
Abstract
This article reports on findings from the quantitative phase of a two-year research project designed to explore end-of-life care experiences and needs of lesbian, gay, bisexual and transgender people. We draw on a subset of the sample (N = 180/237) to analyse the relationship between advance care planning, sexual orientation, living arrangements and self-rated health. The results contribute to a growing body of evidence on how sexual minorities approach and make decisions on advance care planning. A greater understanding of such patterns could help inform the way healthcare professionals engage in conversations about end-of-life care planning with older LGB people.
Introduction
Amid increasing levels of chronic disease and a rapidly ageing population, there is a growing emphasis in the international literature for individuals to engage in advance care planning (ACP) conversations between themselves, their families and healthcare providers to help inform shared decisions about care and treatment at the end-of-life (EOL) (Brighton and Bristowe, 2016; Seymour and Cassel, 2017). The term ‘advance care planning’, refers to a mechanism for individuals to establish and record decisions about future healthcare that take effect when they lose the capacity to make informed decisions (see NICE, 2018; SCIE, 2016). However, very few people in the general population engage in formal conversations and planning about EOL or advance care planning (see Fagerlin and Schneider, 2004). 1 Research suggests this is often due to lack of knowledge, individuals’ avoidance or fear of talking about death and dying, ineffective communication between the patient, family members and healthcare professionals, or feeling overwhelmed by the whole process (Bernacki et al., 2014; Brighton and Bristowe, 2016; Fowler and Hammer, 2013; Simon et al., 2015; Wright et al., 2008; Zhang et al., 2009). Without effective advance care planning, people with a terminal illness or condition may need to engage in complex decision-making processes during a time of great uncertainty or when suffering from significant physical and cognitive changes and/or emotional distress (Banner et al., 2018) or, at worst, have lost capacity to make decisions, thus requiring others to do so without their guidance.
There are additional challenges for lesbian, gay, bisexual and transgender (LGBT) people. Today’s LGBT older adults belong to a generation that experienced criminalisation and social sanctions and whose sexual orientation or gender identity was deemed deviant or abnormal (Heaphy, 2007). Unsurprisingly, they may be less open to disclose their sexual orientation than younger LGBT people (Almack et al., 2010), especially at times of feeling frail, vulnerable or seriously ill (Almack, 2016; National End of Life Care Programme, 2012). For instance, some studies have reported that LGBT people are less likely than others to seek healthcare in a timely manner, particularly due to discomfort in disclosing their sexual orientation and/or gender identity to service providers (e.g. Auger, 2003; Hughes, 2007; National End of Life Care Programme, 2012; Orel, 2013; Smolinski and Colon, 2006). LGBT older people may fear that health and care professionals could still discriminate against them and/or that their ‘families of choice’ – one’s own chosen family-like relationships rather than family of origin, (McCarthy and Edwards, 2011) – may not be involved in the way they wish (Almack et al., 2015a; Bristowe et al., 2018). These barriers can have serious consequences and complicate LGBT people’s experience of EOL care, as well as the experience of their partners and others in their circle of care. Such barriers are underpinned by discrimination, marginalisation and heteronormativity, particularly in the assumption of health and social care professionals that all people using services are heterosexual and thus they often fail to provide appropriate and LGBT-friendly services (Care Quality Commission, 2016; Cartwright et al., 2012; Marie Curie, 2016).
In recent years there has been a growing number of studies paying attention to the role of older adults’ sexual orientation in advance care planning (e.g. Addis et al., 2009; Almack, 2018; Almack et al., 2010; Almack et al., 2015b; Cartwright et al., 2012; de Vries et al., 2009; Duffy and Healy, 2014; Gendron et al., 2013; Higgins et al., 2011; Hughes and Cartwright, 2014, 2015; Kcomt and Gorey, 2017; Stein and Bonuck, 2001). Available evidence highlights concerns that LGBT people’s partners, ex-partners and friends are sometimes not fully recognised as having a legitimate role in end-of-life decision-making by biological family members and healthcare providers (Higgins et al., 2011; MAP/SAGE, 2010). It can thus be especially important for LGBT people to engage in advance care planning, which facilitates the documentation of the individual’s wishes and preferences at the end-of-life and provides crucial support for those nominated to be involved in decisions about their care. As Hughes and Cartwright (2014) point out, early engagement in advance care planning conversations can circumvent heteronormative assumptions about end-of-life care (e.g. biological family members rather than partners or friends are automatically first in line to become substitute decision-makers).
Our knowledge of how LGBT older people experience and plan ahead for care in late life and at the EOL in the UK is still limited and requires further consideration. There has been a growing interest amongst health and social care professionals to improve their knowledge and understanding of how to provide sensitive and quality EOL care to LGBT people (e.g. Care Quality Commission, 2016; National End of Life Care Programme, 2012). However, the emerging evidence also suggests there is still limited awareness and knowledge amongst health and social care professionals to address considerations relevant to sexual orientation and gender identity when discussing EOL issues (Bristowe et al., 2016; Simpson et al., 2018).
Existing research has shown evidence of inequality in the provision of health and care services experienced by LGB older people in comparison with heterosexual people, due to homophobia, biphobia and heteronormativity. This is particularly apparent in respect of concerns over the implications of ageing, specifically in issues regarding care provision (e.g. EOL care), health and living arrangements. Studies also suggest that when compared to their heterosexual counterparts LGB older people, and particularly gay and bisexual men, tend to live alone and are more reliant on friendship than family support (Houghton, 2018; Guasp, 2011; Kim and Fredriksen-Goldsen, 2016). This certainly has practical implications for health and social care professionals to understand the needs and preferences for EOL care for LGB older people living alone, who might also be more vulnerable to loneliness and social isolation (see Cartwright et al., 2012; Chu et al., 2017; Sullivan, 2014). Furthermore, as argued by Cartwright et al. (2018), when LGBT people already face multiple obstacles to having their EOL wishes respected, if health and social care providers do not understand or support a partner’s legal right to make such decisions, the problem is exacerbated. We also know that LGB people have specific health-care needs. Lesbian women and gay men have greater all-cause mortality than heterosexual people and are more likely to present with more advanced disease (Bristowe et al., 2018; Gorman et al., 2015). Thus, following an exploratory and descriptive approach, the aim of this article is to uncover how older LGB people address EOL advance care planning and how this differs by gender, sexual orientation, age, living arrangements and self-rated health.
Method
Research design
The research reported in this article was part of a larger mixed-method study ‘The Last Outing’ (Almack et al., 2015b), designed to explore EOL care experiences and needs amongst LGBT older people (aged 60 and over) in the UK (covering England, Scotland, Wales and Northern Ireland). The study was funded by the Marie Curie Research Programme and approved by the Research Ethics Committee of the University of Nottingham. Voluntary participation, anonymity and confidentiality were ensured. The overall research design and its implementation were informed by a steering committee comprising key stakeholders, including representatives from Age UK and members of the LGBT community.
Participants
The study participants comprised 237 self-identifying LGBT individuals aged 50 to 87 living in the UK. Respondents were recruited through different techniques such as community-based convenience sampling, snowballing, networking and online advertising (e.g. weblogs, Twitter) in an effort to obtain a great number and diversity of participants (e.g. gender, age, ethnicity). The survey was mainly administered online via SurveyMonkey; hard copies were also administered throughout LGBT organisations and upon request to individuals. Sampling was purposive and non-random, and we relied on respondents’ self-definition of sexual orientation. The inclusion criteria were that individuals should be (1) aged 60 and older (or under 60 but with a LGBT partner aged 60 and older), (2) self-identified as LGB and/or T, whether currently in a same-gender relationship or not, (3) currently living in the UK, and (4) with capacity to give informed consent. The survey was distributed so broadly to LGBT communities there was no way of assessing how many people actually received it, and therefore we were unable to determine a response rate. Similar to other hidden and marginalised groups, obtaining a representative sample of LGBT older people is particularly challenging (Westwood, 2017). Furthermore, given the absence of reliable demographic data relating to the LGBT population in the UK, a representative survey sample is not yet possible to be accurately determined.
In this article, we draw on a subset of 180 LGB older adults of the main study sample. Despite strenuous efforts, we did not obtain sufficient data from transgender survey participants to produce any meaningful analysis. We return to this point in the later discussion but to note here, our presentation of findings is restricted to LGB participants. The majority of the participants in the subsample identified themselves as White British (88%), were university-level educated (63%) and considered themselves as being financially secure (78%). Most participants (63%) were living alone and just over half (52%) reported having a religious or spiritual belief, or another belief system. Table 1 offers an overview of the subsample characteristics.
Participants’ characteristics.
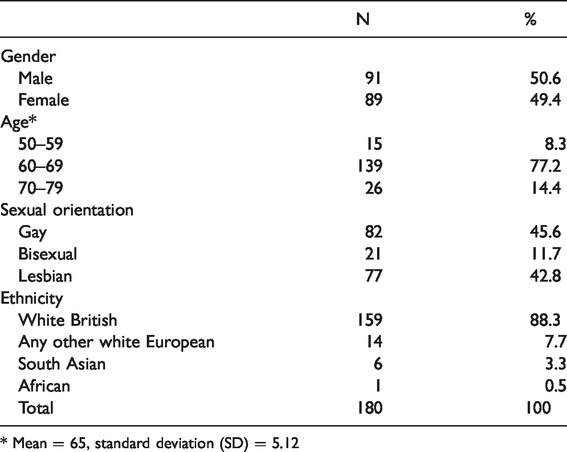
* Mean = 65, standard deviation (SD) = 5.12
Questionnaire instrument
The questionnaire designed included 81 questions developed from academic and grey literature, and some modified, with permission, from the Visible Lives survey (Higgins et al., 2011). The survey mostly comprised closed questions and scale of views/preferences with some open questions. Themes covered included sources of support and care; perceptions of accessibility to and satisfaction with health and care services; positive and negative experiences perceived to be linked to the participant’s sexual orientation and/or gender identity; and views on the need for specific or mainstream services. Sections of the survey pertinent to this article included thinking and acting on advance care planning; preferences for EOL care; living arrangements and self-rated health. For the present analysis we focus on the following items of the questionnaire: To assess how the respondents defined their sexual orientation, the question asked was: ‘Which of the following describes your sexual orientation?’ Answer options were gay, bisexual, lesbian, heterosexual, and others. To assess the notion of plans about care and treatment the statement used was: ‘I have thought about making plans for my preferences for future care and treatment’. The answer options ranged from strongly agree (1); agree (2); uncertain (3); disagree (4); or strongly disagree (5). To carry out the statistical analysis for this article, responses (1) and (2) were grouped together, and (4) and (5) were grouped together. To assess the notions of religiosity or spirituality the question used was: ‘Do you have religious or spiritual beliefs or another belief system?’ The answer options were yes or no. To assess respondents’ self-perception of physical health the question asked was: ‘How do you rate your physical health?’ Answer options were excellent, very good, good, fair, bad and very bad. For the present analysis, responses were grouped as good (including very good, good and fair) or bad (including bad and very bad). To assess respondents’ self-perception of mental health the question asked was: ‘How do you rate your mental health?’ The answer options were excellent, very good, good, fair, bad and very bad. Responses were also grouped as good (including very good, good and fair) or bad (including bad and very bad).
Data analysis
The survey data were analysed using univariate and bivariate descriptive analysis. For this subsample, the variables of interest were age, sexual orientation, living arrangements and self-rated health and advance care planning. First, we carried out a descriptive analysis to show the respondents and percentage of each variable analysed (Table 1). Second, we conducted a Chi-squared test to analyse the relationships between the variables of interest, which showed statistically significant differences in advance care planning across gender, age, and sexual orientation. The Chi-square test is highly sensitive to sample size, meaning that a reasonably robust association may not result as significant if the sample size is small (Mchugh, 2013). Despite the relatively small proportion of bisexual respondents (N = 21) in contrast to lesbian and gay respondents, we have deliberately chosen to keep our sample grouped according to their self-identified sexual orientation as this is indeed the focus of our study. Given the gap in the research evidence specifically on older LGB people, and particularly on older bisexual people, as we will show later, our findings on these groups, while not ‘statistically’ significant, nevertheless offer new insights into an underresearched area.
Results
Gender by sexual orientation and advance care planning
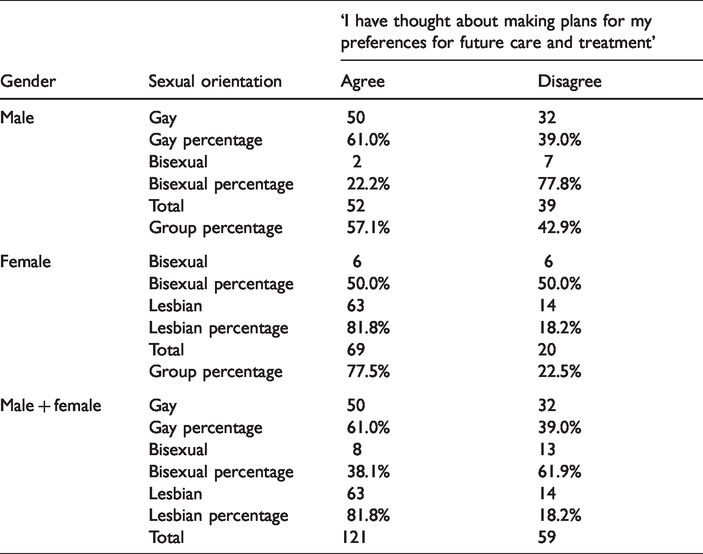
Results showed significant differences in the relationship between gender by sexual orientation and advance care planning (χ2 (2, N = 180) = 16.983, p < 0.001). Gay men were more likely to have thought about their EOL care and advance care planning than bisexual men (χ2 (1, N = 91) = 4.973, p < 0.05), whereas lesbian women were more likely to have thought about EOL care and ACP than women self-identified as bisexual χ2 (2, N = 89) = 6.033, p < 0.05). Overall, most respondents who self-identified as lesbian stated that they had thought about making plans for their EOL care, whilst most of the bisexual respondents reported that they had not thought about making plans for their EOL care and treatment preferences (Table 2).
Sexual orientation by gender and planning for future care and treatment.
Age by sexual orientation and advance care planning
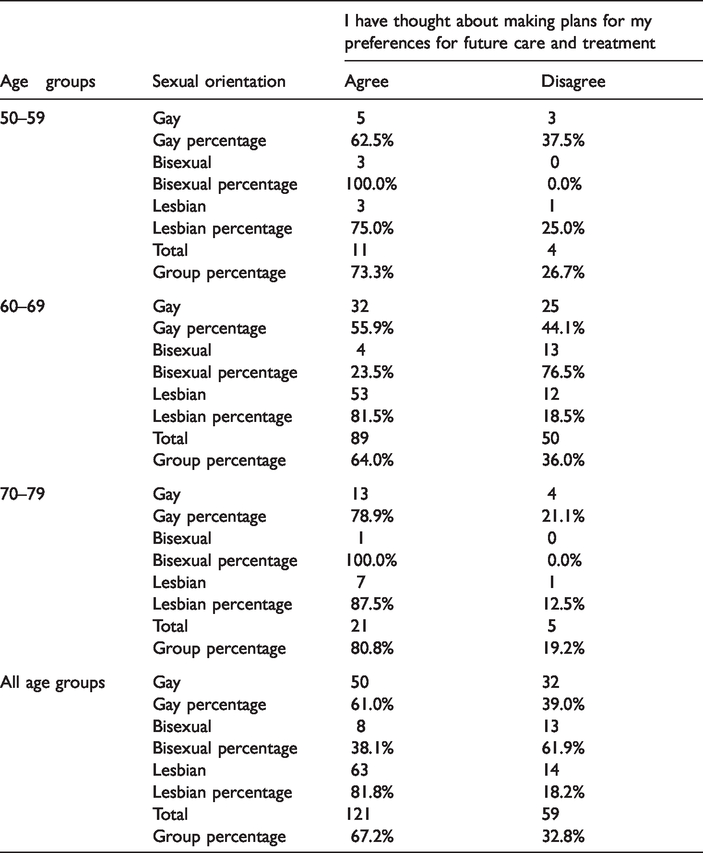
Table 3 presents the differences amongst the age groups in the relationship between sexual orientation and advance care planning (χ2 (2, N = 180) = 16.983, p < 0.001). Only the age group of 60–69 showed statistically significant differences χ2 (2, N = 139) = 22.299, p < 0.001). Within this age group, respondents self-identified as lesbians (N = 52) were more likely to have thought about making plans about their advance care and treatment than bisexuals.
Sexual orientation by age and planning for future care and treatment.
Living arrangements by sexual orientation and advance care planning
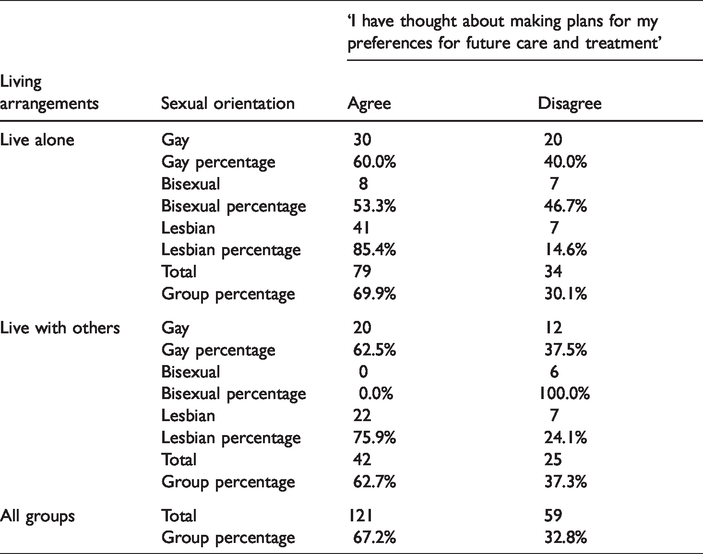
Our statistical analyses indicated that there were significant differences in living arrangements by sexual orientation and advance care planning (χ2 (2, N = 180) = 16.983, p < 0.001). The results in Table 4 show that those respondents living alone were more likely to have thought about making plans for their future care and treatment preferences in comparison to respondents who live with others (χ2 (2, N = 180) = 9.781, p < 0.05). Particularly, lesbians living alone were more likely to have thought about advance care planning than other sexual orientation groups. Furthermore, bisexual respondents who reported to be living with others were less likely to have thought about making plans for future care and treatment preferences (χ2 = (2, N = 67) = 12.233, p < 0.01).
Sexual orientation by living arrangements and planning for future care and treatment.
Age by sexual orientation and self-rated physical health
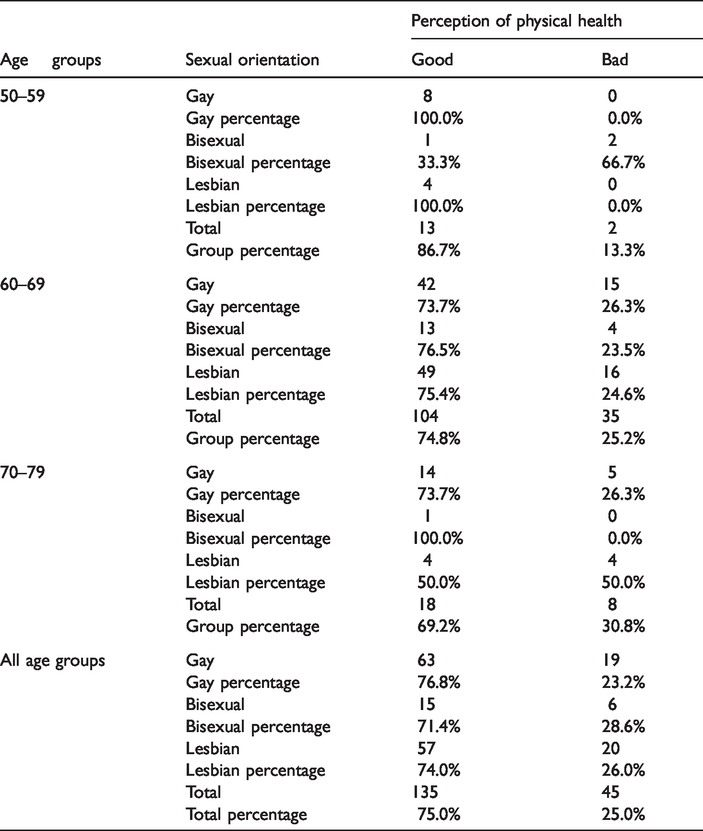
Analysis of the association between age by sexual orientation and self-rated health showed that only the age group of 50–59 presented statistical significance (χ2 (2, N = 15) = 9.231, p < 0.01). Within this age group, gay and lesbian respondents were equally likely to report having ‘good’ physical health, whereas bisexual participants were the only group that rated their physical health as ‘bad’ (Table 5).
Sexual orientation by age and self-rated health.
Finally, we ran another two Chi-squared tests, one to compare planning for EOL care and perception of mental health, and another one to compare planning for EOL care and spirituality; however, no statistical significance was found in either test.
Discussion
Our analysis presented in the article seeks to provide a better understanding of the role of sexual orientation, living arrangements and self-rated health in planning for late life and EOL care amongst LGB older adults. As older LGBT people are more likely to have experienced homophobia, stigma, discrimination and marginalisation throughout their lives, they tend to delay accessing health and social care services out of fear of health and social care professionals being insensitive or even actively hostile to their needs and preferences (Almack et al., 2015b; Marie Curie, 2016). Such fears or concerns exacerbate barriers for LGBT people in accessing EOL care. There may be an association to the uptake of ‘advance planning’ for future care and treatment amongst this group, due to a perceived lack of options, something that warrants further investigation.
In terms of advance care planning, lesbian respondents were found more likely to ‘having thought of making plans for future care and treatment’ than gay men or both male and female bisexuals. Our findings have some similarities here with findings reported by Stein and Bonuck (2001). From their lesbian and gay sample, they reported that women were significantly more likely than men to be aware of healthcare proxies. 2
In our study’s qualitative findings (60 in-depth interviews with a sub-sample of survey respondents), one commonly reported factor in avoiding thinking about making plans for future care and treatment was not knowing who to name as alternative decision-maker. This was raised more often by gay men and bisexual people, in part because of smaller circles of close friends and/or relatives than was the case for lesbian women; this may in part explain our quantitative findings reported earlier.
In our study, only the respondents in the age group of 60–69 were found to be more likely to have thought about making plans about their future care and treatment preferences than the younger group (aged 50–59) and older group (aged 70–79). This may be related to retirement, which usually begins within this age range and prompts changes in daily routines and habits which may contribute to a greater focus on thinking about plans for the remainder of one’s life and future care. However, this incidence is not exclusive to LGB people as it is also found in the general population of older adults. For instance, some other studies have found that a significant life event such as the sudden loss of one’s partner, family member, or friend, or the loss following sustained health-related issues often trigger people to think about advance care planning (Banner et al., 2018).
Another finding from our study identified the relationship of older LGB people’s living arrangements and EOL planning and preferences. Respondents living alone more often reported having thought about making plans for their future care and treatment preferences in contrast to respondents living with others. A previous study by de Vries et al. (2009) found conversely, that being in a relationship – that is, being part of a couple – was associated with a greater likelihood of having a will, a living will, or durable power of attorney. Thus it would appear that they had given advance care planning more thought, taking it through to documenting their thoughts and wishes. However our survey findings, supplemented by our qualitative findings suggest that people living alone might engage more actively in thinking about advance care planning for the very reason that they are not living with others who may help them in everyday activities; which, at the same time, may provide a motivation to think ahead about their care in later life and at the end-of-life. On the other hand, people living with others might not think of their advance care preferences as much because they tend to rely on each other in terms of care and support, forming a social and economic ‘safety net’ in later life as compared to older people living alone. In the discussion of the findings presented by de Vries et al. (2009), they additionally highlighted the need to be aware of the effects of legal recognition for same-sex relationships and the degree to which this may or may not influence and affect single and coupled people differently. This is beyond the remit of our article, but we would agree that jurisdictions with differing historical and legal contexts potentially limit the transferability and comparison of findings. This is an area for further exploration.
In our study, 63% of the respondents were living alone, which is consistent with several studies that suggest older LGB people are more likely to live alone in comparison to their heterosexual counterparts (e.g. Kim and Fredriksen-Goldsen, 2016). In the case of bisexual respondents who were living with others, these did not present any score in thinking about making plans for their future care and treatment preferences. None of our bisexual respondents mentioned making advance care plans and this was borne out in our qualitative investigations. However, as discussed earlier, we only had a low proportion of subjects in the sample with a bisexual orientation, an issue also reported in other studies of LGB older adults and their living arrangements (Kim and Fredriksen-Goldsen, 2016). Older bisexual people appear to be a hard-to-reach population but there is a clear need to develop greater consideration of bisexuality in future research (Monro et al., 2017).
In terms of the role of age and sexual orientation in LGB people’s self-perception of health, our study identified that gay respondents had a better perception of physical health compared to bisexuals and lesbians. This in part, may also explain earlier findings that gay men were less likely to have engaged in advance care planning or thinking. Bisexual respondents were the only group who self-rated their physical health as poor; this concurs with previous UK research which found that of all the larger sexual minority groups, bisexual people have the worst mental health problems including higher rates of depression, anxiety, self-harm and suicide. This has been found in the UK and internationally and is linked to experiences of biphobia and bisexual invisibility (Barker et al., 2012; Fredriksen-Goldsen et al., 2017).
Owing to small response rates, data from bisexual respondents are often merged with other sexual minorities for analytic purposes (Fredriksen-Goldsen et al., 2017; Jones, 2018). Wherever possible, it is important to disaggregate different sexual minorities to fully understand their experiences and further research is needed on the experiences of bisexuals in older age. Researchers, policy makers, and practitioners should be careful not to use findings from research studies with larger numbers of lesbian and gay respondents to extrapolate bisexual experiences – or, indeed those of transgender individuals (who may also identify as heterosexual, not necessarily lesbian, gay or bisexual). We have not been able to extend our analysis to include transgender respondents, but transgender older adults represent a population for which knowledge about the ageing experience and appropriate EOL care is especially lacking, albeit with exceptions such as the work of Witten (2014).
Conclusion
This study adds to a growing body of research evidence on how sexual minority identities approach advance care planning in later life and the differences by age, living arrangements and self-rated health. We acknowledge that there were some limitations to this study, which imply taking caution with some of the study findings and conclusions. On the one hand, the use of self-reported data may create vulnerability to answers bias; on the other, the convenience sample, as with most studies of LGBT ageing (see Cronin and King, 2010; Grossman, 2008; King, 2016) limits our conclusions and does not allow for the generalisation of the findings. Additionally, our comparisons to other research in this area are tentative due to different operationalisations of advance care planning. However, our aim was never this but instead to generate knowledge that may contribute to discussions to inform policy and practice on LGBT older individuals’ preferences of EOL care. Future research therefore could include larger samples and incorporate scales to measure key themes to explore gay, lesbian and bisexual older adults’ experiences of advance care planning. Transgender older adults deserve further attention in research, including in studies of advance care planning and it would be useful to compare LGB and T experiences with those of a similar heterosexual aged cohort.
A better understanding about how sexual minorities approach and make decisions on advance care planning could inform how health and social care professionals working with older LGBT adults engage in conversations on this topic with this population. We noted at the start of this article unique reasons as to why advance care planning and other preparations for care in late life and at the end-of-life for older LGBT people may be complex but important. Ultimately, by developing a greater understanding of the planning amongst LGBT older adults, the better we can support and understand LGBT experiences and improve their experience of ageing into late life and at the end-of-life.
Footnotes
Acknowledgements
We are grateful to all LGBT older adults who took the time to participate in our study as well as the many organisations and individuals across the UK who gave their advice and support, particularly during the recruitment phase. KA and MM participated in the design, collection and analysis of the data as well as the drafting of the manuscript. AB undertook all statistical analyses and contributed to the drafting of the manuscript. All three authors critically revised the contents of the manuscript and approved final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We want to thank the Marie Curie Research Programme for the funding and support, although the funder played no role in the design, collection, analysis or interpretation of the data.
Notes
![]() ).
).