
Abstract
Individuals with dementia and their carers often experience a rupture of relationships that co-occurs with declining functional and cognitive abilities, leading to their increased social exclusion in both intimate relationships and community settings. While initiatives have been developed to support meaningful interaction and participation in society, they have broadly ignored the significance of how cultural factors influence experiences of inclusion/exclusion of these individuals. An ethnographic study was conducted by an interdisciplinary research team between April 2018 and January 2019 to explore the intersections of culture and social inclusion/exclusion in a culturally diverse group of persons with dementia, caregivers and staff members of a non-profit organization located in a multicultural neighborhood of a bilingual Canadian city. The participants’ culture was inextricably linked to their experiences in three overarching themes of social inclusion/exclusion: transformation of the person with dementia and the caregiver; participation in social networks and meaningful relations; and styles of care provision in health and social services. Cultural mandates that prescribe practices of intergenerational care shape the way certain caregivers perceive their role and mitigated experiences of exclusion. Culturally specific notions and views associated with dementia prevalent in certain communities increased experiences of inclusion or exclusion. Engagement with the cultural elements of individuals with dementia was shown to be an effective and underexplored tool for fostering inclusion. The results of this study highlight the value of the ethnographic methods for incorporating the perspective of persons with dementia in research.
Keywords
Introduction
The global trend of population aging has been accompanied by the increasing prevalence of persons with dementia (PWDs). Dementia is a Western disease category, defined as a set of symptoms that are caused by disorders affecting the brain. It is not a specific disease, but the result of many diseases, including Alzheimer’s disease and vascular dementia. Although a culturally-specific notion such as dementia cannot be a universal tool for cross-cultural analysis (Kleinman, 1977; Cohen, 1998), this condition is widely recognized and treated in Euro-America. For example, in Canada, an estimated 564,000 individuals are currently living with dementia, and a 66 per cent increase is expected by 2031, bringing the anticipated total to 937,000 individuals (Alzheimer’s Society of Canada, 2010).
Although the symptoms associated with dementia (e.g. memory loss, lack of self-awareness and individual autonomy, verbal expressivity) are common across individuals, the experience of this condition is strongly mediated by the cultural aspects and relationships in which they are embedded. For example, in Euro-American societies, the loss of rational thinking and autonomy is often associated with a diminished sense of the PWD’s personhood; in contrast, cultural milieus with a relational-dominant understanding of personhood often assess and negotiate dementia through intersubjective knowledge (Kitwood, 1997). Elizabeth Herskovits (1995)’s review of works on Alzheimer’s show that these cultural groups disentangle an individual’s status of “self” from cognitive ability and privilege the relational self over the autonomous self. Lawrence Cohen (1995) illustrates how the embodiment (e.g. self-in-body) of PWDs in India are part of their social relations with their surroundings. In her ethnography of an individual with dementia in Holland, Roma Chatterji (1998) problematizes the concept of voice, extending it beyond verbal expression to other forms of embodiment and social interaction in which the self of the PWD remains present. The findings of these previous studies underscore the cultural confusion presented by PWDs in an institutionalized biomedical context while the sense of their personhood evolves in the course of their ongoing relations with family and carers. The individual experience of dementia is also strongly intertwined with religion and spirituality: many PWDs and their carers rely on their faith systems to cope with the diagnosis (Snyder, 2003), to find meaning post-diagnosis (Bell & Troxel, 2001; McFadden, Ingram, & Baldauf, 2000), and to provide a community of support through churches, synagogues and other places of worship (Gwyther, 1995).
Due to the prevalence of dementia in Euro-American countries and its life-changing effects, most research has considered it as a “burden” that impacts those living with the condition (e.g. Wolter et al., 2019), their family members (e.g. Liu et al., 2018; Konerding et al., 2018), health and social services (e.g. Boustani, Schubert, & Sennour, 2007; Frytaka et al., 2008), and society at large. Relationships between the PWD and their carers often undergo severe strain when speech and communication change. As a result, individuals with severe dementia often find themselves increasingly excluded from the social world, and as such, negated as social agents (Abad, 2002; Bartlett, 2007; Kimura, Maffioletti, Santos, Baptista, & Dourado, 2015; Kitwood, 1997; Meyer et al., 2016; Qazi, Spector, & Orrell, 2010). Carers of PWDs also experience a rupture in their relationships. Many care for loved ones with dementia at home to prevent them from being institutionalized and socially excluded from their communities. However, this arrangement is associated with a significant increase in costs and responsibilities for the family caregivers, which often translates into their decreased participation in local communities (Batsch & Mittelman, 2012; Daly et al., 2013; Rodriguez et al., 2003; Svanström & Dahlberg, 2004; Meyer et al., 2016; Vallée & Vallée, 2017). Carers can also experience an increasing social isolation. Stigma and misunderstanding often cause family, friends and health care providers to distance themselves from those with dementia and their caregivers (Clarke & Bailey, 2016; Daly et al., 2013; Forbes et al., 2011; Duane, Brasher, & Koch, 2011; Svanström & Dahlberg, 2004; Svanström & Sundler, 2015; Upon & Reed, 2006; Tranvåg, Petersen, & Nåden, 2015; Westwood, 2016). The resulting social exclusion is further exacerbated by social and health services that are not available or adapted to their needs (Clarke & Bailey, 2016; Forbes et al., 2011; Gove et al., 2016; Hare, 2016; Innes & Sherlock, 2004; Innes, Page, & Cutler, 2016; Tranvåg et al., 2015; Westwood, 2016; Williams, 2013).
In recognition of the devastating consequences of fractured relationships at both intimate and community levels, recent initiatives have focused on supporting social inclusion of PWDs and their carers by fostering meaningful interactions with others and participation in society. Many strategies are conceived in very general terms (Gilhooly et al., 2016), and have broadly ignored the significance of socio-cultural contexts for these individuals. A growing body of research has underscored the influence of cultural background on experiences of social exclusion (Hinton & Levkoff, 2000; Kong, Deatrick, & Evans, 2010; Navab, Negarandeh, Peyrovi, 2012; Dilworth-Anderson, 2004), but the extent to which culture shapes the experiences of inclusion for PWDs and their carers remains largely unknown (Westwood, 2016). This research paper aims to address this gap in knowledge, exploring the significance of the intersection of culture and social inclusion/exclusion in a group of PWDs and caregivers. More specifically, it focuses on how culture influences the moments, situations and places in which these persons experienced social inclusion/exclusion. An interdisciplinary research team composed by an anthropologist (RMO), three biomedical researchers (JSC, CLW, SBM) and four community-based partners (PB, MW, SS, OJ) conducted an ethnographic study between April 2018 and January 2019, in a non-profit organization that provides services for PWDs and their caregivers in culturally diverse neighborhood of a major Canadian city. In this study, we paid particular attention to the perspective of PWDs, which is still underrepresented in dementia research (Lloyd, Gatherer, & Kalsy, 2006; O’Connor et al., 2007; Smebye, Kirkevold, & Engedal, 2012; Svanström, & Sundler, 2015; Wilkinson, 2002).
Approach and Methods
This study is based on an ethnographic approach that aims to understand the experiences of social inclusion and exclusion of PWDs and their carers from the perspectives of multiple actors (Geertz, 1973; Mattingly, 2010). Ethnographic methods (participant observation, informal interviews and semi-structured interviews) were used to thoroughly explore the points of view of: 1) PWDs; 2) primary caregivers; and 3) staff members about situations, moments and places of social inclusion and exclusion. We focused on the dyad composed of the PWD and the primary carer. This study used a participatory research approach to develop the research questions and methodology in partnership with a non-profit organization (henceforth “the organization”) that provides a wide range of services for PWDs, family caregivers and professional/paid caregivers. The organization was in a culturally diverse area of a bilingual Canadian city and served many immigrants and persons from minority groups. The anthropologist (RMO) conducted nine months of ethnographic fieldwork at this organization and the homes of the organization’s clients. Prior to beginning this research, RMO conducted three months of volunteer work to familiarize herself with the organization and the study’s participants. RMO’s multilingual competence (Spanish, French and English) and her migrant background facilitated her interactions with most research participants, who had similar characteristics. She is not affiliated with the organization other than through this research project.
Ethnographic methods, including participant observation and ethnographic interviews, were used in a sample of individuals (n = 49) who were recruited through purposive sampling (Emmel, 2013). RMO conducted participant observations with PWDs, caregivers and staff members while accompanying PWDs in their activities at the organization (e.g. playing card games and memory games, dancing, doing tai chi, drawing and painting, etc.) and supporting staff members in non-therapeutic practices (e.g. setting tables, distributing lunches and snacks, helping clients to perform activities). This method was deliberately selected to maximize the participation of individuals with dementia in this study; participant observation allowed the researcher to study individuals in settings familiar to them, where they conducted their everyday activities, enabling spontaneous conversations to emerge in real-time, rather than relying on the memory of individuals with dementia. Furthermore, participant observation de-emphasized the focus on verbal expression – which excludes many PWDs from traditional data collection techniques such as interviews and focus groups – and instead shifted the focus of the research to the everyday enactment of implicit cultural values. While participant observations were focused on detailed description, informal interviews were steered toward the subject of social inclusion and exclusion. Additionally, core participants (n = 12) were followed through their everyday routines at the organization 1 to further understand their experience of situations and moments of inclusion and exclusion. Visits to the field occurred between one and four times per week and lasted between four and eight hours per day, for a total of approximately 220 hours of observation. Interactions were conducted in English, French and Spanish. Field notes of observations and conversations were taken and digitally transcribed.
To enhance the validity and comprehensive understanding of the participants’ experiences of social inclusion and exclusion, RMO also conducted semi-structured interviews with a sub-group of participants for triangulation (Patton, 1999). Participants were selected for this subgroup with the help of staff members through purposive sampling. To ensure sample diversification (Pires, 1997), gender, age, and cultural background were considered. In the case of PWDs, we did not formally account for the stage of their dementia, though we tried to include participants at different moments of its progression. In the case of the caregivers, we endeavored to collect diverse perspectives by targeting a variety of relationships with the person with dementia (e.g. spouse, child). Of note, most primary caregivers belonged to the nuclear family of PWD. This subgroup was interviewed individually or in pairs (PWD and caregiver) for 15–90 minutes. The semi-structured interview questions were adapted to the needs of PWDs with the help of staff members and caregivers, which allowed the anthropologist to thoroughly explore the participants’ points of view about specific themes identified through participant observation. This forum also allowed individuals to discuss experiences of exclusion in one-on-one private conversation. Interviews were audio-recorded and digitally transcribed (Table 3).
RMO conducted thematic analysis of semi-structured interview transcripts and fieldnotes of participant observations, and comparatively analyzed both sources of information for triangulation. To ensure validity, four other members of the research team thematically analyzed 20% of the collected information (Miles, Huberman, & Saldana, 2014), identifying emergent themes and sub-themes in an iterative manner (Glaser & Strauss, 1967) and refining the coding process. To obtain consensus on experiences of social inclusion and exclusion, members of the research team discussed the collected information during face-to-face meetings held throughout the study period. In keeping with the participatory research approach of this study, two community-based partners from the organization (PB, MW) were involved in identifying emergent themes from the data, and in discussions about the interpretation and meaning of the findings. Four community-based partners (PW, MW, SS, OJ) reviewed several drafts of this paper. Community partners were selected purposively, based on their interest in the research project and their availability. They were already familiar with ethnographic research and no additional training was provided. The partnership with the organization benefited this study at many dimensions of the research process, including facilitating the recruitment and retention of participants, designing accessible research instruments, validation of results, and drafting a manuscript more reflective of genuine culturally-shaped moments of inclusion and exclusion. However, while working with our community-based partners, we faced certain challenges such as devoting extended time to mutual learning and negotiation. The centrality of culture to the experiences of social inclusion and exclusion emerged over the multiple iterations of this analysis; the theme was not established a priori to the study or the data collection.
The study was approved by the Institutional Review Board of McGill University (A06-B25-17B). Written consent was obtained from all caregivers, and all PWDs who were deemed capable of providing informed consent according to their primary caregiver. For those who did not have the required cognitive capacity, substitute decision makers provided written consent on behalf of the PWD, and assent was sought from the PWD prior to and throughout the course of the study. The data presented in this research article has been anonymized by changing the names of all participants, institutions and places.
Results
Study sample
The ethnographic sample was composed of 49 individuals: 31 PWDs, nine caregivers and nine staff members. Of the 25 persons approached to participate in the semi-structured interview sub-group, 21 agreed to be interviewed (response rate = 84%). The subgroup consisted of PWDs (n = 7), caregivers (n = 8), and staff members (n = 6). The demographics of all participants are presented in Table 1.
Demographics.

Language and cultural background
Participants had a wide variety of linguistic and cultural backgrounds. The linguistic diversity was particularly striking amongst the PWDs: almost two-thirds spoke at least three languages – most commonly English, French and Yiddish. Most caregivers and staff members spoke at least two languages – most predominantly English and French. During the study period, the multiplicity of the participants’ linguistic background shaped their interactions, as illustrated in the following field note excerpt: Today, a new client, Sebastian, incorporated into the group. Sebastian likes to sing. During lunch time, he hummed the background music that was played in the computer. He suddenly started changing the lyrics of a song in English into a different language. Michelle, one of the staff members, asked Sebastian what language this was. He said Russian. Michelle brought Sebastian close to Aretha, who also speaks Russian. Aretha told him that she learned Russian in Siberia, where she and her family escaped after the Nazi occupation of Poland. Sebastian said that he and his brothers also had to escape their hometown in Poland, but they lived for three years in the woods among the partisans and then he moved to Russia. They suddenly switched into Yiddish. Shirley, a staff member who speaks Yiddish, translated parts of the conversation for us. The computer played “Besame mucho” and Alexander, another client, started singing in Spanish, looking at me. I sang with him and before the song ended, I asked him to change the lyrics into French. He changed parts of the last verse of the song. Hughes, who had hearing problems, thought we were speaking Italian and asked me in Italian if I could bring him a glass of water. It seems like I had lunch in the Babel tower: there were conversations in at least five languages. (Field note excerpt June 26, 2018)
Languages spoken and cultural background.
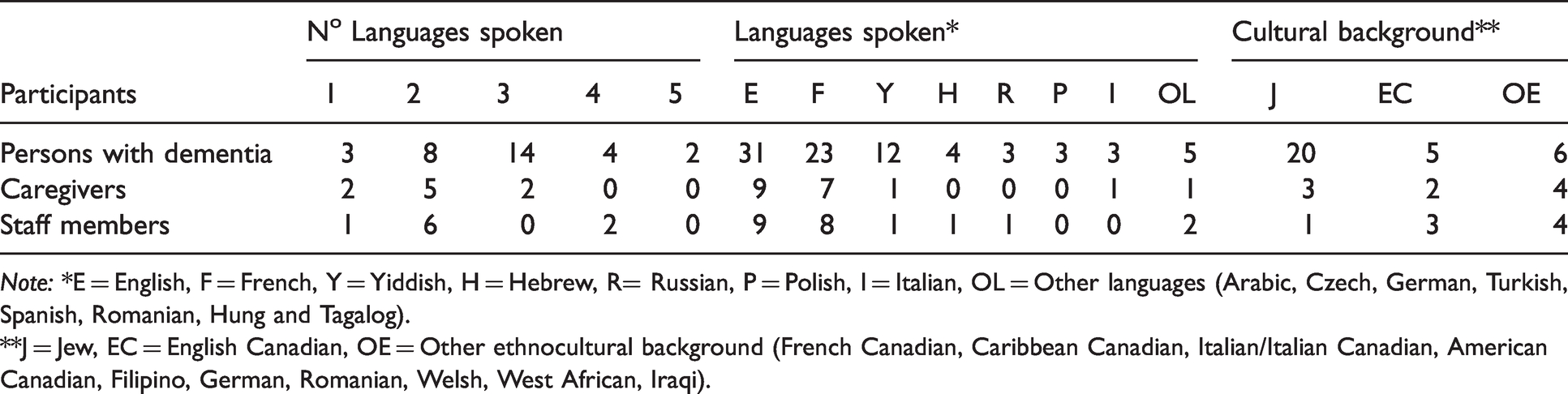
Note: *E = English, F = French, Y = Yiddish, H = Hebrew, R= Russian, P = Polish, I = Italian, OL = Other languages (Arabic, Czech, German, Turkish, Spanish, Romanian, Hung and Tagalog).
**J = Jew, EC = English Canadian, OE = Other ethnocultural background (French Canadian, Caribbean Canadian, Italian/Italian Canadian, American Canadian, Filipino, German, Romanian, Welsh, West African, Iraqi).
Main questions in the semi-structured interview guides for persons with dementia, caregivers and staff members
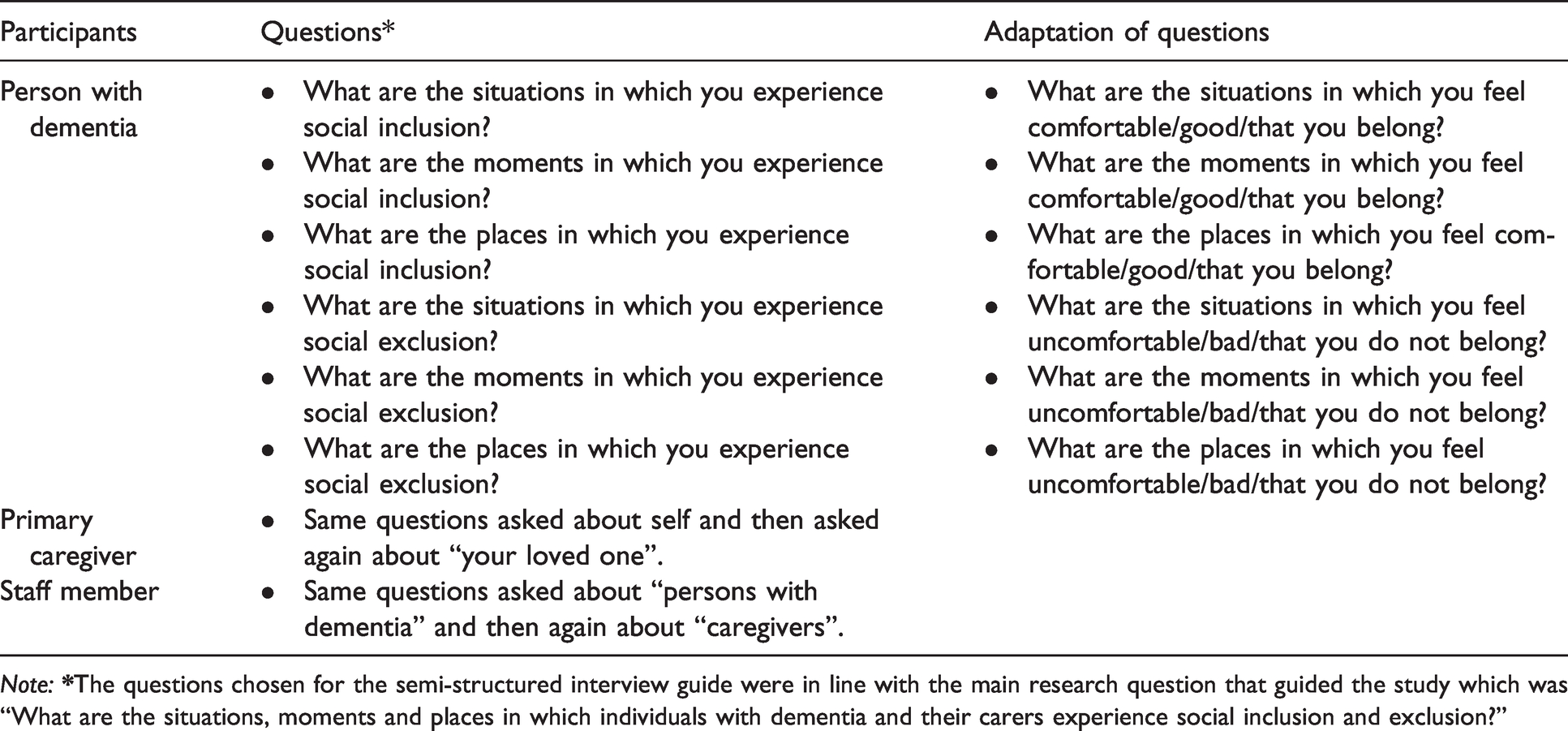
Note:
It was notable that Jewish participants had difficulties identifying experiences of social exclusion. When they were asked about places, situations and/or moments in which they were excluded, they almost reflexively replied that they had not felt that way. The interviewer often had to paraphrase the question and asked them for specific places, situations and/or moments in which they felt “uncomfortable”, “bad”, “did not belong to” or that they “were disliked”, within and outside the Jewish community. These participants reported few experiences of exclusion and frequently highlighted avoiding situations in which they could be excluded (e.g. “I hardly feel uncomfortable because if I go to a place and I don’t feel good, I don’t come back anymore.”). Of note, a significant number of PWDs who participated in the study were Holocaust survivors or children of Holocaust survivors. They shared with us their (or their parents’) ordeal during Nazi occupation 2 and, after immigrating to Canada, the anti-Semitism experienced in the host country. 3 As described in other studies (Winfeld & Sigal, 1981; Shuval, 1957), it is highly possible that certain inherited or personal experiences of extreme discrimination had marked how they perceive certain forms of social exclusion (e.g. anti-Semitism) in the present. Additionally, some studies suggest that Jewish communities have a less negative view about dementia in comparison with other cultures (Cahn, 2005; Jotkowitz, Clarfield, & Glick, 2005). 4 The convergence of these factors likely contributes to the difficulty faced by most Jewish participants in identifying moments of exclusion.
Experiences of social inclusion and exclusion
Three overarching themes of social exclusion and/or inclusion were identified in the experiences of PWDs and their caregivers: a) transformation of the PWD and the caregiver; b) participation in social networks and meaningful relations; and c) styles of care provision in health and social services.
a) Transformation of the PWD and the caregiver
Participants discussed many well-documented and anticipated transformations associated with dementia that hindered social inclusion. Memory loss, for example, strained relationships and led to distress, as described in the in the following field note excerpt: I met John at the beginning of my fieldwork. We immediately clicked and did all the activities together. By the end of the day, when the clients prepared to leave, he grabbed me by the arm and told me that he wanted to introduce me to Janet, his caregiver, who just came to pick him up. “Look who I’ve met today, I got a new friend! We’ve had a really good time.” We all laughed. The following week, I met John again in the activity room. When I made eye contact with him, he looked away uncomfortably. I felt unsettled for a second, but then I thought that he probably did not remember me. I approached him and introduced myself. We did the activities together. By the end of the day he told me that he was happy to have met me and that he wanted to introduce me to his caregiver. Janet smiled and let John introduced me to her again. This set of interactions between John and I repeated few more times: John and I meet in the activity room, he does not recognize me, along the day we become friends and by the end he introduces me to his caregiver. One day, Janet told John that he had already introduced us. John laughed nervously and apologized with me saying: “I’m not the person I used to be! My mind plays games with me and this is something that worries me … this makes me very uncomfortable …” (Field note excerpt June 5, 2018) It’s a second marriage for Julian and I. So, my kids from my first marriage live in Renfrew and he loved those kids … I was in Renfrew [last week]. He never even asked me, “What did you do? How are the kids? I wish I could have gone.” You know, there’s just none of that. It’s very … I don’t know what the word is, but lack of interest, lack of initiative, lack of emotion. It’s like … Somebody in the support group, she’s not there anymore, but she used the phrase “You’re a married widow.” In other words, you’re married in name, but there’s nobody there. (Heidi, caregiver, Jewish, interview) It’s a lot, it’s really a lot. I have to take care of them [her two parents with dementia]. So now I can’t go anywhere. (Lisa, caregiver, Caribbean, interview)
Culture and the effects of transformations
The cultural expectations and values of the participants strongly shaped how they experienced these transformations. For some, the cultural mandate of caring for elderly family members allowed them to accept the transformations, facilitating the maintenance of relationships. Participants of Caribbean, Italian and Jewish origin pointed out that caring for the elderly at home was an integral part of their culture and an opportunity to “give back” to them. These cultural values and mandates often translated into practices that fostered inclusion. For example, a participant of Italian origin proudly showed us the multiple adaptions she had made in her home to build an environment in which her mother could be at the same time “autonomous” and “connected” to the family. Another participant of Caribbean origin quit her job and moved to her parents’ place to take care of them: I made that decision. I know … it’s a weird, unusual situation. But I don’t mind … So, for me, it doesn’t look strange because, in my culture, we take care of our parents until the end of their life … I’ve spoken to people in other communities – and not just people from my culture [the Caribbean culture], but Latinos, southern Europeans – and they’re not into just dumping [their parents] … in these institutions. (Lisa, caregiver, Caribbean, interview) It became very important to say, “Okay. So, am I gonna go down with the ship or not?” And the main thing is caring for the person who’s got dementia. And the important thing is you’re the best person to do that. And that you are healthy enough to do it, and have the patience to do it, you have to do as many of the things as you used to do and that you can do without forgetting your partner. (Fred, caregiver, Jewish, interview)
b) Participation in social networks and meaningful relationships
Participating in social networks and experiencing meaningful relationships among family members and friends was highly valued by most participants, and the basis for many reported experiences of inclusion. All PWDs reported enjoying the company of their family members and feeling included when they were “around”. Today, Michelle asked the clients to describe a happy moment of their life in which they felt “good”, “fulfilled”, “completed” and that they “belonged”. Almost all of them said that they were happy when they were with their family. For example, Ulysses said that every Sunday afternoon he was the “happiest man on earth” because he received the visit of his son, who lived in town, and his beloved grandchildren. (Field note excerpt July 12, 2018) Carl [her husband] has a brother in Ontario, Greg. He feels very uncomfortable. They [Greg and his wife] came about two, three months ago, and they stayed three or four days…I thought it would be nice to invite Carl’s sister and her partner, and then it could be the three siblings, just for a quiet dinner…And so the conversation at dinner was fine…Carl was not really included very much, conversation-wise. But what really surprised me was, the next morning, when his brother’s wife came down and she says, “Greg is feeling very uncomfortable. He was devastated that Carl did not know who he was when he came.” (Lina, caregiver, American Canadian, interview) So, our close friends have remained our close friends…And I can see that they’ve read a little bit [about dementia] on the Internet. When they approach her [his wife], they do it in a very informed way…When Erica’s disease became manifest, at first, they’d be surprised, because she would pick up the wrong utensil when we were eating. And so, it took a little while for them to realize that that was one of the symptoms. And after dinner, on one of those occasions, one of our old friends said, “I have an idea, Fred. Maybe you should not put out so many utensils because it confuses her.” And I said, “You’re right! That’s a very good idea!” and I just give her one utensil, to make sure. (Fred, caregiver, Jewish, interview) Today, I accompanied the clients of the early stage social group that Michelle had started few weeks ago. It was a beautiful summer day, so everyone went for a walk. I walked with Lawrence. When he was sharing with me an adventurous trip to Florida, somebody called his name. It was a man around his age, who was walking a dog. He greeted Lawrence with affection and talked with him for several minutes. At the end of the conversation, the man apologized for not being in touch with Lawrence for the last couple of years. When the man left, Lawrence told me that he was a “golf friend”. He and his wife used to go to Lawrence’s place for dinner, but when the disease started: “He felt uncomfortable I guess…they stopped coming, they called a couple of times and that’s it! They’re keeping their distance.” (Field note excerpt, July 18, 2018) The only thing I can tell you is that, I believe in my heart – no matter how nice people are, and no matter how they want to understand and help, unless they’re in the situation, they cannot possibly understand what it’s all about. And that’s why the support group at [the organization] was so helpful. Because when you’re in that group, and everybody in that group is in the same situation, when you say something, they know exactly what you’re talking about because they’re living the same thing. (Heidi, caregiver, Jewish, interview)
Culture and social participation
Several participants pointed out that simply spending time with family members and doing activities together was an effective way to include PWDs. This was particularly salient among those of Caribbean and Italian origin as well as some Jews who said that they came from “family-oriented cultures” in which it was engrained to integrate elderly people into the family everyday routines. She actually feels better with us…So, we try to do things, you know? And we do. We include her. We – Italians – are very family-oriented. Like in the summer, she’ll do more stuff with us. Like, I’ll bring her. (Janice, caregiver, Italian, interview) Hubert told us that where he lived there were several Jewish institutions. He used to go to a Jewish senior center and to a Jewish social club where staff members and younger friends “kept [him] busy”. He also liked to go to nearby Jewish stores whose owners he knew and to a supermarket with a big Kosher section. His synagogue was also close. He had to go there few times a week because: “The Rabbi keeps assigning me smalls responsibilities here and there to make sure that I go. His official explanation is that as one of the eldest, I’m already 90! I should share my wisdom with the others. But the truth is that he knows I’m not very religious and wants that I stay socially involved.” (Field note excerpt, September 7, 2018) … And then she was going to another place [an Italian social club] …And then you see the friends and the people that said: “Your mom’s repeating herself.” “Yeah. We know.” …I think she was going there 15 years, every Tuesday. And you know what? I was, at first, gonna say, “You know, do you guys have…?” But then, how do you deal with all the other elderly who don’t understand. And that stigma and the talking. I don’t need her to have extra stress… They wouldn’t have the patience for her. (Janice, caregiver, Italian, interview)
c) Styles of care provision in health and social organizations
PWDs and their caregivers generally access mainstream health and social services, where staff are not always aware of their particular needs. In several of these standardized services, health providers did not have enough time to provide personalized care to PWDs, resulting in misunderstandings and incorrect assessments of their health or social issues/needs. Conversely, health and social organizations that provided personalized care facilitated inclusion. PWDs valued when staff members were “warm”, “close” and “accessible”, knew who they were, and respected their preferences and decisions: [What I like of the organization is] the staff. They are very warm and understanding I just enjoy being here. I’ve been to a couple of other places, I don’t even know the staff. It’s the same program, but it’s boring! It just doesn’t come across. It’s the same drinks you’re having, it’s the same paragraphs that they’re doing, they’re following the same syllabus, but it just, you know… This staff here is very warm, and accommodating, and understanding. And I think each learn and bounce off from the other. I decided to stay here rather than go [to other places]. (Natalie, person with dementia, Jewish, interview)
Culture and styles of health provision
Participants reported that the extent to which health and social services acknowledged the cultural background of the PWD and the caregiver was a major determinant of their experiences with these services. For example, the unwillingness to accommodate the language and to understand cultural referents of the clients and carers led to the inability to access services, and placed severe restrictions on the respite afforded to the caregiver. Lisa is a caregiver of Caribbean origin who speaks only English. She takes care of her two parents with dementia. I have been trying to interview her for several weeks, but she has cancelled our appointments because she could not find a personal support worker to take care of her parents. In a phone conversation, she explained to me why this is so difficult for her: “I lived in Balandier and Balandier is basically French. So, the personal support workers who work here mostly speak French. My father does not understand them. So, when I ask for somebody who speak English, they make me wait and wait…. It is very difficult and many days I have to stay at home taking care of my parents.” When we finally met for the interview, she was upset because a few days ago she had to go to a nearby hospital and some health providers criticized her for not speaking French: “Oh, you’re here for so long. You should…be better skilled in speaking French.” She said that this is not the first time she felt judged in that hospital. In a previous visit, a social worker told her that she should do like most people in Canada and placed their parents in a residence to be able to have a “normal life”. (Field note excerpt February 6, 2018) So, you have to acknowledge [the clients’ culture] and to celebrate it with them. I learned some Yiddish because of that. I mean, also, I love languages. And I find that there is this… they find an importance… or they found a role, somehow, because they’re the teacher and I’m the student. So, there is that empowerment on their part. (Marisol, staff member, Filipino, interview) This morning in the organization, Shirley worked in a separated environment with two of the eldest members of the group, Suzanne and Joan. Shirley said that both speak Yiddish, Hebrew and English, and that in addition Joan speaks French and Suzanna Russian. Then, she introduced the activity: “We’re going to start with a word game. Rossio doesn’t speak neither Yiddish, nor Hebrew, nor Russian and we are going to teach her some words.” Shirley writes in the board “beautiful” and asked them their antonym. “Ugly” replied Joan. Shirley asked Suzanne how did she say “Ugly” in Yiddish: “Mieskiets.” Shirley asked Joy how does she says “Ugly” in Hebrew: “Yafe.” She asked them to translate “Ugly” in French and Russian, and me to translate it in Spanish. She repeated the same exercise with other words: “up”, “short”, “nice”. Then she wrote some words in Yiddish and asked Joan and Suzanne to read them aloud and to explain their meanings to me. I noticed that Joan and Suzanne enjoyed this activity very much. Suddenly, Suzanne whispered in my ear: “When I hear my language, I travel back in time and I feel at home.” (Field note excerpt July 24, 2018)
Discussion
The literature on social inclusion and exclusion of PWDs and their carers have found that families are affected by a multitude of overlapping factors, including: transformations of the personality, abilities and behaviors in persons with dementia (Bartlett, 2007; Daly et al., 2013; Qazi, et al., 2010; Kimura et al., 2015; Meyer et al., 2016); feelings of disconnection, loss and grief (Innes, et al., 2016; Navab et al., 2012; Sanders, Ott, Kelber, & Nohan, 2008; Svanström & Dahlberg, 2004; Kimura et al., 2015); increased responsibilities, high economic burden, scarce free time and social isolation in caregivers (Daly et al., 2013; Rodriguez et al., 2003; Svanström & Dahlberg, 2004; Meyer et al., 2016; Vallée & Vallée, 2017); stigma and lack of understanding from family and friends (Clarke & Bailey, 2016; Daly et al., 2013; Forbes et al., 2011; Duane et al., 2011; Svanström & Dahlberg, 2004; Svanström & Sundler, 2015; Upon & Reed, 2006; Tranvåg et al., 2015; Westwood, 2016); and lack of sensitivity to the needs of PWDs in mainstream services (Clarke & Bailey, 2016; Forbes et al., 2011; Gove et al., 2016; Hare, 2016; Innes & Sherlock, 2004; Innes et al., 2016; Tranvåg et al., 2015; Westwood, 2016; Williams, 2013). Few studies have explored how the linguistic and cultural background of PWDs and their caregivers influence their experiences of social inclusion and exclusion (Hinton & Levkoff, 2000; Kong, et al., 2010; Navab et al., 2012; Dilworth-Anderson, 2004). This study included participants with diverse linguistic and cultural backgrounds and is among the first to explore the intersection of culture and social inclusion and exclusion in a multicultural context. The results challenge us to move beyond dichotomized distinctions between ethnic minority vs. non-ethnic minority views of dementia (Hinton & Levkoff, 2000), living well vs. tragedy discourses about dementia in so-called Western societies (McParland, Kelly, & Innes, 2017), and good vs. bad dementia care (Leibing, 2014; Leibing, 2018) to an approach that acknowledges the multiplicity of culturally-situated experiences associated with the complex nature of dementia.
Our results highlight an emerging counter-narrative to the dominant discourse of the “burden” of dementia care (Upton & Reed, 2006). Although our participants reported overwhelming difficulties and responsibilities associated with caring for PWDs, none considered it as a burden. Italian, Caribbean and Jewish caregivers all described their cultures as “family-oriented” and reported a sense of personal fulfillment for being able to give back to their loved ones. These results contrast with the findings of studies in other family-oriented cultural groups, where tensions arising from the coexistence of traditional filial mandates and modern transformations of family structures (e.g. extended to nuclear, women vs. men caring for the elderly) cause stress and burden for the caregivers (e.g. Kumamoto & Arai, 2004; Kim, 2000; Cacciola, 1982). Despite the fact that most PWDs in this study were cared for by only a few members of their nuclear families (spouses or children living in the parents’ household), it is possible that these caregivers’ extensive use of external resources for dementia care – in particular among Jews – had protected them from experiencing their caregiver role as a burden. The extensive use of formal services for dementia among Jews was also reported by Glicksman (1989), which he attributed to the Jewish culture’s emphasis on the relief of suffering, and absence of an associated ennobling or redemptive value to suffering. Overall, our results about mandates and practices of caregiving are in line with ethnographic studies of caring for PWDs among minority groups in Euro-America (e.g. Hinton & Levkoff, 2000; Lee & Sung, 1997; Lawrence, Murray, Samsi, Banerjee, 2008; Ortiz, Simmons, & Hinton, 1999) and in societies outside Euro-America (e.g. Brijnath, 2014; Cohen, 1998; Leibing, 2018). These observations are not intended to idealistically portray certain “ethnic” or “cultural” forms of caregiving as good dementia care by contrasting them with others in which caregiving is perceived as a burden. Following Annette Leibing’s suggestions (2018), we instead aim to contribute to a discussion leading to more nuanced and diverse accounts of dementia care.
In addition, our results suggest diverse and contrasting experiences of social inclusion and exclusion between cultural communities. On the one hand, participants of Jewish origin reported having access to a comprehensive network of social and health institutions that they consider socially inclusive. Certain ethical principles and beliefs prevalent in the Jewish community (e.g. the value of all people despite cognitive impairment due to the presence of a soul, the mandate of honoring the old and respecting their role in Jewish community, and the responsibility of people to care for each other as an extension of God’s mercy) support a more positive view about PWDs, and consequently, a more inclusive environment. On the other hand, Italian and Caribbean carers stated that stigma towards and lack of understanding of dementia were common in their cultural communities, creating tensions against the ingrained mandate of caring for the elderly and the expectation of inclusion. Although several studies explored how ethnic and cultural perceptions of dementia affect caregiving, help-seeking and service use (e.g. Bowes & Wilkinson, 2003; Braun, Takamura, & Mougeot, 1996; Jett, 2006; Ortiz & Fitten, 2000), further research is needed to elucidate the role that culture plays in the social inclusion/exclusion of PWDs and their carers within their own cultural/ethnic communities.
Our multiple perspectives approach allowed us to identify moments, situations and practices in which meanings assigned by one member of the carer-care receiver dyad overlapped or differed from the other. Notable amongst these moments were those experienced as inclusive by one member of the dyad, and as exclusive by the other. For example, a participant reported that “too much inclusion” of her husband with dementia might not be good because it contributed to her social “exclusion” (e.g. no free time for activities or socializing). In an informal conversation, her husband said that he liked when she went out to do “other things”, but after a while he felt anxious because he tended to forget why she was not at home with him. We consider this an example of exclusive inclusion 5 – an inclusion that allows the integration of one person by excluding the other one. We encourage future studies using a multiple perspectives approach, which can shed light on situations of exclusive inclusion and contribute to the growing field of interventions that aim to foster social inclusion for the diverse actors involved in dementia care (e.g. Camic, Tischler, & Pearman, 2014; Harris & Caporella, 2014; Fortune & McKeown, 2016; Marsh, Courtney-Pratt, & Campbella, 2018). In addition, incorporating the perspective of the organization’s staff members allowed us to identify the value of using the language and cultural referents of the clients to foster social inclusion. This is a field of intervention that, to our knowledge, has not been researched yet and that could effectively contribute to the social inclusion of PWDs.
One of the main strengths of our study was the use of ethnographic fieldwork, participant observation and informal interviews to include the perspectives of PWDs in the research. While studies about social inclusion and exclusion of PWDs abound, few include the perspectives of PWDs themselves (Bartlett, 2007; Clarke & Bailey, 2016; Duane et al., 2011; Forbes et al., 2011; Innes & Sherlock, 2004; Innes et al., 2016; Marsh et al., 2018; Qazi, et al., 2010; Svanström & Dahlberg, 2004; Svanström & Sundler, 2015; Tranvåg et al., 2015; Wilkie, 2012, Westwood, 2016). In line with other authors (e.g. Lloyd et al., 2006; O’Connor et al., 2007; Smebye et al., 2012; Svanström & Sundler, 2015; Wilkinson, 2002), we believe that it is essential to involve PWDs in this research and, consequently, to use suitable approaches and methods to capture their experiences. Our approach de-centralized the role of verbal communication to reduce the barriers to participation, which was particularly appropriate for this endeavor. Anthropological research has enormous potential to vividly capture the experiences of PWDs (e.g. Brijnath, 2014; Chatterji, 1998; McLean, 2007; Kontos, 2006; Leibing, 2017; Taylor, 2008), and can be used as a tool to make research more inclusive to these individuals (Bartlett, 2007; Forbes et al., 2011).
This study had several limitations. Our results represent specific experiences of PWDs, caregivers and staff members. While their generalizability to other individuals or cultural groups is limited, we provide a detailed description of the research context to enable an appraisal of the transferability of our findings to similar contexts. Our research was based on ethnographic methods that helped forge personal relationships with the participants; as such, social desirability could have been induced. However, the primary anthropologist cultivated non-judgmental attitudes while conducting research, which helped to control this potential bias. Although most research participants identified themselves as immigrants and belonging to specific cultural groups, they spent most or all their lives in Canada and sometimes were not as clear about the cultural values that articulate their practices as, for example, newly arrived immigrants might be. However, participant observation allowed us to identify how these implicit cultural values influenced how they experienced social inclusion and exclusion.
Conclusion
In our ethnographic study of PWDs and their carers conducted in a non-profit organization in a multicultural neighborhood of a bilingual Canadian city, participants identified three major factors that influenced their experiences of social inclusion and exclusion: transformation of the PWD and the caregiver; participation in social networks and meaningful relations; and styles of care provision in health and social services. The cultural background of the participants fundamentally influenced their experiences of inclusion and exclusion across all three areas. In some instances, certain cultural mandates that prescribe practices of intergenerational care shape the way caregivers perceive caring for their loved ones and mitigated experiences of exclusion. In others, cultural communities contributed to increase either their inclusion due to a less negative perception about dementia and a network of institutions or their exclusion due to the lack of understanding toward and stigma associated with dementia. The deliberate use of cultural elements and language is an effective strategy for fostering social inclusion of PWDs. Our findings also highlight the value of ethnographic methods to include the perspective of PWDs, who is still underrepresented in dementia research.
Supplemental Material
sj-pdf-1-tps-10.1177_13634615211001707 - Supplemental material for “When I hear my language, I travel back in time and I feel at home”: Intersections of culture with social inclusion and exclusion of persons with dementia and their caregivers
Supplemental material, sj-pdf-1-tps-10.1177_13634615211001707 for “When I hear my language, I travel back in time and I feel at home”: Intersections of culture with social inclusion and exclusion of persons with dementia and their caregivers by Rossio Motta-Ochoa, Paola Bresba, Jason Da Silva Castanheira, Chelsey Lai Kwan, Shaindl Shaffer, Omega Julien, Meghan William and Stefanie Blain-Moraes: for the DNA Lacunar 2 investigators in Transcultural Psychiatry
Supplemental Material
sj-pdf-2-tps-10.1177_13634615211001707 - Supplemental material for “When I hear my language, I travel back in time and I feel at home”: Intersections of culture with social inclusion and exclusion of persons with dementia and their caregivers
Supplemental material, sj-pdf-2-tps-10.1177_13634615211001707 for “When I hear my language, I travel back in time and I feel at home”: Intersections of culture with social inclusion and exclusion of persons with dementia and their caregivers by Rossio Motta-Ochoa, Paola Bresba, Jason Da Silva Castanheira, Chelsey Lai Kwan, Shaindl Shaffer, Omega Julien, Meghan William and Stefanie Blain-Moraes: for the DNA Lacunar 2 investigators in Transcultural Psychiatry
Supplemental Material
sj-pdf-3-tps-10.1177_13634615211001707 - Supplemental material for “When I hear my language, I travel back in time and I feel at home”: Intersections of culture with social inclusion and exclusion of persons with dementia and their caregivers
Supplemental material, sj-pdf-3-tps-10.1177_13634615211001707 for “When I hear my language, I travel back in time and I feel at home”: Intersections of culture with social inclusion and exclusion of persons with dementia and their caregivers by Rossio Motta-Ochoa, Paola Bresba, Jason Da Silva Castanheira, Chelsey Lai Kwan, Shaindl Shaffer, Omega Julien, Meghan William and Stefanie Blain-Moraes: for the DNA Lacunar 2 investigators in Transcultural Psychiatry
Footnotes
Acknowledgements
This study was supported by the CIHR operating grant “Moving With and Tuning In: A participatory mixed methods study to foster social inclusion of individuals with dementia and their carers” (CIHR-SII-150704) and the Alzheimer Society of Canada (Grant #17C). We thank Melissa Park, for her contribution to the design of this project and her participation in data analysis. We extend our acknowledgements to our institutional and community-based partners, to Keven Lee for his participation in data analysis and his feedback on this paper, to Yasmin Lalani for coordinating this research and contributing to data analysis and to Alonso Gamarra for his comments on this paper as well as to the research participants without whom this study would not be possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.