
Abstract
Adolescent girls vulnerable to early marriage and school dropout in rural India may be at elevated risk of psychosocial problems. However, few screening instruments have been culturally adapted and validated to measure this risk. This paper describes the process by which the Primary Health Questionnaire PHQ-9, a screening instrument for depression, was tested for cultural validity as part of the Samata evaluation – an intervention to support low caste adolescent girls in rural south India to attend and complete secondary school and to delay marriage until adulthood. Three focus groups discussions (FGDs) were held with 20 adolescent girls and six outreach workers of the Samata programme in rural north Karnataka, south India. The FGDs were used to explore local expressions of psychosocial problems and to understand the acceptability and appropriateness of PHQ-9 items. A thematic content analysis was conducted on the transcripts of the FGDs. Descriptions of local expressions of psychosocial problems generally matched the items on the PHQ-9. However, not all representations of psychological symptoms were captured by this tool. Persistent worry, loneliness and isolation, and externalised behaviours were also described by participants as common expressions of psychosocial distress. Based on the limitations of translation methods, local stakeholders must be involved in evaluating the cultural appropriateness of mental health screening tools. The current research demonstrates a strategy by which to assess the cultural validity of Western psychiatric instruments with key stakeholders in low- and middle-income settings.
Introduction
Psychological problems present significant challenges to the health and wellbeing of the young, and are a large contributor to the disease burden in adolescence (Mokdad et al., 2016; Patel, Flisher, Hetrick, & McGorry, 2007). Yet, action from the global health community has been minimal (Mokdad et al., 2016; Petroni, Patel, & Patton, 2015), especially for adolescents in low- and middle-income countries (LMIC) (Davidson, Grigorenko, Boivin, Rapa, & Stein, 2015). Little is known about the development of psychological problems among adolescents in LMIC, which is concerning given the adversities youth face in these contexts (e.g. poverty, conflicts, gender discrimination, and inadequate access to education) (Davidson et al., 2015).
Of particular concern are adolescent girls in LMIC settings, a group which experiences gender discrimination, such as child marriage, sexual harassment, and exclusion from education (Davidson et al., 2015; Petroni et al., 2015). In India, this is particularly evident among adolescent girls from Scheduled Caste (SC) families, previously known as ‘untouchables,’ and Scheduled Tribes (ST), communities living in tribal areas of India (Government of Karnataka, 2008). These girls are at increased risk of child marriage (before the age of 18) or to become sex workers — a situation that exposes them to HIV infection and often ends their education (Raghavendra & Anderson, 2013). The literature, while small, does suggest an association between gender discrimination and mental health (Aaron, Bose, & Abraham, 2004; Bhola, Rekha, Sathyanarayanan, Daniel, & Thomas, 2014; Petroni et al., 2015). In Vellore, southern India, Aaron and colleagues (2004) found that females have 2.5 times the rate of completed suicide relative to males. Furthermore, females have a greater likelihood of suicide attempts and ideation compared to male counterparts in Bangalore, India (Bhola et al., 2014; Pillai, Andrews, & Patel, 2009). Research from Africa and south Asia have also found that girls engaged or married as minors are vulnerable to depression and suicidality, in great part to its link with varying forms of gender-based violence (e.g., forced marriage and spousal violence) (Raj, 2010).
Given the paucity in mental health research in LMIC settings, documentation and monitoring of adolescent girl’s psychological wellbeing must be implemented (Kohrt, Jordans, Tol, Luitel, Maharjan, & Upadhaya, 2011; Petroni et al., 2015). Screening tools are an essential component in measuring the magnitude of mental health problems and in evaluating the effectiveness of psychological interventions (Ali, Ryan, & De Silva, 2016; Kieling et al., 2011; Petroni et al., 2015).
Measurement of Mental Health
Before studying the burden of psychological distress among adolescent girls, it is necessary to ensure that the tools we use to measure mental health are not only reliable, but also feasible and culturally valid (Robinson, Metzler, & Ager, 2014). A conventional strategy for cross-cultural validation has been to evaluate the capacities of screening instruments that identify probable cases, such as depression, and compare these capacities to the accepted gold standard tests, such as a clinical diagnostic interview (i.e., criterion validity) (Kaiser, Kohrt, Keys, Khoury, & Brewster, 2013; Kohrt et al., 2011; Sweetland, Belkin, & Verdeli, 2014). However, gold standard validation is time-consuming, expensive and resource intensive, and thus, may not be feasible in many LMIC settings (Kohrt et al., 2011; Sweetland et al., 2014; van Ommeren, 2003).
The most common method for adapting mental health screening instruments is to translate Western instruments into the local language (Traube, Dukay, Kaaya, Reyes, & Mellins, 2010). Often, the screening instrument is then used without further assessment (Kohrt et al., 2011; Sweetland et al., 2014). However, it is not always clear if items on an instrument can be translated and applied cross-culturally in such a simplistic manner (Bass, Bolton, & Murray, 2007; Betancourt, Speelman, Onyango, & Bolton, 2009; Bolton, Neugebauer, & Ndogoni, 2002; Kohrt et al., 2011; Tsai, Scott, Hung, Zhu, Matthews, Psaros, & Tomlinson, 2013).
Based on the limitations of translation, and the challenges of establishing criteria-related validity, there is a need to validate screening instruments by involving key stakeholders to understand local concepts of psychological distress (Bass et al., 2007; Bolton, 2001; Brown, Mentha, Rowley, Skinner, Davy, & O’Dea, 2013; Kaiser et al., 2013; Haroz, Bass, Lee, Murray, Robinson, & Bolton, 2014; Rasmussen, Basila, Keller, & Wilkinson, 2011 ; Smit, van den Berg, Bekker, Seedat, & Stein, 2006). Several efficient and low-cost qualitative research methods have been used to guide the selection and adaptation of instruments to local settings (Bass, Ryder, Lammers, Mukaba, & Bolton, 2008; Kaiser et al., 2013; Betancourt et al., 2009; Betancourt et al., 2012; Smit et al., 2006). An example of a rapid cultural analysis method utilized in cognitive anthropology is “Free Listing”, a technique used to identify local expressions of psychological distress (Bass et al., 2008; Betancourt et al., 2009; Bolton et al., 2002). In Free Listing, participants are asked to list items they can think of when presented with a specific question (e.g., what problems do girls face in your community?). The items are then ranked in order of salience. This approach has been used successfully with adolescents in LMIC settings (Betancourt et al., 2009; Ng, Kanyanganzi, Munyanah, Mushashi, & Betancourt, 2014).
Van Ommeren and colleagues (1999) outlined a an approach for the cultural adaptation of Western instruments. This method, too, has been utilised successfully with children to adapt and validate screening instruments in Nepal (Kohrt et al., 2011). At the core of transcultural adaptions are FGDs with community members, where participants assess the acceptability, relevance (i.e., content equivalence), and comprehensibility (i.e., semantic equivalence) of each item in the screening instrument (Kaiser et al., 2013; Kohrt et al., 2011; van Ommeren et al., 1999).
Mental Health and the Samata Intervention
In India, gender norms frequently intersect with other important structural factors, such as caste and rural residence, to influence age at marriage and to limit women’s access to formal education and economic opportunities (Carswell & De Neve, 2013; Harriss-White, 2012). ‘Samata’ is a comprehensive intervention in rural north Karnataka, south India, which aims to delay child marriage and prevent child entry into sex work by increasing entry into and completion of secondary school education for lower caste adolescent girls. This multi-level intervention is being assessed through a cluster-randomised control trial (RCT) design (Beattie et al., 2015). In addition to evaluating educational and marriage outcomes, the research team was interested in understanding the impact of child marriage, school dropout, and other factors on adolescent psychological health in this setting. Researchers were also interested in understanding if the ‘Samata’ intervention had a positive impact on the psychological well-being of adolescent girls. However, there was a paucity of literature on the most appropriate mental health screening tools for this population.
The research team originally selected the Primary Health Questionnaire-9 (PHQ-9) (Kroenke, Spitzer, & Williams, 2001), a nine-item depression module, to measure the presence and severity of psychological problems among adolescent girls who participated in the cluster-RCT surveys. The screening instrument was selected because it was perceived to have brevity, ease of delivery, and comparability to other studies. Originally, the PHQ-9 was designed to measure depressive symptoms in adult populations; however, of late, it has been increasingly used with adolescents and young adults (Adewuya, Ola & Afolabi, 2006; Ganguly, Samanta, Roy, Chatterjee, Kaplan, & Basu, 2013; Richardson et al., 2010; Tsai et al., 2014). Further, the PHQ-9 has been validated with an urban population of adolescents in Kolkata, India (Ganguly et al., 2013).
Objectives
The aim of our study was to assess whether the proposed mental health measurement strategy captured local expressions of mental health among adolescent girls in north Karnataka. As the PHQ-9 was recommended, the Samata research team wanted to determine whether this screening tool would be an acceptable and appropriate (i.e., comprehensible and relevant) measure to assess mental health problems among adolescent girls as part of the evaluation of the Samata intervention. Specifically, concerns were raised about the following: 1) semantic equivalence, i.e., whether the girls would understand the meaning of PHQ-9 items; 2) content equivalence, e.g., the appropriateness of the item relating to appetite and weight loss (‘poor appetite or overeating’), because the girls were from poor rural communities; and, 3) acceptability of items, e.g., whether it was acceptable to ask about suicide and self-harm (‘thoughts that you would be better off dead or of hurting yourself in some way’) because of the sensitivity of this topic in Indian culture. Consequently, we examined the acceptability and appropriateness of PHQ-9 items among adolescent girls participating in Samata programme.
Specifically, the study objectives were to: i) Explore local perceptions of mental health problems among adolescent girls. This was intended to allow the research team to determine if local mental health problems were addressed in the PHQ-9; ii) Assess the comprehensibility (i.e., semantic equivalence), relevance (i.e., content equivalence) and acceptability of the items on the PHQ-9. The study findings would be used to inform the mental health measurement tool used in the Samata evaluation.
Methods
Setting and interviewers
The study was conducted in Bijapur and Bagalkot, north Karnataka, where the Samata programme is currently being implemented. The project covers 3,600 girls, ages 12 to 17, from 119 villages and 69 schools in these two districts. Three researchers (two females and one male) were present at each FGD. The lead facilitator (research coordinator at KHPT) led the FGDs with the assistance of a clinical social worker and local staff member. Two researchers were trained in qualitative interviewing methods; one was bilingual (Kannada and English). The third researcher had experience in conducting workshops with youth and supervising the Samata programme. The FGDs were conducted in the local language, Kannada. Prior to the interviews, the research team translated the PHQ-9 to Kannada and then back-translated items to ensure they retained their original meaning. All qualitative interviews were conducted by researchers mentioned above, with one interviewing participants and the other two recording the responses, which enabled the facilitator to use probes to explore local psychosocial constructs.
Participants and sampling method
The study participants were adolescent girls and outreach workers from the Samata programme. We interviewed a convenience sample of adolescent girls from the Samata intervention communities. These girls were members of the parivartan sports group – an established recreation sports group of the Samata programme. Twenty girls aged between 15 and 16 years, from SC and ST backgrounds, labouring families, participated in two FGDs (13 from Bijapur district and 7 from Bagalkot district). The participants were enrolled in secondary school, 8th and 9th standard, at the time of the study.
A convenience sample of six outreach workers from Bijapur, who had been working with KHPT for between 3 and 10 years, were also interviewed. We could complete only one FGD with outreach staff because of limited time and available staff to assist in translation. Bijapura district was chosen for this outreach worker FGD, as this community had the most experienced Samata workforce.
Interviewing methods
Using techniques described elsewhere (Betancourt et al., 2009; Colucci, 2007), we used a rapid ethnographic method, based on the Free Listing technique, to conduct FGDs with adolescent girls and outreach workers. The Free Listing exercise can be used in focus group discussions (FGDs) (Colucci, 2007; Ellsberg & Heise, 2005); and is a technique that lists answers in response to a primary question. This rapid ethnographic method was designed to explore local mental health concepts, priorities, and the applicability of Western psychiatric concepts among this sample population.
The Free Listing question was “What are the problems faced by girls in your community?” Interviewers probed for a number of problems and generated a list. Their responses were recorded on a large piece of paper. From this list, as a group, each FGD prioritised the major problems in their community (“Can you tell us what problems affect girls most in your community?”). We focused on six leading problems, and the participants were asked to provide a short description of each. This list of problems was then probed for descriptions of associated thinking, feeling and behaviours to explore prevalent psychosocial issues.
To explore the appropriateness and acceptability of PHQ-9, we attempted to present participants with each item in the instrument. The PHQ item on suicide and self-harm was excluded, as community members perceived this to be too sensitive an issue to be addressed in the FGD with the girls. The acceptability of the suicide and self-harm item was discussed in the outreach worker FGD. The cultural translation method described elsewhere (Kaiser et al., 2013; Kohrt et al., 2011; van Ommeren et al., 1999) was used as a guide. Interviewers probed each item for comprehension, relevancy and acceptability. We audio-recorded all responses, as well as took notes.
Data analysis
A thematic content analysis (Smith, 1992) of FGDs was conducted using NVivo 10. Coding and analysis of transcripts were conducted by the lead author, in consultation with the second, third and last two authors. Key themes of our research objectives were incorporated into a thematic framework including: (a) local concepts of mental health problems and manifestations, and (b) the domains of transcultural translation, namely, comprehensibility (i.e., sematic equivalence), relevancy (i.e., content equivalence) and acceptability, as described by van Ommeren and colleagues (1999). After becoming familiar with the transcripts and NVivo coding, the framework was modified to include themes derived inductively from our dataset. The dataset was then coded using this framework and analysis was undertaken. Results were reviewed and approved by local research associates of KHPT. We present the results as narratives describing key themes, using excerpts from participants’ quotes.
Community collaboration and ethics
The topic guide and data collection were created and undertaken in partnership with local research associates and the programme implementation team of KHPT. The study obtained ethical approval from St. John Medical College, Bangalore, India, Hospital Institution Ethics Committee and the LSHTM Ethics Committee, London, UK. Informed consent was obtained from care-givers (parents/guardians) and outreach staff; informed assent was obtained from adolescent girls. Adolescent girls and their families did not receive monetary compensation; they were provided with breakfast and lunch before and after the FGDs.
Results
Local expressions of mental health
Main problems emerging from focus group Free Listing exercise.
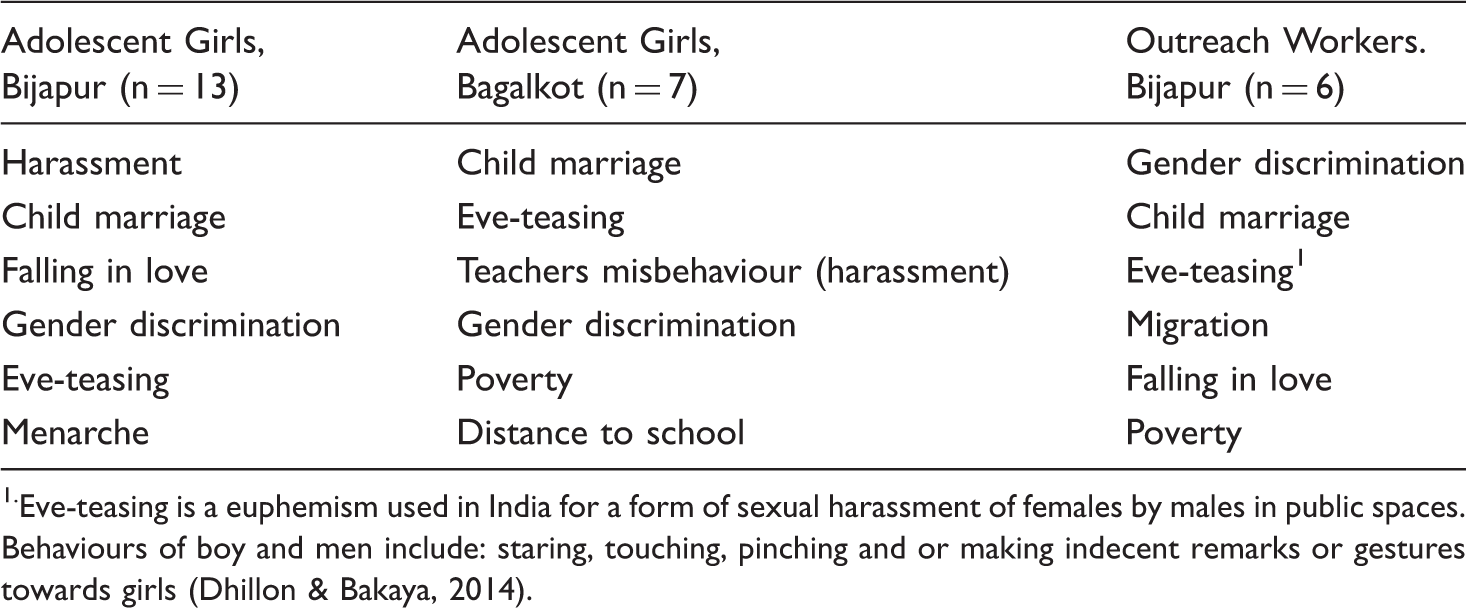
Eve-teasing is a euphemism used in India for a form of sexual harassment of females by males in public spaces. Behaviours of boy and men include: staring, touching, pinching and or making indecent remarks or gestures towards girls (Dhillon & Bakaya, 2014).
When facilitators probed for feelings, thoughts, and behaviours linked to problems listed, girls cited crying, sadness and withdrawal, “alone, they won’t speak to anyone …”. Other features included: shame, “spoiled their family name”; worthlessness and irritability, “she becomes atypical … express anger towards all”; and suicidal ideation, “sometimes evil thoughts of committing suicide arise”. Further, as illustrated below, outreach workers describe how depression presents in adolescent girls when they are married off and forced to discontinue their education. “… feeling deprived of everything desired could make her go into deep mental pains, might make her lose interest in everything, losing focus/attention, non-responsive to anybody’s calls … they would be unable to consume and digest food, not getting proper sleep and even if they sleep, could not be able to do it properly and thinking deeply about the same desire (desire to continue their education). Usually those who are suffering with depression would behave like this only.” “Thinking of such possible negative developments (imaginary) about her future life, she might decide to take the extreme drastic step of committing suicide and ending her life forever.” “They remain silent even at school. And while going out, if they come across any known persons they start looking downwards. They do the same thing even at school.”
Protective and risk factors
Other emergent themes were linked to protective factors that helped girls cope with problems they encountered in their community. Participants reported the assistance they received from external interventions, such as the Samata programme, to help girls avoid child marriage. Participants also cited involvement in activities – singing, dancing and playing with friends as being helpful. However, the presence and support of a network, friends and family, were critical to helping girls deal with the problems they face.
Indicators of depression and anxiety features described in FGDs*.
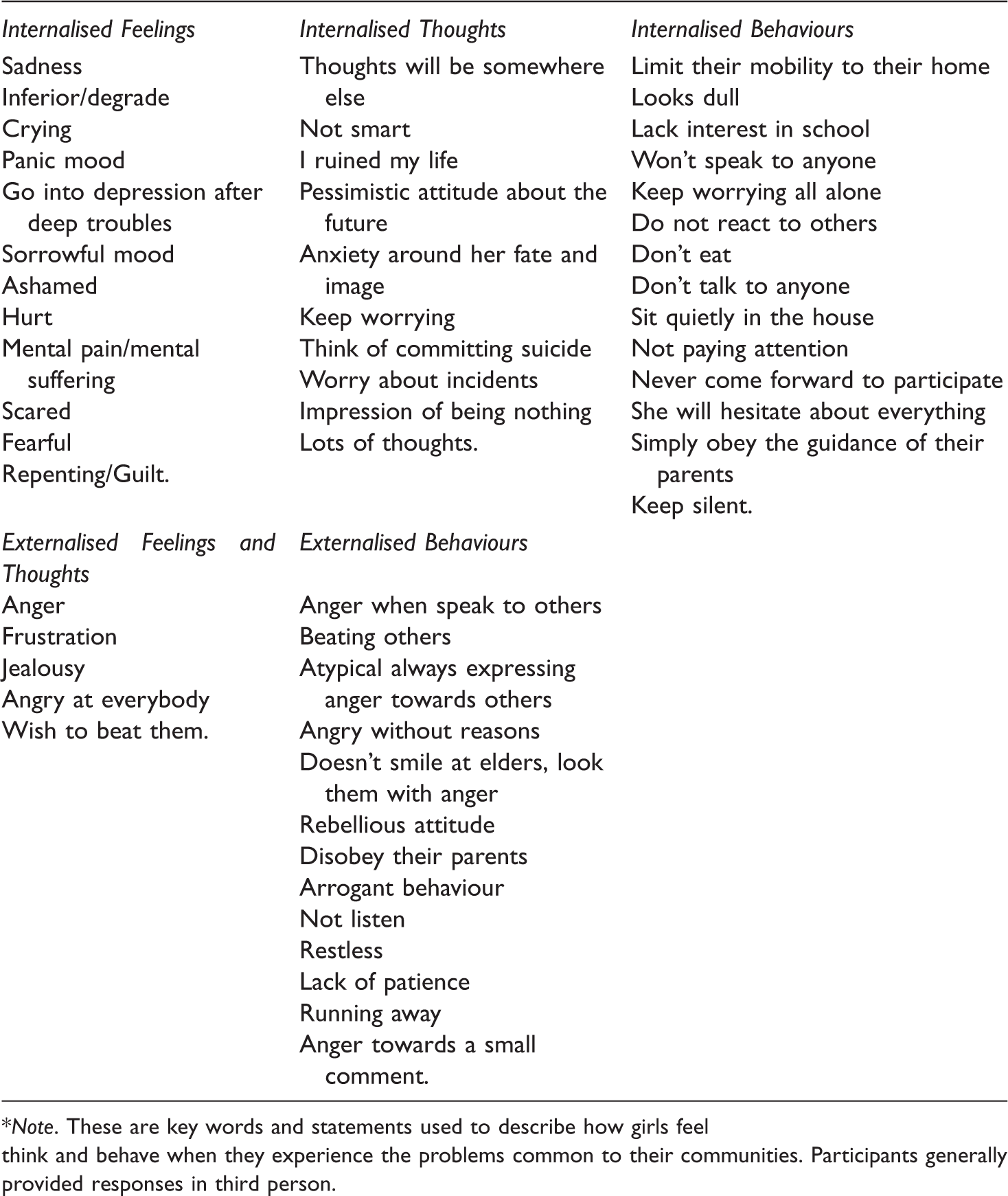
*Note. These are key words and statements used to describe how girls feel think and behave when they experience the problems common to their communities. Participants generally provided responses in third person.
Appropriateness of PHQ-9
Modified mental health measurement tool*
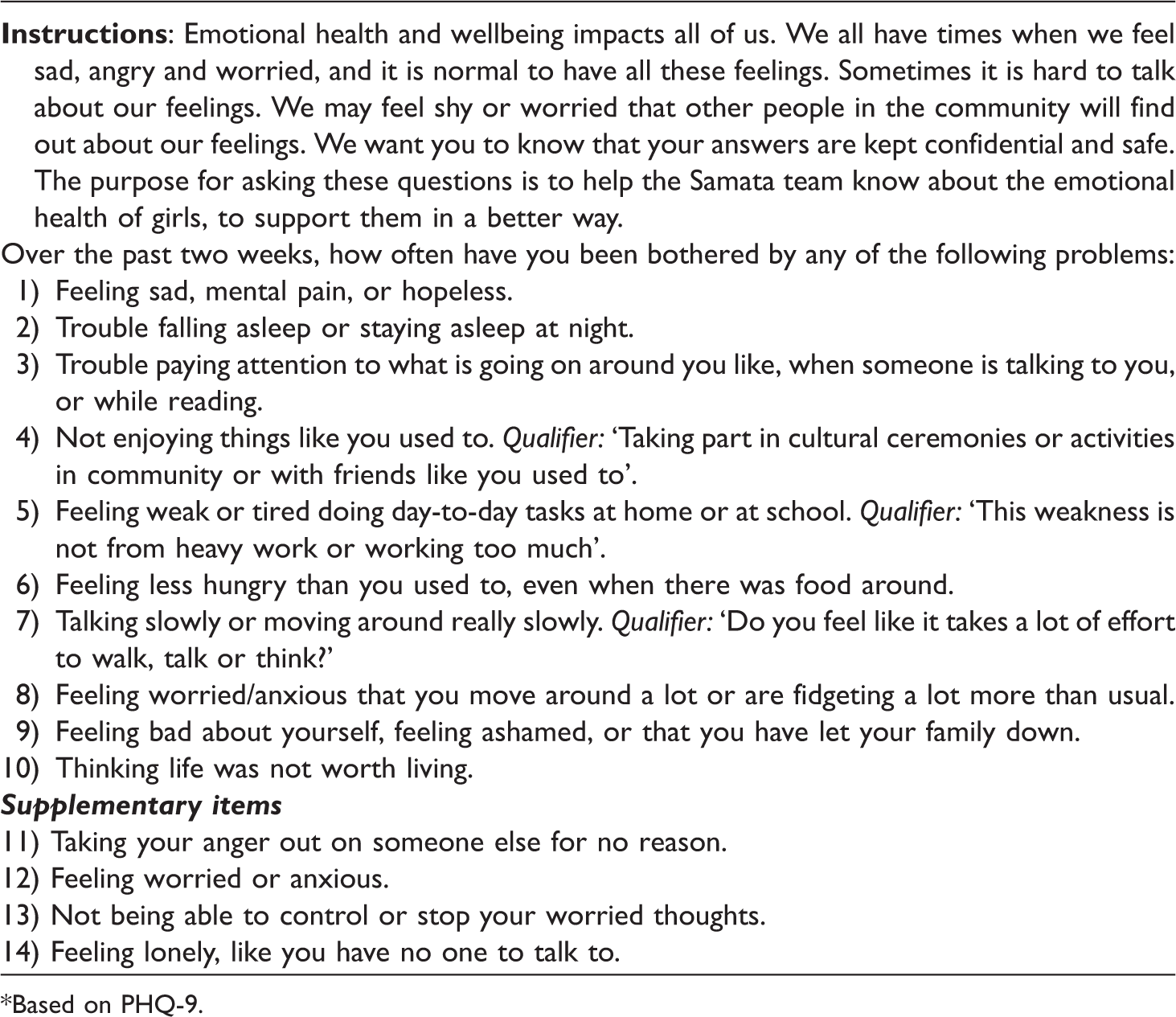
*Based on PHQ-9.
PHQ-9 items associated with depression
Three PHQ-9 items were endorsed by each FGD as having a connection to depression. These items are presented below.
PHQ-9 items associated with anxiety symptoms
Other items were endorsed by each FGD as having a connection to anxiety, such as ‘trouble falling sleeping, staying asleep’, ‘loss of concentration’ and ‘poor appetite’.
PHQ-9 items with a low association to psychosocial problems
No participant endorsed an association between ‘little interest or pleasure in doing things’ and psychological problems, as well as ‘fatigue and little energy’ and mental health. There were mixed findings for ‘moving slowly or being restless’ and psychological problems.
The item ‘talking slowly or moving around really slow’ did not appear to match psychomotor symptoms associated with depression. To enhance clarity and relevance to psychomotor we proposed the following qualifier: “Do you feel like it takes a lot of effort to walk and talk?” For the second statement, we would suggest using the words nervous/anxious for clarity. Based on their comments, we proposed the following modification: ‘Being so worried or anxious that you move around a lot – or are fidgety’.
Acceptability of PHQ-9 items
In the FGDs, participants found PHQ-9 to be an acceptable questionnaire to be carried out in their communities. The participants were candid in their discussions regarding psychosocial problems, including suicidal ideation, as seen in the Free Listing exercise. Although suicide and self-harm is a sensitive question, the outreach workers found it acceptable to be included with modification. However, they cautioned around reporting bias, as girls may think this information will be shared with their family members.
Manifestations of psychosocial problems not captured in PHQ-9
As illustrated in the Free Listing exercise, anxiety, isolation and aggressive outbursts were mentioned often by participants in FGDs. These manifestations of psychological distress were deeply connected to adversities girls faced in their communities. However, these features are not directly addressed in PHQ-9. As a separate questionnaire related to these expressions is not feasible, we propose including supplementary items in addition to using the PHQ-9 to capture worried thoughts, and externalised and internalised behaviours.
Presentation of the mental health survey
Questions related to mental health can be sensitive, particularly questions related to suicide and self-harm for reasons mentioned above. Based on discussions with the outreach workers, researchers must ensure that confidentiality is understood, and mental health experiences are normalised for adolescent girls to make them feel comfortable. Thus, we recommend an introductory statement to the PHQ-9, which reinforces discretion and normalcy of emotional stress. The modified PHQ-9 and the supplementary questions recommended based on the above findings, is presented in Table 3.
Discussion
Based on the qualitative findings, we were able to assess if PHQ-9 is an appropriate and acceptable instrument to measure the psychological health among adolescent girls in rural south India. Overall, our findings suggest that this instrument captures the presentation of depressive symptoms of adolescent girls in this context. Though psychological distress was not cited as a problem girls face in their communities directly, psychosocial problems were deeply connected to the adversities mentioned, such as gender discrimination. (e.g. eve-teasing, child marriage) and poverty. Adolescent girls and outreach workers described psychosocial challenges that appeared to share similarities with depression and anxiety-like features as outlined in the Diagnostic Statistical Manual of Mental Disorder V (DSM-V), thus reflective of Western psychiatric concepts presented in PHQ-9 (American Psychiatric Association, 2013) (Kroenke, Spitzer & Williams, 2001). Our findings were also comparable to other studies in LMIC settings (Betancourt et al., 2009; Pillai et al., 2009), as expressions of depression and anxiety were parallel to Western psychiatric concepts, and strongly associated with hardships experienced by youth.
Many of the PHQ-9 items were connected to psychological distress; however, three items were low on content equivalence: ‘slow movement and restlessness’, ‘tiredness and fatigue’ and ‘little interest and pleasure doing things’. Nevertheless, weakness and decreased participation in activities were expressed by several participants in the FGDs in connection with emotional distress. To increase their relevancy, we modified the items to match local idioms expressed in the FGDs. For instance, the word ‘weakness’ replaced ‘fatigue’, as this term was used to describe the mental distress girls experience from getting married at a young age. It should be noted that the item related to psychomotor changes was challenging to modify as it was unclear if these items, were connected to symptoms of psychological distress. We did modify statements based on comments from FGDs and included words, such as ‘worried’ and ‘anxious’ to increase the relevancy this item. This modification to the PHQ-9 was used in Esler and colleagues (2008), and the authors reported that the adapted instrument maintained good psychometric properties. However, further qualitative work is needed to explore the relationship between psychomotor changes and depression-like symptoms in this population (Bennabi, Vandel, Papaxanthis, Pozzo, & Haffen, 2013).
Slight modifications to each item of the PHQ-9 were required to increase their relevancy. For example, for the item ‘sleeping too much, trouble staying asleep’, participants associated ‘sleeping too much’ with an individual who is free from worries and tension, whereas ‘problems falling asleep’ was connected to the presence of worry. Opposing statements may create confusion for interviewees (Brown et al., 2013; Poongothai, Pradeepa, Ganesan, & Mohan, 2009); therefore, conflicting statements within an item, unconnected to mental health, were discarded. The psychomotor item also contained opposing questions; however, we separated this item into two distinct questions, as both statements appeared to be associated with mental health. Previous studies made a similar modification to the PHQ-9 to enhance clarity for participants (Brown et al., 2013; Poongothai et al., 2009). We also incorporated local idioms, such as ‘mental pain’ as this term was used to describe depression in rural areas of northern Karnataka. A number of qualifiers were also included to further enhance relevancy, by providing culturally appropriate examples based on findings from FGDs. Esler, Johnson, and Thomas’s (2007) evaluation of PHQ-9 called for more “flexibility” within the tool to allow the interviewer to alter wording and provide context-specific examples to enhance cultural validity (p. 262). By incorporating these recommendations into the PHQ-9, researchers found the adapted instrument to demonstrate good reliability and validity in detecting depression among the Indigenous population in Australia (Esler, Johnston, Thomas, & Davis, 2008).
The rate of suicide in south India is reported to be highest among young women in comparison to young men (Aaron et al., 2004). Additionally, in the focus groups, adolescent girls discussed the association between suicidal thoughts and gender discrimination young women face in their communities. Suicidal ideation is an important aspect of mental health for this population; however, the intervention team was concerned that it would be unacceptable to inquire about self-harming behaviours in the villages, as suicide is illegal and highly stigmatised. However, during the Free Listing exercise, the outreach workers understood this question to be acceptable. Moreover, by avoiding questions of self-harm, we may reinforce stigma and further isolate those at risk of suicide.
Still, outreach workers cautioned against the use of the original PHQ-9 item, ‘thoughts you were better off dead, or of hurting yourself in anyway’, as reporting bias linked to issues of confidentiality was likely. The outreach workers recommended a non-intrusive approach to addressing suicidal thoughts to minimise reporting bias. We proposed ‘thinking life was not worth living’, to alleviate participants’ stress in disclosing their experiences with suicidal thoughts. This statement has been used in the literature as an indicator of suicidal ideation (O’Dwyer, Moyle, Pachana, Sung, & Barrett, 2014; Thomas, Crawford, Meltzer, & Lewis, 2002).
Although self-harm behaviours is a topic that is prone to under-reporting due to legal and social consequences in India, measures can be taken to minimise under-reporting (Pillai et al., 2009). For instance, in Pillai et al. (2009), participants were made aware of the precautions taken to maintain their anonymity. van Ommeren et al. (1999) used a similar design to investigate alcohol use among women in Nepal, a cultural taboo. Therefore, introducing the mental health questionnaire by including a statement to reinforce confidentiality and normalise psychological challenges will be important to minimise reporting bias and distress.
Although the PHQ-9 appeared to share similarities to the expression of depressive symptoms in this population, persistent worry, isolation, and externalised behaviours were common representations of mental health not captured by this tool. Although anxiety was connected to trouble sleeping, poor appetite, and concentration, there were no items in PHQ-9 that directly addressed the frequency of worried thoughts. As anxiety features were cited often in relation to the adversities girls face in their communities, we believe that including anxiety-related items in the questionnaire is important to accurately measure their psychological health. Therefore, we recommend the inclusion of the GAD-2, as it demonstrated relevancy based on FGDs and has brevity. Although the GAD-2 is seldom used with adolescents in LMIC, this measure has demonstrated good validity when used in diverse settings (García-Campayo, Zamorano, Ruiz, Pérez-Páramo, López-Gómez, & Rejas, 2012).
Internalised behaviours were cited repeatedly across the focus groups. Girls appeared to keep feelings of sadness and anxiety hidden from others, isolating themselves within their home when experiencing troubled thoughts. The striking fact was that girls felt like no one would listen to them. Social isolation can have devastating consequences to the emotional wellbeing of adolescents. Manoranjitham, Rajkumar, Thangadurai, Prasad, Jayakaran, and Jacob (2010) found that psychological stress and social isolation, over psychiatric morbidity, were major risk factors leading to suicide in rural south India. Therefore, an item which captures the loneliness and isolation attributes of sadness would be essential, and would further enhance the local validity of this instrument.
Lastly, the presence of externalised behaviour was also recounted in FGDs, albeit mentioned less often. They described girls becoming atypical, in the form of becoming verbally aggressive at others for no apparent reason. This was also found in Betancourt et al. (2009) while examining local concepts of mental health in children in a post-conflict setting. Authors perceived this to be reflective of the children’s expression of sadness through irritability, which is a feature of depression in youth (Betancourt et al., 2009; Birmaher et al., 1996). Esler et al. (2007) also found anger as a likely manifestation of psychological distress, and therefore, included it to improve the acceptability and relevancy of PHQ-9. In a subsequent study, the adapted PHQ-9 proved to be a reliable and valid measure (Esler, Johnston & Thomas, 2007). Haroz et al. (2014) also found that with the addition of locally derived items, their instrument had more depth, and performed as well as standardised items.
Limitations
Though this research fulfilled its aim, it had its limitations. The diversity of backgrounds, perspectives and knowledge levels of adolescent girls’ mental health was limited. Time and resource constraints made it impossible for us to consult clinical experts in Karnataka, although attempts were made to include local clinicians. Additional limitations included the small number of FGDs and the homogenous girl sample; adolescent participants were members of the parivartan group – a sports group which comprises part of the Samata intervention. Although adolescent girls were from a Scheduled Caste or Scheduled Tribe, they may not be representative of all girls in these districts. In addition, we were unable to assess the acceptability of the PHQ-9 response set (i.e., technical equivalence).
There were several drawbacks to the topic guide and the qualitative data collected. In two FGDs, we were unable to review the PHQ-9 comprehensibly due to time constraints. Many of PHQ-9 items presented were probed for relevancy; however, there were a few items that were only probed for comprehensibility due to time constraints. Two statements from the 9-item questionnaire ‘feeling bad about yourself’ and ‘feeling tired and less energy’ were only included in one adolescent girl FGD due to time constraints. Therefore, our assessment of the semantic and content equivalence for these items was limited. Further, we were unable to directly assess the appropriateness and acceptability of the item related to suicide and self-harm with adolescent girls, due to concerns presented by the Samata team, given their experience working with community. Although suicide was discussed openly by adolescent girls during the FGDs, their comments were in relation to their peers, not their personal experiences. Our insight into how girls would respond to such a question is limited, as it is solely based on the opinion of outreach worker participants.
Lastly, the qualitative data set used for this study could have been influenced by the positionality of the investigators as well as the absence of inter-coder reliability.
Conclusion
Despite these limitations, this study supports the feasibility and importance of utilising Free Listing methods to assess the cultural validity of Western mental health concepts. Our findings highlight the importance of researchers moving beyond translation and back-translation of mental health survey instruments to assure cultural appropriateness and acceptability. We illustrated the necessity for the involvement of service providers as well as adolescent girls themselves to assess local mental health priorities, and the acceptability and appropriateness of standardised instruments used in this context. Their voices were essential in modifying the PHQ-9 items and including additional survey items to reflect local indicators of psychological distress. By adapting a Western mental health tool to be more reflective of local meaning and experiences in the communities with which we are working, the risk of misrepresentation and error decreases. An adapted mental health instrument provides researchers with an appropriate tool to measure psychological distress among adolescent girls. In turn, this will contribute to Samata researchers’ overall aim of improving the quality of life for adolescent girls in Karnataka. Future research should consider assessing the psychometric properties of the adapted screening measure among this population of girls.
Footnotes
Acknowledgments
Project Samata is funded by the UK Department for International Development (DFID) as part of STRIVE, a 6-year programme of research and action devoted to tackling the structural drivers of HIV (![]() ), the World Bank and the Government of Karnataka. Tara Beattie is supported by a British Academy mid-career fellowship. The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the UK Department of International Development, the World Bank, the Government of Karnataka or The British Academy.
), the World Bank and the Government of Karnataka. Tara Beattie is supported by a British Academy mid-career fellowship. The views expressed herein are those of the authors and do not necessarily reflect the official policy or position of the UK Department of International Development, the World Bank, the Government of Karnataka or The British Academy.
The authors would like to thank the study participants for their enthusiasm and participation in this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.