
Abstract
Suicide is a public health issue that impacts a nation’s resident and non-resident populations alike. Singapore has one of the largest non-resident (work permit holder) populations in the world, yet very little attention has been given to examining suicide in this population. The current study examined the case materials of all 303 non-resident completed suicides in Singapore in the period January 2011 to December 2014. Their basic profiles were compared with that of the 1,507 resident cases in the same period. A sample of 30 death notes written by non-residents were randomly selected and thematically analyzed to supplement the descriptive findings and discussion. Results showed that suicides were highest among males, those aged 21–35 years old, and South Asians. Most non-resident suicide cases did not have known physical or mental health issues, prior suicide attempts, or suicide notes. Suicide decedents from South Asia and Europe most frequently used hanging, while jumping was most common among decedents from other regions. Relationship and health problems emerged as the top two suspected triggers for suicide based on our analysis of the suicide notes. The unique situation of working abroad may increase non-residents’ vulnerability in general, while adverse life events such as relationship and health issues may be too overwhelming to bear, especially when support services are not readily available and accessible. The results have implications for suicide prevention among this neglected group of people who choose to work in foreign lands.
Introduction
Suicide is a serious global public health concern. The World Health Organization (WHO, 2017a) estimates that suicide accounted for 1.4% of deaths globally in 2016. Further, 56% of global deaths by suicide occurred in South East Asia and West Pacific Region (WHO, 2019). Yet epidemiologic reviews of suicide research in Asia have been limited by the absence of suicide research in some countries and lack of validity in extant studies (Ahmed et al., 2017; Chen et al., 2012). Hjelmeland’s (2016) critique of contemporary suicide research also pointed to the paucity of studies on suicide in Asia. In fact, less than five percent of the published literature on suicide concerns Asian populations.
Asia is also the site of massive work-related migration, with the largest non-resident population and the largest gain in the number of non-residents between 1999 and 2017 (United Nations, 2017). The same United Nations (UN) report showed that the non-resident population in Singapore has similarly burgeoned, ranking among the countries with the fastest growth in the proportion of non-residents in the total population.
In Singapore, approximately two percent of all deaths in 2015 were suicides (Immigration and Checkpoints Authority, 2016), while the crude suicide rate was 9.9 per 100,000 (WHO, 2017b). While Singapore’s suicide rate was much lower than several other Asian countries, including Japan, the crude suicide rate surpassed that of neighboring countries like Malaysia (5.8), Vietnam (7.4), and the Philippines (3.4) (WHO, 2017b). Despite this comparatively high suicide rate, there have been few studies of suicide in Singapore and most research focuses on identifying patterns in suicide behavior in the resident population (e.g., Chia et al., 2011; Mak et al., 2015). There have been no published studies on suicide behavior among non-residents, despite their significant presence in the population and corresponding economic contribution to Singapore.
Non-residents and suicides
A review of current literature points to higher suicide risk and suicide rates for non-residents or guest workers as compared to residents in Europe (Lipsicas et al., 2012; Spallek et al., 2014) and globally (Forte et al., 2018). While there is a body of literature comparing suicidal behavior between non-resident and native populations in European countries, there is little or no similar research in Asian countries. Current research has found no conclusive causal factor for elevated suicide risk among non-residents compared to the general population or to the resident suicide rate of their native countries in Europe, although young females from South Asia have been highlighted as a group with higher suicide risk (Spallek et al., 2014; Forte et al., 2018). However, the research suggests that acculturative issues and socio-economic disadvantage were the main causal factors for suicide in non-residents countries (Forte et al., 2018; Spallek et al., 2014; Vazsonyi et al., 2017).
A review of epidemiological research in the Asian context by Chen and colleagues (2012) revealed that, due to cultural differences, findings from studies in Western contexts cannot be generalized to Asia. Available studies suggest that while mental disorders are a major risk factor for suicide in the West, psychosocial factors (e.g., shame and isolation due to family problems or retrenchment) linked to the unique cultures in Asia contribute most to suicides in the region (Snowdon, 2018; Snowdon et al., 2018). There are multiple potential explanations, but the prevalent stigma and attribution of mental illness to personal or spiritual factors in Asia (Ito et al., 2012), together with the concept of shame that is ingrained in various Asian cultures (Abeyasekera & Marecek, 2019; Hagaman et al., 2018; Kageyama, 2012), may lead individuals to believe that there is no way out of their predicament but to take their own lives.
Contextual considerations
The non-resident population can be categorized based on the visas granted by the Singapore government. Those with higher income or profession are granted Employment Passes and are referred to as ‘foreign talent’ by the government (Teo & Piper, 2009) and receive preferential treatment both at the policy and societal level (Yeoh, 2006). ‘Skilled or semi-skilled’ workers, otherwise known as ‘foreign workers’ to Singaporeans, need their employers or employment agents to apply for work permits. These foreign workers are hindered from integrating into Singapore society by both labor immigration policies (Yeoh, 2006) and negative stereotypes in society that discourage integration (Tan, 2014).
While non-residents’ issues span all areas of life, a number of studies in Singapore have placed a strong focus on blue-collar workers, and acculturation and employment concerns (Chib et al., 2013; Lee et al., 2014). ‘Foreign workers’ who have less agency than ‘foreign talents’ commonly face issues like language barriers, loneliness, and unlawful wage deprivation and other employer abuses (Chok & Ng, 2017; Wong, 2010; Yeoh & Huang, 2007, 2010). In 2011, Chia and colleagues studied the Singapore Coroner’s register-based suicides in the period 2000–2004. Since that time, the non-resident population in Singapore has increased significantly, from 17% of the total population in 2004, to 29% as revealed by the latest Census (Singapore Department of Statistics, 2018). Between 2011 and 2014, approximately 17% of all deaths determined to be suicides were by non-residents. In 2014–2016, the suicide rate was 3.25 per 100,000 work-permit holders yearly, or 32 suicides per year on average (Ministry of Manpower, 2017b). In comparison, the non-resident population in Europe, which is the second largest after that in Asia, accounted for 10.5% of the total population (UN, 2017). A review of suicide studies in Europe showed a range in the suicide rates of immigrants relative to that of the general population, between 1.59% and 26.19% (Spallek et al., 2014).
Conceptual relevance for non-residents
Suicide behavior is conventionally construed at both the intra-personal and interpersonal level. Mental health problems (Appleby et al., 1999; Caldwell et al., 2004; Luoma et al., 2002), stress and diminished self-efficacy (Chan, 2002), and coping (Cole, 1989; Spirito et al., 1989; Wilson et al., 1995) are examples of intrapersonal factors that call for attention. Some suicide research favors an explanatory framework that is basically psychological, drawing on concepts like reactive aggression (Conner et al., 2003) and cognitive distortions (Ellis & Ellis, 2006). On the other hand, interpersonal explanations emphasize individuals’ interplay with their immediate and meso-level environment. These explanatory models range from the classical sociological concept of anomie (or detachment from one’s group), to social learning (Agnew, 1998; Lester, 1994; Young, 1991), to a voluminous literature on social support (Heikkinen et al., 1994; Kleiman & Liu, 2013; Winfree & Jiang, 2010) and, more recently, interpersonal conceptualizations (Joiner, 2005; Joiner et al., 2009; Van Orden et al., 2010). Taken together, intrapersonal and interpersonal perspectives provide useful ways to address the complex cultural and contextual factors that transcend individual psychology. In this study, we have applied these perspectives to consider how culture and the experience of working in a foreign environment may contribute to suicide among foreign workers in Singapore.
Objectives
The objectives of the current study were to use official records of death to investigate: (1) the demographic characteristics of non-resident individuals who died by suicide; and (2) major factors that may have contributed to non-residents’ decision to commit suicide, including cultural elements.
Coroners’ records are the most comprehensive source of suicide data in Singapore. Simkin et al. (2012) summarized the various ways in which researchers have extracted valuable information from official suicide records to better inform suicide research, prevention, intervention, and post-intervention strategies. Stack and Wasserman’s (2007) qualitative study of suicide records from an American county medical examiner’s office yielded further insights into the relationship between economic strain and suicide. Subsequent studies have used coroners’ records to identify information pertinent to designing interventions for at-risk individuals in financial crises (Coope et al., 2015; Scourfield et al., 2012). In Hong Kong, findings from studies using coroners’ records (Wong et al., 2008, 2010) have contributed to the region’s efforts to raise awareness on suicide, and helped inform suicide prevention and postvention strategies.
Given the inclusion of suicide notes in the coroners’ records, our study was able to undertake a qualitative examination of a sample of these notes. While there has been debate on how representative suicide note writers are of the completed suicides in the general population (i.e., the differences between suicide note writers and those who did not leave a note) (Callanan & Davis, 2009; Demirel et al., 2008; Haines et al., 2011; Stack & Rockett, 2016), findings from studies on suicide note content suggest that they provide a glimpse into the minds of those who die by suicide and can be used to understand the motives behind a suicidal act (Callanan & Davis, 2009; Leenaars et al., 2001). Our study also aimed to examine potential trigger events in the notes of suicide decedents.
Method
Data collation and population
Ethical approval of the study has been obtained from the IRB of the National University of Singapore and information on deaths by suicide from 2011 to 2014 was extracted from the State Coroner’s records between June 2014 and December 2016, with permission from the State Coroner. Review of records took place within State Court grounds, as hard copies and photographic copies of the evidence presented in the case files were not allowed. Data collection was standardized according to a template based on a literature review of commonly analyzed variables in coroners’ studies (Chen et al., 2006; Chia et al., 2011) and on the information available in case files.
Socio-demographic data were available on a total of 1,815 suicide cases, and suicide notes were transcribed in full where they were mentioned or included in the case files. Of the total number of cases reviewed, 307 were identified as non-residents (i.e., not Singaporean or Permanent Resident (PRs), who are foreigners who reside permanently in Singapore and enjoy most privileges that citizens have). Four non-resident suicide deaths were excluded because of the locality of death (i.e., not in Singapore), or not occurring within the target period. Subsequent analysis was based on the remaining 303 cases.
In this article, we present the demographic profile of the resident and non-resident population which has been summarized in numerical tables. Additionally, we conducted a qualitative analysis of suicide notes from 30 randomly selected individuals to supplement our quantitative findings.
Quantitative analysis
Table 1 presents descriptive statics of both the resident and non-resident population. Bivariate comparison of the groups was conducted with Chi Square statistics where applicable. Age was grouped by 15-year bands to better reflect the life stage of the decedents. Employment was grouped into four categories: Professionals (e.g., managers, engineers, clerks, nurses); Domestic workers, Construction workers; Others (e.g., other blue-collar workers, workers of indeterminate professional status, self-employed), Unemployed, and Economically Inactive (retirees, housewives, homemakers, and National Service (NS) men—applicable to residents only). It is important to note that the job titles of the non-residents were not always clear; hence, non-residents of indeterminate professional status, whether white or blue collar, were grouped under the category of ‘Others.’ Regions of birth were divided into South Asia (India, Bangladesh, Sri Lanka), Southeast Asia (Malaysia, Indonesia, Myanmar, Philippines, Thailand, Vietnam), East Asia (China, Japan, Korea, Taiwan), Oceania (Australia), America (United States of America), Europe (e.g., United Kingdom, France, Germany, Russia), and Africa. In Table 2, the numbers of non-residents in each region were aggregated with the corresponding percentages. Chi Square statistics were not computed for Table 2 because many categories were either not applicable to certain non-resident groups or had cell sizes smaller than 5. The test of independence between variables was unreliable; aggregating the sample into larger racialized groups was not done because it was not consistent with the focus of the study on cultural differences, which necessitated examination of the suicides in these distinct groups.
Profile of suicide decedents in Singapore (residents and non-residents): 2011–2014.
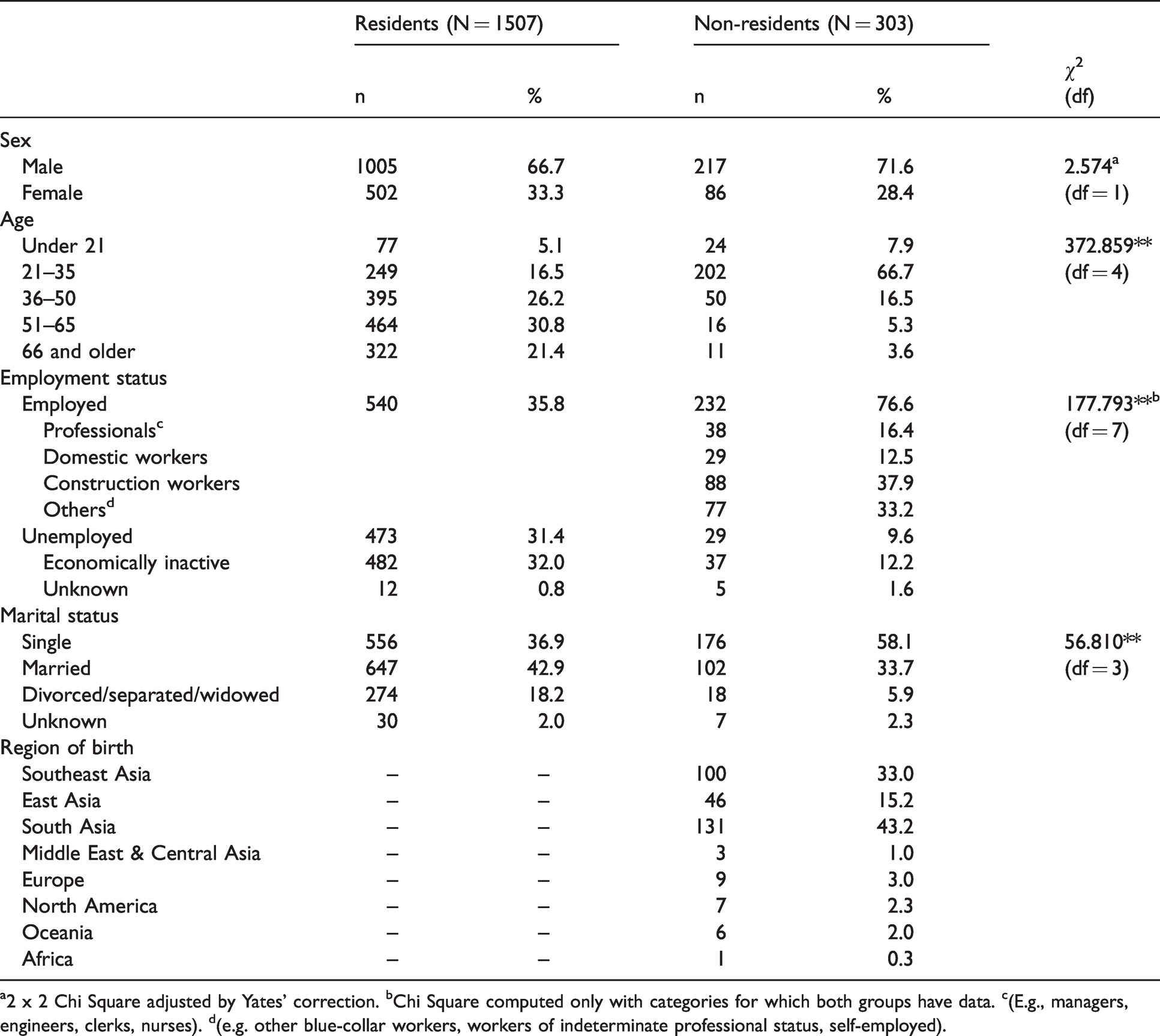
a2 x 2 Chi Square adjusted by Yates’ correction. bChi Square computed only with categories for which both groups have data. c(E.g., managers, engineers, clerks, nurses). d(e.g. other blue-collar workers, workers of indeterminate professional status, self-employed).
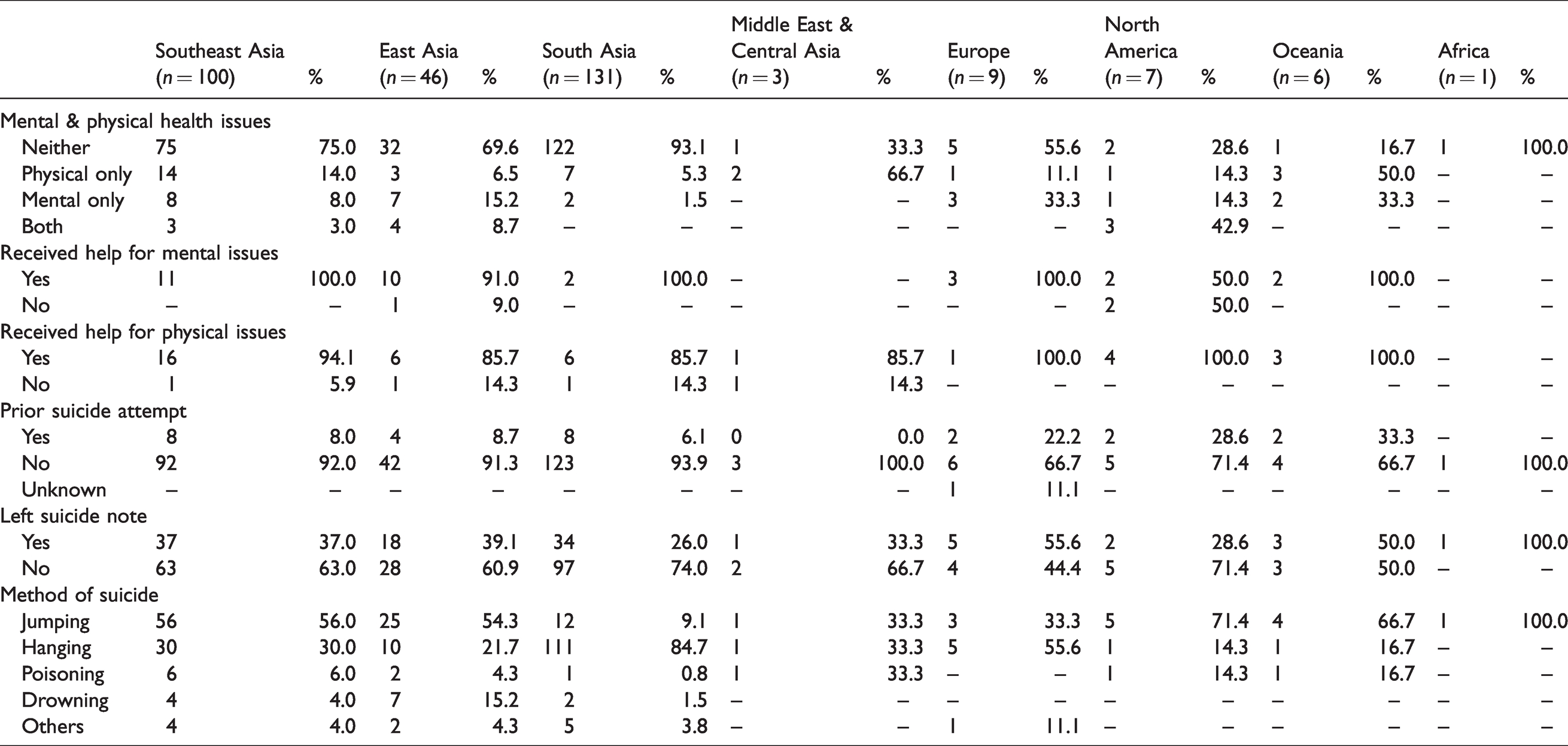
Methods of suicide, mental and physical health profile, other related information of non-residents (N = 303).
Study of suicide notes
To supplement the demographic information, a qualitative analysis of the available suicide notes was undertaken. Of the 303 foreigners who died by suicide, 101 individuals left suicide notes (33.3%). Other studies similarly have reported that only a minority of individuals who die by suicide leave notes. For example, a literature review conducted by Callanan and Davis (2009) found between 15.0% and 38.1% of note writers in samples across different countries. In the present study, 30 non-resident suicide note writers (18 males and 12 females) of ages ranging between 17 and 64 (M = 32.1, SD = 12.2) were randomly selected from the pool of 101. Of this sample, the majority was from Southeast, South, and East Asia, and 23 note writers were working in Singapore at the time of death. Twenty-two note writers left handwritten notes, and the other eight writers left notes that were typed and saved on their devices, sent via messaging applications, or shared on social networking sites. Given that the sample consisted of an international population, the notes were written in their native languages including English, Mandarin, Tamil, and other languages. A number of notes were written in two languages. Translations were carried out professionally by the police and kept as court evidence alongside the original notes for notes that were written in a language other than English (e.g., Malay, Tamil, or Chinese).
Two research staff members reviewed and coded the suicide notes to identify themes, using NVivo 11 software. To facilitate a probability selection of the notes over the period, suicide notes were numbered chronologically. The random selection did not go by particular nationality groups in order to avoid potential biases. Following the familiarization process, notes were randomly extracted separately for each of the two coders. Each coder independently coded reasons for the suicide. Later, the two coders cross-checked each other’s initial codes, discussed them, and reach consensus on the broader themes. These themes were further reviewed and agreed on in the project team meeting.
Results
Table 1 compares the demographic characteristic and the profile of suicide decedents in Singapore from 2011 to 2014 by residents (Singaporeans and PRs) and non-residents. While both groups (Singaporeans/PRs, and non-residents) had a similar proportion of suicides between sexes, with males being overrepresented in both groups, the demography of the non-resident group understandably differed from that of the resident group.
In the resident population, the 51–65-year-old group had the highest suicide rate (30.8%), while in the non-resident population, suicide was most prevalent among 21–35-year-olds (66.7%). A majority of the non-residents were employed (76.6%), while the residents had more varied employment status. Among non-residents, the majority of suicides were from South Asian groups (43.2%), and construction workers (29.0%). With regard to marital status, more non-residents than residents who were single (58.1%) died by suicide.
Table 2 documents the non-residents’ mental and physical health status—whether they received medical or psychiatric treatment, had prior suicide attempts, left suicide notes, and their suicide method. Most of the non-residents did not have a known mental or physical health issue (78.9%) and of those who had known health issues, most received medical (90.2%) or psychiatric (90.9%) help. A majority (91.1%) did not have prior suicide attempts, and more than half did not leave a suicide note (66.7%). The most common suicide method among non-residents from most regions was jumping, except those from South Asia and Europe, where hanging was more common. This difference was less obvious in the European population due to the small number of suicides.
Thematic analysis of suicide note content: Suspected triggers for suicide
Four broad themes were identified from the thematic analysis of the suicide notes: relationship, physical and mental health, employment and study, and financial matters. Importantly, the themes are meant to be understood as suspected triggers and not conclusive reasons for suicide, as most note writers did not explicitly state a specific reason or trigger for why they committed suicide. Of the 30 note writers, eight did not state nor hint at a specific reason for suicide. Note writers who had written multiple notes hinted at issues that may have contributed to their deaths, but did not always write about them in every note. Eight note writers also had notes that contained more than one suspected trigger for suicide.
Relationship
Ten note writers (one-third) mentioned relationships or relationship problems in their notes. Nine note writers wrote about romantic relationships, while one note detailed an unexpected and psychologically jarring physical and verbal assault by dormitory mates. From the notes on romantic relationships, the three notes suggested unrequited love, while one note writer expressed a desire to marry someone. Two note writers wrote about their significant others mistreating them, and one expressed threats towards what seemed to be a romantic partner. Another two note writers expressed melancholic thoughts about love, and one person spoke of the relationship being thwarted by external parties. Despite the varying issues raised, a majority of the notes portrayed a sense of unmet expectations towards potential or existing intimate relationships: “I have fallen in love with the wrong [person] again, isn’t that so? Became that outsider again”; “You cannot marry anyone else as long as I am alive. I will also not marry. If you go against this [not only I die], you will die [too].”
Physical and mental health
Ten individuals specifically mentioned health or mental health issues in their suicide notes, of which three individuals either explicitly diagnosed themselves with a mental health issue or casually associated themselves with a mental health label. More specifically, one individual mentioned feeling depressed while another individual mentioned an inability to control the urge to gamble and described it as an addiction. One individual wrote in such an incoherent way, it suggested writings from an unsound mind. The same individual mentioned feeling “crazy” and stated that there was “something weird” within: “I could not tolerate my stomach ache. I have also been vomiting blood for the past 10 days”; “The closest I would diagnose myself as was dysthymia, which is expressed as a lack of drive or ambition, with a mildly depressive personality”; “From then on, I was very scared of him and got into depression.”
Employment and studies
Five people specifically mentioned their employment or study situation in their suicide notes. Of the five, two individuals, one of whom was a student who may have been on a work internship, appeared to be stressed due to workplace dynamics, despite expressing appreciation for their co-workers or employers, and an inability to perform at their desired level. Two individuals recounted being scolded or humiliated by their employers, one of whom recalled receiving verbal and physical abuse, while another individual’s company denied his requests to return to his country of origin for a sibling’s funeral. Of note, stress arose both from external factors, such as one’s employers, and from expectations individuals had placed on themselves or their companies: “Lately I always made them angry with me but I know that it is my fault … I never think [that I am only here as a maid] that's all; at home I can do this”; “He used vulgar word at me and told me that I am not worth working for him. I also do not want to work for his house anymore.”
Financial matters
One person wrote about being cheated and needing to borrow money, which negatively impacted his view of himself and his own capacity to carry on with life, while another individual had no money to see a doctor after getting injured at work: “I have no peace of mind because I had borrowed money with high interests. The people I trusted had cheated me and that was the reason why I borrowed money.”
Discussion
Consistent with most studies of suicide, the number of males who died by suicide was more than double that of females in both the resident and non-resident samples. Although research has shown that females engage in deliberate self-harm more frequently, males often do so with greater suicidal intent, tend to adopt more lethal suicide methods, and are less concerned with disfiguring themselves during the suicide (Hawton, 2000; Stack & Wasserman, 2009). Previous studies on suicide in Singapore have similarly found that the male suicide rate was higher than the female rate (Chia et al., 2010; Khaw et al., 2011).
In the resident population, suicides were highest among the 51–65-year-olds (30.8%) followed by the 36–50-year-olds (26.2%). From 1955 to 2004, suicide rates of older males in Singapore, not broken down by nationality, remained higher than any other group (Chia et al., 2010). Conversely, the number of suicides was overwhelmingly high among younger non-residents aged 21–35 years (66.7%). Correspondingly, most non-residents were of an employable age. Non-residents typically come to Singapore for employment purposes, compared to Singaporeans and PRs who can be in different life stages. In 2014, the total number of non-residents in Singapore was 1,599,000 (Singapore Department of Statistics, 2016), while the foreign workforce number in the same year was 1,355,700 (Ministry of Manpower, 2017a).
Although the divorced are generally at a higher risk of suicide than the married (Kposowa, 2000; Yip et al., 2015), suicide rates among the divorced and separated were lowest among both non-residents and residents. It is possible that among residents, higher education, better gender equality, and more accessibility to support services make suicide less attractive for the separated or divorced. Among non-residents, living abroad comes with numerous daily stressors that can impact marital relationships and their quality (McNulty, 2014). Married persons may also have the additional responsibility of providing financially for their family overseas, particularly Asian men, who may be seen as the head of the household, and low-wage workers, and so have to work longer hours for more pay (Noor & Shaker, 2017). However, this does not explain the large number of suicides among single non-residents. It could be that more non-residents come to work at their most productive age (when they are single). Married persons might be more reluctant to put up with prolonged separation, given that many of these non-residents were blue-collar workers, whose low wages, and laws and regulations, did not make them eligible to apply for a Dependant’s Pass to bring their family to Singapore. This resulted in an over-representation of single persons among non-resident workers, and subsequently an over-presentation of single non-residents among the suicide cases.
Our study found a disproportionately high number of suicides among South Asian non-residents. Suicides in India are among the highest in the world (Patel et al., 2012). For as yet confirmed common factors, high suicide rates have also been found in Indian populations living or working in some countries like the United States (Shore, 1972), Fiji (Forster et al., 2007), the United Arab Emirates (Al-Maskari et al., 2011; Dervic et al., 2012), and Guyana (Shako, 2020). For example, in Dubai, 73.8% of suicides among the expatriate population from 2003 to 2009 were Indian (Dervic et al., 2012). Many researchers suggest the culture of one’s Indian origin would have shaped both the rate and the ways people committed suicide. Indian cultural acceptability of suicide is prevalent, and suicidal thoughts and behaviors appear to be relatively common (Kar & Thirthalli, 2015), though religious teachings frown upon suicide. The cultural idea is to preserve an intact/undamaged body for future life, and also the masculinity role is not to follow the common use of poison among Indian women. In fact, in Guyana, Indian men were three times more likely to commit suicide by hanging instead of drinking poison compared to females (Shako, 2020). Although none of these studies provided definitive explanation on the role and impact process of culture, cultural factors are surely involved. For the only exception—Indians or Asians had the lowest suicide rate in South Africa (Kootbodien et al., 2020)—there is no cross-tabulation information on ethnicity and education level / occupation. It is likely that unlike other countries importing low-skill migrant workers, these Indians in South Africa were more educated expatriates who were different in profile from the subjects in other countries.
A majority of the non-residents who died by suicide were not found to have physical or mental health issues, although this could be due to the sparse information on the non-residents who committed suicide. Interestingly, most non-residents who had mental or physical health issues had received help, which raises the question of what help was given, and of how, if possible, services could be improved to identify and reduce suicide risk among non-resident populations. Unfortunately, the dates of decedents’ last medical and psychiatric visits were not collected, and a clear link between the proximity of suicide to the date of help received could not be drawn. Even if these data might have been available in some cases, caution has to be taken in interpreting the result that mental health problems did not emerge as a key contributing factor in suicides among the non-resident populations. Firstly, the mental health literacy level was found to vary between countries. In an experimental study, Loo et al. (2012) found that British participants displayed better mental health literacy than did those from Hong Kong or Malaysia in the identification of nine different mental health diagnoses; Malaysian participants as a whole consistently had the lowest level of mental health literacy in the comparison. Unfortunately, there is no sub-sample comparisons among Chinese, Malay, and Indian Malaysians. In fact, the Indian Malaysians took up only 12.7% of the 150 Malaysian participants. At the same time, more British participants than other groups approved of the professional help scenario in the vignette case. It may be that concepts, beliefs, and knowledge levels about mental health shape the perceived availability of alternatives and avenues for help, resulting in group differences in help-seeking. Beliefs about and interpretation of symptoms may be very different among non-residents who carried their own cultural understanding about mental health and illness. Secondly, availability and accessibility of current mental health services (i.e., in Singapore) may be perceived differently by non-residents in general. Some of the common ‘barriers’ to accessibility are being discouraged by a lack of information, language barriers, and expensive transportation costs (relative to their income) (Pepin et al., 2009). Non-residents may simply not take steps to seek professional help and be diagnosed. All these factors may have obscured the relationship between existing mental health problems and suicide among non-residents.
Although prior suicide attempts pose a risk for suicide in the Asian context (Chen et al., 2012), most of the non-residents in our sample had no documented prior suicide attempt. There could be different explanations for this. It is possible that motivations and events leading up to their suicides only culminated in Singapore, or pertained to novel life events specific to the Singapore context. The absence of social networks for non-residents may also have prevented access to information, resources, or help. Other possibilities include the concealment or under-reporting of previous suicide attempts as a means to avoid dismissal threats, for fear of being sent back to home countries. All these factors might have made repeaters less visible in the non-resident populations.
While jumping was a prevalent suicide method among Southeast Asians (56.0%) and East Asians (54.3%), hanging was by far the most common method among South Asians (84.7%) and marginally more common among the small European sample (55.6%). Jumping has previously been reported as the most common suicide method in Singapore (Chia et al., 2010), which may be due to the accessibility of high-rise buildings. Accessibility has been found to influence one’s choice of suicide method (Chia et al., 2011). Evidence suggests that restricting accessibility to the tops of buildings may lower suicide numbers in some areas (Chen et al., 2015; Sarchiapone et al., 2011). Migrant workers would likely be checked and questioned if they wandered into estates built by the Housing Development Board, whereas residents who live there mostly have no issue accessing high places. Accordingly, it is possible that many non-residents chose jumping due to its easy access in Singapore. Fatality may be another consideration. Sometimes, what worries attempters is not death, but the serious disability one might suffer in failed attempts. Conversely, hanging is the most common suicide method in India (Rane & Nadkarni, 2014) and Europe (Office for National Statistics, 2015; Värnik et al., 2008), which suggests the cultural acceptability of hanging among both Indian and European nationals. A study conducted in Singapore based on the coroners’ records from 2000 to 2004 similarly found that Indians were twice as likely to hang themselves compared to other nationalities (Chia et al., 2011), although there was no mention of the breakdown by nationality.
While the descriptive statistics provide some insight into the demography of non-resident suicide decedents, we were unable to draw a conclusive comparison between the resident and non-resident populations on the significant factors for non-residents’ suicides.
Despite the small sample of notes analyzed, our qualitative findings add to the literature on Singapore’s unique cultural context. Suicide notes are thought to contain insights into the minds and motivations of those who die by suicide (Callanan & Davis, 2009; Leenaars et al., 2001). However, messages may not always be straightforward. Even among writers whose suspected triggers for suicide could be elicited, some may not state all factors explicitly. For instance, some note writers may have written about an issue they were facing without stating that it was driving them to suicide, while others might seem preoccupied, though not overly distressed, with the issues they write about. Consistent with existing literature (Rogers et al., 2007), we also found that individuals tend to mention more than one trigger.
Findings from our thematic analysis point to the paradoxical nature of suspected suicide triggers as both idiosyncratic and universal. Although the situations that note writers faced varied within each theme, the suspected triggers identified in our study were also universal, consistent with Chia et al.’s (2008) analysis of 387 suicide notes in Singapore, which found school, relationship, and marital issues associated with social problems such as gambling, and physical illness as reasons for suicide across different age groups.
As there was no information collected on the number of years that non-residents had lived or worked in Singapore, it is difficult to estimate the impact of culture or acculturation in the suicides of our non-resident sample. In addition, studies on non-residents in Singapore (Chib et al., 2013; Lee et al., 2014) tend to discuss employment-related stressors apart from acculturation issues such as language barriers. However, the population in such studies usually consists of blue-collar workers of a lower socioeconomic status, whereas the non-residents in our sample come from a wider range of socioeconomic backgrounds, which include, but are not limited to, blue-collar non-residents. In our suicide note analysis, it was triggers pertaining to note writers’ relationships and health that featured most strongly.
Relationship issues have been found to be a common motive for suicide. Interpersonal conflicts or loss, largely with a romantic partner (Weyrauch et al., 2001) are common. Romantic problems occurred more frequently than work or school issues in the notes of both men and women in a U.S. study (Canetto & Lester, 2002), while younger men were found to express romantic problems in their notes frequently in an Australian study (Lester et al., 2004). Living abroad is a potential trigger for suicide. A study on domestic workers from the Philippines found that they faced more loneliness while living overseas and relied on emotion-focused (e.g., seeking social support) coping strategies due to their increased isolation (van der Ham et al., 2015). These findings suggest that relationships with others may be even more critical among non-residents as these enable them to cope with migration-related stress. Consistent with a few of the notes in our analysis that mentioned fighting with one’s dormitory mates and threatening a significant other, evidence suggests that acute conflicting relationships can lead to suicides for some. Rather than a personal attribute of impulsivity, acute relationship conflicts may trigger an anticipated threat of arrest, conviction, imprisonment, and ultimate repatriation, which may further be construed as cultural shame, personal degradation, and financial hardship.
Physical and mental health problems were another suspected trigger that stood out in our analysis. Physical health problems and related issues such as reduced quality of life and an inability to function independently were mentioned by a considerable portion of older people in their suicide notes (Cheung et al., 2015), while mental health issues were present in the notes of adolescents online (Cash et al., 2013). We suspect that health problems may hold an even greater significance for non-residents who were in Singapore primarily for work, or in blue-collar jobs, as deterioration in health can signify threats, such as mounting treatment costs, a drop in productivity, and the repatriation back to their home country. In Singapore, research conducted among migrant workers found that many had a poor awareness of their health insurance coverage, and medical leave was accepted in several companies only when workers saw company doctors. Lower income, perception of inadequate finances, and a view of the illness as not serious were found to be risk factors for not seeking timely care (Ang et al., 2017; Lee et al., 2014). Unfortunately, exposure to various physical and psychological health risks is common for blue-collar workers, who view potential health problems as part of their work (Panikkar et al., 2015). Health problems may also prevent non-residents from realizing their commitment to financially support their family in their country of origin.
The prevalence of relationship and health issues in our sample adds preliminary evidence of their importance as suicide triggers in the Singapore context. Our findings also suggest that more attention should be placed on relationships and health when it comes to ensuring the well-being and reducing the suicide rate of non-residents in Singapore. It is apparent that both intra- and interpersonal issues dynamically interact with the socio-cultural contexts of both home and host countries.
Limitations
The present study had a number of limitations. First, information pertinent to the study may not have been consistently required or recorded. Bennewith et al.’s (2005) study on the usefulness of coroners’ data noted that information relevant to suicide research, such as contact with professional help, and medical and psychiatric history, is occasionally unavailable or not required. We faced similar challenges in the current study. For non-residents, information on suicide history including prior attempts, suicide within the family, medical and psychiatric history as well as history of professional help sought, and prior verbalization of suicide intent was particularly sparse, perhaps reflecting a lack of contactable social support networks from which such information would typically have been gleaned. Second, not all suicide notes were written in English, which increases the possibility that translated notes may have lost some of the cultural nuances that note writers meant to convey. Third, as information on the number of non-residents in Singapore, broken down by nationality, was unavailable, we were unable to determine whether the number of non-resident deaths by region was accounted for in proportion to Singapore’s non-resident population by region, or if other factors were responsible for the high number of suicide deaths. Fourth, there are limits to the generalizability of findings from the suicide note analysis in view of the small sample size, which was drawn out of only 33.3% of non-residents who left suicide notes. Finally, we are also aware of the complexity of intra-ethnic and intra-cultural variation in the different non-residents’ home countries, which would require larger samples to generate and test hypotheses.
Conclusion
Despite its limitations, the present study provides some directions for future research that have the potential to increase our understanding of suicides in Singapore among the non-resident populations, and may help inform prevention efforts. In light of the finding that a majority of non-resident suicide decedents were from South Asia, more research is needed to clarify whether this is due to the relative size of the South Asia population in Singapore and to identify commonalities and differences among non-residents from this region, in areas such as demographics, psychological and personality profiles, and cultural acceptability towards suicide. Research should also focus on non-residents from other regions, particularly Southeast Asians, among whom suicide numbers were also high. To gain a better understanding of culture-specific factors, a more stringent research design is needed, as well as a more comprehensive recruitment of participants from Singapore-born South Asians, South Asian migrant worker communities, and South Asians living in India.
Our analysis of the suicide notes, while limited by issues of generalizability, brought attention to relationship and health issues and how they are culturally interpreted as suspected triggers of suicide among non-residents in Singapore, and highlighted the potential to strengthen research and interventions in these areas. Based on our suicide note analysis, personal coping skills appear important in handling the types of relationship issues faced, and relief is unlikely to come solely from top-down intervention strategies. Nonetheless, as relationships are of importance in managing migration-related stress (van der Ham et al., 2015), interventions that are targeted at helping non-residents to build healthy relationships and manage relationship expectations between themselves, significant others, and colleagues would be useful. Cultural interpretation of calamity in relationships can also be addressed. Preparation of foreign talents or migrant workers may include discussing or rehearsing the scenario of ‘catastrophic’ situations. On one hand, migrant workers should be educated on the employment laws and their rights in order to minimize issues of exploitation. On the other hand, service provision for foreign workers should address the question of access by those who work long hours and may not enjoy a rest day. Conflict resolution and possibly legal aid may be another area of need if one is left to fend for oneself. Although by law, workers are not allowed to work more than 12 hours a day, it is common for employers to ask for overtime work and to lure workers with overtime pay. As a result, long working hours can make it difficult for non-residents to seek or develop social support from friends and relationships. Providing alternative sources of support, such as encouraging an inclusive workplace, may be beneficial in expanding the community that non-residents can turn to in times of distress. Creating opportunities for sharing with workmates may require broader psychoeducation initiatives encouraging people not to construe help-seeking as a sign of personal weakness. Fostering more supportive responses from immediate supervisors is also needed. Employers need to improve their understanding of human capital and provide more supportive environments, rather than rely on intimidation of what they view as a replaceable workforce.
With regard to the frequent mention of health issues in the suicide notes, there is a need for medical and psychiatric professionals to be increasingly sensitive to suicide risk in non-residents. For non-residents of blue-collar status, sensitivity to suicide risk may be insufficient, as financial or other considerations might prevent them from seeking timely or adequate help. We suggest that non-residents should be supported by positive employment practices, including preventive measures, such as observing work safety, creating channels for feedback between employer and employee, raising non-residents’ awareness of their insurance coverage on health and mental health issues, broadening coverage and including more clinics, and providing additional financial support for those with severe conditions. At other times, physical and mental health problems may also arise or be exacerbated by surrounding circumstances. To reduce health-related stress for foreign workers, clearer and more widespread promotion of health policies both on the job and during pre-job workshops might be helpful in raising non-residents’ awareness of and connectedness with appropriate healthcare services. Both governmental and non-governmental organizations like the Ministry of Manpower, Migrant Workers’ Centre, and HealthServe can help enforce health and safety, prevention, and public information measures to ensure that non-residents have knowledge about and access to the healthcare services they need.
Footnotes
Acknowledgements
We would like to thank Samaritans of Singapore (SOS) for their support of this research, particularly their assistance in data collection for the figures and the content of the death notes. We must also thank the State Coroner Mr. Marvin Bay for his support and kind permission to access the coroners’ records.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.