
Abstract
What happens when lesbian and gay people, who are more likely to be childless and single than their heterosexual peers, get older and need support and care? Who can they turn to? In addressing this question, this article draws on data collected as part of a wider project concerning the housing preferences, experiences and concerns of older LGBT people in the United Kingdom. The article explores the social networks that older lesbian and gay people expect to utilise later in life if they require different forms of care. It uses social capital theory and considers the role of ‘families of choice’ in older lesbian and gay people’s lives, questioning whether such bonds may or may not be useful for different forms of care and support older lesbian and gay people may require late in life.
Introduction
Existing evidence suggests that compared to heterosexual people who tend to rely more on their family of origin for help, support and care later in life, lesbian and gay people rely more on a ‘family of choice’, comprised of friends, partners and ex-partners (Allen and Roberto, 2016; Brennan-Ing et al., 2014; Weeks et al., 2001). However, what has been under-explored in research so far is the question of who older lesbian and gay people say they will turn to for specific forms of care and support, together with their concerns and preferences regarding the characteristics of the people who undertake this and in what context it will take place. In effect, the question who to turn to remains pertinent and this article seeks to contribute to knowledge in that respect.
In this article we draw on findings from the Secure, Accessible, Friendly, Equal (SAFE) Housing study, the largest mixed-methods study to date of older lesbian, gay, bisexual and trans (LGBT) people’s housing preferences, concerns and experiences in the United Kingdom (UK). The study examined housing in its broadest sense, including questions about the forms of support and care individuals may need to remain in their current home and the types of housing with care they might prefer should they need it towards the end of their lives. In this article we focus solely on survey responses of older lesbian and gay individuals in the study, because of issues of statistical power related to older bisexual and trans individuals. Although the literature we draw on frequently comes from studies that relate to older LGBT people, we have differentiated lesbian and gay responses from those of bisexual and trans people where possible.
There have been relatively few studies concerning older lesbian and gay people’s housing and care needs and preferences, but some research has suggested that like their heterosexual counterparts, they want to remain in their own homes for as long as possible in later life (Gerlach and Szillat, 2017; Wallace et al., 2011). These and other issues, such as fears about discrimination in retirement housing and care homes (Willis et al., 2014) affect how older lesbian and gay people view their future housing and especially who they think they would turn to for help and support. In addressing these issues here, we draw on theories of social capital, with particular reference to the connections and social relationships that older lesbian and gay people expect to utilise later in life, if they require care and support and require alternative forms of housing. The first section of the article therefore discusses social capital theory (SCT) and considers its suitability for assessing networks of care and support amongst older lesbian and gay people towards the end of their lives. Subsequently, the article considers the significance of family of choice and social connections which capture the commitment of chosen, rather than fixed, relationships and ties of intimacy, care and support. Subsequently, the methodology of the SAFE Housing study is outlined. Key findings related to older lesbian and gay people’s preferences and concerns about support, housing and care are then considered, before the article discusses the ramifications of these for theory and future research and policy.
Theoretical background
Housing preferences and receiving a good quality of care are not individual choices. Both involve a social network (relatives, friends, neighbours, etc.) and connections and participation in wider communities and society (being part of an organisation, neighbourhood, support group, etc.). Networks and connections to others are an important resource for social, practical and emotional support as well as care for older lesbian, gay and bisexual people later in life (Brennan-Ing et al., 2014). SCT understands – as a function of social structure – that social relations (e.g. social networks and relationships) are a resource that can generate advantages for individuals – within that structure (Erosheva et al., 2016). Putnam (2000), for instance, emphasised the relevance of people’s social ties and bonds in his work on social capital: those ‘connections among individuals – social networks and the norms of reciprocity and trust that arise from them’ (Putnam, 2000: 19). Evidence suggests these have a positive impact for an individual’s well-being, whilst a lack of social capital can lead to isolation for an individual and poorer outcomes later in life (King, 2016). However, as King (2016) has also noted, conceptualisations and understandings of social capital need to be queered, that is connections and networks that lesbian and gay individuals form with institutions are often marked by heteronormativity (the privileging of heterosexuality) including health care systems. Hence, the link between ‘good care’, ‘poor care’ and social capital is already structurally unequal for lesbian and gay people.
SCT differentiates two important types of social connections and relationships. Bonding refers to connections, relationships and forms of trust between people within one’s social group, people with who one has something in common, as in the case of sexual identity groups. Bridging refers to broader alliances, wider social relationships and connections to those who are dissimilar. Both are related to each other (see King and Cronin, 2016; Lin, 2001) – minority groups, such as lesbians and gay men, form connections of trust and reciprocity with each other, but they are also reliant, to a greater or lesser extent, on wider society, i.e. heterosexual people. However, it is not simply the existence of networks and connections that are important. Lin (2001) refers to the strength of connections, to strong and weak ties, which also play a part in the usefulness and effectiveness of networks. Hence, individual lesbians and gay men may have bonds and bridges, but the strength of them may differ and therefore their ability to rely on them when necessary will also vary.
Why networks matter for older lesbian and gay people
Older lesbians and gay men rely more on family of choice later in life, especially for forms of support and care than their heterosexual peers (Heaphy, 2009; Weeks et al., 2001). Whilst heterosexual people are more likely to turn to spouses and children, as well as more distant relatives before they ask friends for support and care, this is less so for older lesbian and gay people (Brennan-Ing et al., 2014; Lehr, 2003). Relationships with friends and ex-partners play a particularly important role (Heaphy, 2009). In part, this reflects the greater likelihood that older lesbians and particularly gay men are childless. For instance, studies conducted in the UK and United States of America indicate that older lesbians are more likely to have children than older gay men, but still less likely than the heterosexual average (Fredriksen-Goldsen et al., 2013; Guasp, 2011). Regular face-to-face contact with members of one’s family of origin is also higher for older heterosexuals. In a UK survey, 57% of the heterosexual respondents saw members of their family of origin either daily or more than once a week, whilst 28% of the lesbian, gay and bisexual respondents did so (Guasp, 2011). This has led some researchers to suggest that friends are the ‘backbone of the social support network’ for older lesbian and gay people (Braukmann and Schmauch, 2007; Brennan-Ing et al., 2014: 44; Gerlach and Szillat, 2017; Hughes and Kentlyn, 2011). Nevertheless, Kneale (2016) has pointed out that compared to their heterosexual peers, older LGB people are less likely to have seen a friend the previous day (63.9% versus 72.1%) (Kneale, 2016). Older lesbians and gay men are also more likely to be single and to live alone in later life than their heterosexual peers (Guasp, 2011; Wallace et al., 2011).
Cornwell (2009), however, emphasises a differentiated perspective on social networks. The size and the diversity of a social network are as relevant as indicators for a network’s bridging potential in accordance with SCT (Erosheva et al., 2016; Putnam, 2000). In a recent study concerning the social networks of older LGBT people (Erosheva et al., 2016), the median size was 36, with trans participants reporting the largest network size (M = 54.5) and gay men the smallest (M = 31). Women also have larger and more diverse social networks than men (Erosheva et al., 2016).
Heaphy et al. (2004) demonstrate that for older LGB people, partners are the main source for help and support if care is needed (50% for lesbians: 29.9% for gay men). Relationships to siblings, nieces and nephews often fail as a source of help and support (Heaphy et al., 2004). Compared to gay men, lesbians have a larger family network who provide assistance to a greater extent. However, they also report more negativity from such family networks (Brennan-Ing et al., 2014). One study suggested that LGB people are up to four times more likely to turn to a friend if they are ill and/or need help than heterosexual people (Guasp, 2011). However, Misoch (2016) has pointed out that LGB people have age-homogenous social networks in later life, potentially limiting the possibilities of providing support.
Because of the social network characteristics of older lesbians and gay men, they may depend more on formal services as well as institutional housing with care services (Guasp, 2011). Yet this is not straightforward. For instance, older lesbian and gay people describe feelings of discomfort in their use of older adult social services because of institutional heterosexism, the assumption that everyone is heterosexual (Westwood, 2016). Studies have shown that older lesbians and gay men, despite a relatively high dependency on mainstream care services for older people, are often uncomfortable in them. Gerlach and Szillat (2017) found that 80% of the gay men said residential care homes are not aware of LGB people (similar figures were provided by older lesbians, see Braukmann and Schmauch, 2007).
All this evidence raises further questions about who older lesbians and gay men will turn to later in life for care and support and whether they believe they can rely on a family of choice or family of origin or both. It also has implications in terms of future housing with care choices and whether lesbians and gay men want the same options. These issues were explored in the SAFE Housing study and we will now outline its methodology, before discussing relevant findings.
Methodology
Research design
The SAFE Housing study took place in 2016 and the research design included a survey and four focus groups. For the purposes of this article, we will be discussing the survey responses only.
Recruitment
The survey was open to people 50 years of age or older, who self-identified as LGBT and who lived in two areas of England: a major inland city and a provincial county with rural communities. It was administrated both online (via a survey data collection platform) and offline (papers copies were also available). A purposive sampling strategy was used to try to ensure representation across the LGBT spectrum. This was facilitated by working with key older LGBT charities and forums in the two areas chosen who had agreed to disseminate the survey via their online platforms and mailing lists, along with a call for focus group participants. The study was submitted to the University of Surrey ethics committee and received a favourable opinion. The study also adhered to the ethical principles of the British Sociological Association.
Survey measures
Survey questions covered the following topic areas: neighbourhood and community, current home environment, expectations about housing, care and support, social networks and demographic information. Most questions were specifically formulated for this study, although ones about housing tenure were drawn from existing surveys. The questionnaire was piloted to determine clarity and accessibility with a small group of experts comprising academic researchers who research LGBT ageing, members of older LGBT support organisations and older LGBT community members.
Characteristics of the sample
One hundred and seventy-five people completed the survey in enough detail to provide a range of useable responses, although not all participants completed all questions. Fifty per cent of respondents self-identified themselves as women, 47% identified themselves as men and 3% gave their own terms (7% of the sample specifically identified as trans). Forty-two per cent of the sample identified as lesbians, 43% as gay men, 5% as bisexual women, 2% as bisexual men, 2% as heterosexual women, 1% as heterosexual men, 4% provided their own terms and 1% preferred not to say. In terms of ethnic diversity, 10% of the survey sample identified as having a Black, Asian and Minority ethnic (BAME) identities/background, 90% identified as White British or White Other. 1 In terms of age cohorts, most of the sample were in ‘younger-old’ groups: 50–54 years (30%), 55–59 (22%), 60–64 (25%), 65–69 (13%), 70–74 (5%), whilst 5% of the sample were over 75 years of age.
Two-thirds of the entire sample were in some form of relationship, whilst a third indicated that they were single. Despite this, considerable numbers of the sample of gay men and lesbians lived alone: 42% of the gay male participants lived alone and 41% of the lesbians. Seventeen per cent of the lesbian participants had children compared to 9% of the gay men. Most respondents (92%) were currently living in independent accommodation without formal support.
Analysis
Descriptive statistics were produced for all questions to demonstrate the frequency of responses and those relevant to the article are reported below. In addition, where relevant for the purposes of this article, we have conducted tests of significance and association and these are reported in the results below. 2
Findings
In this section of the article we address first who older gay and lesbian survey respondents thought they would turn to for support, in terms of informal sources and then their feelings about receiving more formal support in their home. We then examine findings concerning their feelings about moving into residential housing with care.
Imagining future sources of support
As noted earlier, older lesbians and gay men are likely to be connected to members of both families of origin and of choice, although the latter are said to predominate. This has ramifications for later life and who they might envisage they would turn to for specific types of support. As Table 1 indicates, the survey asked respondents to indicate who they might turn to for emotional support, practical help, personal care and full-time assistance. Respondents were asked about different groups of individuals, representing informal support from members of family of origin and choice. In effect, the question was asking them to indicate who they would turn to and whether they were likely to turn to them – an assessment of the strength of a tie (see Putnam, 2000).
Who respondents would turn to for specific forms of support.
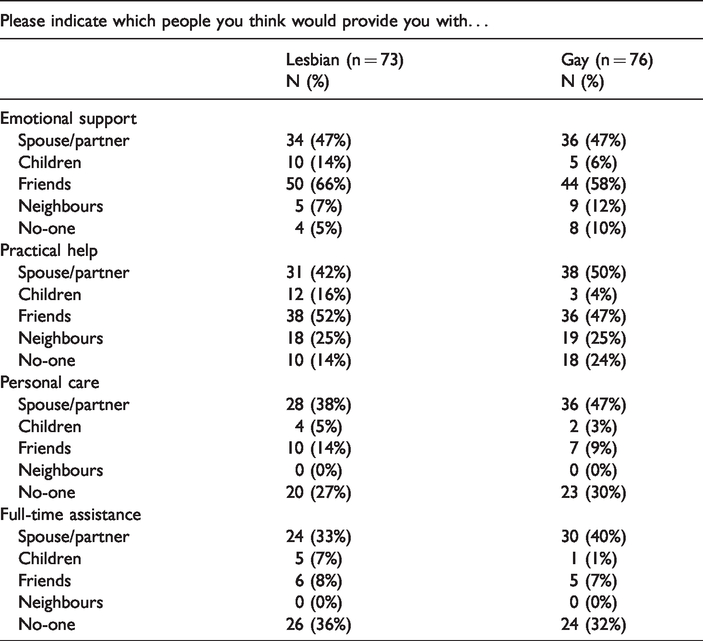
As Table 1 indicates, a spouse/partner was viewed as significant person for all categories of support, although it is very notable that friends were also viewed as the most relevant source for emotional support and practical help. Indeed, for emotional support, 66% of the older lesbians and 58% of the older gay men believed they would rely on friends. The number of cases is 149 as only gay and lesbian respondents are included and some respondents chose not to answer this specific question.
For personal care and full-time assistance, perhaps the most intensive form of support, friends were still perceived to be a significant source of help, second only to a spouse/partner, but to a much lower degree than emotional support and practical help. Neighbours were not viewed as possible sources of these forms of support at all. Furthermore, it is important to note that in all categories other than emotional support, many respondents felt they had no-one to turn to. This was especially the case for full-time assistance.
Children were seen as a relevant source of help for some participants and there were expectations that they would support them in later life for emotional, practical and personal help. Although not statistically significant, there were gender differences, as the lesbians were more likely to have children than gay men. However, it is worth recalling that compared to older heterosexual people, only a minority of older lesbians and gay men will have children and therefore they cannot be seen as a widespread source of support.
The durability and depth of friendships noted above may not be significant enough for older lesbians and gay men, who consequently must rely on more formal sources of support. This means opening one’s home to others was something that was investigated through the survey with questions concerning how comfortable, or not, older lesbian and gay respondents felt about certain groups of people entering their homes to provide support.
Figure 1 shows the results regarding feelings of comfort/discomfort for five groups of people who may enter the homes of older people later in life to provide support and services: trades persons, health professionals, public officials, home care workers and neighbours. As the figure indicates, there were some differences between them.
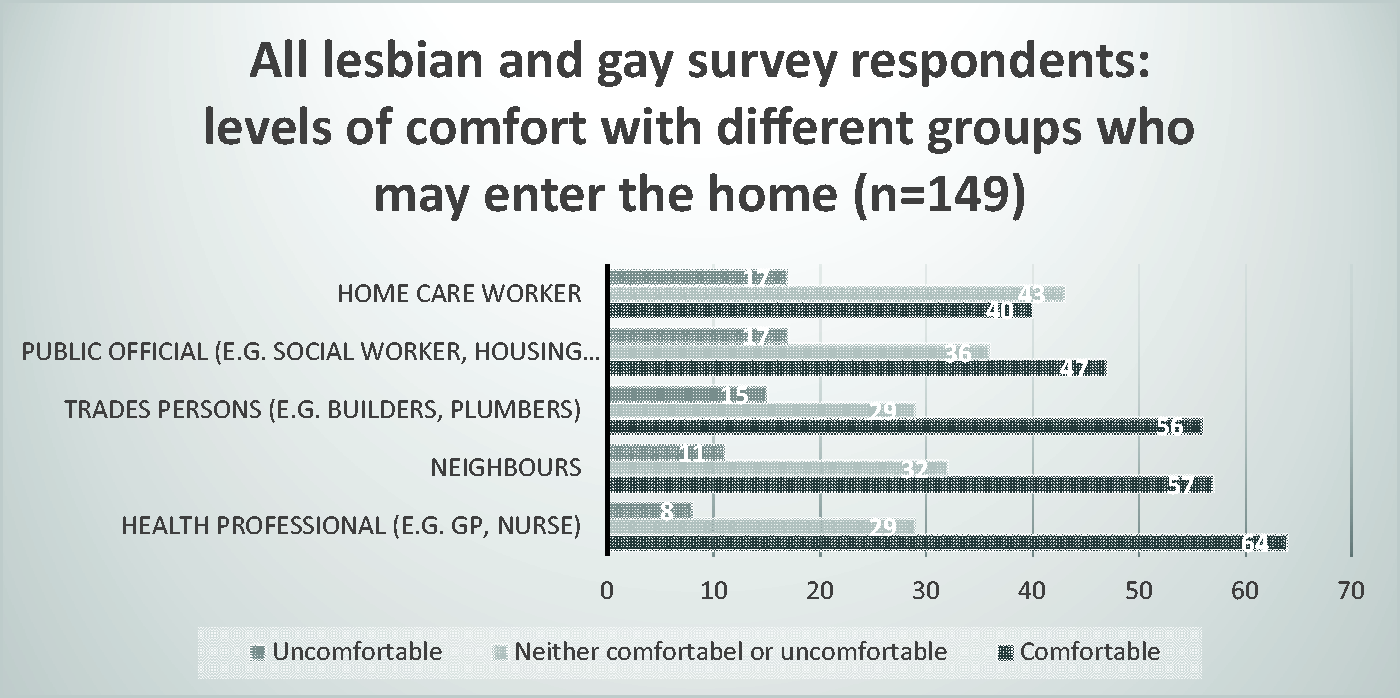
Feelings of comfort/discomfort and who enters the home (in %).
Figure 1 combines the responses of older lesbians and gay men since there were no significant gender differences when a Chi-square test was conducted. The figure indicates that mostly respondents were comfortable with all these different groups of people entering their homes. However, it is also clear that respondents were most comfortable (64%) with health professionals, such as their doctor (GP) or a nurse, suggesting that these medical professionals are deemed to be trustworthy. Fifty-six per cent of the survey respondents felt comfortable with tradespeople who undertake repairs coming into their home, but less than half (40%) were comfortable with home care workers, suggesting that those who provide a level of intimate care may be viewed more warily (King and Stoneman, 2017). This may also relate to professional reputation and the type of care they deliver. In comparison to other health professionals, home care workers are often paid less and stay longer in the home of a client providing more personal care. It indicates that reliance on formal care is of concern and, moreover, that bridging forms of social capital needed for care later in life may have a higher trust premium.
Needing formal care at home
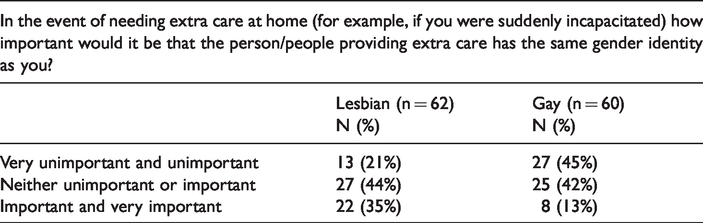
As the previous section has indicated, older lesbians and gay men have concerns about formal home care workers entering their home to provide support. For this reason, the survey also asked respondents about preferences regarding these home care workers. In particular, they were asked if they had preferences about their carers’ gender identity and/or sexuality. The findings are presented in Tables 2 and 3.
Needing extra care at home by gender identity of carer.
Needing extra care at home by sexuality of carer.
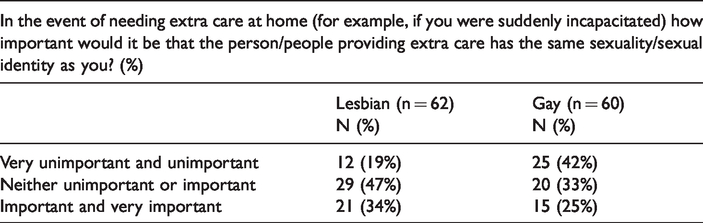
Table 2 indicates that although considerable numbers were ambivalent, a third (35%) of the older lesbians who completed this question in the survey thought it was ‘important’ or ‘very important’ that they had a carer of the same gender identity as themselves compared to only 13% amongst gay men. The association between gender identity and needing extra care is 0.35 (Cramer’s V) and statistically significant at the level of p = 0.004.
When the same question was asked, but in relation to sexuality/sexual identity (Table 3) it is again possible to see a gender difference. Nineteen per cent of the older lesbians who completed this question deemed it ‘very unimportant’ or ‘unimportant’ compared to 42% of the older gay male respondents. The association is less strong (Cramer’s V = 0.27) than that regarding gender identity and significant only at the level of p = 0.06. However, it is worth noting that 25% of the older gay men did regard it as ‘important’ or ‘very important’, almost double what they thought for gender identity.
Formal housing with care and support
Respondents were asked about future formal housing with care and support. As Table 4 indicates, the majority of older lesbian and gay respondents did not want to live in a mainstream care or nursing home, for anyone if they had the opportunity to live in accommodation specifically for LGBT people. Fifty-two per cent of the lesbians and 42% of the gay men selected ‘undesirable’ if given the option of living in a care/nursing home for anyone in the event that they needed accommodation with high levels of extra support. Over half of those who completed this question in the survey, both older lesbians and gay men, regarded LGBT-specific housing as ‘desirable’.
Desirability of different types of formal housing with care.
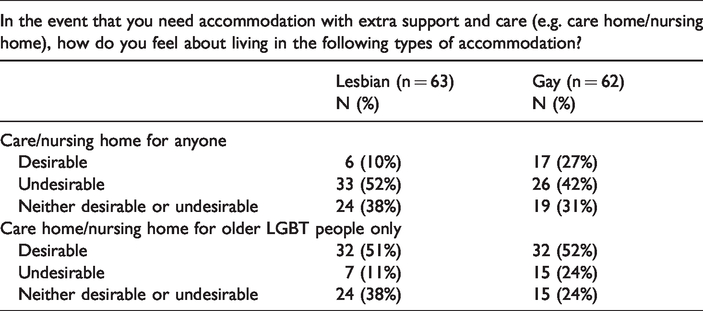
It was noticeable that the number feeling that care/nursing homes for anyone were desirable was generally low, although there was a clearer gender difference: 10% of the older lesbians, compared to 27% for gay men. Indeed, there was a stronger preference for gender-specific housing amongst the lesbians respondents, where the gay men disliked housing for anyone to a lesser extent. Further inferential analyses have shown that there is only a weak association between the preference for an LGBT-specific care home and feeling part of a LGBT community (Cramer’s V = 0.18; significant at the level of p = .09), and a similar association between gender identity and the preference for LGBT-specific care home (.20; significance level of p = 0.08). Only 9% (n = 11) of the gay and lesbian respondents who do not feel part of a LGBT community favour a LGBT-specific care home compared to 42% (n = 53) of lesbian and gay respondents who feel part of it. Indeed, 49% of the lesbian respondents who feel part of a LGBT community do not want a care home for anyone (desirable 10%; neither, or: 37%). It should be noted that the number of cases of several combinations was below 20.
Discussion and conclusion
In terms of imagining who to turn to informally, if in need of future care and support, it was clear that most survey respondents in the SAFE Housing study felt that they did have people they could turn to, particularly for emotional and practical support/help. These findings echo those of other studies (Brennan-Ing et al., 2014; De Vries and Blando, 2003; Weeks et al., 2001), which indicate that older lesbians and gay men predominantly rely on family of choice later in life, but with the added caveat that those networks are only seen as applicable for certain forms of support and rarely focus on care needs. For more intensive and potentially intrusive forms of support, such as personal care and full-time assistance, the majority of the survey respondents in our study indicated they would turn to a spouse or partner (if they had one) or indicated that they had no-one to turn to. In effect, when older lesbians and gay men imagine a ‘fourth age’ (Laslett, 1987), considerable numbers in our study did not envisage family of choice members providing support when they needed intensive forms of care. Friends, the backbone of support in older age for older LGBT people (Brennan-Ing et al., 2014), appear to be a fragile source of support when facing these needs in our study. Hence, when compared to the support people with HIV/AIDS received from LGBT communities, long-term general care seems to be an overlooked challenge. Even if older lesbian and gay adults can turn to friends in their social network, they still have to rely on wider support.
As we noted, older lesbians and gay men are more reliant on formal services. Yet in imagining turning to these, concerns were expressed. First, when asked about how comfortable they were with different groups of people entering their home, again it was possible to see from our findings that those groups who provide more intrusive forms of support, e.g. home care workers, were more concerning, receiving the lowest score of all groups amongst the selection available. Second, when needing formal care at home, it was apparent that having carers who were similar in terms of gender and sexuality was more important, especially for older lesbians. Finally, when our respondents imagined they would need residential care and support, both older lesbians and gay men in the survey expressed a preference for LGBT-specific forms of housing.
These findings add to the weight of evidence concerning social capital and older LGBT people too (King and Cronin, 2016). Many of the preferences and choices that the older lesbians and gay men suggested in our study regarding support, i.e. when they were at a point in their lives when they were more vulnerable and possibly frailer, are indicative of the importance of bonding social capital – they wanted and expected support to be provided by networks of people who were like themselves. For instance, support from a family of choice member is an important form of bonding. However, this also extended to formal services where the possibility of bridging social capital comes into play. Respondents expressed a preference for those services being provided by those of a similar gender identity and/or sexual orientation to themselves or to be cared for in LGBT-specific environments; in effect, bridges that are more like bonds were seen as desirable and valued, although it is worth noting that there was variability here. First, we found similar gender differences noted by others (Westwood, 2016) and second ambivalence too – not all older lesbians and gay men want the same type of formal service or service provider as we noted in Table 4. Indeed, other evidence we have presented shows that bridging forms of social capital remain important but being able to trust services provided by these dissimilar others, e.g. heterosexual service providers, is imperative (see Morey, 2007). Yet evidence also exists that formalised social support and care are not equal – both are likely to be sources of discrimination and sometimes outright prejudice (Lottmann, 2020; Westwood, 2016).
There are important policy implications from our findings, ensuring that all care and support services are LGBT-inclusive and fully comply with the UK Equality Act (2010) and that these services are ‘culturally competent’ and staff have received adequate education and training. In this respect, staff education initiatives in the UK such as Opening Doors’ Pride in Care quality standard, Stonewall Housing’s Inclusion Standard or others such as The Pink Passkey in the Netherlands (see Linschoten et al., 2016) are important initiatives that service providers should consider.
Our findings also provide further support for the view that social capital itself and how it is conceptualised in relation to older lesbian and gay people later in life needs to be ‘queered’ (King and Cronin, 2016). By this we mean that how social networks are measured and understood will be qualitatively different for lesbian and gay people, compared to their heterosexual peers and it is important that these differences are captured. If a heterosexualised model of social capital predicated on family of origin is imposed on lesbian and gay people, it is a form of heterosexism: a form of discrimination, appearing under the guise of equality (Castro Varela and Lottmann, 2018; King and Cronin, 2016). We also believe that it is important that other methodologies are used to explore the importance of social networks and their influence on the care and support choices of older lesbians and gay people later in life. More research is therefore needed into the distinct social networks of care and support that older lesbian and gay people require, exploring the depth of those ties and some of the complexities we have pointed to. The same applies to the social networks of bisexual and trans people, which we have been unable to explore here.
This article has illustrated important findings regarding housing and care preferences amongst older lesbians and gay men. However, the study on which this article is based does have some limitations, especially regarding the needs of specific groups of older LGBT people, particularly those from working class and minority ethnic backgrounds, LGBT people older than 75 years of age, and gender diverse and nonbinary people. Taking these limitations into account means that it is even more relevant to focus on the potential social risks that a more diverse group of older LGBT people may experience. Moreover, a comparative study with childless older heterosexual people could also reveal interesting insights regarding lifestyles and life course decisions.
To address some of the limitations in our own and other LGBT ageing research we have been using agent-based modelling (ABM), a form of social simulation computer modelling. This draws on existing data but also theory to populate a virtual environment with ‘agents’ who make decisions concerning some phenomenon (see Gilbert and Troitzsch, 2005). ABM is often used to generate new ideas and ways of considering an issue or problem, especially when existing data are incomplete or have limitations. For us, this has involved LGBT ‘agents’ making choices about domiciliary care or residential care with different criteria, including LGBT-inclusivity. In our model, their choices are influenced by a Social Network Dependency Index score that is based on different degrees of bonding and bridging social capital which then impacts likelihood of needing care, especially formal care. Differences within a heterogeneous group of older LGBT people regarding dependency on formal care infrastructure are used with findings from the SAFE Housing study on the preferences of older LGBT people for LGBT-affirmative care. Our ABM is therefore shedding new light on ways of addressing these issues beyond a binary of quantitative and qualitative methods and measures (Lottmann, 2019).
Footnotes
Acknowledgements
The SAFE Housing study was conducted by Professor Andrew King, Dr Paul Stoneman, Dr Sue Westwood and Dr Ann Cronin in 2016 with the support of Opening Doors, Stonewall Housing and Safe Age No Discrimination (SAND).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ralf Lottmann has received funding from the European Union's Horizon 2020 research and innovation programme under the Marie Sk?odowska-Curie grant agreement no. 749760 for research of this article. The SAFE Housing study was funded by the University of Surrey.