
Abstract
In the (near) future, a growing number of older LGBT people will ‘age in place’, receiving health and social care in their homes and wider ageing environments until a very advanced age. This article discusses the results of a survey research among 115 LGBT people aged 65 years and over who are ageing in place and who are weekly and monthly receivers of health and social care services, and follow-up interviews with 10 people. The research was situated in the Netherlands. The results show that older LGBT people’s experiences with ageing in place are related to differences in how ageing environments are able to accommodate LGBT lifestyles. The results further shed light on the meaning of receiving health and social care at home as an older LGBT person, and the ways in which LGBT life histories and identities are expressed in care relationships, both in verbal and in home-making practices. Finally, the results suggest that the links between older LGBT people and the wider LGBT community are vulnerable, and neighbourhood-based activities may not be sufficiently responsive to older LGBT people.
Keywords
Introduction
In the (near) future, a growing number of older LGBT people will ‘age in place’, living at home and receiving health and social care until an advanced age. This article discusses the results of a survey research situated in the Netherlands among 115 LGBT people aged 65 years and over who are ageing in place and who are weekly and monthly receivers of health and social care services, and follow-up interviews with 10 people. The article tries to understand these experiences by bringing them into dialogue with ideas from the literature on ageing in place (AIP) and LGBT ageing, contributing to this literature by engaging more in-depth with older LGBT people’s experiences with AIP and care, and the meaning of the home and the wider ageing environment. The research question asked is how older LGBT people are enacted as care receivers, that is, how do they respond to the care they receive, and how do they link it to their life histories and identities? Here, the notion of care-receiving as responding to care is borrowed from Tronto (2013).
The article starts by discussing AIP as both a policy and an academic concept, the role of the homespace within AIP, and the attention hitherto paid to AIP in LGBT ageing research. This is followed by a discussion and critical reflection of the methods of data collection and analysis used. Three overarching themes have resulted from this analysis, discussed at length in the subsequent three sections. The ensuing conclusion offers a discussion of the limitations of the study, the contribution to the literature on LGBT ageing and AIP, policy recommendations and a brief outlook on future research.
LGBT and ageing in place
AIP, as an umbrella term for the experience of living in one’s home environment as an older person for a prolonged period of time, is used both in policy documents and academic literature (Jansen et al., 2018). AIP as a policy concept can be traced back to several initiatives launched by the World Health Organisation (WHO) during the 1990s and early 2000s (Phillipson, 2015). In these initiatives, the WHO called attention to the need to develop ‘age-friendly’ cities for urban ageing populations worldwide. Underpinned by WHO’s ‘Global Age-Friendly Cities’ guide (WHO, 2007), many cities have crafted strategic and practical policies, often accompanied with place-based approaches such as a district or neighbourhood approach. In this way, cities aim to address the social and physical ageing environment simultaneously, investing in the quality of housing and public space, and in local community building (Jansen et al., 2018). In the Netherlands, attempts are made to integrate services provision in neighbourhoods, with providers of health care, social care and housing jointly operating venues, and calling in each other’s expertise. Place-based integrated service provision is part of a neoliberal transfer of responsibility for supporting vulnerable populations to local governments, accompanied by budget cuts. This may imply older LGBT people find themselves in trimmed-down localised structures of provision with little attention to sexual and gender diversity.
AIP as an academic concept resonates with the classic environmental-gerontological notion of ‘person–environment fit’ (Lawton, 1983), the degree to which the needs associated with continuing daily life activities and maintaining autonomy of an older individual match with environmental conditions. Oswald et al. (2005) found a positive relation between person–environment fit and attachment to the wider neighbourhood. Even in challenging inner-city neighbourhoods, older people’s daily well-being remains positively affected by their place attachment (Buffel et al., 2013; Smith, 2009). Peace, Holland and Kellaher (2011) show that older people adapt their behaviour to balance environmental stress in the context of both the home and the wider ageing environment. When adaptation is no longer sufficient to prevent a decrease in well-being, older people start to consider alternative options for (more) care and aid at home, or for relocation – this process has been referred to as ageing in the right place, see Golant (2015).
Moving away from behaviouralist adaptation strategies, research on the homespace in AIP settings has focused more on issues of meaning-making. Sixsmith, Sixsmith, Fange et al. (2014), for example, have found that, compared to middle-age, the meaning of the home changes from a place from where to start from and return to from outdoor activities to a place for meaningful activity all day round. Also, the materiality of the home (arrangement of furniture and personal items) helps older people to emphasise life-course events and significant others of the past and the present (Sixsmith et al., 2014). In addition, attention has been called to the increasing publicness of the home as a space of care (Cloutier et al., 2015; Milligan, 2003).
The literature on older LGBT adults has only recently begun to discuss AIP, charting expectations and preferences for the future. Boggs, Dickman Portz, King et al. (2017) find that most older LGBT people prefer AIP, partly because they fear rejection and exclusion in nursing and care homes. To facilitate AIP, older LGBT people would like to have specific buddy programmes, and providers that are knowledgeable concerning LGBT life histories and identities (Boggs et al., 2017). Willis, Raithby and Maegusuku-Hewett (2018) identify problems with accessibility of social and scene spaces for older LGBT people living in rural areas. Both studies report mixed feelings with respect to receiving health and social services at home. While some people anticipate not being understood or being rejected by caregivers, others have positive experiences, and yet others are hopeful about being able to find LGBT-identifying caregivers (Boggs et al., 2017; Willis et al., 2018). The social support networks of older LGBT people ageing in place may include relative large shares of partners who are not legal relatives and friends (Croghan et al., 2014; Hawthorne et al., 2020; Hughes and Kentlyn, 2011).
In her overview of the literature on the meaning of social spaces to LGBT people, Formby (2017) posits the home as a contested space, at once a safe space and a space of fear, for example of neighbours. Pilkey (2014), on the basis of research among middle-aged and older gay men, finds a diversity of domestic materialities applied in the homespace. These range from explicit, such as the visible presence of homo-erotic objects, to more subtle, for instance playing opera music to celebrate one’s inner diva, and also to home-making practices in which gay and other identities and interests are combined, thus expressing the normality of being gay. Although these latter practices may appear ‘homonormative’, for Pilkey they are rather alternative ways of queering heteronormativity at home. This corresponds with work on home-making practices of heterosexual men, that are found to nourish various alternative manifestations of masculinity other than hegemonic masculinity (Gorman-Murray, 2013).
Methods of data collection and analyses
For the research informing this article, multiple methods of investigation were used. The first is a survey completed by 115 older LGBT adults aged 65 years and over. This survey was composed of six parts, with Part A asking filter questions to ensure respondents met three criteria: self-identifying as LGBT (to be precise: as ‘pink’ – a notion which encompasses LGBT+ identities yet is more widely accepted among older generations in the Netherlands than a term like ‘queer’); being at least 65 years of age (to avoid an overrepresentation of respondents aged between 50/55 and 65); and currently receiving at least one form of health and social care a month. This latter criterion has helped to ensure a focus on experiences with care and services that are most relevant to the AIP experience. These include home care, home aid, informal care, day care, and meals and transportation services, but visits to physiotherapists, dentists and medical doctors only insofar as these occur frequently, and have an impact on the experience. Toward the end of the survey collection period I relaxed this criterion a bit in the case of people who received care in the recent past and can be considered experienced care users. The share of respondents currently receiving monthly care or support is 74%.
Part B asks questions on experiences and preferences with respect to health and social care, adapted from Davis (1998), including an open question about the possible benefits of openness to caregivers; Morten, Farmer-Smith, Smith et al. (2012); and previous surveys administered in two Dutch cities (Felix and Dun, 2016; Van Eijck et al., 2017). Parts C and D borrow from the same sources and ask, respectively, about participation in social activities and social contacts, and about informal support networks. Part E administers questions adapted from Burdon’s Openness Scale (Burdon, 1996; see also Orel, 2014). The Cronbach’s alpha of this scale is 0.84. Part F, finally, asks about respondents’ sociodemographic characteristics, borrowing questions about sexual orientation and gender identity from the Netherlands Institute for Social Research (Keuzenkamp et al., 2012; Kuyper and Vanden Berghe, 2017; Van Lisdonk and Kuyper, 2015), which publishes periodically on LGBT emancipation. Questions about housing were taken from a previous research on AIP to which the author contributed (De Kam et al., 2012) and the outForever (2019) survey published by an Amsterdam-based citizen initiative. The survey was pre-tested with six older people (lesbian or gay, one bisexual woman), and questions and answer categories were revised on the basis of their comments.
Survey sample and procedure
The survey was available from February 2018 until March 2019, both online and in print. Four strategies were used to recruit respondents. About half of the respondents were recruited via the channels of COC Netherlands, a large advocacy organisation for LGBTI+ people with various regional chapters. COC Netherlands has a tradition of 30 years of organising meeting activities for older LGBT adults. Associated with COC Netherlands are so-called ‘Pink Ambassadors’, locally based volunteers committed to raising awareness about the life histories and situation of older LGBT adults. The organisation is also one of the initiators of the Pink Passkey, a quality mark for care and welfare organisations. I approached Pink Ambassadors, activity leaders, and spokespersons of organisations with a Pink Passkey with the request to distribute the questionnaire. Several ambassadors and group organisers were able to find one or two respondents, and sometimes qualified as respondents themselves. I visited five meeting activities in four different cities to introduce the research.
The second strategy entailed a publicity campaign in selected local newspapers that are free of charge and distributed weekly in the majority of Dutch households all over the country. The third strategy entailed distribution of the online version of the survey to the client panel of an advocacy organisation for care receivers. The remaining respondents were recruited through snowball sampling, which started with personal contacts of the researcher. Compared to the previous strategies, snowball sampling has a higher risk of selection bias in the sense of recruiting respondents within the same extended social network.
The resulting sample features 34 surveys that were not fully completed; 19 respondents, who used the print version of the survey, seem to have overlooked one or two questions. The other 15 respondents did not finish the online version, although they did answer most of the questions. This implies that the number of respondents is lower than 115 for some of the questions, approaching N = 100 for questions positioned toward the end of the survey. The decision was made to include these 34 surveys because the evidence base they do represent and the effort it has taken to collect them outweigh the loss of information caused by the missing answers.
Follow-up interviews
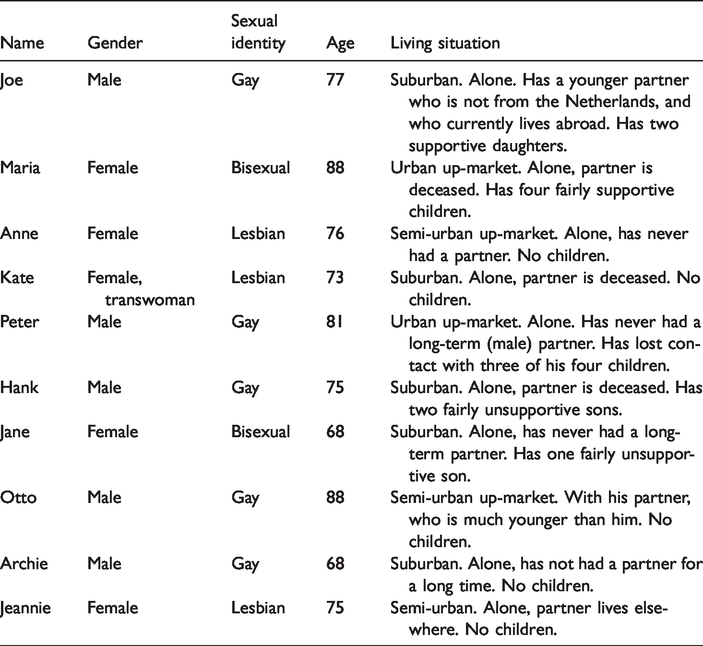
Ten respondents who took part in the survey and provided contact details were selected for follow-up interviews. All of them use care and services on a weekly basis, and reported one or more social issues, for example, a low involvement in social activities, dissatisfaction with social contacts, or issues with neighbours or family. They have diverse AIP experiences, from long-time living in the same home to recently moved. The follow-up interviews allowed me to probe into respondents’ life histories with the aim to understand how these histories are, directly and indirectly, connected to their satisfaction with care and services, and unmet needs. The interviews all lasted in between 1.5 and 2 hours and were recorded and transcribed verbatim. The interviewees are presented in Table 1. The names used are pseudonyms. Otto's partner participated in the interview.
Overview of participants’ follow-up interviews.
The survey and interview procedures complied with the Research Data Management (RDM) policy at Radboud University and the General Data Protection Regulation which went into effect in May 2018. Precautions taken included informed consent (separate procedures for the survey and the interviews), strict separation of survey questions and questions to respondents who agreed to a follow-up interview, and safe data storage. During the interviews, I carefully checked whether people were willing to elaborate on a particular question. For interviewees who had reported several social issues, I prepared contact details of support organisations and activities in the city where they live.
Analyses
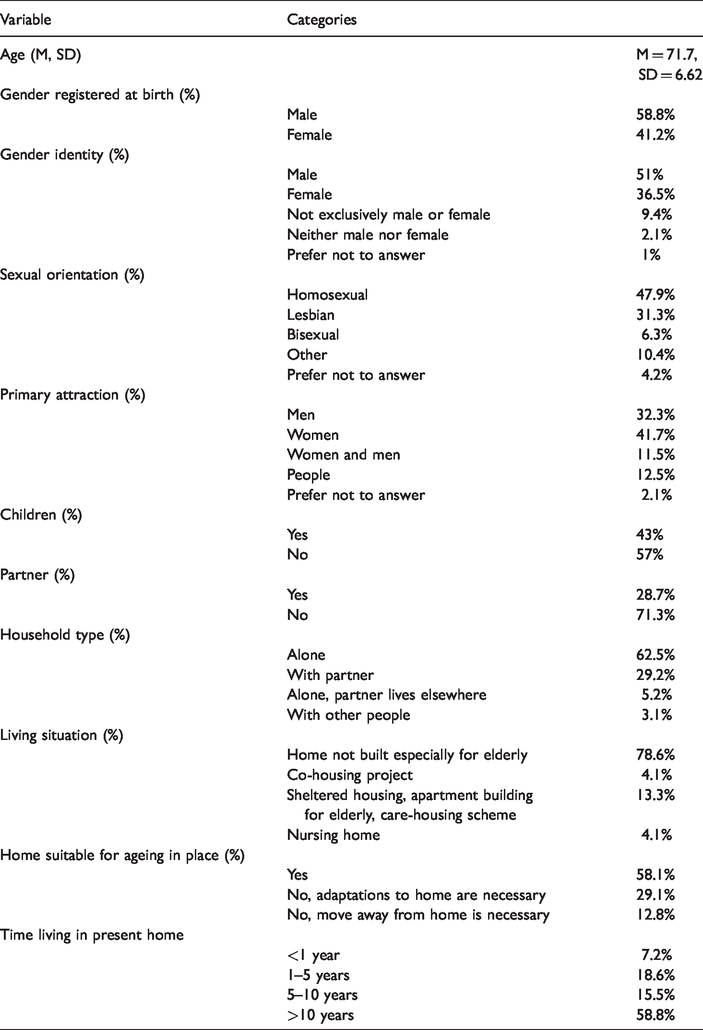
Survey data were analysed using simple SPSS techniques such as frequencies and crosstabs. The non-probability sampling procedure applied, as well as the lack of insight into a target population of LGBT care receivers aged 65 years and over, imply that the findings cannot be generalised and should be interpreted with caution. However, the statistics lend themselves well for additional qualitative analysis, bringing them into dialogue with background literature and interview data. The sociodemographic characteristics of the survey respondents are presented in Table 2.
Sociodemographic characteristics of older lesbian, gay, bisexual, and transgender adults (N = 115).
The follow-up interviews were coded with an inductive coding procedure, guided by the overall aims to expose experiences with AIP in the home and the ageing environment, and experiences with receiving health and social care while ageing in place. Following the coding process, a qualitative content analysis was conducted using ATLAS.ti, in which quotations were interpreted as representations of shared themes. The process of aligning individual quotations and emergent themes was rehearsed until no more new substantial ideas about new themes or reformulation of themes were out on the table.
Three overarching themes have resulted from the analyses. The first theme is experiences with AIP in ordinary ageing environments, notably urban extension areas. A second theme is experiences with AIP and care-receiving in the home, in which hitherto separate discussions about negotiating openness to caregivers and home-making practices come together. The third theme concerns the challenges to include older LGBT people in LGBT community activities and neighbourhood-based activities.
Findings
Older LGBT people and ordinary ageing environments
The results presented in Table 2 show that 82.7% of respondents are currently ageing in place, with close to 60% percent having lived in their current home for more than 10 years, 41.9% considering options to age in the ‘right’ place, and 17.4% already having opted for relocation. The interview findings, accordingly, provide further insight into the ageing environments where people live. While some interviewees, such as Maria and Otto, live in up-market (semi-)urban areas, others live in more mundane, ordinary ageing environments. Joe, Kate, Hank and Jeannie live in urban extension areas developed in the 1970s and 1980s, which count for 20% of housing stock in the Netherlands (Wassenberg and Lupi, 2011). Located at the fringe of cities, these areas are not especially poor or working class, yet they are increasingly less popular among city residents, who move into these neighbourhoods only if there are no other options. As a result, these neighbourhoods are characterised by low levels of experienced quality of life and social cohesion (Wassenberg and Lupi, 2011). This experience resonates, for example, in the words of Kate, who herself has moved to such an area because she was able to buy a house there: ‘No, well, you are just being ignored … [p]eople all live parallel lives.’
Also Joe laments a lack of social contacts: R: Do you feel attached to this living environment? J: Well not very much. R: Cos you have lived here for quite a long time uh? J: One and a half years ago I had a dog. Always when you do your round and you are walking, you have much more contacts. And now when I am outside people just pass me by. The contacts have gone. You don’t have it anymore, just ‘hi’ and a wave from a distance and that’s it.
Other characteristics relevant to ageing in place with care experiences.
Yes, two doors down. I had quite a problem with them, the wife even called on the door here and did this [gesturing] … It went like ‘dirty faggot’ and ‘you left your wife’ … When my boyfriend was there, it went well. But I only had to walk past that door and … Those children called me names as well. They are raised with it. We were happy they were gone.
Transwoman Kate fears an aggressive neighbour whom, she says, does not want to have contact with such a ‘strange bird’. After this neighbour accused her of neglecting problems with the surface on which both of their houses are built, Kate suffered mental and financial problems that took some time to resolve.
Jeannie remembers with indignation comments from local children, which were not directed towards her yet made her anxious: J: A boy in the neighbourhood, oh God, he used to yell ‘fags!’ through the street and, well … R: Why did he do that? Just because he could? J: Oh well, in the past, there just used to be children who would curse ‘dirty faggot’. R: The most widely used term of abuse … J: Probably yes uh? But well, that came close.
Further, the interview with Anne, who has moved to a senior apartment a few years ago because she was no longer able to maintain a large garden on her own, reveals that ageing in the right place can lead to new worries about neighbours:
A: It is possible that it is my own problem, of how do I deal with it in this apartment building. That may have been it [positive answer to survey question about problems with neighbours], and what do I show, what do I not show. Do I talk about it or not. People do not talk about it. It’s accepted and not accepted here.
R: If no one knows, you may not run into trouble.
A: But it sticks with me, that’s the point.
Anne’s caution backfires on her in the sense that she is experiencing discomfort in the contact with neighbours that will not go away until she feels safe enough to be open to them – a discomfort that may well be felt by many older LGBT people who decide to move in order to age in the right place.
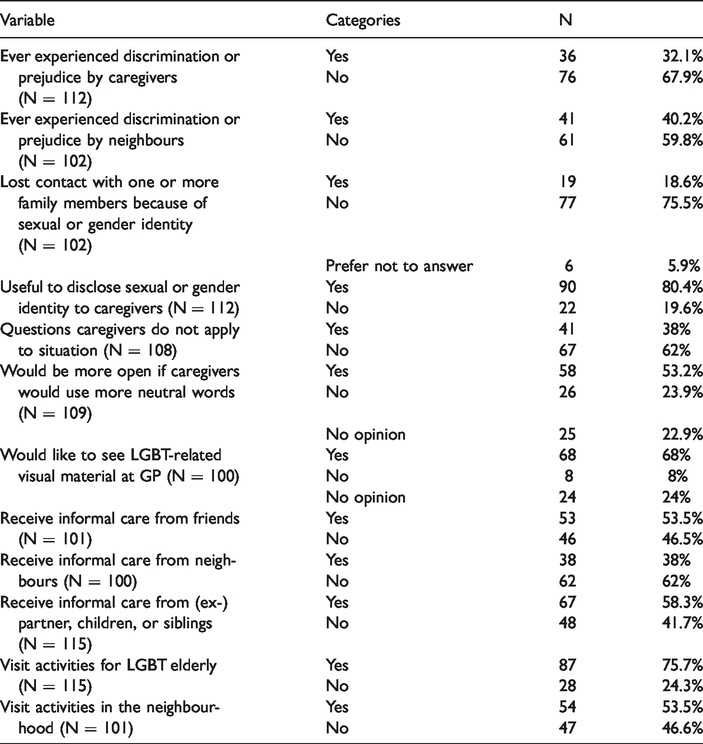
Whereas 38% of survey respondents receive informal care from neighbours (Table 3), the only interview respondent with functional neighbours is Otto, who is also the only one living with a partner. Otto and his partner have a loyal circle of neighbours who regularly cook for them. His partner explains this by the fact that they live in a liberal and affluent large village, where Otto is known as an informal carer himself: P: I think that what makes a difference in his case that he is accepted in the neighbourhood is that he has helped many people all his life and the whole neighbourhood knows that. How many AIDS-patients that you helped did you host here, at home? O: Well at home two, but some twelve more I attended to every day.
Experiences with ageing in place and care-receiving at home
The second theme discusses the issue of openness in more detail, zooming in on care-receiving in the home as both a highly relevant space for expressing LGBT identities, and as an increasingly important space of care. Table 3 shows that over 30% of respondents have experienced discrimination or prejudice from formal caregivers with respect to their sexual orientation, in a small number of cases in combination with their age or class position. However, the survey also shows that respondents have almost always, with very few exceptions, disclosed their identity and/or life history to caregivers, and that this openness almost always improves the perceived quality of contact with caregivers. At the same time, the reverse, namely that the quality of contact decreases with openness, is never the case. The idea that ‘the benefits of disclosure are significant’ is only briefly hinted at in the literature (Grossman et al., 2000; Steele et al., 2006, in Hughes and Kentlyn, 2011: 439), but emerges as a crucial finding from the survey part of the research. The many responses to an open question about the possible benefits of openness included visibility (‘If you are invisible, you don’t exist’), the quality of contact (‘Makes contact easier’), sameness and difference (‘For sure it is useful! Straight and LGBTI people are equal, but different. Attention to their life story, loneliness, feelings of safety is very important’), and normalisation (‘The advantages depend on whether you have fully accepted yourself as a lesbian, regarding it as a normal lifestyle. My experience is that the more normal I find it, the more I am accepted for who I am’).
The interviews revealed a somewhat more complex picture, however. Hank, for example, receives personal care at home for a number of medical problems, including a sexually transmitted disease, from a team of personal caregivers. Hank explains: ‘Well, you never know in advance who will come, it’s a rotation schedule. So in itself it is quite normal [not to know who will come]. They are with about ten [caregivers], and it rotates, all the time. Sometimes I happen to know, but most of the times I do not.’ This implies that Hank, with his sensitive health condition, has to come out to each of these caregivers, and again in each new care relationship. To deal with this situation, Hank has devised a twofold coping strategy. One strategy is having his sexual identity registered in his medical file: ‘Then they don’t have to ask questions like ‘how is your wife’ or ‘do you have a girlfriend’ or one of those things. I’m not keen on that.’ The other strategy, applied in the case of home aids, is even more pro-active: My regular home aid had been here three, four, five years. She left the organisation after a conflict, she had been here for five years. So I was assigned a new one. Then someone enters the house and I think after five minutes, this isn’t going to work. Then I let her go and I think well, bye, somebody else next time. At some point a lady came in and there was a click rightaway, well then I tell it, because I want to keep them. Then I think they should know, that is much easier, also for them.
The interview with Joe revealed that, although he did not have a preference for a likeminded caregiver when he first started to receive home aid, he enjoyed the ability to connect around gay men’s issues with his gay home aid so much, that he changed care organisations when the home aid did. This suggests having an LGBT-identifying caregiver may add an emotional layer to the care relationship one may not expect in advance.
Grigorovich (2016) shows that older lesbian and bisexual women want caregivers to demonstrate their awareness about and openness to sexual diversity in the language they use and the questions they ask. In the present research, more than half of the respondents can imagine being more open if caregivers would use more neutral wordings, and 38% of respondents think that the way they are addressed in the language used and questions asked by their caregivers insufficiently applies to their situation (see Table 3). Peter, for example, who, like 18.6% of respondents (see Table 3) has lost contact with his family after his coming out, struggles with the fact that his caregivers mention their grandchildren so often: ‘But I have to say, that hurts. And that does not have to do with being gay but I always struggle very much with the people here if they are rambling on about the children and the grandchildren’.
The case of Otto and his partner show another way in which LGBT lifestyles feed in to the care relationship. The partner explains: Just like this week, we started to receive home aid recently, because I have to do everything, and now there is home aid. And this home aid enters saying ‘I have to leave half an hour earlier today because I need to go to the dentist’. Then I think yes, what a coincidence for us. I help her with cleaning, and when she is there I start cleaning too so we do it together. I really have the idea, [she thinks] I can do this with them because that boy can still do it all by himself. And the same thing with home care!
The interviews display a range of domestic materialities that signal clues about LGBT life histories and identities. Hank, for example, displays homoerotic art and rainbow flags in his home. Jane, by contrast, expresses her (bisexual) identity in a subtle way. In the course of my interview with Jane, I became aware of a screen saver on the computer behind her, showing pictures of movie star Nicole Kidman. Starting out with one picture, the screen slowly filled with dozens of Kidman pictures of memorable roles and red carpet appearances. As a young teenager, Jane lived in various places of foster care, both within private homes and in an institutional setting. All but one of these places were very unsafe for Jane, which has had ramifications for her ability to relate to others. In the course of her life, Jane’s bisexuality has revolved around sexual involvement with opposite-sex couples. She much regrets never having had a romantic relationship with another woman, but has not been able to practice or negotiate alternative meanings of bisexuality. As a bisexual person, she does not just pass as straight (Maliepaard, 2017), she is invisible to the caregivers who enter her home – yet her bisexual life history is related to her overall well-being.
Yet other interviewees mingle relatively subtle clues, such as photos of a deceased partner, with other materialities that are important to them, such as books (Maria) and self-made sculptures (Jeannie). For these interviewees, having led a lesbian lifestyle is explicitly only one part of a multiple identity (see Pilkey, 2014). Clues about Archie’s sexual orientation can be found not so much in his home, but online, in LinkedIn posts, where he writes about his volunteer work. Like in the case of Jane, caregivers to Maria, Jeannie and Archie may not be able to pick up signs that could actually help open up conversations that in turn could improve their satisfaction with care relationships, even if they emphasise normality in their home-making practices.
Finally, lack of openness may be relevant to the provision of informal care, too. The survey shows that less than 30% of respondents have a partner, 43% have children (Table 2) and respondents without children appear to receive informal care from friends slightly more often than those with children (crosstab indicating 45.7% versus 39.6%). This resembles the situation of Anne, who neither has a partner nor children yet does have functional social contacts. Recently, Anne was hospitalised with appendicitis. When she found herself suddenly released after her operation, she struggled greatly with the transfer from the hospital to her home, not knowing where to begin organising help. She attributes this struggle to having been closeted until the age of sixty, never having had a partner, and having grown used to resolving everything by herself. This suggests that a need to learn to mobilise social contacts may coincide with a life history of closetedness.
LGBT community activities and neighbourhood-based activities
The third theme that emerges from the empirical material is the way in which older LGBT people ageing in place are supported by the LGBT community and by activities in the neighbourhoods where they live. In the Netherlands, meeting activities for older LGBT people are organised by local chapters of COC Netherlands that serve the wider region of a city. These activities usually take place in LGBT community centres in inner-city venues. Table 3 shows that 75% of respondents visit LGBT community activities, and many of these indicated that they visit meeting activities for older LGBT people. This is especially the case for respondents who are open about their identity and/or life history in general, and somewhat less so for people who are less or only partly open in general (crosstab indicating 85.5% versus 61.1%). Of the 24% who do not visit community activities, 40% say this is because they meet too few people their age there, and 16% because they fear ageist attitudes. Also the interviews revealed a number of critical ideas about LGBT community activities and spaces (see also Formby, 2017). Some respondents do not like the ways in which LGBT identities are presented in community activities. Archie, for example, is critical about how hypersexualised performances have come to dominate community activities. Maria dislikes practices of claiming space coming from the more activist corners of the LGBT community, which she finds loud and unpleasant (especially poor choir singing is a thorn in her flesh).
Joe, Jane and Kate, by contrast, were interested in linking up with the community, but have not managed to do so. They have visited meeting activities for LGBT people, but have not been able to join in. Joe experienced that atmosphere fell flat: I went to COC, over at the [name of street]. I went there twice, but I find the atmosphere uninviting and they are just looking at you and almost nothing is said. I managed to talk to one guy and that is what I told him. He asked how do you like it here? I replied well, I think it’s uninviting. Then I did not go there again. I find it so uninviting. J: When I started to live here, I went to COC once when I saw on the Internet that they organised evenings, but I did not feel at home in one way or the other. I, if you think you go there and they see you entering there and ask you where and how. That no one says, come-on I’ll show you. Well, that is what I found a bit difficult and they were all standing together in small groups and you don’t know what to do. R: …that is a pity, yes. J: Because I had rang them; oh you can just walk in. And yes, it’s there and then and I arrived there, and I did have a drink, but no one said, are you a newby here and whatever. And no one came over to me. R: What a pity. J: I think yes, that is not going anywhere. And I am not shy, but … R: It has to be a two-sided effort, yes, yes. Do you feel the need now to…? J: Back then I was probably also, a bit older, that they thought, what is this old woman doing here, for there were a lot of young people.
Some people have withdrawn from clubs and activities when they started to become more frail. Only one survey respondent reported lack of transport as an insurmountable barrier, others get by, sometimes with a little difficulty. Hank, for example, a proud coordinator of the monthly meeting activity in his city, manages to bridge the 8 km distance on his mobility scooter, the large pan of soup cooked especially for the occasion firmly placed between his legs and the scooter frame. Open answers of survey participants respectively, ‘My health doesn’t allow it’ and ‘I don’t go out the door too much anymore’ suggest that some people do not have the energy any more to invest in the groups. Pete explains that in his case, his decision to withdraw was made on the basis of growing frailty coinciding with changes in the composition of the group of volunteers at the local COC chapter that he was also volunteering for.
Finally, Table 3 shows that 53.5% of respondents visit activities in the neighbourhood. The nature of neighbourhood activities varies, from low-threshold meeting activities to meeting groups organised by social work professionals. Possibly, some of these activities may be an alternative to LGBT community activities that are experienced as less attractive because of (perceptions about) accessibility, ageism, atmosphere, or a combination. However, it is not self-evident that neighbourhood-based activities are able to include older LGBT people either. Jeannie and Archie have experienced group conversation falling silent after talking about having been left by a female partner (Jeannie), and a volunteer turning red after bringing up the issue of older LGBT people (Archie). Experiences such as these may cause people to suppress their LGBT identity and/or life history, to various degrees of resignation and dissatisfaction.
Conclusion
Since LGBT ageing now and in the future takes place in private homes and home environments, at least for many older LGBT people for a prolonged period of time, there is an urgent need to understand their experiences with care and support. The present article has studied how older LGBT people are enacted as care-receiving subjects (Tronto, 2013) while ageing in place with care, by means of a survey and interview research. Due to the sample size, the sampling procedure and the lack of a target population, the scope of the study is limited. The difficulty to relate findings to each other in a meaningful way without drawing heavily on background literature poses another limitation. Further, the emphasis on the Netherlands, with its relatively high social acceptance of LGBT identities and lifestyles, implies that findings cannot be generalised to other countries.
Given these limitations, the contributions to the literature on LGBT ageing in place are threefold. First, the study entailed a shift in focus from expectations about (see Boggs et al., 2017; Willis et al., 2018) to current or very recent experiences with care receiving, showing that openness is beneficial for contact with caregivers. In this respect, domestic materialities and broader home-making practices were identified as sources of understanding which could potentially improve the quality of this contact. This substantiates the idea that home-making practices, even as private expressions of LGBT life histories and identities, may have a transformative dimension beyond the homespace (see Gorman-Murray, 2013; Pilkey, 2014). Despite this, the fact that time is tight in home care and support may create particular problems for older LGBT people and their informal carers. Second, extending the findings of Willis, Raithby and Maegusuku-Hewett (2018), the study showed that variety in ageing environments relates to variety in AIP experience. The person–environment fit of older LGBT people who live in ageing environments that do not accommodate LGBT ageing well may be compromised, either directly through discrimination and prejudice from the side of neighbours, or indirectly through a lack of place attachment. Also ageing in the right place (Golant, 2015) may pose challenges to contacts with neighbours. This suggests that AIP research using the notion of person–environment fit may benefit from a stronger engagement with (intersecting) identities (see Ziegler, 2012.) The third contribution is a deeper understanding of how LGBT life histories and identities are relevant to care needs and preferences, sometimes in ways that were unexpected for respondents themselves. This, once more, underlines the need to conduct research on LGBT-friendly care and services with people who actually are care receivers and are able to relate experiences of subject formation and care-receiving.
On the basis of these contributions, a number of recommendations for providers of health and social care can be made. Seconding other authors in the area of LGBT-friendly service provision, it is highly recommended to invest in caregivers’ awareness and knowledge about older LGBT clients (see Hughes et al., 2011). For caregivers working in neighbourhood-based teams, this may revolve around sensitisation about how LGBT lifestyles might be displayed in people’s homes, both in verbal and through home-making practices. Being more aware, caregivers could then be more pro-active in signalling their openness towards older LGBT people. To prevent further pressure on the shoulders of caregivers, it may make sense to direct staff trainings at one or two team members who can share with colleagues. For professional organisers of meeting activities in neighbourhoods and, by extension, volunteers involved in these meetings, this would include learning the moderating skills to encourage older LGBT people to share stories in a safe way and to refer casually, but regularly, to LGBT issues. Subtly queering meeting spaces with visual material would also help in this respect. In addition, a need can be identified to develop partnerships with the LGBT community for a more systematic knowledge exchange, not only about LGBT issues but also about ways to include newcomers and people who may be at risk of dropping out. Alongside these efforts, however, follow-up research on the experiences of older LGBT people ageing in place is needed in order to establish a longitudinal evidence base for the critical assessment of neighbourhood-based support structures that may limit people’s choice for providers, and providers’ options to invest in sexual and gender diversity.
Footnotes
Acknowledgements
The author would like to thank the two anonymous reviewers and the special issue guest editors for their careful reading of the manuscript and their constructive feedback, and Bob Baxendell and Simone Haarbosch for research assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The research presented in this article was funded by a VIDI-grant from the Netherlands Scientific Organisation (NWO), grant number 452-16-008.