
Abstract
Culture and socialization influence how individuals perceive and express emotional distress. Research therefore, must consider the context to capture individual experiences. However, the majority of studies on factors associated with emotional distress among migrants use quantitative approaches, limiting an in-depth understanding. This study investigates emic themes of emotional distress among Vietnamese migrants by integrating anthropological and psychiatric approaches. The mixed methods study first quantified differences in reported themes of distress between Vietnamese (n = 104) and German (n = 104) patients, who utilized two psychiatric outpatient clinics in Berlin, Germany. Based on these differences, ethnographic interviews were conducted with 20 Vietnamese patients. In the quantitative part, differences in frequency of reported distress between Vietnamese and German patients indicate cultural and migration-related issues among Vietnamese migrants, such as the upbringing of children in a transcultural context. In the qualitative part, interviews with Vietnamese patients elicited contextualizing information and additional themes of distress. Besides commonly expressed socioeconomic themes, such as work and finances, we identified affectively charged themes concerning roles toward partnership and children. A central emic theme is expressed as “moments of speechlessness,” which go beyond a lack of language proficiency and challenge patients in different spheres of life. Migration entails complex affective dynamics, determined by a specific migratory and post-migratory context. Within this context, norms and values determine which themes of distress patients articulate openly. Therefore, an interdisciplinary, mixed-methods approach can yield a contextualized understanding of emotional distress and the complex nature of migration.
Keywords
Introduction
Ongoing processes of global migration require that local mental health institutions provide adequately tailored treatment for changing populations of migrants. In 2015 alone, about 2.1 million people migrated to Germany (Federal Office of Statistics of Germany, 2018a). A significant body of research shows that only a fraction of migrants in need use existing mental health services (Abebe et al., 2017; Kirmayer et al., 2011; Ta et al., 2015). Numerous factors influence access to mental health institutions, including language barriers, gender, level of acculturation, perceived stigmatization, insufficient knowledge about services, and different concepts of illness and treatment (Augsberger et al., 2015; Lauber & Rössler, 2007). Thus, a deeper understanding of migrants’ needs and difficulties and their heterogeneous experiences is necessary. In this article, we pursue this by investigating a population of Vietnamese psychiatric outpatients living in Germany, using an interdisciplinary, mixed-methods approach.
Cultural impact and emotional distress
We consider culture as intrinsically dynamic and malleable (von Poser, Lanca, Heyken et al., 2017). Rather than being defined by clear-cut boundaries, ethnicity, or nationality, we view culture as a process of meaning-making and as a basis for collective and societal cohesion and belonging (Pfaff-Czarnecka, 2013). Culture thus relates to shared knowledge, practices, frameworks, and conventions and allows for identification and legibility within a group. Culture is acquired and (re)shaped in lifelong processes of learning and impacts perceptions and embodiments along with discourses and emotions.
Culture influences how individuals perceive and express their emotional distress (Kirmayer, 1989; Kirmayer & Young, 1998). For example, East and Southeast Asian patients with mental health problems tend to present clinically with somatic symptoms that are more socially accepted, such as pain or dizziness, rather than with emotional symptoms, such as sadness or hopelessness (Kleinman, 1988; Ryder et al., 2008). However, if asked directly, they acknowledge emotional symptoms at a similar rate as patients from Western societies (Dreher et al., 2017; Keyes & Ryff, 2003). Moreover, reactions to distress vary across cultures. For example, Vietnamese patients may present a culturally specific response to traumatic events described as orthostatic panic, with sensations of dizziness and palpitations when they stand up (Hinton et al., 2007). Understanding cultural notions of illness and distress can help to promote effective mental health care services, especially among minority populations with different cultural backgrounds.
Migration-related stressors and distress
Previous research has identified a number of migration-related stressors or factors associated with emotional distress, such as migration regimes, trauma during migration, legal status, and language proficiency (Jurado et al., 2017; Salvo & Williams, 2017; Wolf et al., 2017). However, symptoms of mental illness can pose an additional obstacle to acquiring language skills or to obtaining legal status (Eamer et al., 2017). Although most migrants hope to improve their lives, some experience losses at various levels, such as their socioeconomic status, social (support) network, or close family ties, and they are often confronted with some forms of discrimination (Chou, 2012; Pantelidou & Craig, 2006). Furthermore, migrants have to continually navigate between different cultural contexts and emotional orientations (Boccagni & Baldassar, 2015; Röttger-Rössler, 2016). Such navigations may entail stressful experiences, especially when cultural norms conflict with each other (Ta et al., 2017).
Etic vs. emic perspectives
Current psychiatric and psychological knowledge about factors associated with migrants’ emotional distress stems mainly from quantitative research, which aims to formulate generalizable statistical descriptions about larger populations. However, such approaches rarely target patients’ individual experiences and their heterogeneous affective lives (von Poser, 2018). Furthermore, the majority of studies on migrants’ mental health are based on current diagnostic classification systems (e.g., DSM-5, ICD-10) and a nosology primarily developed from studies in Western, educated, industrialized, rich, democratic (WEIRD) contexts (Henrich et al., 2010).
Social sciences label approaches that are embedded in the researchers’ viewpoint as etic perspectives. While etic constructs are potentially transferrable, reliable, and generalizable, they are not designed to capture emic knowledge, that is, knowledge situated in the cultural and subjective life contexts of the affected research participants. Emic knowledge encompasses culturally shaped notions, individual views, or interpretations that form perceived realities. Therefore, an inductive, qualitative research design that targets the patients’ emic perspectives can reveal distress related to individual experiences of migration.
Interdisciplinarity
Recognition of the relevance of culture and context for mental health has led to collaborations between anthropologists and psychiatrists with a joint interest in theoretical and methodological questions (Heyken et al., 2019; Kleinman, 2001). In general, anthropologists draw on qualitative ethnographic approaches to understand local contexts and peoples’ different responses to crises. One example for the strengths of combining psychiatric and anthropological methods is a study by Mendenhall et al. (2016), who used the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), a commonly used standardized assessment in mental health care, to complement and interpret ethnographic interviews. The study aimed to investigate the meaning of psychological distress by analyzing the symptomatology. The authors concluded that incorporating standardized mental health assessments into clinical anthropology facilitates the process of researchers drawing conclusions from smaller data sets, such as ethnographies, and also increases the robustness of the interpretation of results.
Mixed-methods designs can add to the benefits of qualitative and quantitative research by integrating different kinds of data. Several studies have demonstrated the validity of such approaches in research on culture, society, and mental health (Doucerain et al., 2016; Groleau et al., 2007). Terpe (2015) suggests combining data and methods in the process of methodological triangulation, in which qualitative data is quantified, allowing researchers to relate and to complement qualitative outcomes with quantitative data—and vice versa. Such interdisciplinary mixed methods approaches can balance the need for generalizability and sensitivity for specific emic perspectives when investigating migrants’ emotional distress, even in smaller samples.
Vietnamese cultural contexts
According to the Federal Office of Statistics of Germany, (2018b),roughly 185,000 people of Vietnamese heritage lived in Germany, making them the largest Southeast Asian migrant population. Nevertheless, little research has been conducted in this population to date. Various philosophical and religious influences shape Vietnam’s cultural and social life (Nguyen, 2016; Vuong et al., 2018). Confucian principles emphasize social order, respect for authority, and filial piety (hiếu thảo), e.g., respecting one’s parents and the elderly. Taoism and its striving for thrift, humility, compassion, and harmony have also strongly influenced Vietnam. Additionally, over 70% of Vietnamese identify as Buddhists, and a minority is either exclusively or syncretistically Christian. Most Vietnamese persons practice some form of ancestor worship (thờ cúng tổ tiên), which reflects the importance of the family unit. In this frame of reference, sociocentrism is usually valued more highly than individualism, with corresponding moral norms and role expectations (Kim, 2014).
This background is palpable in the everyday experiences of cultural difference for overseas Vietnamese persons (Việt Kiều); worldwide, their population amounts to roughly three million. Migration motives have been shaped by Vietnam’s more recent history of decolonization—35 years of consecutive wars, and socioeconomic hardships. While Vietnamese populations in the United States and Western Europe consist mainly of refugees from after 1975, others migrated to Europe as students in the context of French colonial rule from 1883 to 1954. In Eastern Europe, a large number of Vietnamese arrived before 1989 through international socialist cooperation, e.g., as students or labor migrants. Apart from that, migration continues for various reasons, causing a unique diversity of migration biographies (GIZ, 2016).
The Department of Psychiatry and Psychotherapy at Charité – Universitätsmedizin Berlin, Campus Benjamin Franklin (CBF), has acknowledged cultural variations in symptom presentation and the demand for cross-cultural openness in mental health care services, and opened Germany’s first specialized outpatient clinic for Vietnamese migrants in 2010. This outpatient clinic offers culturally sensitive psychiatric and psychotherapeutic treatment in the Vietnamese language, especially for patients who refrain from seeking out mental health care elsewhere due to their language barrier. In cooperation with this initiative, a second outpatient clinic dedicated to Vietnamese migrant patients opened in 2012 in the psychiatric department of a large general hospital, Evangelical Hospital Queen Elisabeth Herzberge (KEH), in Berlin. These clinics provide the setting for this study.
Objectives
This study aimed to investigate emic themes of distress among Vietnamese psychiatric outpatients. In the first part of this mixed-methods study, we explored quantitative differences in reported distress between Vietnamese and German outpatients. We contrasted both groups in order to gain an initial point of reference to identify possible experiences of cultural and migration-related distress in the community of Vietnamese migrant patients living in Berlin. In the second, qualitative part of our study, we used semi-structured ethnographic interviews with Vietnamese patients to contextualize, broaden, and increase the external validity of the quantitative analyses. The study also sought to demonstrate the synergetic benefits of interdisciplinary work among psychiatrists, psychologists, and anthropologists and to show how ethnographic interviews can contextualize patients’ reports and reveal new emic themes of emotional distress that are relevant for clinicians.
Methods
Recruitment
Patients were recruited from a psychiatric-psychotherapeutic outpatient clinic specialized in the care of Vietnamese migrants at the Department of Psychiatry and Psychotherapy, Charité – Universitätsmedizin Berlin, CBF, in Germany, and from the outpatient clinic of the Department of Psychiatry and Psychotherapy at KEH in Berlin.
All patient-related quantitative data was collected between 2013 and 2016. All participants were born and socialized in Vietnam and sought culturally sensitive counseling and psychiatric or psychotherapeutic treatment in the Vietnamese language. All patients in the present study initially met the ICD-10 criteria either for depressive episodes, anxiety disorders, or adjustment disorders diagnosed by a board-certified psychiatrist in Vietnamese. Patients with acute psychosis, acute suicidality, a neurodegenerative disorder, severe PTSD, or a comorbid substance-related disorder did not participate in the study. Ethical approval of this study was obtained from the ethical committee at the Charité – Universitätsmedizin, Berlin. All patients gave informed, written consent that collected data would be anonymized and used for research and scientific publication purposes only. This study uses a cross-sectional design. Before the first consultation and treatment, all patients were asked to complete a structured survey. This survey included questionnaires assessing socio-demographic information, clinical psychiatric evaluation, and psychometric scales such as the Patient Health Questionnaire (PHQ; Spitzer et al., 2000). Vietnamese patients were asked to fill out surveys in the Vietnamese language (Dreher et al., 2017; Ta et al., 2015).
In the first part of the study, the sample consisted of 104 Vietnamese and 104 German outpatients. The German sample was selected to match the Vietnamese patients’ demographic characteristics, considering age, sex, education, and diagnosis. In the second part of the study, a new sample of 20 Vietnamese patients was selected and individually interviewed. Patients were included in the qualitative study if they were first-generation Vietnamese migrants (i.e., born and socialized in Vietnam) and met all the criteria for the quantitative study as described above. Moreover, the sample was chosen to capture the range of demographic variation on age, sex, and length of stay in the larger sample.
Measures
Patient Health Questionnaire (PHQ)
The PHQ (Spitzer et al., 2000) is a self-report questionnaire, which is widely used in primary care to screen for mental disorders based on diagnostic criteria from the DSM-IV. The central question for our study was one item asking: “What currently burdens you the most?” (German: Was belastet Sie zur Zeit am Meisten?; Vietnamese: Điều gì làm anh/chị bận tâm nhất hiện nay?). The survey was translated from German into Vietnamese using a four-step back-translation approach (e.g., Beaton et al., 2000).At first, a native Vietnamese psychiatrist translated it into Vietnamese. Then, a state-certified Vietnamese translator back-translated the Vietnamese draft version to German. Afterward, the original survey was compared with the back-translated German versions and was edited to address resulting issues. Based on the corrected back-translation, a final Vietnamese translation was agreed upon by both translators.
Emotional Distress Interview
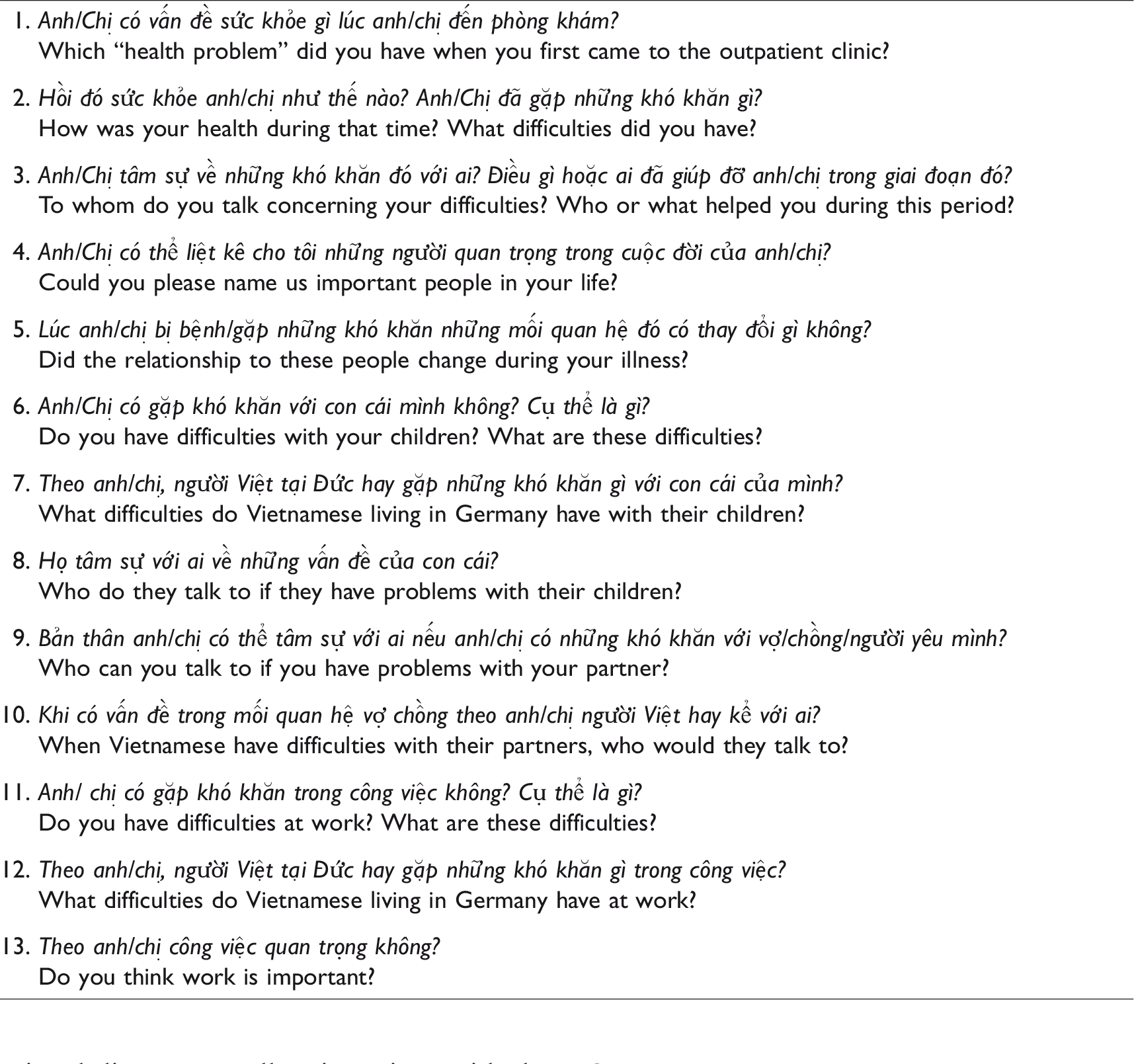
Based on the quantitative results on the relative frequency of reported distress in Vietnamese and German patients, relevant themes for the Emotional Distress Interview (Table 1) were chosen. We considered themes to be relevant if there were (1) statistically significant differences in frequencies between the two groups, indicating possible themes related to special experiences and/or to the migration experience of Vietnamese patients; or (2) overall high frequencies within the group’s responses. This selection and the subsequent phrasing of the semi-structured interview were discussed by an interdisciplinary team 1 that had extensive research experience with Vietnamese migrants in Germany. We applied the method of person-centered ethnography, addressing interviewees as both informants and respondents (Hollan, 2001), to generate a detailed narrative of patients’ phenomenological experiences and understandings of their reported emotional distress. The interviews were conducted by the first authors of this article in 2017 at the outpatient clinic at Charité –Universitätsmedizin in Vietnamese language and lasted approximately two hours.
Emotional distress interview in Vietnamese and English.
Data analyses
Quantitative analysis
Statistical analyses were conducted with IBM SPSS Statistics for Mac OS X, Version 22. Demographic group differences regarding continuous variables (age) were analyzed with t-tests. Differences regarding ordinal variables (sex, education) were tested with chi-square tests and Mann-Whitney U tests. If cell size was < 5, Fisher’s exact test was used instead of the Chi-square test because of its sensitivity to sample size. Patients’ answers on their emotional distress and the generated codes were quantified by rating the codes as present (1) vs. absent (0). Chi-square tests were conducted to explore differences in the frequency of reported themes of distress between Vietnamese and German patients.
Qualitative analysis
Qualitative data was analyzed using MAXQDA 11 for Mac OS X. Patients’ answers on their emotional distress as well as interviews with the Vietnamese patients were analyzed by applying qualitative content analysis (e.g. Hsieh & Shannon, 2005). Next, a coding scheme for patients’ answers to the open question in the survey was developed. Answers were then separately coded; any differences were resolved in interdisciplinary discussions. Afterward, codes were quantified and statistically analyzed. Based on these results, a semi-structured interview was developed, and n = 20 Vietnamese patients were interviewed. Further themes of distress beyond these categories were identified and clustered, generating new categories.
Results
Participants characteristics
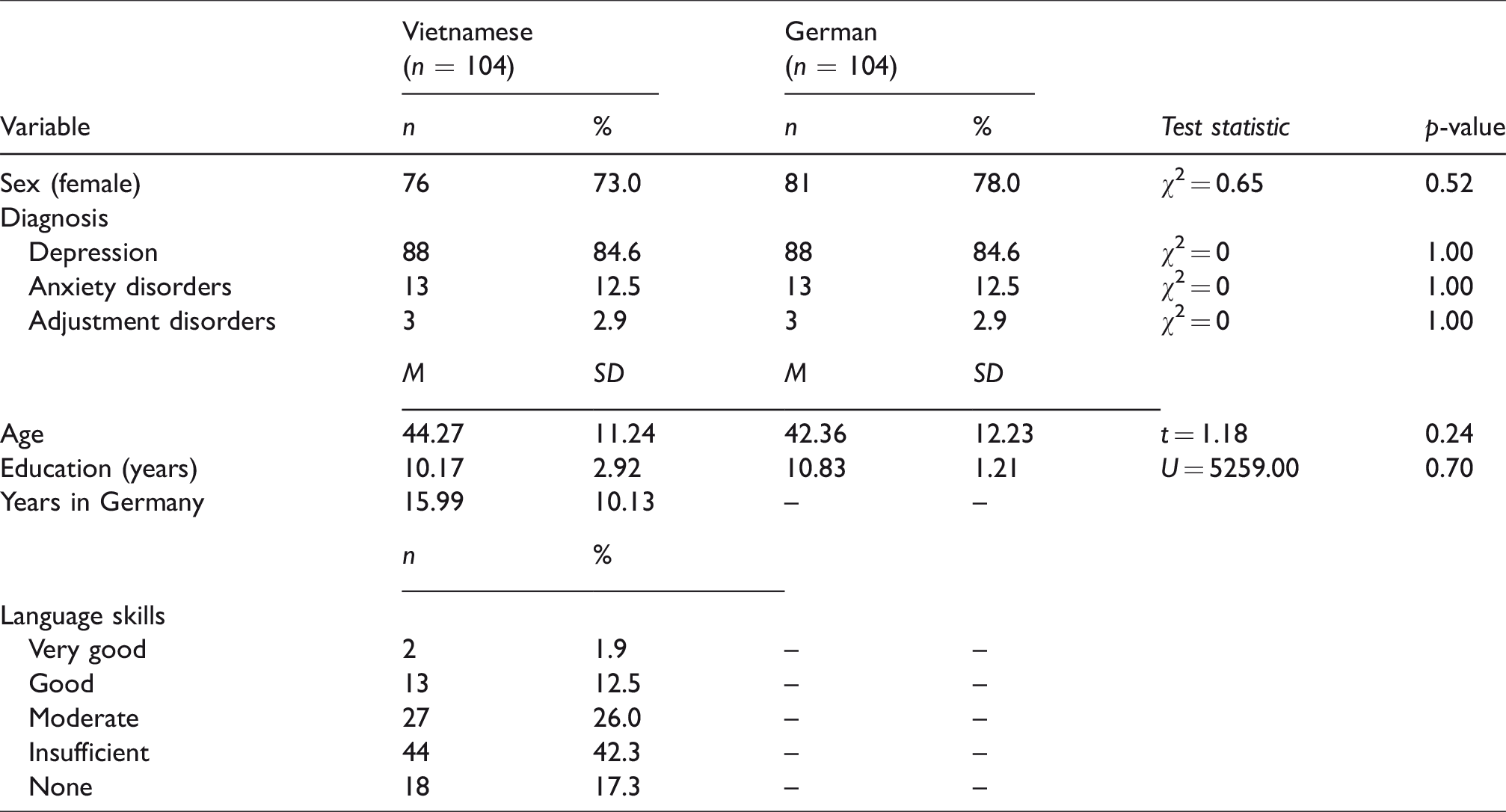
The final sample consisted of n = 104 German patients and n = 104 Vietnamese outpatients. Descriptive statistics of both samples and statistics testing group differences are presented in Table 2.
Comparison of sociodemographic and diagnostic characteristics of Vietnamese and German groups.
Quantitative results
In the survey, Vietnamese patients reported more concerns regarding their health or illness compared to German patients, p < .01. Vietnamese patients also reported worries about their children more frequently compared to German patients, p < .05. However, German patients reported psychological issues to be more burdensome compared to Vietnamese patients, p < .01. Psychological issues comprised worries about stress, the mind, and depression. German patients also reported more burdens involving their partners, p < .01 (see Table 3).
Comparison of themes from the survey by ethnicity.
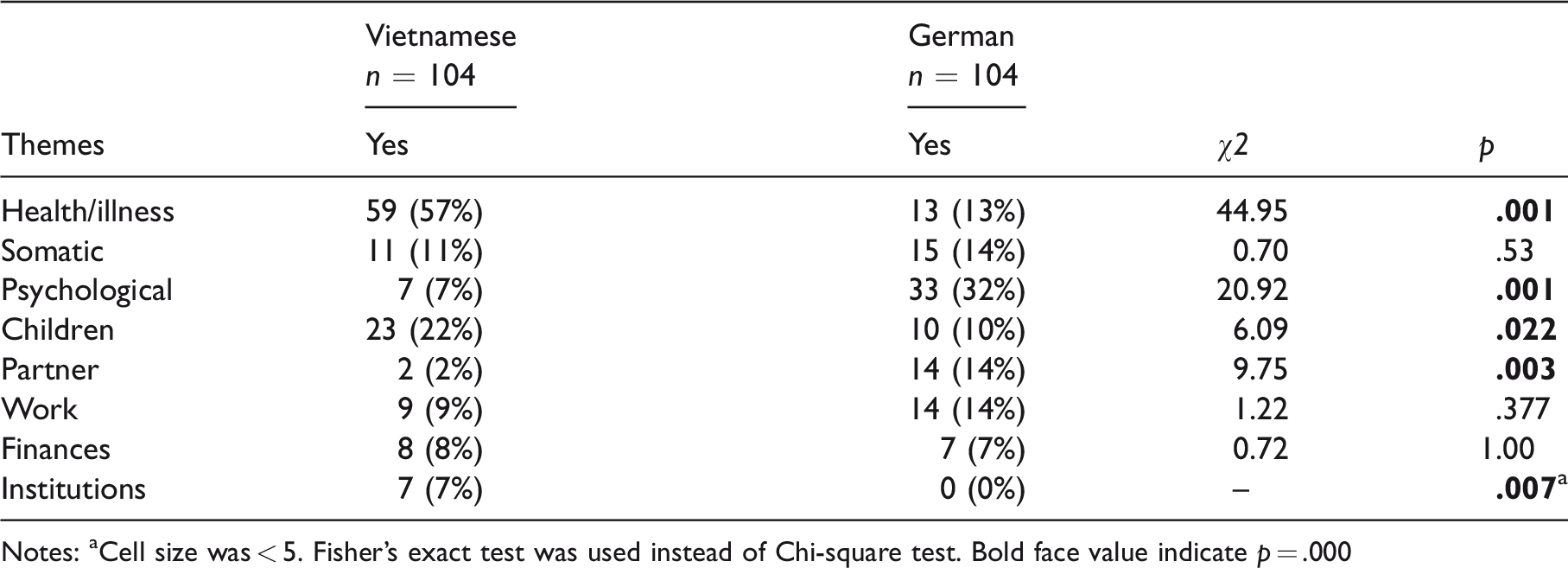
Notes: aCell size was < 5. Fisher’s exact test was used instead of Chi-square test. Bold face value indicate p = .000
Qualitative results
In total, 11 themes emerged from Vietnamese patients’ interview narratives. Six themes that were previously found in the quantitative survey responses were also found in the subsequent interviews (work (n = 18), children (18), partnership (18), psychological (17) and somatic symptoms (18), finances (16), institutions (14)). In addition, five new themes of distress emerged from the in-depth interviews (past (n = 16), future (15), speechlessness (15), isolation (11), language (11)). In the following, these themes will be described and illustrated with quotes from a patient. First, we present themes that were identified in the survey responses and elaborated in the semi-structured interviews (Themes 1.1–1.6). Second, we present new themes that were unmentioned in the survey, but which emerged as relevant during the interviews (Themes 2.1–2.5).
1.1 Work
The majority of patients considered their work to be burdensome due to physical exhaustion, long working hours, and the pressure to perform well. Almost all patients reported that they had maintained an intense work-related level of stress for several years without taking a break, while taking care of their local family and kin overseas. Struggles with an unresolved residence status were also addressed as distress and related to their illness, eventually leading some of them to quit their work. The following quotes summarize common responses: I worked so much back in Vietnam and here. I sold flowers, owned a restaurant. And then it [the illness] happened. It was too much pressure; I had to hire people, file the paperwork, I had to organize everything until I was overworked. (Mr. U., 53) They [the Vietnamese] are carried away by their work. They work so much in order to make money and are totally immersed. They work from dawn till dusk. Once I talked to a doctor; she said that Vietnamese only go to treatment when it’s almost too late. Vietnamese don’t have a vacation. (Mr. A., 54)
1.2. Children
The second most often mentioned theme of distress referred to children. Patients worried about the “right parenting” of their children. They experienced a clash between parenting beliefs and practices prevalent in Germany and their own upbringing in Vietnam. Vietnamese parents wanted their children to be autonomous and integrated into German society, or even considered their children to be German-Vietnamese (Việt-Đức). Meanwhile, their own parenting style was strongly influenced by Vietnamese cultural values: I find it difficult. The two cultures. We want the Vietnamese upbringing as a benchmark, but we have to adopt the German culture. For example, they want to have a partner too soon. I wanted to forbid it. (…) But when you forbid it, it’s also not working. (Mrs. B., 51) The Vietnamese [first generation] press Vietnamese upbringing methods on their children. But the children, who live here, they live like Germans. It’s difficult to change their thinking. They don’t understand a lot of Vietnamese, but a lot of German. (…) Back then I had to play at home, but nowadays the children here go out in cafes, put make-up on, or have boyfriends at 14or 15. I’m afraid my children will turn out like that. (Mrs. I., 32)
Moreover, the elder generation of Vietnamese patients complained that their children did not support them sufficiently in chores, such as filing paperwork or translating at doctors’ appointments. Patients were often disappointed, because their expectations were not fulfilled by their children: “I’m sad when I can’t ask them a favor. For example, translating. It’s just a small favor, but they won’t do it. Every time I’m sick I ask them, but they never come along” (Mrs. P., 60).
1.3. Partnership
In contrast to the quantitative results, which showed that Vietnamese patients did not report partnership problems, the interviews revealed numerous difficulties with partners. Among the listed burdens, the majority of female patients reported longtime domestic violence in relationships with Vietnamese or German men. Moreover, female patients reported distress because they did not get enough support from their partners in household tasks, especially during pregnancy and the postpartum period. Patients also said that it was especially burdensome to suppress all difficulties in social encounters instead of addressing them with others, in order to adhere to the norm of social harmony to “save face” (thể diện): “My husband took all my money. He beat me. Back in Vietnam my husband also beat me. I was very scared” (Ms. X., 48); “I just wanted to be healthy and wanted to work. (…) Here [in Germany] I had a beating husband and I had to call the police. (…) Now I’m just scared that he’ll find me” (Mrs. V., 57); “They’re afraid the man will lose face. They [Vietnamese women] are afraid that their happiness will break; that’s why they swallow everything” (Mrs. V., 57); He always said “bye” and went away with his friends. I was alone, pregnant. I told him to stay at home and to help, but he always went away with his friends. (…) He was gone every day and I was alone with the baby, had to run errands all by myself with the baby. Or when the baby was sick … I had to go alone to the doctor. I was very sad because of my husband. (Mrs. H., 44)
1.4. Psychological and somatic symptoms
A theme that emerged repeatedly in the interviews was the impact of psychological or somatic symptoms, which occupied and burdened patients’ daily lives. Psychologically, patients named the core symptoms of depression; for instance, feelings of sadness, hopelessness, and experiencing little interest or pleasure. Moreover, patients reported fear, stress, and worries and used the Vietnamese term for depression (trầm cảm): “I don’t feel any joy. That is why I have this trầm cảm” (Mr. U., 53); “I just want to disappear, I am so hopeless. When I go out, I don’t feel joy. Outside, I’m just scared” (Mrs. V., 57).
Furthermore, patients listed numerous somatic complaints, such as weak nerves, pain all over the body, and trouble sleeping: “I feel a lot of tension. It’s like something with my nerves. I often fight with others and I’m aggressive. My nerves are too weak and I just wanted to break everything” (Mr. U., 53); “I couldn’t sleep and had pain all over the body. The right side of my body was in pain. It feels like little crabs bite my body. And my head hurts brutally” (Mrs. L., 54).
1.5. Finances
Patients named financial burdens, such as the discrepancy between their longing for wealth and their inability to achieve this goal due to health problems. Moreover, for those depending on welfare, limited income was also experienced as burdensome. In addition to this limitation, some patients still have to support their family in Vietnam financially: “My husband and I worked a lot. I worked in kindergarten and he was a cook. But then he sent all the money to Vietnam to support the family. And I didn’t have any control” (Mrs. B., 51); In the past, I also wanted to be wealthy. But I couldn’t do it. I think everyone wants to be wealthy. When one has enough money, one can buy things, food – whatever you want. I receive €300 per month, and I have to buy a ticket for public transportation and food for the family. It’s not a lot. (Mrs. R., 49)
1.6. Institutions
Patients repeatedly reported the pressure of government authorities and the formalized bureaucracy in these institutions as a major source of distress. They often felt pressured and humiliated by pending decisions regarding residency titles and employment permits, by child protective services, or by obligations to the federal employment agency “Jobcenter,” which administers unemployment benefits. The following quotes outline the dense network of institutions about which the patients are concerned: I do not want to depend on the Jobcenter. One has to be independent, to receive a permit of residency from the department of foreigners, in order to have work. One has to be diligent, to have less stress, and not to think too much. (Ms. I., 32) You have to file all the paperwork. They always ask you, every two weeks you have an appointment, only because you receive a couple of Euros. Good Lord, they make me crazy! They make my head explode. It’s like you’re homeless. If I had the strength, I would work. Life like this … it isn’t quiet.(Mrs. T., 47) Child protective services didn’t allow me to see my children. I didn’t know where they were, and I didn’t see them for six months. I felt like I lost my children and I was so scared and thought that I’m going crazy. At home, it was so cold because my children were not there. (Mrs. X., 48)
2.1 Past
One of the new emerging themes was the impact of the past and the strategy of not thinking too much about the past. Patients report having had burdensome and traumatic experiences in the past, such as war or violence. They urgently avoid thinking about the past to avoid physical pain or additional psychological stress: “One tries not to talk about the past. It’s not useful” (Mr. U., 53); “Of course I sometimes think about the past. But I think it’s not useful. It just hurts you, and it’s a waste of time. I always tell myself: I don’t think about it” (Mr. E., 58).
However, memories of the past cannot always be suppressed, which our patients experience as very burdensome: “From time to time I think about the past. I cannot forget it. Especially, when I’m alone, the past comes back and I cannot throw it away” (Ms. B., 51).
2.2. Future
Concerning the future, reports of patients were ambivalent. Some stated that they felt pressured into thinking about the future and tried to avoid thinking about it, which is comparable to the avoidance of the past: I think it’s better not to think about the future. It’s not too late to paint a picture of the future. I used to sit around and paint my future. But the reality is different. That’s why one shouldn’t think about it. (Mrs. L., 54). You cannot avoid thinking about the future. You have to make an effort for the future. And if you know that, you just have to find a way for yourself. When I think about the future, I always tell myself that my health is the most important thing.(Mr. A., 54)
2.3. Speechlessness
Another burdensome theme that was reported in interviews was a state that we labeled as “speechlessness.” Speechlessness was mentioned in different domains, mostly expressed in terms such as “difficult to say” (khó nói) or “not being able to speak” (không nói được). It encompassed the difficulty in articulating certain experiences, norms against explicit mention of painful events, and the absence of a trusted person to confide in. Patients mentioned mistrust and fear that people would circulate their personal stories around the Vietnamese community: “I don’t have anyone to talk to. My husband is dead and my daughter works from the morning until the evening. I have to solve my difficulties by myself. I don’t want to burden her” (Mrs. L., 54); The Vietnamese … I used to tell something about myself, about my family, but very often they told it to other people. Once I made her promise not to tell it to anyone … but afterwards, she talked about everything to others. (Mrs. H., 44)
Speechlessness was also reported between parents and children due to language difficulties: The children don’t speak Vietnamese. It’s difficult to convey one’s affection. That’s why I have to show my affection through actions; for instance, I stroke their backs. And then they ask me whether I can stroke their back again. (Ms. X., 48) I mostly talk to my friends here. Only here are they able to understand reality. I am scared to talk about my situation, that I have a boyfriend here. In Vietnam, I would have to marry. Abroad they don’t understand this. (Ms. X., 48)
2.4 Isolation
Vietnamese patients also reported feelings of marginalization and isolation, and limited contact with other people. Their social withdrawal was a symptom of the depression, but mental illness also reinforced social withdrawal tendencies: “Because of the illness, I don’t have any contact with people anymore” (Mrs. L., 54); “No one understands how ill I am. No one understands us [depressive patients]. I act as if I’m fresh from the outside, but inside I’m dead. I can’t meet people” (Mrs. T., 47); “I live alone and I am sad. But if I had to go back to Vietnam, I would be sad as well. I cannot find friends; that’s why I have this depression” (Mr. U., 53).
2.5. Language
Finally, patients also addressed language difficulties as a heavy burden. Patients often felt guilty and ashamed of their limited ability to speak the German language: “The difficulty the Vietnamese have is that they cannot speak the language. And if you don’t understand it, you have to ask others” (Mr. A., 54); I think it’s hard for them because they don’t speak the language very well. For instance, when I worked at the kindergarten back then, I had difficulty understanding everything. And there were a lot of misunderstandings. I understand most of it, but sometimes I can’t respond. (Mrs. B., 50)
Discussion
The first quantitative part of the study suggests that the differences, and perceptions of emotional distress, between Vietnamese and German patients partly reflect cultural and migration-related experiences of Vietnamese migrants. In the second, qualitative part, we gathered additional contextualizing information through in-depth interviews with Vietnamese patients, and found new themes of distress that were not mentioned in the survey. Therefore, this study suggests that an interdisciplinary, mixed-methods approach can reveal migrants’ emic themes of emotional distress and contribute to a broader understanding of migrants’ mental health. In the following, we discuss our findings in light of migrants’ diverse sociocultural backgrounds, and their implications for research and clinical work.
Work and finances
In the survey, both German and Vietnamese patients mentioned work as a source of distress. Almost all of the interviewed Vietnamese patients mentioned work as a major burden, but most of them also acknowledged that being able to work was a resource as well. This finding is in line with other studies, which have associated work or unemployment with stress among various migrant groups (Chen et al., 2012; Jurado et al., 2017; Warfa et al., 2012). In the context of Vietnamese cultural values, work is an obligatory contribution to the family’s welfare and to social harmony. In Confucian ethics, work is viewed not as an individual contribution, but instead as a relational contribution to stability and harmony in one’s family and society, and by extension in the universal order (Kim, 2014).
Different migratory pathways structured the meaning-making about work in this population. After the war and reunification of Vietnam in 1975, thousands of South Vietnamese sought refuge under hazardous conditions. The Federal Republic of Germany accepted about 40,000 Vietnamese refugees. They were uprooted and had to start anew. Hard work allowed them to build a future for themselves and their family.
During the 1980s, the German Democratic Republic recruited more than 60,000 temporary labor migrants from Vietnam through a bilateral agreement (GIZ, 2016). Becoming a ‘contract worker’ was initially prestigious and allowed one to financially support one’s family during Vietnam’s economic crisis. The German reunification, however, rendered these migrants largely unemployed and disenfranchised. According to ethnographic research in the community, gainful employment was a pathway of paramount importance to structural security, social entitlements, and successive migration of their families (von Poser, Lanca, & Heyken, 2017).
Today’s ongoing Vietnamese migration to Germany consists mainly of people from rural regions of Vietnam with limited access to education, seeking to improve their economic situation and to support their families. Due to irregular migration pathways, many of them are indebted to traffickers and lack a working permit, as well as legal residency. Another large group of Vietnamese migrated to Germany for educational or training purposes (e.g., nurses) (GIZ, 2016). However, the pressure to earn money is omnipresent and burdensome. Therefore, work (or the lack thereof) has a different meaning depending on individual migration pathways. Additionally, work and the wish to contribute to society are highly valued among Vietnamese, and receiving social welfare is associated with shame and loss of face. Our ethnographic data indicate that work is perceived as both a burdensome obligation and a central strategy of self-validation.
Children
Compared to German patients, Vietnamese patients mentioned children more often as a source of distress. Worries often revolved around parenting, especially the need to find a balance between local parenting styles and those acquired in Vietnam. Our results are in line with the existing literature on parenting of Vietnamese migrants living in the United States, Australia, and Norway (Nguyen, 2015; Tingvold et al., 2012). For instance, Confucianism values filial piety, which comprises children’s obligations to honor their parents through displays of obedience and respect. This more authoritarian parenting style does not allow children to disagree with their parents. In contrast, current educational notions in Germany value children’s autonomy and more democratic parenting styles. Thus, children socialized in Germany may find their Vietnamese parents’ beliefs to be anachronistic and unjust compared to the values that structure their German peers’ experiences (Beth & Tuckermann, 2008).
Moreover, support systems and strategies connected with the paramount societal value of collectivism in Vietnam often fail to work in a more individualistic society and instead engender further difficulties. For instance, in Vietnam, children stay in full-time (pre)school and teachers, grandparents, and neighbors are much more involved in their upbringing. Family members’ intervention often mediates conflicts. With life in a nuclear family in Germany, however, such socio-centric solutions are often no longer available (Röttger-Rössler & Lam, 2019).
Partnership
German patients mentioned difficulties with partners significantly more often than Vietnamese patients in the quantitative part. However, when we asked directly for partnerships as a possible source of distress, this theme appeared more frequently in the Vietnamese population. A recent study investigating explanatory models of primary health care providers in Vietnam also identified social and familial expectations to be linked as a cause of depression (Murphy et al., 2018). Keeping the familial harmony and saving face (Hwang, 2012; Pham, 2014)may be one reason why Vietnamese patients withheld such issues in a written account. The Vietnamese proverb “Xấu chàng hổ ai” reflects this notion and means: If the husband’s negative traits are shared with others, it will bring shame upon the wife. However, directly addressed in confidential interviews, patients shared both their views on Vietnamese partnerships in general and their personal experiences. While they mostly described ideal partnerships as a relation of solidarity in which partners co-shoulder struggles, a lack of open communication was mentioned as a common problem in Vietnamese marriages. Reported difficulties encompassed unreliability, unfaithfulness, and lack of commitment. For several patients and regardless of gender, their partners’ disdain was a major source of distress, and several women even reported experiences of domestic violence.
Ethnographic data from different contexts underscore that, for migrants, altered norms, discrimination, and structural marginalization can elicit feelings of disempowerment and inferiority, especially in men (Farahani, 2012; Khosravi, 2009). In response to being excluded from hegemonic masculinity (Connell, 1987), some men perform aggressive hypermasculinity as a means of self-assurance. With notions of Germans’ partnerships as egalitarian, hierarchical partnerships can also serve some men to construct and consolidate a gendered sense of cultural identity by exaggerating traditional patriarchal Vietnamese values, such as the Confucian ideal of male dominance over women (Do et al., 2013). This might account in part for reported male domestic violence and calls for further qualitative investigations.
According to our clinical observation, some of our female patients reported that their partners displayed longstanding sleeping disorders, impulsive behaviors, or social withdrawal. Rather than seeking professional help, they often used alcohol for self-treatment. Statistics on the utilization of mental health services among Vietnamese migrants in Germany showed an underrepresentation of male patients (Ta et al., 2015). The lack of appropriate coping strategies paired with alcoholism elevates the risk for conflicts. Other studies have also reported an elevated prevalence for domestic violence among Vietnamese (Do et al., 2013; Garcia-Moreno et al., 2006; Nguyen, 2006).
Psychological/somatic symptoms and isolation
German patients reported significantly more psychological symptoms explicitly than did Vietnamese patients. The frequency of somatic symptoms was not significantly different between the two groups. When we interviewed our patients, both psychological and somatic symptoms were equally articulated as sources of distress. Our findings are in line with the existing literature, indicating that the mind-body dualism—rooted in European enlightenment philosophy—is less influential for Asian patients, whose spontaneous symptom presentation instead typically emphasizes somatic symptoms (Choi et al., 2016; Dreher et al., 2017; Ryder & Chentsova-Dutton, 2012). A new theme of distress that emerged from the interviews was social isolation, either as a symptom or a consequence of patients’ psychiatric illness. Previous acculturation research on Vietnamese migrants has shown that marginalization—meaning being oriented toward neither the mainstream nor the heritage society—is associated with higher levels of depression (Nguyen et al., 2017). Losing one’s social network and difficulties with establishing and maintaining new social ties after the act of migration are frequently reported experiences among migrants (e.g., Hurtado-de-Mendoza et al., 2014).
Past and future
During the interviews with the Vietnamese patients, the past was often articulated as being associated with distress. Patients repeatedly said that they tried not to think about the past. Our results echo the existing literature. Kaiser and colleagues (2015) have identified “thinking too much” (suy nghĩ nhiều) to be a worldwide idiom of distress, which overlaps with “Western” symptoms such as rumination. Studies among Southeast Asian societies have explained the negative experience of “thinking too much” by referring to valued and shared Buddhist principles, which emphasize equanimity or non-attachment toward emotions or thoughts (Cassaniti, 2011; Nhat Hanh, 1999). Thus, inability to control one’s mind is associated with weakness and with the failure to practice the Noble Eightfold Path to liberate oneself (Kaiser et al., 2015; Merkel, 1996). Patients try to distract themselves by suppressing their thoughts; however, when the illness is too severe, these coping mechanisms fail (Wenzlaff & Luxton, 2003). Hinton et al. (2016) relate “thinking too much” among patients with a Southeast Asian background to negative moods as well as to mental and somatic symptoms, and point out their potential to engender catastrophic cognitions.
Concerning the future, patients were ambivalent. Some patients avoided thinking about the future to prevent “thinking too much,” while others hope for a better future to motivate themselves. In our therapeutic context, we used these findings and practice to return to the present by applying mindfulness-based interventions, which are rooted in Buddhism and therefore very accessible to our patients (Fung, 2015). Acceptance and mindfulness techniques have also been successfully applied in culturally adapted CBT (CA-CBT) among Latino and Southeast Asian refugee populations with PTSD (Hinton et al., 2013). Moreover, in psychoeducation, we reframe rumination as a depressive symptom rather than a flaw in character, which helps patients to accept themselves more.
Speechlessness and language
Another theme that emerged in the interviews we labelled as “speechlessness.” Importantly, this theme was related to, but went beyond, communication barriers, which involved difficulties with German language. Moments of speechlessness occurred in different spheres of life, concerning interactions with the mainstream society in Germany, the nuclear family, and relatives in Vietnam or the local Vietnamese communities. Research on acculturation has shown that language proficiency is often a gateway to a society (Berry, 2005; Schachner et al., 2014). These results also matched the described difficulties of our patients when dealing with German institutions and bureaucracy. Such challenges were often perceived as overwhelmingly burdensome, mainly because the patients lacked language skills, but also because of the uncertainty regarding culturally accepted modes of interaction or previous intimidating experiences in their migration histories. Similar results were obtained in previous studies, which also concluded that administrative obstacles were an additional barrier to receiving mental health care for migrants (Kung, 2004; Straßmayr et al., 2012).
On another level, within the nuclear family, communication difficulties between parents and children were aggravated due to language barriers. Children born in Germany did not speak enough Vietnamese to engage in profound communication with their parents. Meanwhile, parents did not speak German sufficiently for deep conversational exchange. Ethnographic research with children of former Vietnamese contract workers living in Berlin (Röttger-Rössler & Lam, 2019) has shown that asymmetries in German language competencies between parents and children may subvert the hierarchical family structure and notions of filial piety. These new asymmetries may engender affective dissonances and emotional distress within the family. Additionally, deeply ingrained norms may appear natural to parents, making it hard to recognize and explicate them verbally to their children, who underwent different socialization in Germany.
Beyond the nuclear family, disruption and speechlessness were also reported when communicating with family members in Vietnam. Migrants have had to adjust to the new social and cultural norms and practices in Germany. Their everyday life differs from that of their distant relatives. Thus, relatives in Vietnam often cannot imagine life in Europe. In addition to the problem of conveying their local experiences, migrants do not want to burden their relatives in Vietnam with concerns about their transnational lives. Interview data suggest that these hardships can result in a disruption of belonging and feelings of alienation (Röttger-Rössler, 2016).
Lastly, patients reported a distinct mistrust of and grave concern about gossip within the Vietnamese communities (von Poser, Lanca, & Heyken, 2017). They feared that their private matters, once entrusted to friends or acquaintances, might be passed on to others, circulate more widely, and lead to adverse judgment and loss of face among their countrypeople (đồng hương). The migrant communities were reportedly prone to gossip, given the small size and tightly interconnected nature. Ethnographic accounts and our own cultural knowledge suggest that difficulties in transposing previously acquired social strategies and practices to the German context might explain this phenomenon. In Vietnamese society, losing face (mất mạ˘t or mất thể diện) is associated with social disapproval of one’s image or of the family’s image; therefore, face-threatening contents are kept within the extended family (Nguyen, 2015; Nhung, 2014). This is also reflected in the common Vietnamese proverb “Vạch áo cho người xem lưng” (Don’t take off your shirt to show your back), which conveys the notion that one should not talk about private family problems in public. However, during the process of migration, extended family structures shrink to the nuclear family (Tingvold et al., 2012). Attempts to share private matters with members of the local, extended community instead often disappoint; without clear affiliation, the rule of keeping private matters within the family to “save face” fails.
In summary, moments of speechlessness are experienced in various spheres of our patients’ life (see Figure 1) and demand consideration in therapy. Encounters in a neutral therapeutic space may serve as a safe third space in which patients can productively address feelings of mistrust toward fellow Vietnamese migrants, and that enables new experiences (Bhabha, 2004). Responding to this need, the specialized psychiatric-psychotherapeutic outpatient clinic in Berlin has offered culturally sensitive group therapies in the Vietnamese language, focusing on concepts such as belonging and acknowledging the hardships of migration (e.g., Pfaff-Czarnecka, 2013; Ta et al., 2017).
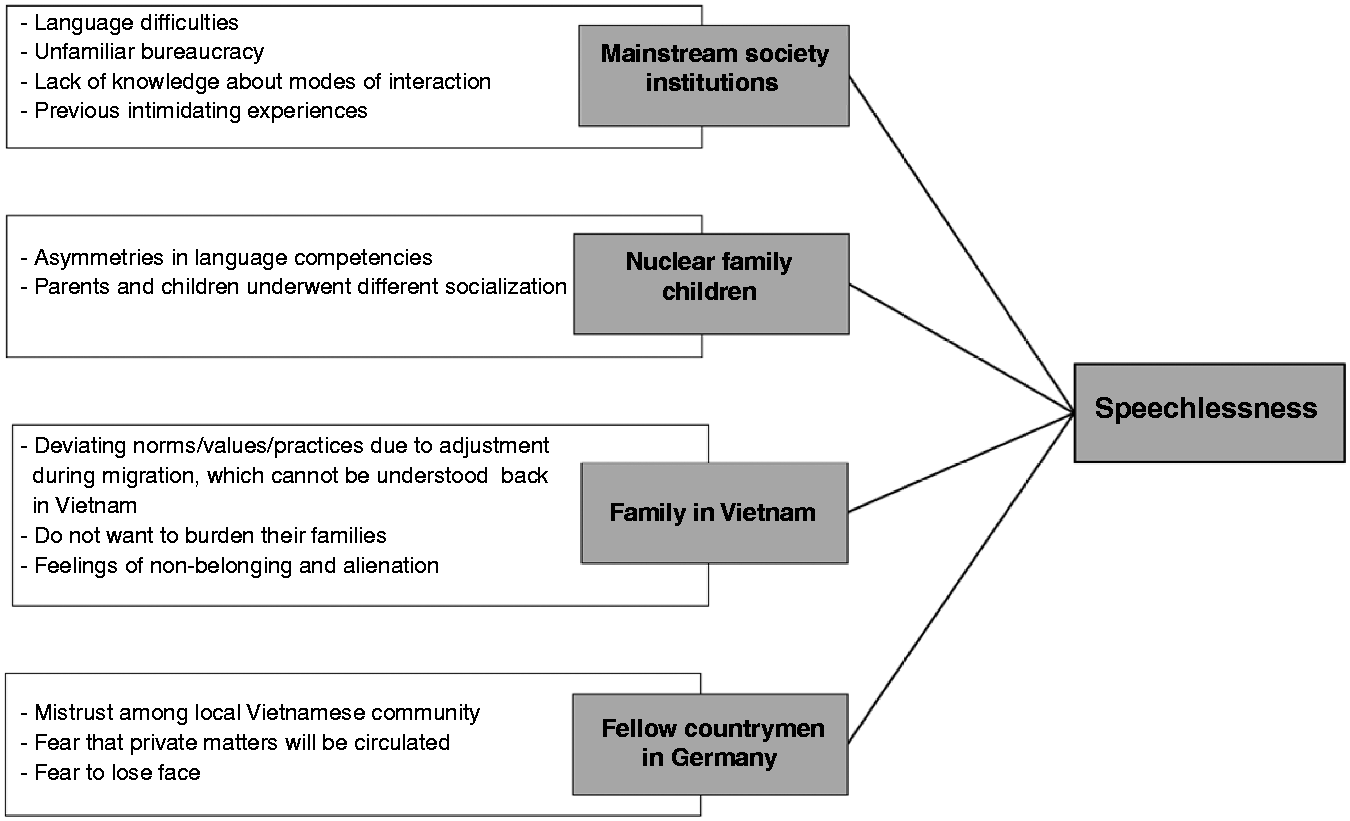
Reported experiences of speechlessness in different spheres of life among the n = 20 interviewed Vietnamese outpatients living in Germany.
Limitations
The findings of the present study should be interpreted in light of several limitations, which should be addressed in future studies. First, our study is a cross-sectional study and cannot determine causal relationships. Second, our sample consists of a population utilizing mental health care services, and their experience with psychiatry and with particular forms of distress might influence their perception of social stressors. Therefore, our results cannot be generalized to the overall local Vietnamese population or communities. Third, we focused on investigating migration-related emotional distress and did not interview a German group to compare social structural stresses that might be common across the groups.
Conclusion
The interdisciplinary, mixed-methods approach employed in this study provided valuable information of areas of distress for Vietnamese immigrants. While generalizations are usually misleading in the heterogeneous Vietnamese population of Berlin, there were clear parallels in the biographies of our interlocutors based on shared experiences, accounting for commonalities in their intersectional positionality and group-specific characteristics in our sample. In addition to commonly expressed themes of distress related to socioeconomic conditions including work, finances, or language, we identified affectively charged themes, such as partnership and children, and particular moments of speechlessness, which were burdensome and influenced multiple spheres of life. Our results also highlight that, besides socioeconomic burdens, migration processes entail potentially stressful affective dynamics. Future studies should investigate perceived distress among other populations of migrants who underutilize mental health services, and evaluate whether there are differences in perceptions of distress. The identified themes can be utilized to develop clinical questionnaires to promote culturally sensitive assessments. In terms of intervention, psychotherapy may address the themes of distress that we have uncovered and offer specific coping strategies. In conclusion, we believe that this research approach can provide better understanding of the complex and entangled phenomena of mental health and migration, as well as helping to advance culturally sensitive, person-centered medicine.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was conducted in part within the subproject A02 of the CRC 1171 “Affective Societies – Dynamics of Coexistence in Mobile Worlds” granted by the German Research Foundation (DFG – Deutsche Forschungsgemeinschaft). Dr. T. M. T. Ta is a member of the Clinician Scientist Program in the Berlin Institute of Health. We wish to thank all participants who agreed to take part in the study.