of “using Brua on someone,” for example by placing an artefact made of mud and leaves or chicken bones in front of someone’s door. In a similar vein, one participant related how she had once received an old silver two-and-a-half-guilder coin from her father’s new spouse, upon which her mother and her new-born son had died in close succession. This had been proof for her that, through the coin, a “Brua spell had been put on her.” Another participant confided to us that she had grown up in a family of witches and had wielded Brua practices herself in the past, claiming to have been gifted with the “cursed mouth,” which entailed that, when in an intoxicated state, she would speak out words that were “revealed” to her, which allegedly resulted in particular adverse events she described. After she had fallen mentally ill, she claimed she had realized that these practices were not without danger, which was why she had since renounced them. Another participant described how members from her family had gone to the cemetery the night after her grandmother had been buried and had turned the tombstone upside down as part of a Brua curse because they did not want her spirit to find peace. Yet another participant told us about an elaborate ritual that she and her seven-year-old daughter had undergone to get rid of the Brua spell that had purportedly been put on the two of them by her own mother. The participant had deduced this from her own physical weakness and the allegedly jealous behaviour of her mother. She had been told by the kurioso that her daughter would have to die symbolically in order to be “reborn” and no longer be under the spell, after which the little girl had been placed inside a coffin surrounded by flowers and candles. The mother paid over US$4,000 for the ritual to be performed, amounting to four to five months’ pay for someone earning the minimum wage on the islands.
Brua and mental illness
When asked whether Brua could be the cause of their mental illness, four participants (13.8%) were certain it was, while six (20.7%) considered it possible. A female patient recounted that her mother had allegedly grown so jealous of her marriage that she had taken the patient’s wedding ring to a kurioso, forcing her to get it back herself and thus providing the kurioso with an opportunity to “put a Brua spell on her” that had eventually led to her ending up in our psychiatric hospital. Other participants had more general explanations and “just knew that some person had wielded Brua on them,” mostly in connection with interpersonal conflicts or jealousy. Providing a detailed view, another participant claimed her mental illness had not been caused by Brua itself but that her current psychotic episode had been brought about by three people who had “used Brua to harm her.” All the participants who were convinced that their mental illness was caused by Brua gave descriptions of personal feuds that had culminated in their current health situation. In addition to the patient whose mother had been jealous of her marriage or the one who had received the bewitched coin from her father’s new wife, another participant told us that her mother had been a jealous witch who always wielded Brua practices to control her, “sucking all the luck and fortune out of her life.” She had never seen her mother perform any rituals, but after reading a book that said “to control someone is witchcraft,” she knew that her mother had caused her illness by using Brua.
Fear and protection
Although many participants characterized Brua as a means to bring about disease and—in a general sense—misfortune, only 27.6% admitted to being afraid of it. One patient in this percentage noted, “It is simply frightening, because everything about Brua is so dark.” Tellingly, one of the participants who had claimed not to be afraid said, “I cannot be afraid of Brua, because if I do, it will get me,” indicating that it was still something to be reckoned with. Another participant held onto his mother’s distinctive opinion that “One doesn’t need to be afraid of Brua but rather of the people practising it.” A recurring explanation for the lack of fear of Brua was the strength and protection God provides. Those who stated to be unafraid had also claimed they did not believe in Brua. Remarkably, with 37.9%, the number of participants who used some form of protection against Brua was larger than in this group the group that had confided to be afraid of it (27.6%). This may indicate that, in some instances, the use of protective devices helped to minimize the fear of Brua, or that some individuals were afraid after all without admitting it. Of the group that had admitted to fear Brua, 25% took recourse to protective objects, which mainly consisted of Christian artefacts such as rosaries, candles, and prayer cards, but sometimes also horseshoes, aloe plants, and strong-smelling products such as cigarettes, cigars, garlic, and coffee. One of the participants explained that you can also carry with you the black-red bean of the Abrus precatorius (also called rosary pea) as it is believed to burst open when something bad is about to happen. None of the participants admitted to being involved in sorcery to ward off evil.
Brua healing practices
When asked about Brua healing practices, 48.2% of the participants indicated that they had actively practised some, which mostly involved the use of herbs like oregano, aloe, chamomile, yerba bueno, morenga, or basora pretu. One participant told that she was in the habit of giving advice about herbal teas and aloe to purify the inner body. Another explained how she had been involved in a cleansing ritual after her first menses, during which she was made to stand on three big round stones by her aunt, who kept circling her, sprinkling water and saying prayers. Yet another participant recounted how he had had to wash himself with a mixture of yerba di hole and cane, which he had to keep on his head for three days. In all, 10 participants (34.5%) admitted to using natural healing methods in addition to the medication prescribed by their psychiatrist, but, as none of them considered these a substitute, none would consider refusing to take the prescribed medication. When asked if they would consider going to a kurioso or kuradó for treatment, only two of the participants (6.9%) said they would, albeit in addition to consulting a physician.
Talking about Brua
All participants showed themselves reluctant to talk about Brua with their treating health professional(s) and many of them doubted whether it would be useful or necessary. A majority (69.0%) added that they would only consider discussing the topic if the attending professional had the same cultural background as the patient or was at least well-informed about Brua. As one of the participants explained: “Some people move to music by learning the steps and counting, whereas others really feel the music,” thus indicating her opinion that a merely theoretical knowledge of Brua would not suffice. Another participant offered: “Brua is about being on the ‘good’ side of the scale and you have to be knowledgeable of these scales to understand.” Only one patient had spoken about Brua with her treating psychiatrist in the past and this occurred only after she was explicitly asked about it.
Discussion
To gain an impression of the role Brua plays in shaping the idioms of distress and the illness conception of psychiatric patients originating from the ABC islands, we interviewed 2.4% of the Dutch-Antillean patients receiving treatment at Parnassia Psychiatric Institute in The Hague. All 29 interviewees had been diagnosed by their treating health professional with one or more mental disorders as defined in the DSM-5 (APA, 2013). Of the patients interviewed, 93.1% knew what Brua involved, 72.4% believed in it, 48.2% had first-person experience with Brua practices, and 13.8% were certain that Brua had caused their mental illness, while another 20.7% considered it a possibility. Only one patient had discussed her belief in Brua with her psychiatrist and only when invited to do so.
Belief in Brua and the biomedical approach
Thus, even though all but one patient had not previously shared this information with their treating health professionals, Brua played a substantial role in the majority of participants’ lives. The high level of familiarity with Brua is in line with the findings reported by Hoffer (2012), who estimated that some 80% of the population from the ABC islands are at least to some extent involved with Brua, and Méance (2014), who estimated a similar number for the belief in Vodou in nearby Haiti. The numerous references to magic, sorcery, and protective measures indicated that this involvement shaped the idioms of distress of the majority of participants, and hence also the way individuals conceived of mental illness. Since all participants also acknowledged the necessity to adhere to treatments as prescribed by their health professional, we suggest that the belief in Brua can allow for a broader and perhaps even richer conceptualization of illness and disease, i.e., as a disequilibrium of physical, mental, social, and spiritual elements rather than as a “disease of the brain or mind.” The finding that only one of the 29 interviewees had shared her thoughts about Brua with her psychiatrist fits in with our group’s earlier observations on the reluctance of former islanders to discuss this subject with outsiders (Blom et al., 2015). Although we lacked insight into the participants’ pathways to care, their ending up at our institution at least indicates that their belief in traditional Brua practices did not negatively affect their help-seeking behaviour and trust in Western-based biomedical care. Since 93% of the participants spent their formative years on the ABC islands, we argue that exposure to Brua beliefs and practices during critical years does not seem to diminish faith in biomedical models of disease. This can be seen as tentative support for our previous findings (Blom et al., 2015) and those of Khoury et al. (2012), documented in the study they conducted on Haiti. Based on the results obtained from semi-structured interviews with 31 religious leaders, community leaders, traditional healers, and biomedical health providers, 10 focus group discussions, and four in-depth case studies of psychiatric patients, the authors concluded that the widespread belief in Vodou was, in and of itself, not a primary barrier for most Haitians to seek biomedical care but that its interventions were not always considered effective for the treatment of mental disorders, while many could not afford such help (Khoury et al., 2012). This is strikingly at odds with Rosario and de la Rosa (2013) who, analysing the extant literature on the use of Santería practices by Latino cancer patients in the US, concluded that those in need of mental health services in addition to their cancer treatment often took recourse to Santería rather than to Western biomedical care services. Principal reasons they outlined for this included the perceived incompatibility of Latino and Western illness and treatment needs, and the insufficiency of Western mental health services to adequately incorporate foundational cultural values. Why these Latino cancer patients are so much more inclined to embrace traditional healing systems for their mental health issues than Haitian and Dutch-Antillean psychiatric patients remains unexplained. Possibly, Rosario and de la Rosa’s findings are due to a selection bias in that our study and Khoury et al.’s study focused on mental health patients who had chosen to make use of Western biomedical care services, whereas the Latino cancer patients in the US had opted to seek help outside this context. For a definitive explanation of the disparity, further study is required.
Christianity
With almost all (89.7%) of the patients interviewed reporting that they were still actively involved with their religion, our results also underline the importance of Christianity in the lives of the patients we interviewed, all of whom were raised Christian. These findings are consistent with statistical data showing that 79.4% of the inhabitants of the ABC islands are a member of a Christian church (Centraal Bureau voor de Statistiek, 2015). This number is high in comparison to the native Dutch, of whom 49.9% report commitment to a religious movement and 39% to a Christian church. Since Brua is in no small part founded on Christian values and beliefs—even though it is generally characterized as being ‘unchristian’ in nature—we were not surprised about the many cross-references we noted in terms of spirits being equated to entities described in the Bible. As one of the interviewees explained, “In the Bible, there’s the Father, the Son, and the Holy Spirit. Now, if there is one spirit, why wouldn’t there be more?” Perhaps this is best understood from the vantage point of Brua as a syncretism, in which different religions are merged, parts of which (i.e., the Christian belief system) may remain instantly recognizable.
Crab antics
Jealousy, too, was a recurring theme in the discourse of many of the participants, especially in those who attributed their psychiatric illness to Brua. Individuals would often recount how conflicts with a family member, acquaintance, business partner, or former lover had led up to their current situation, with jealousy being the common thread. When such conflicts were followed by signs of illness or other misfortune, they were often attributed to the oyada or evil eye, the best-known metaphor for jealousy in the world (Berger, 2012). And yet, the same held true when either party experienced an unexpected success. Wilson (1973) described the ensuing envious reactions, known as “crab mentality,” “crabs in the bucket,” or “crab antics,” as follows: Crab antics is behavior that resembles that of a number of crabs who, having been placed in a barrel, all try to climb out. But as one nears the top, the one below pulls him down in his effort to climb. Only a particularly strong crab ever climbs out—the rest, in the long run, remain in the same place. (p. 58)
Culture-sensitive diagnosis
From a biomedical point of view, it may be tempting to interpret these convictions as paranoid delusions, but that would not do justice to the cultural background and the personal beliefs of many of the people from the ABC islands, nor to the fact that jealousy, in any society, may spark a cascade of beliefs and behaviours akin to the crab antics as described by Wilson (1995). In clinical practice, it is crucial to establish the point at which a healthy dose of paranoia has evolved into a paranoid delusion. As with any religious system—or any world view—an overly strong commitment to Brua, be it positive or negative, may elicit delusions and other psychopathological symptoms, for example when ordinary setbacks in life are attributed to Brua. Yet, distinguishing between what is and what is not culturally accepted can be difficult, especially for health professionals unfamiliar with Brua. Here, consultation with a biomedical expert specialized in the topic and/or a kurioso may be warranted, while, if the patient so wishes, a dual-track approach including both biomedical and traditional care may be considered (Blom et al., 2013). A factor that complicates the diagnostic process is that the operationalization of Brua beliefs and practices tends to differ from person to person, sometimes preventing experts from suggesting viable treatment options. To assess what is culturally sanctioned may be challenging in any situation but even more so in the context of oral traditions such as Brua where written canonical touchstones are lacking. Promisingly, with phenomena such as the evil eye and crab antics also being found in other cultures, albeit expressed in different idioms of distress, certain aspects of what used to be called “culture-bound syndromes” are increasingly being recognized as being less exotic and alien than assumed (Ventriglio et al., 2016), potentially fostering accurate diagnoses and effective treatments for patients from different cultural backgrounds.
Implications for clinical practice
Our findings offer several opportunities to improve diagnosis and treatment in patients from the ABC islands, notably by improving the therapeutic relationship. In clinical practice, culturally oriented interviews have the potential to improve the diagnosis and thus the treatment plan through which adherence, effectiveness, and patient satisfaction can be augmented (Lewis-Fernández et al., 2015). Moreover, patient engagement can be boosted by means of patient-specific clinical negotiations and reciprocity in clinician–patient perspectives. In the light of these observations and the findings presented above, when dealing with psychiatric patients originating from the ABC islands we recommend mental health professionals to primarily adhere to the current guidelines for diagnosis and treatment as based on the biomedical model. It is a model that many of these patients are well acquainted with and apparently also prefer—except, as noted, when problems are considered too trivial (e.g., love sickness) or too complex for biomedical consultation (e.g., terminal lung cancer or chronic schizophrenia; Blom et al., 2015). In our survey, none of the participants disagreed with the diagnosis or the treatment regimen offered by their treating health professionals. A minority even mentioned the Dutch healthcare system as the principal reason for migrating to the Netherlands. In addition to biomedical interventions, we advise to adopt a culture-sensitive approach, for which we propose the Cultural Formulation Interview (APA, 2013) or a topical, tailored questionnaire such as the one we developed for our specific population (Appendix A). As observed, the fear of Brua may form a powerful obstacle in the patient–physician relationship and impose limits on what patients are willing to share. Shame is another closely related obstacle. As many of the interviewees reported, they often looked back with embarrassment at the things they used to believe and the practices they used to keep. Two patients even became so agitated while being questioned about their prior involvement with Brua that they refused to discuss the topic any further. The other 29 interviewees, by contrast, showed themselves appreciative of the opportunity to discuss their ideas about Brua and explore its role in in their illness conception and their idioms of distress. None of the participants in our study reported using or having used psychotropic substances in the context of Brua practices, described as having a potentially grave influence on the clinical presentation (Brenneker, 1966; Rutten, 2003). This may seem at odds with the relatively high prevalence of comorbid alcohol abuse (13.8%) and use of illicit substances (34.5%) that we recorded. Taken at face value, it might indicate a certain reluctance to use substances in the context of Brua rituals but not in a recreational context. However, it might also indicate a certain disinclination to discuss this aspect with health professionals, however much they could be trusted with other sensitive issues. A final recommendation we would like to make is that, besides providing state-of-the-art treatment, health professionals should allow their patients to seek out alternative therapies so long as engaging in these practices does not interfere with the prescribed medication or give rise to new pathology. This could be as simple as providing inpatients with the opportunity to go to church or permitting the use of certain herbs or cleansing rituals. In a broader sense, an integrated care management system may be warranted, an approach aimed at expanding the exclusive focus on biomedical diagnoses and treatments by also paying attention to the disruption of psychiatric disorders to individual lives, using more holistic approaches, such as narrative methods, offering strategies to learn to cope with disability, and promoting inclusion (Dean et al., 2019).
Limitations
Our study has several limitations. First, the sample size is relatively small. Although our findings are clear that most patients were familiar with Brua and had prior involvement with Brua practices, further research with a larger sample is needed. Secondly, since the focus of our study was on psychiatric patients residing in the Netherlands, generalizibility to psychiatric patients or the general population in Aruba, Bonaire, or Curaçao is uncertain. After all, those in the Netherlands are more likely to assimilate (even more) to Dutch cultural and scientific values than those still residing on the islands. Moreover, we do not know whether and to what extent Brua practices may have been modified following their migration to the Netherlands; this is a topic that also needs further study. A third limitation has to do with our decision to take notes during the interviews rather than audio record them. This may have led to loss of valuable information. However, some participants may have been less willing to share personal stories with us in the knowledge that these would be recorded. Furthermore, we were unable to gain insight into the temporal course of individuals’ mental health problems and their use of biomedical and traditional interventions. Finally, the study did not allow us to comprehensively explore the association between Brua-related beliefs and different psychiatric disorders, and the way in which beliefs impacted the participants’ understanding of mental illness, which are both aspects worthy of further study in a larger population sample.
Conclusion
In this article, we seek to add to the burgeoning literature on global mental health by charting the way in which the idioms of distress and illness conception of psychiatric patients from Aruba, Bonaire, and Curaçao are shaped by their belief in Brua. Although relatively small, our survey of 29 mental health patients originating from the ABC islands is the largest of its kind to date. Based on our findings, we conclude that Hoffer (2012) was right in pointing out the reluctance of former islanders to discuss their involvement with Brua with Western mental health professionals and in assuming that it nonetheless plays an important role in the lives of most. The great majority of our patients were familiar with Brua and its practices, half had first-hand experiences, and a third tentatively attributed their mental illness to it. To optimize diagnoses and treatment for this specific population, we hence advise health professionals to inform themselves on Brua and use this knowledge to adopt a culture-sensitive approach. Despite a general fear of its influence and its taboo status, all but two of the interviewees expressed their appreciation for the opportunity to discuss their involvement with Brua. Opinions were divided as to whether the cultural background and topical knowledge of the treating health professional were of relevance. Above all, an open attitude and a respectful, culture-sensitive approach appeared to be essential. We found little evidence for the oft-reported ritualistic use of psychoactive substances or any influence on the patients’ clinical presentation. It would be interesting to clarify whether former islanders have benefited from Brua practices and to chart which particular methods have worked. The fact that many people continue to practice Brua suggests that its holistic worldview may have advantages that the biopsychosocial model of present-day biomedicine does not offer. Since all participants had already found their way to Western biomedical care and none reported having experienced any significant tension between the two approaches, it remains uncertain whether adherence to Brua forms an obstacle to seeking biomedical help.
Footnotes
Acknowledgments
We would like to thank the participating patients of Parnassia Psychiatric Institute for their generous contributions to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.